
DIZZINESS Vertigo Light-headedness Dysequilibrium Imbalance Near Syncope Floating Whooziness Visual distortion Ataxia Anxiety.
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


DIZZINESS
• Vertigo • Light-headedness• Dysequilibrium • Imbalance • Near Syncope
• Floating• Whooziness• Visual distortion• Ataxia• Anxiety

Evaluation of patient with dizziness
History
Physical exam
Vestibular function test
3

HistoryVertigo? (unsteadiness/dysequilibrium)• Illusory sense of motion
(internal or objects-linear/rotatory or change in orientation)
• Vertigo indicates a problem within the vestibular system (anywhere)
4
History
Episodic or Continuous?
• Most vestibulopathies cause flactuating or episodic symptom
• Episodic: <1min BPPV >1day Vestibular Neuritis
5

History
Semicircular canals or otolith?
• Movement of objects: semicircular canals• Abnormal sense of tilt or sudden drop : otolith
organs
6
HistoryMedical problem?• Cause or exacerbate patient’s symptomsDisease: DM, Thyroid, Anemia, Arrhythmia, Orthostatic hypotensionDrugs : AG, Cis-platin, Antiepileptic, Amiodarone,
Alcohol, Barbiturates, Tricyclics, Anticoagulant
7

HistoryPsychogenic disorder?
• Anxiety• Panic disorder• Phobic disorder• Depression / OCD
agoraphobia: mimics vestibulopathy Phobic postural vertigo: fluctuating unsteadiness
and subjective disturbance of balance
8

HistoryTriggers?
• Rolling over in bed/head backward and toward BPPV• Foods vestibular migraine• Loud noise (Tullio’s phenomenon) Meniere’s
dis.
9

HistoryEffect of head movement?
• Oscillopsia Vestibular hypofunction
• Brief periods of vertigo induced by certain head movements Vascular compression
10

HistoryAssociated symptoms?
• Aural fullness/tinnitus/HL Meniere’s dis.• Dysarthria/Diplopia/Paresthesia VBI• Sweating/Dyspnea/Palpitation Panic attacks• Aura/Headache Migraine related vertigo
11
History
• Must begin in open ended fashion
• Complete a quastionaire
12

Evaluation of patient with dizziness
History
Physical exam
Vestibular function test
13

Vestibular System Function
Balance maintained by :1. Vestibular system2. Eyes3. Proprioceptors in the muscles
• Allows for:– gaze & postural stability– sense of orientation– detection of linear & angular accelerations

BalanceAnatomy & Physiology
• Vestibular sense organ, consists of :
# 3 semicircular canals angular acceleration. # Utricle & saccule linear
acceleration.

Bedside examination
vestibular functions:
Vestibulo-ocular: ocular motor function
Vestibulospinal: maintain posture and muscular tone
16

Vestibulo-ocular pathway


• The three planes of operation of the vestibuloocular reflex (VOR). Sagittal pitch plane (green), frontal roll plane (gray), horizontal yaw plane (green) [23].
• Nystagmus in defined disorders in the three planes of operation of the VOR. Tonus imbalance in the pitch plane leads to a vertical nystagmus (upbeat or downbeat nystagmus). Disorders in the roll plane cause a torsional nystagmus while disorders of the VOR in the yaw plane cause a horizontal nystagmus.

