Diabetic Ketoacidosis… …when we are too sweet for our own good! Brenda Morgan RN BScN MSc Clinical Nurse Specialist, CCTC London Health Sciences Centre

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diabetic Ketoacidosis……when we are too sweet for our own good!
Brenda Morgan RN BScN MScClinical Nurse Specialist, CCTCLondon Health Sciences Centre

Pancreas
Endocrine�Alpha cells: glucagon�Beta cells: insulin �Delta: somatostatin�Delta: somatostatin�Pancreatic Polypeptide
Exocrine�Pancreatic juices

Physiology
Insulin
Glucagon

Insulin:Glucagon
Insulin Glucagon
Stimulated by: Stimulated by:Stimulated by:
�Increased BS
Stimulated by:
�decreased BS
�Exercise
�malnutrition
�increased AA
�SNS

Insulin Glucagon
Effects:
�Movement of glucose and K into cell
�Decreased fat mobilization
Effects:
�Raise blood sugar
�Gluconeogenesis
�Glycogenolysis�Decreased fat mobilization
�Decrease protein breakdown leaving protein available for cell growth
�Maintains serum osmolality
�Glycogenolysis
�Fat mobilization
�Protein mobilization

Fed State
� Insulin > Glucagon (insulin activity dominates)
� Movement of nutrients into cells
� Storage of nutrients for later use� Storage of nutrients for later use

Fasting State
� Glucagon > Insulin (glucagon activity dominates)
� Use of endogenous fuels to maintain blood sugar for energy and metabolismblood sugar for energy and metabolism

Fasting State
� Liver becomes major source for glucose
� Stored sugar in liver (glycogen) is converted to glucose (glycogenolysis)
� Decreased insulin causes lipolysis to � Decreased insulin causes lipolysis to increase free fatty acids (used for muscle fuel)

Fasting State
� Free fatty acids converted to ketones in liver by glucagon (another energy source for brain and muscle)– Beta-hydroxybutyrate vs acetoacetate– Beta-hydroxybutyrate vs acetoacetate
� Glycerol (released by lipolysis) and alanine (from protein catabolism) provides additional substrates for gluconeogenesis in liver

Other Triggers
� Cortisol
� Catecholamines
� Growth hormones

Renal Regulation
� Glucose filtered in glomerulus
� Filtered glucose reabsorbed in proximal tubules to maintain serum glucose
� Kidney removes excess glucose� Kidney removes excess glucose
� Decreased renal perfusion impairs glucose removal

Diabetic Complications
Effects of Diabetes� chronic complications develop in 75% of patients� magnitude and duration of hyperglycemia correlates to:
microvascular disease:� retinopathy� retinopathy� nephropathy
neuropathy� gastroparesis� diarrhea� impotence� resting tachycardia, bradyarrhythmias� postural hypotension� limb sensation

Diabetic Complications
Macrovascular diseases� coronary artery disease� peripheral vascular disease � cerebrovascular disease� hypertension� hypertension
Macrovascular and Neuropathy� foot disease
� risk increases with smoking, obesity, hyperglycemia, lipid abnormalities.
� increased lipid alterations increases with hyperglycemia� neuroglycopenia
Diabetic Ketoacidosis
� Primarily Type I DM risk
� Exaggerated expression of fasting state
� Little has changed in mortality� Little has changed in mortality
� Prevention of deaths through early detection
� Role for urine testing for ketones

DKA
Glucagon>Insulin
increased hepatic glucose production
Insufficient Insulin
LipolysisIncreased serum
osmolality
Ketosis
Anion Gap Acidosis
Osmotic Diuresis
Dehydration
Kushmaul breathing

Signs and SymptomsSigns and Symptoms

Key Features of DKA� Hyperglycemia� Anion gap metabolic acidosis� Ketonuria� Dehydration, secondary tachycardia and hypotensionhypotension
� Polyuria, polydipsia � Increased serum:urine osmolarity� Kussmaul's respiration; fruity acetone breath� Normal to low temperature� Hyperkalemia� Hyponatremia

Diabetic Ketoacidosis
� Hyperglycemia
� Metabolic acidosis with ketosis
� Fluid and electrolyte imbalance
� Altered mental state� Altered mental state� Only 10% in coma; 20% clear mentated
� Hypothermia may be present, but fever not due to DKA
� Look for precipitating event!

