9 9 Diseases of the Ear, Diseases of the Ear, Nose, and Throat Nose, and Throat Chapter Outline DISEASES OF THE EAR, NOSE, AND THROAT THE EAR: ANATOMY AND PHYSIOLOGY DIAGNOSTIC PROCEDURES IN DISORDERS OF THE EAR INFECTIONS OF THE OUTER AND MIDDLE EAR Otitis Externa (Swimmer’s Ear) Otitis Media DISORDERS OF THE INNER EAR Tinnitus Vertigo Hearing Loss THE NOSE: ANATOMY AND PHYSIOLOGY DIAGNOSTIC PROCEDURE IN DISORDERS OF THE NOSE DISEASES OF THE NOSE Coryza (Common Cold) Allergic Rhinitis (Hay Fever) Sinusitis (Rhinosinusitis) Epistaxis (Nosebleed) (Outline continued on next page) 127 LEARNING OBJECTIVES Upon completion of this chapter, you should be able to • describe the basic anatomy and physiol- ogy of the ears, nose, and throat; • explain diagnostic procedures and treat- ments used for diseases of the ears, nose, and throat; • classify common diseases of the ears, nose, and throat by their signs, symptoms, and treatment.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

99Diseases of the Ear, Diseases of the Ear,
Nose, and ThroatNose, and Throat
Chapter Outline
DISEASES OF THE EAR, NOSE, AND THROAT
THE EAR: ANATOMY AND PHYSIOLOGY
DIAGNOSTIC PROCEDURES IN DISORDERSOF THE EAR
INFECTIONS OF THE OUTER AND MIDDLE EAROtitis Externa (Swimmer’s Ear)Otitis Media
DISORDERS OF THE INNER EARTinnitusVertigoHearing Loss
THE NOSE: ANATOMY AND PHYSIOLOGY
DIAGNOSTIC PROCEDURE IN DISORDERSOF THE NOSE
DISEASES OF THE NOSECoryza (Common Cold)Allergic Rhinitis (Hay Fever)Sinusitis (Rhinosinusitis)Epistaxis (Nosebleed)
(Outline continued on next page)
127
LEARNING OBJECTIVES
Upon completion of this chapter, youshould be able to
• describe the basic anatomy and physiol-ogy of the ears, nose, and throat;
• explain diagnostic procedures and treat-ments used for diseases of the ears, nose,and throat;
• classify common diseases of the ears,nose, and throat by their signs, symptoms,and treatment.

DISEASES OF THE EAR, NOSE, AND THROAT(continued)
THE THROAT: ANATOMY AND PHYSIOLOGY
DIAGNOSTIC PROCEDURES IN DISORDERSOF THE THROATAcute Pharyngitis (Sore Throat)Obstructive Sleep Apnea (OSA)
QUESTIONS FOR STUDY AND REVIEW
128 • Human Diseases

DISEASES OF THE EAR, NOSE, AND THROAT
The ears, nose, and throat are adjacent to oneanother anatomically, similar in histologic structure,and subject to many of the same diseases. Diseases,injuries, and abnormalities of the ear, nose, andthroat (ENT) are the special field of the otorhino-laryngologist. This chapter briefly surveys the morecommon disorders to which these parts of the bodyare subject. If you encounter unfamiliar terms, lookthem up in the Glossary or the Index.
THE EAR
ANATOMY AND PHYSIOLOGY
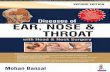
Each ear has three parts (See Figure 7):
1. The outer ear, consisting of the pinna (thecartilaginous appendage on either side of the head,which collects sound waves like a funnel) and theexternal auditory meatus (a tube that conductssound waves from the pinna to the middle ear). Themeatus is lined with skin that secretes cerumen (ear-wax), a mildly antimicrobial substance that trapsdust and other particulate foreign material.
2. The middle ear, a cavity in the temporal boneseparated from the external auditory meatus by thetympanic membrane, which vibrates in response tosound waves and imparts the vibration to a series ofvery small bones (malleus, incus, and stapes), whichin turn transmit them to the inner ear.
