Disease Management for Depression

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Disease Managementfor Depression

DISCLAIMER: The information contained in this annotated bibliography was obtained from the publications listed. The NationalPharmaceutical Council (NPC) has worked to ensure that the annotations accurately reflect the information contained in the publications, but cannot guarantee the accuracy of the annotations or the publications. There are articles available on the treatment of depression that are not included in this bibliography, which may include relevant information not covered herein. Theinclusion of any publication in this bibliography does not constitute an endorsement of that publication by NPC or an endorsementof the services, programs, treatments, or other information contained in such publication.
This bibliography is designed for informational purposes only, and should not be construed as professional advice on any specificset of facts and circumstances. This bibliography is not intended to be a comprehensive source of disease management servicesor programs in the treatment of depression, or a substitute for informed medical advice. If medical advice or other expert assistance is required, readers are urged to consult a qualified health care provider or other professional. NPC is not responsiblefor any claims or losses that may arise from any errors or omissions in the information contained in this bibliography or in the listedpublications, whether caused by NPC or originating in any of the listed publications, or any reliance thereon, whether in a clinicalor other setting.
© June 2003 National Pharmaceutical Council, Inc.
IntroductionThe Centers for Medicare and Medicaid Services
and the Disease Management Association of Americadefine disease management as a system ofcoordinated health care interventions andcommunications for populations with conditions inwhich patient self-care efforts are substantial.1 Diseasemanagement supports the clinician-patient relationshipand plan of care, and emphasizes prevention ofdisease-related exacerbations and complications usingevidence-based guidelines and patient empowermenttools.2 Disease management also evaluates clinical,humanistic, and economic outcomes on an ongoingbasis with the goal of improving overall health.2,3 Thespecific goals of disease management include:3
• Improving patient self-care through patienteducation, monitoring, and communication.
• Improving physician performance throughfeedback and/or reports on patient progress incompliance with protocols.
• Improving communication and coordination ofservices among patients, physicians, diseasemanagement organizations, and other providers.
• Improving access to services, including preventionservices and prescription drugs as needed.
The following functions are the main components ofdisease management:2,3
• Identification of patient populations.• Use of evidence-based practice guidelines.• Support of adherence to evidence-based medical
practice guidelines by providing practiceguidelines to physicians and other providers,reporting on the patient’s progress in compliancewith protocols, and providing support services toassist the physician in monitoring the patient.
• Provision of services designed to enhance patientself-management and adherence to the patient’streatment plan.
• Routine reporting and feedback to the health careproviders and to the patient.
• Communication and collaboration among providersand between the patient and the patient’s providers.
• Collection and analysis of process and outcomesmeasures, along with a system to makenecessary changes based on the findings of thosemeasures.
Disease management programs are used widely formany chronic diseases; but the most commondiseases include asthma, congestive heart failure,diabetes mellitus, and hypertension. Considerations inselecting a disease for disease management ofteninclude:2,3
• Availability of treatment guidelines with consensusabout what constitutes appropriate and effectivecare.
• Presence of generally recognized problems intherapy that are well documented in the medicalliterature.
• Large practice variation and a range of drugtreatment modalities.
• Large number of patients with the disease whosetherapy could be improved.
• Preventable acute events that often areassociated with the chronic disease (e.g.,emergency department or urgent care visits).
• Outcomes that can be defined and measured instandardized and objective ways, and that can bemodified by application of appropriate therapy(e.g., decreased number of emergencydepartment visits or hospitalizations).
• The potential for cost savings within a short period(e.g., less than 3 years).
Three major not-for-profit organizations whosemission is to promote quality health care haverecognized the contribution of disease managementactivities to quality health care by establishing diseasemanagement certification or accreditation programs.The Joint Commission on Accreditation of HealthcareOrganizations, an independent, not-for-profitorganization and the nation’s predominant standard-setting and accrediting body in health care, offersdisease-specific care program certification. Programcertification is based on an assessment of compliancewith consensus-based national standards, effective useof established clinical practice guidelines to manageand optimize care, and activities for performancemeasurement and improvement.4 The NationalCommittee for Quality Assurance (NCQA) recentlybegan accrediting disease management programs onthe basis of standards that are patient oriented,practitioner oriented, or both. It also offersorganizations certification for program design (e.g.,
[1]
Disease Managem
ent for Depression
Disease Management for Depression
content development), systems (e.g., clinicalinformation and other support systems), or patientcontact (i.e., for nurse call centers and otherorganizations without comprehensive activities).5 Manydisease management organizations were so eager toundergo the accreditation or certification process thatthey volunteered to do so before the standards werefinalized.6
The Utilization Review Accreditation Commission(URAC), also known as the American AccreditationHealthCare Commission, establishes standards for thehealth care and insurance industry. URAC’s goal is topromote continuous improvement in the quality andefficiency of health care delivery by achieving excellenceamong purchasers, providers, and patients through theestablishment of standards, education andcommunication programs, and a process ofaccreditation. URAC has accreditation programs fordisease management as well as case management,claims processing, core accreditation, credentialverification, health call centers, health networks, healthplans, health provider credentialing, health utilizationmanagement, health Web sites, Health InsurancePortability and Accountability Act (HIPAA) privacy andsecurity, independent review organizations, vendorcertification, and workers’ compensation utilizationmanagement. URAC has goals for diseasemanagement accreditation and case management.7
Why Focus on Depression?To date, disease management programs are more
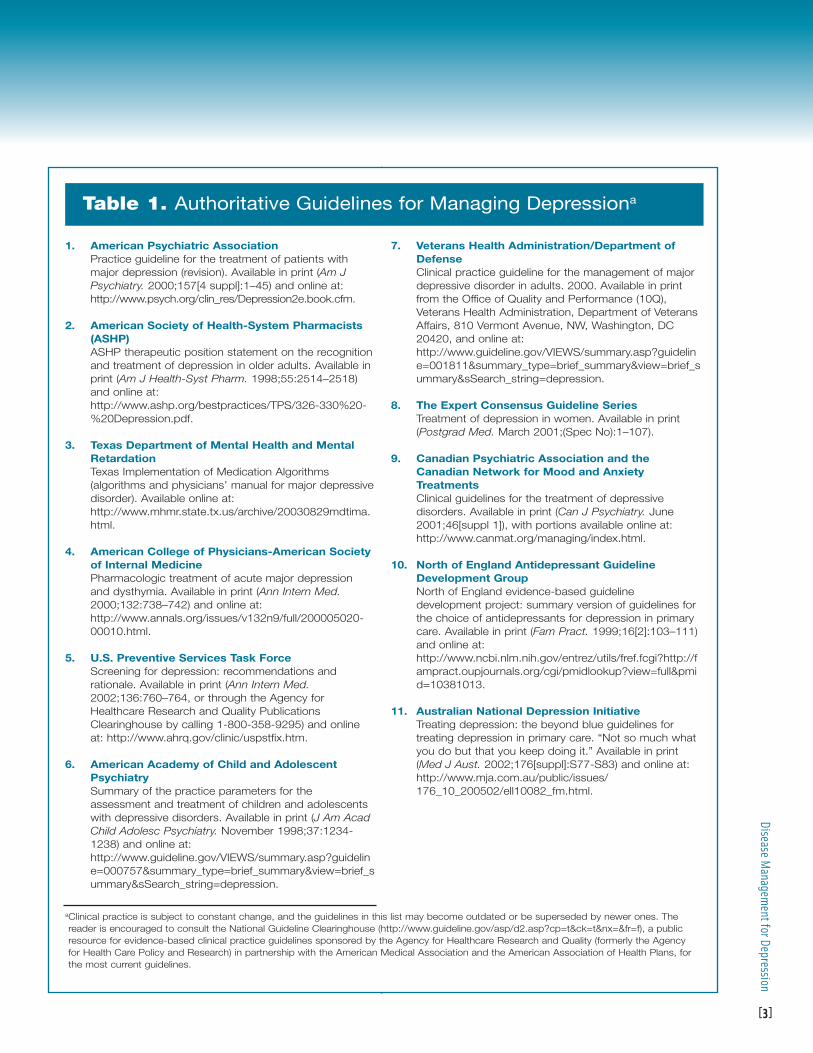
common for the treatment of asthma, congestive heartfailure, diabetes mellitus, and hypertension becausemany of the considerations outlined in the introductionclearly apply to these chronic diseases. However, muchattention has turned to depression in recent yearsbecause many of the same considerations apply tobehavioral health. For example, authoritative guidelinesfor managing depression have become availablerecently from the American Psychiatric Association andother reputable sources (Table 1).8 Up-to-dateinformation on treatment guidelines from varioussources also is available online from the NationalGuideline Clearinghouse (http://www.guideline.gov/body_home_nf.asp?view=home).