Hyperglycemic Hyperosmolar Non-Ketotic Syndrome (HONK, HHNS)
� Similar to DKA except hepatic ketogenesis is inhibited (insulin presence)
� Symptoms similar to DKA without ketosis and acidosis
� Hyperglycemia (and hyperosmolality) often � Hyperglycemia (and hyperosmolality) often worse (syndrome usually persists longer before seeking treatment; +/- renal impairment)
� Mortality higher than DKA� Larger volume deficit

Hypo or Hyper?
� Coma may occur in either
� Cold, clammy and shaky vs volume depleted, acidotic
� When in doubt?� When in doubt?
� Coma…look for other causes
Fluid and Electrolyte Impairment
� Dry, dry, dry
� Overall loss of sodium, potassium, chloride, phosphate and magnesium but serum levels often elevated due to serum levels often elevated due to hypovolemia or shifts

Management of DKA
� ABC’s with fluid resuscitation
� Insulin
� Electrolyte replacement
� Lab monitoring� Lab monitoring

Critical Lab Monitoring
• Glucose
• Sodium
• Bicarbonate
• Anion Gap• Anion Gap– Albumin
– Chloride

Osmolality
Calculated Osmolality
= (2 X Na + urea + Glucose + [EtoH])
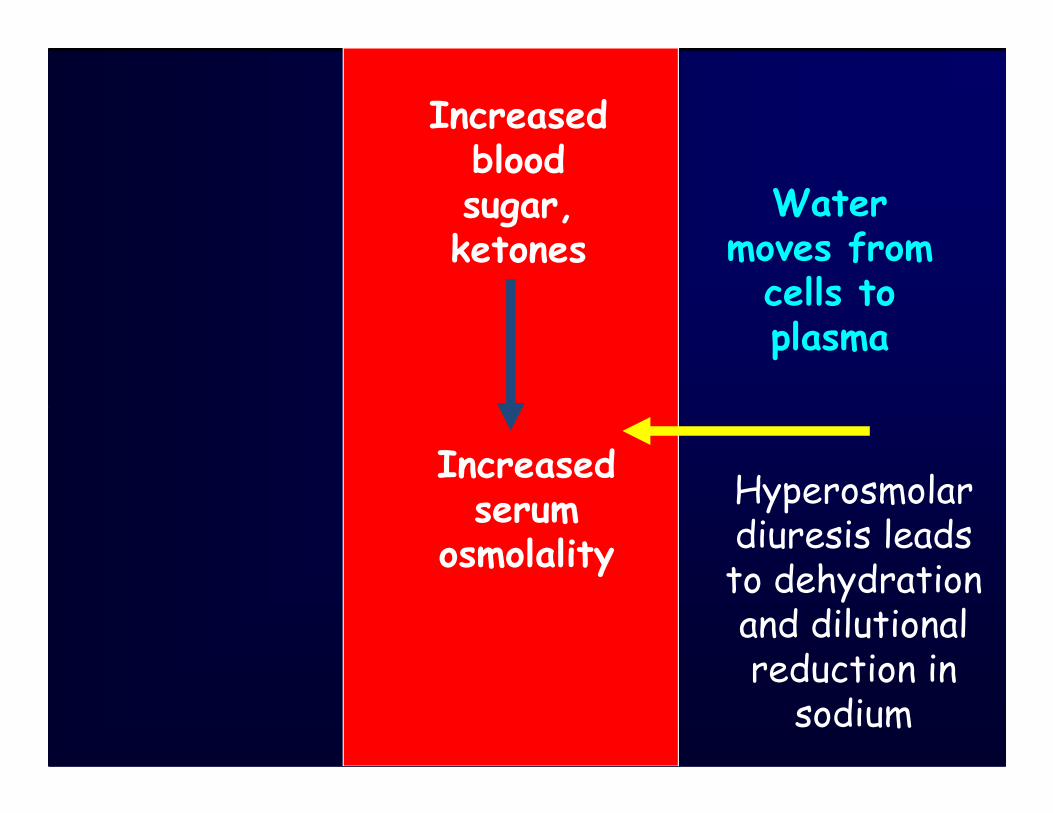
Increased blood sugar, ketones
Water moves from cells to plasma
Increased serum
osmolality
Hyperosmolar diuresis leads to dehydration and dilutional reduction in sodium

Sodium
� High or low
� Mild dilutional hyponatremia common
� High sodium in severe dehydration
� Net sodium deficit due to urinary loss � Net sodium deficit due to urinary loss (bound to ketones)
� Sodium can be falsely low with hyperglycemia
� Recalculate prior to changing IV infusion

Sodium Correction
� Several methods used
� Correction of sodium for hyperglycemia to identify underlying sodium deficit
� For every 10 mmol/L rise in blood glucose > 8 � For every 10 mmol/L rise in blood glucose > 8 mmol/L, upwardly correct Na by 3 mmol/L

Sodium Correction
Glucose-8 X 3 + Na10

Sodium Correction
Na = 138
Glucose = 49
What is the corrected sodium?

