Review Distress in unaffected individuals who decline, delay or remain ineligible for genetic testing for hereditary diseases: a systematic review Louise Heiniger 1,2 *, Phyllis N. Butow 1,2 , Melanie A. Price 1,2 and Margaret Charles 2 1 Centre for Medical Psychology and Evidence-based Decision-making, School of Psychology, University of Sydney, New South Wales, Australia 2 School of Psychology, University of Sydney, New South Wales, Australia *Correspondence to: Centre for Medical Psychology and Evidence-based Decision- making, Transient Building (F12), University of Sydney, New South Wales, Australia. E-mail: Louise. [email protected] Received: 26 June 2012 Revised: 4 November 2012 Accepted: 6 November 2012 Abstract Objective: Reviews on the psychosocial aspects of genetic testing for hereditary diseases typically focus on outcomes for carriers and non-carriers of genetic mutations. However, the majority of unaffected individuals from high-risk families do not undergo predictive testing. The aim of this review was to examine studies on psychosocial distress in unaffected individuals who delay, decline or remain ineligible for predictive genetic testing. Method: Systematic searches of Medline, CINAHL, PsychINFO, PubMed and handsearching of related articles published between 1990 and 2012 identified 23 articles reporting 17 different studies that were reviewed and subjected to quality assessment. Results: Findings suggest that definitions of delaying and declining are not always straightforward, and few studies have investigated psychological distress among individuals who remain ineligible for testing. Findings related to distress in delayers and decliners have been mixed, but there is evidence to suggest that cancer-related distress is lower in those who decline genetic counselling and testing, compared with testers, and that those who remain ineligible for testing experience more anxiety than tested individuals. Psychological, personality and family history vulnerability factors were identified for decliners and individuals who are ineligible for testing. Conclusions: The small number of studies and methodological limitations preclude definitive conclusions. Nevertheless, subgroups of those who remain untested appear to be at increased risk for psychological morbidity. As the majority of unaffected individuals do not undergo genetic testing, further research is needed to better understand the psychological impact of being denied the option of testing, declining and delaying testing. Copyright © 2012 John Wiley & Sons, Ltd. Introduction Despite early concerns over the potential for adverse psychological responses to genetic testing for disease risk [1], no systematic negative long-term psychological out- comes have been demonstrated [2,3]. This may be attribut- able to the success of genetic counselling in facilitating adaptation to receiving genetic results as well as the benefits of reducing uncertainty regarding risk and providing infor- mation to guide screening, prevention or treatment decisions [4,5]. However, little is known about the impact of not receiving genetic test results in the presence of a family history of disease. Most unaffected individuals from families with a strong history of disease are ineligible for personal testing [6] as they are usually only tested after a mutation has been identified in an affected relative [7,8]. For this reason, the majority of unaffected relatives are assumed to be at increased risk but do not benefit from genetic counselling or the reduced uncertainty of knowing their actual risk. In addition, over a third of individuals who are eligible for testing choose not to be tested (decliners) or are undecided about testing or plan to be tested at a later date (delayers) [9–11]. The few studies of those who are ineligible for testing suggest that anxiety may be higher in this group compared with identified mutation carriers and population controls [12,13], and studies comparing those who decline to those who opt for testing have produced mixed results [14–17]; few, if any, studies focus on those individuals who delay genetic testing. In light of the growing list of diseases for which a family history has been identified as a risk indicator, a systematic review of the psychological factors associated with delay- ing, declining or remaining ineligible for testing is timely. The aim of this systematic review was to answer the follow- ing questions: (i) What are the distress profiles of decliners and delayers? (ii) What are the psychological outcomes for individuals who decline, delay or remain ineligible for testing? (iii) What are the vulnerability factors for indivi- duals who decline, delay or remain ineligible for testing? Method Search strategy Searches were conducted in PsychINFO, Medline, CINAHL and PubMed between 27 April 2012 and 8 May 2012, and the results were limited to articles relating to adult humans that were published in English in a peer-reviewed journal since 1 January 1990. Search terms were developed, and adapted for each database, from the concepts of genetic Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology Psycho-Oncology (2012) Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/pon.3235

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Review
Distress in unaffected individuals who decline, delay orremain ineligible for genetic testing for hereditary diseases:a systematic review
Louise Heiniger1,2*, Phyllis N. Butow1,2, Melanie A. Price1,2 and Margaret Charles21Centre for Medical Psychology and Evidence-based Decision-making, School of Psychology, University of Sydney, New South Wales, Australia2School of Psychology, University of Sydney, New South Wales, Australia
*Correspondence to:Centre for Medical Psychologyand Evidence-based Decision-making, Transient Building (F12),University of Sydney, New SouthWales, Australia. E-mail: [email protected]
Received: 26 June 2012Revised: 4 November 2012Accepted: 6 November 2012
AbstractObjective: Reviews on the psychosocial aspects of genetic testing for hereditary diseases typically focuson outcomes for carriers and non-carriers of genetic mutations. However, the majority of unaffectedindividuals from high-risk families do not undergo predictive testing. The aim of this review was toexamine studies on psychosocial distress in unaffected individuals who delay, decline or remain ineligiblefor predictive genetic testing.
Method: Systematic searches of Medline, CINAHL, PsychINFO, PubMed and handsearching ofrelated articles published between 1990 and 2012 identified 23 articles reporting 17 different studiesthat were reviewed and subjected to quality assessment.
Results: Findings suggest that definitions of delaying and declining are not always straightforward,and few studies have investigated psychological distress among individuals who remain ineligible fortesting. Findings related to distress in delayers and decliners have been mixed, but there is evidence tosuggest that cancer-related distress is lower in those who decline genetic counselling and testing,compared with testers, and that those who remain ineligible for testing experience more anxiety thantested individuals. Psychological, personality and family history vulnerability factors were identifiedfor decliners and individuals who are ineligible for testing.
Conclusions: The small number of studies and methodological limitations preclude definitiveconclusions. Nevertheless, subgroups of those who remain untested appear to be at increased riskfor psychological morbidity. As the majority of unaffected individuals do not undergo genetic testing,further research is needed to better understand the psychological impact of being denied the option oftesting, declining and delaying testing.Copyright © 2012 John Wiley & Sons, Ltd.
Introduction
Despite early concerns over the potential for adversepsychological responses to genetic testing for disease risk[1], no systematic negative long-term psychological out-comes have been demonstrated [2,3]. This may be attribut-able to the success of genetic counselling in facilitatingadaptation to receiving genetic results as well as the benefitsof reducing uncertainty regarding risk and providing infor-mation to guide screening, prevention or treatment decisions[4,5]. However, little is known about the impact of notreceiving genetic test results in the presence of a familyhistory of disease.Most unaffected individuals from families with a strong
history of disease are ineligible for personal testing [6] asthey are usually only tested after a mutation has beenidentified in an affected relative [7,8]. For this reason,the majority of unaffected relatives are assumed to be atincreased risk but do not benefit from genetic counsellingor the reduced uncertainty of knowing their actual risk. Inaddition, over a third of individuals who are eligible fortesting choose not to be tested (decliners) or are undecidedabout testing or plan to be tested at a later date (delayers)[9–11].The few studies of those who are ineligible for testing
suggest that anxiety may be higher in this group compared
with identified mutation carriers and population controls[12,13], and studies comparing those who decline to thosewho opt for testing have produced mixed results [14–17];few, if any, studies focus on those individuals who delaygenetic testing.In light of the growing list of diseases for which a family
history has been identified as a risk indicator, a systematicreview of the psychological factors associated with delay-ing, declining or remaining ineligible for testing is timely.The aim of this systematic review was to answer the follow-ing questions: (i) What are the distress profiles of declinersand delayers? (ii) What are the psychological outcomesfor individuals who decline, delay or remain ineligible fortesting? (iii) What are the vulnerability factors for indivi-duals who decline, delay or remain ineligible for testing?
Method
Search strategy
Searches were conducted in PsychINFO,Medline, CINAHLand PubMed between 27 April 2012 and 8 May 2012, andthe results were limited to articles relating to adult humansthat were published in English in a peer-reviewed journalsince 1 January 1990. Search terms were developed, andadapted for each database, from the concepts of genetic
Copyright © 2012 John Wiley & Sons, Ltd.
Psycho-OncologyPsycho-Oncology (2012)Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/pon.3235

testing, hereditary cancer, psychosocial factors and uncer-tainty, as well as additional terms such as absence of demon-strated mutation.Reference lists of eligible articles were examined to iden-
tify additional relevant studies. Reference lists of reviewsidentified through searches were screened, and articlesciting included papers were identified through Web ofKnowledge and assessed for eligibility.
Selection of eligible articles
Articles were eligible for inclusion in this review if theyreported original research and included (i) participants atincreased risk for disease based on family history, knowngenetic mutation or ethnic descent; (ii) results for partici-pants who were ineligible for testing (and had, therefore,not undergone the testing procedure), eligible but declinedto learn results and/or eligible but delayed testing; (iii) atleast 10 participants in the group of interest [18]; and(iv) at least one measure of distress or explored copingwith risk qualitatively. Articles were excluded if the study(i) assessed affected individuals only; (ii) did not reportresults separately for affected and unaffected individuals(studies not reporting results separately but which con-trolled for personal cancer history or found no effect ofaffected status were included); (iii) did not provide a cleardescription of the genetic testing statuses of the groups;(iv) were review articles; or (v) assessed only intentionsto test. This last exclusion criterion was based on evidencethat intention to undergo genetic testing is not necessarilyindicative of behaviour [19,20].
Information extraction and quality assessment
A data extraction sheet was used to record variables such asstudy participants, research question, study design, diseasetype, measures used, results and limitations relevant to thepresent review. The QualSyst tool was used to documentstudy quality, as it provides criteria for assessing a rangeof research designs [21]. All articles were independentlyassessed by LH and PB and discrepancies discussed untilan agreement was reached.The studies relevant to the three review questions have
been summarised under subheadings in Tables 1–5 andordered according to quality of evidence, year of publicationand alphabetically. Quality of evidence was ranked to reflectpreviously defined cut-offs [22] representing high (>80),moderate (70–80), adequate (50–70) and low (<50) quality.Importantly, differences in disease characteristics and
associated risk management and treatment options (seeAppendix A for a summary) have the potential to influ-ence testing decisions and psychological outcomes, andshould be considered in reviewing the results. How thesedifferences are likely to impact decisions and outcomesis beyond the scope of this paper and has been outlinedelsewhere [23].
Results
The search yielded 1898 articles potentially eligible forreview. Screening of titles, abstracts and exclusion ofduplicate publications resulted in 91 articles being retrieved
for full text screening. Application of inclusion/exclusioncriteria and resolution of discrepancies reduced the numberof articles for review to 17. Six additional articles were iden-tified through reviews, citing articles and reference lists,resulting in 23 articles representing 17 different studiesavailable for the review. Articles related to the same datasetor sample but reporting different data have been noted butreported separately. Articles presenting data relevant tomore than one question of interest have been listed in allappropriate tables.
Definitional challenges
The distinction between declining and delaying testingwas commonly acknowledged, but the classification ofdelayers and the concept of declining varied, reflecting thecomplexity of genetic test decision-making. Individualswho initially declined and either went on to undergo testingor indicated future testing as a possibility were variablygrouped with testers and decliners but never investigatedindependently. Decliners were sometimes separated intosubgroups according to the stage at which they declined(e.g. precounselling or postcounselling) or whether theirtesting decision was consistent with their precounselling testintention, and in one study, it was not completely clear whetherdeclining was test decline or study participation decline. Theauthors of the current review chose to retain group classifica-tions made by the study authors, but these complexities shouldbe considered in the interpretation of the findings.
