Do depressed patients without activation of the hypothalamus—pituitary—adrenal (HPA) system have metabolic disturbances? Barbara Scharnholz a,1, * , Maria Gilles a,1 , Annika Marzina b , Marcel Kommer b , Florian Lederbogen a , Stefan A. Wudy c , Michaela F. Hartmann c , Sabine Westphal d , Heinz Ju¨rgen Roth e , Kai G. Kahl f , Andreas Meyer-Lindenberg a , Henrik J. Michaely b,1 , Michael Deuschle a,1 a Department of Psychiatry and Psychotherapy, Central Institute of Mental Health, Medical Faculty Mannheim/ Heidelberg University, 68159 Mannheim, Germany b Institute of Clinical Radiology and Nuclear Medicine, University Medical Center Mannheim, 68167 Mannheim, Germany c Steroid Research and Mass Spectrometry Unit, Division of Pediatric Endocrinology and Diabetology, Center of Child and Adolescent Medicine, Justus Liebig University Giessen, 35390 Gießen, Germany d Institute of Clinical Chemistry, Magdeburg University Hospital, 39120 Magdeburg, Germany e Laboratory Limbach, 69126 Heidelberg, Germany f Department of Psychiatry, Social Psychiatry and Psychotherapy, University of Hannover, 30625 Hannover, Germany Received 11 June 2013; received in revised form 2 September 2013; accepted 25 September 2013 Psychoneuroendocrinology (2014) 39, 104—110 KEYWORDS Depression; Metabolic syndrome; HPA system; Autonomic nervous system; Blood pressure; Fasting glucose; Body composition; Visceral fat Summary This study compared features of the metabolic syndrome between healthy controls and depressed patients without activation of the hypothalamus—pituitary—adrenal (HPA) system. After exclusion of non-suppressors to 1 mg dexamethasone, we included 20 depressed inpatients and 34 healthy controls in the analyses. We assessed HPA system activity (diurnal saliva cortisol profile, cortisol excretion), normetanephrine excretion as well as fasting glucose, lipid profile and blood pressure. With regard to body composition, we measured waist circumference as well as visceral fat and adrenal volume by magnetic resonance (MR) imaging. Five depressed patients (25%) and five healthy controls (15%) fulfilled the criteria of the metabolic syndrome according NCEP-ATP-III. Depression was significantly related with fasting glucose and negatively associated with mean blood pressure (BP) and, by trend, with low HDL-cholesterol. We conclude that depressed patients may have modest metabolic disturbances even in the complete absence of * Corresponding author. Tel.: +49 621 1703 1783; fax: +49 621 1703 2325. E-mail address: [email protected] (B. Scharnholz). 1 These authors contributed equally to this work. Available online at www.sciencedirect.com ScienceDirect jou rn a l home pag e : ww w. el sev ier. com/ loca te /psyn eu en 0306-4530/$ — see front matter # 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.psyneuen.2013.09.030

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Do depressed patients without activation ofthe hypothalamus—pituitary—adrenal (HPA)system have metabolic disturbances?
Barbara Scharnholz a,1,*, Maria Gilles a,1, Annika Marzina b,Marcel Kommer b, Florian Lederbogen a, Stefan A. Wudy c,Michaela F. Hartmann c, Sabine Westphal d, Heinz Jurgen Roth e,Kai G. Kahl f, Andreas Meyer-Lindenberg a,Henrik J. Michaely b,1, Michael Deuschle a,1
aDepartment of Psychiatry and Psychotherapy, Central Institute of Mental Health, Medical Faculty Mannheim/Heidelberg University, 68159 Mannheim, Germanyb Institute of Clinical Radiology and Nuclear Medicine, University Medical Center Mannheim, 68167 Mannheim,Germanyc Steroid Research and Mass Spectrometry Unit, Division of Pediatric Endocrinology and Diabetology, Center ofChild and Adolescent Medicine, Justus Liebig University Giessen, 35390 Gießen, Germanyd Institute of Clinical Chemistry, Magdeburg University Hospital, 39120 Magdeburg, Germanye Laboratory Limbach, 69126 Heidelberg, GermanyfDepartment of Psychiatry, Social Psychiatry and Psychotherapy, University of Hannover, 30625 Hannover,Germany
Received 11 June 2013; received in revised form 2 September 2013; accepted 25 September 2013
Psychoneuroendocrinology (2014) 39, 104—110
KEYWORDSDepression;Metabolic syndrome;HPA system;Autonomic nervoussystem;Blood pressure;Fasting glucose;Body composition;Visceral fat
Summary This study compared features of the metabolic syndrome between healthy controlsand depressed patients without activation of the hypothalamus—pituitary—adrenal (HPA) system.After exclusion of non-suppressors to 1 mg dexamethasone, we included 20 depressed inpatientsand 34 healthy controls in the analyses. We assessed HPA system activity (diurnal saliva cortisolprofile, cortisol excretion), normetanephrine excretion as well as fasting glucose, lipid profile andblood pressure. With regard to body composition, we measured waist circumference as well asvisceral fat and adrenal volume by magnetic resonance (MR) imaging. Five depressed patients(25%) and five healthy controls (15%) fulfilled the criteria of the metabolic syndrome accordingNCEP-ATP-III. Depression was significantly related with fasting glucose and negatively associatedwith mean blood pressure (BP) and, by trend, with low HDL-cholesterol. We conclude thatdepressed patients may have modest metabolic disturbances even in the complete absence of
* Corresponding author. Tel.: +49 621 1703 1783; fax: +49 621 1703 2325.E-mail address: [email protected] (B. Scharnholz).