Sodium Correction
Na = 138
Glucose = 49
Glucose-8 X 3 + Na10

Sodium Correction
Na = 138
Glucose = 49
49-8 X 3 + 13810

Corrected Sodium
Na = 150

Chloride
� Net chloride loss is often less than sodium (not bound to ketones)
� Hyperchloremia commonly develops following fluid resuscitation with 0.9% following fluid resuscitation with 0.9% NaCl
� Vomiting causes loss of chloride ions (favouring alkalosis)� Mixed picture

Potassium� May have normal, hyper or hypokalemia (20%)
� Deficit usual present due to diuresis, GI loss and dehydration induced aldosterone releaserelease

Potassium� Insulin deficit causes shift from cells:
� May present with hyperkalemia despite overall deficit
� Renal impairment may be associated with hypekalemiahypekalemia

Ketones
• In DKA, beta hydroxybutyrate to acetacetate ratio is 3:1
• Most labs measure acetoacetate (nitroprusside reagent test strip)
• Ketonuria may be under-detected in early DKA• Ketonuria may be under-detected in early DKA• Insulin converts beta-hydroxybutyrate to acetoacetate, increasing ketonuria during recovery
• Ketonuria detection ~36 hours post stabilization; poor marker of resolution

Anion gap is calculated when metabolic acidosis is diagnosed, to help narrow down the possible cause.
Anion Gap =
Assessment of Metabolic Acidosis
Anion Gap =
Cations (+ charges) – Anions (- charges)

Measured Cations Measured Anions
Sodium
Potassium
chloride
bicarb
Total Cations:
135-145
3.5-5.0
98-107
22-29
Total Cations: Total Anions:
144 mmol/L 130 mmol/L
Normal = ~7-15 (if K is included)
-
Normal = ~3-11 (if K excluded)

Measured Charges:
Cations > Anions

Unmeasured Anions (-) Unmeasured Cations (+)protein 15 mmol/L potassium 4.5 mmol/LPO4 2 mmol/L calcium 5.0 mmol/LSO4 1 mmol/L magnesium 1.5 mmol/Lorganic acids 5 mmol/L
Total 23 mmol/L Total 11 mmol/L
Unmeasured Charges:
Anions > Cations