Research question 1: distress profiles of declinersand delayers
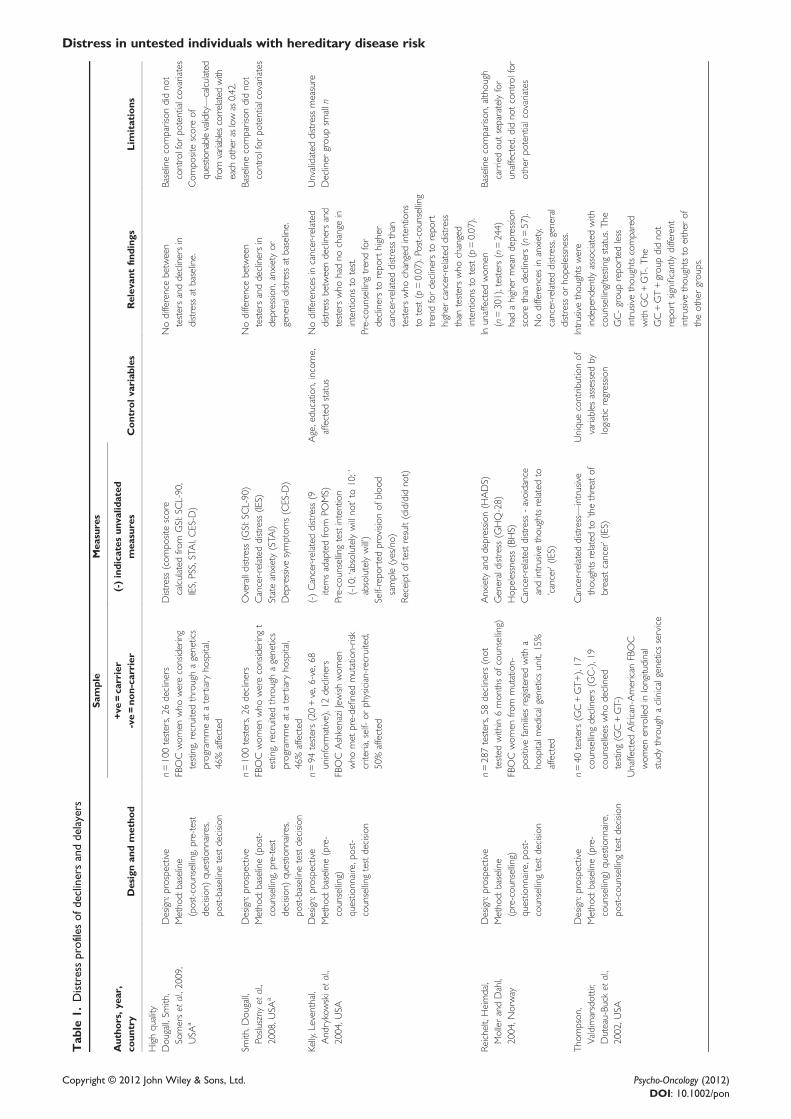
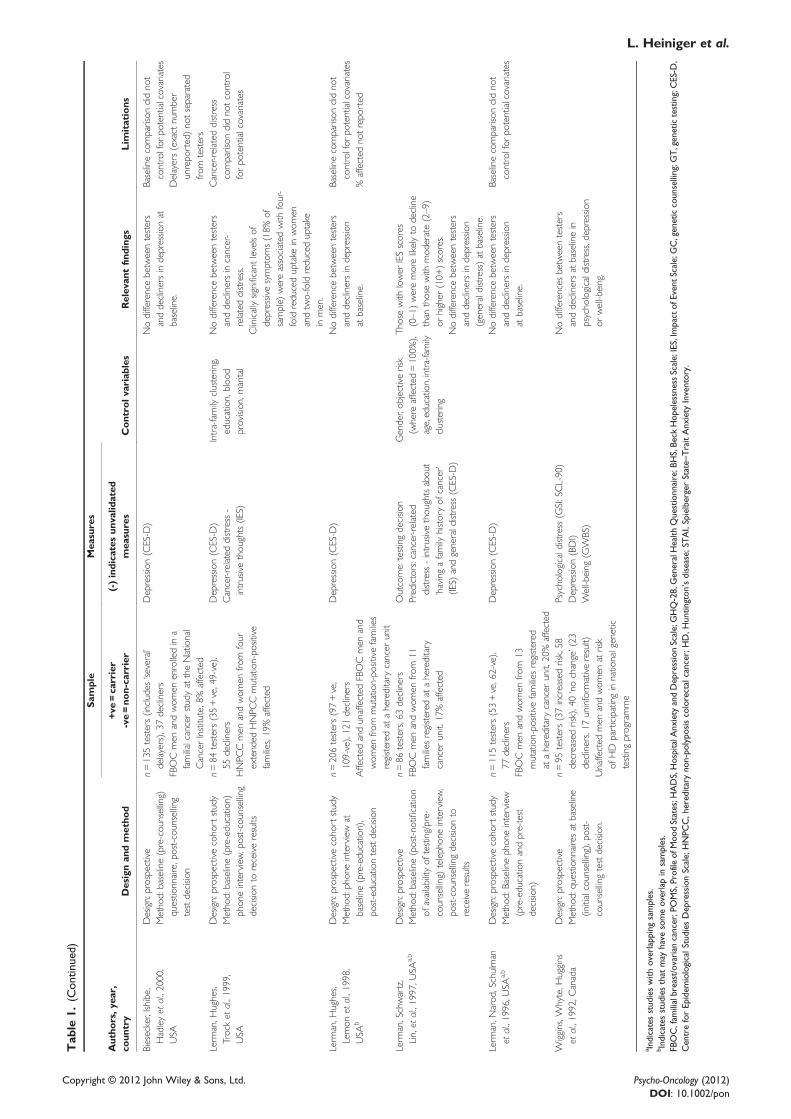
Eleven high-quality articles presenting prospective data onthis topic were identified (Table 1). These articles assessedpsychological distress prior to a decision about genetictesting being made, that is, explored psychological predic-tors of decisions about testing. The majority of studiesrelated to individuals at risk for familial breast and ovariancancer (FBOC) with one each on hereditary non-polyposiscolorectal cancer [HNPCC; [16]] and Huntington’s disease[HD; [24]]. Types of distress reported included depression,anxiety, cancer-related distress (most often represented bythe intrusion subscale of the Impact of Event Scale [IES;[25]]), general distress, subjective well-being and hopeless-ness. The stressor referred to in the IES varied; participantsresponded in relation to cancer [17], threat of breast cancer[26] or having a family history of cancer [27]. In twostudies, the focus of the cancer-related distress measurewas not reported [16,28].
Depression and anxiety
Of eight studies comparing depression of decliners to tes-ters, six reported no difference, one reported higher depres-sion and one lower depression. Overall, contradictoryfindings may be attributable to differences in disease groupsand/or measures used.On the basis of the larger and more recent studies, decli-
ners of FBOC testing report lower depression, whereasdecliners of HNPCC testing report higher depression com-pared with testers. Lerman et al. [16] found that depressionwas associated with declining in those at risk for HNPCC,
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le1.
Distressprofilesof
declinersanddelayers
Autho
rs,y
ear,
coun
try
Designan
dmetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Highquality
Dou
gall,Sm
ith,
Somerset
al.,2009,
USA
a
Design:prospective
n=100testers,26
decliners
Distress(com
positescore
calculated
from
GSI:SCL-90,
IES,PSS,STAI,CES-D
)
Nodifferencebetween
testersanddeclinersin
distressat
baseline.
Baselinecomparison
didno
tcontrolfor
potentialcovariates
Metho
d:baseline
(post-counsellin
g,pre-test
decisio
n)questio
nnaires,
post-baselinetestdecisio
n
FBOCwom
enwho
wereconsidering
testing,recruitedthroughagenetics
programmeat
atertiary
hospital,
46%affected
Com
positescoreof
questionablevalidity—calcu
lated
from
variables
correlated
with
each
otheraslowas0.42.
Smith,D
ougall,
Poslu
szny
etal.,
2008,U
SAa
Design:prospective
n=100testers,26
decliners
Overalldistress(G
SI:SCL-90)
Nodifferencebetween
testersanddeclinersin
depressio
n,anxietyor
generaldistressat
baseline.
Baselinecomparison
didno
tcontrolfor
potentialcovariates
Metho
d:baseline(post-
counsellin
g,pre-test
decisio
n)questio
nnaires,
post-baselinetestdecisio
n
FBOCwom
enwho
wereconsideringt
esting,recruitedthroughagenetics
programmeat
atertiary
hospital,
46%affected
Cancer-related
distress(IE
S)Stateanxiety(STA
I)Depressivesymptom
s(CES-D
)
Kelly,Leventhal,
Andrykowskieta
l.,2004,U
SA
Design:prospective
n=94
testers(20+ve,6-ve,68
uninform
ative),12decliners
(-)Cancer-related
distress(9
itemsadaptedfro
mPO
MS)
Age,educatio
n,income,
affected
status
Nodifferences
incancer-related
distressbetweendeclinersand
testerswho
hadno
change
inintentions
totest.
Unvalidated
distressmeasure
Metho
d:baseline(pre-
counsellin
g)questio
nnaire,post-
counsellin
gtestdecisio
n
FBOC
AshkenaziJewish
wom
enwho
met
pre-definedmutation-risk
criteria,self-or
physician-recruited,
50%affected
Pre-counsellin
gtestintention
(-10;‘absolutelywillno
t’to
10;’
absolutelywill’)
Pre-counsellin
gtrendfor
declinersto
repo
rthigher
cancer-related
distressthan
testerswho
changedintentions
totest(p=0.07).Po
st-cou
nselling
trendfordeclinersto
repo
rthigher
cancer-related
distress
than
testerswho
changed
intentions
totest(p=0.07).
Decliner
grou
psm
alln
Self-repo
rted
provision
ofbloo
dsample(yes/no)
Receiptof
testresult(did/didno
t)
Reichelt,Heimdal,
MollerandDahl,
2004,N
orway
Design:prospective
n=287testers,58
decliners(not
tested
within6mon
thsof
counsellin
g)Anxiety
anddepressio
n(H
ADS)
Inunaffected
wom
en(n=301),testers
(n=244)
hadahigher
meandepressio
nscorethan
decliners(n=57).
Nodifferences
inanxiety,
cancer-related
distress,general
distressor
hopelessness.
Baselinecomparison
,althou
ghcarriedou
tseparatelyfor
unaffected,didno
tcontrolfor
otherpo
tentialcovariates
Metho
d:baseline
(pre-cou
nselling)
questio
nnaire,post-
counsellin
gtestdecisio
n
FBOCwom
enfro
mmutation-
positivefamilie
sregistered
with
aho
spitalm
edicalgeneticsunit,15%
affected
Generaldistress(G
HQ-28)
Hop
elessness(BHS)
Cancer-related
distress-avoidance
andintrusivethou
ghtsrelatedto
’cancer’(IE
S)
Thom
pson
,Valdimarsdottir,
Duteau-Bu
cket
al.,
2002,U
SA
Design:prospective
n=40
testers(G
C+GT+
),17
counsellin
gdecliners(G
C-),19
counsellees
who
declined
testing(G
C+GT-)
Cancer-related
distress—
intrusive
thou
ghtsrelatedto
’thethreat
ofbreastcancer’(IES)
Uniquecontrib
utionof
variables
assessed
bylogisticregressio
n
Intrusivethou
ghtswere
independently
associated
with
counsellin
g/testingstatus.T
heGC-grou
prepo
rted
less
intrusivethou
ghtscompared
with
GC+GT-.T
heGC+GT+grou
pdidno
trepo
rtsignificantlydifferent
intrusivethou
ghtsto
either
oftheothergrou
ps.
Metho
d:baseline(pre-
counsellin
g)questio
nnaire,
post-cou
nsellingtestdecisio
nUnaffected
African-American
FBOC
wom
enenrolledinlongitudinal
studythroughaclinicalgeneticsservice
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le1.
(Con
tinued)
Autho
rs,y
ear,
coun
try
Designan
dmetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Biesecker,Ish
ibe,
Hadleyet
al.,2000,
USA
Design:prospective
n=135testers(includes
‘several’
delayers),37
decliners
Depression(CES-D
)Nodifferencebetweentesters
anddeclinersindepressio
nat
baseline.
Baselinecomparison
didno
tcontrolfor
potentialcovariates
Metho
d:baseline(pre-cou
nselling)
questio
nnaire,post-counsellin
gtestdecisio
nFBOCmen
andwom
enenrolledina
familialcancerstudyat
theNational
CancerInstitute,8%affected
Delayers(exact
number
unrepo
rted)no
tseparated
from
testers
Lerm
an,H
ughes,
Trocket
al.,1999,
USA
Design:prospectivecoho
rtstudy
n=84
testers(35+ve,49-ve),
55decliners
Depression(CES-D
)Intra-family
clusterin
g,education,bloo
dprovision
,marital
Nodifferencebetweentesters
anddeclinersincancer-
relateddistress.
Cancer-related
distress
comparison
didno
tcontrol
forpo
tentialcovariates
Metho
d:baseline(pre-educatio
n)phon
einterview,post-counsellin
gdecisio
nto
receiveresults
HNPC
Cmen
andwom
enfro
mfour
extended
HNPC
Cmutation-po
sitive
familie
s,19%
affected
Cancer-related
distress-
intrusivethou
ghts(IE
S)Clinicallysignificant
levelsof
depressivesymptom
s(18%
ofsample)
wereassociated
with
four-
foldreduceduptake
inwom
enandtwo-foldreduceduptake
inmen.
