9/24/2015 1 Page 1 ©2013 Hill-Rom Services, Inc. ALL RIGHTS RESERVED 184229 Zinc: US-AC-0313-0123w ©2013 Hill-Rom Services, Inc. ALL RIGHTS RESERVED 184229 Zinc: US-AC-0313-0123w Advancing Early Mobility in Critical Care: Evidence Based Strategies for Making it Happen Created in Conjunction With Kathleen M. Vollman, MSN, RN, CCNS, FCCM, FAAN/[email protected] Disclosures • Sage Products Speaker Bureau & Consultant • Eloquest Healthcare Speaker Bureau & Consultant • Hill-Rom Speaker Bureau & Consultant

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
9/24/2015
1
Page 1
©2013 Hill-Rom Services, Inc. ALL RIGHTS RESERVED184229 Zinc: US-AC-0313-0123w
©2013 Hill-Rom Services, Inc. ALL RIGHTS RESERVED
184229Zinc: US-AC-0313-0123w
Advancing Early Mobility in Critical Care: Evidence Based Strategies for Making it HappenCreated in Conjunction With Kathleen M. Vollman, MSN, RN, CCNS, FCCM, FAAN/[email protected]
Disclosures
• Sage Products Speaker Bureau & Consultant
• Eloquest Healthcare Speaker Bureau & Consultant
• Hill-Rom Speaker Bureau & Consultant
9/24/2015
2
• Create the link of patient advocacy to mobilizing critically ill patients
• Understand the importance of early patient mobility
• Recognize the traditional standards of care for patient mobility– Identify current practice patterns
• Understand institutional costs associated with immobility
• Recognize what evidence supports the use of early mobility
• Determine how to implement an early mobility protocol
• Strategies for creating sustainability
Learning Objectives
Notes on Hospitals: 1859
“It may seem a strange principle to enunciate as the very first requirement in a Hospital that it should do the sick no harm.”
Florence Nightingale
Advocacy = SafetyNightingale F. Notes on Hospitals. Third Edition [Online]. London: Longman; 1863.Available from: http://www.archive.org/stream/notesonhospital01nighgoog
9/24/2015
3
PROTECT THE PATIENT FROM BAD THINGS HAPPENING ON YOUR WATCH
Interventional Patient Hygiene
• Hygiene…the science and practice of the establishment and maintenance of health
• Interventional Patient Hygiene….nursing action plan directly focused on fortifying the patients host defense through proactive use of evidence based hygiene care strategies
Incontinence Associated Dermatitis Prevention
Program
9/24/2015
4
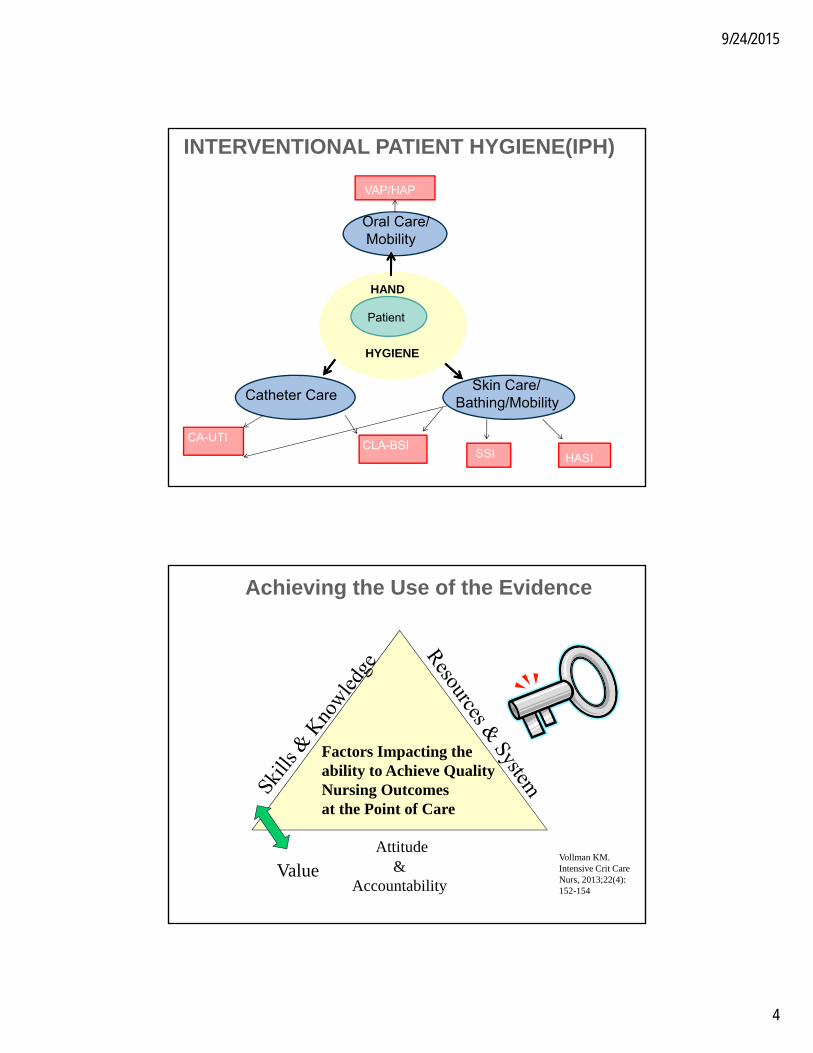
INTERVENTIONAL PATIENT HYGIENE(IPH)
Oral Care/ Mobility
VAP/HAP
Catheter Care
CA-UTICLA-BSI
Skin Care/ Bathing/Mobility
HASISSI
HAND
HYGIENE
Patient
Vollman KM. Intensive Crit Care Nurs, 2013;22(4): 152-154
Attitude &
Accountability
Factors Impacting theability to Achieve QualityNursing Outcomesat the Point of Care
Achieving the Use of the Evidence
ValueVollman KM. Intensive Crit Care Nurs, 2013;22(4): 152-154
9/24/2015
5
Why Is Early Patient
Mobility Important?
