S The Feasibility of Implementing a Diabetes Distress Toolkit to Improve Outcomes in Adults with Uncontrolled Type 2 Diabetes: A DNP Project Daneeka Armont-Woods, MSN, APRN, NP-C DNP Candidate Southeastern Louisiana University Laurie Kinchen, DNP, APRN, PNP, DNP Project Committee Chair Christine Hadeed, DNP, APRN, ACNP, Second Faculty Committee Member Karen Rice, DNS, APRN, ACNS-BC, ANP, Facility Mentor

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
S
The Feasibility of Implementing a Diabetes Distress Toolkit to Improve Outcomes in Adults with Uncontrolled Type 2 Diabetes: A DNP Project
Daneeka Armont-Woods, MSN, APRN, NP-CDNP Candidate
Southeastern Louisiana University
Laurie Kinchen, DNP, APRN, PNP, DNP Project Committee ChairChristine Hadeed, DNP, APRN, ACNP, Second Faculty Committee Member
Karen Rice, DNS, APRN, ACNS-BC, ANP, Facility Mentor
Daneeka Armont-Woods, MSN, APRN, NP-C
S Adult Nurse Practitioner
S Graduated with BSN in 2002 from Dillard University of New Orleans, LA
S Graduated with MSN in 2009 from Southeastern Louisiana University of Hammond, LA
S Has worked as a Nurse Practitioner in the Diabetes Specialty Clinic of Ochsner Medical Center of New Orleans since February 2010
INTRODUCTION: BACKGROUND
S Over 29 million people in the United States have diabetes
S Diabetes is the seventh leading cause of death in the United States
S Medical expenditures for those with diabetes are significantly higher than those without diabetes
S Direct (medications/treatments, hospitalizations) and indirect costs (disability, premature death, lost of income) of diabetes=$245 billion
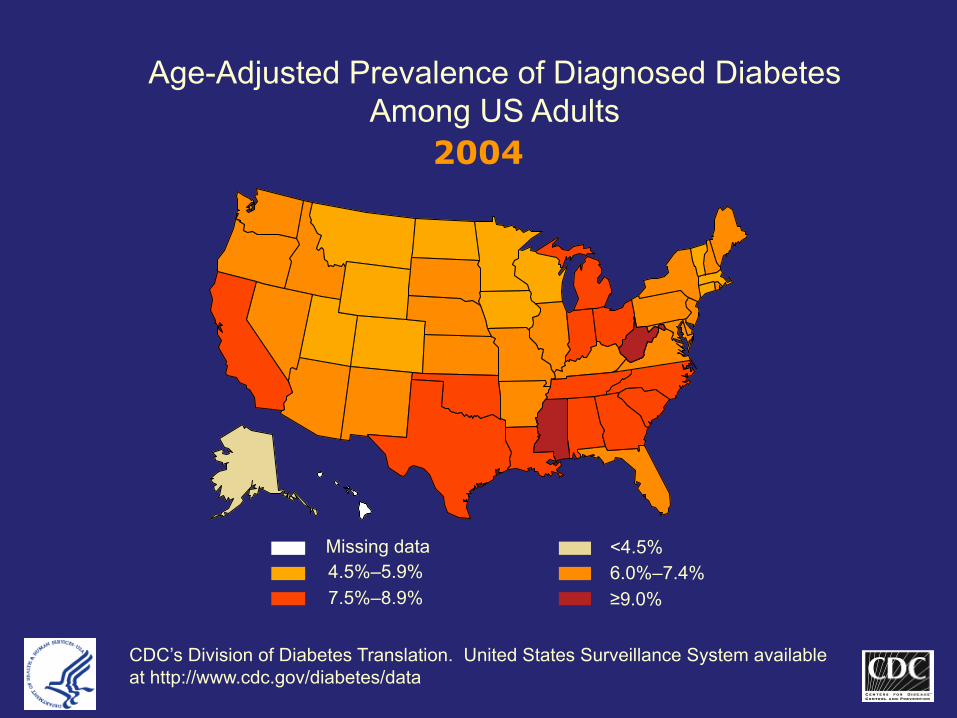
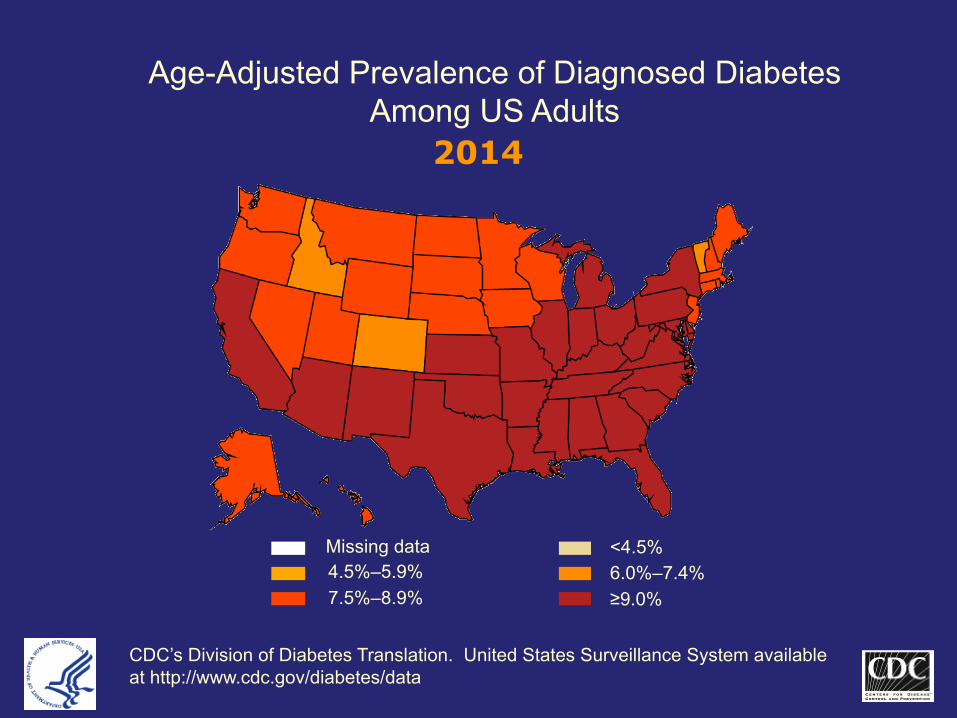
Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults
<4.5%Missing data4.5%–5.9% 6.0%–7.4%7.5%–8.9% ≥9.0%
CDC’s Division of Diabetes Translation. United States Surveillance System available at http://www.cdc.gov/diabetes/data
2004
Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults
<4.5%Missing data4.5%–5.9% 6.0%–7.4%7.5%–8.9% ≥9.0%
CDC’s Division of Diabetes Translation. United States Surveillance System available at http://www.cdc.gov/diabetes/data
2014
INTRODUCTION
S Diabetes Distress (DD) are those emotional concerns, worries, fears, and anxieties that frequently accompany a chronic disease such as diabetes (Fisher, Hessler, Masharani, & Strycker, 2014, p. 740).
S DD is associated with poor diabetes control and self-management (Fisher et al., 2014, p. 740).
S DD impacts as many as 40% of people diagnosed with diabetes and can increase over time, especially in those with Type 2 Diabetes (T2DM) (Berry, Lockhart, Davies, Lindsay, & Dempster, 2015, p. 279).
INTRODUCTIONS Increases in DD are associated with feelings of
fear, anger, and resentment, which can lead to worsening diabetes control (Philips, 2014, p. 615).
S Interventions to reduce DD can lead to improvements in diabetes care.
