DISCUSS THE OPERATION OF SIMPLE NEPHRECTOMY By Dr BADMUS A.M

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DISCUSS THE OPERATION OF SIMPLE NEPHRECTOMY
By Dr BADMUS A.M

OUTLINE
• Definition
• Indication
• Brief Anatomy
• Preoperative Evaluation
• Positioning and Anaesthesia
• Incision : Subcostal flank
11th & 12th Rib incision
Subcostal abdominal incision
Vertical abdominal incision
• Surgical technique
• Closure
• Post op care
• Complication
• Follow-up
• Others methods

Definition
• The term “simple nephrectomy” describes the technique of
removing the kidney from within Gerota’s fascia and in no
manner is meant to indicate that the operation is technically
easy.
• This procedure is usually performed in the setting of a non-
neoplastic disease state

Indications
The more common specific indications include
1. severe trauma
2. Renal infections (e.g., Xanthogranulomatous pyelonephritis
and emphysematous pyelonephritis).
3. Nonfunctioning kidneys with stones or obstruction.
4. Renal vascular hypertension (when all attempts at medical
and surgical therapy have failed).
5. Renal fistula.
6. Transplantation
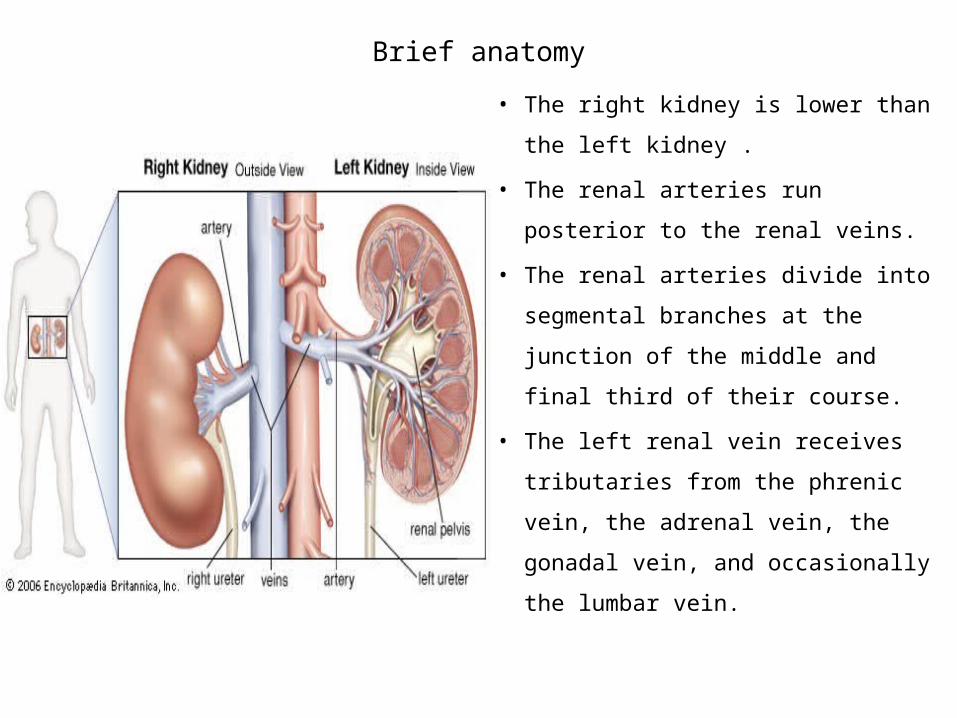
Brief anatomy
• The right kidney is lower than the
left kidney .
• The renal arteries run posterior to
the renal veins.
• The renal arteries divide into
segmental branches at the junction
of the middle and final third of their
course.
• The left renal vein receives
tributaries from the phrenic vein,
the adrenal vein, the gonadal vein,
and occasionally the lumbar vein.
Preoperative Evaluation
The preoperative evaluation has two purposes
• Full history and thorough physical examination
• An IVP (now CT Urogram more appropriate) .
• In indeterminate cases, a nuclear renogram may be required to
demonstrate sufficient renal function.
• The scout film of the IVP is useful for determining the level of a flank
incision. Note which rib is superimposed on the middle of the lateral
border of the kidney.
• An appropriate flank incision should be made at the level of this rib or
above.

• History of pulmonary disease is essential The decubitus position with an elevated kidney rest can decrease the vital
capacity by 20%. In the decubitus position, there is also preferential ventilation of the upper
lung and perfusion of the lower lung.
• Traumatic injury must be done through an abdominal approach.
• In an obese patient, a flank approach optimizes exposure and minimizes wound complications.
• Previous abdominal surgery also favors a flank approach.
• An extraperitoneal flank approach is preferable in a patient with a chronically infected kidney.
• In other cases, the choice of incision depends largely on the surgeon’s preference.