Depression is now recognized as a serious chronic
mental illness. It is characterized by depressed mood orloss of interest in or pleasure from activities thatordinarily are enjoyed (see Appendix A for diagnosticcriteria for major depression).9 It may be accompaniedby severe weight loss or gain, sleep disturbances,fatigue, diminished ability to concentrate, and suicidalthoughts. The symptoms of depression can have aprofound impact on an individual’s interpersonal, social,and occupational function, resulting in family discordand unemployment.
Depression is very common; 5.8% of Americanadults will experience depression sometime in theirlifetime.8 In any given year, approximately 9.9 millionAmerican adults are affected.10 The illness is nearlytwice as common in women as in men, and hormonalfactors may contribute to gender differences inprevalence.10,11 Women who give birth are particularlyvulnerable to depression during the postpartumperiod.11 The risk of depression is up to three timesmore likely in first-degree biological relatives (e.g.,daughter, father) of a patient diagnosed with the illnessthan in the general population, which suggests agenetic component to the illness.8 Certain medicalconditions (e.g., stroke, Parkinson’s disease, diabetes)can lead to depression; up to 25% of patients withthese medical conditions develop depression.9,11
Depression often goes unrecognized anduntreated.12 This illness is accurately diagnosed in only30% to 40% of cases.13 Symptoms often are notreported to a health care professional because of a lackof patient awareness that the symptoms constitute anillness or the stigma associated with mental illness.13,14
Patients and clinicians may fear insurance oremployment discrimination.15 Many people do not seektreatment because they do not recognize that theillness is treatable.11 Some patients (and clinicians) viewdepressive symptoms as a natural consequence ofaging or a normal reaction to stressful life events. Often,feelings of shame, guilt, or hopelessness may present abarrier to diagnosis.13
Failure of health care professionals to detectdepression may be due to inadequate training inrecognizing the illness.13 About half of patients treatedfor depression receive treatment in the primary caresetting, where training and experience in the diagnosisof depression may be limited.13 Physical complaintsmay distract primary care providers from making the
[2]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n
[3]
Disease Managem
ent for Depression
1. American Psychiatric AssociationPractice guideline for the treatment of patients withmajor depression (revision). Available in print (Am JPsychiatry. 2000;157[4 suppl]:1–45) and online at:http://www.psych.org/clin_res/Depression2e.book.cfm.
2. American Society of Health-System Pharmacists(ASHP)ASHP therapeutic position statement on the recognitionand treatment of depression in older adults. Available inprint (Am J Health-Syst Pharm. 1998;55:2514–2518)and online at:http://www.ashp.org/bestpractices/TPS/326-330%20-%20Depression.pdf.
3. Texas Department of Mental Health and MentalRetardationTexas Implementation of Medication Algorithms(algorithms and physicians’ manual for major depressivedisorder). Available online at:http://www.mhmr.state.tx.us/archive/20030829mdtima.html.
4. American College of Physicians-American Societyof Internal Medicine Pharmacologic treatment of acute major depressionand dysthymia. Available in print (Ann Intern Med.2000;132:738–742) and online at:http://www.annals.org/issues/v132n9/full/200005020-00010.html.
5. U.S. Preventive Services Task ForceScreening for depression: recommendations andrationale. Available in print (Ann Intern Med.2002;136:760–764, or through the Agency forHealthcare Research and Quality PublicationsClearinghouse by calling 1-800-358-9295) and onlineat: http://www.ahrq.gov/clinic/uspstfix.htm.
6. American Academy of Child and AdolescentPsychiatrySummary of the practice parameters for theassessment and treatment of children and adolescentswith depressive disorders. Available in print (J Am AcadChild Adolesc Psychiatry. November 1998;37:1234-1238) and online at:http://www.guideline.gov/VIEWS/summary.asp?guideline=000757&summary_type=brief_summary&view=brief_summary&sSearch_string=depression.
7. Veterans Health Administration/Department ofDefenseClinical practice guideline for the management of majordepressive disorder in adults. 2000. Available in printfrom the Office of Quality and Performance (10Q),Veterans Health Administration, Department of VeteransAffairs, 810 Vermont Avenue, NW, Washington, DC20420, and online at:http://www.guideline.gov/VIEWS/summary.asp?guideline=001811&summary_type=brief_summary&view=brief_summary&sSearch_string=depression.
8. The Expert Consensus Guideline SeriesTreatment of depression in women. Available in print(Postgrad Med. March 2001;(Spec No):1–107).
9. Canadian Psychiatric Association and theCanadian Network for Mood and AnxietyTreatmentsClinical guidelines for the treatment of depressivedisorders. Available in print (Can J Psychiatry. June2001;46[suppl 1]), with portions available online at:http://www.canmat.org/managing/index.html.
10. North of England Antidepressant GuidelineDevelopment GroupNorth of England evidence-based guidelinedevelopment project: summary version of guidelines forthe choice of antidepressants for depression in primarycare. Available in print (Fam Pract. 1999;16[2]:103–111)and online at:http://www.ncbi.nlm.nih.gov/entrez/utils/fref.fcgi?http://fampract.oupjournals.org/cgi/pmidlookup?view=full&pmid=10381013.
11. Australian National Depression InitiativeTreating depression: the beyond blue guidelines fortreating depression in primary care. “Not so much whatyou do but that you keep doing it.” Available in print(Med J Aust. 2002;176[suppl]:S77-S83) and online at:http://www.mja.com.au/public/issues/176_10_200502/ell10082_fm.html.
Table 1. Authoritative Guidelines for Managing Depressiona
aClinical practice is subject to constant change, and the guidelines in this list may become outdated or be superseded by newer ones. Thereader is encouraged to consult the National Guideline Clearinghouse (http://www.guideline.gov/asp/d2.asp?cp=t&ck=t&nx=&fr=f), a publicresource for evidence-based clinical practice guidelines sponsored by the Agency for Healthcare Research and Quality (formerly the Agencyfor Health Care Policy and Research) in partnership with the American Medical Association and the American Association of Health Plans, forthe most current guidelines.
diagnosis.13,15 Health care professionals may lack theconfidence to ask the patient about symptoms specificto mood or may hesitate to broach the subject becauseof pressure to minimize time spent with the patient.13,15
Clinicians’ beliefs and attitudes (e.g., understanding ofthe effectiveness of antidepressant drug therapy,misconceptions about the extent to which patients bearsome responsibility for their illness) also may influencethe likelihood of diagnosis.13 Detection may depend ona clinician’s level of skill in interviewing andcommunicating with patients.13
Treatment of depression often is inadequate despitethe availability of effective therapies and a high rate ofhealth service utilization by patients with depression.16–18
In a 4-year study of elderly enrollees in an HMO, only12% to 25% of patients with clinically significantdepressive symptoms received treatment for depression,and fewer than half of patients receiving antidepressantdrug therapy received an adequate trial of an appropriatedosage.19 In a survey of younger adults with depression,fewer than 10% received appropriate medicationmanagement and follow-up visits.17
The large gap between best care and usual care fordepression (i.e., inadequate detection and treatment ofdepression) serves as an impetus to apply diseasemanagement strategies to the treatment of depression.Education and training of health care providers toimprove detection and treatment could help fill this gap.The availability of new and improved tools for use byprimary care physicians to diagnose and treatdepression and self-administered screening tools forpatients have led to increased interest in depressiondisease management.20
Depression increasingly is a focus of diseasemanagement initiatives because of its large economicimpact. It is a chronic illness with recurrent acuteepisodes that are costly.21 Depression is the leadingcause of short- and long-term disability in the UnitedStates—persons with untreated depression report alarger number of days spent in bed and days ofdisability or restricted activity than the generalpopulation.10,22–25 Depression also is associated withhigher than average rates of physical illness and healthcare utilization.25 Health care costs are higher fordepressed patients than for patients withoutdepression, even after adjusting for medical morbidity.18
Mortality rates are increased in depressed patients,
usually as a result of suicide; up to 15% of patientshospitalized for depression commit suicide.25
In 1990, the estimated annual costs of depression inthe United States amounted to $43.7 billion, including$12.4 billion for direct costs, $7.5 billion for mortalitycosts (costs due to suicide), and $23.8 billion formorbidity costs (costs arising from workplaceabsenteeism and reduced workplace productivity).26
Employers increasingly recognize the impact ofdepression in the workplace.20,22,23 However, convincingemployers of the cost-effectiveness of drug therapy fordepression can be a challenge because of the highcost of this therapy.21,27 In the 2002 Novartis PharmacyBenefit Report, antidepressants represented the mostcostly and widely prescribed drug class (among 32drug classes evaluated) with respect to HMO spendingand use.28 Therapy for depression has the potential toreduce the indirect costs of illness.29 It could saveemployers an estimated $93 per patient in reduceddisability costs in the first 30 days after initiation oftherapy, and this figure does not reflect cost savings tothe employer from reduced workplace absenteeismand improved productivity.30 Antidepressant drugtherapy improves workplace performance, with aresponse within 4 weeks after initiating therapy.31 Thenatural history of depression and the methods used tomanage depression are outlined in Appendix B.