Lerm
an,H
ughes,
Lemon
etal.,1998,
USA
b
Design:prospectivecoho
rtstudy
n=206testers(97+ve,
109-ve),121decliners
Depression(CES-D
)Nodifferencebetweentesters
anddeclinersindepressio
nat
baseline.
Baselinecomparison
didno
tcontrolfor
potentialcovariates
Metho
d:phon
einterview
atbaseline(pre-educatio
n),
post-educatio
ntestdecisio
nAffected
andunaffected
FBOCmen
and
wom
enfro
mmutation-po
sitivefamilie
sregistered
atahereditary
cancer
unit
%affected
notrepo
rted
Lerm
an,Schwartz,
Lin,et
al.,1997,U
SAa,b
Design:prospective
n=86
testers,63
decliners
Outcome:testingdecisio
nGender,ob
jectiverisk
(where
affected
=100%
),age,education,intra-family
clustering
Thosewith
lower
IESscores
(0–1)
weremorelikelyto
decline
than
thosewith
mod
erate(2–9)
orhigher
(10+
)scores.
Metho
d:baseline(post-no
tificatio
nof
availabilityof
testing/pre-
counsellin
g)telephon
einterview,
post-cou
nsellingdecisio
nto
receiveresults
FBOCmen
andwom
enfro
m11
familie
sregistered
atahereditary
cancer
unit,17%
affected
Predictors:cancer-related
distress-intrusivethou
ghtsabou
t’havingafamily
historyof
cancer’
(IES)
andgeneraldistress(CES-D
)Nodifferencebetweentesters
anddeclinersindepressio
n(generaldistress)at
baseline.
Lerm
an,N
arod
,Schulman
etal.,1996,U
SAa,b
Design:prospectivecoho
rtstudy
n=115testers(53+ve,62-ve),
77decliners
Depression(CES-D
)Nodifferencebetweentesters
anddeclinersindepressio
nat
baseline.
Baselinecomparison
didno
tcontrolfor
potentialcovariates
Metho
d:Baselinephon
einterview
(pre-educatio
nandpre-test
decisio
n)FBOCmen
andwom
enfro
m13
mutation-po
sitivefamilie
sregistered
atahereditary
cancer
unit,20%
affected
Wiggins,W
hyte,H
uggins
etal.,1992,C
anada
Design:prospective
n=95
testers(37increasedrisk,58
decreasedrisk),40‘nochange’(23
decliners,17
uninform
ativeresult)
Psycho
logicaldistress(G
SI:SCL-90)
Nodifferences
betweentesters
anddeclinersat
baselinein
psycho
logicaldistress,depression
orwell-being.
Metho
d:questio
nnairesat
baseline
(initialcounsellin
g),post-
counsellin
gtestdecisio
n.Unaffected
men
andwom
enat
risk
ofHD
participatinginnatio
nalgenetic
testingprogramme
Depression(BDI)
Well-being
(GW
BS)
a Indicatesstudieswith
overlappingsamples.
b Indicates
studiesthat
may
have
someoverlapin
samples.
FBOC,fam
ilialbreast/ovarian
cancer;POMS,Profileof
Moo
dStates;H
ADS,HospitalA
nxiety
andDepressionScale;GHQ-28,GeneralHealth
Questionnaire;B
HS,Be
ckHop
elessnessScale;IES,Im
pactof
EventS
cale;G
C,geneticcounselling;G
T,genetictesting;CES-D
,CentreforEpidem
iologicalStudies
DepressionScale;HNPC
C,h
ereditary
non-po
lypo
siscolorectalcancer;H
D,H
untin
gton
’sdisease;ST
AI,SpielbergerState–
TraitAnxiety
Inventory.
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le2.
Outcomes
fordecliners(cross-sectio
nal)
Autho
rs,y
ear,
coun
try
Designan
dmetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Highquality
Foster,Evans,
Eeleset
al.,2004,U
K
Design:Cross-sectio
nal
n=275testers,27
decliners(including
five
delayers[testedpo
st-participation])
Cancerworry
(CW
S)Age
Nodemographicdifferences
betweendeclinersanddelayers
andtesters.
Delayerssm
alln.
Metho
d:Baseline(atcounsellin
g,pre-test
decisio
n)questio
nnaire,com
paredto
declinersCW
Sscores
from
separate
questio
nnaire
completed
12-m
onth
post-baseline
Unaffected
FBOCmen
andwom
enfro
mmutation-po
sitivefamilie
swho
attended
genetic
centresforgenetic
counsellin
g
Aftercontrollin
gforage,
declinersrepo
rtlesscancer
worry
than
testers.
Delayersno
tseparated
from
decliners.
Timingof
assessments
may
have
impacted
distresslevels.
Cod
ori,Peteresen,
Migliorettieta
l.,1999,
USA
Design:cross-sectional
n=77
testers,181decliners
Dependent
variable:testing
decisio
nDistance
from
hospital,
intra-family
clusterin
gMorefre
quentcancer
thou
ghtsweresignificantly
associated
with
studyparticipation
and,consequently,
testuptake.
Test
declineconfou
nded
with
studydecline.
Metho
d:self-repo
rtquestio
nnaire
for
testers,phon
einterview
fordecliners
Unaffected
men
andwom
enat
risk
ofHNPC
Cparticipatinginacolorectal
cancer
registry
Independentvariable:fre
quency
ofcancer
thou
ghtsinpast
mon
th(one
item,fou
r-point
Likertscale)
Age
andeducationno
tcontrolled,despite
differences.
Singleitem
tomeasure
cancer-related
distress
Decruyenaere,Evers-
Kieboo
ms,Bo
ogaerts
etal.,1997,Belgium
Design:cross-sectional
n=63
testers,14
decliners(appliedfor
testing),36sib
lings
(never
applied
fortesting)
Anxiety
(STA
I)Untestedgrou
pswerepo
oled.
Nodifferenceinanxietybetween
testersanddecliners.
Bivariate
statistical
analyses
precluded
controllin
gforparity,
which
differedbetween
tested
anduntested.
Metho
d:self-repo
rtquestio
nnaire
Unaffected
men
andwom
enat
riskof
HD
who
appliedfortestingat
agenetics
centre
(and
theirsib
lings)
Mod
eratequality
Lammens,Aaron
son,
Wagneret
al.,2010,
TheNetherlands
Design:cross-sectional
n=52
testers(27+ve,25-ve),18
decliners/delayers(fo
urhadfuture
testingintentions,eight
unsure
abou
ttesting,six
nointentionto
betested)
Cancer-related
distress-
intrusivethou
ghtsrelatedto
‘LFS’(IES)
Age,gender
Nodifferences
inthenumberof
decliners(17%
),carriers
(22%
)and
non-carriers
(29%
)repo
rtingclinically
significant
levelsof
intrusivethou
ghts.
Insufficientn.
Metho
d:self-repo
rtquestio
nnaire
Men
andwom
enfro
m11
LFSmutation-
positivefamilie
s,14%
affected
Cancerworry
(CW
S)Nodifferences
betweengrou
psin
cancer
worry.
Unableto
controlfor
familialclustering.
Lodder,Frets,Trijsburg
etal.,2003,
TheNetherlands
Design:cross-sectional
n=85
testers,13
decliners
Anxiety
anddepressio
n(H
ADS)
Nodifferenceincasesof
borderline–
high
anxietyand/or
depressio
nbetweendeclinersandtesters.
Affected
status
unrepo
rted
but
assumed
tobe
unaffected.
Metho
d:self-repo
rtquestio
nnaire
and/or
telephon
einterview
(declinersaw
areof
possibilityof
testing>1year
earlier
anddid
notapplyfortesting,testersassessed
betweenbloo
dsamplingandresult
notificatio
n)
Decliners:wom
enat
riskof
Testers:
wom
enwho
underw
enttesting
betweenDecem
ber1995
andApril1998
(-)Cancer-related
distress
(9itemsfro
mIES)
Nodifferenceinanxietyor
depressio
nbetweendecliners
andtesters.
Timingof
testers’
assessmentmay
have
affected
distress.
FBOCparticipatinginsurveillance
programmeat
acancer
institute.
4/13
ofthedeclinersrepo
rted
atleast1item
inthecancer-related
distressscaleappliedto
them
‘often’.
Theauthorsstated
that
‘theothers
repo
rted
lower
cancer-related
distresslevels’,how
ever
nosignificancetestwas
repo
rted.
Insufficientn.
Evidence
ofbetween
grou
pdemographic
differences
butsm
all
sampleprecluded
multivariate
analyses.
Significanceof
between
grou
pdifferences
incancer-related
distress
notrepo
rted.
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon

Tab
le2.
(Con
tinued)
Autho
rs,y
ear,
coun
try
Designan
dmetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Adequatequality
deSnoo
,Riedijk,van
Milet
al.,2008,
TheNetherlands
Design:cross-sectional
n=75
testers,19
decliners
Anxiety
anddepressio
n(H
ADS)
Gender,education
‘Fears
inducedby
thetestresult’and‘
worrie
s’abou
tmelanom
aand
pancreaticcancer
(from
DNAtest
expectancies)weresignificantly
associated
with
testdecline.
Unclear
whether
psycho
logical
questionnaire
before
orattim
eof
decline.
Metho
d:self-repo
rtquestio
nnaire
0to
6-weekpo
st-cou
nselling/pre-testing
Men
andwom
enat
riskof
FMfro
m13
mutation-po
sitivefamilie
sassociated
with
atertiary
medicalcentre
skinscreeningclinic
(Note:Th
emelanom
amutationisalso
associated
with
a17%
pancreatic
cancer
risk)
Cancer-related
distress(IE
S)
Both
testersanddeclinershadlow
scores
ontheHADS,butno
significancetestswererepo
rted.D
idno
trepo
rtdifferences
between
testersanddeclinersforImpact
ofpancreaticcancer
inform
ation,
despite
saying
thiswas
assessed.
Usedunvalidated
measures.
(-)DNAtestexpectancies
(12
items,five-point
Likertscale)
Insufficientnandpo
orrespon
serate
(51%
)
(-)Impact
ofpancreaticcancer
inform
ation(th
reeitems,five-point
Likertscale)
‘Given
therelativelysm
all
samplesize,on
lygender
andeducationallevel
wereenteredaspossible
covariates’(p.793).
Significanceof
between
grou
pdifferences
inHADSscores
not
repo
rted.
FBOC,fam
ilialbreast/ovarian
cancer;C
WS,CancerW
orry
Scale;HNPC
C,hereditary
non-po
lypo
siscolorectalcancer;H
D,H
untin
gton
’sdisease;ST
AI,SpielbergerState–
TraitAnxiety
Inventory;LFS,Li–Fraumenisyndrom
e;IES,Im
pact
ofEventS
cale;H
ADS,Hospital
Anxiety
andDepressionScale;FM
,fam
ilialmelanom
a.
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le3.
Outcomes
fordecliners(lo
ngitu
dinal)
Autho
rs,y
ear,
coun
try
Designan
dMetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Highquality
Dou
gall,Sm
ith,Som
ers
etal.,2009,U
SAa
Design:Prospective
n=100testers(positive,negative
[uninformative],variant),26
decliners
Distress(com
positescore
calculated
from
GSI:SCL-90,
IES,PSS,STAI,CES-D
)
Age,incom
e,useof
psychiatric
medication
Nodifferencebetweentesters
anddeclinersindistressat
any
timepo
int.
Com
positedistressscore
ofquestionablevalidity—
calcu
lated
from
variables
correlated
with
each
otheraslowas0.42.
Metho
d:questio
nnairesat
baseline
(post-counsellin
g,pre-testdecisio
n),
1-weekpo
st-resultor
3to
4-mon
thpo
st-baselinefordecliners(T2),3-
mon
thpo
st-T2,6-mon
thpo
st-T2
FBOCwom
enwho
wereconsidering
testing,recruitedthroughagenetics
programmeat
atertiary
hospital,
46%affected
Tested
subgroup
nsunrepo
rted
Smith,D
ougall,Po
sluszny
etal.,2008,U
SAa
Design:prospective
n=100testers(positive,negative
[uninformative],variant),26
decliners
Overalldistress(G
SI:SCL-90)
Age,incom
e,education,use
ofpsychiatric
medication
Nodifferencebetweengrou
psincancer-related
distressat
baseline
or1-weekpo
st-result,but3mon
thpo
st-testthosewith
uninform
ative/
negativeor
variant
results
repo
rted
lessintrusionthan
declinersand
carriers.A
t6mon
ths,decliners
repo
rted
significantlymorecancer-
relateddistressthan
thosewith
variant
results.