3. The inner ear, consisting of the cochlea (anorgan shaped like a snail shell, in which sound vibra-tions are converted to nerve impulses to be sentthrough the eighth cranial, or vestibulocochlear,
Figure 7 Ear
Reprinted by permission of Pearson Education, Inc., from Martini & Bartholomew, Structure & Function of the Human Body (Prentice Hall, 1999)
Chapter 9 • Ear, Nose, and Throat • 129

130 • Human Diseases
nerve) and the vestibular system (the organ of bal-ance, containing minute position sensors in a fluidmedium, which send information about head posi-tion to the balance center in the brain, also throughthe eighth cranial nerve).
The middle ear communicates with the pharynxby a minute passage called the auditory (eustachian)tube, which serves to equalize air pressure betweenthe middle ear and the atmosphere (see box). It alsocommunicates with epithelium-lined air cells withinthe skull, called mastoid air cells.
DIAGNOSTIC PROCEDURES IN DISORDERS OF THE EAR
Inspection and palpation of the pinna.
Otoscopy: Inspection of the external auditorymeatus and tympanic membrane with an otoscope,an instrument that directs light into the ear througha conical speculum, and is equipped with a magnify-
ing lens; mobility of the tympanic membrane can beassessed when the subject swallows or performs theValsalva maneuver (or when, in children, the exam-iner blows a puff of air into the ear with a rubberbulb attached to the otoscope).
Measurements of hearing: (1) simple tests withticking watch or tuning fork; (2) audiography, a pre-cise measurement of the faintest loudness (in deci-bels) that the subject can hear, each being ear testedseparately at each of several pitches (for example,250, 500, 1000, 2000, 3000, 4000, 6000, and 8000Hz); this can be performed by a technician withcarefully calibrated testing equipment, or by auto-mated machinery activated by the subject; (3) moreelaborate testing of the subject’s ability to discrimi-nate spoken words.
Weber test: A vibrating tuning fork placedfirmly against a bony surface of the head at themidline sends vibrations through the bones of theskull. These should be heard equally in the twoears; if there is hearing loss due to blockage of theexternal auditory meatus or to injury or disease ofthe middle ear, the tone of the fork will be heardlouder in the affected ear; in hearing loss due to dam-age to the inner ear or acoustic nerve, however, thetone will be heard louder in the more normal ear.
Rinne test: The sound of a vibrating tuning forkpositioned so that the tines are near the pinna (airconduction) should be heard by the subject evenafter the sound sensed when the shank of the tuningfork is placed on the mastoid process behind the ear(bone conduction) can no longer be heard; whenbone conduction is heard longer than air conduc-tion in an ear with reduced hearing, the hearing lossis due to obstruction of the meatus or disease of themiddle ear.
Tympanocentesis: Puncture of the tympanicmembrane and withdrawal of fluid from the middleear for examination, including culture.
Pneumotympanometry: Assessment of the mo-bility of the tympanic membrane by applying pres-sure to its outer surface with a device fitting tightlyin the external meatus.
The auditory tube between the middle earand the pharynx was discovered by Bartolo-meo Eustachio (1524-1574), an Italian anat-omist who also made important studies of theheart, the kidney, and the nervous system.
It has been suggested that when WilliamShakespeare wrote Hamlet, he had in mind thethen recent discovery of this passage. In Act I,Scene 5, the ghost of Hamlet’s father tellsHamlet how he was murdered by his brotherClaudius, who poured “juice of cursed hebona. . . in the porches of my ears.”
According to Nomina Anatomica (NA)and Terminologia Anatomica (TA), the nameof this tube is tuba auditoria (or auditiva), usu-ally rendered auditory tube in English.
Many health professionals nonethelesscling to the traditional name, eustachian tube,and most of them pronounce it with the softFrench ch sound (as in champagne) ratherthan the more appropriate hard Italian ch (asin Chianti).

INFECTIONS OF THE OUTER AND MIDDLE EAR
Otitis Externa (Swimmer’s Ear)Infection of the external auditory meatus.Causes: Infection with bacteria (Proteus, Pseudo-
monas) and sometimes fungi (Aspergillus). Predis-posing causes include water exposure (swimming,showering), excessive cerumen, mechanical trauma(probing with paperclip), foreign body (cotton,pencil eraser), diabetes mellitus, and immune com-promise.