An increased anion (fewer measured negatives) usually indicates there are more unmeasured negatives.
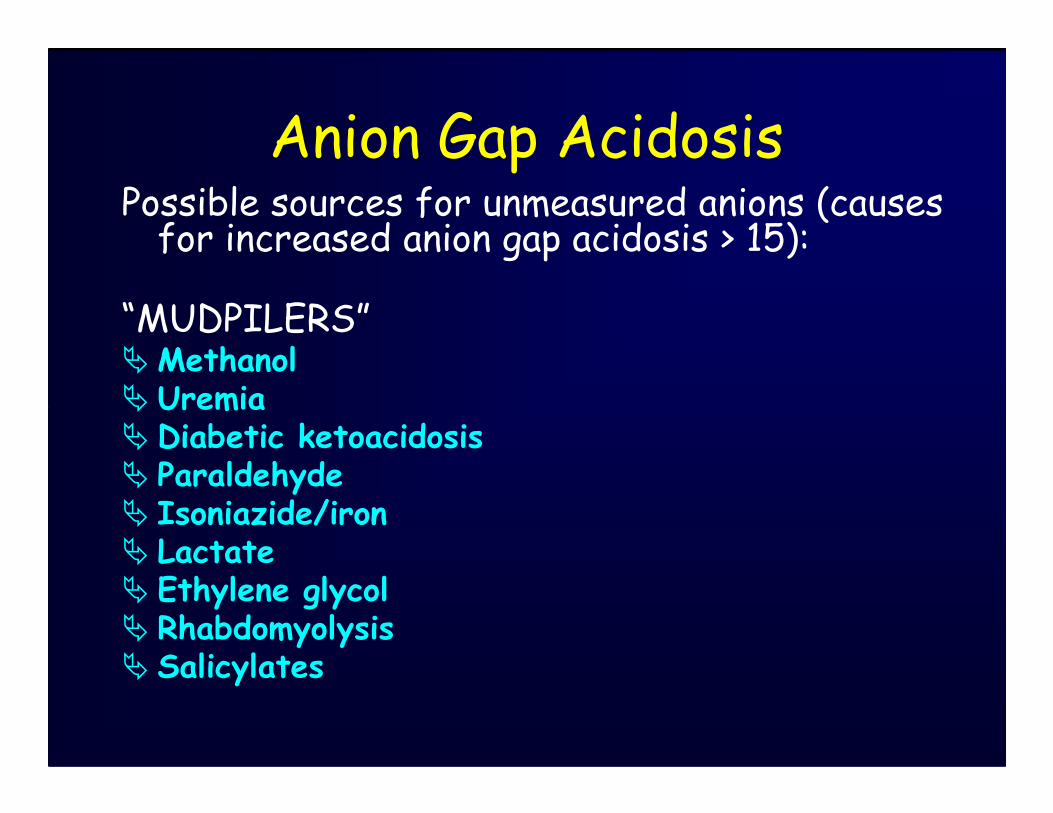
Anion Gap AcidosisPossible sources for unmeasured anions (causes for increased anion gap acidosis > 15):
“MUDPILERS”�Methanol� Uremia� Uremia� Diabetic ketoacidosis� Paraldehyde� Isoniazide/iron� Lactate� Ethylene glycol� Rhabdomyolysis� Salicylates

Na 144
K 5.2
Cl 95
144
104
40
Is this an anion gap acidosis?
HCO3 9
Glucose 45
104

Na 144
K 3.2
Cl 118
144
136
8
Is this an anion gap acidosis?
HCO3 18136

Unmeasured Anions (-) Unmeasured Cations (+)protein 15 mmol/L potassium 4.5 mmol/LPO4 2 mmol/L calcium 5.0 mmol/LSO4 1 mmol/L magnesium 1.5 mmol/Lorganic acids 5 mmol/L
Total 23 mmol/L Total 11 mmol/L
6.5
What is the effect of a low albumin?

Na 144
K 3.2
Cl 118
144
136
8
Is this an anion gap acidosis?
HCO3 18
Albumin 11
136
Corrected:
8 + 2.5 (3) = 15.5

Decreased or Falsely Normal Anion Gap Acidosis
� Decreased measured cations (e.g., sodium)
� Low serum protein � Low serum protein � Causes decrease in number of unmeasured protein anions
� If anion gap is normal, other unmeasured anions must be present

In ketoacidosis:
• Insulin decreases ketosis
• Ketones excreted with hydrogen or ammonium reduce ketosis and acidosisammonium reduce ketosis and acidosis
• Ketones also excreted with sodium or potassium (causing loss of bicarb precursors); acidosis persists despite reduction in anion gap

In ketoacidosis:
� Hyperchloremia (0.9% NaCl administration) a common cause of non-anion gap acidosis
� Non-anion gap acidosis very common for day or two post resolution of DKA (due to potential two post resolution of DKA (due to potential bicarb loss and chloride administration)
• Anion gap increases by 1 for every decrease in bicarbonate with ketoacidosis
• An anion gap increase > fall in bicarb suggests additional organic acids present (e.g., lactate)

Na 144
K 4.6
Cl 114
HCO3 8
144
122
22
Is this an anion gap acidosis?
HCO3 8
Albumin 38
122
Normal bicarb (24) – Actual bicarb (10) = 14
Measured gap (22) – Normal gap (8) = 14
AG = bicarb deficit

Na 149
K 5.2
Cl 108
149
114
35
Is this anion gap due to ketoacidosis?
HCO3 6
Glucose 35
Albumin 38
114
Normal bicarb (24) – Actual bicarb (6) = 18
Measured gap (35) – Normal gap (8) = 27
AG > bicarb deficit

Na 142
K 4.0
Cl 119
142
136
6
Is this an anion gap acidosis?
HCO3 17
Glucose 12
136
Normal bicarb (24) – Actual bicarb (17) = 7
Measured gap (6) – Normal gap (8) = 0
Bicarb deficit > AG