Current Status of DiseaseManagement Programs forDepression
The importance of a person’s mental health tooverall health and quality of life and the need for mentalhealth services to restore and maintain mental healthare increasingly recognized by the government and theprivate sector. Policy makers also have gained a greaterunderstanding of the high prevalence and chronicnature of depression and the role of antidepressantdrug therapy in managing the illness on a long-termbasis. Mental health utilization (the percentage ofmembers receiving services, inpatient discharges, andaverage length of stay), follow-up after hospitalizationfor mental illness, and antidepressant medicationmanagement are among the NCQA 2002 Health PlanEmployer Data and Information Set (commonly referredto as HEDIS) measures, which apply to Medicaid and
[4]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n

Medicare recipients as well as participants in
commercial health plans.43
Disease management strategies have great potential
to improve therapeutic outcomes for patients with
depression. However, the management of depression
presents a challenge to many health care providers
because it usually is first seen in the primary care
setting due to of a lack of access to specialty care or
the stigma associated with seeking treatment from a
mental health professional.42
Primary care providers usually have limited time to
spend with patients and what time is available often is
inadequate for patients with multiple chronic illnesses.13 In
a managed care system, depression often competes with
other chronic disease states and conditions for limited
health care dollars.14 Clinicians must prioritize their time,
and patients may be forced to set priorities for their needs.
Patients may be reluctant to accept the diagnosis of
depression, and access to medications also may be a
barrier to successful treatment.14 Failure to adhere to
drug therapy and follow up with clinic visits
compromises patient outcomes.
Although there can be some challenges in managing
depression through a disease management program,
many disease management vendors have taken on the
challenge and have seen great success. Some of the
experiences to date with depression disease
management programs are described here.
Depression Disease ManagementProgramsCedars-Sinai Medical Center (Los Angeles, CA)
The clinics of Cedars-Sinai Medical Center are
exploring new educational initiatives for treating
depression in patients with cardiovascular disease.
Their past disease management programs involving
hypertension, hyperlipidemia, diabetes, asthma, and
the anticoagulation therapy have shown strong cost-
savings results. For additional information, see Disease
Management News, March 25, 2001 (page 5), or
contact Jeff Borenstein, MD, at Cedars-Sinai Medical
Care Foundation (310) 247-7700, ext. 502.
Group Health Cooperative of PugetSound (Seattle, WA)
Group Health Cooperative of Puget Sound, an HMOwith more than 450,000 members in western Washingtonstate, has been a national leader in implementing diseasemanagement for patients with depression.16 The diseasemanagement program at Group Health Cooperative hasevolved over the past decade, during which variousstrategies were used to improve the accuracy ofdiagnosis and optimize acute-phase management.16
Models for collaborative management of depression byprimary care physicians and specialists were evaluated inrandomized controlled trials.44,45
Consultation Liaison Primary Care CollaborativeModel. In a 12-month trial, 217 patients withdepression who agreed to receive antidepressant drugtherapy were randomized to receive a multifacetedintervention or usual care by the primary carephysician.44 The multifaceted intervention entailedfrequent, intensive visits over the first 4–6 weeks oftreatment (the first and third visits were with the primarycare physician and the second and fourth visits werewith a psychiatrist). Patients (and family members asappropriate) were educated about the biology ofdepression and its etiology and treatment (e.g.,behavioral therapies, antidepressant drug therapy).Videotaped and written educational materials also wereprovided. Patients were asked to complete aquestionnaire about adverse effects from drug therapyand any concerns for subsequent discussion with theprimary care physician; completing this questionnairewas designed to encourage the patient to assume anactive role in his or her treatment.16 Adherence to drugtherapy (e.g., refill frequency) was monitored during thecontinuation and maintenance phases of treatment.
At the start of the study, primary care physiciansparticipated in a half day workshop on the diagnosisand treatment of depression and study methods.44 Thepsychiatrist assisted the primary care physician withmodification of drug therapy when severe adverseeffects occurred or response to drug therapy wasinadequate. Either the primary care physician or thepsychiatrist could make changes to the drug dosage ortype of drug after oral consultation. Psychiatristsprovided the primary care physicians with oral andwritten feedback about patient progress. Monthlyconferences involving the primary care physicians andpsychiatrists were conducted to discuss cases.44
[5]
Disease Managem
ent for Depression

Compared with usual care, the intervention wasassociated with significantly greater patient adherenceto antidepressant drug therapy, patient satisfaction withoverall quality of care and antidepressant drug therapy,and improvement in depressive symptoms.44
Brief Therapy Primary Care Model. A multifacetedintervention involving antidepressant drug therapy andcognitive-behavioral treatment was evaluated in 153patients with depression.45 Patients were randomized toreceive the intervention or usual care by the primary carephysician. Patients in the intervention group participatedin four to six sessions with a psychologist over the first 2months of the study. Cognitive-behavioral treatment andcounseling on the importance of medication adherencewere provided in these sessions. Cognitive-behavioraltreatment was designed to promote the use of adaptivecoping strategies and encourage the patient to adoptpositive thought patterns and activities instead ofnegative ones. The psychologists met with a psychiatriston a weekly basis to discuss each patient’s medicationadherence and response. The psychiatrist maderecommendations to the primary care physician fordosage adjustments as needed. Primary care physiciansparticipated in training on drug therapy and cognitive-behavioral treatment for depression at the start of thestudy. Videotapes and written materials aboutdepression and its treatment were provided to patients.
Patient medication adherence, satisfaction withquality of care for depression and antidepressant drugtherapy, and improvement in depressive symptomswere significantly greater in patients in the interventiongroup than in patients in the usual-care group.45
Cost-Effectiveness of Collaborative Care. Thesuccess of the Consultation Liaison Primary CareCollaborative Model and the Brief Therapy Primary CareModel was attributed to patient education, physiciantraining, the reorganization of care, and the availabilityof information systems to facilitate tracking and sharingof key patient data.16 An analysis of costs associatedwith the two models revealed that the intervention wasassociated with a modest increase in the cost-effectiveness of treating depression compared withusual care, despite increased costs due to the need forextra visits by the intervention group.46 The costs foreach patient successfully treated were approximately$1700 to $1800 in the intervention group and $1950 to$2150 in the usual-care group. The investigators
speculated that further improvement in cost-effectiveness of the intervention might be achieved ifthe intervention was reserved for patients with aninadequate response after 6 to 8 weeks of usual care.16
Telephone Counseling and Computerized
Monitoring. The effectiveness of conducting diseasemanagement interventions by using telephone calls topatients instead of clinic visits was studied. In a pilotstudy, 28 patients initiating antidepressant drug therapyreceived written information about depression and sixweekly telephone counseling and support sessions by atrained therapist (the intervention). The transtheoreticalmodel of behavioral change (i.e., stages of change, suchas contemplation) and cognitive-behavioral strategieswere used to enhance patient self-management andcoping skills.47 After 3 months and 6 months, patients inthe intervention group had significantly fewer depressivesymptoms than did a group of 94 patients receivingusual care. Patient adherence was twice as likely in theintervention group as in the usual-care group. Thenumber of clinic visits did not differ significantly betweenthe two groups (i.e., the benefits associated with theintervention did not require extra visits).48
The use of computerized systems for providingfeedback to primary care physicians aboutantidepressant dosages and prescription refills, follow-up visit frequency (i.e., adequacy), and algorithm-basedrecommendations for treatment (an approach referredto as feedback) was evaluated alone and incombination with care management in a 6-month,randomized, controlled trial of 613 patients who wereinitiating antidepressant drug therapy.49 Caremanagement entailed telephone calls to patients by acare manager at the initiation of therapy and 8 weeksand 16 weeks later to discuss antidepressant drugtherapy, adverse effects, and response. Feedbackprovided to primary care physicians included treatmentrecommendations on the basis of a computerizedalgorithm that took into consideration actual andrecommended antidepressant dosages and follow-upvisit frequency. Usual care was used as a control.