History: Earache, itching in the external audi-tory meatus, purulent discharge. Hearing loss if themeatus is occluded by swelling or exudate.
Physical Examination: Redness and swelling ofthe meatus, sometimes with complete occlusion;purulent exudate, perhaps with excessive cerumenor foreign body visible. Tenderness on manipulationof the pinna.
Course: Generally benign, but in diabetes melli-tus and AIDS an external ear infection may resist con-servative treatment and become chronic, perhapsinvading the skull or brain, with resulting neurologicdamage.
Treatment: After gentle cleansing and removal ofany foreign material, cerumen, or exudate, topicalantibiotics (ear drops), often with hydrocortisone tocombat local inflammation, are instilled several timesa day. Sometimes a gauze wick is inserted to facilitatepenetration of ear drops when edema of the meatusis extreme. In invasive infections, intravenous antibi-otics and even surgery may be required.
Otitis MediaBacterial infection of the middle ear and adjoin-
ing mastoid air cells.Cause: Infection by Streptococcus pneumoniae,
Haemophilus influenzae, Streptococcus pyogenes, andother bacteria. Otitis media commonly occurs as asequel to a viral upper respiratory infection. Ob-struction of the auditory tube by edema leads topressure changes within the middle ear and secre-tion of mucus and serous fluid, which becomesinfected by bacteria already present in the tissues.Otitis media is often bilateral. It is commoner ininfants and small children than in adolescents andadults, accounting for one-third of all pediatricoffice visits.
History: Pain and pressure in one or both ears,hearing loss, sometimes fever.
Physical Examination: Redness of the tympanicmembrane, sometimes with formation of bullae.Immobility of the tympanic membrane, reflectingmalfunction of the auditory tube. Occasionallybulging of the membrane. If spontaneous ruptureoccurs, blood or purulent exudate in the externalauditory meatus.
Course: It is estimated that 20-80% of all cases ofotitis media will resolve spontaneously without treat-ment. When there is fever or severe pain, antibiotictreatment is usually prescribed because of the risk ofserious complications in a few patients. Neglect ofthe infection, its failure to respond to standard ini-tial treatment, or a series of recurrent infections canlead to chronic otitis media, typically due to differ-ent organisms (Proteus, Pseudomonas, staphylococci)than acute infection. Complications of chronic otitismedia include spontaneous rupture of the tympan-ic membrane, with chronic purulent drainage;destruction of the bones within the middle ear thattransmit sound; invasion of mastoid air cells (mas-toiditis), skull bones, and even the central nervoussystem by infection; formation of cholesteatoma, abenign but locally invasive growth of the tympanicmembrane caused by prolonged negative pressure(partial vacuum) in the middle ear. Chronic otitismedia can lead to permanent conductive hearingloss and, in small children, speech defects becauseof inability to hear speech sounds properly.
Treatment: In the absence of fever and severepain in patients over age 2, analgesics and observa-tion are preferred to antibiotic treatment. For se-lected patients, systemic antibiotics (amoxicillinwith or without clavulanic acid, erythromycin,trimethoprim-sulfamethoxazole), decongestants,analgesics. If tympanic membrane rupture threatens,myringotomy (surgical puncture of the membrane,with release of pus). In children with recurrent orrefractory infections, polyethylene tubes may beplaced in the tympanic membrane(s) to aerate themiddle ear(s) and allow for escape of purulentsecretion. Cholesteatoma and mastoiditis are treatedsurgically. Chronic perforation of the tympanicmembrane requires surgical repair (tympanoplasty).
Chapter 9 • Ear, Nose, and Throat • 131

132 • Human Diseases
DISORDERS OF THE INNER EAR
TinnitusPerception of abnormal sounds in the ear(s) or
head. When pulsatile (simultaneous with heart-beat), it may result from vascular disease (arterialstenosis, aneurysm). Tinnitus is generally a hum-ming or squealing noise heard constantly or inter-mittently in one or both ears, especially at nightwhen external sounds are at a minimum. It is gen-erally due to degenerative disease of the inner ear,and frequently accompanies sensorineural hearingloss (discussed below). Common causes are exces-sive noise exposure and certain medicines. Aspirinand other salicylates at higher doses cause tinnituslasting only as long as they remain in the body.Other drugs (certain antibiotics) can cause perma-nent tinnitus. Treatment of tinnitus is generallyunsatisfactory but includes masking with othersounds (music, “static” on a radio).