S Reduced DD is anticipated to improve diabetes outcomes
PURPOSE
S Evaluate the feasibility of measuring DD and piloting a toolkit anticipated to improve DD and diabetes-related outcomes.
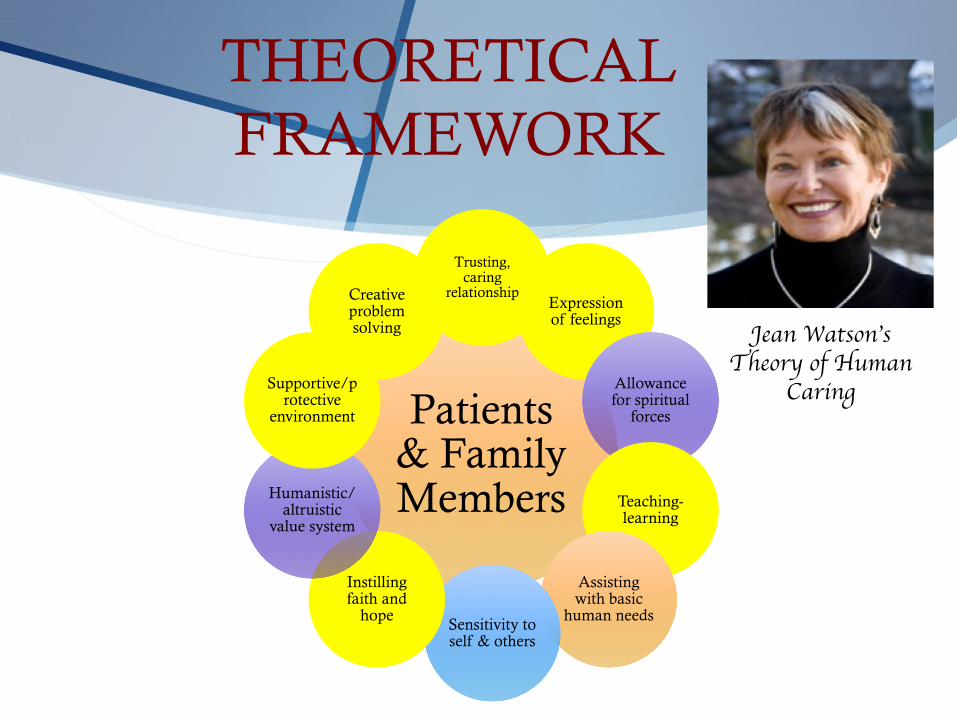
THEORETICAL FRAMEWORK
Patients & Family Members
Trusting, caring
relationshipExpression of feelings
Allowance for spiritual
forces
Teaching-learning
Assisting with basic
human needsSensitivity to self & others
Instilling faith and
hope
Humanistic/altruistic
value system
Supportive/protective
environment
Creative problem solving Jean Watson’s
Theory of Human Caring
LITERATURE REVIEW
S Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medline, and Pubmed searched.
S Keywords: T2DM, diabetes distress, glycemic control, support
S 225 articles initial yield
S Excluded articles: Type 1 diabetes, depression, group support without diabetes.
S 24 articles included
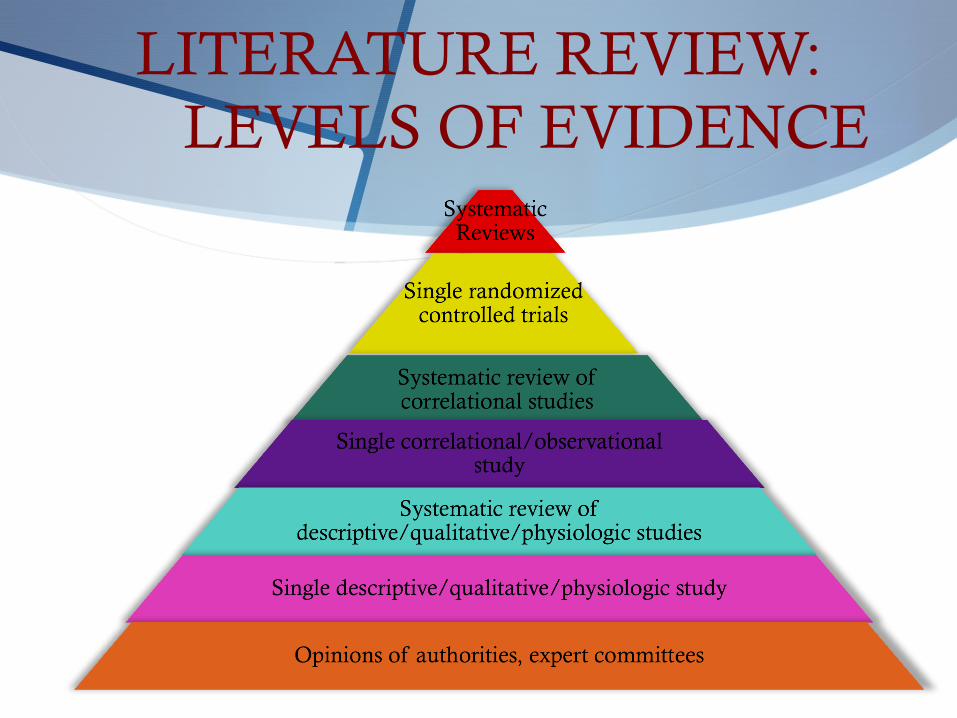
LITERATURE REVIEW: LEVELS OF EVIDENCE
LITERATURE REVIEW: SUMMARY OF FINDINGS
S Intervention trials should target individuals with high A1C and DD levels (Berry et al., 2015).
S There is a significant association between distress and A1C (Fisher, Glasgow, & Strycker, 2010).
S DD is responsive to interventions (Fisher, Hessler, Glasgow, Arean, Masharani, Naranjo, & Strycker, 2013).
S Decreases in regimen distress are associated with improvements in A1C and self-management (Hessler, Fisher, Glasgow, Strycker, Dickinson, Arean, & Masharani, 2014).
S More attention should be given to non-clinical factors when addressing diabetes related distress (Karlsen & Bru, 2014).
S Changes in DD are associated with changes in glycemic control for patients with uncontrolled T2DM (Zagarins, Allen, Garb, & Welch, 2012).
S Adherence to diabetes treatment is linked to DD more than depression (Zhang, Xu, Wu, Xue, Xu, Li, Gao, & Liu, 2013).