1 These authors contributed equally to this work.
Available online at www.sciencedirect.com
ScienceDirect
jou rn a l home pag e : ww w. el sev ie r. com/ loca te /psyn eu en
0306-4530/$ — see front matter # 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.psyneuen.2013.09.030
activation of stress-responsive systems. Hence some metabolic disturbances in depressed patientsmay not be explicable by HPA activation. Additional factors are required to mediate the link betweenaffective and metabolic disorders.# 2013 Elsevier Ltd. All rights reserved.
Metabolic syndrome in eucortisolemic depression? 105
1. Introduction
It has been recognized for almost three decades thatdepressed patients suffer a substantially increased risk formetabolic syndrome (Kinder et al., 2004), diabetes mellitustype 2 (Wannamethee et al., 2005) and insulin resistance(Kan et al., 2013) as well as coronary artery disease (Rugulies,2002). Based on Bjorntorp’s groundbreaking observation thatstress and cortisol may cause abdominal obesity and themetabolic syndrome (Bjorntorp, 2001), psychiatric researchbegan to investigate the hypothesis that activation of thehypothalamus—pituitary—adrenal (HPA) system duringdepression may lead to secondary metabolic disorders. Infact, it has been shown in epidemiological studies that theimpact of depression on the development of the metabolicsyndrome may be, at least partially, mediated by cortisol(Vogelzangs et al., 2007). Moreover, studies in clinical sam-ples found a positive relation between HPA system activityand visceral obesity (Weber-Hamann et al., 2002) as well asinsulin resistance (Weber-Hamann et al., 2005). Thus, acti-vation of the HPA system may explain some, but not allfeatures of the metabolic syndrome in depressed patients.
In addition to metabolic disturbances, body compositionmay differ between healthy controls and depressed patients,not only with regard to the well-known effects of depression onvisceral obesity (Weber-Hamann et al., 2002) or bone mineraldensity (Schweiger et al., 1994). Adrenal volume has beenfound increased in depressed patients in several studies, whichindicates that adrenal volume may reflect long-term ACTHoverdrive leading to hyperplasia in this clinical population(Kessing et al., 2011). Thus, increased visceral fat and adrenalvolume can be considered proven morphological adaptationsto chronic stress and hypercortisolemia in depression.
However, not all depressed patients show signs of stresssystem activation. Interestingly, several studies failed todemonstrate increased HPA system activity in depressedoutpatients (Strickland et al., 2002; Peeters et al., 2004;Van Den Eede et al., 2006; Carpenter et al., 2009). Also, theclinical subtype may play a role with melancholic and aty-pical depression displaying different features of HPA regula-tion (Gold and Chrousos, 2002). Accordingly HPA activity wasconcluded to vary strongly between patient groups withpronounced HPA activation in depression with melancholicor psychotic features as well as in elderly patients (Stetlerand Miller, 2011), but not in patients with atypical depres-sion, less severe depression or depressed outpatients(O’Keane et al., 2012).
On grounds of these observations one may wonderwhether depressed patients without evidence for increasedHPA system activity may in fact be precluded from metabolicrisks. This hypothesis, to the best of our knowledge, hasnever been tested. In contrast, previous studies on metabolicdisturbances in depressed patients by our group and othersrather aimed at melancholic and hypercortisolemic
depressed patients (Schweiger et al., 1994; Weber-Hamannet al., 2002, 2005; Kessing et al., 2011). Therefore, our studyintended to compare symptoms of the metabolic syndromeand body fat distribution between healthy controls andmoderately depressed patients without activation ofstress-responsive systems as defined by a negative dexa-methasone suppression test.
2. Methods
2.1. Subjects
2.1.1. Ethical aspectsThe trial was registered at the German Clinical Trial Registry(DRKS00004324), was approved by the local ethics committeeand all subjects gave signed informed consent. The study wasconducted with inpatients at a university psychiatric hospitalin Germany. Healthy controls were recruited via ads in localnewspapers.
2.1.2. Inclusion/exclusion criteriaInclusion criteria for patients were (1) major depressionaccording DSM-IV criteria, (2) a score of at least 18 pointson the 21-item Hamilton Depression Rating Scale (HDRS), (3) nohistory of substance abuse or dependency (except nicotine),(4) absence of neurological or relevant medical disorders and(5) body mass index (BMI) below 35 kg/m2, (5) no dieting ormedication for hypertension, dyslipidemia, diabetes mellitus,(6) suppression of morning cortisol after nighttime dexametha-sone (morning cortisol <5 mg/dl after 1.0 mg dexamethasoneat 11 p.m.), (7) no pre-treatment with fluoxetine or long-acting injectable antipsychotics. The criteria (3)—(7) werealso applied for healthy controls and none of the healthycontrols was treated with any psychopharmacological drug.Significant psychiatric or somatic diseases were excluded by adetailed history, psychiatric interview (SCID I), physical exam-ination and routine laboratory tests. Healthy volunteersunderwent the same study procedures as patients at baseline,but were not hospitalized.
2.1.3. Healthy controlsWe excluded three subjects (controls only) from the analysissince post-dexamethasone cortisol more than 5 SDs abovemean and interview indicated that dexamethasone was mostlikely not ingested. Finally, we selected 34 healthy volun-teers who were matched to participating patients withrespect to age and BMI.
2.1.4. Depressed patientsWe excluded subjects with dexamethasone suppression test(DST) nonsuppression and found no evidence for HPA systemactivation in our group of patients when considering DST,saliva cortisol, cortisol excretion in urine or adrenal volume(see Table 1). After exclusion of DST nonsuppressors, we

Table 1 Demographics, BMI, HPA measures and normetanephrine excretion in depressed patients and healthy controls (all data:mean � SD or percentage). Abbreviations: post-dex cortisol (morning cortisol after ingestion of 1 mg dexamethasone at 22.00), CAR(cortisol awakening response), AUC (area under the curve).