VertigoA sense of motion (spinning, falling, floor tip-
ping) when no such motion is occurring.Causes: Labyrinthitis, often following respira-
tory infection and hence often called viral. De-generative changes in the balance-sensing mecha-nism of the inner ear. Increased pressure within theendolymphatic sac (Ménière disease). Vascular orneoplastic disease of the inner ear or temporal lobeof the cerebral cortex. Diplopia, head injury, multi-ple sclerosis, drugs, alcohol.
History: A feeling of spinning or falling to oneside, or a sense that the floor is tipping or rotating,coming on suddenly, often with head movement,and lasting seconds, minutes, hours, days, weeks, ormonths. When severe, vertigo may make it impossi-ble for the patient to stand or walk, and may beaccompanied by nausea and vomiting. There mayalso be tinnitus and hearing loss.
Physical Examination: May be essentially nor-mal. The Romberg test (patient standing with eyesclosed) may indicate inability to maintain equilib-rium. Eyes may show nystagmus.
Treatment: May be limited to treatment of theunderlying cause. In Ménière disease, salt restrictionand diuretic therapy may help by reducing the pres-sure of the endolymph. Medicines such as meclizineand dimenhydrinate may diminish or abolish vertigo
temporarily. In some cases of positional vertigo,head manipulation can reduce symptoms by pro-moting reorientation of the balance mechanism.
Hearing LossReduction, often permanent, in the acuity of
hearing in one or both ears. Hearing loss is dividedinto three types depending on the location of theabnormality.
Conductive hearing loss due to disease or abnor-mality in the outer or middle ear: cerumenimpaction, otitis media with effusion, hardening ofthe tympanic membrane (otosclerosis), injury or dis-ease of the ossicles.
Sensory hearing loss due to disease of thecochlea: acoustic trauma, ototoxicity (aminoglyco-sides, loop diuretics, cisplatin), aging.
Neural hearing loss due to eighth nerve lesionsor cerebrovascular disease.
Hearing loss is assessed by audiometry and theWeber and Rinne tests. Treatment is that of theunderlying cause, if possible.
Generally no treatment is effective.
THE NOSE
ANATOMY AND PHYSIOLOGY
The external nose is supported by a frameworkof cartilage and covered by skin. The nostrils (ante-rior nares) open into paired passages lined withmucous membrane, which is rich in serous andmucous glands and blood vessels. The lining mem-brane of these passages is closely attached to convo-luted ridges of bone called turbinates (three oneach side), which increase the surface area of mem-brane that is exposed to inspired air. Adjacent to thenasal passages, and communicating with them bynarrow orifices, are the paranasal sinuses. These arecavities within the bones of the skull, somewhat vari-able in size and shape, and lined with mucosa likethat of the nose. The nasal passages end at thechoanae, or posterior nares, where they enter thenasopharynx, the uppermost part of the pharyngealcavity. The nasal passages warm and moisturizeinspired air, and the mucus film lining them trapsparticulate matter in the air.

itching, sneezing (often many times in a row), anditching and watering of the eyes. Symptoms mayoccur consistently at certain seasons (spring, fall) or,especially when due to house dust, may be perennial.
Physical Examination: Watery, red eyes. Pale orbluish, markedly swollen nasal mucosa. Nasal polyps(massive overgrowths of chronically inflamedmucosa) may be present.
Diagnostic Tests: Nasal smear shows eosinophils.Skin testing or RAST (radioallergosorbent testing)can identify causative allergens.
Treatment: Decongestants, antihistamines, nasalcorticosteroid spray. Avoidance of known allergenswhen possible. Use of air filters as appropriate.Continued administration of desensitizing antigensoften markedly reduces symptoms.