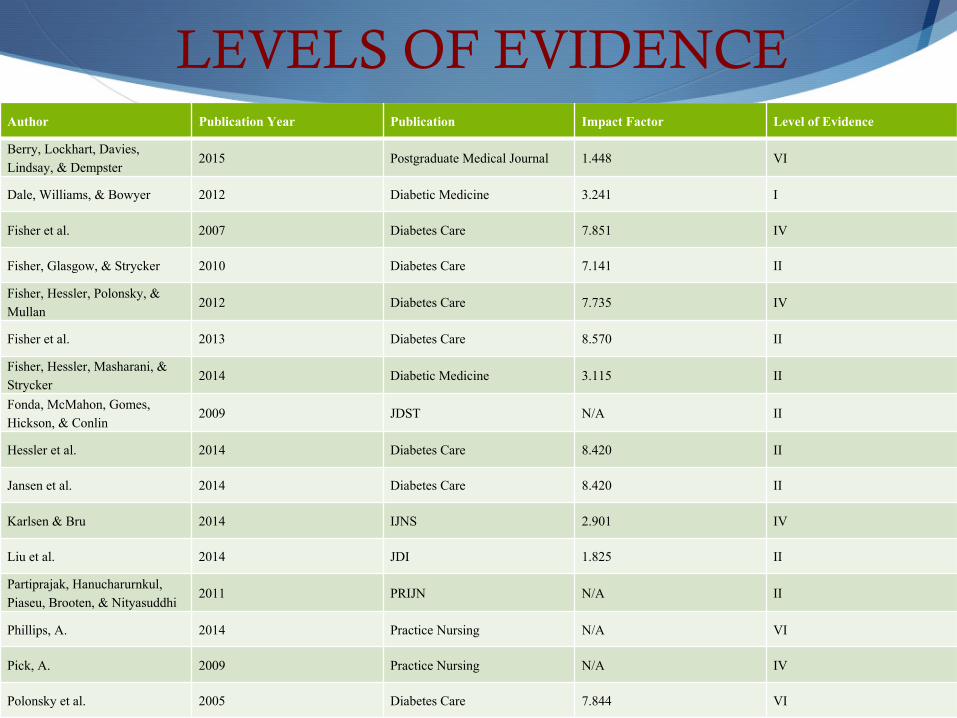
Author Publication Year Publication Impact Factor Level of Evidence
Berry, Lockhart, Davies, Lindsay, & Dempster
2015 Postgraduate Medical Journal 1.448 VI
Dale, Williams, & Bowyer 2012 Diabetic Medicine 3.241 I
Fisher et al. 2007 Diabetes Care 7.851 IV
Fisher, Glasgow, & Strycker 2010 Diabetes Care 7.141 II
Fisher, Hessler, Polonsky, & Mullan
2012 Diabetes Care 7.735 IV
Fisher et al. 2013 Diabetes Care 8.570 II
Fisher, Hessler, Masharani, & Strycker
2014 Diabetic Medicine 3.115 II
Fonda, McMahon, Gomes, Hickson, & Conlin
2009 JDST N/A II
Hessler et al. 2014 Diabetes Care 8.420 II
Jansen et al. 2014 Diabetes Care 8.420 II
Karlsen & Bru 2014 IJNS 2.901 IV
Liu et al. 2014 JDI 1.825 II
Partiprajak, Hanucharurnkul, Piaseu, Brooten, & Nityasuddhi
2011 PRIJN N/A II
Phillips, A. 2014 Practice Nursing N/A VI
Pick, A. 2009 Practice Nursing N/A IV
Polonsky et al. 2005 Diabetes Care 7.844 VI
LEVELS OF EVIDENCE
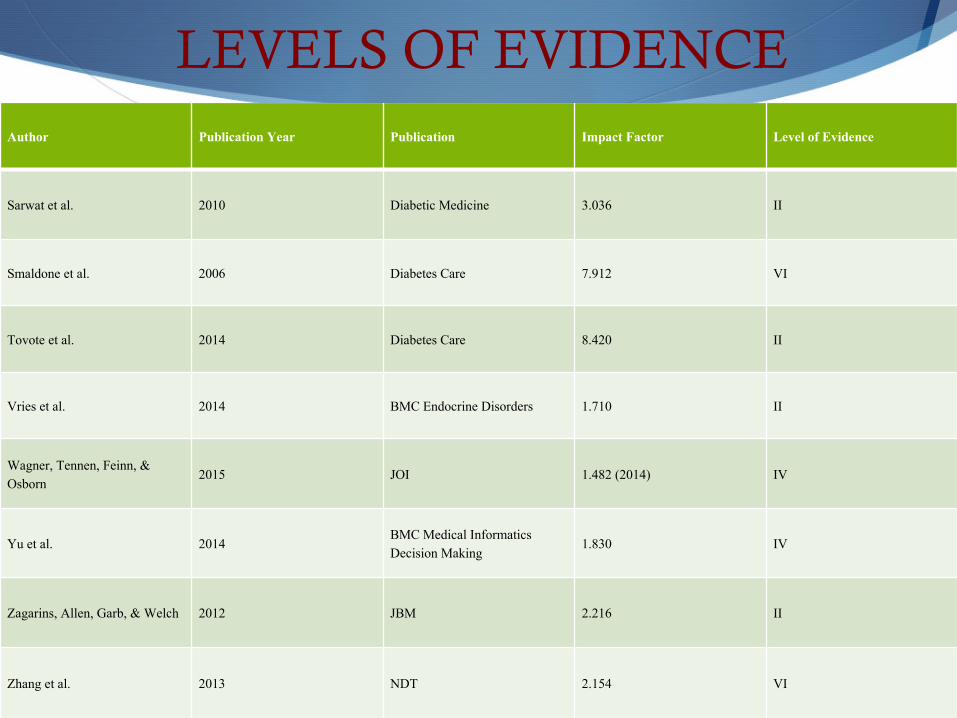
Author Publication Year Publication Impact Factor Level of Evidence
Sarwat et al. 2010 Diabetic Medicine 3.036 II
Smaldone et al. 2006 Diabetes Care 7.912 VI
Tovote et al. 2014 Diabetes Care 8.420 II
Vries et al. 2014 BMC Endocrine Disorders 1.710 II
Wagner, Tennen, Feinn, & Osborn
2015 JOI 1.482 (2014) IV
Yu et al. 2014BMC Medical Informatics Decision Making
1.830 IV
Zagarins, Allen, Garb, & Welch 2012 JBM 2.216 II
Zhang et al. 2013 NDT 2.154 VI
LEVELS OF EVIDENCE
LEVELS OF EVIDENCE
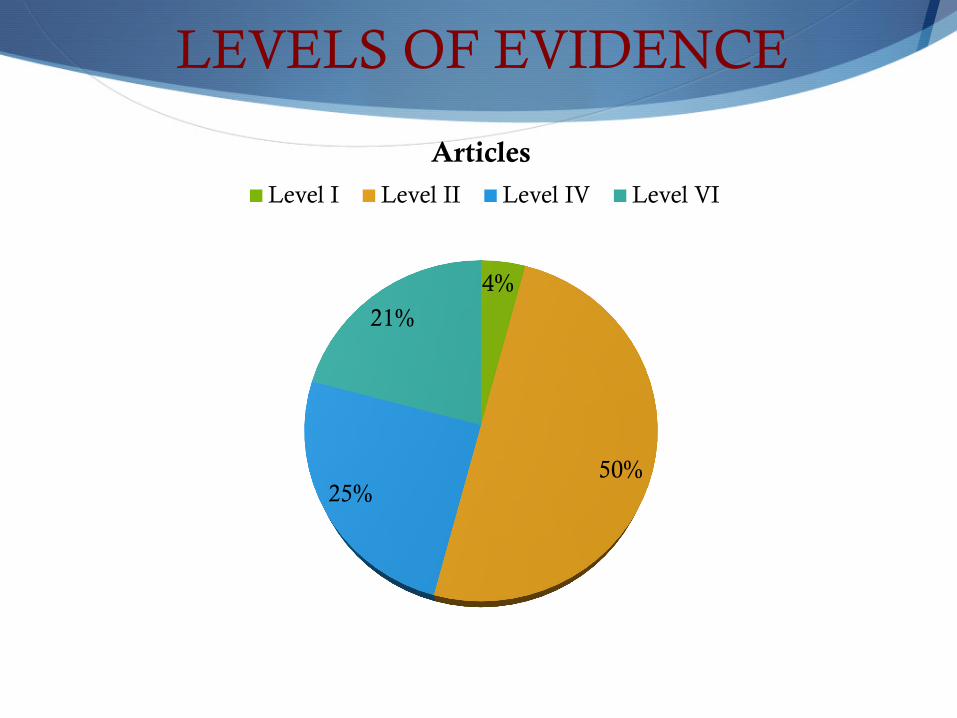
4%
50%25%
21%
ArticlesLevel I Level II Level IV Level VI
CLINICAL QUESTIONS
S Is it feasible to measure DD and implement a DD toolkit in patients with T2DM being treated in an APRN-led diabetes specialty clinic?
