Diseases of White Blood Cells(2) Lecturer :Yiran Ni, MD Department of Pathology China Three Gorges University Email:[email protected] Dec.2012

Diseases of White Blood Cells(2) Lecturer :Yiran Ni, MD Department of Pathology China Three Gorges University Email:[email protected] Dec.2012.
Jan 11, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Diseases of White Blood Cells(2)
Lecturer :Yiran Ni, MD
Department of Pathology
China Three Gorges University
Email:[email protected]
Dec.2012
What we’ve learned
• Leukopenia;
• Reactive leukocytosis;
• Lymphadenitis;
• General aspects and classification of neoplastic proliferation of white cell;
• Acute myeloid leukaemia
Target of this class
• Myelodysplastic Syndromes
• chronic myeloid leukaemia
• histiocytoses
• splenomegaly

Myelodysplastic Syndromes
General aspect
• The term "myelodysplastic syndromes" (MDS) refers to a group of clonal stem cell disorders characterized by maturation defects associated with ineffective hematopoiesis and an increased risk of transformation to acute myelogenous leukemias (AML).
• In patients with MDS, the bone marrow is partly or wholly replaced by the clonal progeny of a mutant multipotent stem cell that retains the capacity to differentiate into red cells, granulocytes, and platelets but in an ineffective and disordered fashion.
• These disturbances usually manifest as peripheral blood cytopenias.
General aspect
• In patients with MDS, the bone marrow is partly or wholly replaced by the clonal progeny of a mutant multipotent stem cell that retains the capacity to differentiate into red cells, granulocytes, and platelets but in an ineffective and disordered fashion.
• These disturbances usually manifest as peripheral blood cytopenias.
General aspect
• MDS arises in two distinct settings:
• Idiopathic or primary MDS occurs mainly at ages over 50 and often develops insidiously.
• Therapy-related MDS (t-MDS) is a complication of previous genotoxic drug or radiation therapy that appears 2 to 8 years after treatment.
General aspect
• All forms of MDS can transform to AML, but transformation occurs most rapidly and with highest frequency in t-MDS.
• Although characteristic morphologic changes are typically seen in the marrow and the peripheral blood, definitive diagnosis frequently requires correlation with other laboratory tests.
• Cytogenetic analysis is particularly helpful in confirming the diagnosis, as certain chromosomal aberrations are often observed.
General aspect
Pathogenesis
• The pathogenesis of MDS is unknown.
• Although the marrow is usually hypercellular at diagnosis, it can also be normocellular or, less commonly, hypocellular.
Pathogenesis
• Myelodysplastic bone marrow progenitors undergo apoptotic cell death at an increased rate, the hallmark of ineffective hematopoiesis.
• Given this, it is difficult to understand how myelodysplastic progenitors could displace any remaining normal marrow progenitors, suggesting that MDS arises within a background of stem cell damage or depletion.
Pathogenesis
• Both primary MDS and t-MDS occurring after exposure to radiation or alkylating chemotherapeutic drugs are associated with similar clonal chromosomal abnormalities, including monosomy 5 and monosomy 7, deletions of 5q and 7q, trisomy 8, and deletions of 20q.
Morphology
• The most characteristic finding is disordered (dysplastic) differentiation affecting all non-lymphoid lineages (erythroid, granulocytic, monocytic, and megakaryocytic)
Morphology
• Within the erythroid series, common abnormalities include: ringed sideroblasts, erythroblasts with iron-laden mitochondria visible as perinuclear granules in Prussian blue-stained biopsies; megaloblastoid maturation resembling that seen in vitamin B12 and folate deficiency; and nuclear budding abnormalities, recognized as nuclei with misshapen, often polypoid, outlines
Morphology
• Neutrophils often contain decreased numbers of secondary granules, toxic granulations.
• neutrophils with only two nuclear lobes, are frequently observed, and neutrophils may even be seen that completely lack nuclear segmentation.
Morphology
• Megakaryocytes with single nuclear lobes or multiple separate nuclei (pawn ball megakaryocytes) are also characteristic.
• Myeloblasts may be increased but make up less than 20% of the overall marrow cellularity.
Morphology
• The peripheral blood often contains pseudo-Pelger-Hüet cells, giant platelets, macrocytes, poikilocytes, and a relative or absolute monocytosis.
• Myeloblasts usually make up less than 10% of the peripheral leukocytes.
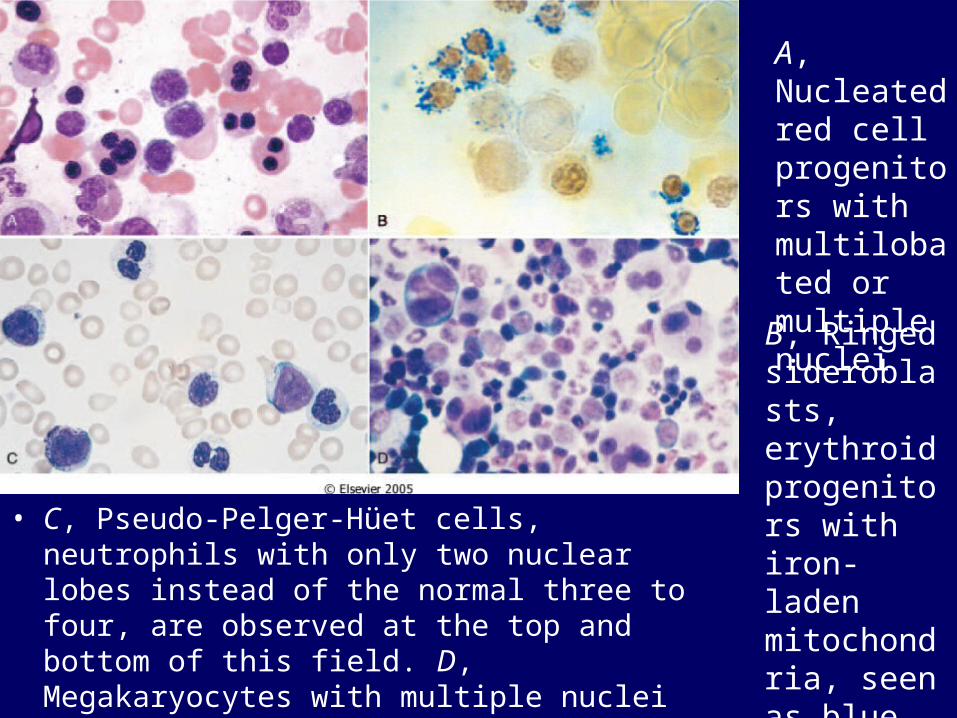
• C, Pseudo-Pelger-Hüet cells, neutrophils with only two nuclear lobes instead of the normal three to four, are observed at the top and bottom of this field. D, Megakaryocytes with multiple nuclei instead of the normal single multilobated nucleus
A, Nucleated red cell progenitors with multilobated or multiple nuclei
B, Ringed sideroblasts, erythroid progenitors with iron-laden mitochondria, seen as blue perinuclear granules
Clinical Course
• Primary MDS affects mainly individuals older than 60 years of age.