Patients in the feedback group were no more likelyto receive appropriate antidepressant drug therapy orexperience at least moderate improvement indepressive symptoms than patients in the usual-caregroup. However, patients in the feedback group whoreceived care management were more likely to receive
[6]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n
appropriate antidepressant drug therapy andexperience improvement in depressive symptoms thanwere those in the usual-care group. The incrementalcosts per patient were $22 for the feedback approachand $83 for feedback plus care management.49
Relapse Prevention. Recent disease managementefforts at Group Health Cooperative have addressedpatients with persistent depression who are at high riskfor relapse. In a randomized trial, 386 patients withdepression who had recovered to a large extent after 8weeks of treatment but who were at high risk for relapsewere randomized to a relapse prevention program orusual care.50 The relapse prevention program wasdesigned to promote medication adherence andincrease patient self-monitoring of symptoms andrecognition of the prodromal symptoms that precede arelapse. The program involved two primary care visitswith a depression specialist (a psychologist, a nursewith a master’s degree in psychosocial nursing, or asocial worker) and three telephone calls over a 1-yearperiod. A written relapse prevention plan was devisedfor each patient. Primary care physicians receivedintermittent reports about patient progress.
Medication adherence, the use of an adequatedosage, and refill frequency were significantly better inthe intervention group than in the usual-care group.Depressive symptoms also were significantly improvedin the intervention group at the end of the study.However, the number of episodes of relapse was nodifferent in the two groups.50 The investigatorsspeculated that more intensive relapse preventioninterventions may be required to reduce relapse rates.Future disease management efforts at Group HealthCooperative will address relapse prevention.
Health Hero Network, Inc. (MountainView, CA)
Involving patients in their care is critical to effectivelymanaging a chronic illness. Health Hero Network, atechnology company, has designed the Health HeroPlatform, a group of electronic devices that health careproviders can use to send patients reminders to taketheir medicine, provide them with feedback on theirprogress, and provide tips for managing their diseasemore effectively. This empowers patients to feel more incontrol and to practice better self-care. Health HeroNetwork customers are using Health Hero solutions forprograms in heart failure, cardiovascular disease,
diabetes, asthma, chronic obstructive pulmonarydisease, and many other chronic conditions.
The company is collaborating with the Department ofVeterans Affairs to develop a disease managementprogram for depression. The use of telemedicine tocommunicate with patients will be an integralcomponent of this program and will include reminders totake medications and to keep scheduled appointments.For additional information about the Health HeroNetwork, go to http://www.healthhero.com/index.html.
Heritage Information Systems Inc.(Richmond, VA)
Heritage Information Systems Inc. is a privately heldconsulting company providing clinical management andpharmacy cost containment services to governmentprograms, insurance companies, and large employers.The company serves 10 state Medicaid programs,several national commercial insurers, 5 Blue Cross BlueShield licensees, and some of the largest employergroups in the country.
A mail-based disease management program toimprove the treatment of depression by reducingphysician practice variation was implemented. HeritageInformation Systems educated physicians to better useclinical practice guidelines. This educational interventionled to substantial cost savings; physicians prescribedmore appropriate treatments that were more cost-effective. Education of the physicians also led toimproved medication adherence by patients.Educational information along with treatment guidelineinformation was mailed to physicians of patients withexcessively long or short antidepressant drug therapy,possible drug interactions, and nonadherenceproblems. For additional information, see Disease
Management News, March 10, 2001 (pages 3 and 5),or go to http://www.heritage-info.com.
Kaiser Permanente Care ManagementInstitute (Oakland, CA)
The Care Management Institute was created in 1997to help Kaiser Permanente improve the quality of careand health outcomes for its members. Depression,asthma, cardiovascular disease, diabetes mellitus, eldercare, heart failure, chronic pain, and cancer were theclinical priorities because they represented anopportunity to improve care for members of the HMO.
Kaiser Permanente received certification from the
[7]
Disease Managem
ent for Depression
NCQA for design of a depression disease managementprogram in September 2002. Non-compliant patientswere identified and targeted interventions encouragedimproved treatment compliance. The percentage ofpatients starting antidepressant drug therapy who hadat least three follow-up visits within the first 12 weeksof therapy and the percentages of patients continuingantidepressant drug therapy for at least 3 months andat least 6 months increased between 1998 and 1999 atKaiser Permanente. For additional information, go tohttp://www.kpcmi.org.
Keystone Health Plan Central (Camp Hill, PA)Keystone Health Plan Central is a 225,000-member,
jointly owned subsidiary of Capital Blue Cross andPennsylvania Blue Shield. Its depression diseasemanagement program dates back to 1998. Screeningscales and depression practice guidelines aredistributed to primary care providers. Then, anonymoustelephone and Internet-based depression screeningmechanisms are offered. Patient education materialsabout the illness and the importance of medicationadherence are given to providers and patients. Foradditional information see Disease Management News,May 10, 2001 (pages 1, 6, and 7), contact DevoraSherfy at Keystone Health Plan Central (717) 730-1941,or go to http://www.pahealthcoverage.com/keystonecentral.html.
LifeMasters Supported SelfCare (Irvine, CA)LifeMasters Supported SelfCare is an interactive
disease management company that provides toolssuch as health education, training in self-monitoring,and personalized coaching. Timely, clinically-validatedinformation is provided to physicians to prevent seriousmedical episodes that can result in unnecessaryemergency department visits and hospitalizations.
In the past, LifeMasters managed depression as acomorbidity with other diseases, but it recently launcheda stand-alone depression program. The programfocuses on primary care providers and newly diagnosedpatients. A nurse call center and other support tools willbe used to monitor patients to ensure adherence tomedication regimens and to prevent relapse. Foradditional information, see Disease Management News,May 10, 2001 (pages 1, 6, and 7), contact Jeffrey Davis,MD, at LifeMasters Supported SelfCare (650) 941-1066,or go to http://www.lifemasters.net.
The Merck-Medco Experience (WestPoint, PA)
Merck-Medco, a pharmacy benefits management(PBM) company, developed Transitions to BetterHealth, a depression disease management programdesigned to optimize the cost-effective use ofantidepressant drug therapies and clinical outcomes.21
The program was available to pharmacy benefitsmanagement clients, who decided whether to offer it toplan members. Plan members (i.e., patients) decidedwhether to participate and authorize the release ofpersonal data. Member prescription claims data (andmedical claims data, if available) were reviewed, andone or more of three interventions was offered asappropriate.
One intervention was designed to identify andrecognize undiagnosed or untreated depression.Prescription claims data for certain types ofmedications (e.g., certain analgesics) and, if available,medical claims data were used to identify the planmembers who are responsible for the highest 10% ofplan costs because of the link between depression andhigh medical resource use. Patients who had agreed toparticipate in the program were screened fordepressive symptoms by telephone interviewconducted by a trained psychiatric nurse. Physicianswere promptly notified if the patient appeared to meetthe criteria for depression based on this screening.Published information from authoritative sources,including diagnostic criteria and treatment guidelines,was provided to the physician. Follow-up phone calls tothe physician were made within one week to offerdecision support based on the treatment guidelines.Additional follow-up contact with physicians took place35 to 50 days later to ascertain the outcome ifantidepressant drug therapy was not initiated.