S What are the reports of patients with uncontrolled T2DM and moderate to high DD in those that used the interventions in the toolkit versus those that did not use the interventions?
S What are the diabetic outcomes in those with T2DM with moderate to high DD that used the toolkit compared to those that did not use the toolkit?
S What are the barriers and facilitators in those patients with T2DM and moderate to high DD that used the DD toolkit?
METHODOLOGY: DESIGN
S Quality improvement design
S Quality improvement projects in healthcare entail efforts that seek to improve services for the future (Moran, Burson, & Conrad, 2014).
METHODOLOGY: INTERVENTION
S Screen patients presenting to the advanced practice registered nurse (APRN)-led diabetes specialty clinic for DD. S 17-item DD survey (DDS-17) completed in the waiting room
or the exam room with the APRN. S DDS-17: Developed by Dr. Polonsky and Dr. Fisher
S Emotional burdenS Physician/provider related distressS Regimen DistressS Interpersonal Distress
S All patients completing the DDS-17 received a copy of the DD toolkit
METHODOLOGY: INTERVENTION
S Uncontrolled T2DM (A1C ≥ 7%), and at least moderate DD via a score of 3 or more in overall DD or any of the subscales were invited to be consented and all interventions were explained in detail. S A1C. S Exclusion: Type 1 Diabetes, depression, A1C <7%, altered mental status. S Clinic visit evaluation completed