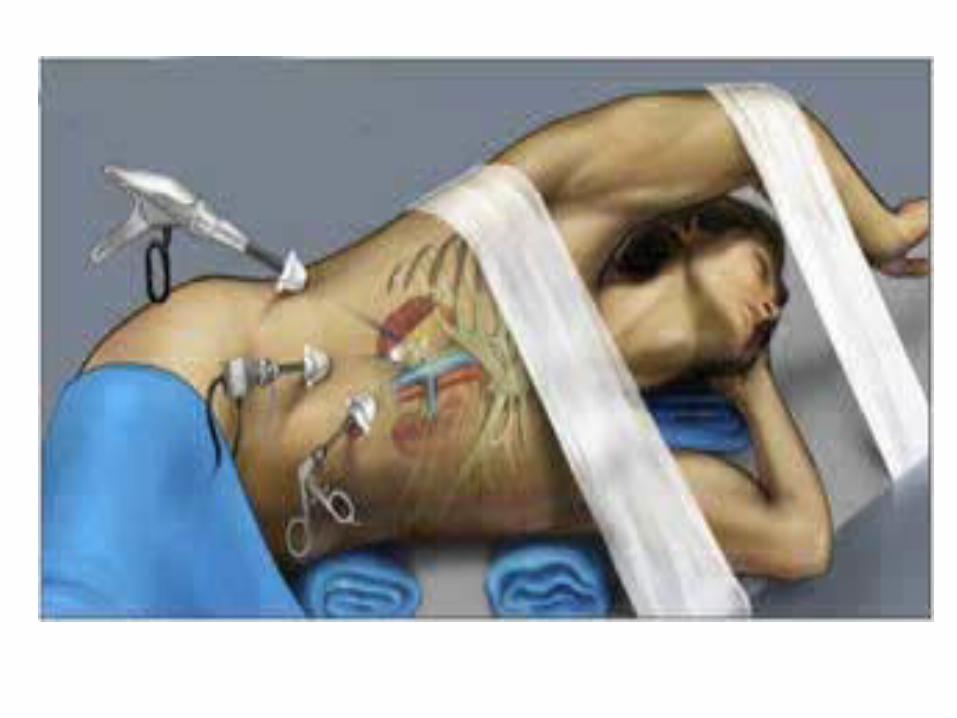
Positioning

• The patient is placed on the operating table so that the kidney rest is just cephalad to the anterior superior iliac spine.
• The patient is turned to the lateral decubitus position with his or her back toward the edge of the table.
• The contralateral leg is flexed and padded at the knee and ankle. • The ipsilateral leg is appropriately padded with pillows and kept only gently
flexed.
• The table is then flexed, and the kidney rest elevated. • The patient should then be secured to the table with 2-inch tape over the
patient’s hip.
• The patient should have an axillary roll placed to avoid brachial plexus injury, and upper extremities should be secured to arm board and sling support or Mayo stand.

Subcostal flank Incision• The incision is made approximately 2 cm inferior to the 12th rib starting
posterior to the angle of the 12th rib or at the inferior border of the paraspinous muscles.
• The incision usually is gently curved toward the umbilicus to the lateral edge of the rectus muscle.
• The latissimus dorsi and external oblique are divided with cautery, exposing the serratus posterior inferior and the internal oblique, which are then divided.
• A small incision in the lumbodorsal fascia provides access to the retroperitoneum.
• The peritoneum is dissected medially off the transversalis fascia with blunt dissection.
• The transversus can then be divided with cautery or bluntly divided between the muscle fibers.
11th and 12th Rib Incision• An 11th or 12th rib resection may be preferred if the kidney is high up. • The patient is positioned as detailed above for the flank subcostal
approach.
• The incision is made over the selected rib from the costovertebral angle over the tip of the rib medially to the edge of the rectus muscle.
• Once the rib is exposed, the periosteum is incised along the length of the rib.
• The periosteum is dissected off the rib using the periosteal elevator and the Alexander periosteotome.
• The Doyen periosteal elevator is guided beneath the rib to complete the dissection posteriorly.
• Once free, the rib can be divided with a rib cutter, and the edges
smoothed with a rongeur.
• The posterior periosteum is divided, exposing the fascial attachments
of the pleura to the diaphragm.
• The peritoneum is bluntly dissected from the deep surface of the
transversalis fascia by sweeping it medially with the fingers. The medial
extent of the incision, including the external oblique, the internal
oblique, and the transversus, can now be completed.
Subcostal Abdominal Incision• The subcostal abdominal incision is preferred by some surgeons because of:
1.Early exposure of the renal pedicle
2.Lower risk of inadvertent pleurotomy
3.Decreased effect on ventilation in patients with pulmonary disease
• The patient is positioned with the table break at the level of the 12th rib, and
the operative side is elevated with a rolled sheet. The table is then flexed to
maximize exposure.
• The incision is typically two fingerbreadths below the costal margin with its
medial extent being approximately two fingerbreadths below the xyphoid
process.
• After the skin incision, the anterior rectus fascia is divided along with
the rectus muscle and the external oblique.
• The superior epigastric artery is divided. The internal oblique is divided.
• The lumbodorsal fascia is incised laterally, and the peritoneum can be
opened or bluntly stripped off the anterior abdominal wall.
• The transversus can then be divided with cautery or bluntly divided
between the muscle fibers.
• If peritoneum is opened, one must reflect the colon medially to expose
Gerota’s fascia, which is then incised
Vertical Abdominal Incision• This incision is typically from the xyphoid process to the pubic symphysis.
• After incision of the skin and subcutaneous fat, the linea alba is identified and incised.
• The peritoneum can be identified beneath preperitoneal fat and is incised sharply and carefully to avoid bowel injury.
• The colon is reflected medially to expose Gerota’s fascia.
• In a patient who has suffered renal trauma, it is important to obtain early vascular
control by dissecting along the aorta for a left renal injury and along the inferior vena
cava for a right renal injury.
• The dissection is carried superiorly to the level of the renal vessels. Vessel loops are
placed around the renal artery and vein before exploration of the injured kidney.