The second intervention was designed to improvepatient medication adherence and avoid prematurediscontinuation of drug therapy, relapse, and costlyhospitalization. Patients filling a new prescription for anantidepressant for a first episode or recurrence ofdepression were contacted by telephone to obtainauthorization to participate. Patients who agreed toparticipate received five education and support callsfrom a psychiatric nurse over a 12-month period. Ifneeded, a pharmacist provided counseling on adverseeffects from drug therapy. Educational mailings andbehavioral reinforcement also were provided.
[8]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n

The third intervention encouraged physicians toprescribe antidepressant drug therapy for an adequatebut not excessive duration, in accordance withauthoritative treatment guidelines. After a year oftreatment, the physician was asked to indicate whetherthe patient was a candidate for maintenance therapy ortapering and discontinuation of drug therapy. Writtentreatment guidelines that govern this determinationwere provided to the physician.
The information system capabilities of the PBMfacilitated this disease management program andenabled plans to monitor NCQA HEDIS indicators.21
For example, prescription refill frequency was readilymonitored. Results from the program to date arelimited. Undiagnosed depression was detected in 9%of screened patients. The rate at which newantidepressant prescriptions for first episodes orrecurrences were refilled at least once (presumablyreflecting medication adherence) increased by 20%.Nearly 5% of patients monitored 18 months afterstarting antidepressant therapy had discontinued it(presumably reflecting avoidance of unnecessary use).Additional experience with the program is needed toevaluate the impact on patient outcomes and costs.
PacifiCare Behavioral Health (LagunaHills, CA)
PacifiCare Behavioral Health, a wholly ownedsubsidiary of PacifiCare Health Systems, providesbehavioral health services to members in 10 states andGuam. In 1999, the company developed Taking Charge
of Depression, a disease management program forpatients with depression that emphasizes self-management. A patient self-care resource kit with aninformation booklet about depression, medications, andlifestyle changes, and physician encounter cards forpatient use in discussions during physician visits isprovided to patients. Patients have monthly telephonecontact with counselors to ensure adherence withmedications and scheduled visits. Medicationadherence is monitored through prescription refillactivity and phone calls to the patient. For additionalinformation, see Disease Management Advisor, July2000;6(7):110-111, or go to http://www.pbhi.com.
PARTNERS Health Plan (South Bend, IN)PARTNERS Health Plan is a regional health plan that
developed PARTNERS in Mental Wellness, a
depression disease management program. Theprogram helps primary care providers use betterscreening tools for depression. Another component ofthe program is TxAlert, a reminder system thatgenerates a review of claims and pharmacy data usingnational treatment standards. TxAlert allowedPARTNERS to alert physicians when patients were nottaking their medication as prescribed. The goals of theprogram included increased medication adherence anduse of counseling by behavioral health providers. Foradditional information, see Disease Management News
May 10, 2001 (page 6) or contact Patricia Kirkpatrick atPARTNERS Health Plan (219) 236-7720.
Pfizer Inc. (New York, NY)Pfizer Inc., a pharmaceutical company, oversees the
Prime-MD® Today program, which uses a diagnosticinstrument to help primary care physicians recognizethe symptoms of depression, as well as anxiety,alcohol, eating, and somatoform disorders. The Prime-MD® Patient Health Questionnaire (PHQ-9) is avalidated self-administered diagnostic instrument, whichevolved from the Prime-MD diagnostic instrumentadministered by physicians. A depression self-quiz forconsumer use is also available at http://www.zoloft.com/index.asp?pageid=4. For additional information aboutPrime-MD Today, go to http://www.zoloft.com/psd/healthmanagement/primemd.pdf.
Protocol Driven Healthcare Inc.(Bernardsville, NJ)
Protocol Driven Healthcare Inc. develops andmarkets health application software and services thatare used to deliver health, wellness, and diseasemanagement programs. The company provides anInternet-based patient education and self-care programfor depression to help patients adhere to medicationregimens and allow physicians to provide betterpatient-specific information. For more information, go tohttp://www.pdhi.com/.
RAND Health (Santa Monica, CA)RAND Health is the nation’s largest private health
care research organization. RAND Health’s Partners in
Care program is an integrated approach to improvingcare for depression in primary care. The program usescollaborative care and is suitable for a variety ofpractice settings. A study using the program
[9]
Disease Managem
ent for Depression
[10]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n
demonstrated that patients’ mental health and dailyfunctioning can be significantly improved by treatment.Favorable outcomes for employers, managed careorganizations, and insurers, including a reduction in job-loss rates, were achieved with the use of modest,practical programs in primary care settings. Programmaterials are available athttp://www.rand.org/health/pic.products/ or from RANDDistribution Services by calling (877) 584-8642.
Tufts Health Plan (Boston, MA)Tufts Health Plan was founded in 1979 as a not-for-
profit HMO. It has expanded into a family ofcompanies, offering a full array of health care coverageoptions to individuals and employer groups. Depressionis among the mental health disease managementprograms offered by the Tufts Health Plan. Thedepression program focuses on patients in the primarycare setting. Patient education materials about theillness and medications are provided by mail and on theInternet. For additional information, go tohttp://www.tufts-healthplan.com/.
Additional Depression DiseaseManagement ResourcesEli Lilly and Company (Indianapolis, IN)
Eli Lilly and Company, a pharmaceutical company,provides Internet-based patient information about thetreatment of depression and information about where toseek treatment. A Zung scale self-assessment test isavailable online at: http://www.prozac.com/.
Forest Laboratories (St. Louis, MO)Forest Laboratories, a pharmaceutical company,
provides Internet-based patient information about thetreatment of depression. In addition, a physician locator(by zip code) and a depression self-rating (i.e.,screening) test are available online at:http://apps.redidata.com/forest/surv/survey.asp?one=&two=&three=&four=&wherefrom=WEBSITE&missing=true&accept=on.
QualityMetric Inc. (Lincoln, RI)QualityMetric Inc., an independent, privately held
corporation, is a provider of health outcomesassessment tools. The company was founded in 1997
by John E. Ware, Jr., PhD, principal developer of theSF-36®, SF-12®, and SF-8™ health surveys, widelyused health assessment surveys. Internet-based toolsfor measuring outcomes in patients with depression areavailable from QualityMetric. For more information, goto http://www.qualitymetric.com/.
The Future of DepressionManagement
Disease management—an important approach tointegrated care—has been shown to improve patientoutcomes and quality of life while potentially reducingoverall costs. Applying the key components of diseasemanagement to the treatment of depression can helpensure successful treatment. Disease management is auseful, efficient approach to health care. It hascontinued to gain widespread acceptance over the past10 years, and health plans that provide multipleservices to patients who need coordinated services areseeing the most success in their chronically ill patients.
Challenges in Managing DepressionThe management of depression does present
challenges to clinicians. Depression usually is treated in theprimary care setting because of a lack of access tospecialty care or the stigma associated with seekingtreatment from a mental health professional.42 Changes inthe financing and structure of the health care systemduring the 1990s affected patterns of referral of patients tospecialists.14 In the early 1990s, referral was uncommonbecause of the negative economic impact on primary careproviders under a capitation system (i.e., the primary careprovider bore the cost for referrals).14 In the late 1990s,referral became more common with the establishment ofmanaged behavioral health organizations.14 Nevertheless,only one in five patients with major depression is treatedby a mental health specialist.51
The structure of managed care systems increasesreliance on primary care providers for mental healthservices. However, the primary care system is more effectivein managing acute illnesses than chronic conditions such asdepression.42 Primary care providers have limited time tospend with patients and what time is available often isinadequate for patients with chronic illnesses.13 In amanaged care system, depression often competes withother disease states and conditions for limited health care

[11]
Disease Managem
ent for Depression
dollars.14 Clinicians must prioritize their time, and patientsmay be forced to set priorities for their needs.52
The physician-patient relationship typically is not longlasting because of frequent changes in healthinsurance, especially in patients who change employersfrequently.14 Mental health “carve outs” (i.e.,subcontracting of mental health services to mentalhealth providers separate from other health careservices) may result in fragmented care.14 Continuity ofcare for patients with depression usually is lacking.