Tested
subgroup
nsunrepo
rted
Metho
d:questio
nnairesat
baseline
(post-counsellin
g,pre-testdecisio
n),
1-weekpo
st-resultor
3to
4-mon
thpo
st-baselinefordecliners(T2),3-
mon
thpo
st-T2,6-mon
thpo
st-T2
FBOCwom
enwho
wereconsidering
testing,recruitedthroughagenetics
programmeat
atertiary
hospital,
46%affected
Cancer-related
distress(IE
S)Stateanxiety(STA
I)Depressivesymptom
s(CES-D
)
Lerm
an,H
ughes,Lemon
etal.,1998,U
SAb
Design:Prospectivecoho
rtstudy
n=206testers(97+ve,109-ve),
121decliners
Cancer-related
distress-
intrusivethou
ghts
abou
t‘havingcancer
inthe
family’(IES)
Baselinedepressio
n,gender,
affected
status,m
aritalstatus
Nodifferencebetweengrou
psindepressio
nat
baseline.Significant
differenceinprevalence
ofdepressio
nat
1mon
th—
8%no
n-carriers,14%
carriers
and19%decliners.
Multivariate
analyses
revealed
that
higher
ratesof
depressio
nat
follow-
upwereon
lyseen
fordeclinerswith
elevated
baselinecancer-related
distress(Table5).
%affected
notrepo
rted
Metho
d:phon
einterview
atbaseline(pre-educatio
n),1-m
onth
and6-mon
thfollow-up
FBOCmen
andwom
enfro
mmutation-po
sitivefamilie
sregistered
atahereditary
cancer
unit
Depression(CES-D
)
Lerm
an,N
arod
,Schulman
etal.,1996,U
SAb
Design:prospectivecoho
rtstudy
n=115testers(53+ve,62-ve),
77decliners
Depression(CES-D
)Intra-family
clusterin
g,affected
status,baselinelevelsof
outcom
evariables
Forunaffected
participants,there
weregreaterreductions
indepressio
nforno
n-carriers
comparedwith
carriers
anddeclinersat
1-mon
thfollow-up.
Metho
d:baseline(1
to2-mon
thpre-education)
phon
einterview,
1-mon
thfollow-upphon
einterview
(1-m
onth
post-testingdecisio
n/result
notificatio
n)
FBOCmen
andwom
enfro
m13
mutation-po
sitivefamilie
sregistered
atahereditary
cancer
unit,19%
affected
Wiggins,W
hyte,H
uggins
etal.,1992,C
anadac
Design:prospective
n=95
testers(37increasedrisk,
58decreasedrisk),40‘nochange’
(23decliners,17
uninform
ativeresult)
Psycho
logicald
istress(G
SI:SCL-90)
Difference
scores
used
tominimise
effect
ofbaselinedifferences
onou
tcom
es
At6mon
ths,increase
inwell-being
forthedecreasedriskgrou
psignificantlydifferent
toreductions
inwell-being
in’nochange’group.
At12
mon
ths,improvem
ents
inpsycho
logicaldistressintested
grou
psdifferedsignificantly
from
deterio
ratio
nin‘nochange’
Metho
d:questio
nnairesat
baseline
(atinitialcounsellin
g,pre-decisio
n),
6-mon
thand12-m
onth
follow-up.
Unaffected
men
andwom
enat
risk
ofHD
participatinginnatio
nal
genetic
testingprogramme
Depression(BDI)
Well-being
(GW
BS)
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le3.
(Con
tinued)
Autho
rs,y
ear,
coun
try
Designan
dMetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
grou
p.Re
ductions
inwell-being
relativeto
baselinein‘nochange’
grou
pat
6and12
mon
ths.At
12mon
ths,depressio
nhad
increased,comparedto
baseline,
for‘nochange’group
compared
tobo
thtested
grou
ps.
Adequatequality
Lawson,W
iggins,G
reen
etal.,1996,C
anadac
Design:retrospective
n=95
testers(37increasedrisk,58
decreasedrisk),23decliners,17
uninform
ativeresult
Adverse
eventsin
cebaseline—
whether
clinicaland/or
quantitative
criteria
weremet.C
linical=suicide
attempt/plan
,psychiatric
hospitalisation,
depressio
n>2months,increase
insubstanceuse,breakdow
nofimpo
rtant
relationships.Q
uantitative=clinically
relevant
changesinGSIandBD
I
N/A
Nosignificant
differencebetween
grou
psinnumberof
adverse
events.
Baselinedepressio
nno
tcontrolledfor.
Metho
d:utilisedata
from
Wiggins
etal.,1992
studyas
wellas
questio
nnaire
completed
byclinicians
andcounsellors
Men
andwom
enat
riskof
HD
participatinginnatio
nalgenetic
testingprogramme
They
didno
tuseself-
repo
rtofadverseevents.
Chi-squareconducted
where
therewere<5
casesintwocells.
aand
c Indicate
studieswith
overlapping/samesamples.
b Indicates
studiesthat
may
have
someoverlapin
samples.
FBOC,fam
ilialbreast/ovarian
cancer;G
SI:SCL-90,G
lobalSeverity
Indexof
Symptom
Checklist-90;IES,Impact
ofEventScale;PSS,PerceivedStress
Scale;ST
AI,SpielbergerState–
TraitAnxiety
Inventory;CES-D
,CentreforEpidem
iologicalStudies
DepressionScale;
BDI,Be
ckDepressionInventory;HD,H
untin
gton
’sdisease;
GW
BS,G
eneralW
ell-B
eing
Scale.
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le4.
Outcomes
forindividualswho
areineligiblefortesting
Autho
rs,y
ear,
coun
try
Designan
dmetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Highquality
GeirdalandDahl,2008b,
Norway
aDesign:cross-sectional
n=68
carriers,174
ineligiblefor
testing,Unaffected
wom
enat
riskof
FBOCwho
attended
ahereditary
cancer
registry.
Anxiety
anddepressio
n(H
ADS)
Education
Com
paredwith
thecarriers,anxiety
was
higher
inwom
enwho
wereineligible
fortesting,butprevalence
ofdisorder
inbo
thgrou
pswas
24%.
Cross-sectio
naldesign
precludescontrollin
gfor
pre-existingdifferences
betweengrou
ps.
Metho
d:self-repo
rtquestio
nnaires;
3-mon
thpo
st-cou
nsellingfor
ineligiblefortesting,6-weekpo
st-
resultforcarriers
Didno
tcontrolfor
differences
betweengrou
psinfamilialcancer-related
events.
Geirdal,M
aehle,Heimdal
etal.,2006,N
orway
aDesign:cross-sectional
n=239ineligiblefortesting,1195
age-matched
populatio
ncontrols.
MentalQ
oL(M
CS:SF-12)
Age
Nodifferencebetweenwom
enwho
wereineligiblefortestingandcontrolsin
prevalence
ofmentalqualityof
lifecases.
Metho
d:self-repo
rtquestio
nnaires
3-mon
thpo
st-cou
nselling
Wom
enfro
mfamilieswith
noidentified
mutationwho
areatriskof
FBOC
(n=176)
orHNPC
C(n=63);mem
bers
ofahereditary
cancer
registry.Risk
grou
pscombineddueto
lack
ofclinically
significant
differences.
Cancer-related
distress-intrusion
andavoidancerelatedto
‘cancer
risk’(IE
S)
Geirdal,R
eichelt,Dahl
etal.,2005,N
orway
aDesign:cross-sectional
n=68
carriers,239
ineligiblefor
testing,10
000age-matched
populatio
ncontrols.
Anxiety
anddepressio
n(H
ADS)
Children,relatives
with
cancer,affected
parent,
maritalstatus,education
Nodifferencebetweencarriersandineligible
fortestingincancer-related
distress.W
omen
ineligiblefortestingrepo
rted
higher
anxiety,
moreanxietycases,andlower
depressio
nthan
controls.
Cross-sectio
naldesign
precludescontrollin
gforpre-
existingdifferences
between
grou
ps.
Metho
d:self-repo
rtquestio
nnaires
3-mon
thpo
st-cou
nsellingfor
ineligiblesand6-weekpo
st-result
forcarriers
Unaffected
wom
enat
riskof
FBOC(n=176)
orHNPC
C(n=63)who
attended
ahereditary
cancer
registry.R
iskgrou
pscombineddueto
lack
ofclinicallysignificant
differences.
Psycho
socialdistress(G
HQ-28)
FBOCwom
enineligiblefortesting
repo
rted
higher
anxiety,depressio
nandpsycho
socialdistress,and
moredepressio
nandpsycho
social
distresscasesthan
carriers.
Didno
tcontrolfor
differences
betweengrou
psinfamilialcancer-related
events.
Hop
elessness(BHS)
Cancer-related
distress-intrusio
nand
avoidancerelatedto
’cancer
risk’(IES)
Meiser,Bu
tow,Friedlander
etal.,2002,A
ustralia
Design:prospective
n=90
testers(30+ve,60-ve),53
ineligiblefortestingcontrols
Cancer-related
distress-intrusion
andavoidancerelatedto
’being
atriskof
developing
breastcancer’(IES)
N/A
Carriers
hadhigher
cancer-related
distress
7–10
days
and12-m
onth
post-notificatio
ncomparedwith
baselineandineligible
fortesting,andatrend
forhigher
cancer-related
distress4-mon
thpo
st-notificatio
n(p=0.054).C
ompared
with
ineligiblefortesting,carriers
repo
rted
reductions
inanxietyat
12mon
thsand
non-carriers
repo
rted
reductions
inanxiety
at7–
10days.Trend
forlower
stateanxiety
inno
n-carriers
comparedwith
ineligible
fortesting4-mon
thpo
st-notificatio
n.
Didno
tcontrolfor
differences
betweengrou
psinfamilialcancer-related
events
Metho
d:questio
nnairesat
baseline
(pre-cou
nsellingfortested
wom
en),
7–10
days
post-notificatio
n(post-
baselineforuntested),4-mon
thand
12-m
onth
post-baseline
Unaffected
FBOCwom
enwho
hadapproached
afamilialcancer
clinicor
outreach
clinic
Anxiety
(STA
I)Depression(BDI)
a Indicatesstudieswith
overlappingsamples.
FBOC,fam
ilialbreast/ovarian
cancer;H
ADS,HospitalA
nxiety
andDepressionScale;HNPC
C,hereditary
non-po
lypo
siscolorectalcancer;Q
oL,qualityof
life;MCS:SF-12,MentalC
ompo
nent
Scaleof
theShort-Fo
rm12
Health
Survey;IES,Impactof
EventS
cale;G
HQ-
28,T
heGeneralHealth
Questionnaire;B
HS,Be
ckHop
elessnessScale;ST
AI,SpielbergerState–
TraitAnxiety
Inventory;BD
I,Be
ckDepressionInventory.
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Tab
le5.
Vulnerabilityfactorsforindividualswho
decline,delayor
remainineligiblefortesting
Autho
rs,y
ear,
coun
try
Designan
dmetho
d
Sample
Mea
sures
Con
trol
variab
les
Relev
antfind
ings
Lim
itations
+ve=ca
rrier
(-)indica
tesun
valid
ated
mea
sures
-ve=no
n-ca
rrier
Highquality
GeirdalandDahl,
2008a,Norway
aDesign:cross-sectional
n=238ineligiblefortesting
Person
ality
traits(TCI)
N/A
HADS—
numberof
affected
femalerelatives,harm
avoidant
andpersistenttemperamental
traits,lessself-directednessand
lessop
timism
associated
with
higher
mentaldistress;harm
avoidancestrongestassociation.
Metho
d:self-repo
rtquestio
nnaires
3-mon
thpo
st-cou
nselling
Unaffected
wom
enfro
mfamilie
swith
noidentified
mutationat
riskof
FBOC(n=175)
orHNPC
C(n=63);
attendeesof
ahereditary
cancer
registry.
Risk
grou
pscombineddueto
lack
ofclinicallysignificant
differences.
Optimism
(LOT)
Hop
elessness(BHS)
Mentaldistress(H
ADS)
IES—
cancer
inaparent,harm
avoidance,persistence
andless
optim
ismassociatedwith
cancer-
related
distress,optimism
had
strongestassociation.
Cancer-related
distress-intrusivethou
ghts
relatedto
’theriskof
developing
breast
cancer’(IES)
GeirdalandDahl,
2008b,Norway
aDesign:cross-sectional
n=174ineligiblefortesting,68
carriers
Cop
ingstrategies
(COPE)
Education
‘Focus
onandventingof
emotions’,‘restraintcop
ing’and‘
behavio
uraldisengagem
ent’
associatedwith
increased
prevale
nceofanxietydisorderin
wom
enwho
wereineligiblefor
testing.