Sinusitis (Rhinosinusitis)Infection of one or more paranasal sinuses.Cause: Involvement of the paranasal sinuses
often occurs along with any type of rhinitis, includ-ing particularly the common cold. Swelling of thenasal mucosa leads to blockage of the sinus open-ings, with accumulation of secretions within thesinuses affected. Persons with allergic rhinitis may besubject to recurring episodes of sinusitis due tochronic blockage of sinus openings (ostia). Acutesinusitis is nearly always viral. Recurrent or persistentobstruction to sinus drainage can lead to chronicsinusitis with secondary bacterial infection.
History: Pressure or pain in one or more sinuscavities, often aggravated by bending forward. Painmay be manifested as a severe headache or mayradiate into the teeth. Purulent or bloody nasal orpostnasal discharge may be present. Occasionallyfever, chills, and malaise.
Physical Examination: Edema and erythema ofnasal mucosa. Purulent discharge in nasal passagesor oropharynx (postnasal drip).
Diagnostic Tests: In chronic sinusitis, x-ray orother diagnostic imaging shows thickening of sinusmembranes and often presence of fluid within cav-ities.
Treatment: Decongestant, analgesic. A shortcourse of nasal decongestant spray may help toopen and drain sinuses. Control of allergic compo-nent if present. When symptoms (severe, persistentpain) or clinical picture (fever, bloody discharge)suggests bacterial infection, an oral antibiotic(amoxicillin, trimethoprim-sulfamethoxazole) is
DIAGNOSTIC PROCEDURE IN DISORDERS OF THE NOSE
Direct inspection with nasal speculum orrhinoscope.
Posterior rhinoscopy: Inspection of posteriornares with angled mirror placed in the oropharynx.
Nasal smear: Examination of a stained smear ofscrapings from the nasal mucosa for evidence ofinfection (neutrophilic leukocytes) or allergy(eosinophilic leukocytes).
Culture of nasal secretions to identify bacterialpathogens.
Diseases of the Nose
Coryza (Common Cold)A common, mild rhinitis caused by viruses.Causes: Any of numerous viruses, which can be
spread readily from person to person. Risk of catch-ing cold may be heightened by exposure to severewinter weather (especially whole-body chilling), dry-ing of indoor air by heating systems, or crowdingindoors during the winter.
History: Headache, nasal stuffiness, runny nose,sneezing, throat irritation, malaise. Occasionallyfever, chills, anorexia, and muscle aching.
Physical Examination: Erythema and edema ofnasal mucosa. Temperature may be slightly elevated.
Course: Generally self-limited. Sometimescomplicated by sinusitis, otitis media, pharyngitis,bronchitis.
Treatment: Purely symptomatic. Oral deconges-tants are moderately effective. Aspirin, aceta-minophen, or ibuprofen relieve discomfort. Rest,fluids. Antihistamines do not decongest, antibioticsdo not kill cold viruses, and nasal decongestantsprays cause rebound congestion worse than thedisease.
Allergic Rhinitis (Hay Fever)A recurrent, often seasonal, inflammation of the
nasal mucous membrane caused by allergy toinhaled materials.
Causes: Sensitivity to pollens, grasses, moldspores, dust mites, animal dander, second-handcigarette smoke, and other inhalant allergens.
History: Recurrent or constant nasal conges-tion and irritation, with copious watery discharge,
Chapter 9 • Ear, Nose, and Throat • 133

prescribed. Chronic sinusitis may respond to pro-longed antibiotic therapy. Surgical procedures canbe used to correct anatomic lesions predisposing tosinusitis, or to improve drainage of a chronicallyinfected sinus.
Epistaxis (Nosebleed)Bleeding from the nose may be due to nasal
trauma, irritation of the mucosa by dust or dry air,upper respiratory infection or allergic rhinitis, orcoagulation defect. Treatment of acute nosebleed isby application of direct pressure and, if necessary,topical vasoconstrictor. If bleeding persists or recurs,cautery with silver nitrate or anterior nasal packingmay be necessary. Rarely bleeding comes from theposterior nares (usually in middle-aged or elderlypatients with hypertension or arteriosclerosis) andrequires a posterior nasal pack. Prevention of fur-ther nosebleeds may include use of lubricatingapplications to the mucosa, humidification of air,and avoidance of dusts and other irritants.