12
6
39
“Teach us to live that we may dread,Unnecessary time in bed,Get people up and we may save,Our patients from an early graved”
RAJ Asher
RAJ. The dangers of going to bed. British Medical Journal,1947 December 13
9/24/2015
6
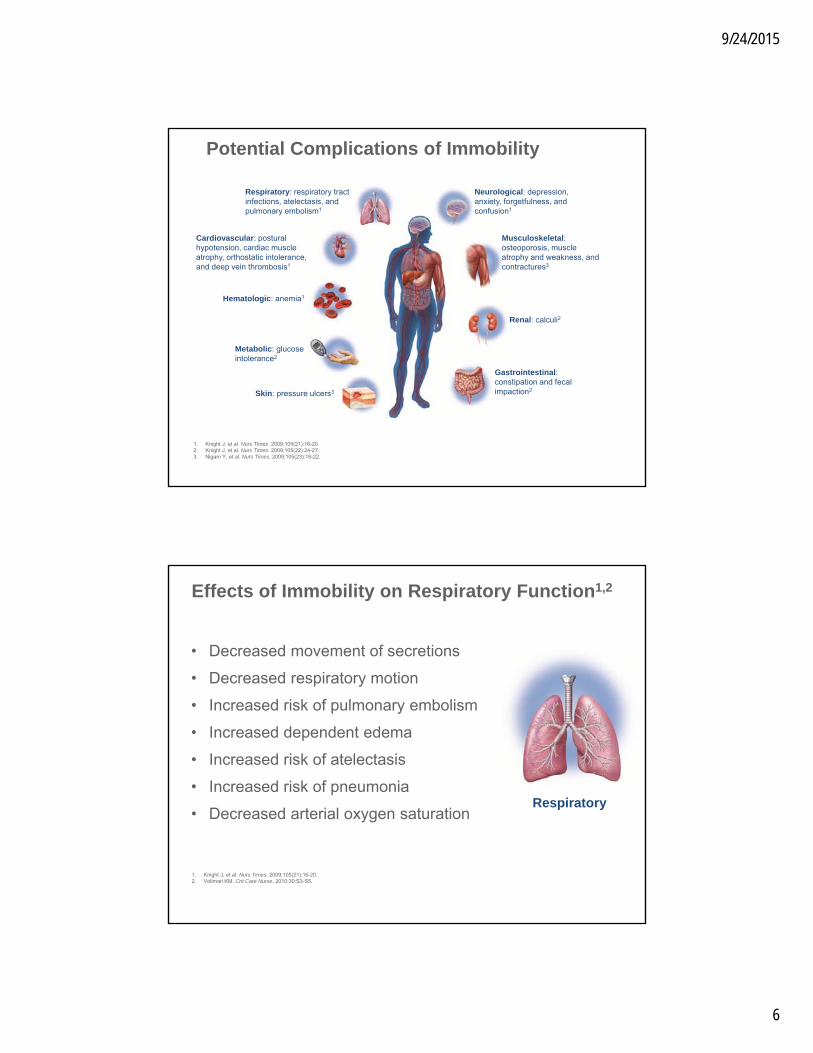
Respiratory: respiratory tract infections, atelectasis, and pulmonary embolism1
Cardiovascular: postural hypotension, cardiac muscle atrophy, orthostatic intolerance, and deep vein thrombosis1
Hematologic: anemia1
Metabolic: glucose intolerance2
Skin: pressure ulcers3
Neurological: depression, anxiety, forgetfulness, and confusion1
Musculoskeletal: osteoporosis, muscle atrophy and weakness, and contractures3
Renal: calculi2
Gastrointestinal: constipation and fecal impaction2
1. Knight J, et al. Nurs Times. 2009;105(21):16-20.2. Knight J, et al. Nurs Times. 2009;105(22):24-27.3. Nigam Y, et al. Nurs Times. 2009;105(23):18-22.
Potential Complications of Immobility
• Decreased movement of secretions
• Decreased respiratory motion
• Increased risk of pulmonary embolism
• Increased dependent edema
• Increased risk of atelectasis
• Increased risk of pneumonia
• Decreased arterial oxygen saturation
Effects of Immobility on Respiratory Function1,2
1. Knight J, et al. Nurs Times. 2009;105(21):16-20.2. Vollman KM. Crit Care Nurse. 2010;30:S3-S5.
Respiratory
9/24/2015
7
• In North America– In the United States, the Centers for Disease
Control (CDC), through the National Healthcare Safety Network, has reported critical care unit VAP rates, per 1,000 ventilator-days, ranging from 0.2 (pediatric cardiothoracic) to 4.4 (burn ICU)2
– On average, ICU patients with VAP had an additional 10.5-day LOS3
– Per case: VAP $40,144. (95% CI, %36,286-$44,220)4
Ventilator-Associated Pneumonia (VAP) Rates
1. Rosenthal VD, et al. Am J Infect Control. 2012;40(5):396-407.2. Dudeck MA, et al. National Healthcare Safety Network (NHSN) Report, Data Summary for 2012, Device-Associated Module. American Journal
of Infection Control. 2013,41:1148-66.3. Restrepo MI, et al. Infect Control Hosp Epidemiol. 2010;31(5):509-515.4. Zimlichman E. et al. JAMA Internal Med, 2013;173(22):2039-465. Accessed 10/2013 at http://www.phac-aspc.gc.ca
Respiratory
The CDC defines ventilator-associated events (VAE) as deterioration in respiratory status after a period of stability, possible infection/inflammation, and laboratory evidence of respiratory infection.
Ventilator-Associated Events-Not a New Definition for VAP
Device-associated module: ventilator-associated event protocol. NHSN website. http://www.cdc.gov/nhsn/PDFs/pscManual/10-VAE_FINAL.pdf. Accessed 2/22/13.
Before:
VAP was the only VAE that the National Healthcare Safety Network (NHSN) collected data on
Now:
NHSN has revised its policy to include surveillance of all VAE, including
• Ventilator-associated conditions (VAC)• Infection-related ventilator-associated complications (IVAC)• Possible and probable VAP
Patient criteria for VAE surveillance• Included patients: mechanically-ventilated patients ≥18 years
who have an event on or after calendar day 3 of mechanical ventilation
• Excluded patients: patients receiving rescue therapies)
9/24/2015
8
Cardiovascular
1. Winkelman C. AACN Adv Crit Care. 2009;20:254-266. 2. Knight J, et al. Nurs Times. 2009;105(21):16-20.3. Harms MP, et al. Exp Physiol. 2003;88:611-616.4. Sjostrand T. Physiol Rev. 1953;33:202-228.
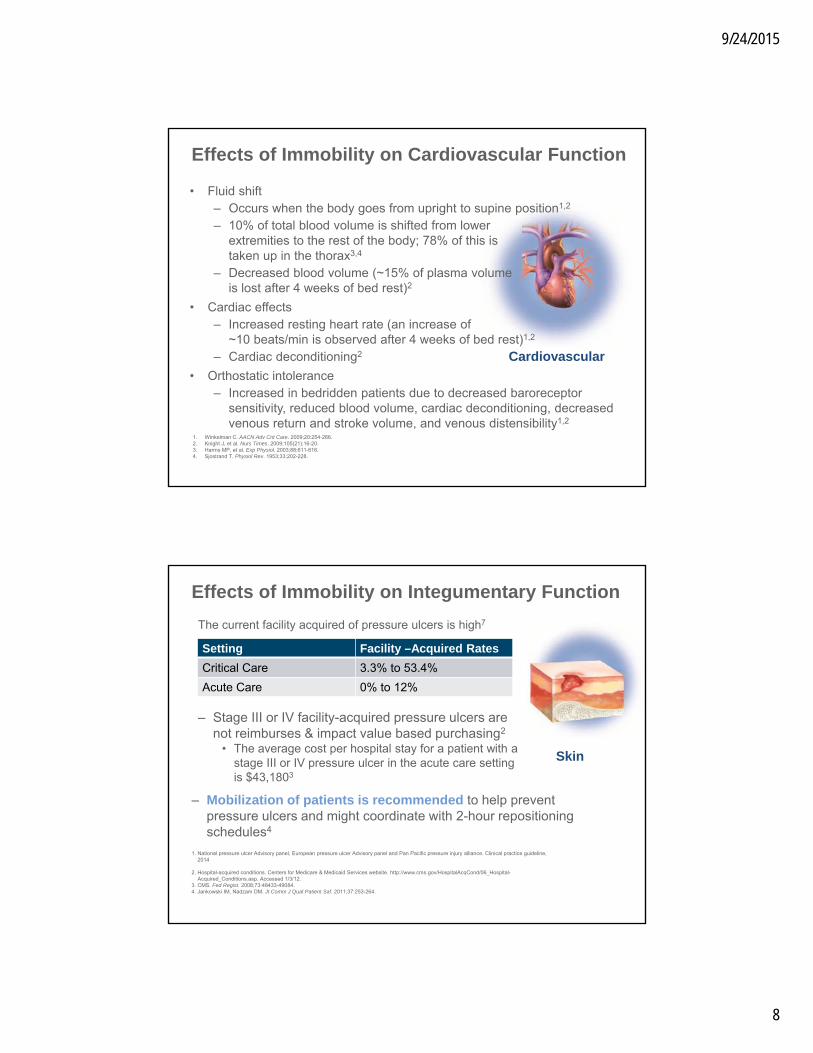
• Fluid shift– Occurs when the body goes from upright to supine position1,2
– 10% of total blood volume is shifted from lower extremities to the rest of the body; 78% of this is taken up in the thorax3,4
– Decreased blood volume (~15% of plasma volume is lost after 4 weeks of bed rest)2
• Cardiac effects– Increased resting heart rate (an increase of
~10 beats/min is observed after 4 weeks of bed rest)1,2
– Cardiac deconditioning2
• Orthostatic intolerance– Increased in bedridden patients due to decreased baroreceptor
sensitivity, reduced blood volume, cardiac deconditioning, decreased venous return and stroke volume, and venous distensibility1,2
Effects of Immobility on Cardiovascular Function
The current facility acquired of pressure ulcers is high7
– Stage III or IV facility-acquired pressure ulcers are not reimburses & impact value based purchasing2
• The average cost per hospital stay for a patient with a stage III or IV pressure ulcer in the acute care setting is $43,1803
Effects of Immobility on Integumentary Function
Skin
1. National pressure ulcer Advisory panel, European pressure ulcer Advisory panel and Pan Pacific pressure injury alliance. Clinical practice guideline, 2014
2. Hospital-acquired conditions. Centers for Medicare & Medicaid Services website. http://www.cms.gov/HospitalAcqCond/06_Hospital-Acquired_Conditions.asp. Accessed 1/3/12.