Depressedpatients(n = 20)
Healthycontrols(n = 34)
t-Test p value Effect ofdepression,controlled forage and sex
Effect ofdepression,controlled forBMI, age and sex
Sex, f/m, % fem 13/7 (65%) 15/19 (42%) Chi2 = 2.2, n.s. n.a. n.a.Age, yrs 40.3 � 12.5 45.1 � 14.5 0.22 n.a. n.a.BMI, kg/m2 25.2 � 4.9 25.2 � 3.8 0.97 n.a. n.a.CortisolPost-dex, mg/dl 9.6 � 8.0 7.0 � 2.5 0.16 0.04 0.30Urine, mg/24 h 9.96 � 6.31 11.16 � 6.94 0.81 0.91 0.68Saliva
CAR (13/27) 5.1 � 9.4 5.4 � 17.1 0.94 0.10 0.18Slope (13/27) �0.88 � 0.66 �1.01 � 1.14 0.64 0.92 0.91AUC (12/26) 99 � 29 129 � 68 0.16 0.35 0.33
Normetanephrineexcretion mg/24 h
0.22 � 0.12 0.24 � 0.12 0.55 0.64 0.35
Adrenal volume, ml 1.40 � 0.45 1.26 � 0.58 0.35 0.22 0.72Metabolic syndrome 5/20 (25%) 5/34 (15%) Chi2 = 0.884 p = 0.47 n.a. n.a.
Significant value is bolded.
106 B. Scharnholz et al.
included 20 depressed patients (13 f/7 m) and 34 healthycontrols (15 f/19 m) in this analysis. Age tended to be higherin healthy controls compared to depressed patients(45.1 � 14.5 vs. 40.3 � 12.5 yrs; p = 0.22), while BMI didnot differ (25.2 � 3.8 vs. 25.2 � 4.9 kg/m2; p = 0.97). Sever-ity of depression was in the moderate range (HRDS25.0 � 4.8; range: 18—35) in depressed patients and noneof the healthy controls showed relevant depressive symptoms(HDRS 1.8 � 1.5; range: 0—5).
2.2. Study procedures
All study procedures were done within the first days ofinpatient treatment in order to minimize effects of changeof diet and physical activation. Patients were kept off anypsychopharmacological treatment for 6 days except zolpi-dem in case of sleep difficulties and lorazapam in case ofagitation. At the end of that period, saliva was sampled forthe determination of cortisol at wake-up (F0), ½ h (F1/2), 8 h(F8) and 14 h (F14) after waking. We calculated cortisolawakening response (CAR), slope (F0 to F14, without F1/2)and area under the curve (AUC) as described earlier by ourresearch group (Lederbogen et al., 2011). The following nightand day we sampled 24-h urine (10 p.m. to 10 p.m.) foranalysis of steroid excretion. The next morning blood wasdrawn for endocrine and metabolic parameters at 8.30 a.m.Heart rate and blood pressure were measured under strictresting conditions. Weight to the nearest 0.1 kg, height to thenearest 0.1 cm and waist circumference to the nearest0.1 cm at the level of the uppermost lateral border of theiliac crest were measured after overnight fasting using stan-dard operating procedures. As last endocrine procedure, weperformed a DST with 1 mg dexamethasone at 11 p.m. andblood sampling for analysis of cortisol the following morningat 8.30 a.m. All blood samples were immediately centrifugedand serum frozen at �80 8C. Saliva samples were stored in a
refrigerator (healthy control: at home) and immediatelyfrozen at �20 8C upon receipt.
2.3. MRI measures
Body composition (visceral fat, adrenal volume) were ana-lyzed using MRI in all healthy controls and those patients thatshowed no clear evidence for HPA system activation asassessed by the 1 mg dexamethasone suppression test. Within14 days after study inclusion and at most 8 days after the startof antidepressant medication, patients received MR imaging,which was performed using a 1.5 T 32-channel whole-bodyMR-scanner (Siemens Avanto, Erlangen, Germany) with allindividuals in a head-first supine position. The study parti-cipants were covered by two 6-element body matrix coils andplaced on the inbuilt 32-element spine matrix coil. A volume-interpolated breath-hold-exam (VIBE) sequence in axialorientation was acquired (TR/TE1/TE2 — 7.5/2.4/4.8 ms,flip angle — 108, slice thickness — 3 mm). This sequence useda Dixon-type fat saturation based on the subsequent acquisi-tion of two echoes. From these two echoes, which wereacquired at in-phase and opposed-phase conditions fat-onlyand water-only images were reconstructed. The study wasplanned to include the adrenal glands completely. We aver-aged left and right adrenal volume measured on the water-only images and used mean adrenal volume for furtheranalysis. The visceral fat was measured on the fat-onlyimages using a region growing algorithm after the subcuta-neous fat had been manually removed.