THE THROAT
ANATOMY AND PHYSIOLOGY
The throat, or pharynx, is a cavity lined withmucous membrane that conducts air from the noseand mouth into the trachea, and food and drink fromthe mouth into the esophagus. It consists of threeportions: the nasopharynx, on a level with the nasalpassages and communicating with them; the orophar-ynx, on a level with the mouth and communicatingwith it; and the hypopharynx or laryngopharynx,which lies below the oropharynx and gives entry tothe esophagus and the larynx. (See Figure 8.)
The tonsils and adenoids are masses of lym-phoid tissue surrounding the zone between themouth and the oropharynx. At the boundarybetween the oropharynx and the hypopharynx liesthe epiglottis, a flexible valve that closes the respira-tory passage during swallowing of food or drink.
The lining of the pharynx secretes mucus,which keeps the surface moist, traps inhaled parti-cles, and supplements the saliva as a lubricant forfood. Lymph glands in the front and back of theneck receive lymphatic drainage from the throatand adjacent structures.
DIAGNOSTIC PROCEDURES IN DISORDERS OF THE THROAT
Inspection of the throat with a focused light,often with the aid of a tongue depressor (tongueblade) to press the tongue out of the field of vision.
Palpation of cervical lymph glands and of masses,swellings, or other structures within the throat.
Throat culture to identify bacterial pathogens.Strep screen (faster than culture, but detects
only group A beta-hemolytic streptococci).Biopsy of masses or lesions suspected of being
malignant.X-ray or other imaging to identify foreign bod-
ies, masses, or abnormalities of the airway due toinjury or disease.
Acute Pharyngitis (Sore Throat)Acute inflammation of the throat due to infec-
tion.Cause: Usually viruses, including the Epstein-
Barr virus, which causes infectious mononucleosis(discussed in Chapter 3). Occasionally bacteria such
134 • Human Diseases
Figure 8 Pharynx
Reproduced with permission from Melloni’s Illustrated Medical Dictionary, 4th ed. (2002)

as Streptococcus pneumoniae and Group A beta-hemolytic Streptococcus pyogenes (“strep throat”), orfungi such as Candida. Infection with cold virusesmay predispose to bacterial infection. Sore throat ismore prevalent in cold weather.
History: Pain, irritation, or a sense of fullness orswelling in the throat, accentuated by swallowingand often radiating to the ears. Fever, painful glan-dular swelling in the neck.
Physical Examination: May be essentially nor-mal. Fever is often present. Edema and erythema ofthe oropharynx, often involving the tonsils, softpalate, and uvula, occur in most bacterial and manyviral throat infections. Severe infections, includingstreptococcal pharyngitis (strep throat) and infec-tious mononucleosis, cause formation of white orgray exudate (consisting of dead tissue, white bloodcells, and bacteria) on pharyngeal walls and espe-cially on the tonsils. A firmly adherent exudate ischaracteristic of Candida infection (thrush). Thepresence of vesicles or ulcers suggests viral infection(herpes simplex virus, coxsackievirus). Severe painand swelling may cause a hollow or “hot potato”voice, and may make swallowing virtually impossible,so that the patient drools to avoid swallowing saliva,and becomes dehydrated from lack of fluid intake.Extreme swelling may compromise the airway.Cervical lymph glands may be swollen and tender.Some strains of beta-hemolytic streptococci cause awidespread red rash (scarlet fever, scarlatina).
Diagnostic Tests: Throat culture or strep screenmay identify the causative organism. Blood studies(white blood cell count and differential, antistrep-tolysin O titer, heterophile antibodies) help to diag-nose strep throat and infectious mononucleosis.Smears or scrapings of exudate can confirm pres-ence of Candida.
Course: Viral sore throat runs its course within aweek or two. Occasionally it becomes complicatedby streptococcal infection, which may lead to acuterheumatic fever. It may also progress to otitis media,acute or chronic tonsillitis, or lower respiratoryinfection. Peritonsillar abscess (quinsy) is a severebacterial infection developing above and behindone tonsil and causing extreme pain and swelling,with deviation of the uvula away from the affectedside.