3. CMS. Fed Regist. 2008;73:48433-49084.4. Jankowski IM, Nadzam DM. Jt Comm J Qual Patient Saf. 2011;37:253-264.
– Mobilization of patients is recommended to help prevent pressure ulcers and might coordinate with 2-hour repositioning schedules4
Setting Facility –Acquired Rates
Critical Care 3.3% to 53.4%
Acute Care 0% to 12%
9/24/2015
9
• Muscle wasting (almost half of the normal muscle strength is lost after 3-5 weeks of bed rest)1,2
• Change in type or density of muscle fibers (muscle protein synthesis decreases by 50% after 2 weeks of bed rest)2
• Muscle wasting occurs early & rapidly during first week of critically illness3
– protein synthesis & protein breakdown
– Severity increased with multiple organ failure
• Separate phenotypes of muscle atrophy1
– Primary: bed rest, space flight, limb casting, and denervation
– Secondary: pathology
Effects of Immobility on Skeletal Muscle
Musculoskeletal
1. Morris PE. Crit Care Clin. 2007;23:1-20.2. Nigam Y, et al. Nurs Times. 2009;105(23):18-223. Puthucheary ZA, et al. JAMA 2013;310(15):1591-1600
• During immobilization, the muscle groups involved with transferring and posture lose strength most quickly (shoulders, hip girdle)1,2,4
• After less than a day of immobility, contractures start to develop. After 2-3 weeks of immobility, firmer contractures develop, and after 2-3 months of immobility, surgical correction may be needed2
• Recovering from muscle atrophy caused by immobility takes ~4 weeks. With exercise, disuse weakness is reversed at a rate of ~6%/week2
• Respiratory muscle weakness may occur 4 & is a predictor for prolonged mechanical ventilation and delayed weaning3
Effects of Immobility on Skeletal Muscle (Cont.)
Musculoskeletal
1. Topp R, et al. AACN Clin Issues. 2002;13(2):263-276.2. Nigam Y, et al. Nurs Times. 2009;105(23):18-22.3. De Jonghe B, et al. Crit Care Med. 2007;35(9):2007-2015.4. Kress JP, Hall JB. N Engl J Med, 2014;370:1626-1635
9/24/2015
10
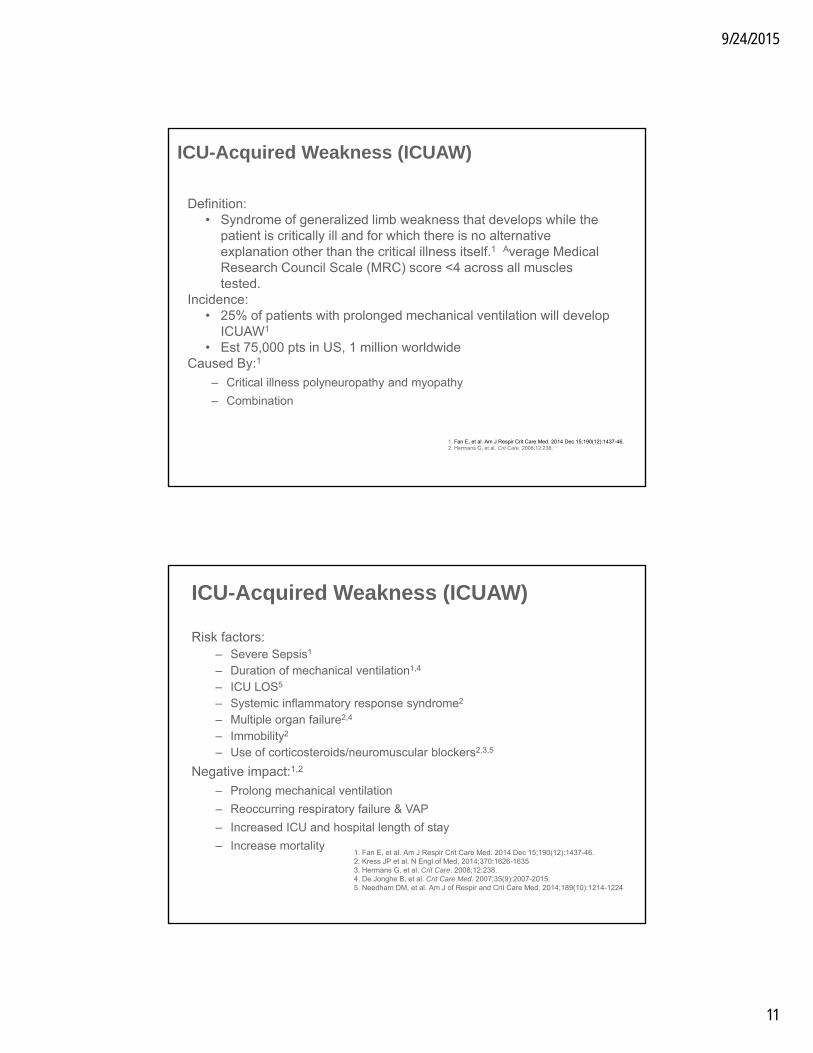
• Delirium1
– Acute, fluctuating change in consciousness and cognition
– Develops over a brief time period
– Hyperactive or hypoactive (most common)
– Associated with higher mortality3,4
• Depression2
• Anxiety2
• Forgetfulness2
• Confusion2
Effects of Immobility on Neurological Function
Neurological
1. Vasilevskis EE, et al. Chest. 2010;138:1224-1233.2. Knight, et al. Nurs Times. 2009;105(21):16-20.3. Ely EW, et al. JAMA 2004;291:1753-17624. Pisani MA, et al. AM J Resp Crit Care Med 2009;180:1092-1097
Neurological: depression, anxiety, forgetfulness, and confusion1
Brain-ICU Study
• Multicenter RCT- medical-surgical ICU’s
• 821 patients with ARF or Shock
• Evaluated in-hospital delirium and cognitive impact 3-12 months post d/c
Results
• 74% of patients developed delirium during hospital stay
• 3 months: 40% had global cognition scores 1.5 SD below population mean, 26% had scores 2 SD below pop mean
• 12 months: 34%(older) & 24%(younger) global cognition scores below the mean
Pandharipande, PP. et al. N Engl J Med;369:1306:1316
1 out of 4 cognitive
Impairment at 12
months
9/24/2015
11
Definition: • Syndrome of generalized limb weakness that develops while the
patient is critically ill and for which there is no alternative explanation other than the critical illness itself.1 Average Medical Research Council Scale (MRC) score <4 across all muscles tested.