S Telephone survey 4-6 weeks after initial visit. S Telephone visit evaluation completed
S Return visit in 3-4 monthsS 17-item DD survey and review A1C .
S All information entered into an Excel spreadsheet for data analysis
METHODOLOGY: OUTCOME MEASURES
S Primary endpoint: the feasibility of measuring DD and implementing the toolkit.
S Secondary outcomesS A1C
S DD levels
METHODOLOGY: DATA COLLECTION TOOLS
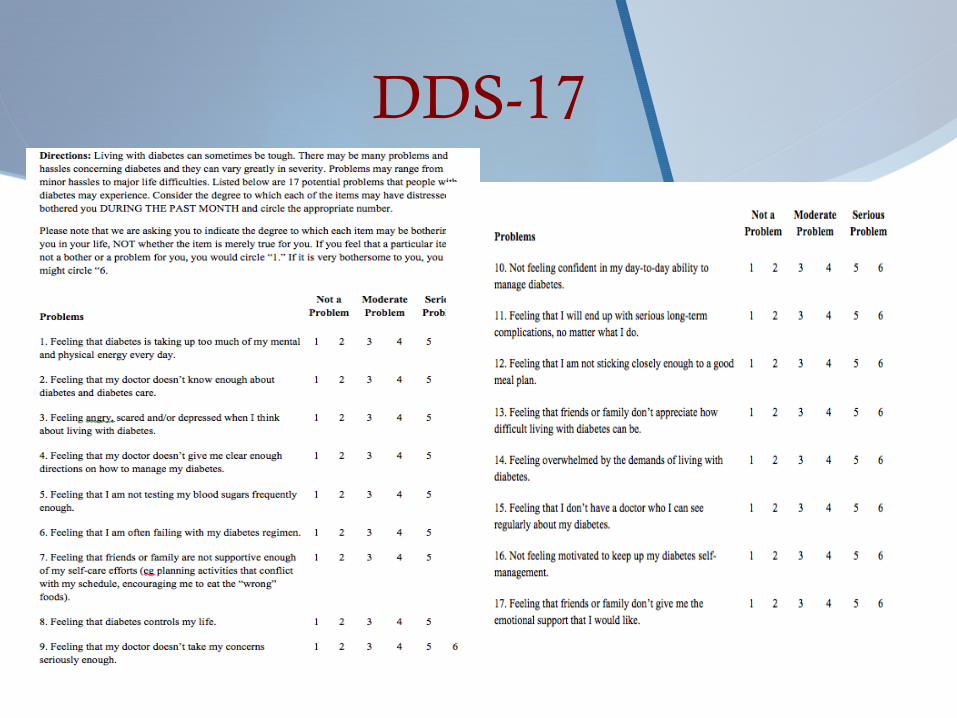
DDS-17
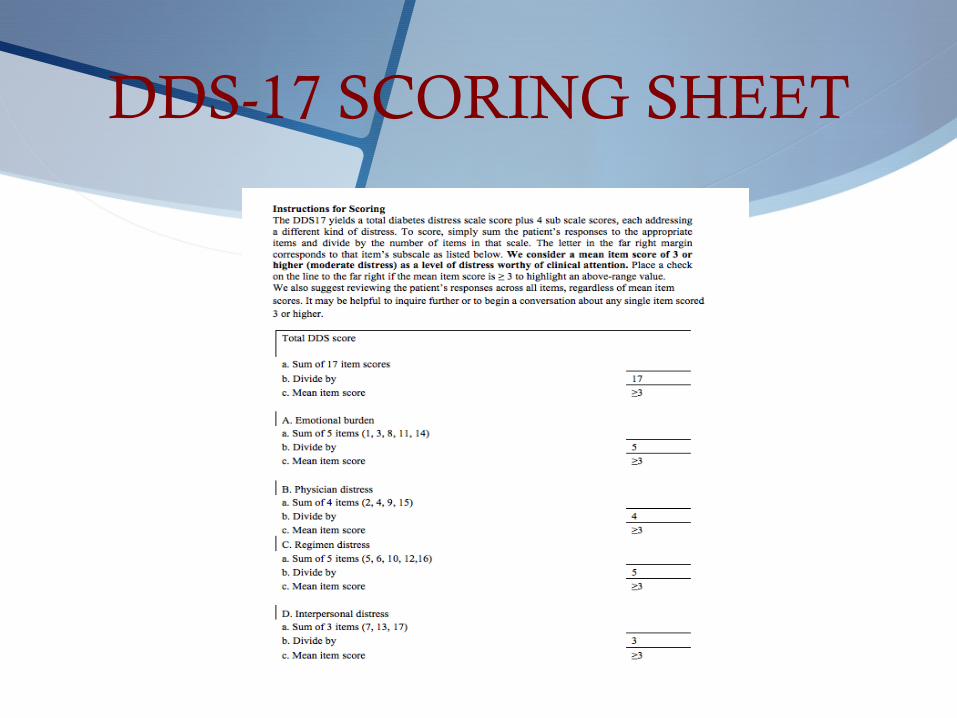
DDS-17 SCORING SHEET
A1C
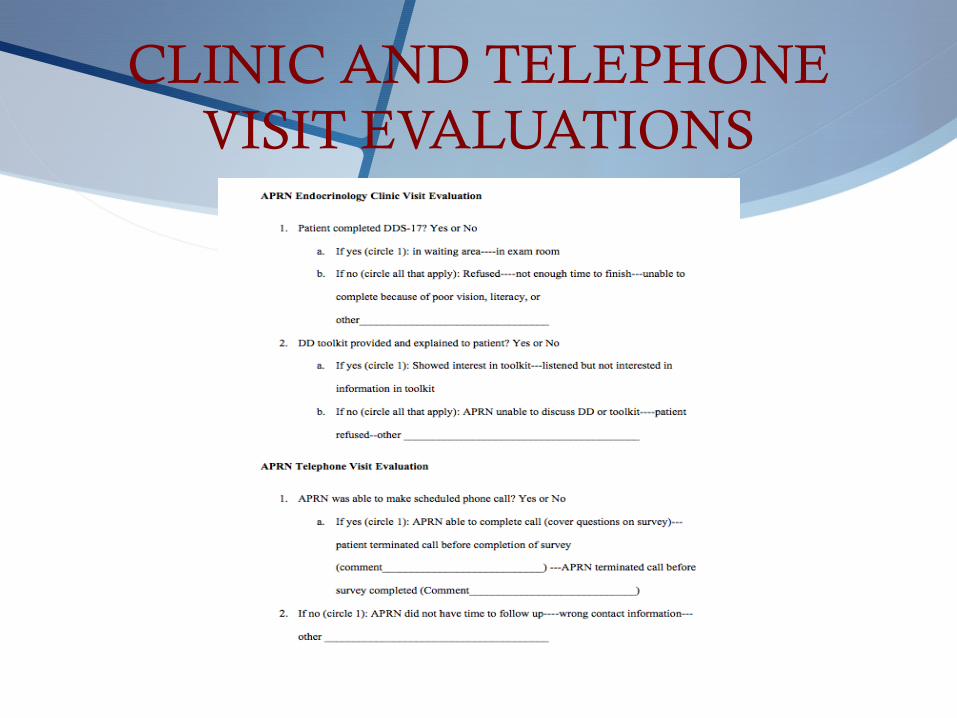
CLINIC AND TELEPHONE VISIT EVALUATIONS
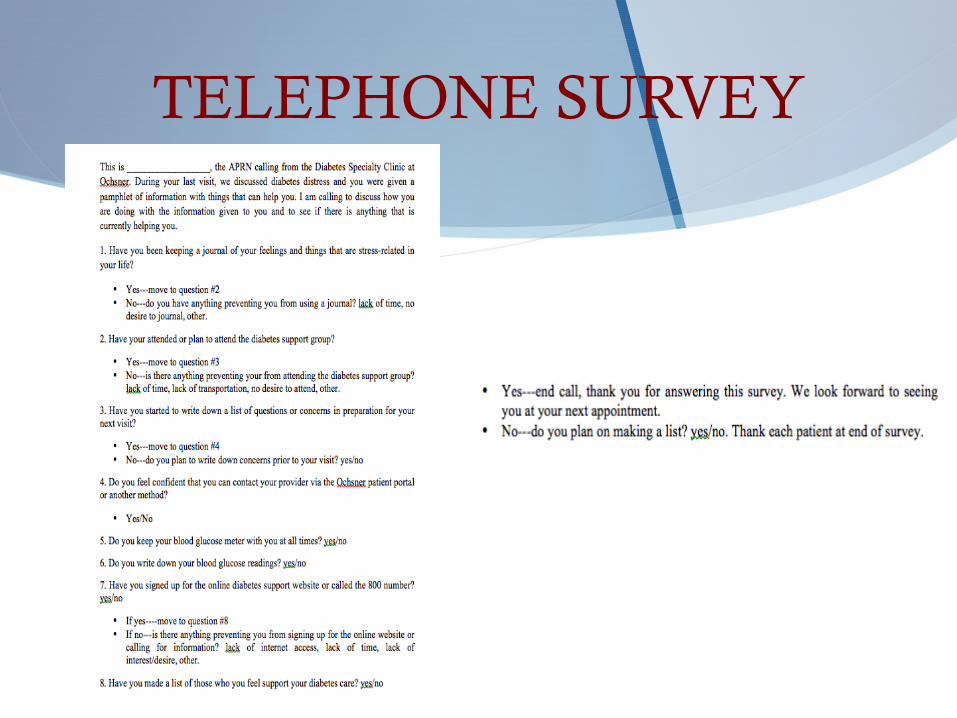
TELEPHONE SURVEY
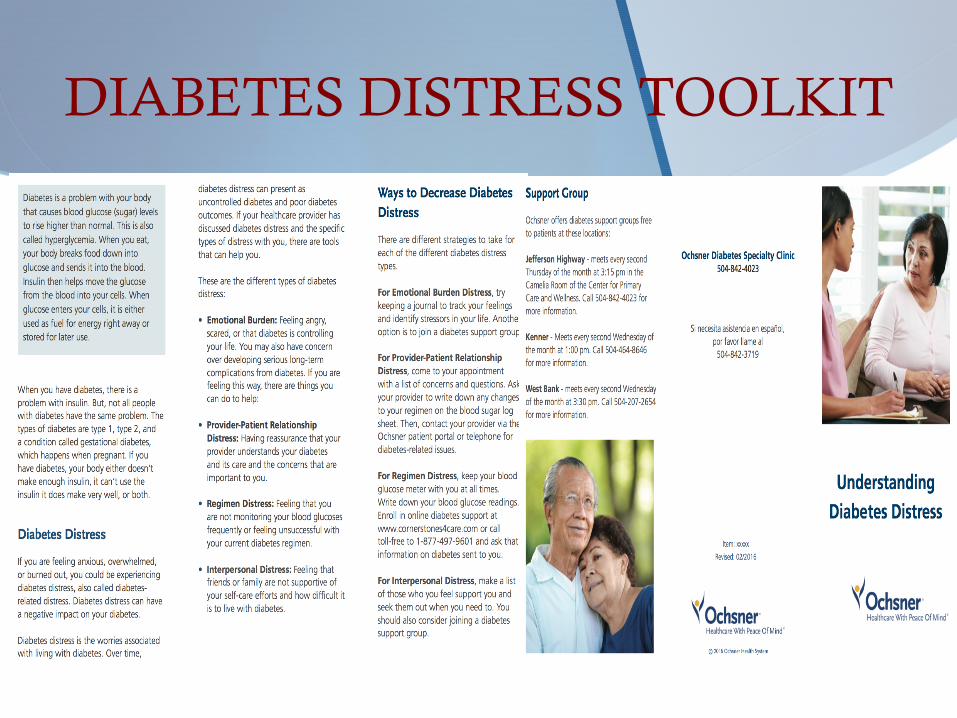
DIABETES DISTRESS TOOLKIT
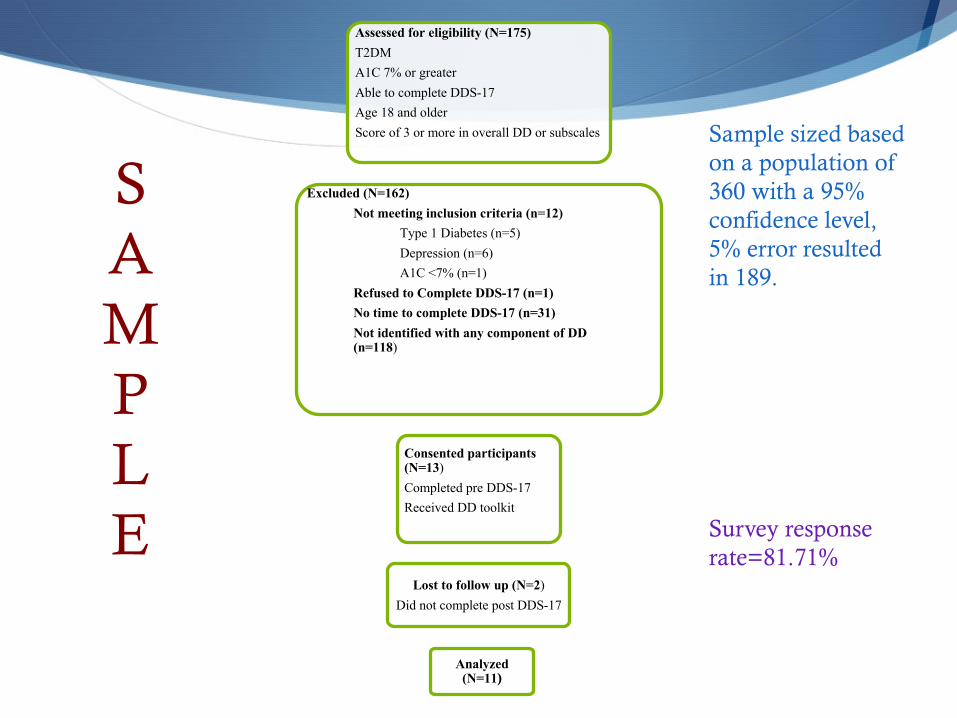
Assessed for eligibility (N=175) T2DMA1C 7% or greaterAble to complete DDS-17Age 18 and olderScore of 3 or more in overall DD or subscales
Excluded (N=162)Not meeting inclusion criteria (n=12)
Type 1 Diabetes (n=5)Depression (n=6)A1C <7% (n=1)
Refused to Complete DDS-17 (n=1)No time to complete DDS-17 (n=31)Not identified with any component of DD (n=118)
Consented participants (N=13)Completed pre DDS-17Received DD toolkit
Lost to follow up (N=2)Did not complete post DDS-17
Analyzed (N=11)
SAMPLE
Sample sized based on a population of 360 with a 95% confidence level, 5% error resulted in 189.