Treatment: Acute viral pharyngitis requires notreatment except analgesics, gargles, soothinglozenges, and perhaps a soft diet. Adrenal cortico-steroid may be administered orally or by injection forsevere pain and swelling. If streptococcal infection is
diagnosed, a 10-day course of an antibiotic known tobe able to eradicate streptococci (such as penicillinV, erythromycin, or cephalexin) is mandatory.Candidal oropharyngitis (thrush) is treated withtopical or systemic antifungal medicine. The treat-ment of peritonsillar abscess is surgical drainage.
Obstructive Sleep Apnea (OSA)A disorder in which breathing is repeatedly
interrupted during sleep by intermittent obstructionof the airway.
Cause: Lax, excessively bulky, or malformedpharyngeal tissues (soft palate, uvula, and sometimestonsils). Obesity, hypothyroidism, cigarette smoking,alcohol, and some medicines (particularly benzodi-azepines) are predisposing factors. The swallowingreflex may be impaired during sleep. The conditionis twice as common in men. Incidence increases withadvancing age.
History: Loud snoring and recurrent episodes ofapnea (respiratory arrest) during sleep followed bygasping inspiration with partial or complete arousal.The period of apnea may last for 10-120 seconds, andmay be accompanied by sinus bradycardia or atrio-ventricular block.
Physical Examination: The shape and caliber ofupper respiratory passages may be abnormal.
Diagnostic Tests: Polysomnography (continu-ous monitoring of heart rate, respiratory action andair flow, eye movements, and electroencephalogramduring sleep), supplemented by recording of chinmovements and arterial oxygen saturation.
Course: Nocturnal hypoxemia (deficiency ofoxygen in blood) and shallow, non-refreshing sleepmay lead to daytime lethargy, difficulties with mem-ory and concentration, and even personality changeand accident-proneness. About 15% of persons withOSA develop sustained pulmonary hypertension.
Treatment: Weight loss, smoking cessation,avoidance of alcohol and benzodiazepines. Anappliance worn inside the mouth may reduce symp-toms by holding the lower jaw in a forward position.The nightly use of continuous positive airway pres-sure (CPAP), which provides a steady flow of roomair at low pressure through the nose to overcomeintermittent upper respiratory obstruction, is ofteneffective. Surgical trimming and reshaping of theuvula and soft palate can be performed by laser orradiofrequency ablation under local anesthesia. Amore elaborate procedure is mandibular osteotomywith genioglossus muscle advancement.
Chapter 9 • Ear, Nose, and Throat • 135

136 • Human Diseases
QUESTIONS FOR STUDY AND REVIEW
1. List and classify several reasons for hearing loss:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
2. List some common causes of nosebleed:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
3. Define or explain these terms:
a. audiography____________________________________________________________________________
_______________________________________________________________________________________
b. auditory tube____________________________________________________________________________
_______________________________________________________________________________________
c. cerumen_______________________________________________________________________________
_______________________________________________________________________________________
d. coryza__________________________________________________________________________________
_______________________________________________________________________________________
e. epistaxis _______________________________________________________________________________
_______________________________________________________________________________________
f. mastoiditis _____________________________________________________________________________
_______________________________________________________________________________________
g. pharyngitis_____________________________________________________________________________
_______________________________________________________________________________________
h. pinna __________________________________________________________________________________
_______________________________________________________________________________________
i. vertigo _________________________________________________________________________________
_______________________________________________________________________________________

4. Point out some ways in which the ear, nose, and throat are related anatomically, physiologically, and withrespect to diseases affecting two or more of them.
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
5. Discuss the inappropriate treatment of viral respiratory infections with antibiotics. State some objectionsto this practice. What share of the blame would you assign to patients, pharmaceutical manufacturers, andphysicians respectively?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
CASE STUDY: YOU’RE THE DOCTOR
1. Approximately one-third of adults queried report that they have had a sinus infection during the past year.What do you think is the likelihood that Mr. Rahman has bacterial rhinosinusitis requiring antibiotic treat-ment?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Chapter 9 • Ear, Nose, and Throat • 137
Rashid Rahman is a 37-year-old computer programmer from Pakistan who has been in the United Statesfor a year and a half as part of a cultural exchange program. He visits an urgent care clinic where you areon duty because of a "sinus infection."