• When symptomatic, it presents with weakness, infections, and hemorrhages, all due to pancytopenia.
• In up to half of the cases, MDS is discovered incidentally on routine blood testing.
Clinical Course
• The median survival in primary MDS varies from 9 to 29 months.
• Overall, progression to AML occurs in 10% to 40% of individuals and is often accompanied by the appearance of additional clonal cytogenetic changes.
• Patients often succumb to the complications of thrombocytopenia (bleeding) and neutropenia (infection
Clinical Course
• The outlook is even grimmer in t-MDS, which has an overall median survival of only 4 to 8 months. Cytopenias tend to be more severe than in primary MDS, and progression to AML is often rapid.
Clinical Course
• Treatment options in MDS are limited.
• In younger patients, allogeneic bone marrow transplantation offers some hope for reconstitution of normal hematopoiesis and long-term survival.
• Older patients with MDS are treated supportively with antibiotics and blood product transfusions
Chronic Myeloproliferative Disorders/ Chronic Myelogenous Leukemia
General aspects of CMD
• In most disorders of this group, the neoplastic cell is a multipotent progenitor cell that is capable of giving rise to mature erythrocytes, platelets, granulocytes, monocytes.
• The only exception is chronic myelogenous leukemia, in which the pluripotent stem cell that gives rise to lymphoid and myeloid cells is affected.
General aspects of CMD
• As in AML, the neoplastic cells and their offspring flood the bone marrow and suppress residual normal progenitor cells;
• however, in the chronic myeloproliferative disorders, terminal differentiation is relatively unaffected. This combination leads to marrow hypercellularity and increased hematopoiesis, often accompanied by elevated peripheral blood counts.
Classification
• The four most common chronic myeloproliferative disorders (MPDs) are:
• (1) chronic myelogenous leukemia
• (2) polycythemia vera
• (3) essential thrombocytosis
• (4) primary myelofibrosis.

Classification
• All four have some similar features.:
• The neoplastic stem cells have the capacity to circulate and home to secondary hematopoietic organs, particularly the spleen, where they give rise to extramedullary hematopoiesis. As a result, all chronic MPDs cause varying degrees of splenomegaly.
Classification
• They also share the propensity to terminate in a spent phase characterized by marrow fibrosis and peripheral blood cytopenias.
• Further, all can progress over time to acute leukemia, but only chronic myelogenous leukemia (CML) does so invariably.

General aspects of CML
• Chronic myelogenous leukemia (CML) is a disease primarily of adults between the ages of 25 and 60 years, with the peak incidence in the fourth and fifth decades of life.
Pathophysiology
• CML is distinguished from other chronic MPDs by the presence of a distinctive molecular abnormality;
• namely, a translocation involving the BCR gene on chromosome 9 and the ABL gene on chromosome 22. The resultant BCR-ABL fusion gene directs the synthesis of a 210-kDa fusion protein with tyrosine kinase activity.
• .
Pathophysiology
• In more than 90% of CML cases, karyotyping reveals the so-called Philadelphia chromosome (Ph), which is created by a reciprocal (9;22)(q34;q11) translocation.
• However, in 5% to 10% of cases, the rearrangement is complex or cytogenetically cryptic; in such cases, other methods such as FISH RT-PCR can be used to detect the BCR-ABL fusion gene or transcript.