Metho
d:self-repo
rtquestio
nnaires;
3-mon
thpo
st-cou
nsellingfor
ineligiblefortesting,6-weekpo
st-
resultforcarriers
Unaffected
wom
enat
riskof
FBOC
who
attended
ahereditary
cancer
registry.
Anxiety
(HADS)
Geirdal,M
aehle,Heimdal
etal.,2006,N
orway
aDesign:cross-sectional
n=239ineligiblefortesting,1195
age-matched
populatio
ncontrols
Risk
grou
p:MentalQ
oL(M
CS:SF-12)
Risk
ofpo
ormentalQ
oLassociated
with
being
unpartneredforcontrolsand
wom
enineligiblefortesting.
Metho
d:self-repo
rtquestio
nnaires
3-mon
thpo
st-cou
nselling
Unaffected
wom
enfro
mfamilie
swith
noidentified
mutationwho
areat
riskof
FBOC(n=176)
orHNPC
C(n=63);attendeesof
ahereditary
cancer
registry.R
iskgrou
pscombined
dueto
lack
ofclinicallysignificant
differences.
Cancer-related
distress-intrusionand
avoidancerelatedto
‘cancerrisk’(IE
S)
Poor
mentalQ
oLwasassociated
with
intrusionandavoidancein
both
grou
ps.
Con
trols:Qualityof
life(SF-36)
Lerm
an,H
ughes,Lemon
etal.,1998,U
SADesign:Prospectivecoho
rtstudy
n=206testers(97+ve,109-ve),121
decliners
Low-m
oderatestressvs
high
stress;0–10
versus
11–33,respectivelyscored
for
intrusivethou
ghtsabou
t’havingcancer
inthefamily’(IES)
Baselinedepressio
n,gender,affected
status,
maritalstatus
Forhigh
stress,declinerseight
times
morelikelyto
become
depressedcomparedwith
non-
carriersat1-mon
thfollow-up.
%affected
notrepo
rted
Metho
d:baseline(pre-educatio
n)phon
einterview,1-m
onth
and6-
mon
thfollow-upphon
einterviews
FBOCmen
andwom
enfro
mmutation-po
sitivefamilie
sregistered
atahereditary
cancer
unit
Depression(CES-D
)Forunaffected
high
stress,higher
ratesof
depressio
nindecliners
(44%
)comparedwith
carriers
(24%
)and
non-carriers(16%
)at
6-month
follow-up.
a Indicatesstudieswith
overlappingsamples.
FBOC,fam
ilialbreast/ovarian
cancer;H
NPC
C,hereditary
non-po
lypo
siscolorectalcancer;T
CI,The
Tem
peramentand
Character
Inventory;LO
T,Life
Orientatio
nTest;BH
S,Be
ckHop
elessnessScale;HADS,HospitalA
nxietyandDepressionScale;IES,Im
pactof
Event
Scale;COPE,C
opingOrientatio
nto
Prob
lemsExperiencedScale;QoL
,qualityof
life;MCS:SF-12,
MentalC
ompo
nent
Scaleof
theShort-Fo
rm12
Health
Survey;SF-36,Sho
rt-Form
36Health
Survey;C
ES-D
,CentreforEpidem
iologicalStudies
DepressionScale.
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
whereas all studies of individuals at risk of FBOC reportedno difference or lower depression in decliners. For example,Reichelt et al. [17] investigated unaffected women (n=301)separately and found that those who went on to declineBReast CAncer risk (BRCA)1/2 testing had significantlylower levels of Hospital Anxiety and Depression Scale(HADS)-defined depressive symptoms, compared withtesters (M=2.0, standard deviation [SD] = 2.6 vs M=1.3,SD= 1.8, p< 0.05), although other potential confounderswere uncontrolled. Lerman et al. [27] found no differencebetween testers and decliners in depression, controlling forpotential confounders. Five comparisons that found nodifference for FBOC did not control for potential confoun-ders including affected status [1,27–30]. Notably, all studiesusing the Centre for Epidemiological Studies DepressionScale reported no difference or higher depression in decli-ners [1,16,27–30], whereas Reichelt et al. [17] reportedlower depression in decliners as assessed by the HADS.Only two studies prospectively compared anxiety between
testers and decliners, and these show no difference betweenthe groups. In women at risk of FBOC, there were nodifferences between testers and decliners in anxiety in 301unaffected women [17] or 126 women (46% affected)[28]; however, the analyses did not control for potentialconfounders.
Cancer-related distress
We identified six studies that prospectively comparedcancer-related distress in decliners and testers, with fourreporting a lack of differences between the groups andtwo finding lower distress in decliners. However, the find-ings suggest that those who decline counselling and test-ing report lower levels of distress than testers and thosewho undergo counselling and then decline. For example,Lerman et al. [27] found that decliners (n= 63) at risk ofFBOC who did not attend prenotification education weremore likely to report lower cancer-related distress (IESintrusion score 0–1) than testers (n= 86), controlling forpotential confounders. Similarly, Thompson et al. foundthat FBOC women who declined both counselling andtesting reported the lowest levels of intrusion (M= 5.5,SD= 2.2) compared with those who declined aftercounselling (M= 11.9, SD= 2.0, p< 0.05) and those whowere tested (M= 9.5, SD= 1.5, not significant), with highlevels in 18%, 73% and 58% of individuals in each group,respectively, (Χ2 (1, n=75) = 11.2, p=0.004) [26]. In con-trast, decliners in four studies with no difference betweengroups all received counselling or education [16,17,19,28].Null findings were restricted either by uncontrolled analyses[16,17,28] or a small decliner group (n=12) and unvali-dated cancer-related distress measure [19].
General distress, hopelessness and well-being
Four studies found no differences between decliners and tes-ters on general distress [17,24,28,31], hopelessness [17] orsubjective well-being [24]. These analyses did not controlfor potential confounders, although findings of Reichelt et al.[17] relate to unaffected women only. The general distressmeasure used in one studywas a composite score derived froma number of measures, some of which correlated with eachother at only r=0.42 [31], bringing into question its validity.
Research question 2: psychological outcomes forindividuals who decline, delay or remain ineligiblefor testing
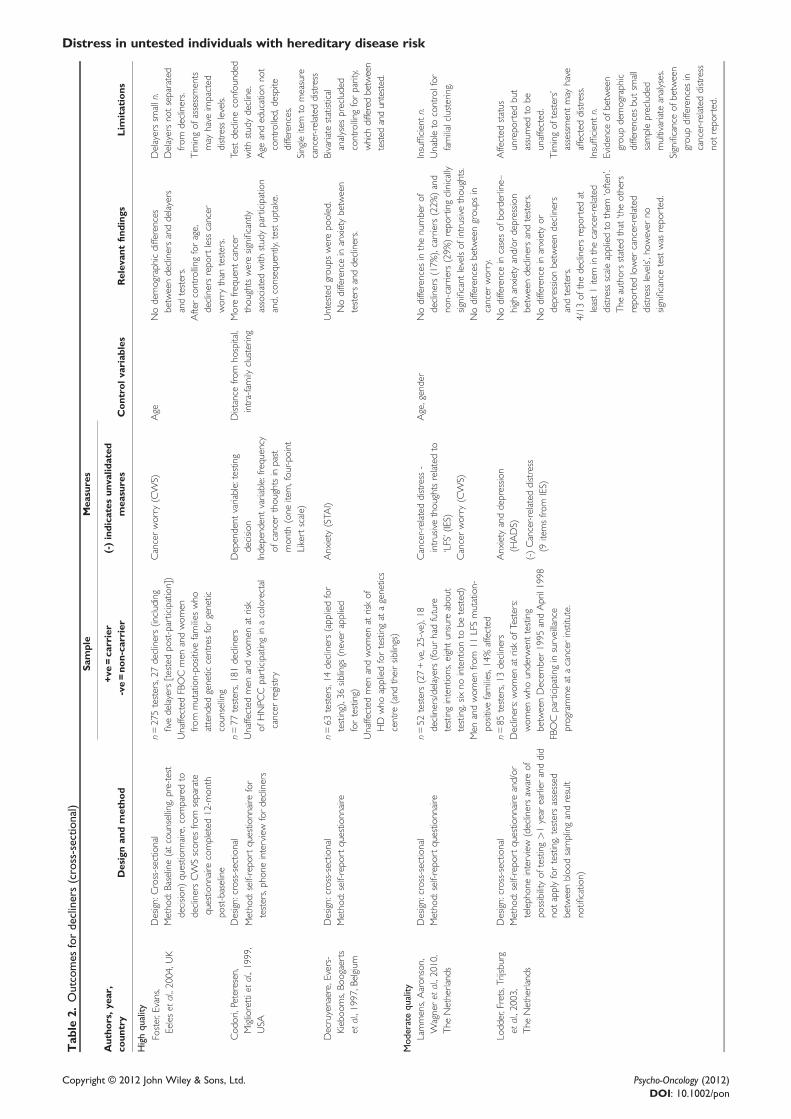
Psychological outcomes—decliners (cross-sectional studies)
Six studies compared distress of testers and decliners incross-sectional analyses, that is, after a decision had beenmade regarding genetic testing, with three high, two moder-ate and one adequate quality (Table 2). Two studies relatedto FBOC and one each to HNPCC, HD, Li–Fraumeni syn-drome and familial melanoma (FM). Studies assessed anxi-ety, depression and cancer-related distress, and, where theIES was used, the stressor was having a family history ofcancer [27], Li–Fraumeni syndrome [4] or FM [32].
Depression and anxiety
There were no significant differences between testers anddecliners in anxiety or depression, although the relevantstudies suffered a number of methodological limitations.Using the HADS, Lodder et al. and de Snoo et al. foundno differences between testers and decliners at risk ofFBOC [33] or FM [32], yet both decliner groups weresmall (n< 20) and overall sample size was deemed inade-quate. As a result, potential confounders were uncon-trolled. In addition, de Snoo et al. [32] did not reportresults of significance tests to support their finding.Decruyenaere et al. [34] also found no difference betweentesters and decliners in anxiety in bivariate analyses thatprecluded controlling for identified demographic differ-ences between groups.
Cancer-related distress
Five studies assessed cancer-related distress; two foundlower levels of cancer-related distress in decliners, one foundno difference and two found higher cancer-related distress indecliners. Taking study quality into consideration, the find-ings suggest decliners may experience less cancer-relateddistress than testers. Two large studies, of 302 individualsat risk of FBOC [35] and 258 individuals at risk of HNPCC[36], found lower levels of cancer-related distress in decli-ners compared with testers. However, in one study, timingof assessment for testers was unclear [35] and may haveimpacted distress levels, whereas in the other, decliningparticipation in the study, presented as an opportunity toobtain ‘free genetic counselling, and the option of freegenetic testing through a research study’, was the outcomevariable of test decline [36]. Therefore, test declinemay havebeen confounded with study decline. In addition, a singleitem measured cancer-related distress, and age andeducation were uncontrolled, despite evidence of differ-ences between groups on these variables [36] and well-established correlations between these variables andcancer-related distress [37–40]. In spite of these limitations,we prioritised these findings on the basis of adequate samplesize and the seriousness of the limitations in the otherstudies.