Nephrectomy• After Gerota’s fascia is incised and the kidney is dissected free from
surrounding perinephric fat.
• The renal artery should be identified. One must keep in mind possible aberrant vessels, particularly lower-pole branches.
• Ligation of the artery before the vein prevents renal congestion and is thus preferred.
• Two size-0 silk ties are placed proximally, and a single silk is placed distally. The artery is divided with scissors; a scalpel is used when there is minimal distance between the proximal and distal ligatures.
• To minimize the possibility that the proximal tie will slip off the arterial stump, some surgeons place a suture ligature distal to the 0 silk ties.
• The ureter is quickly identified by blunt dissection in the fat inferior to the kidney.
• It is divided between ligatures or clips. The connective tissue and lymphatics are
dissected off the kidney, revealing the renal vein.
• On the left, particular attention is paid to the gonadal vein, inferior adrenal vein,
and lumbar venous branches. These branches are divided between silk ties if distal
to the area dissected.
• The renal vein is doubly ligated, as was the artery.
• The adrenal gland can be dissected off with sharp dissection, taking care to clip all vessels.
• If the nephrectomy is secondary to an infectious process, a drain is left in the posterior flank.

Subcapsular Approach
• In patients undergoing simple nephrectomy for stone disease or for
infection, previous surgery or chronic inflammation can make dissection
very difficult.
• In these cases, it is advantageous to come down to the capsule, incise it,
and continue the dissection under the capsule to the hilus.
• It is important to remember that the renal vessels have already divided
into several branches once they reach the renal hilum and to continue
searching for additional arterial branches once the apparent main
branch has been divided.
Closure• There is general agreement that the abdominal portion of a flank wound should be closed in
two layers.
• The bean bag is deflated, the kidney rest is lowered, and the flexion is taken out of the table.
• The closure should be initiated at each end of the incision and continued toward the middle of the incision.
• Anteriorly, the internal oblique is closed with a running PDS suture.
• In the posterior portion of the wound, the inferiorly reflected periosteum is approximated to the periosteum and intercostal muscle of the superior rib.
• When the rib has been resected, the periosteum and intercostal muscles above and below the rib are approximated.
• The latissimus dorsi fascia is then closed in continuity with the external oblique fascia using a running PDS suture.
• A single-layer closure is often sufficient over the ribs

Post-op Care
• Antibiotics
• IV fluid
• Analgesic
• Chest X-ray
• Sequential compression devices +TED stockings
• Incentive spirometry
• Ambulate from 1DPO
• Removal of urethral catheter

Complications
• Superficial wound infection
• DVT
• Iathrogenic colonic injury
• Bleeding and re-exploration
• Pneumonia
• Pneumothorax
• Paralytic ileus
• Septicemia

Laparoscopic Simple nephrectomy
• For this procedure, 3 to 5 small incisions (5-12 mm) are placed into the
abdomen.
• A telescope connected to a camera and several working instruments
are passed through these “keyholes”.
• This allows the surgeon to have an enlarged view of inside the body on
a video monitor to guide him through the procedure. The kidney is
freed from surrounding organs and placed in a sterile retrieval bag and
removed through a small incision for the pathologist to evaluate for an
accurate diagnosis.


Related Documents











![Novel technique: direct access partial nephrectomy ...nuf.nu/NoRenCa/Novel technique direct access... · of its equivalent oncological results compared to radical nephrectomy [3].](https://static.cupdf.com/doc/110x72/606c80ba9bb7de31a926ad1d/novel-technique-direct-access-partial-nephrectomy-nufnunorencanovel-technique.jpg)