Treatment Principles
� ABCs with fluid resuscitation� Rehydration reduces hepatic glucose production, promotes insulin action and renal glucose clearance.renal glucose clearance.
� Insulin (stop ketogenesis, liploysis and gluconeogenesis)
� Assess potassium or add to IV empirically if producing urine
Treatment Principles
� Fluid and electrolye replacement
� Correct blood pH
� Monitor glucose q 1 h and lytes q2h for patient in shockpatient in shock
� Monitor bicarbonate, anion gap and calculated osmolality

Osmolality:
2(Na) + urea + glucose2(Na) + urea + glucose

Rapid reduction in osmolality
(rapid reduction of Na or glucose)
Water moves from plasma to interstitium and cells
Decreased
osmolality
Cerebral edema can occur

Glucose Correction
� Insulin 0.1 unit/kg IV bolus plus� Insulin 0.1 unit/kg/h infusion
� Higher doses exceed insulin saturation capacitycapacity
� Q 1 H blood sugar checks (lab)
� Double infusion if glucose has not dropped after first hour
� Double again once if glucose has not dropped in second hour

Glucose Correction
� SC regimen with insulin Lispo for non-shock patients
� Requires hourly blood sugar measurementmeasurement
� 0.3 u/kg SC bolus, then 0.1 u/kg q 1h until glucose 13-15 mmol/L

Glucose Correction
� Goal: 3-5 mmol/L/hr reduction
� If glucose falls > 5 mmol/L, reduce infusion (do not stop)
� Add 5% dextrose to saline once glucose � Add 5% dextrose to saline once glucose ~15-16 mmol/l

Glucose Correction
� Correct to 10-12 mmol/L; avoid lower levels in first 24 hours
� DO NOT use Intensive Insulin protocol for DKAfor DKA
� When glucose <13-15 mmol/L, anion gap is < 12, bicarb > 18 and patient eating, return to usual insulin Rx
� Continue infusion 1-2 hours after initial sliding scale dose

Fluid Replacement
� 5-8 L average loss; aggressive replacement to maintain MBP >70 and adequate urine output
� Start with 0.9% NaCl (correct Na � Start with 0.9% NaCl (correct Na deficit, protects against rapid reduction in osmolality) � Hypernatremia usually volume deficit
� 4-15 mL/kg/hr; usually 1 L/hour for average adult
Fluid Replacement
� Conversion to 0.9% NaCl after volume deficit replaced
� Additional of 40 mmol KCl/L IV increases osmolality of solution and will increases osmolality of solution and will delay correction of hyperosmolality
� 0.45 % NaCl with 40 mmol KCl/L or Ringers following hemodynamic stabilization and correction of defict

Saline
� 0.9% � 154 mmol sodium and chloride/L, 300 mosmol
� 0.45%� 0.45%� 77 mmol sodium and chloride/L
� 0.25%� 39 mmol sodium and chloride/L

Saline
� Lactated Ringers� 130 mmol sodium and 109 mmol chloride/L
� 28 mmol lactate, 4 mmol potassium� 28 mmol lactate, 4 mmol potassium

Goals
� Slow downward correction in sodium if hypernatremic
� If sodium rising or not improving after rehydration, consider Ringers or 0.45% rehydration, consider Ringers or 0.45% NaCl
� Recheck corrected sodium before downscaling sodium

Potassium
� Insulin and rehydration will lower potassium
� Add 20 mmol/L if K < 5.5 and patient producing urine with initial producing urine with initial resuscitation; bolus prn
� Safer to add K if potassium value unknown

Phosphate
� May be low, treatment controversal except� If low at presentation should be treated (insulin will drop it further)(insulin will drop it further)
� Monitor phosphate and magnesium and treat according to usual protocol

Acidosis
� Corrects slowly, hours post glucose normalization
� Ketosis corrects faster than hyperchloremic acidosishyperchloremic acidosis� Acidosis may persist after anion gap is corrected
� Anion gap is best method of determining that ketosis is corrected

Acidosis
� Avoid bicarb, not usually given unless pH <7.00 or patient has life-threatening hyperkalemia
� Bicarb administration increase CO2 � Bicarb administration increase CO2 production with drop in cerebral pH as CO2 crosses blood brain barrier
� Alkali administration may slow resolution of ketosis and/or cause alkalosis