2.4. Laboratory analyses
Metabolic parameters were analyzed as described earlier(Hummel et al., 2011). Saliva and serum cortisol weremeasured using a time-resolved immunoassays with fluores-cence detection with coefficients of intra- and inter-assay
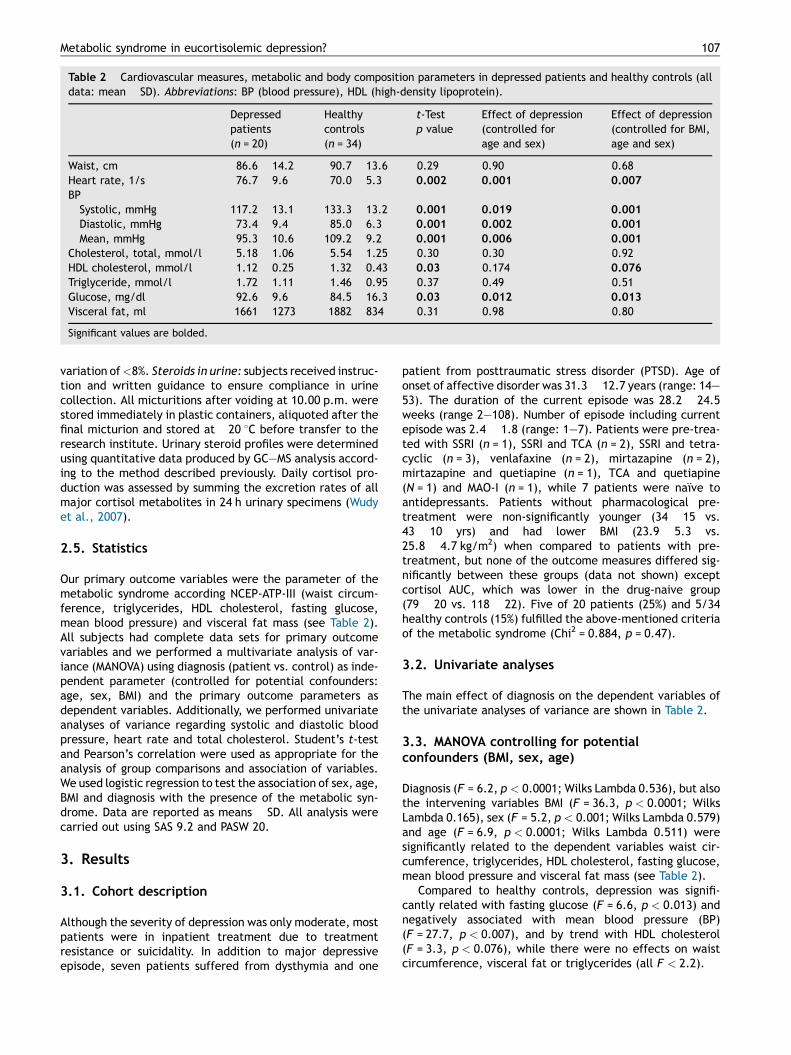
Table 2 Cardiovascular measures, metabolic and body composition parameters in depressed patients and healthy controls (alldata: mean � SD). Abbreviations: BP (blood pressure), HDL (high-density lipoprotein).
Depressedpatients(n = 20)
Healthycontrols(n = 34)
t-Testp value
Effect of depression(controlled forage and sex)
Effect of depression(controlled for BMI,age and sex)
Waist, cm 86.6 � 14.2 90.7 � 13.6 0.29 0.90 0.68Heart rate, 1/s 76.7 � 9.6 70.0 � 5.3 0.002 0.001 0.007
BPSystolic, mmHg 117.2 � 13.1 133.3 � 13.2 0.001 0.019 0.001
Diastolic, mmHg 73.4 � 9.4 85.0 � 6.3 0.001 0.002 0.001
Mean, mmHg 95.3 � 10.6 109.2 � 9.2 0.001 0.006 0.001
Cholesterol, total, mmol/l 5.18 � 1.06 5.54 � 1.25 0.30 0.30 0.92HDL cholesterol, mmol/l 1.12 � 0.25 1.32 � 0.43 0.03 0.174 0.076
Triglyceride, mmol/l 1.72 � 1.11 1.46 � 0.95 0.37 0.49 0.51Glucose, mg/dl 92.6 � 9.6 84.5 � 16.3 0.03 0.012 0.013
Visceral fat, ml 1661 � 1273 1882 � 834 0.31 0.98 0.80
Significant values are bolded.
Metabolic syndrome in eucortisolemic depression? 107
variation of <8%. Steroids in urine: subjects received instruc-tion and written guidance to ensure compliance in urinecollection. All micturitions after voiding at 10.00 p.m. werestored immediately in plastic containers, aliquoted after thefinal micturion and stored at �20 8C before transfer to theresearch institute. Urinary steroid profiles were determinedusing quantitative data produced by GC—MS analysis accord-ing to the method described previously. Daily cortisol pro-duction was assessed by summing the excretion rates of allmajor cortisol metabolites in 24 h urinary specimens (Wudyet al., 2007).
2.5. Statistics
Our primary outcome variables were the parameter of themetabolic syndrome according NCEP-ATP-III (waist circum-ference, triglycerides, HDL cholesterol, fasting glucose,mean blood pressure) and visceral fat mass (see Table 2).All subjects had complete data sets for primary outcomevariables and we performed a multivariate analysis of var-iance (MANOVA) using diagnosis (patient vs. control) as inde-pendent parameter (controlled for potential confounders:age, sex, BMI) and the primary outcome parameters asdependent variables. Additionally, we performed univariateanalyses of variance regarding systolic and diastolic bloodpressure, heart rate and total cholesterol. Student’s t-testand Pearson’s correlation were used as appropriate for theanalysis of group comparisons and association of variables.We used logistic regression to test the association of sex, age,BMI and diagnosis with the presence of the metabolic syn-drome. Data are reported as means � SD. All analysis werecarried out using SAS 9.2 and PASW 20.
3. Results
3.1. Cohort description
Although the severity of depression was only moderate, mostpatients were in inpatient treatment due to treatmentresistance or suicidality. In addition to major depressiveepisode, seven patients suffered from dysthymia and one
patient from posttraumatic stress disorder (PTSD). Age ofonset of affective disorder was 31.3 � 12.7 years (range: 14—53). The duration of the current episode was 28.2 � 24.5weeks (range 2—108). Number of episode including currentepisode was 2.4 � 1.8 (range: 1—7). Patients were pre-trea-ted with SSRI (n = 1), SSRI and TCA (n = 2), SSRI and tetra-cyclic (n = 3), venlafaxine (n = 2), mirtazapine (n = 2),mirtazapine and quetiapine (n = 1), TCA and quetiapine(N = 1) and MAO-I (n = 1), while 7 patients were naıve toantidepressants. Patients without pharmacological pre-treatment were non-significantly younger (34 � 15 vs.43 � 10 yrs) and had lower BMI (23.9 � 5.3 vs.25.8 � 4.7 kg/m2) when compared to patients with pre-treatment, but none of the outcome measures differed sig-nificantly between these groups (data not shown) exceptcortisol AUC, which was lower in the drug-naive group(79 � 20 vs. 118 � 22). Five of 20 patients (25%) and 5/34healthy controls (15%) fulfilled the above-mentioned criteriaof the metabolic syndrome (Chi2 = 0.884, p = 0.47).