Incidence:• 25% of patients with prolonged mechanical ventilation will develop
ICUAW1
• Est 75,000 pts in US, 1 million worldwideCaused By:1
– Critical illness polyneuropathy and myopathy
– Combination
ICU-Acquired Weakness (ICUAW)
1. Fan E, et al. Am J Respir Crit Care Med. 2014 Dec 15;190(12):1437-46.2. Hermans G, et al. Crit Care. 2008;12:238.
Risk factors:– Severe Sepsis1
– Duration of mechanical ventilation1,4
– ICU LOS5
– Systemic inflammatory response syndrome2
– Multiple organ failure2,4
– Immobility2
– Use of corticosteroids/neuromuscular blockers2,3,5
Negative impact:1,2
– Prolong mechanical ventilation
– Reoccurring respiratory failure & VAP
– Increased ICU and hospital length of stay
– Increase mortality
ICU-Acquired Weakness (ICUAW)
1. Fan E, et al. Am J Respir Crit Care Med. 2014 Dec 15;190(12):1437-46.2. Kress JP et al. N Engl of Med, 2014;370:1626-16353. Hermans G, et al. Crit Care. 2008;12:238.4. De Jonghe B, et al. Crit Care Med. 2007;35(9):2007-2015.5. Needham DM, et al. Am J of Respir and Crit Care Med. 2014;189(10):1214-1224

9/24/2015
12
• Society of Critical Care Medicine: Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the ICU1
– “Recommend performing early mobilization of adult ICU patientswhenever feasible to reduce the incidence and duration of delirium
• AACN Practice Alert: Delirium Assessment and Management2
– Strategies to decrease delirium risk factors should be used, including early exercise
SCCM and ACCN Practice Guidelines to Address Delirium
1. Barr J, et al. Crit Care Med. 2013;41(1):263-306.2. AACN practice alert: delirium assessment and management.
http://www.aacn.org/WD/practice/docs/practicealerts/delirium-practice-alert-2011.pdf. Accessed 02/25/13.
Effects of Immobility: Conclusion
Because the consequences of immobility and bed rest
are so severe, mobilizingcritically ill patients early
appears to have merit.–K.M. Vollman
Vollman KM. Crit Care Nurse. 2010;30:S3-S5.
9/24/2015
13
• Early mobility/rehabilitation is associated with a decrease in the incidence and duration of delirium, as well as numerous adverse effects on the different body systems
• Benefits of early mobility appear to be associated with reduced time on the ventilator, shorter hospital LOS and lower mortality rates.
• In addition, early mobility can improve quality of life after the ICU stay
Summary: Importance of Early Patient Mobility
Early mobility in critically ill patients is essential to the prevention of complications associated with immobility
What Are Some Traditional
Standards of Care for
Patient Mobility?
9/24/2015
14
What Are Some Traditional Standards of Care for Patient Mobility?
The old standby physician order…The old standby physician order…
Traditional intervention• Every 2 hours*• Manual turning• Head of bed at 30°
Traditional intervention• Every 2 hours*• Manual turning• Head of bed at 30°
Pressure ulcers and pneumonia
Out of bedto chair
*Although 80%-90% of surveyed ICU physicians believe that every-2-hour turning should occur, only 57% of them believe that it is currently happening in their ICU.1
1. Krishnagopalan S. Crit Care Med. 2002;30:2588-2592.
How Well Are We Really Doing?Every-2-Hour Turning
9/24/2015
15
Methodology
• 74 patients/566 total hours of observation
• 3 tertiary hospitals
• Change in body position recorded every 15 minutes
• Average observation time 7.7 hours
• Online MD survey
Results
• 49.3% of observed time no body position change for > 2 hours
• 2.7% had an every-2-hour demonstrable body position change
• 80% to 90% believed every-2-hour position change should occur, but only 57% believed it happened in their ICU
Body Position: Clinical Practice vs Standard
Krishnagopalan S. Crit Care Med. 2002;30:2588-2592.
Positioning Prevalence
• Prospectively recorded, 2 days, 40 ICUs in the UK
• Analysis on 393 sets of observations
• Turn defined as supine position to a right or left side lying
• Five patients prone at any time, 3.8% (day 1) and 5% (day 2) rotating beds
• Patients on back 46% of observation
• Left 28.4%
• Right 25%
• Head up 97.4%
• Average time between turns 4.85 hours (3.3 SD)
• No significant association between time and age, weight, height, respiratorydiagnosis, intubation, sedation score, day of week, nurse/patient ratio, hospital
Goldhill DR, et al. Anaesthesia. 2008;63:509-515.
Results:
Methodology:

9/24/2015
16
• Heavier patients1*
• Patients receiving vasopressors*
• Patients receiving a paralytic agent at least once1
• Trauma patients with multiple fractures or high intracranial pressure1
• Fear of line dislodgement• Heavy sedation• Patient comfort• Human and technological resources• Fear of further decreases in oxygenation or
hemodynamic parameters
Potential Barriers to Early Mobilization
1. Schallom L, et al. Am J Crit Care. 2005;14:476-478.2. Morris PE. Crit Care Clin. 2007;23:1-20.* *not statistically significant
Patients noted to be turned less
Perceived patient and environmental barriers to mobilizing ICU patients2:
EBP Recommendations to Achieve Offloading & Reduce Pressure
• Turn & reposition (avoid positioning patients on a pressure ulcer)– Repositioning should be undertaken to reduce the duration &
magnitude of pressure over vulnerable areas– Cushioning devices to maintain alignment /30 ° side-lying &
prevent pressure on boney prominences– Use lifting device or other aids to reposition & make it easy to
achieve the turn• Do not leave moving and handling equip underneath the
patient– Assess whether actual offloading has occurred
National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel. And Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Emily Haesler (Ed,) Cambridge Media: Perth, Australia; 2014.American Nurses Association. Safe patient handling and mobility: Interprofessional national standards. Silver Spring, MD: author; 2013

9/24/2015
17
• Every-2-hour turning is considered the current practice to help offset the effects of immobility
• Keeping the head of bed at 30°-45° is an intervention to help prevent VAP
Summary: Traditional Standards of Care
What Are the Average Costs of
Immobility for Organizations?

9/24/2015
18
In the United States:• >6,000 ICU beds1
• >5 million patients admitted annually to the ICUs1
• ICU patients represent 10% of admissions but 30% of hospital costs2
• Average mortality in ICUs is 10%-29%1
• Average LOS in the ICU is 6.1-9.3 days1
ICU Statistics
1. Society of Critical Care Medicine. Critical care statistics in the United States. Mount Pleasant, IL: Society of Critical Care Medicine; 2012. http://www.sccm.org/SiteCollectionDocuments/StatisticsBroch_d4.pdf. Accessed 7/27/12.