•
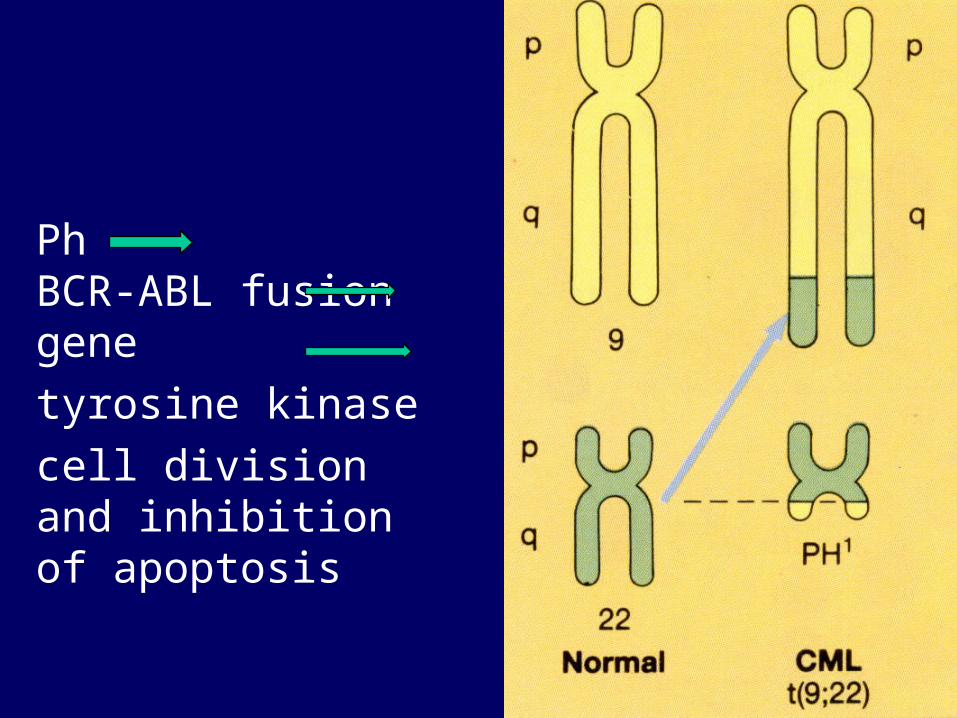
Ph BCR-ABL fusion gene
tyrosine kinase
cell division and inhibition of apoptosis
Pathophysiology
• Introduction of the BCR-ABL fusion gene into murine bone marrow cells gives rise to a syndrome resembling human CML; hence, its acquisition is considered to be a critical pathogenetic event.
Pathophysiology
• The activity of diverse tyrosine kinases is normally regulated by ligand-mediated dimerization, followed by the activation of multiple downstream pathways, which control cell survival and proliferation.
• Detailed molecular dissection has shown that BCR contributes a dimerization domain that promotes self-association of the BCR-ABL fusion protein, resulting in constitutive BCR-ABL autophosphorylation and activation of downstream pathways.
Pathophysiology
• The net effect of these events is cell division and inhibition of apoptosis, independent of ligand binding. Such autonomous triggering contributes to unregulated myeloproliferation
Pathophysiology
• In CML, multiple myeloid lineages, B lymphoid cells and possibly T lymphoid cells express the BCR-ABL fusion protein, indicating that the target of transformation is a pluripotent stem cell.
• For unknown reasons, the effect of the constitutively active BCR-ABL kinase early in the course of CML is evident mainly in granulocytic progenitors and, to a lesser degree, in megakaryocytic progenitors.
Morphology
• In contrast to normal bone marrow, which is usually about 50% cellular and 50% fat, CML marrows are usually 100% cellular, with maturing granulocytic precursors comprising most of the increased cellularity.
• Increased numbers of megakaryocytes, often including small dysplastic forms, are also frequently observed, whereas erythroid progenitors are usually present in normal or decreased numbers.
Morphology
• A characteristic finding is the presence of scattered storage histiocytes with wrinkled, green-blue cytoplasm (sea-blue histiocytes).
• Increased deposition of reticulin fibers is typical, but overt marrow fibrosis is rare at presentation.
Morphology
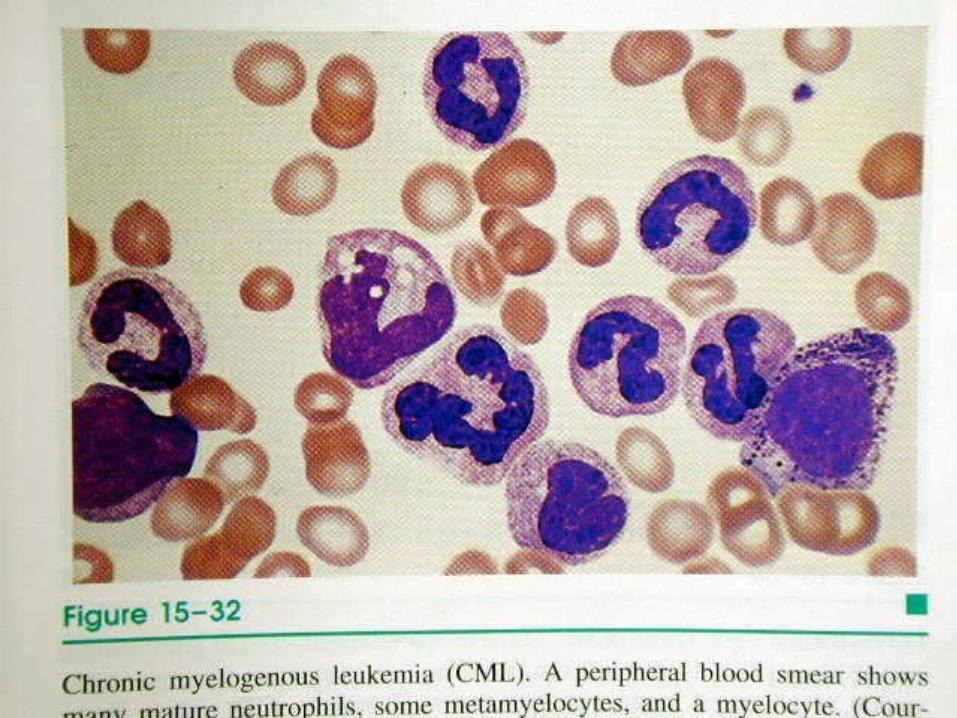
• Peripheral blood examination reveals a marked leukocytosis, often exceeding 100,000 cells per mm3. The circulating cells are predominantly neutrophils, metamyelocytes, and myelocytes, with less than 10% myeloblasts.
• Peripheral blood eosinophilia and basophilia are also common, and up to 50% of patients have thrombocytosis early in the course of their disease.