VOR of LSCC origin

vestibulo-ocular reflex of otolith-organ origin. When the
head is tilted to the left, the eyes rotate to the right to
assume a new angular position
about the visual axes, as shown.
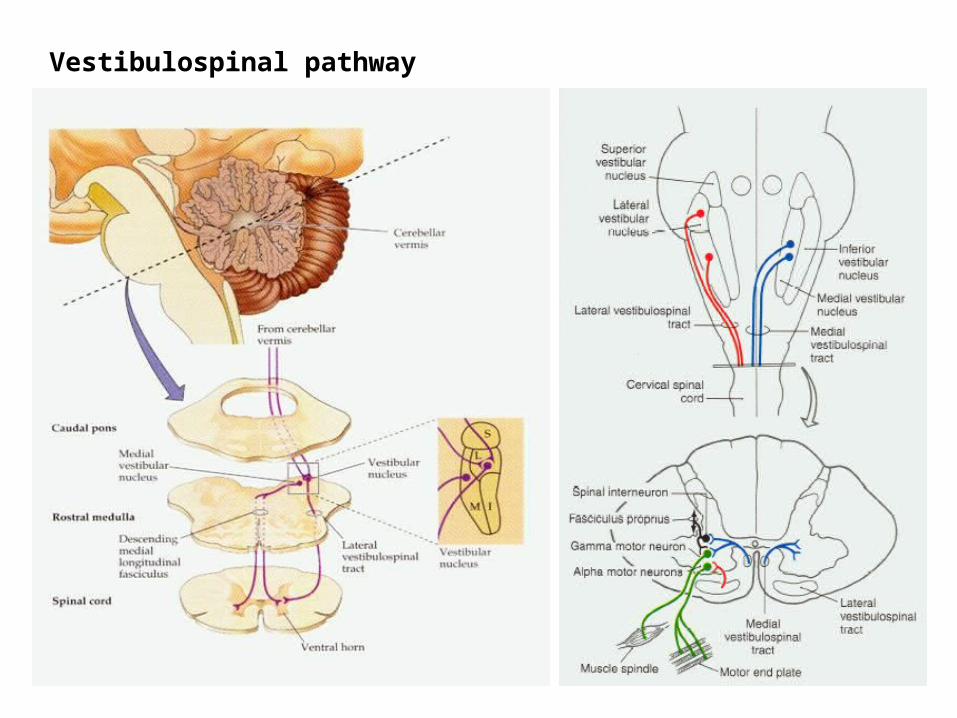
Vestibulospinal pathway


Bedside examination
• Evaluation of vestibular function
-Ocular -Postural
24

Vestibulo-ocular evaluation• Nystagmus -Spontaneous -Evoked • Skew deviation and ocular tilt• Oscillopsia -Dynamic visual acuity -Head-shaking nystagmus -Head-thrust nystagmus• Position test -Positional nystagmus -Positioning nystagmus
25

Vestibulo-spinal evaluation
• Static Romberg test Fukuda test Pastpointing test• Dynamic Turning test External perturbation
26

Vestibulo-ocular evaluation• Nystagmus -Spontaneous -Evoked • Skew deviation and ocular tilt• Oscillopsia -Dynamic visual acuity -Head-shaking nystagmus -Head-thrust nystagmus• Position test -Positional nystagmus -Positioning nystagmus
27
Nystagmus evaluation“No true vertigo without nystagmus”
• Visual acuity suffers appreciably if images that are focused upon retina slip more than 2-3 degree/s
• VOR , stabilized retinal images during head movement
28

Nystagmus evaluation
• VOR , triggered by head acceleration and generated within the semicircular canals.
Nystagmus can be the result of any disorder causing a malfunction of the VOR.
29

Nystagmus evaluation
• Nystagmus can be suppressed in voluntarily by visual fixation (Frenzel lenses : prevent visual fixation)
• Drugs : Caffeine(12h) , Alcohol(24h) , Anticonvulsant, Antidepressant, Antihistamines, BZDs, Narcotics(48h)
30
Nystagmus evaluation
• Accuracy of direct inspection: 0.1 degree/s• Accuracy of ENG : 0.5 degree/s
• Trained investigator : down to 7 degree/s• ENG : 2-3 degree/s
31

Nystagmus evaluation5-10 degree/s or less be dismissed as within
normal limit
Others : if observable or recordable in patient with dizziness considered pathologic
32

Nystagmus
Jerk nystagmus• Slow drift and fast jerk• Due to abnormality in vestibular system• Peripheral or centralPendular nystagmus• Two opposite slow phase without jerk• Due to abnormality in the visual fixation system (M.S ,
brain stem infraction)• Treatment : gabapentin
33

Vestibular Nystagmus
Spontaneous
Evoked
34

Vestibular Spontaneous Nystagmus
Peripheral nystagmus
Central nystagmus
35

Peripheral vestibular spontaneous nystagmus
• Horizontal-torsional or vertical-torsional • Fixed direction , regardless of direction of gaze• Fatigability • Suppressed by visual fixation
36
Vestibular Spontaneous Nystagmus
Peripheral nystagmus
Central nystagmus
37

Central vestibular spontaneous nystagmus
• Prominent vertical component • Visual fixation has no effect on the nystagmus• Nystagmus often changes when gaze is
directed away from the fast phase• Significantly less vertigo
38

Central vestibular spontaneous nystagmus
Down beat SN:• Disorders of cerebellum • Intensified by lateral gaze , convergence or
visual fixation• Oscillopsia and postural instability (cerebellar
degeneration & Chiari type I)
39
Central vestibular spontaneous nystagmus
Up beat SN:• Less common• Intensified by upward gaze, convergence may
alter or reverses it• Vertical oscillopsia and postural instability• Not well defined pathology but , most commonly
associated with medullary lesion• Other : M.S, brain stem or cerebellar infraction,
neoplasms
40