2. Pendergraft TB, et al. Ann Allergy Asthma Immunol. 2004;93:29-35.3. Rhodes A, et al. Intensive Care Med. 2012;38:1647-1653. 4. Vincent J, et al. Crit Care Med. 2006;34:344-353.5. Edbrooke DL, et al. Crit Care. 2011;15:R56.
Unplanned ICU Readmissions
Reintubation is associated
with increased
risk of developing
VAP2,3
Average ICU readmission
rate of 7% and average
ICU daily costs of $3,1841,4
ICU readmissions
have twicethe average
hospital LOS1
Hospital death rates
are 1.5-10 times
higher1
1. Rosenberg AL, Watts C. Chest. 2000;118:492-502. 2. Torres A, et al. Am J Respir Crit Care Med. 1995;152:137-141. 3. Elward AM, et al. Pediatrics. 2002;109:758-764.4. Dasta JF, et al. Crit Care Med. 2005;33(6):1266-71.5. Emerson CB, et al. Infect Control Hosp Epiemiol, 2012:33:539-544
Respiratory complications are the major
reason1
Development of an HAI is associated
with readmission of 27days6

9/24/2015
19
• Single center retrospective cohort study of 9405 consecutive patients admitted from an acute care hospital to an inpatient rehab
• Functional status on admission to rehab was assessed (FIM score) and categorized into low, middle and high functional status
• Results– 13% readmission rate– Low and middle FIM score was significantly associated with readmission in
comparison to high FIM scores across diagnostic categories– Medical patients with the lowest functional status had the highest readmission rate
Functional Status at Discharge: Impact on Readmission
The Centers for Medicare and Medicaid Services will reduce payments to hospitals with excess readmissions
(admissions within 30 days of discharge)2
FIM= functional independent measure
1.Hoyer EH, et. al. Journal of Hospital medicine. 2014;9:277-2822. Readmissions reduction program. CMS website. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed.
In the United States:• Acute care facility-acquired pressure ulcer rate: 0-12%1
• 60,000 deaths from facility-acquired pressure ulcer complications per year2
• Average cost of facility-acquired stage III or IV pressure ulcers: $43,1803
• $11 billion per year in preventable costs4
Impact of Pressure Ulcers
1. National pressure ulcer Advisory panel, European pressure ulcer Advisory panel and Pan Pacific pressure injury alliance. Clinical practice guideline, 2014
2. Courtney BA, et al. Nurs Manage. 2006;37:36,38,40.3. CMS Office of Public Affairs. Fact sheet: CMS proposes additions to list of hospital-acquired conditions for fiscal year 2009.
Baltimore, MD: Centers for Medicare & Medicaid Services; 4/14/08. 4. Reddy M, et al. JAMA. 2006;296:974-984.5. Phillips L, Buttery J. Nurs Times. 2009;105:34-36.6. Bennett G, et al. Age Ageing. 2004;33:230-235.

9/24/2015
20
Quality Implications
1. 2014 clinical quality measures tipsheet. http://www.cms.gov/RegulationsandGuidance/Legislation/EHRIncentivePrograms/Downloads/ClinicalQualityMeasures Tipsheet.pdf. 2. FY2009 quality measure reporting for 2010 payment update. http://www.cms.gov/Medicare/Quality-Initiatives-Patient-AssessmentInstruments/
HospitalQualityInits/Downloads/HospitalRHQDAPU200808.pdf. 3. CMS quality measurement programs characteristics. http://www.cms.gov/medicare/quality-initiatives-patient-assessmentinstruments/qualitymeasures/
downloads/cmsqualitymeasurementprogramscharacteristics.pdf. 4. Readmissions reduction program. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. 5. Hospital value-based purchasing program. CMS website. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/
Hospital_VBPurchasing_Fact_Sheet_ICN907664.pdf.6. 2015 Patient Safety Goals http://www.jointcommission.org/assets/1/6/2015_HAP_NPSG_ER.pdf
• Increasing number of quality measures1
• CMS financial pressures for quality reporting2,3
• Excessive readmission penalties begin in 20134
Centers for Medicare & Medicaid Services
(CMS)
• CMS-based program
• Started in October 2012
• Pay-for-performance
• CMS will withhold in 2015 1.5% of payments and redistribute the money based on how well hospitals meet quality measures compared to baseline measures
CMS Value-Based Purchasing5
• National patient safety goals for 2015:
– Patient identification– Infection prevention– Medication safety– Effective
communication– Surgical mistakes– Patient safety risks
The Joint Commission6
• ICU patients represent a disproportionate amount of hospital costs
• Respiratory complications are the major reason for unplanned ICU readmissions– ICU readmissions average longer hospital LOS and higher
mortality rates
• Facility-acquired pressure ulcers represent a large preventable cost
• There may be long-term financial implications associated with poor performance with regard to healthcare safety indicators through the CMS Value-Based Purchasing Program
Summary: Institutional Costs Associated With Immobility

9/24/2015
21
It is not enough to do your best; you must know what to do, and THEN do your best.
–W. Edwards Deming
Introduction to Early Mobility
9/24/2015
22
• Early mobility definition:– Planned movement in a sequential manner beginning at a patient’s
current mobility status and returning the patient to baseline
• Early mobility includes:– Head elevation– Manual turning– Passive and active range of motion– Continuous lateral rotation therapy/prone positioning– Movement against gravity– Physiologic adaptation to an upright/leg down position (Tilt Table,
bed egress)– Chair position– Dangling– Ambulation
Definition of Early Mobility1
1. Vollman KM. Crit Care Nurse. 2010;30:S3-S5.
What Does Clinical Evidence
Tell Us About Early Mobility?