3.2. Univariate analyses
The main effect of diagnosis on the dependent variables ofthe univariate analyses of variance are shown in Table 2.
3.3. MANOVA controlling for potentialconfounders (BMI, sex, age)
Diagnosis (F = 6.2, p < 0.0001; Wilks Lambda 0.536), but alsothe intervening variables BMI (F = 36.3, p < 0.0001; WilksLambda 0.165), sex (F = 5.2, p < 0.001; Wilks Lambda 0.579)and age (F = 6.9, p < 0.0001; Wilks Lambda 0.511) weresignificantly related to the dependent variables waist cir-cumference, triglycerides, HDL cholesterol, fasting glucose,mean blood pressure and visceral fat mass (see Table 2).
Compared to healthy controls, depression was signifi-cantly related with fasting glucose (F = 6.6, p < 0.013) andnegatively associated with mean blood pressure (BP)(F = 27.7, p < 0.007), and by trend with HDL cholesterol(F = 3.3, p < 0.076), while there were no effects on waistcircumference, visceral fat or triglycerides (all F < 2.2).

108 B. Scharnholz et al.
Regarding the potential confounders, BMI was strongly andpositively associated with waist circumference, mean BP,triglycerides, visceral fat, mean adrenal volume and nega-tively with HDL-cholesterol (all F > 8.0), but not fastingglucose. Female sex was positively associated with waistcircumference and visceral fat (all F > 8.3), but none ofthe other parameters (all F < 1.1). Age was positively relatedto waist circumference, fasting glucose, mean BP and visc-eral fat (all F > 4.9).
3.4. MANOVA controlling for sex and age
In order to exclude potential overcorrection, we repeatedthese analyses without controlling for BMI (see Tables 1 and2). These analyses confirmed all findings except the effect of‘diagnosis’ on HDL cholesterol. Also, this analysis revealed aneffect of ‘diagnosis’ on post-dexamethasone cortisolalthough the cortisol concentrations were well within therange of dexamethasone suppression, both in patients andcontrols.
3.5. Risk for metabolic syndrome
Using logistic regression, we found that BMI ( p < 0.001), butnot age ( p = 0.49), sex ( p = 0.75) and diagnosis of depression( p = 0.41), was associated with the metabolic syndrome.
4. Discussion
The main findings of our study are that depressed patientswithout current evidence for activation of the HPA systemand sympathoadrenergic system have modest metabolic dis-turbances (e.g. increased fasting glucose, low blood pres-sure, trend for low HDL cholesterol), but no HPA-relatedmorphological changes like increased visceral fat or waistcircumference.
Clearly, major depressive disorder is associated withincreased HPA system activity, although this may be truefor only a subset of patients, especially those with melan-cholic features (Stetler and Miller, 2011). There are severalstudies with different methodological approaches that showonly modest HPA activation (effect size: 0.17—0.25; Vreeburget al., 2009), virtual no HPA system activation in premeno-pausal depressed women (Young et al., 2001) or evendecreased HPA activity (Strickland et al., 2002) in depressedpatients. A recent meta-analysis showed saliva cortisol to notdiffer between controls and depressed patients (Knorr et al.,2010). While there is an abundance of research on thepathophysiology as well as the sequelae of HPA activationin depression, the ‘‘eucortisolemic’’ majority of depressedpatients has hitherto deserved less attention. In this study,we did not specifically exclude patients with melancholia,severe depression or anxious depression. Nevertheless, afterexclusion of only four depressed patients being non-suppres-sors to dexamethasone, our sample did not differ at all fromhealthy controls with regard to cortisol excretion, salivacortisol and adrenal volume.
Recently, it has been reported that disturbed autonomicnervous system (ANS) rather than HPA system activation maybe related to the metabolic syndrome (Licht et al., 2010).Therefore, we measured heart rate and normetanephrine
excretion in urine that may be taken to reflect sympatheticactivity (Oeltmann et al., 2004). The group of depressedpatients showed a higher heart rate than the control group,so their might be some small ANS alterations, independent ofthe measured catecholamine levels. But with reference tothe normetanephrine excretion, as a measure of the cate-cholamine levels (effector hormones of the ANS), our nega-tive findings strongly suggest that in our included group ofdepressed patients neither HPA nor ANS were activated.
Thus, our cohort allowed studying the impact of depres-sion on metabolic features, completely independent ofstress—responsive systems.
We controlled for potential confounders that had strongeffects on the metabolic features. Especially, BMI (waist cir-cumference, mean BP, triglycerides, HDL-cholesterol, visceralfat) and age (waist circumference, fasting glucose, mean BP,visceral fat) had strong effects on the dependent metabolicand morphometric variables, while the effects of ‘‘diagnosis’’on fasting glucose and blood pressure were of moderate size.We found low HDL cholesterol to be related to depression onlyby trend. Thus, high fasting glucose, low blood pressure and,potentially, low HDL cholesterol are associated with depres-sion, independent from HPA activity. Interestingly, this obser-vation is in accordance with a recently published study showingthat atypical and eucortisolemic rather than melancholic andhypercortisolemic depression is associated with metabolicdysregulation, for example high triglycerides and low HDL-cholesterol (Lamers et al., 2013).