Morphology
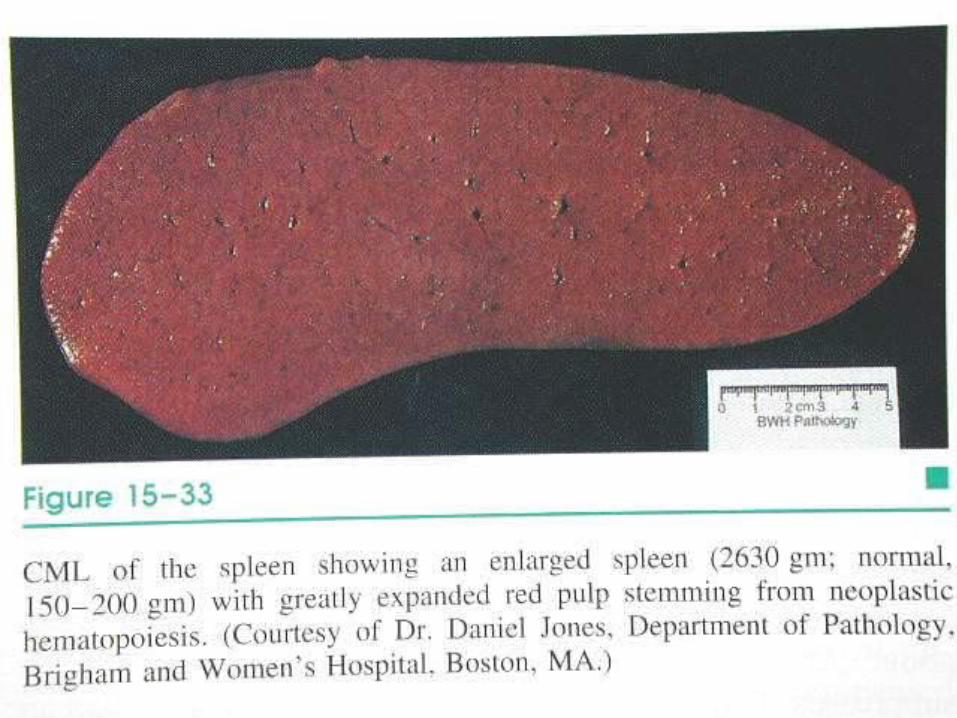
• Neoplastic extramedullary hematopoiesis within the splenic red pulp produces marked splenomegaly , often complicated by focal infarction. Extramedullary hematopoiesis can also lead to hepatomegaly and mild lymphadenopathy.

Clinical Features
• The onset of CML is insidious.
• Mild-to-moderate anemia and hypermetabolism due to increased cell turnover lead to easy fatigability, weakness, weight loss, and anorexia.
• Sometimes the first symptom is a dragging sensation in the abdomen caused by the extreme splenomegaly, or acute onset of left upper quadrant pain due to splenic infarction.
Clinical Features
• CML is best differentiated from other chronic myeloproliferative disorders by detection of the BCR-ABL fusion gene, through either chromosomal analysis or PCR-based molecular tests.
Clinical Features
• The natural history of CML is one of slow progression, and even without treatment, a median survival of 3 years can be expected.
• After a variable period averaging 3 years, approximately 50% of patients enter an "accelerated phase," during which there is increasing anemia and thrombocytopenia and sometimes striking peripheral blood basophilia.
Clinical Features
• Additional clonal cytogenetic abnormalities, such as trisomy 8, isochromosome 17q, or duplication of the Ph, can also appear.
• Within 6 to 12 months, the accelerated phase terminates in a picture resembling acute leukemia (blast crisis).
• In the remaining 50%, blast crises occur abruptly without an intermediate accelerated phase.
Clinical Features
• In 70% of blast crises, the blasts have the morphologic and cytochemical features of myeloblasts, whereas in most of the remainder, the blasts contain the enzyme TdT and express early B-lineage markers such as CD10 and CD19. Rarely, the blasts resemble precursor T cells.
• These observations further support the notion that the target cell for transformation is a pluripotent stem cell.
Clinical Features
• Understanding of the molecular pathogenesis of CML has led to the introduction of drugs that inhibit the BCR-ABL kinase, which induce complete hematologic remissions in more than 90% of patients.
• However, BCR-ABL inhibitors suppress but do not extinguish the CML clone and, as a result, may not prevent progression to blast crisis.
Clinical Features
• Moreover, while patients in blast crisis initially respond to BCR-ABL kinase inhibitors, they recur rapidly with refractory disease.
• For these reasons, allogeneic bone marrow transplantation, which is most effective when performed in the stable phase, is the favored treatment in younger patients. Of those with a suitable donor, about 75% are cured.
Summary of CMLSummary of CML
• Differentiation of leukemic cells is Differentiation of leukemic cells is relatively relatively maturemature,while ,while myeloblasts myeloblasts increase only slightlyincrease only slightly. .
• Marked elevation of the leukocyte of the leukocyte count in peripheral blood count in peripheral blood
• Myelocytic leukemic cells Myelocytic leukemic cells infiltrateinfiltrate in in sinusoidssinusoids of the liver and spleenof the liver and spleen
• extreme hepatosplenomegaly extreme hepatosplenomegaly
• slow onset, slow progression slow onset, slow progression
finally finally blast crisisblast crisis
• PhPh11 chromosome chromosome: abnormal : abnormal chromosome translocation t(9;22)chromosome translocation t(9;22)
Summary of CMLSummary of CML
Neoplastic Proliferations of White Cells
• Malignant proliferative diseases constitute the most important disorders of white cells.
• These diseases can be classified into several categories:
• 1. Lymphoid neoplasms (next lecture)
• 2. Myeloid neoplasms (finished)
• 3. Langerhans cell histiocytosis
General aspects of histiocytoses
• The term histiocytosis is an "umbrella" designation for a variety of proliferative disorders of dendritic cells or macrophages.
• Some, such as the rare "histiocytic" lymphomas, are clearly malignant, whereas others, such as reactive proliferations of macrophages in lymph nodes, are clearly benign.
General aspects of histiocytoses
• Between these two extremes is a small cluster of conditions characterized by proliferation of a special type of immature dendritic cell (DC) called the Langerhans cell.