9/24/2015
23
1
3
2
4
Start at the Top: Which Head of Bed Is at 30°?1
1. Garcia R. Presented at: APIC. 2004.
The Clinical Impact of 45° Head of Bed on Ventilator-Associated Pneumonia (VAP)1
1. Drakulovic MB, et al. Lancet. 1999;354:1851-1858.
Number of patients 86
Patient populationMonitored clinically suspected and microbiologically confirmed nosocomial pneumonias
InterventionRandomly assigned to:• Supine position (n=47)• Head of bed 45° (n=39)
Results
• Microbiologically confirmed nosocomial pneumonia lower in the semirecumbent group, 2/39 (5%) vs 11/47 (23%)
• Supine position and enteral nutrition were independent risk factors for VAP and had the greatest number of VAP cases 14/28 (50%)
9/24/2015
24
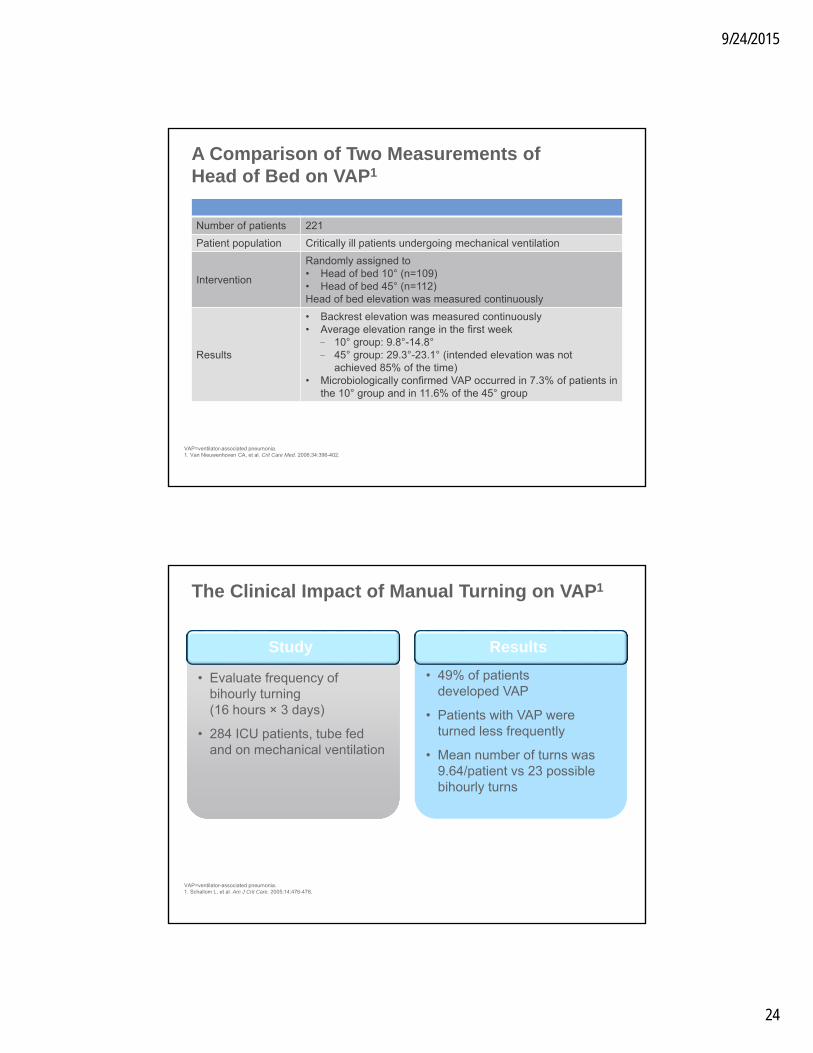
A Comparison of Two Measurements of Head of Bed on VAP1
Number of patients 221
Patient population Critically ill patients undergoing mechanical ventilation
Intervention
Randomly assigned to• Head of bed 10° (n=109)• Head of bed 45° (n=112)Head of bed elevation was measured continuously
Results
• Backrest elevation was measured continuously• Average elevation range in the first week
- 10° group: 9.8°-14.8°- 45° group: 29.3°-23.1° (intended elevation was not
achieved 85% of the time)• Microbiologically confirmed VAP occurred in 7.3% of patients in
the 10° group and in 11.6% of the 45° group
VAP=ventilator-associated pneumonia.1. Van Nieuwenhoven CA, et al. Crit Care Med. 2006;34:396-402.
• Evaluate frequency of bihourly turning (16 hours × 3 days)
• 284 ICU patients, tube fed and on mechanical ventilation
• Evaluate frequency of bihourly turning (16 hours × 3 days)
• 284 ICU patients, tube fed and on mechanical ventilation
Study
• 49% of patients developed VAP
• Patients with VAP were turned less frequently
• Mean number of turns was 9.64/patient vs 23 possible bihourly turns
• 49% of patients developed VAP
• Patients with VAP were turned less frequently
• Mean number of turns was 9.64/patient vs 23 possible bihourly turns
Results
The Clinical Impact of Manual Turning on VAP1
VAP=ventilator-associated pneumonia.1. Schallom L, et al. Am J Crit Care. 2005;14:476-478.

9/24/2015
25
• CLRT mechanism of action– A gentle side-to-side, full-body motion of the patient in which one
lung is placed above the other– This motion allows for gravitational flow and mobilization of
pulmonary secretions, as well as enhance gas exchange
• What impact does it have on gas exchange?– Increased oxygen– Decreased CO2
– Improved blood flow– Decreased atelectasis
• What happens inside the airways when patients are turned?
Continuous Lateral Rotation Therapy
Table-Based vs Cushion-Based Rotation
• Turning on the long axis
• Measured in degrees of angle/turn– 124° (62° per side) in 3.5 minutes