In addition, some patients may be reluctant toaccept the diagnosis of depression; and access tomedication can be a barrier to successful treatment.14
Failure to adhere to drug therapy and follow up withclinic visits also compromises patient outcomes.
Strategies for Overcoming Barriers toManaging Depression
Strategies to overcome barriers to managingdepression include developing educational campaignsfor the public to reduce the stigma associated with thetreatment of depression and other mental illnesses.16,53
Many mental health associations (Table 2) haveundertaken such efforts.54
Education and training of primary care providers incommunication skills and the use of screening toolscan improve the detection rate of depression.15,55,56
Health systems can be redesigned to increasecollaboration between primary care providers andspecialists in the management of patients withdepression (e.g., using collaborative managementmodels) without compromising cost-effectiveness.Rebundling resources and delegating responsibility(e.g., patient education tasks that can be performed bynurses) can make such collaborations economicallyfeasible.52 Information systems can be developed tofacilitate communication among providers and trackingof patient data and outcomes. Identifying patients athigh risk for relapse or recurrence so that they canreceive maintenance therapy and other relapseprevention strategies (e.g., patient education, extraclinic visits, follow-up phone calls) and patients at lowrisk for relapse or recurrence so they can discontinuetherapy (after tapering) optimizes the use of limitedresources. Outcomes-based performance standardsshould be established to provide a basis for healthplans to compare operational successes (e.g., relapserates in patients with depression).53
Patient education should motivate patients to
assume a more active role in their own care and
improve their self-management skills and adherence to
prescribed therapy. The use of information systems can
help promote patient adherence and improve outcomes
by tracking prescription refill and clinic visit frequency
and timing, and by identifying patients who discontinue
drug therapy prematurely. Telephone calls to patients
(especially those whose adherence is poor) may result
in better adherence and outcomes.
Health management is a strategy that has been
advocated as an alternative to disease management.14
The patient (not the disease) is the focus of this
approach; patients are partners in care and they
negotiate priorities with the physician and managed
care organization. Quality-of-life measures are used to a
greater extent than disease-specific measures in
American Psychiatric Association1000 Wilson Boulevard, Suite 1825Arlington, VA 22209-3901(888) 357-7924http://www.psych.org
National Alliance for the Mentally IllColonial Place Three2107 Wilson Boulevard, Suite 300Arlington, VA 22201(703) 524-7600Help Line: 800-950-NAMI [6264]http://www.nami.org
National Institute of Mental Health6001 Executive Boulevard, Room 8184, MSC 9663Bethesda, MD 20892-9663(866) 615-NIMH[6464]http://www.nimh.nih.gov/publicat/depression.cfm
National Mental Health Association2001 North Beauregard Street,12th FloorAlexandria, VA 22311(800) 969-NMHA[6642]http://nmha.org
Table 2. Mental Health Associationswith Information for the Public

[12]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n
evaluating outcomes. Physician efficiency in detectingand triaging mental illnesses and prioritizing time isincreased through the use of ReACT, a strategy thatentails recognizing the presence of distress, assessingthe type and severity of the problem, categorizing theproblem, and treating the problem. Support staff andvarious technologies (e.g., information systems,telephone interviews, interactive voice responsesystems) are used to optimize efficiency. Collaborationbetween primary care providers and mental healthspecialists is emphasized.
ConclusionDepression is a costly mental illness that often goes
undetected or inadequately treated.9,10,15,56 Diseasemanagement programs for depression are not as wellestablished as those for other chronic medical
conditions because of the structure of the health care
system and patient attitudes and behavior. However,
many vendors are taking on the challenge of
implementing depression disease management
programs and seeing success.
Strategies to overcome barriers to managing
depression include training of health care providers in
detection and diagnosis of the illness, increasing
collaboration among primary care providers and
specialists, and providing patient education to increase
motivation, self-management skills, and adherence to
the treatment regimen.
Disease management can improve patient outcomes
and quality of life while potentially reducing overall health
care costs. It is key to integrating care. As more health
care payers incorporate disease management principles
into the delivery of care, we will begin to see many more
depression disease management programs.

A. Five (or more) of the following symptoms have beenpresent during the same 2-week period and represent achange from previous functioning; at least one of thesymptoms is either (1) depressed mood or (2) loss ofinterest or pleasure.
Note: Do not include symptoms that are clearly due to ageneral medical condition, or mood-incongruent delusions orhallucinations.
(1) depressed mood most of the day, nearly every day,as indicated by either subjective report (e.g., feelssad or empty) or observation made by others (e.g.,appears tearful). Note: In children and adolescents,can be irritable mood.
(2) markedly diminished interest or pleasure in all, oralmost all, activities most of the day, nearly everyday (as indicated by either subjective account orobservation made by others)
(3) significant weight loss when not dieting or weightgain (e.g., a change of more than 5% of bodyweight in a month), or decrease or increase inappetite nearly every day. Note: In children,consider failure to make expected weight gains.
(4) insomnia or hypersomnia nearly every day(5) psychomotor agitation or retardation nearly every
day (observable by others, not merely subjectivefeelings of restlessness or being slowed down)
(6) fatigue or loss of energy nearly every day(7) feelings of worthlessness or excessive or
inappropriate guilt (which may be delusional) nearlyevery day (not merely self-reproach or guilt aboutbeing sick)
(8) diminished ability to think or concentrate, orindecisiveness, nearly every day (either bysubjective account or as observed by others)
(9) recurrent thoughts of death (not just fear of dying),recurrent suicidal ideation without a specific plan, ora suicide attempt or a specific plan for committingsuicide
B. The symptoms do not meet criteria for a Mixed Episode.C. The symptoms cause clinically significant distress or
impairment in social, occupational, or other importantareas of functioning.
D. The symptoms are not due to the direct physiologicaleffects of a substance (e.g., a drug of abuse, amedication) or a general medical condition (e.g.,hypothyroidism).
E. The symptoms are not better accounted for bybereavement, i.e., after the loss of a loved one, thesymptoms persist for longer than 2 months or arecharacterized by marked functional impairment, morbidpreoccupation with worthlessness, suicidal ideation,psychotic symptoms, or psychomotor retardation.
Appendix A. Diagnostic Criteria for Major Depression
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Copyright 2000American Psychiatric Association.
[13]
Disease Managem
ent for Depression

[14]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n
Depression usually first manifests when a person is inher or his late 20s, although the onset can occur atany age.8 Untreated episodes usually last for 6–24
months.8,25 Depression has a variable course.8,25 About twothirds of untreated patients have only a single episode andreturn to their previous level of functioning (i.e., achievespontaneous remission).25 However, residual symptoms andimpairment of interpersonal, social, and occupationalfunctioning persist in 20% to 35% of cases.8 Approximately50% to 85% of patients have at least one more episode (i.e.,a recurrence), usually within 2 or 3 years.8
The goals of treatment for depression in the acute phaseare to eliminate all symptoms and restore psychosocialfunction (i.e., achieve remission).32,33 Prevention of relapse(i.e., a return of symptoms before full recovery within 6months after remission) is the primary goal of treatmentduring the continuation phase. Prevention of recurrence (anew episode following a full recovery) is the goal ofmaintenance therapy.32
Initial therapeutic options in the acute phase of adepressive episode are pharmacotherapy, psychotherapy, orboth.8 Considerations in choosing among these optionsinclude symptom severity, patient preference, and pastresponse of the patient and family members toantidepressant therapy.8 Demographic variables (e.g., age,sex, marital status) are not good predictors of treatmentoutcome.34 Antidepressant drug therapy should be providedfor patients with moderate or severe symptoms and, ifpreferred by the patient, may be used for mild symptoms aswell.8 Psychotherapy alone may be considered for patientswith mild or moderate symptoms.8 Combinationpharmacotherapy and psychotherapy is sometimes used forpatients with psychosocial or interpersonal problems, or apersonality disorder and moderate or severe depression.8
PharmacotherapyDepression has been attributed in part to the depletion
of neurotransmitters (norepinephrine, serotonin, dopamine, ora combination) in the central nervous system, althoughtheories about the pathogenesis of depression are stillevolving and subject to debate.35,36 Most antidepressantmedications inhibit neuronal reuptake of one or more of theseneurotransmitters, thereby enhancing neurotransmission.However, the effects of antidepressants are complex andremain to be fully elucidated.