In presumably hypercortisolemic depressed patients withpsychotic features, low glucose utilization that improvesafter recovery has been described as early as 1969 (Muelleret al., 1969). An association between depression and insulinresistance has been confirmed in epidemiological studies(Pearson et al., 2010; Kan et al., 2013) and severe HPA systemactivation in clinically depressed patients was found to beassociated with impaired glucose tolerance (Weber-Hamannet al., 2005). However, using the euglycemic clamp techni-que, Schweiger’s group showed patients with atypicaldepression and low cortisol also to have low glucose disposal,which was attributed to a hypoactive allocation system(Schweiger et al., 2008). Therefore, depression with stronglyincreased HPA activity, but also atypical depression with lowHPA activity was found to be associated with impaired glu-cose disposal. Thus, our finding of increased fasting glucose indepressed patients without HPA activation is not necessarilyin contrast to previous findings, although our group ofpatients suffered neither predominantly from atypicaldepression nor from adiposity.
Depression increases the risk for incident hypertension(Meng et al., 2012) and dexamethasone non-suppression hasbeen found related to hypertension (Pfohl et al., 1991). How-ever, there is evidence from epidemiological studies (Hildrumet al., 2007; Dogan et al., 2011) that depression is related tolow blood pressure, at least in subgroups of patients. Long-itudinal cohort studies suggest that low blood pressure mayprecede depression and could be a risk factor for affectivedisorders (Godin et al., 2012). These scarce reports on thephysiology of blood pressure regulation in depressed patientsmight fit our observation of low blood pressure in depressedpatients without HPA system activation.
While atypical (Van Reedt Dortland et al., 2010) or undif-ferentiated depression (Cizza et al., 2012) have been found

Metabolic syndrome in eucortisolemic depression? 109
associated with increased LDL cholesterol, most studiesfound low total and LDL cholesterol, both using epidemio-logical (Lindberg et al., 1994) as well as clinicalapproaches (Hummel et al., 2011). Also, HDL cholesterolhas been repeatedly found to be low in clinically depressedpatients (Maes et al., 1997; Sagud et al., 2009; Hummelet al., 2011), especially in patients with melancholic fea-tures (Van Reedt Dortland et al., 2010). Interestingly,atypical rather than melancholic depression might berelated to the metabolic syndrome (Lamers et al., 2010)suggesting that HPA system activation is not the onlymechanism leading to metabolic disturbances in depressedpatients. In our group of patients without major HPAsystem activation, we found a trend for lowered HDLcholesterol, which suggests HDL cholesterol in depressedpatients to be low independent from HPA system activity.Also, independent from the activation of stress—responsivesystems, we found an increased rate of subjects fulfillingthe criteria of the metabolic syndrome when comparingdepressed patients with healthy controls.
In contrast to the metabolic examinations, we found nodifference in visceral fat or adrenal volume when comparingeucortisolemic depressed patients and healthy controls.There is at least limited evidence that activation of theHPA system during depression, especially increased ACTH,is related to an increased adrenal volume (Rubin et al., 2006)and visceral fat (Weber-Hamann et al., 2002; Arnaldi et al.,2010). Thus, our negative finding in patients without HPAsystem activation is not surprising.
Thus, it may be assumed that additional factors next toHPA activation may be operative in linking affective andmetabolic disorders. We assume that biological factors likedisrupted circadian rhythm (Bray and Young, 2007) or inflam-mation (Lee et al., 2013) and behavioral factors, likeimpaired sleep (Mezick et al., 2011) and lifestyle factors,especially physical activity and diet, may play a role in thevascular risk architecture of depressed patients. These fac-tors deserve more attention both in patient care as well as inclinical research.
We consider our comprehensive approach of intensivephenotyping with ANS as well as various HPA measures,metabolic assessments and morphometric MRI a strength ofour study. Clearly, the relatively small number of depressedpatients is a limitation, even though we controlled for con-founders and the group of patients was rather homogenous.Also, potential pathophysiological mediators like inflamma-tion or disruption of circadian rhythm were not studied. Itcould be speculated that the pre-treatment with antidepres-sants induced increased fasting glucose values. However,some of our patients were drug-naıve and our earlier findings(Weber-Hamann et al., 2006, 2008) rather suggest that anti-depressive treatment is neutral with regard to fasting glucoseor, in the case of response, rather improves glucose meta-bolism.
In conclusion, we found some metabolic disturbances indepressed patients without any endocrinological or morpho-logical evidence of increased HPA system activity.
Role of the funding source
Funding source does not have any influence on this study.
Conflict of interest statement
MD and his group received honoraria for consulting andlectures from Otsuka Pharma, BristolMyers Squibb and Ser-vier. All other authors claimed no conflict of interest regard-ing the content of this manuscript.
Acknowledgement
We gratefully acknowledge the expert technical assistance ofSusanne Laubender.
References
Arnaldi, G., Scandali, V.M., Trementino, L., Cardinaletti, M., Appol-loni, G., Boscaro, M., 2010. Pathophysiology of dyslipidemia inCushing’s syndrome. Neuroendocrinology 1 (92 Suppl) 86—90.
Bjorntorp, P., 2001. Do stress reactions cause abdominal obesity andcomorbidities? Obes. Rev. 2, 73—86.
Bray, M.S., Young, M.E., 2007. Circadian rhythms in the developmentof obesity: potential role for the circadian clock within theadipocyte. Obes. Rev. 8, 169—181.
Carpenter, L.L., Ross, N.S., Tyrka, A.R., Anderson, G.M., Kelly, M.,Price, L.H., 2009. Dex/CRH test cortisol response in outpatientswith major depression and matched healthy controls. Psycho-neuroendocrinology 34, 1208—1213.
Cizza, G., Ronsaville, D.S., Kleitz, H., Eskandari, F., Mistry, S., Torvik,S., Sonbolian, N., Reynolds, J.C., Blackman, M.R., Gold, P.W.,Martinez, P.E., 2012. Clinical subtypes of depression areassociated with specific metabolic parameters and circadianendocrine profiles in women: the power study. PLoS One 7 (1)e28912.