• In most instances, these proliferations are monoclonal and therefore likely to be neoplastic in origin.
General aspects of histiocytoses
• The distribution of neoplastic DCs in lymphoid tissues and viscera, characteristic of these disorders, is likely attributable to aberrant expression of chemokine receptors.
• Whereas normal, skin resident DCs express CCR6, their neoplastic counterparts co-express CCR6 and CCR7, and this allows the abnormal DCs to migrate into tissues that express the relevant chemokines-CCL20 in skin and bone (the ligand for CCR6) and CCL19 and 21 in lymphoid organs (ligands for CCR7).
Classification
• Langerhans cell histiocytosis presents as three clinicopathologic entities:
1.Multifocal multisystem Langerhans cell histiocytosis (Letterer-Siwe disease)
2.Unifocal and multifocal unisystem Langerhans cell histiocytoses (eosinophilic granuloma)
3.Pulmonary Langerhans cell histiocytosis

•Eosinophilic granuloma,
•Multifocal langerhans cell histiocytosis
•Letterer-siwe disease
Langerhans cell histiocytosis
Benign Malignant
Classification
Clinicopathology
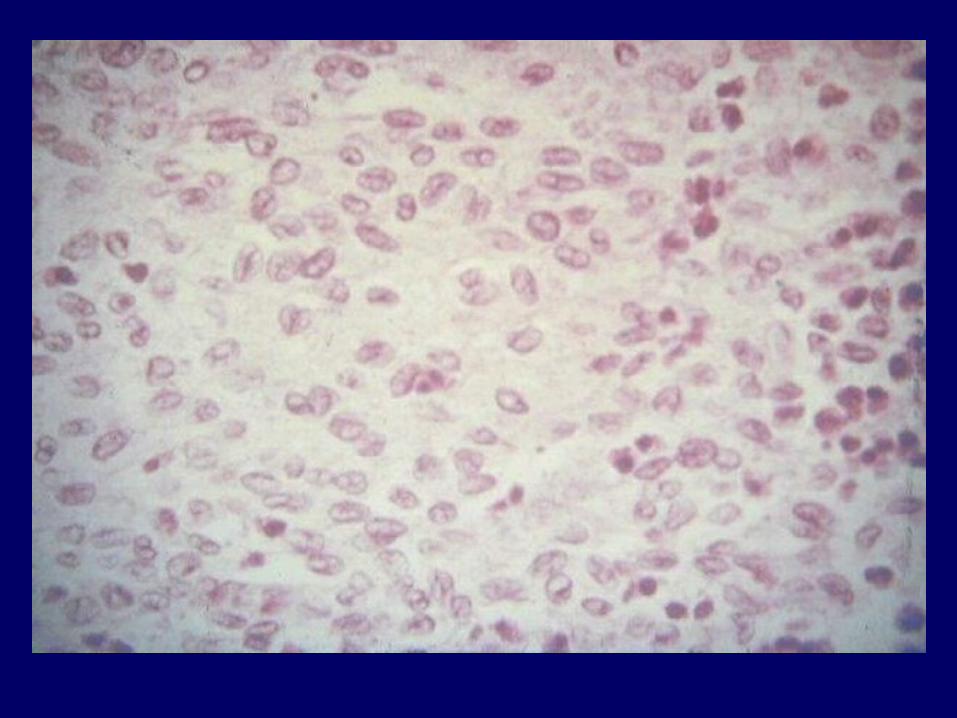
• 1. Multifocal multisystem Langerhans cell histiocytosis (Letterer-Siwe disease) occurs most frequently before 2 years of age but occasionally affects adults.
• A dominant clinical feature is the development of cutaneous lesions resembling a seborrheic eruption, which is caused by infiltrates of Langerhans cells over the front and back of the trunk and on the scalp.

seborrheic eruption
which is caused by infiltrates of Langerhans cells over the front and back of the trunk and on the scalp

cutaneous lesions
Clinicopathology
• Most of those affected have concurrent hepatosplenomegaly, lymphadenopathy, pulmonary lesions, and, eventually, destructive osteolytic bone lesions. Extensive infiltration of the marrow often leads to anemia, thrombocytopenia, and predisposition to recurrent infections such as otitis media and mastoiditis.
• The course of untreated disease is rapidly fatal. With intensive chemotherapy, 50% of patients survive 5 years.
Clinicopathology
• 2. Unifocal and multifocal unisystem Langerhans cell histiocytoses (eosinophilic granuloma) are characterized by expanding, erosive accumulations of Langerhans cells, usually within the medullary cavities of bones.
• Histiocytes are variably admixed with eosinophils, lymphocytes, plasma cells, and neutrophils.
Clinicopathology
• The eosinophilic infiltrate is usually prominent but is sparse in a subset of cases.
• Virtually any bone in the skeletal system can be involved, most commonly the calvarium, ribs, and femur. Less commonly, unisystem lesions of identical histology arise in the skin, lungs, or stomach.