• Unstable spine patients
• Rotates patient by inflation/deflation of air cushions
• Longitudinal, full-body rotation
• Measured in percent of air bladder inflation

9/24/2015
26
Key Differences
Table-Based Rotation
• Ideally suited for patients with unstable heads, necks, and spines (neuro and trauma patients)1
• Uses a firm mattress essential for maintenance of spine alignment1– Can potentially put skin integrity
at risk
• Can be set by degree of angle desired– Requires 2 fixed planes to
accurately determine angle– Table-based products can
achieve this as both the surface and the frame are moving at the same angle
Cushion-Based Rotation
• Usually does not require transfer to a different surface, allowing it to be initiated more readily
• More user-friendly for clinicians1
• Beds may include additional features such as assist modes for patient positioning1
1. Basham KA, et al. Respir Care Clin N Am. 1997;3:109-134.
Cross Section of a Chest in the Supine Position
Rib
HeartLung
Bronchi
Spine
PulmonaryInfiltrates
Sternum
9/24/2015
27
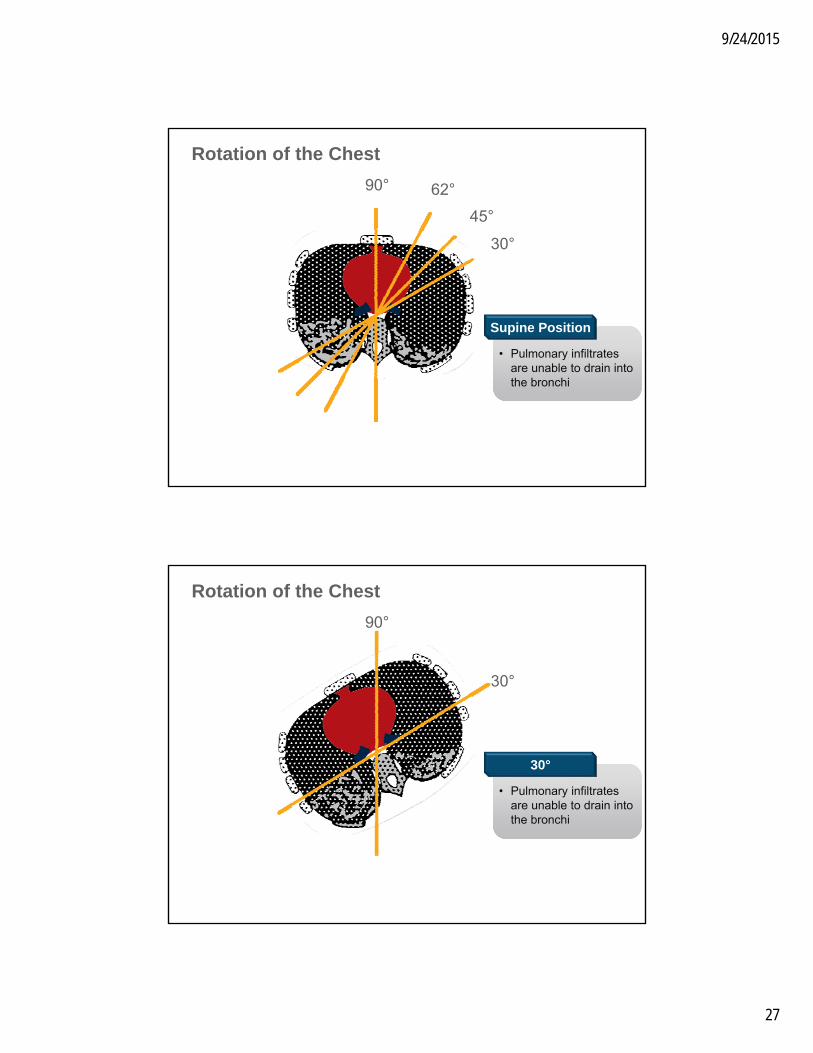
Rotation of the Chest
90°
45°
30°
62°
• Pulmonary infiltrates are unable to drain into the bronchi
• Pulmonary infiltrates are unable to drain into the bronchi
Supine Position
• Pulmonary infiltrates are unable to drain into the bronchi
• Pulmonary infiltrates are unable to drain into the bronchi
Rotation of the Chest
90°
30°
30°

9/24/2015
28
• Pulmonary infiltrates are unable to drain into the bronchi
• Pulmonary infiltrates are unable to drain into the bronchi
Rotation of the Chest
90°
45°
45°
Rotation of the Chest
90° 62°
• Some amount of drainage of pulmonary infiltrates into the bronchi
• Some amount of drainage of pulmonary infiltrates into the bronchi
62°
9/24/2015
29
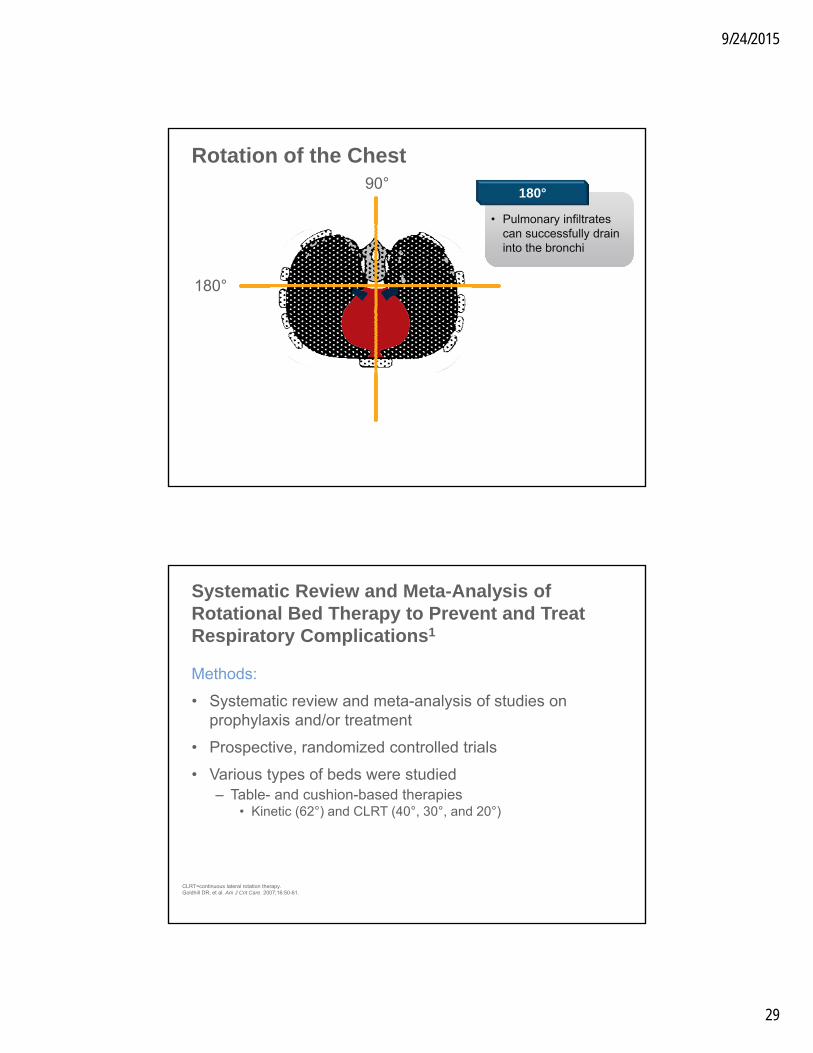
Rotation of the Chest
180°
90°
• Pulmonary infiltrates can successfully drain into the bronchi
• Pulmonary infiltrates can successfully drain into the bronchi
180°
Methods:
• Systematic review and meta-analysis of studies on prophylaxis and/or treatment
• Prospective, randomized controlled trials
• Various types of beds were studied– Table- and cushion-based therapies
• Kinetic (62°) and CLRT (40°, 30°, and 20°)
Systematic Review and Meta-Analysis of Rotational Bed Therapy to Prevent and Treat Respiratory Complications1
CLRT=continuous lateral rotation therapy.Goldhill DR, et al. Am J Crit Care. 2007;16:50-61.
9/24/2015
30
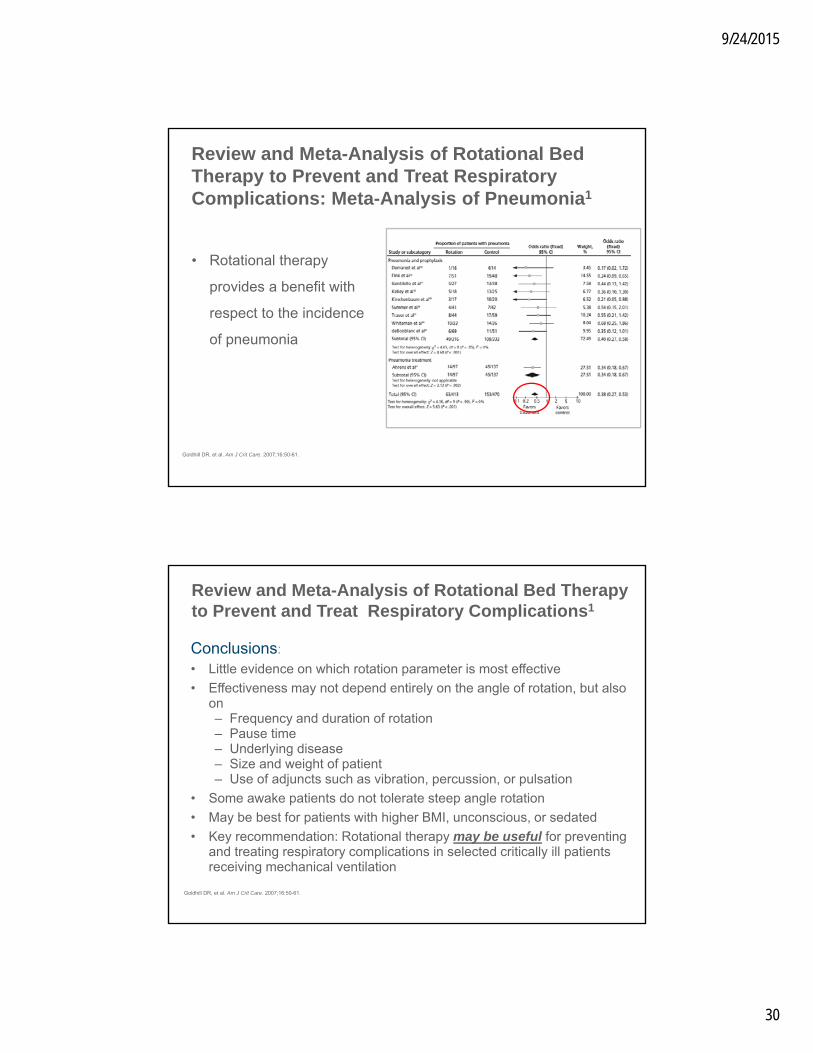
• Rotational therapy
provides a benefit with
respect to the incidence
of pneumonia
Review and Meta-Analysis of Rotational Bed Therapy to Prevent and Treat Respiratory Complications: Meta-Analysis of Pneumonia1
Goldhill DR, et al. Am J Crit Care. 2007;16:50-61.