Survey response rate=81.71%
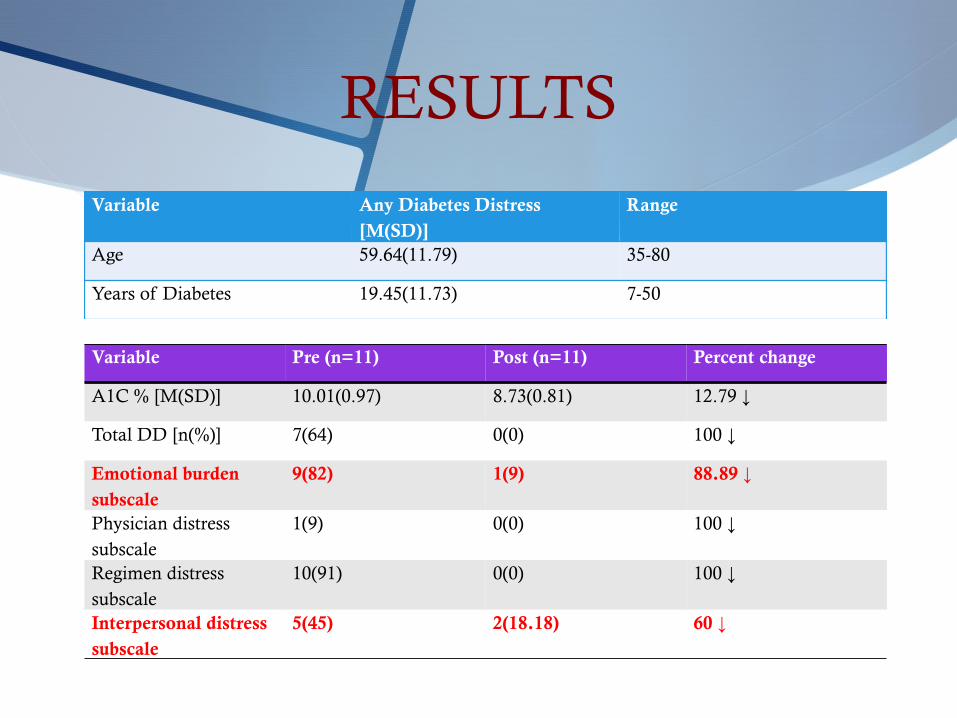
RESULTS
Variable Any Diabetes Distress [M(SD)]
Range
Age 59.64(11.79) 35-80
Years of Diabetes 19.45(11.73) 7-50
Variable Pre (n=11) Post (n=11) Percent change
A1C % [M(SD)] 10.01(0.97) 8.73(0.81) 12.79 ↓
Total DD [n(%)] 7(64) 0(0) 100 ↓
Emotional burden subscale
9(82) 1(9) 88.89 ↓
Physician distress subscale
1(9) 0(0) 100 ↓
Regimen distress subscale
10(91) 0(0) 100 ↓
Interpersonal distress subscale
5(45) 2(18.18) 60 ↓
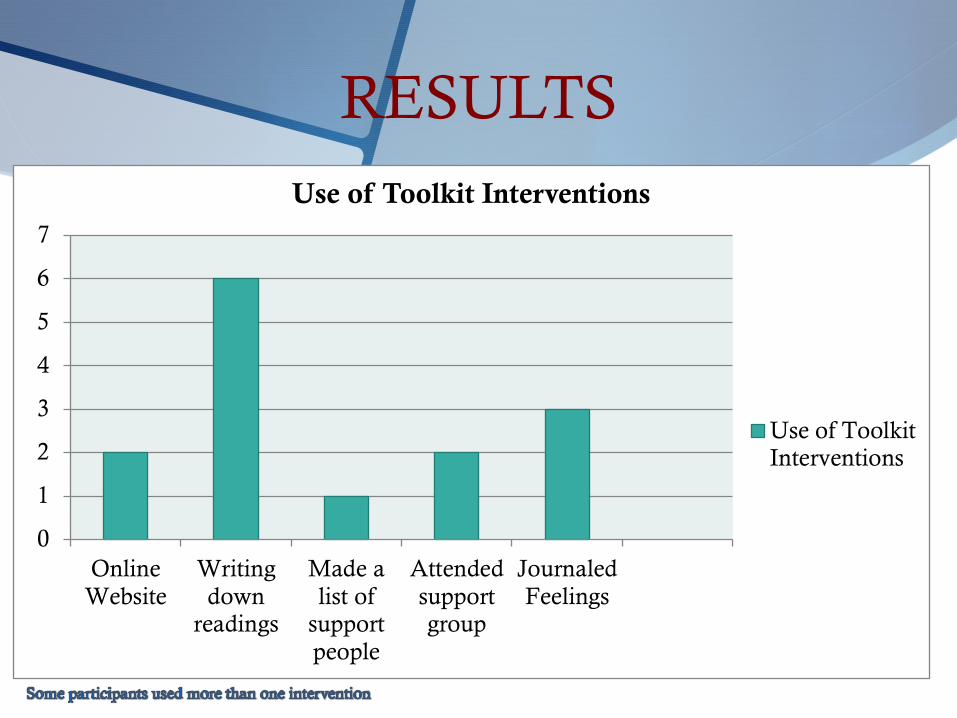
RESULTS
0
1
2
3
4
5
6
7
OnlineWebsite
Writingdown
readings
Made alist of
supportpeople
Attendedsupportgroup
JournaledFeelings
Use of Toolkit Interventions
Use of ToolkitInterventions
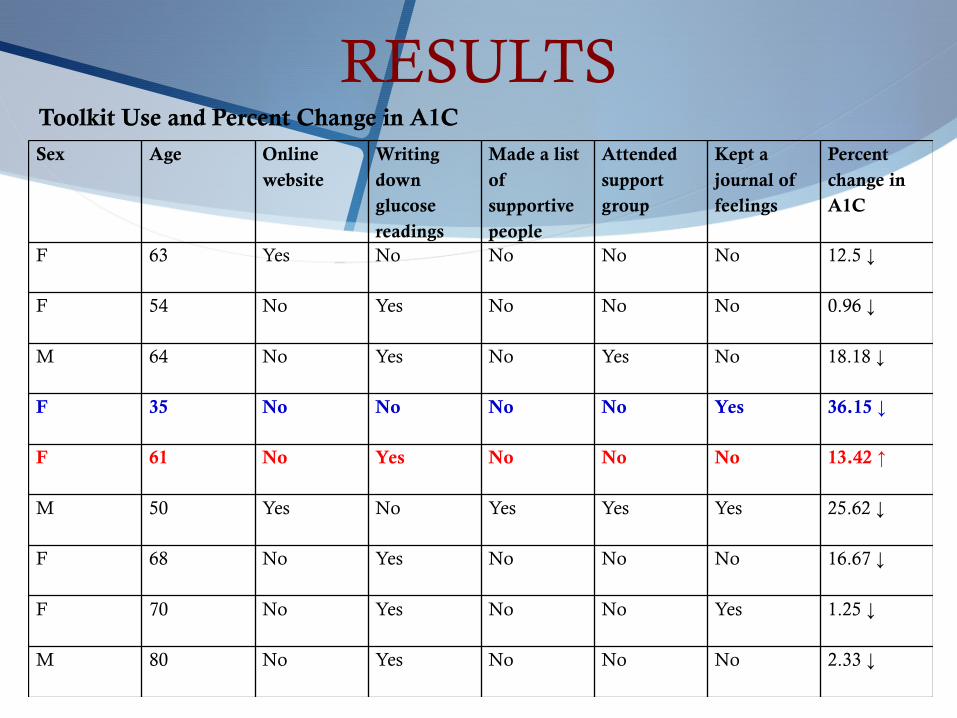
RESULTSSex Age Online
websiteWriting down glucose readings
Made a list of supportive people
Attended support group
Kept a journal of feelings
Percent change in A1C
F 63 Yes No No No No 12.5 ↓
F 54 No Yes No No No 0.96 ↓
M 64 No Yes No Yes No 18.18 ↓
F 35 No No No No Yes 36.15 ↓
F 61 No Yes No No No 13.42 ↑
M 50 Yes No Yes Yes Yes 25.62 ↓
F 68 No Yes No No No 16.67 ↓
F 70 No Yes No No Yes 1.25 ↓
M 80 No Yes No No No 2.33 ↓
Toolkit Use and Percent Change in A1C
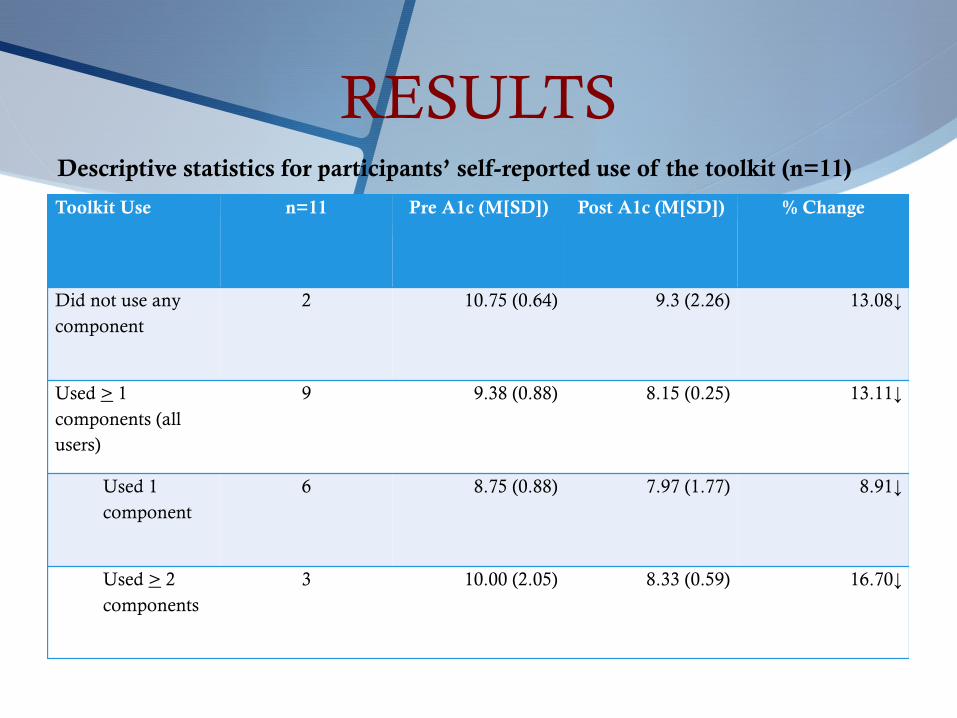
RESULTS
Toolkit Use n=11 Pre A1c (M[SD]) Post A1c (M[SD]) % Change
Did not use any component
2 10.75 (0.64) 9.3 (2.26) 13.08↓
Used > 1 components (all users)
9 9.38 (0.88) 8.15 (0.25) 13.11↓
Used 1 component
6 8.75 (0.88) 7.97 (1.77) 8.91↓
Used > 2 components
3 10.00 (2.05) 8.33 (0.59) 16.70↓
Descriptive statistics for participants’ self-reported use of the toolkit (n=11)
RESULTS
S Is it feasible to measure DD and implement a DD toolkit in patients with T2DM being treated in an APRN-led diabetes specialty clinic?
S What are the reports of patients with uncontrolled T2DM and moderate to high DD in those that used the interventions in the toolkit versus those that did not use the interventions?