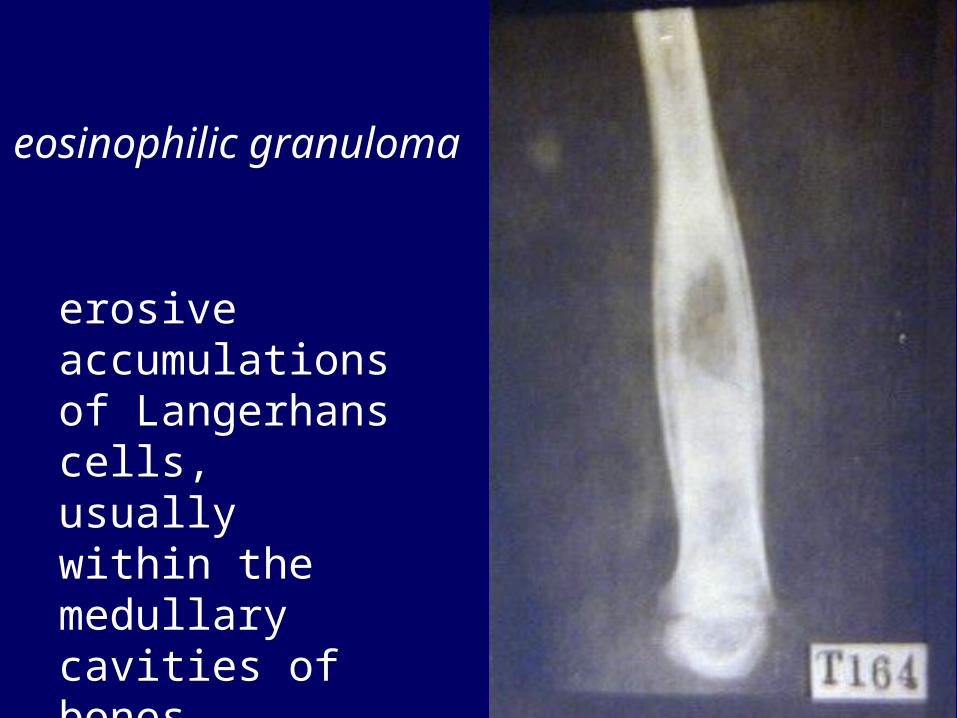
erosive accumulations of Langerhans cells, usually within the medullary cavities of bones.
eosinophilic granuloma
Clinicopathology
• Unifocal lesions usually affect the skeletal system in older children or adults.
• They can be asymptomatic, or they can cause pain, tenderness, and, in some instances, pathologic fractures.
• This is an indolent disorder that can heal spontaneously or be cured by local excision or irradiation.
Clinicopathology
• Multifocal unisystem Langerhans cell histiocytosis usually affects young children, who present with multiple erosive bony masses that sometimes expand into adjacent soft tissue.
• In about 50% of patients, involvement of the posterior pituitary stalk of the hypothalamus leads to diabetes insipidus.
Clinicopathology
• The combination of calvarial bone defects, diabetes insipidus, and exophthalmos is referred to as the Hand-Schuller-Christian triad.
• Many patients experience spontaneous regression; others can be treated successfully with chemotherapy.
Clinicopathology
• 3. Pulmonary Langerhans cell histiocytosis represents a special category of disease most often seen in adult smokers.
• It can regress spontaneously on cessation of smoking and usually comprises a polyclonal population of Langerhans cells, suggesting it is a reactive hyperplasia rather than a true neoplasm.
splenomegaly
Normal spleen• The spleen is to the circulatory system as the lymph
nodes are to the lymphatic system. Among its functions are filtration from the bloodstream of all foreign matter, including obsolescent and damaged blood cells, and participation in the immune response to blood-borne antigens.
• Designed ingeniously for these functions, the spleen is a major repository of mononuclear phagocytic cells in the red pulp and of lymphoid cells in the white pulp.
Normal spleen
• Normally, in the adult, it weighs about 150 gm and measures some 12 cm in length, 7 cm in width, and 3 cm in thickness.
• It is enclosed within a thin, glistening, slate-gray connective tissue capsule, through which dusky red, friable splenic parenchyma is seen.

Normal spleen
• The cut surface of the spleen is dotted with gray specks: the splenic, or white pulp follicles. The white pulp consists of aggregates of lymphoid cells that surround medium-sized splenic arteries.
• A cross-section of such an artery reveals an eccentric collar of T lymphocytes, the so-called periarteriolar lymphatic sheath.
Normal spleen
• At intervals, this lymphatic sheath expands, usually on one side of the artery, to form lymphoid nodules composed principally of B lymphocytes.
• On antigenic stimulation, typical germinal centers form within these B-cell areas. Eventually, the arterial system terminates in fine penicilliary arterioles enclosed within only a thin mantle of lymphocytes, which disappears entirely as these vessels enter the red pulp.
Normal spleen
• The red pulp of the spleen is traversed by numerous thin-walled vascular sinusoids, separated by the splenic cords.
• The endothelial lining of the sinusoid is of the open or discontinuous type, providing passage of blood cells between the sinusoids and cords.
Normal spleen
• The splenic cords are spongelike and consist of a labyrinth of macrophages loosely connected through long dendritic processes to create both a physical and a functional filter through which blood slowly seeps.
Normal spleen
• As it traverses the red pulp, the blood likely takes two routes to reach the splenic veins. Some flows through capillaries into the splenic cords, from which it then gradually filters out into the surrounding splenic sinusoids to reach the veins; this is the so-called open circulation or slow compartment.
Normal spleen• In the other pathway, blood passes directly from the
capillaries to the splenic veins. This "closed circuit" is understandably the compartment with the more rapid blood flow.
• Although only a small fraction of the blood entering the spleen at any given time pursues the "open" route, during the course of a day, the entire blood volume passes through the filtration beds of the splenic cords, where it is "screened" by the remarkably sensitive and effective sinusoidal macrophages.
Splenic function
• Most anatomic alterations of the spleen are enlargements caused by systemic disorders that enhance some aspect of normal splenic function.
• These functions can be segregated into four categories
Splenic function
• 1. Removal of unwanted elements from the blood by splenic phagocytosis in the cords is a major function. As you know, 1/120th of all red cells are removed daily by the phagocytes of the mononuclear phagocyte system. This amounts to removal of 2 × 10∼ 11 red cells per day in a 70-kg adult, about 50% of which are phagocytosed in the spleen.
Splenic function
• Splenic phagocytes are also remarkably efficient in culling damaged red cells and leukocytes, red cells rendered foreign by antibody coating, and abnormal red cells encountered in several hereditary hemolytic anemias (e.g., hereditary spherocytosis).