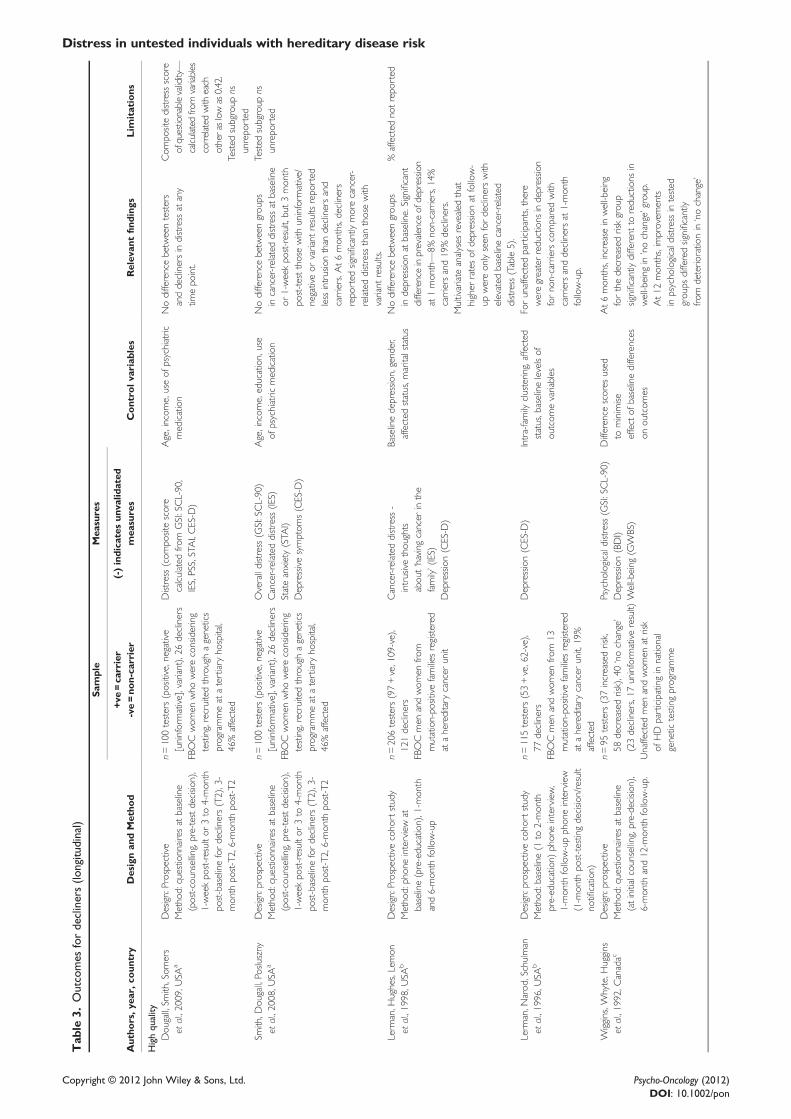
Psychological outcomes—decliners (longitudinal studies)
Six articles examined psychological outcomes of declinersin longitudinal studies that controlled for baseline levels
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon

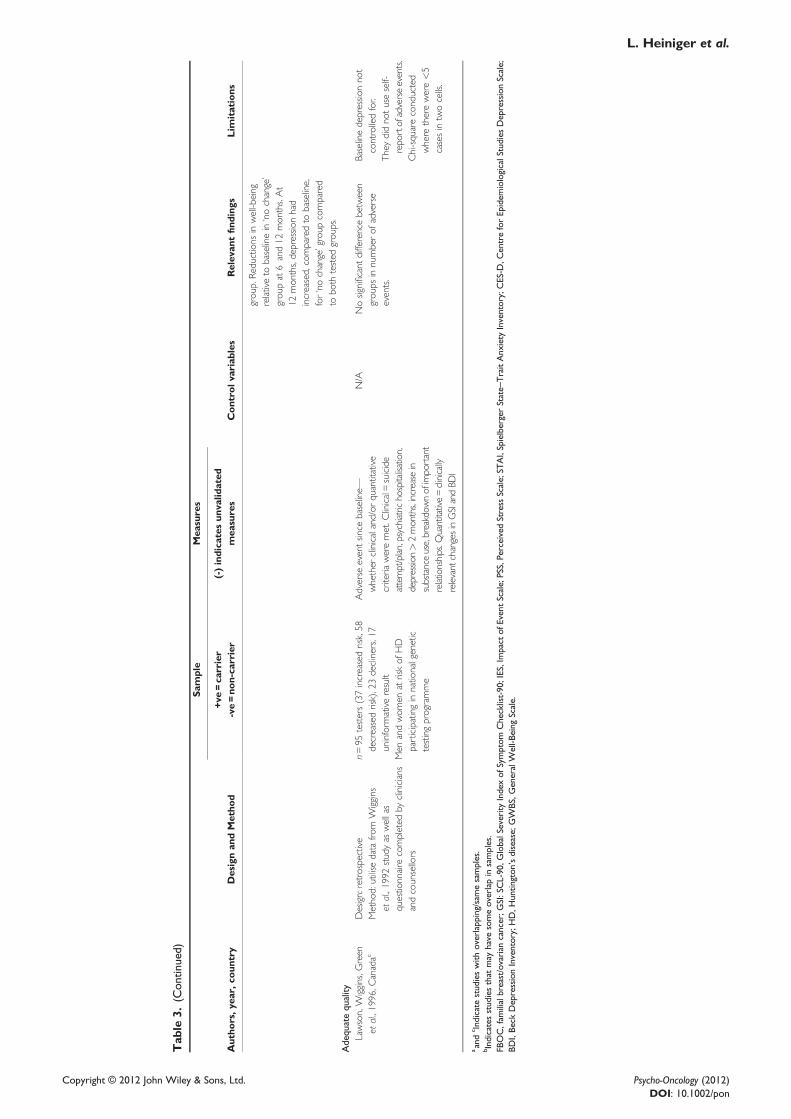
(Table 3). Direct comparison is limited by variations inmeasurement and conceptualisations of distress, and find-ings are complicated by methodological aspects. None ofthe studies reported better psychological outcomes fordecliners. One study examined individuals with familyhistories of HD [24,41], another study surveyed womenat risk of FBOC [28,31] and the samples in two articleson men and women at risk of FBOC may have overlapped[1,30]. Compared with various groups, three of these stud-ies reported worse outcomes for decliners, two reported nodifference in outcomes for decliners and one study reportedmixed findings according to the comparison group and typeof distress [28].There is evidence of worse outcomes for decliners of
HD testing across a range of outcomes, whereas there isstronger evidence of higher distress in decliners only inrelation to cancer-related distress and only compared withnon-carriers, in individuals at risk of FBOC. Among indi-viduals at risk of FBOC, decliners and carriers reportedmore intrusive thoughts than those with uninformativenegative and variant results 3 months after baseline [28],more intrusive thoughts than those with variant results6 months after baseline [28] and smaller reductions indepression compared with non-carriers one-month post-testing decision [30]. Despite the evidence of differencesbetween groups, changes over time within groups of thoseat risk for FBOC were either unassessed [1,30] or showedno effect of time [28]; although decliners may not reportthe same benefits as non-carriers, it is unknown whetherchanges in depression for decliners reflected deteriorationsin psychological functioning. Wiggins et al. [24] com-pared individuals at risk of HD who either received resultsindicating an increased (n= 37) or decreased (n= 58)risk, or had no change in risk due to declining (n= 23)or uninformative results (n= 17) (groups combinedbecause of lack of significant demographic or psycholog-ical differences). The no change group reported deteriora-tions in psychological functioning compared withbaseline, compared with testers and across a range ofoutcomes.Smith et al. [28] did not find significant differences in
overall distress, state anxiety or depression between testersand decliners, but the two other studies that reported noeffect of study group on distress suffered from variouslimitations. FBOC decliners and testers did not reportsignificantly different courses of distress over a six-monthperiod [30]; however, the composite distress measuremay have been of questionable validity (refer to researchquestion 1 results). No significant difference was foundbetween the groups at risk for HD (increased-risk,decreased-risk, no change in risk, decliners) in rates ofadverse events [41]; however, the objective assessment ofoccurrence of an adverse event was not supplementedby the participant’s self-report, and the small number ofparticipants who had reported an adverse event precludedmultivariate analyses.
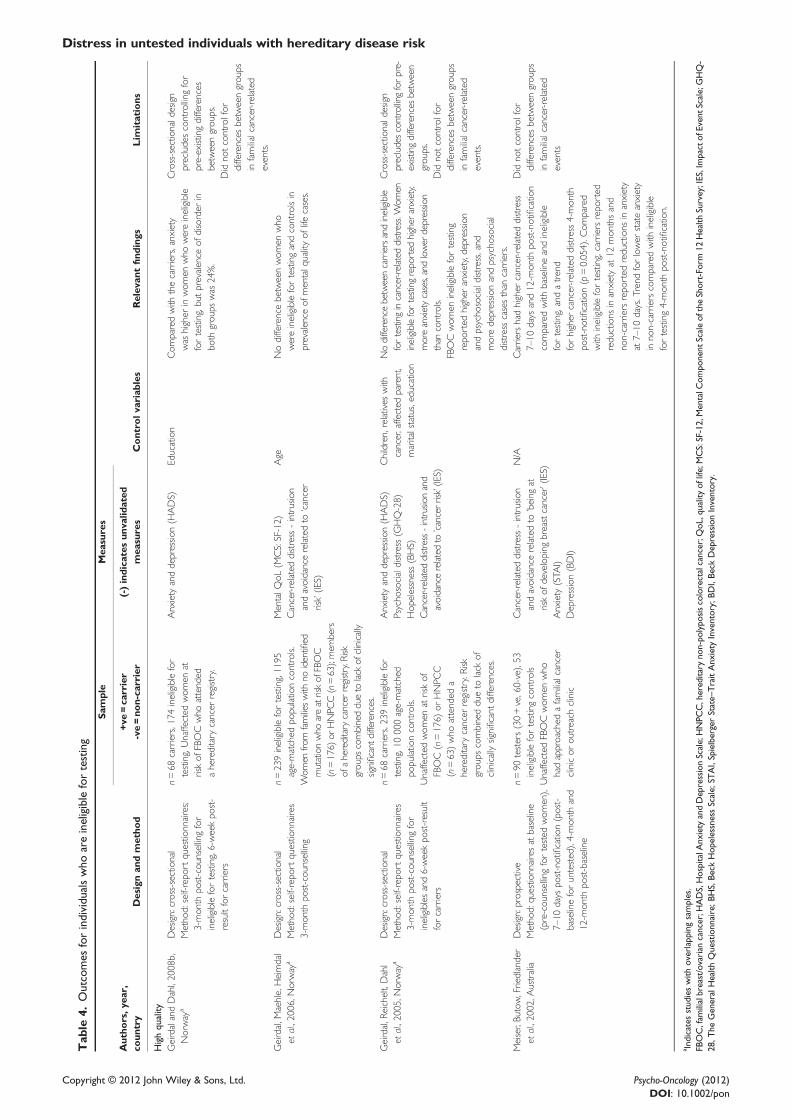
Psychological outcomes—ineligible for testing
Two high-quality studies of psychological outcomes inindividuals who were ineligible for testing were identifiedin the literature [12,13,42,43] (Table 4). Overall, women
at risk for FBOC who were ineligible for testing tendedto report higher anxiety than mutation carriers, althoughfindings for depression and cancer-related distress weremixed. Psychosocial distress (represented by scores onthe General Health Questionnaire-28), mental qualityof life, hopelessness, anxiety, depression, cancer-relateddistress (intrusion and avoidance related to cancer risk andbeing at risk of developing breast cancer) were investigated.In a series of cross-sectional comparisons, Geirdal et al.
compared women at risk for FBOC (n = 176) and HNPCC(n = 63) who were ineligible for testing to each other,BRCA1 mutation carriers (n= 68) and population controls[12,42,43]. Compared with mutation carriers, there wereno significant differences in anxiety, depression, hopeless-ness, psychosocial distress, intrusion or avoidance forineligible HNPCC women; however, ineligible FBOCwomen reported higher levels of depression, psychosocialdistress and mean anxiety, and no significant differencesin prevalence of anxiety disorder, intrusion, avoidanceand hopelessness [12,42]. The combined FBOC/HNPCCgroup reported less depression, more anxiety and compa-rable mental quality of life compared with populationcontrols [43,12].In a prospective study, Meiser et al. [13] compared 90
women at risk of FBOC who underwent testing to 53women who were ineligible for testing on anxiety, depres-sion and cancer anxiety. Testers reported significant redu-ctions in anxiety over time, controlling for potentialconfounders. Interestingly, there was an increase in stateanxiety for women who were ineligible for testing frombaseline (M=33.6, SD=10.7) to 12 months (M=39.0,SD=12.2). Although not reported, we estimated an effectsize of 0.5, a moderate effect, using the baseline standarddeviation [44] ([39–33.6]/10.7) and used the group size tocalculate t=3.39, p< 0.05, demonstrating a significantincrease in anxiety from baseline to 12 months for womenwho were ineligible for testing. Carriers tended to reporthigher cancer-related distress compared with the womenwho were ineligible for testing; however, this may be dueto differences in levels of familial cancer-related eventsbetween participants with and without a known familialmutation. Depression levels did not differ between groups.Note that the ineligible women in the study of Geirdal
et al. had undergone genetic counselling 3 months priorto participation, at which time they had been advised amutation was assumed to be responsible for the familycancer history despite no mutation being identified [12].In contrast, no risk information was available for ineli-gible women in the study of Meiser et al [13].