Yes. Decreases in A1C, total DD, and distress in each subscale occurred.
Online website helpful in choosing foods and aiding in diabetes self-care
Glucose monitoring increased self-accountability; support group helpful
Common themes in those not using any interventions were lack of time, no desire, no transportation, or no computer/Internet access.
RESULTS
S What are the diabetic outcomes in T2DM with moderate to high DD that used the toolkit compared to those that did not use the toolkit?
S What are the barriers and facilitators in those patients with T2DM and moderate to high DD that used the DD toolkit?
No use: 13.08% decrease1 component: 8.91% decrease2 or more components: 16.70% decrease
Computer/Internet accessTransportationSelf-motivationLack of financial burden
LIMITATIONSS Conducted in one setting
S Some interventions required access to a computer and/or transportation
S Recall bias in telephone surveys
S Low participation
S Established relationship with APRN
S Consenting process during clinic appointment
S Changes in diabetes medications/doses
SIGNIFICANCE
S These findings of improved DD and A1C levels from this project reinforce the need to change the current practice in the clinical setting and screen patients for DD.
S APRN education on DD and implementing a screening tool with interventions can be helpful in improving patient care.
S Guidelines on diabetes care could eventually change to reflect the need to screen for DD as a part of routine diabetes care.
SUSTAINABILITY AND IMPROVEMENTS
S Low cost and minimal use of additional resources.
S Screening for DD supported in the literature.
S Suggestions for improvementS Expand screening for DD to all APRN patients in the diabetes
specialty clinic
S Provide patients with information on DD before using the screening tool.