The various antidepressant agents and antidepressantdrug classes are comparable in efficacy in treating depressive
episodes; 50% to 75% of patients respond to antidepressantdrug therapy.8 Because the response rates are similar amongthe available agents, selection of an antidepressant agentusually is made on the basis of safety, tolerability, patientpreference, and cost.8
Regular and consistent monitoring—a key component ofdisease management—of antidepressant drug therapy iscritical to managing depression successfully. Accurate patientmonitoring helps to ensure that the health care providerselects a drug with maximum therapeutic effect and minimaladverse effects and also helps to ensure proper dosetitration. Regular monitoring of the patient and provision offeedback to the health care provider can address anypotential problems with adverse effects and efficacy at anearly stage. Early intervention also can resolve issues thatcould affect compliance. Patient monitoring is key in the earlystages of the treatment process. Disease managementprograms can help to ensure successful treatment.
PsychotherapyVarious types of psychotherapy have been used to treat
depression, including cognitive-behavioral therapy,interpersonal therapy, psychodynamic psychotherapy,problem-solving therapy and other behavior therapies, andmarital, family, and group therapy.8,37 Cognitive-behavioraltherapy and interpersonal therapy are the two forms ofpsychotherapy with the most documentation of benefit intreating depression.8 Cognitive-behavioral therapy challengesand reverses irrational beliefs and distorted attitudes towardthe self, the environment, and the future.8 It helps patientschange negative styles of thinking and behaving.11
Interpersonal therapy focuses on disturbed relationshipsthat cause and exacerbate depressive symptoms.11 Itfacilitates mourning after losses, resolves role disputes andtransitions, and overcomes deficits in social skills to reducesocial isolation and increase social support.8
Cognitive-behavioral therapy has been found to be aseffective as (or perhaps even more effective than)antidepressant drug therapy.8,38 Evidence suggests thatinterpersonal therapy and antidepressant drug therapy arecomparable in efficacy.8,39 However, the available comparativedata are insufficient to draw conclusions about the relativeeffectiveness of psychotherapy and antidepressant drugtherapies.40
Disease management programs can help improveaccess to psychotherapy services, which are critical toimproving patient self-management skills. This is where the
Appendix B. Natural History, Management, and Treatment of Depression
{Continued on next page}
[15]
Disease Managem
ent for Depression
use of disease management services can be especiallybeneficial; psychotherapy services often are not part ofmainstream health care services. A disease managementprogram can help integrate multiple types of services tooptimize patient care and ensure successful treatment ofdepression.
Acute PhaseAntidepressant drug therapy usually is best initiated
using a small dosage followed by gradual dosage increasesover the initial week or weeks to avoid or minimize adverseeffects.8 If a patient does not have at least a moderateimprovement in symptoms (i.e., if the patient has noresponse or a partial response) after 6 to 8 weeks ofantidepressant drug therapy despite the use of fulltherapeutic dosages, switching to another antidepressantagent should be considered.8
A goal of disease management is to improve thecoordination of services among the patient, physician,disease management organization, and other health careproviders. The acute phase of treatment can be a potentiallyvolatile phase and is key to successfully treating the patient.Coordinating care across health care providers at this phaseis critical to successfully managing the patient; diseasemanagement programs can help to optimize services so thatpatients can focus on adhering to their new medicationregimen.
Continuation PhasePatients who receive antidepressant drug therapy in the
acute phase should continue therapy using the same dosagefor 16 to 20 weeks after remission is achieved to preventrelapse.8 About 25% of patients will relapse within 2 monthsif therapy is not continued.8 Antidepressant drug therapyreduces relapse rates by at least 50%.41
Disease management programs are designed tooptimize patient self-management so that patients areempowered to adhere to their medication regimens. Diseasemanagement can promote adherence in the continuationphase to help prevent relapse.
Maintenance PhaseContinuing antidepressant drug therapy, psychotherapy,
or both on a long-term basis after the continuation phase may be considered for patients at high risk for recurrence.8
Full antidepressant dosages are used for maintenance
therapy.8 The duration of maintenance therapy depends onthe prognosis.41 For example, it may be 5 or more years forpatients at high risk for recurrence, and indefinite or lifelongfor patients with two or three episodes, each of whichoccurred within a year after discontinuing antidepressantmedication.41
Disease management programs facilitate medicationadherence in the maintenance phase and help preventrelapse and recurrence.
Discontinuation of TherapyThe decision to discontinue therapy is based on the risk
of recurrence.8 The dosage of antidepressants should begradually reduced over a period of at least several weeksbefore discontinuing therapy to allow for the detection ofemerging symptoms or recurrences and to preventmedication discontinuation syndromes (i.e., withdrawalsymptoms).8 These syndromes may be mistaken for or masksigns of a relapse because they affect mood, energy, sleep,and appetite.8
Patients should be monitored for signs of relapse orrecurrence over a period of several months afterdiscontinuation of therapy.8 Patient counseling shouldaddress the possibility of relapse or recurrence, the earlywarning signs, and what to do if these signs occur.
Disease management can provide services designed toenhance patient self-management skills. If the health careprovider and patient decide to discontinue therapy, theseskills enable the patient to reduce his or her risk of relapseand recognize the signs and symptoms of relapse and seektreatment.
Patient Self-ManagementSelf-management skills (e.g., recognizing the prodromal
symptoms that precede a relapse) are considered vital foreffectively treating depression.42 Developing a relapseprevention plan in the event that prodromal symptoms occuris recommended.
Disease management programs have services designedto enhance patient self-management and help patientsadhere to a strict medication and psychotherapy treatmentplan. Depending on the needs of the patient, diseasemanagement programs can encourage and facilitate thedevelopment of critical self-management skills.
Appendix B. Natural History, Management, and Treatment of Depression (continued)
The information in this appendix is adapted from the sources in Table 1, found on page 3 of this document.
[16]
Dise
ase
Man
agem
ent f
or D
epre
ssio
n
References1. Centers for Medicare and Medicaid Services. Discussion
of disease management. Available at:http://cms.hhs.gov/media/press/release.asp?Counter=418. Accessed October 1, 2002.
2. Disease Management Association of America. Definitionof disease management. Available at:http://www.dmaa.org/definition.html. Accessed August28, 2002.
3. National Pharmaceutical Council. Medicaid diseasemanagement & health outcomes. Available at:http://www.dmnow.org/. Accessed August 1, 2002.
4. Joint Commission on Accreditation of HealthcareOrganizations. Disease-specific care certification.Available at: http://www.jcaho.org/dscc/index.htm.Accessed October 24, 2002.
5. National Committee for Quality Assurance. NCQA diseasemanagement accreditation/certification information.Available at: http://www.ncqa.org/Programs/Accreditation/DM/dmmain.htm. Accessed October 24,2002.
6 Final NCQA DM accreditation standards hit the street. DMNews. December 25, 2001;7(5):1,4,5.
7. American Accreditation HealthCare Commission. URACAccreditation Programs. Available at: http://www.urac.org.Accessed May 22, 2003.
8. American Psychiatric Association. Practice guideline forthe treatment of patients with major depression (revision).Am J Psychiatry. 2000;157(4 suppl):1-45. Available at:http://www.psych.org/clin_res/Depression2e.book.cfm.
9. American Psychiatric Association. Diagnostic andStatistical Manual of Mental Disorders DSM-IV-TR (TextRevision). 4th ed. Washington, DC: American PsychiatricAssociation; 2000.
10. National Institute of Mental Health. The numbers count:mental disorders in America. Available at:http://www.nimh.nih.gov/publicat/numbers.cfm.Accessed September 23, 2002.
11. National Institute of Mental Health. Depression. Availableat: http://www.nimh.nih.gov/publicat/depression.cfm.Accessed August 29, 2002.
12. Crawford MJ, Prince M, Menezes P, Mann AH. Therecognition and treatment of depression in older people inprimary care. Int J Geriatr Psychiatry. 1998;13:172–176.
13. Docherty JP. Barriers to the diagnosis of depression inprimary care. J Clin Psychiatry. 1997;58(suppl 1):5–10.
14. Strategies for effective management of depression inprimary care. Based on a presentation by Michael S.Klinkman, MD. Am J Manag Care. 1999;5(13suppl):S783–S788.