Dogan, Y., Onat, A., Kaya, H., Ayhan, E., Can, G., 2011. Depressivesymptoms in a general population: associations with obesity,inflammation, and blood pressure. Cardiol. Res. Pract. 740957.
Godin, O., Elbejjani, M., Kaufman, J.S., 2012. Body mass index,blood pressure, and risk of depression in the elderly: a marginalstructural model. Am. J. Epidemiol. 176, 204—213.
Gold, P.W., Chrousos, G.P., 2002. Organization of the stress systemand its dysregulation in melancholic and atypical depression: highvs low CRH/NE states. Mol. Psychiatry 7, 254—275.
Hildrum, B., Mykletun, A., Stordal, E., Bjelland, I., Dahl, A.A.,Holmen, J., 2007. Association of low blood pressure with anxietyand depression: the Nord-Trøndelag Health Study. J. Epidemiol.Community Health 61, 53—58.
Hummel, J., Westphal, S., Weber-Hamann, B., Gilles, M., Lederbo-gen, F., Angermeier, T., Luley, C., Deuschle, M., Kopf, D., 2011.Serum lipoproteins improve after successful pharmacologic anti-depressant treatment: a randomized open-label prospective tri-al. J. Clin. Psychiatry 72, 885—891.
Kan, C., Silva, N., Golden, S.H., Rajala, U., Timonen, M., Stahl, D.,Ismail, K., 2013. A systematic review and meta-analysis of theassociation between depression and insulin resistance. DiabetesCare 36, 480—489.
Kessing, L.V., Willer, I.S., Knorr, U., 2011. Volume of the adrenal andpituitary glands in depression. Psychoneuroendocrinology 36,19—27.
Kinder, L.S., Carnethon, M.R., Palaniappan, L.P., King, A.C., For-tmann, S.P., 2004. Depression and the metabolic syndrome inyoung adults: findings from the Third National Health and Nutri-tion Examination Survey. Psychosom. Med. 66, 316—322.
Knorr, U., Vinberg, M., Kessing, L.V., Wetterslev, J., 2010. Salivarycortisol in depressed patients versus control persons: asystematic review and meta-analysis. Psychoneuroendocrinology35, 1275—1286.

110 B. Scharnholz et al.
Lamers, F., de Jonge, P., Nolen, W.A., Smit, J.H., Zitman, F.G.,Beekman, A.T., Penninx, B.W., 2010. Identifying depressive sub-types in a large cohort study: results from the Netherlands Studyof Depression and Anxiety (NESDA). J. Clin. Psychiatry 71, 1582—1589.
Lamers, F., Vogelzangs, N., Merikangas, K.R., de Jonge, P., Beekman,A.T., Penninx, B.W., 2013. Evidence for a differential role of HPA-axis function, inflammation and metabolic syndrome in melan-cholic versus atypical depression. Mol. Psychiatry 18, 692—699.
Lederbogen, F., Hummel, J., Fademrecht, C., Krumm, B., Kuhner, C.,Deuschle, M., Ladwig, K.H., Meisinger, C., Wichmann, H.E., Lutz,H., Breivogel, B., 2011. Flattened circadian cortisol rhythm intype 2 diabetes. Exp. Clin. Endocrinol. Diabetes 119, 573—575.
Lee, S.Y., Chen, S.L., Chang, Y.H., Chen, P.S., Huang, S.Y., Tzeng,N.S., Wang, Y.S., Wang, L.J., Lee, I.H., Wang, T.Y., Yeh, T.L.,Yang, Y.K., Hong, J.S., Lu, R.B., 2013. Inflammation’s associationwith metabolic profiles before and after a twelve-week clinicaltrial in drug-naıve patients with bipolar II disorder. PLoS One 8 (6)e66847.
Licht, C.M., Vreeburg, S.A., van Reedt Dortland, A.K., Giltay, E.J.,Hoogendijk, W.J., DeRijk, R.H., Vogelzangs, N., Zitman, F.G., deGeus, E.J., Penninx, B.W., 2010. Increased sympathetic anddecreased parasympathetic activity rather than changes in hy-pothalamic—pituitary—adrenal axis activity is associated withmetabolic abnormalities. J. Clin. Endocrinol. Metab. 95, 2458—2466.
Lindberg, G., Larsson, G., Setterlind, S., Rastam, L., 1994. Serumlipids and mood in working men and women in Sweden. J.Epidemiol. Commun. Health 48, 360—363.
Maes, M., Smith, R., Christophe, A., Vandoolaeghe, E., Van Gastel,A., Neels, H., Demedts, P., Wauters, A., Meltzer, H.Y., 1997.Lower serum high-density lipoprotein cholesterol (HDL-C) inmajor depression and in depressed men with serious suicidalattempts: relationship with immune-inflammatory markers. ActaPsychiatr. Scand. 95, 212—221.
Meng, L., Chen, D., Yang, Y., Zheng, Y., Hui, R., 2012. Depressionincreases the risk of hypertension incidence: a meta-analysis ofprospective cohort studies. J. Hypertens. 30, 842—851.
Mezick, E.J., Hall, M., Matthews, K.A., 2011. Are sleep and depres-sion independent or overlapping risk factors for cardiometabolicdisease? Sleep Med. Rev. 15, 51—63.
Mueller, P.S., Heninger, G.R., McDonald, R.K., 1969. Intravenousglucose tolerance test in depression. Arch. Gen. Psychiatry 21,470—477.
Oeltmann, T., Carson, R., Shannon, J.R., Ketch, T., Robertson, D.,2004. Assessment of O-methylated catecholamine levels in plas-ma and urine for diagnosis of autonomic disorders. Auton. Neu-rosci. 116, 1—10.
O’Keane, V., Frodl, T., Dinan, T.G., 2012. A review of Atypicaldepression in relation to the course of depression and changesin HPA axis organization. Psychoneuroendocrinology 37, 1589—1599.