S Provide those without internet access or transportation with additional resources could be beneficial
S Avoid consenting during the clinic visit time
SUSTAINABILITY AND IMPROVEMENTS
S Explore ways to combat possible social desirability
S Avoid changing diabetes regimen during the intervention
S If regimen changed, keep track of which participants regimen was changed
DISSEMINATION
S Diabetes Specialty Clinic department presentation: March 7, 2017
S Podium presentation at Sigma Theta Tau Research Day: April 21, 2017
S Podium and poster presentation at OHS Research Night: May 16, 2017
S OHS RN residency program: June 14, 2017
S Speaker at Endocrinology and Diabetes Summit: September 2017
CONCLUSION
S DD is related to uncontrolled diabetes and poor outcomes
S It is feasible to screen for DD in the clinical setting and implement interventions
S Interventions aimed at improving DD and diabetes should extend into the personal environment of patients as well as family members
S Diabetes is a chronic problem that requires the use of evidence based practices and quality improvement initiatives
S Screening for DD and implementing interventions to target DD can help to improve diabetes outcomes
REFERENCESAmerican Diabetes Association. (2015). Statistics about diabetes. National Diabetes Statistics Report.
Retrieved from http://www.diabetes.org/diabetes- basics/statistics/Berry, E., Lockhart, S., Davies, M., Lindsay, J.R., & Dempster, M. (2015). Diabetes distress:
Understanding the hidden struggles of living with diabetes and exploring intervention strategies. Postgraduate Medical Journal, 91, 278-283.
Centers for Disease Control and Prevention. (2014). Estimates of Diabetes and its burden in the Untied States. National Diabetes Statistics Report. Retrieved from cdc.gov/diabetes/pdfs/data/2014-report-estimates-of-diabetes-and-its-burden-in-the-United-States.pdf.
Dale, J.R., Williams, S.M., & Bowyer, V. (2012). What is the effect of peer support on diabetes outcomes in adults? A systematic review. Diabetic Medicine, 1361-1377.
Fisher, L., Skaff, M.M., Mullan, J.T., Arean, P., Mohr, D., Masharani, U., Glasgow, R., & Laurencin, G. (2007). Clinical depression versus distress among patients with type 2 diabetes. Diabetes Care, 30(3), 542-548.
Fisher, L., Glasgow, R.E., & Strycker, L.A. (2010). The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care, 33(5), 1034-1036.
Fisher, L., Hessler, D.M., Polonsky, W.H., & Mullan, J. (2012). When is diabetes distress clinically meaningful? Establishing cut points for the diabetes distress scale. Diabetes Care, 35, 259-264.
Hessler, D., Fisher, L., Glasgow, R.E., Strycker, L.A., Dickinson, L.M., Arean, P.A., & Masharani, U. (2014). Reductions in regimen distress are associated with improved management and glycemic control
over time. Diabetes Care, 37, 617-624.
REFERENCESJansen, H.J., Vervoort, G.M.M., de Haan, A.F.J., Netten, P.M., de Grauw, W.J., Tack, C.J. (2014). Diabetes-
related distress, insulin dose, and age contribute to insulin-associated weight gain in patients with type 2 diabetes: Results of a prospective study. Diabetes Care, 37, 2710-2717.
Karlsen, B. & Bru, E. (2014). The relationship between diabetes-related distress and clinical variables and perceived support among adults with type 2 diabetes: A prospective study. International Journal of Nursing Studies, 51, 438-447.
Liu, Y., Han, Y., Shi, J., Li, R., Li, S., Jin, N., Gu, Y., & Guo, H. (2014). Effect of peer education on self-management and psychological status in type 2 diabetes patients with emotional disorders. Journal of Diabetes Investigation, 6(4), 479-486.
Moran, K., Burson, R., & Conrad, D. (2014). The doctor of nursing practice scholarly project: A framework for success. Jones and Bartlett Learning: Burlington, MA.
Fisher, L., Hessler, D., Glasgow, R.E., Arean, P.A., Masharani, U., Naranjo, D., & Strycker, L.A. (2013). REDEEM: A pragmatic trial to reduce diabetes distress. Diabetes Care, 36, 2551-2558.
Fisher, L., Hessler, D., Masharani, U., & Strycker, L. (2014). Impact of baseline patient characteristics on interventions to reduce diabetes distress: the role of personal conscientiousness and diabetes self-efficacy. Diabetes Medicine, 31(6), 739-746.
Fonda, S.J., McMahon, G.T., Gomes, H.E., HIckson, S., & Conlin, P.R. (2009). Changes in diabetes distress related to participation in an internet-based diabetes care management program and glycemic control. Journal of Diabetes Science and Technology, 3(1), 117-124.
Partiprajak, S., Hanucharurnkul, S., Piaseu, N., Brooten, D., & Nityasuddhi, D. (2011). Outcomes of an advanced practice nurse led type 2 diabetes support group. Pacific Rim International Journal of Nursing, 15(4), 288-304.
REFERENCESPhillips, A. (2014). Diabetes-related grief and distress: Recognition in practice. Practice Nursing 2014, 25(12), 615-618.Pick, A. (2009). An evaluation of patient participation groups for people. Practice Nursing, 20(1), 41-46. Polonsky, W.H., Fisher, L., Earles, J., Dudi, R.J., Lees, J., Mullan, J., & Jackson, R.A. (2005). Assessing
psychosocial distress in diabetes: Development of the diabetes distress scale. Diabetes Care, 28(3), 626-631.
Sarwat, S., Ilag, L., Carey, M.A., Shrom, D.S., & Heine, R.J. (2010). The relationship between self-monitored blood glucose values and glycated haemoglobin in insulin-treated patients with Type 2 diabetes. Diabetic Medicine, 27, 589-592.
Smaldone, A., Ganda, O.P., McMurrich, S., Hannagan, K., Lin, S., Caballero, A.E., & Weinger, K. (2006). Should group education classes be separated by type of diabetes. Diabetes Care, 29(7), 1656-1658.
Tovote, K.A., Fleer, J., Snippe, E., Peeters, A.C.T.M., Emmelkamp, P.M.G., Sanderman, R., Links, T.P., & Schroevers, M.J. (2014). Individual mindfulness-based cognitive behavior therapy for treating depressive symptoms in patients with diabetes: Results of a randomized controlled trial. Diabetes Care, 37, 2427-
2434. Vries, L.D., Heijden, A.A.V.D., Riet, E.V., Baan, C.A., Kostense, P.J., Rijken, M., Rutten, G.E., & Nijpels, G.
(2014). Peer support to decrease diabetes-related distress in patients with type 2 diabetes mellitus: Design of a randomized controlled trial. BMC Endocrine Disorders, 14, 21.
Wagner, J.A., Tennen, H., Feinn, R., & Osborn, C.Y. (2015). Self-reported discrimination, diabetes distress, and continuous blood glucose in women with type 2 diabetes. Journal of Immigrant and Minority Health, 17, 566-573.
REFERENCESYu, C.H., Parsons, J.A., Mamdani, M., Lebovic, G., Hall, S., Newton, D., Shah, B.R., Bhattacharyya, O., Laupacis,
A., & Straus, S.E. (2014). A web-based intervention to support self-management of patients with type 2 diabetes mellitus: Effect on self-efficacy, self-care, and diabetes distress. BMC Medical Informatics and Decision Making, 14(117), 1-14.
Zagarins, S.E., Allen, N.A., Garb, J.L., & Welch, G. (2012). Improvement in glycemic control following a diabetes education intervention is associated with change in diabetes distress but not change in depressive symptoms. Journal of Behavioral Medicine, 35, 299-304.
Zhang, J., Xu, C., Wu, H., Xue, X., Xu, Z., Li, Y., Gao, Q., & Liu, Q. (2013). Comparative study of the influence of diabetes distress and depression on treatment adherence in Chinese patients with type 2 diabetes: A
cross-sectional survey in the People's Republic of China. Neuropsychiatric Disease and Treatment, 9, 1289-1294
Related Documents