Splenic function
• Red cells undergo extreme deformation during passage from the cords into the sinusoids.
• In conditions in which red cell elasticity is decreased, red cells become entrapped within the cords and are more readily phagocytosed by cordal macrophages.
Splenic function
• Splenic phagocytes also actively remove other particulate matter from the blood, such as bacteria, cell debris, and abnormal macromolecules produced in some inborn errors of metabolism (e.g., Gaucher disease, Niemann-Pick disease).
Splenic function
• 2. The spleen is a major secondary organ of the immune system.
• Dendritic cells in the periarterial lymphatic sheath trap antigens and present them to T lymphocytes.
• T and B cells interact at the edges of white pulp follicles, leading to the generation of antibody-secreting plasma cells, which are found mainly within the sinuses of the red pulp.
Splenic function
• 3. The spleen can be a source of hematopoietic cells.
• Splenic hematopoiesis normally ceases before birth, but in severe anemia, extramedullary splenic hematopoiesis can be reactivated.
Splenic function
• 4. Because of its rich vascularization and sluggish circulation, the spleen sequesters a portion of the formed blood elements.
• In animals with contractile spleens, such as the dog, these elements can be mobilized and thus constitute a reserve pool.
• The human spleen lacks contractility, however, limiting its function in this regard.
Splenic function
• In humans, the normal spleen contains only about 30 to 40 mL of red cells, but with splenomegaly, this is greatly increased.
• The normal spleen also harbors approximately 30% to 40% of the total platelet mass in the body. With splenomegaly, up to 80% to 90% of the total platelet mass can be sequestered in the interstices of the red pulp, producing thrombocytopenia.
• Similarly, the enlarged spleen can trap a sufficient number of white cells to induce leukopenia.
Splenic function• Despite the diverse functions of the spleen, deficient
splenic function due to splenectomy or autoinfarction has a single major clinical manifestation: increased susceptibility to disseminated infection with encapsulated bacteria such as pneumococcus, meningococcus, and Haemophilus influenzae.
• The reduced filtering and antibody production functions of the spleen probably contribute to these infections, which often cause fatal sepsis in asplenic individuals
Pathology
• As the largest unit of the mononuclear phagocyte system, the spleen is involved in all systemic inflammations, generalized hematopoietic disorders, and many metabolic disturbances.