Acidosis
� Insulin administration key
� Continue insulin infusion until anion gap corrected; give additional glucose if needed to maintain blood glucoseneeded to maintain blood glucose
� Monitor pH (venous pH acceptable) and anion gap for resolution

Cerebral Edema
� Highest risk in children
� Rapid reduction of osmolality poses risk, bicarb administration associated with more cerebral edemamore cerebral edema
� Monitor for headache, lethargy, altered LOC

Cerebral Edema
� Consider 0.25-1 g/kg mannitol or 5-10 ml/kg 3% saline
� 70% mortality; 7-14% good neurological recoveryrecovery

Case 1
• 25 year old woman, 26 weeks gestation
• Flu like symptoms, vomiting and diarrhea
• Felt too unwell to eat, withheld insulin
• Resumed eating and insulin on following • Resumed eating and insulin on following day
• Still feeling week

Case 1
In ED:
• Glucose 16.8
• Lytes: Na 145 K 4.9 Cl 109 Bicarb 15
• 3+ ketones• 3+ ketones
• “Resolving DKA, resume diabetic management”
Corrected Na: ~148
Anion Gap: 21

Case 1
• Labs following day:
• Na 148 K 4.9 Cl 111 Bicarb 12
• Glucose 22
• Sleepy• Sleepy
Corrected Na: ~153
Anion Gap: 25

Case 1
� Treated as DKA with IV insulin, 0.9% Nacl with potassium replacement
� The following day:� Na 143 K 3.9 Cl 118 Bicarb 18� Na 143 K 3.9 Cl 118 Bicarb 18
� Concern regarding persistent acidosis
Anion Gap: 7
Bicarb Gap: 6

Case 2
• 28 year old woman, DMI since childhood
• “poor control”
• Admitted in coma with DKA
• Lab on admission:• Lab on admission:Glucose: 42Lytes: Na 144 K 5.1 Cl 108 Bicarb 8
• Ketones: 1+
Anion Gap: 28
Corrected Sodium: 152

Case 2
• Blood glucose drops to 3.5 after 12 hours
• Insulin infusion stopped and D50 administeredadministered
• Over next 12 hours, glucose < 8 mmol/L
• Bicarb dropping; anion gap widening

Case 3• 81 year old woman, DMI since 27
• Admitted in coma
• Blood glucose 36
• Na 148 K 5.5 Cl 110 Bicarb 4• Na 148 K 5.5 Cl 110 Bicarb 4
• What is her anion gap?
• Is this DKA alone?
Anion Gap: 34
Corrected Sodium: 156
Bicarb Gap: 20

Case 4
� 18 year old woman, DMI since age 12
� Well controlled
� Celebration
� Admitted with DKA� Admitted with DKA
� Transferred to Level 3 on Day 2
� CT shows no differentiation between grey and white

Summary
� Rehydration to restore and maintain MBP
� Initial resuscitation with 0.9% NaCl
� Maintain renal perfusion� Maintain renal perfusion
� Insulin bolus 0.1 unit/kg and continuous infusion 0.1 unit/kg/hr with potassium to IV
� Add potassium to IV unless hyperkalemic; monitor lytes q 1h

Summary
� Avoid glucose reduction > 5 mmol/L/hr
� Add dextrose to IV once glucose < 16 mmol/L
� Treat with insulin until glucose < 13-15; � Treat with insulin until glucose < 13-15; AG < 12, bicarb > 18 and eating
� Continue IV insulin 1-2 hours after initial SC

Summary
� DO NOT STOP INSULIN
� DO NOT USE INSULIN PROTOCOL DURING ACUTE PHASE

References
� Kitabchi (2006). Hyperglycemic crisis in adult patients with diabetes: a consensus statement from the American Diabetes Association. Diabetes Care. Diabetes Association. Diabetes Care. 29:2739.
� Kitabchi (2009). Treatment of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults. Uptodate on-line. Last update: May 1, 2009.
Related Documents






![1 Developed by the Canadian Nurses Association and the Registered Nurses Association of Ontario Adapted for use by [name of PEACE site]](https://static.cupdf.com/doc/110x72/5516abfd550346f0208b5068/1-developed-by-the-canadian-nurses-association-and-the-registered-nurses-association-of-ontario-adapted-for-use-by-name-of-peace-site.jpg)