2. Which, if any, of these historical points favor a diagnosis of bacterial rhinosinusitis?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
3. Does this additional history change your view as to the likelihood of bacterial infection? How?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
4. Do you now have grounds for agreeing with Mr. Rahman that he needs an antibiotic? Explain yourrationale.
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
138 • Human Diseases
The patient states that he began having nasal congestion and rhinorrhea yesterday, associated with painand pressure in the frontal and maxillary areas. His nasal discharge is thick and yellow. He denies sorethroat, cough, eye or ear symptoms, and fever. He sneezes often, sometimes four or five times in a row.He began taking pseudoephedrine and acetaminophen as soon as the symptoms appeared, but has hadno relief yet. When closely questioned, he admits that his facial pain is really more of a stuffiness or pres-sure than a pain, and that it seems to wax and wane, being worst when he bends forward to tie or untiehis shoes.
Mr. Rahman gives a long history of recurrent sinus infections, for which he has had numerous x-ray exam-inations in his own country. He states that his infections invariably progress to the point of disabling painand fever unless treated with an antibiotic, and he tells you which antibiotic consistently works for him.His general health is good. He does not smoke or drink alcohol and he takes no prescription medicines.He is allergic to cats and some plants but not to any foods or medicines.
On examination the patient appears alert, normally oriented, and in no distress. He is afebrile and hispulse and blood pressure are normal. His voice is somewhat nasal and he is breathing predominantlythrough his mouth, but there is no dyspnea, hoarseness, or cough. He sneezes repeatedly into a facial tis-sue during the consultation. The conjunctivae are slightly injected. Both nares show edema and pallor ofthe mucosa, with scant glairy secretion. There is slight tenderness to palpation above and below the eyes.The pharyngeal mucosa is normally hydrated and not injected. A thin postnasal discharge is evident onthe posterior pharyngeal wall. The ear canals are clear and the tympanic membranes are not injected.The neck is supple, without masses. The lungs are clear to auscultation.

5. Will you agree? Why or why not?
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
SUGGESTIONS FOR ADDITIONAL LEARNING ACTIVITIES
1. Role-play a physician office visit with you as the doctor. Ask your patient (another student or family mem-ber) to choose a condition from this chapter and assume the history and symptoms of that condition. Askrelevant questions of your patient in order to elicit the information you need to formulate a differentialdiagnosis. Order lab tests by asking the patient to give you the results from those described in the chap-ter. If you order a lab test that isn’t discussed, the patient should not tell you this but instead just say theresults of that particular test were within normal limits. Make your final diagnosis and ask your patient totell you if you were right.
2. Starting at the beginning of the chapter, make a list of all the anatomical terms that are discussed, includ-ing the structures of the ear, nose, and throat. Organize them down the left side of one or more sheets ofpaper, but don't number them. Label this list “A.” Then starting with a separate sheet of paper but begin-ning at the back of the chapter and working in reverse, list all the diseases and symptoms that are associ-ated with the ears, nose, and throat. Number the items in this list beginning with the number 1. Label thislist “B.” Starting with the first item on list A, write down the numbers of all the diseases or symptoms asso-ciated with that structure from list B. Continue through all the items on list A. When you are finished,make sure that you have used every number from list B.
3. You have been asked to be part of an expert panel on obstructive sleep apnea at the annual meeting ofthe American Academy of Otolaryngology–Head and Neck. You will give a 5-minute summary on thelatest findings in the treatment of this condition. Use medical journals, the library, or the Internet foryour research. Prior to your presentation, prepare questions on slips of paper and distribute them toyour audience (class members, study group participants, or family members). After your presentation,“field” the planted questions. In the classroom, form multiple expert panels, three students to a group,assigning each panel a topic.
Chapter 9 • Ear, Nose, and Throat • 139
You advise Mr. Rahman that his condition has not yet progressed to the point where antibiotic treatmentis appropriate. In fact, there are indications (staccato sneezing, pale nasal mucous membranes, absenceof fever, history of inhalant allergies) that his symptoms may be due partly or entirely to respiratory allergy.He vigorously resists the idea of allergic rhinitis, since he hasn’t been around any animals or floweringplants. He also says that since he knows from prior experience that he will eventually need an antibiotic,and since he doesn’t want to spend the time and money to make a second visit to the clinic, your clearmedical duty is to prescribe an antibiotic now.
Related Documents