Central vestibular spontaneous nystagmus
Periodic alternating nystagmus (PAN) :• Every 1-2 min changes direction• Visual fixation will have no effect• Chiari type I , lesions of brainstem and
cerebellum• Treatment : baclofen , gamma-aminobutyrate
41
Central vestibular spontaneous nystagmus
See saw nystagmus : • Elevation and intorsion of one eye while the
other depresses and extorts• Pituitary tumor, brain stroke, congenitally
with albinism
Purely torisonal :• syringobulbia , sringomyelia
42

Vestibular Nystagmus
Spontaneous
Evoked
43

Evoked NystagmusGaze-evoked nystagmus (GEN) :• Disorders of CNS involving cerebellum
(cerebellar flocculus ) or brainstem (MVN, nucleus prepositus in medulla, neural integrator)
• Many medications interfere with the neural integrator (anticonvulsants , hypnotics, sedatives , anxiolytics , alcohol)
-EPN : 1-3 cycle/s , Low intensity
44
Evoked Nystagmus• GEN , seen in three types of patients : -Brainstem or vestibulocerebellar disorders -Peripheral vestibular dysfunction (CPA tumors) -Neuromuscular junction disease (M.G.)
• Brun’s nystagmus : GEN and SN combination in CPA tumors high amplitude , Low frequency looking toward the lesion low amplitude , high frequency looking away from the lesion
Large amplitude asymmetric GEN……Brun’s nystagmus Low amplitude symmetric GEN……… EPN
45

Evoked Nystagmus
Valsalva-induced nystagmus :
-SSSC dehiscence (closed glottis … ICP)
-Perilymphatic fistula (open glottis... MEP)
(OW,RW,LSCC)
-Arnold-Chiari (CCJ malformation)
46
Evoked Nystagmus
Sound/pressure evoked :• (Tullio’s phenomenon : sound evoked)• (Hennebert’s sign : pressure evoked)
-Otic syphilis -Perilymphatic fistula -SSCC dehiscency
47

Evoked Nystagmus
Hyperventilation evoked:
-Anxiety -Phobic -Demyelinating lesions on vestibular nerve -Compression by small vessle -Central lesion (M.S)
Rarely noted in patients with pathologies of vestibular end organs alone
48

Vestibulo-ocular evaluation• Nystagmus -Spontaneous -Evoked • Skew deviation and ocular tilt• Oscillopsia -Dynamic visual acuity -Head-shaking nystagmus -Head-thrust nystagmus• Position test -Positional nystagmus -Positioning nystagmus
49

Skew deviation and ocular tilt
• Skew deviation :
• Vertical misalignment that can not be explained on the basis of an ocular muscle palsy
50

Skew deviation and ocular tilt
• Cover test , Maddox Rod test
• Hall mark of disturbance anywhere along otolith-ocular pathway: labyrinth , vestibular nerve , vestibular nucleus , medulla , MLF , midbrain , nucleus of Cajal

Skew deviation and ocular tilt• Skew deviation :
• The compensatory head tilt is in a direction opposite to the apparent head tilt
• The lower eye is on the side of lesion with peripheral or vestibular nucleus lesions and lesions above that are on the side of higher eye.
53

Vestibulo-ocular evaluation• Nystagmus -Spontaneous -Evoked • Skew deviation and ocular tilt• Oscillopsia -Dynamic visual acuity -Head-shaking nystagmus -Head-thrust nystagmus• Position test -Positional nystagmus -Positioning nystagmus
54

Oscillopsia
Dynamic visual acuity
Head-shaking nystagmus
Head-thrust nystagmus
55

Oscillopsia
• Deficient VOR displacement or slip of the retinal image perceived as an apparent motion of target oscillopsia
56
OscillopsiaMild unilateral reduction of VOR oscillopsia
only after very rapid movement
Unilateral reduction of VOR oscillopsia primarily with movements toward the affected ear
Bilateral reduction of VOR oscillopsia during any head movement
57

Oscillopsia
Dynamic visual acuity
Head-shaking nystagmus
Head-thrust nystagmus
58

Dynamic visual acuity
• Patient’s head to and fro in horizontal plane through an 60 degree arc with frequency between 1-2cycle/s.
(below 1cycle/s pursuit system)
• Unilateral loss : lose 2 to 4 lines• Bilateral loss : lose 5 to 6 lines
• Excellent test for ototoxicity
59