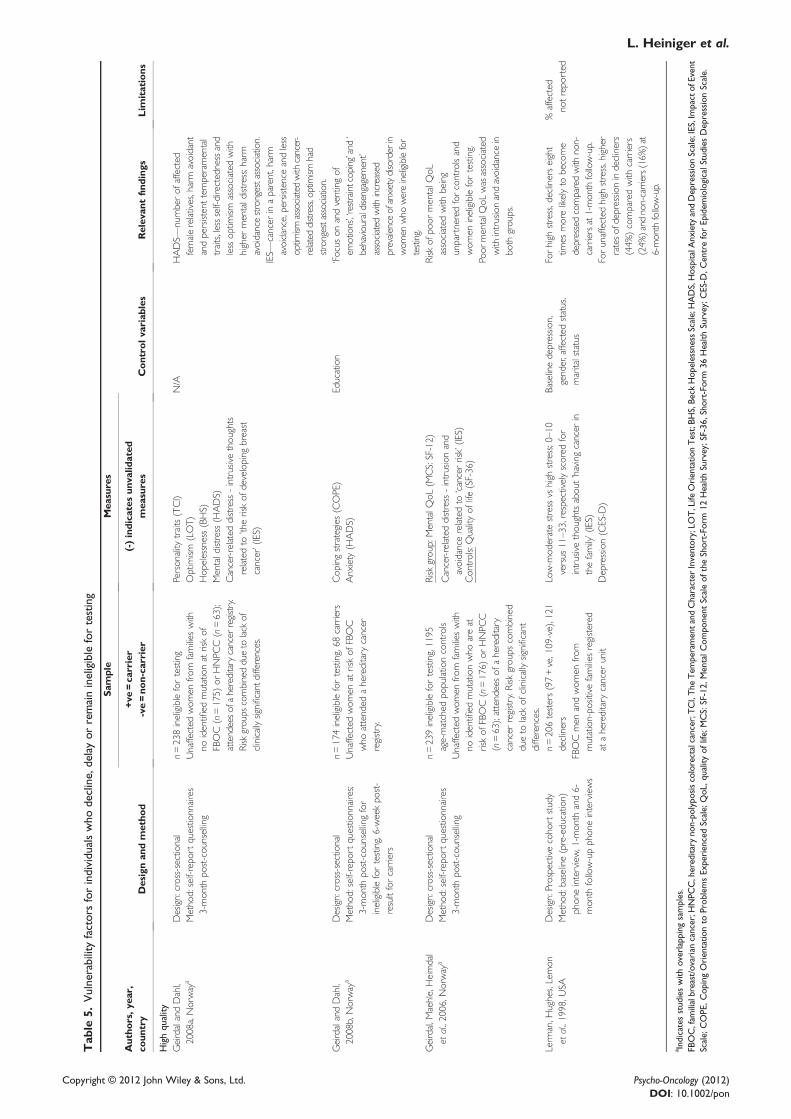
Research question 3: vulnerability factors forindividuals who decline, delay or remain ineligiblefor testing
Four high-quality articles identified factors increasing anindividual’s vulnerability to distress (Table 5). One prospec-tive study assessed affected and unaffected American menand women at risk of FBOC who declined testing [1].Geirdal et al. reported a cross-sectional data on unaffectedwomen who were ineligible for testing from Norway inthree articles with considerable sample overlap [42,43,45].Two articles report cross-sectional data from a study of
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
women at risk of FBOC and HNPCC. Because of a lack ofsignificant differences between the risk groups, their dataare combined in the analyses. One article reports the rela-tionships between variables within the risk group [45], theother investigates relationships between variables andcompares the risk group with population controls [43].The third Norwegian article reports data from the FBOCgroup in the aforementioned study and compares them witha group of BRCA1 mutation carriers [42].The four articles report that cancer-related distress (IES
stressor having cancer in the family [1]), demographics,family history, personality and coping style are vulnerabil-ities for poorer mental quality of life, anxiety and depres-sion. Evidence from these studies suggests that
(1) decliners who report high levels of cancer-relateddistress at baseline are more likely to develop clini-cally significant depressive symptoms than carriersand non-carriers [1];
(2) among women at risk of FBOC who remain ineligiblefor testing, focus on emotions, venting of emotionsand avoidance through behavioural disengagementare associated with increased prevalence of anxietydisorder [42];
(3) among women at risk of FBOC and HNPCC whoremain ineligible for testing,
• persistence, the tendency to avoid harm, less self-directedness and less optimism are associated withhigher levels of mental distress (combined anxietyand depression), and these traits demonstrate stron-ger associations with mental distress than demo-graphic and cancer-related variables [45];
• not having a partner is associated with increasedrisk of poorer mental quality of life [43];
• higher levels of intrusion and avoidance areassociated with poorer mental quality of life [43].
Discussion
We reviewed studies investigating distress in unaffectedindividuals at increased familial risk for disease who hadnot undergone genetic testing. These individuals comprisethe majority of unaffected, at-risk family members andhave been under-researched thus far. The majority of theidentified studies have been conducted with members ofhereditary cancer registries and involve individuals at riskfor FBOC. At this time, research investigating distress inindividuals who decline, delay or remain ineligible forHD genetic testing is sparse and insufficient to allow ameaningful comparison with individuals at risk of heredi-tary cancer. The included studies, from seven differentcountries, are a mixture of longitudinal and cross-sectionalstudies with most of the relevant findings pertaining todecliners. This review identified few studies of individualswho were ineligible for testing and no studies reportingresults for delayers as a group distinct from decliners. Pastresearch has, justifiably, focused on the psychologicalwell-being of individuals who undergo genetic testing;however, this review points to a need to monitor distresslevels in those who remain untested as well.
Those who declined to be involved in the genetic test-ing process altogether tended to report less cancer-relateddistress than testers. However, decliners have reportedlittle confidence in their ability to cope with an unfavour-able test result compared with testers [32,36], implying thedecision to decline involvement is made in the interest ofavoiding distress. This indicates that test takers are likelyto be self-selected [46], highlighting the importance ofpreserving autonomy in genetic testing decisions [41]and supporting the idea that anticipatory distress may leadto avoidance, while current distress may motivate a desirefor genetic testing as a means to manage distress [26].Some at-risk individuals perceive little value in findingout their result, particularly if they have no intentions ofchanging their risk management strategies regardless ofthe outcome [47]; therefore, the anticipated distress of apositive result justifies declining testing. Longer-termpsychological benefits of declining mutation testingremain unclear, and further research is needed to elucidatethe nature of these.What is clear from this review is that not all decliners
are the same. Some are passive decliners who are awareof the opportunity to undergo testing and choose not toapproach genetic services. Such individuals often alsodecline to be involved in research studies [30] or arenever invited to participate in research as a result of theirnon-attendance at familial cancer clinics. Consequently,the true denominator of potential testers is likely unknown.Further, significantly more test decliners, compared withtesters, withdraw from studies prior to completion [1]. Bothissues may account for the small numbers of decliners, andthe associated lack of statistical power, in many of thereviewed studies. Thus, the findings from this review maynot be generalisable to the population of individuals whochoose not to undergo genetic testing.Another group of decliners seeks risk information from
genetic services but these individuals do not seek genetictesting. Others commence the testing process by giving ablood sample but do not return for the testing results.Some of these decliners undergo testing at a later date orat least indicate interest in later testing [19,34,35]. Thefindings of this review support the assertion that one groupconsciously decides to remain untested, whereas anothergroup engages in an avoidant coping strategy and may notcope as well as the former group [34], confirming a needfor delayers to be considered separately.Individuals with increased familial risk for disease who
remain ineligible for genetic testing are an understudiedgroup. The available evidence to date indicates thatwomen who remain ineligible for testing for FBOC havehigher levels of general anxiety than both women whohave undergone testing and the general population.Whether general anxiety is directly related to genetictesting is unclear. The model of stress and genetic testing[48] suggests that reducing uncertainty through genetictesting may be psychologically beneficial; thus, theongoing uncertainty of remaining ineligible for testingmay be experienced as distressing. This model alsoproposes that being identified as a carrier may exacerbatedistress related to the disease itself, and this might explainwhy carriers reported more cancer-related distress thanwomen who were ineligible for testing. However, we
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon

know that stress related to non-familial cancer events isassociated with increased anxiety in women at increasedrisk of FBOC and that stress specifically related to familialcancer events is associated with increased cancer-relateddistress rather than general anxiety [39]. Therefore, be-cause familial cancer-related events are likely to be morecommon in families with identified mutations, any actualdifference between the groups on this variable may haveconfounded results. Future studies comparing womenwith and without identified familial mutations should con-sider assessing this variable as a potential covariate.The findings of this review indicate a need for support to
be available for untested individuals. A number of demo-graphic, psychosocial and family history factors have beenassociated with an increased risk of distress in untested indi-viduals, consistent with research on those at risk for FBOC[39,49] and HD [50]. Formal risk assessment and/or geneticcounselling may not be sought in the absence of an identifiedmutation, but many of the high-risk individuals in the studiesreviewed here were members of hereditary cancer registries,and this membership may present opportunities to offer sup-port. For example, additional support could be offered tothose who decline testing following education or counsellingand to decliners who present with elevated cancer-relateddistress. Individuals who remain ineligible for testing mayfind the shared understanding of support groups helpful inrelieving general anxiety. However, to date, there is insuffi-cient evidence to justify the cost-effectiveness of providingadditional support. Further research is needed to establishwhat, if any, resources should be considered for use in thesepopulations and how to best identify individuals whose dis-tress levels warrant referral for additional support.One limitation of this review was that our criteria
excluded a number of potentially eligible qualitative stud-ies of individuals who were ineligible for testing that didnot report separate results for affected and unaffected indi-viduals (e.g. [51–53]). Because of the nature of qualitativeinquiry, separate reporting of results for affected and unaf-fected individuals may not be appropriate. However, we
deemed this exclusion criterion necessary because motiva-tions for testing and distress responses to testing outcomesdiffer between affected and unaffected individuals [54].Although this criterion was applied in the search process,we still reported results of bivariate analyses whereaffected status was uncontrolled. We did so because iftest status was unrelated to distress in bivariate analyses,these distress variables were often not included in multi-variate analyses, particularly when these variables werenot central to the study’s aims. Future studies focused onthe needs and functioning of unaffected individuals willexpand our knowledge in this area. Most of the articleson women who were ineligible for testing included inthis review used the same sample, limiting generalisabilityof these findings. Further, international variations in theprocedures and rules governing risk assessment, geneticcounselling and genetic testing complicate the generalisa-bility of any study in this field [55].The majority of unaffected high-risk individuals remain
untested. The absence of research on delayers, mixed find-ings on decliners and our limited understanding of how indi-viduals cope with being ineligible for testing indicate anurgent need to assess psychosocial functioning in thesegroups. Future studies could explore the experience of beingineligible for testing, how risk is understood withinthis context, what type of information, if any, is soughtand the relationship between being ineligible for testingand psychological distress. Once these aspects are betterunderstood, psychological functioning and risk factors fordistress in individuals who are ineligible for testingshould be assessed in settings that accurately reflect theirexperiences to improve generalisability of the findings.Psychosocial support is routine for those seeking genetic
testing. The results of this review indicate that individualswho do not undergo testing may also benefit from such sup-port. Because one-on-one counselling resources are limited,this highlights the need for further research to identify thoseat highest risk for poorer psychological outcomes so that inter-ventions can be targeted to individuals with the greatest need.
Appendix A. Disease characteristicsDisease Risk for mutation carriers Prevention options Screening options Treatment options
Familialbreast/ovariancancer
Up to 85% breast cancer risk and60% ovarian cancer risk by age70 years
Chemoprevention Mammogram SurgeryProphylactic surgery—removalof breasts and/or ovaries
Breast ultrasound ChemotherapyMRI Radiation therapyTransvaginal ultrasound Hormone therapyCA-125 blood test for ovarian cancer Targeted therapies
Hereditary non-polyposis colorectalcancer
80–85% Prophylactic surgery—removalof part or all of colon
Fecal occult blood test SurgeryIncreased risk also for cancer of theuterus, stomach, small intestine, pancreas,kidney, ureter and ovary
Colonoscopy ChemotherapyUrine cytology RadiationTVUCA-125
Li–Fraumeni syndrome—high risk of various cancersfrom early childhood
Up to 90% lifetime risk, 20% riskbefore age 20 years
None (possible prophylacticmastectomy for femalemutation carriers)
Unclear due to risk of cancer atmultiple sites and possible increasedsensitivity to radiation, but regularmedical checks are carried out
Available but varydepending on the typeof cancer
Familial melanoma 60–90% Limitation of sun exposure Skin examination SurgeryPossibility of concomitant increasedpancreatic cancer risk (<20%)
ChemotherapyImmunotherapyRadiation
Huntington’s disease—progressiveneuropsychiatric disorder
100%—late onset None Physical and psychological screeningto identify signs of disease onset
None, although treatmentsare available to manage andlessen symptoms
MRI, magnetic resonance imaging; TVU, transvaginal ultrasound.