15. Cole MG, Elie LM, McCusker J, Bellavance F, Mansour A.Feasibility and effectiveness of treatments for depressionin elderly medical inpatients: a systematic review. IntPsychogeriatr. 2000;12:453–461.
16. Katon W, Von Korff M, Lin E, et al. Population-based careof depression: effective disease management strategiesto decrease prevalence. Gen Hosp Psychiatry.1997;19:169–178.
17. Katz SJ, Kessler RC, Lin E, Wells KB. Medicationmanagement of depression in the United States andOntario. J Gen Intern Med. 1998;13:77–85.
18. Simon G, Ormel J, VonKorff M, Barlow W. Health carecosts associated with depressive and anxiety disorders inprimary care. Am J Psychiatry. 1995;152:352–357.
19. Unutzer J, Simon G, Belin TR, Datt M, Katon W, PatrickD. Care for depression in HMO patients aged 65 andolder. J Am Geriatr Soc. 2000;48:871–878.
20. Interest in depression DM programmes picking up in theUS. PharmacoEconomics and Outcomes News.2001;1(317):2.
21. Fulop G, Kelly MA, Robinson D Jr, et al. Opportunities fordepression disease management: a pharmacy benefitmanager’s experience. Depress Anxiety. 1999;10:61–67.
22. Burton WN, Conti DJ. Disability management: corporatemedical department management of employee health andproductivity. J Occup Environ Med.2000;42(10):1006–1012.
23. Burton WN, Chen CY, Conti, DJ, Schultz AB, EdingtonDW. The value of the periodic executive healthexamination: experience at Bank One and summary ofthe literature. J Occup Environ Med. 2002;44(8):737–744.
24. Wethington, E, Kessler RC. Employment, parentalresponsibility, and psychological distress: a longitudinalstudy of married women. J Fam Issues.1989;10(4):527–546.
25. Depression Guideline Panel. Depression in Primary Care:Volume 1. Detection and Diagnosis. Clinical PracticeGuideline, Number 5. Rockville, MD. U.S. Department ofHealth and Human Services, Public Health Service,Agency for Health Care Policy and Research; April 1993.AHCPR publication 93-0550.
26. Greenberg PE, Stiglin LE, Finkelstein SN, Berndt ER. Theeconomic burden of depression in 1990. J ClinPsychiatry. 1993;54:405–418.
27. Vodoor M, Southwell YP, Grubin M, et al. Themanagement of depression: the implications for managedcare—roundtable discussion: part 3. Manag CareInterface. 2000;suppl B:26–32.
28. Novartis Pharmacy Benefit Report: Facts & Figures. EastHanover, NJ: Novartis Pharmaceuticals Corporation;2002.
29. Goetzel RZ, Ozminkowski RJ, Sederer LI, Mark TL. Thebusiness case for quality mental health services: whyemployers should care about the mental health and well-being of their employees. J Occup Environ Med.2002;44:320–330.
30. Birnbaum JG, Cremieux PY, Greenberg PE, Kessler RC.Management of major depression in the workplace:impact on employee work loss. Disease Management &Health Outcomes. 2000;7:163–171.
[17]
Disease Managem
ent for Depression
31. Berndt ER, Finkelstein SN, Greenberg PE, et al.Workplace performance effects from chronic depressionand its treatment. J Health Econ. 1998;17:511–535.
32. Depression Guideline Panel. Depression in Primary Care:Volume 2. Treatment of Major Depression. ClinicalPractice Guideline, Number 5. Rockville, MD. U.S.Department of Health and Human Services, Public HealthService, Agency for Health Care Policy and Research;April 1993. AHCPR publication 93-0551.
33. Kupfer DJ. Long-term treatment of depression. J ClinPsychiatry. 1991;52:28–34.
34. Mynors-Wallis L, Gath D. Predictors of treatment outcomefor major depression in primary care. Psychol Med.1997;27:731–736.
35. Delgado PL. Depression: the case for a monoaminedeficiency. J Clin Psychiatry. 2000;61(suppl 6):7–11.
36. Leonard BE. Evidence for a biochemical lesion indepression. J Clin Psychiatry. 2000;(61 suppl 6):12–17.
37. Townsend E, Hawton K, Altman DG, et al. The efficacy ofproblem-solving treatments after deliberate self-harm:meta-analysis of randomized controlled trials with respectto depression, hopelessness and improvement inproblems. Psychol Med. 2001;31:979–988.
38. DeRubeis RJ, Gelfand LA, Tang TZ, Simons AD.Medications versus cognitive behavior therapy for severelydepressed outpatients: mega-analysis of four randomizedcomparisons. Am J Psychiatry. 1999;156:1007–1013.
39. Barkham M, Hardy GE. Counselling and interpersonaltherapies for depression: towards securing an evidence-base. Br Med Bull. 2001;57:115–132.
40. Gerson S, Belin TR, Kaufman A, Mintz J, Jarvik L.Pharmacological and psychological treatments fordepressed older patients: a meta-analysis and overviewof recent findings. Harv Rev Psychiatry. 1999;7:1–28.
41. Paykel ES. Continuation and maintenance therapy indepression. Br Med Bull. 2001;57:145–159.
42. Researchers hot on the trail of modest interventions toboost depression care. Dis Manag Advis. July2001;7(7):107–110.
43. National Committee for Quality Assurance. HEDIS‚ 2002summary table of measures, product lines and changes.Available at:http://www.ncqa.org/Programs/HEDIS/02measures.pdf.Accessed September 23, 2002.
44. Katon W, Von Korff M, Lin E, et al. Collaborativemanagement to achieve treatment guidelines. Impact ondepression in primary care. JAMA. 1995;273:1026–1031.
45. Katon W, Robinson P, Von Korff M, et al. A multifacetedintervention to improve treatment of depression in primarycare. Arch Gen Psychiatry. 1996;53:924–932.
46. Von Korff M, Katon W, Bush T, et al. Treatment costs,cost offset, and cost-effectiveness of collaborativemanagement of depression. Psychosom Med.1998;60:143–149.
47. Berger BA, Hudmon KS. Readiness for change:implications for patient care. J Am Pharm Assoc.1997;NS37:321–329.
48. Tutty S, Simon G, Ludman E. Telephone counseling as anadjunct to antidepressant treatment in the primary caresystem. A pilot study. Eff Clin Pract. 2000;3:170–178.
49. Simon GE, VonKorff M, Rutter C, Wagner E. Randomisedtrial of monitoring, feedback, and management of care bytelephone to improve treatment of depression in primarycare. BMJ. 2000;320:550–554.
50. Katon W, Rutter C, Ludman EJ, et al. A randomized trialof relapse prevention of depression in primary care. ArchGen Psychiatry. 2001;58:241–247.
51. Burns BJ, Ryan Wagner H, Gaynes BN, Wells KB,Schulberg HC. General medical and specialty mentalhealth service use for major depression. Int J PsychiatryMed. 2000;30:127–143.
52. Rost K, Nutting P, Smith J, Coyne JC, Cooper-Patrick L,Rubenstein L. The role of competing demands in thetreatment provided primary care patients with majordepression. Arch Fam Med. 2000;9:150–154.
53. Von Korff M, Katon W, Unutzer J, Wells K, Wagner EH.Improving depression care: barriers, solutions, andresearch needs. J Fam Pract. 2001;50:528.
54. Lewis L. The role of mental health patient organizations indisease management: focus on the US NationalDepressive and Manic-Depressive Association. DiseaseManagement & Health Outcomes. 2001;9:607–617.
55. Pignone MP, Gaynes BN, Rushton JL, et al. Screening fordepression in adults: a summary of the evidence for theU.S. Preventive Services Task Force. Ann Intern Med.2002;136:765–776.
56. Ustun TB, Kessler RC. Global burden of depressivedisorders: the issue of duration. Br J Psychiatry.2002;181:181–183.

The National Pharmaceutical Council1894 Preston White DriveReston, VA 20191-5433
Phone: 703-620-6390Fax: 703-476-0904www.npcnow.orgwww.dmnow.org
1DXM0110603
Related Documents