• In each of these disorders, the spleen undergoes enlargement, which is the major manifestation of disorders of this organ.
• It is rarely the primary site of disease.
Splenomegaly
• Splenic enlargement can be an important diagnostic clue to the existence of an underlying disorder, but it can itself also cause problems.
• When sufficiently enlarged, the spleen causes a dragging sensation in the left upper quadrant and, through pressure on the stomach, discomfort after eating.
Splenomegaly
• In addition, its enlargement can lead to sequestration of significant numbers of blood elements. This gives rise to a syndrome known as hypersplenism.
Splenomegaly
hypersplenism is characterized by the triad of (1) splenomegaly;
(2) anemia, leukopenia, thrombocytopenia, or any combination of these, in association with hyperplasia of the marrow precursors of the deficient cell type;
(3) correction of the blood cytopenia(s) by splenectomy.
Splenomegaly
The likely cause of the cytopenias in this syndrome is increased sequestration of formed elements and the consequent enhanced phagocytosis by the splenic macrophages.
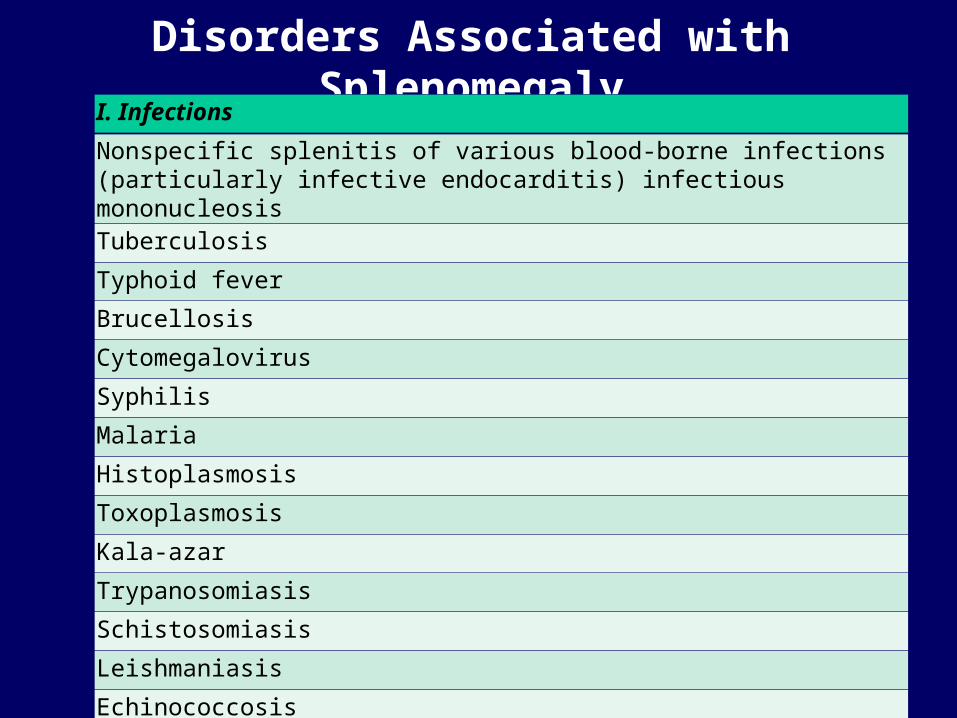
Disorders Associated with SplenomegalyI. Infections
Nonspecific splenitis of various blood-borne infections (particularly infective endocarditis) infectious mononucleosisTuberculosis
Typhoid fever
Brucellosis
Cytomegalovirus
Syphilis
Malaria
Histoplasmosis
Toxoplasmosis
Kala-azar
Trypanosomiasis
Schistosomiasis
Leishmaniasis
Echinococcosis
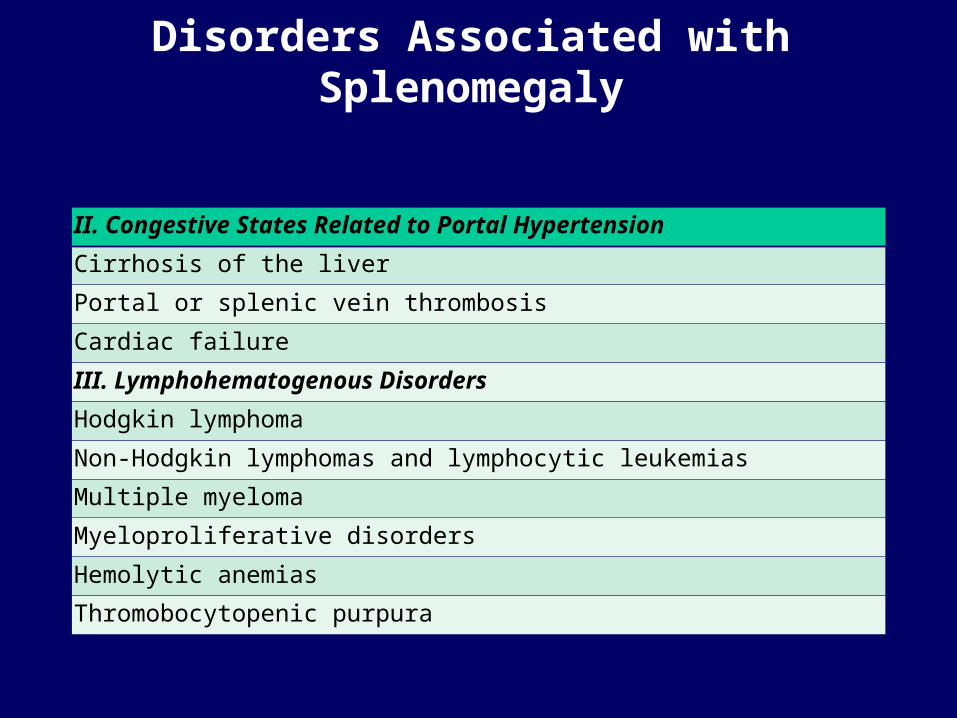
Disorders Associated with Splenomegaly
II. Congestive States Related to Portal Hypertension
Cirrhosis of the liver
Portal or splenic vein thrombosis
Cardiac failure
III. Lymphohematogenous Disorders
Hodgkin lymphoma
Non-Hodgkin lymphomas and lymphocytic leukemias
Multiple myeloma
Myeloproliferative disorders
Hemolytic anemias
Thromobocytopenic purpura
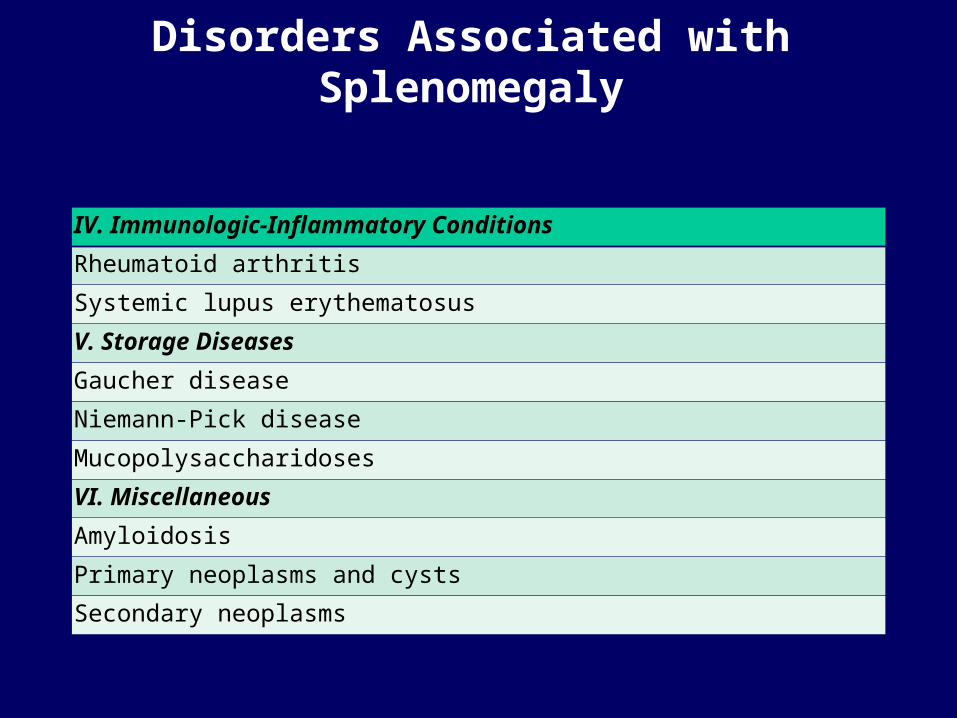
Disorders Associated with Splenomegaly
IV. Immunologic-Inflammatory Conditions
Rheumatoid arthritis
Systemic lupus erythematosus
V. Storage Diseases
Gaucher disease
Niemann-Pick disease
Mucopolysaccharidoses
VI. Miscellaneous
Amyloidosis
Primary neoplasms and cysts
Secondary neoplasms
Key point of this class
• 1. Philadelphia chromosome
• 2. Morphology of CML
• 3. Eosinophilic granuloma Clinicopathology
• 4. HypersplenismSplenomegaly
• 5. Disorders Associated with Splenomegaly
Related Documents