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
AcknowledgementsPhyllis Butow is supported by an NHMRC Research FellowshipAward.
Conflict of interest
There are no potential conflicts of interest.
References
1. Lerman C, Hughes C, Lemon SJ, et al. Whatyou don’t know can hurt you: adverse psycho-logic effects in members of BRCA1-linkedand BRCA2-linked families who declinegenetic testing. Journal of Clinical Oncology1998;16(5):1650–1654.
2. Hamilton JG, Lobel M, Moyer A.Emotional distress following genetic testingfor hereditary breast and ovarian cancer: ameta-analytic review. Health Psychology2009;28(4):510–518.
3. Heshka JT, Palleschi C, Howley H, Wilson B,Wells PS. A systematic review of perceivedrisks, psychological and behavioral impactsof genetic testing. Genetics in Medicine2008;10(1):19–32.
4. Lammens CR, Aaronson NK, Wagner A, et al.Genetic testing in Li–Fraumeni syndrome:uptake and psychosocial consequences. J ClinOncol 2010;28(18):3008–14.
5. van Asperen CJ, van Dijk S, Zoeteweij MW,et al. What do women really want to know?Motives for attending familial breast cancerclinics. Journal of Medical Genetics2002;39(6):410–414.
6. van Dijk S, Otten W, Timmermans DR, et al.What’s the message? Interpretation of anuninformative BRCA1/2 test result for womenat risk of familial breast cancer. Genet Med2005;7(4):239–45.
7. Bish A, Sutton S, Jacobs C, Levene S,Ramirez A, Hodgson S. No news is (notnecessarily) good news: impact of preliminaryresults for BRCA1 mutation searches. Geneticsin Medicine 2002;4(5):353–358.
8. Kirk J, Tucker K. National Best PracticeGuidelines for Familial Cancer Clinics, N.N.B.C. Centre. 1997: Sydney.
9. Ropka ME, Wenzel J, Phillips EK, Siadaty M,Philbrick JT. Uptake rates for breast cancergenetic testing: a systematic review. CancerEpidemiology Biomarkers & Prevention2006;15(5):840–855.
10. Keogh LA, van Vliet CM, Studdert DM, et al.Is uptake of genetic testing for colorectalcancer influenced by knowledge of insuranceimplications? Medical Journal of Australia2009;191(5):255–258.
11. Morrison PJ. Accurate prevalence and uptakeof testing for Huntington’s disease. LancetNeurology 2010;9(12):1147–1147.
12. Geirdal AO, Reichelt JG, Dahl AA, et al.Psychological distress in women at risk ofhereditary breast/ovarian or HNPCC cancersin the absence of demonstrated mutations.Familial Cancer 2005;4(2):121–6.
13. Meiser B, Butow P, Friedlander M, et al.Psychological impact of genetic testing inwomen from high-risk breast cancerfamilies. European Journal of Cancer2002;38(15):2025–31.
14. Collins V, Halliday J, Warren R, WilliamsonR. Cancer worries, risk perceptions andassociations with interest in DNA testingand clinic satisfaction in a familialcolorectal cancer clinic. Clinical Genetics2000;58(6):460–8.
15. Coyne JC, Kruus L, Racioppo M, CalzoneKA, Armstrong K. What do ratings ofcancer-specific distress mean among womenat high risk of breast and ovarian cancer?American Journal of Medical Genetics PartA 2003;116A(3):222–228.
16. Lerman C, Hughes C, Trock BJ, et al.Genetic testing in families with hereditarynonpolyposis colon cancer. Jama-Journalof the American Medical Association1999;281(17):1618–1622.
17. Reichelt JG, Heimdal K, Moller P, Dahl AA.BRCA1 testing with definitive results: aprospective study of psychological distress ina large clinic-based sample. Familial Cancer2004. 3(1):21–8.
18. Tabachnick BG, Fidell LS. Using MultivariateStatistics. Harper & Row: New York, 1983.
19. Kelly K, Leventhal H, Andrykowski M, et al.The decision to test in women receivinggenetic counseling for BRCA1 and BRCA2mutations. Journal of Genetic Counseling2004;13(3):237–257.
20. Keller M, Jost R, Kadmon K, et al.Acceptanceof and attitude toward genetic testing forhereditary nonpolyposis colorectal cancer: acomparison of participants and nonparticipantsin genetic counseling. Dis Colon Rectum,2004;47(2):153–62.
21. Kmet LM, Lee RC, Cook LS. StandardQuality Assessment Criteria for EvaluatingPrimary Research Papers from a Variety ofFields. I.o.H. Economics, Editor. AlbertaHeritage Foundation for Medical Research:Edmonton, Alberta, 2004.
22. Lee L, Packer TL, Tang SH, Girdler S. Self-management education programs for age-related macular degeneration: a systematicreview. Australasian Journal on Ageing2008;27(4):170–176.
23. Meiser B, Gleeson MA, Tucker KM.Psycholgoical impact of genetic testingfor adult-onset disorders: an update forclinicians. Medical Journal of Australia2000;172(3):126–129.
24. Wiggins S, Whyte P, Huggins M, et al. Thepsychological consequences of predictivetesting for Huntington’s disease. CanadianCollaborative Study of Predictive Testing.New England Journal of Medicine1992;327(20):1401–5.
25. Horowitz MJ, Wilner N, Alvarez W.Impact of Event Scale: a measure of sub-jective stress. Psychosomatic Medicine1979;41(3):209–218.
26. Thompson HS, Valdimarsdottir HB, Duteau-Buck C, et al. Psychosocial predictors ofBRCA counseling and testing decisionsamong urban African-American women.Cancer Epidemiology Biomarkers & Preven-tion 2002;11(12):1579–1585.
27. Lerman C, Schwartz MD, Lin TH, Hughes C,Narod S, Lynch HT. The influence of psycho-logical distress on use of genetic testingfor cancer risk. Journal of Consulting andClinical Psychology 1997;65(3):414–420.
28. Smith AW, Dougall AL, Posluszny DM,Somers TJ, Rubinstein WS, Baum A. Psycho-logical distress and quality of life associated
with genetic testing for breast cancer risk.Psycho-Oncology 2008;17(8):767–773.
29. Biesecker BB, Ishibe N, Hadley DW, et al.Psychosocial factors predicting BRCA1/BRCA2 testing decisions in members ofhereditary breast and ovarian cancer families.American Journal of Medical Genetics2000;93(4):257–263.
30. Lerman C, Narod S, Schulman K, et al.BRCA1 testing in families with hereditarybreast-ovarian cancer. A prospective study ofpatient decision making and outcomes. JAMA1996;275(24):1885–92.
31. Dougall AL, Smith AW, Somers TJ,Posluszny DM, Rubinstein WS, Baum A.Coping with genetic testing for breast cancersusceptibility. Psychosomatic Medicine2009;71(1):98–105.
32. de Snoo FA, Riedijk SR, van Mil AM, et al.Genetic testing in familial melanoma: up-take and implications. Psycho-Oncology2008;17(8):790–796.
33. Lodder, L, Frets PG, Trijsburg RW, et al.Attitudes and distress levels in women atrisk to carry a BRCA1/BRCA2 gene muta-tion who decline genetic testing. AmericanJournal of Medical Genetics Part A2003;119A(3):266–72.
34. Decruyenaere M, Evers-Kiebooms G, BoogaertsA, et al. Non-participation in predictive testingfor Huntington’s disease: individual decision-making, personality and avoidant behaviour inthe family. European Journal of HumanGenetics, 1997;5(6):351–363.
35. Foster C, Evans DR, Eeles R, et al. Non-uptake of predictive genetic testing forBRCA1/2 among relatives of known carriers:attributes, cancer worry, and barriers to testingin a multicenter clinical cohort. GeneticTesting 2004;8(1):23–29.
36. Codori AM, Petersen GM, Miglioretti DL,et al. Attitudes toward colon cancer gene test-ing: factors predicting test uptake. CancerEpidemiol Biomarkers Prev 1999;8(4 Pt 2):345–51.
37. Vodermaier A, Esplen MJ, Maheu C. Canself-esteem, mastery and perceived stigmapredict long-term adjustment in womencarrying a BRCA1/2-mutation? Evidencefrom a multi-center study. Familial Cancer2010;9(3):305–11.
38. Lodder L, Frets PG, Trijsburg RW, et al. Pre-symptomatic testing for BRCA1 and BRCA2:how distressing are the pre-test weeks? Journalof Medical Genetics 1999;36(12):906–913.
39. Price MA, Butow PN, Lo SK, Wilson J. Pre-dictors of cancer worry in unaffected womenfrom high risk breast cancer families: risk per-ception is not the primary issue. Journal ofGenetic Counseling 2007;16(5):635–44.
40. Bjorvatn C, Eide GE, Hanestad BR, HamangA, Havik OA. Intrusion and avoidance in sub-jects undergoing genetic investigation andcounseling for hereditary cancer. SupportiveCare in Cancer 2009;17(11):1371–1381.
41. Lawson K,Wiggins S, Green T, Adam S, BlochM, Hayden MR. Adverse psychological eventsoccurring in the first year after predictive testingfor Huntington’s disease. Journal of MedicalGenetics 1996;33(10):856–862.
Distress in untested individuals with hereditary disease risk
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon

42. Geirdal AO, Dahl AA. The relationshipbetween coping strategies and anxietyin women from families with familialbreast-ovarian cancer in the absence ofdemonstrated mutations. Psycho-Oncology2008a;17(1):49–57.
43. Geirdal AO, Maehle L, Heimdal K, StormorkenA, Moller P, Dahl AA. Quality of life and itsrelation to cancer-related stress in women offamilies with hereditary cancer without demon-strated mutation. Quality of Life Research2006;15(3):461–70.
44. Hadzi-Pavlovic D. Effect sizes III: differenceson repeated measurements. Acta Neuropsy-chiatrica 2008;20(1):48–49.
45. Geirdal AO, Dahl AA. The relationshipbetween psychological distress and personal-ity in women from families with familialbreast/ovarian or hereditary non-polyposiscolorectal cancer in the absence of demon-strated mutations. Journal of Genetic Counsel-ing 2008b;17(4):384–93.
46. Codori AM, Hanson R, Brandt J. Self-selectionin predictive testing for Huntington’s disease.
American Journal of Medical Genetics1994;54(3):167–173.
47. Caruso A, Vigna C, Maggi G, Sega FM,Cognetti F, Savarese A. The withdrawalfrom oncogenetic counselling and testing forhereditary and familial breast and ovariancancer. A descriptive study of an Italiansample. J Exp Clin Cancer Res 2008;27:75.
48. Baum A, Friedman AL, Zakowski SG. Stressand genetic testing for disease risk. HealthPsychology 1997;16(1):8–19.
49. Audrain J, Schwartz MD, Lerman C,Hughes C, Peshkin BN, Biesecker BB.Psychological distress in women seekinggenetic counseling for breast-ovarian cancerrisk: The contributions of personality andappraisal. Annals of Behavioral Medicine1997;19(4):370–377.
50. Pakenham K, Goodwin V, MacMillan J.Adaptation to being at-risk for Huntington’sdisease and the availability of genetic test-ing: application of a stress and copingmodel. Psychology, Health & Medicine2004;9(3):380–396.
51. Bottorff JL, Balneaves LG, Buxton J, et al.Falling through the cracks—women’s experi-ences of ineligibility for genetic testing for riskof breast cancer. Canadian Family Physician2000;46:1449–1456.
52. Persson E, Lindholm E, Berndtsson I, LundstamU, Hultén L, Carlsson E. Experiences of livingwith increased risk of developing colorectaland gynaecological cancer in individuals withno identified gene mutation. ScandinavianJournal of Caring Sciences 2012;26(1):20–27.
53. Crump RJ, Fitzgerald RP, Legge M. ‘Going-to-have-cancerness’: a study of living withincreased risk of BRCA1 and BRCA2mutations for six South Island women. J PrimHealth Care 2010;2(4):311–7.
54. Croyle RT, Smith KR, Botkin JR, Baty BJ,Nash J. Psychological responses to BRCA1mutation testing: preliminary findings.Health Psychology 1997;16(1): 63–72.
55. Meiser B, Gaff C, Julian-Reynier C, et al.International perspectives on genetic counsel-ing and testing for breast cancer risk. BreastDisease 2006;27:109–25.
L. Heiniger et al.
Copyright © 2012 John Wiley & Sons, Ltd. Psycho-Oncology (2012)DOI: 10.1002/pon
Related Documents