Pearson, S., Schmidt, M., Patton, G., Dwyer, T., Blizzard, L., Otahal,P., Venn, A., 2010. Depression and insulin resistance: cross-sec-tional associations in young adults. Diabetes Care 33, 1128—1133.
Peeters, F., Nicolson, N.A., Berkhof, J., 2004. Levels and variabilityof daily life cortisol secretion in major depression. Psychiatry Res.126, 1—13.
Pfohl, B., Rederer, M., Coryell, W., Stangl, D., 1991. Associationbetween post-dexamethasone cortisol level and blood pressure indepressed inpatients. J. Nerv. Ment. Dis. 179, 44—47.
Rubin, R.T., Miller, T.H., Rhodes, M.E., Czambel, R.K., 2006. Adrenalcortical responses to low- and high-dose ACTH(1-24) administra-tion in major depressives vs. matched controls. Psychiatry Res.143, 43—50.
Rugulies, R., 2002. Depression as a predictor for coronary heartdisease: a review and meta-analysis. Am. J. Prev. Med. 23,51—61.
Sagud, M., Mihaljevic-Peles, A., Pivac, N., Jakovljevic, M., Muck-Seler, D., 2009. Lipid levels in female patients with affectivedisorders. Psychiatry Res. 168, 218—221.
Schweiger, U., Deuschle, M., Korner, A., Lammers, C.H., Schmider,J., Gotthardt, U., Holsboer, F., Heuser, I., 1994. Low lumbar bonemineral density in patients with major depression. Am. J. Psychi-atry 151, 1691—1693.
Schweiger, U., Greggersen, W., Rudolf, S., Pusch, M., Menzel, T.,Winn, S., Hassfurth, J., Fassbinder, E., Kahl, K.G., Oltmanns,K.M., Hohagen, F., Peters, A., 2008. Disturbed glucose disposal inpatients with major depression; application of the glucose clamptechnique. Psychosom. Med. 70, 170—176.
Stetler, C., Miller, G.E., 2011. Depression and hypothalamic-pitui-tary-adrenal activation: a quantitative summary of four decadesof research. Psychosom. Med. 73, 114—126.
Strickland, P.L., Deakin, J.F., Percival, C., Dixon, J., Gater, R.A.,Goldberg, D.P., 2002. Bio-social origins of depression in thecommunity. Interactions between social adversity, cortisol andserotonin neurotransmission. Br. J. Psychiatry 180, 168—173.
Van Den Eede, F., Van den Bossche, B., Hulstijn, W., Sabbe, B.G.,Cosyns, P., Claes, S.J., 2006. Combined dexamethasone/CRF testin remitted outpatients with recurrent major depressive disorder.J. Affect. Disord. 93, 259—263.
Van Reedt Dortland, A.K., Giltay, E.J., van Veen, T., van Pelt, J.,Zitman, F.G., Penninx, B.W., 2010. Associations between serumlipids and major depressive disorder: results from theNetherlands Study of Depression and Anxiety (NESDA). J. Clin.Psychiatry 71, 729—736.
Vogelzangs, N., Suthers, K., Ferruccci, L., Simonsick, E.M., Ble, A.,Schrager, M., Bandinelli, S., Lauretani, F., Giannelli, S.V., Pen-ninx, B.W., 2007. Hypercortisolemic depression is associated withte metabolic syndrome in late-life. Psychoneuroendocrinology32, 151—159.
Vreeburg, S.A., Hoogendijk, W.J., van Pelt, J., Derijk, R.H., Verha-gen, J.C., van Dyck, R., Smit, J.H., Zitman, F.G., Penninx, B.W.,2009. Major depressive disorder and hypothalamic-pituitary-ad-renal axis activity: results from a large cohort study. Arch. Gen.Psychiatry 66, 617—626.
Wannamethee, S.G., Shaper, A.G., Walker, M., 2005. Overweight andobesity and weight change in middle aged men: impact oncardiovascular disease and diabetes. J. Epidemiol. CommunityHealth 59, 134—139.
Weber-Hamann, B., Hentschel, F., Kniest, A., Deuschle, M., Colla, M.,Lederbogen, F., Heuser, I., 2002. Hypercortisolemic depression isassociated with increased intra-abdominal fat. Psychosom. Med.64, 274—277.
Weber-Hamann, B., Kopf, D., Lederbogen, F., Gilles, M., Heuser, I.,Colla, M., Deuschle, M., 2005. Activity of the hypothalamus-pituitary-adrenal system and oral glucose tolerance in depressedpatients. Neuroendocrinology 81, 200—204.
Weber-Hamann, B., Gilles, M., Lederbogen, F., Heuser, I., Deuschle,M., 2006. Improved insulin sensitivity in 80 nondiabetic patientswith MDD after clinical remission in a double-blind, randomizedtrial of amitriptyline and paroxetine. J. Clin. Psychiatry 67,1856—1861.
Weber-Hamann, B., Gilles, M., Schilling, C., Onken, V., Frankhauser,P., Kopf, D., Lederbogen, F., Deuschle, M., 2008. Improved insulinsensitivity in 51 nondiabetic depressed inpatients remitting dur-ing antidepressive treatment with mirtazapine and venlafaxine.J. Clin. Psychopharmacol. 28, 581—584.
Wudy, S.A., Hartmann, M.F., Remer, T., 2007. Sexual dimorphism incortisol secretion starts after age 10 in healthy children: urinarycortisol metabolite excretion rates during growth. Am. J. Physiol.Endocrinol. Metab. 293, E970—E976.
Young, E.A., Carlson, N.E., Brown, M.B., 2001. Twenty-four-hourACTH and cortisol pulsatility in depressed women. Neuropsycho-pharmacology 25, 267—276.
Related Documents