Oscillopsia
Dynamic visual acuity
Head-shaking nystagmus
Head-thrust nystagmus
60

Head-shaking• Abrupt stop after shaking the head rapidly for 10-20s Slow phases initially directed toward the affected side A reverse phase with slow phase toward unaffected side
• Head shake test does not elicit oscillopsia but instead exploits changes in central vestibular processing produced by asymmetric inputs from vestibullar labyrinths
Not sensitive or specific enough to be used as a routine
screening test for peripheral vestibular lesions
61
Head-shaking• Head shaking vestibular labyrinths activity charge up central vestibular system (velocity
storage) discharge over 5-20s (constant of VOR)
Symmetric inputs cancellation no nystagmusAsymmetric input no cancellation nystagmus
62

Head-shaking
• Bilateral vestibular hypofunction and acute[?] unilateral vestibular hypofunction, head shake is negative
• Central vestibular lesions : perverted nystagmus (plane other than stimulation)
63

Oscillopsia
Dynamic visual acuity
Head-shaking nystagmus
Head-thrust nystagmus
64
Head thrust
Based on doll’s eye reflex Loss of doll’s eye implies bilateral and extensive
involvement of the brainstem
• Refixation saccades will occur during head movement toward the affected side
Highly sensitive in detecting asymmetry of VOR +Head thrust 68% weakness in caloric test - Head thrust 90% normal caloric test
65

Vestibulo-ocular evaluation• Nystagmus -Spontaneous -Evoked • Skew deviation and ocular tilt• Oscillopsia -Dynamic visual acuity -Head-shaking nystagmus -Head-thrust nystagmus• Position test -Positional nystagmus -Positioning nystagmus
66

Position testPositional nystagmus (sustained) Presents in static head posture and induced by
new head position
Positioning nystagmus (transient) Presents in head motion and caused by head
movement
67

Positional nystagmus
• Eyes in center gaze (with or without fixation) for 30s
• Up right/supine/right ear-down/left ear-down
• Position as slowly as possible
68

Positional nystagmus
Type 1 nystagmus : persistent, lasting longer than 1 min, change
direction in the same or different head position
• Central pathology/barbiturates/salicylates/ alcohol/ horizontal BPPV
69

Positional nystagmus
Type 2 nystagmus: Longer than 1 min, direction is the same
whenever present (consistently rotatory, horizontal or vertical in one or more head positions)
• Either central or unilateral peripheral lesion pathology.
70

Positional nystagmus
Type 3 nystagmus: Transient, lasting less than 1 min ( =positioning nyst.)
• BPPV
71

Positional nystagmus(SUSTAINED)
• Positional nystagmus almost always indicates a vestibular disorder, but it is often non-localizing due to overlap among finding in peripheral and central disorders
72

Positioning nystagmus(TRANSIENT)
• Dix-Hallpike maneuver
• Peripheral : BPPV, Meniere’s disease, vestibular neuritis,perilymphatic fistula, SSCC dehiscence syndrome
• Central : M.S, vascular insufficiency, mass lesion,Chiari malformation, alcohol intoxication
73

Dix-Hallpike Maneuver

Positioning nystagmus
Central Peripheral
Latency None 2-15s
Duration 30 to >120s 5-30s
Fatigability +/- +
Vertigo - +
Fixation Suppression - +
Direction Vertical, Horizontal Rotatory, Horizontal
Direction Change + -
75
Vestibulo-spinal evaluation
• Static Romberg test Fukuda test Pastpointing test• Dynamic Turning test External perturbation
76

Romberg test
• Examine proprioception and vestibulospinal
• Acute peripheral vestibular lesion will usually veer toward the side of problem
• Chronic vestibular injury may not produce abnormality
Sharpened Romberg (tandem Romberg) is more sensitive for vestibular impairment
77

Fukuda test
• With and without vision, marches in place March forward up to 50cm or turn within
30degree is normal
• Unilateral vestibular weakness leads to slowly marches toward the side of weakness
• Non specific but quite remarkable(+) 71% in A.Neuroma
78

Pastpointing test
Should not be used in place of the term “dysmetria”
• Although it may be a result of cerebellar abnormality, often considered a vestibulospinal test and shows vestibular abnormality (peripheral or central) without cerebellar dysfunction
79

Turning test
• Patient walk with closed eye and then turn quickly 180degree to right or left, stopping at the point of attention
• Sway or staggering represent a positive test Patient’s tend to fall toward the side of vestibular
weakness
• Perilymphatic fistula
80

Related Documents