Conclusions:
• Little evidence on which rotation parameter is most effective
• Effectiveness may not depend entirely on the angle of rotation, but also on– Frequency and duration of rotation– Pause time– Underlying disease– Size and weight of patient– Use of adjuncts such as vibration, percussion, or pulsation
• Some awake patients do not tolerate steep angle rotation
• May be best for patients with higher BMI, unconscious, or sedated
• Key recommendation: Rotational therapy may be useful for preventing and treating respiratory complications in selected critically ill patients receiving mechanical ventilation
Review and Meta-Analysis of Rotational Bed Therapy to Prevent and Treat Respiratory Complications1
Goldhill DR, et al. Am J Crit Care. 2007;16:50-61.

9/24/2015
31
• The Medical Center of Central Georgia evaluated the impact of CLRT
• A CLRT protocol was implemented in patients who were identified as at risk for pulmonary complications, and outcomes were compared with a historical comparison group
• When introduced early, CLRT may reduce critical care length of stay and cost to treat
• CLRT is an option for patient mobility
Rotational Therapy Using Cushion-Based Rotation
Vent Days ICU DaysHospital
Days
Cost to Treat, Thousands of
Dollars
ICU Readmission
Rates, %
Reintubation Rates, %
No CLRT 17.4 18.4 29.7 59.4 21 19
CLRT after 48 hours
16.6 18.9 28.8 62.1 17 13
CLRT within 48 hours
12.4 13.1 23.4 45.2 4 4
CLRT=continuous lateral rotation therapy.No CLRT: 75 patients; CLRT after 48 hours: 46 patients; CLRT within 48 hours: 50 patients.Swadener-Culpepper L, et al. Crit Care Nurs Q. 2008;31:270-279.
• Methodology– Prospective randomized controlled trial, 3 medical ICUs at a single center– Eligible if ventilated <48 hours and free from pneumonia, ALI, or in ARDS– 150 patients with 75 in each group– 35 patients with CLRT allocated to undergo percussion before suctioning– Measures to prevent VAP were standardized for both groups including
head of bed
• Results: CLRT vs control– VAP: 11% vs 23% P=0.048– Ventilation duration: 8 ± 5 days vs 14 ± 23 days, P=0.02– LOS: 25 ± 22 vs 39 ± 45 days, P=0.01– Mortality: no difference
CLRT to Prevent VAP: Controlling the Variables1
ALI=acute lung injury; ARDS=acute respiratory distress syndrome; CLRT=continuous lateral rotation therapy; VAP=ventilator-associated pneumonia.Staudinger T, et al. Crit Care Med. 2010;38:486-490.
9/24/2015
32
• Introduction of CLRT into patient care can provide an efficient way of providing early mobility to those critically ill patients whose condition or instability prevents implementation of other forms of mobility1,2
Introducing CLRT Into Patient Care
Systematic method of approaching placement and removal of CLRT therapy… a protocol
CLRT=continuous lateral rotation therapy.1. Swadener-Culpepper L, et al. Crit Care Nurs Q. 2008;31:270-279.2. Basham KA, et al. Respir Care Clin N Am. 1997;3:109-134.
• Target high-risk patient populations– Pulmonary-hemodynamic instability with manual turning– FiO2 50% or more– Positive end-expiratory pressure (PEEP) 8 or more– Existing pulmonary complications– FiO2 increases by 20% (20 points) or PEEP >3 cm H2O from baseline within 2
calendar days
• Which patients should NOT receive CLRT?– Those with unstable spines– Those with long bone fractures or patients requiring traction– Those with unstable intracranial pressure– Marked agitation without therapeutic management– Those with severe, uncontrolled diarrhea and patients that weigh more than 300lbs
Moving Those Who Cannot Move Themselves: Which Patients Should Receive CLRT?
CLRT=continuous lateral rotation therapy.Swadener-Culpepper L, et al. Crit Care Nurs Q. 2008;31:270-279.Basham KA, et al. Respir Care Clin N Am. 1997;3:109-134.
9/24/2015
33
• Assess for potential complications frequently– Malposition of endotracheal tube– Positional transient desaturation– Positional hemodynamic instability
• Every 2 hours check to see if patient is in optimal position to promote effective turn
• Every 2 hours manually turn patient and evaluate skin and lungs, then resume rotational therapy
• Document in medical record: degree of rotation, pause time settings, hours of rotation, turn for skin check and lung evaluation every 2 hours
• Discontinue CLRT when the patient:– May be mobilized safely using other means (head of bed, chair position, out-of-bed chair,
and/or ambulation)– Shows improvement in respiratory status– Has agitation that is not therapeutically managed
Ongoing Monitoring/Evaluation and Documentation
CLRT=continuous lateral rotation therapy.
• Early CLRT intervention
• The therapy must be driven by a protocol and changes in settings are nursing orders
• Monitor initial rotation cycle to ensure one lung is above the other
• Automation of rotation requires insertion of usual assessment practices
• Minimum of 18 hours per day and 6 cycles per hour
• If done incorrectly, can cause skin injury– Shorter pause times– Assessment to ensure one lung above the other– Every two-hour assessment of the lungs and skin
• Yearly competency-based education to ensure proper use of the therapy
CLRT Strategies for Success
CLRT=continuous lateral rotation therapy.

9/24/2015
34
Prone Positioning: 2013 Evidence
• RCT 466 patients with severe ARDS (26 ICU’s in France/1 Spain)– Severe ARDS P/F ratio < 150 mm Hg, with Fio2 0.6, PEEP of at least
5 cm of water, & a Vt of 6 ml per kg of PBW– Initiation 12-24hrs
• Prone-positioning 16hrs/or supine position/ (proned within 1hr of randomization)
• NMB used 5 days
• Stopping prone treatment– After 4hrs in supine meeting oxygenation criteria– in PaO2/FiO2 ratio of 20% (after 2 consecutive prone positions)– Complications leading to immediate interruption
• Applied for 28 days, then clinician discretion
Guerin C. et al. N Engl J Med, 2013, 368(23): 2159-2168
Results: Guerin C, et. al. Prone Study
• Results:– Baseline characteristics similar
except for, vasopressors (S), sepsis related SOFA score (S) & use of NMB’s (P)
– Prone 16% mortality, supine 32.8% p< 0.0001
– Prone group ICU LOS (2 days, & VFD (4 days) (NS)
– No differences in complications except > cardiac arrest in supine position (31 S vs. 16 P)
Guerin C. et al. N Engl J Med, 2013, 368(23): 2159-2168
9/24/2015
35
• When muscles are immobilized in shortened positions, there is remodeling of muscle fibers
• Bed rest entails immobilization of limb extensor muscles in shortened positions
• Passive movement has been shown to enhance ventilation, prevent contractures in patients in high-dependency units
• Low-resistance multiple repetition muscle training can augment muscle mass and strength
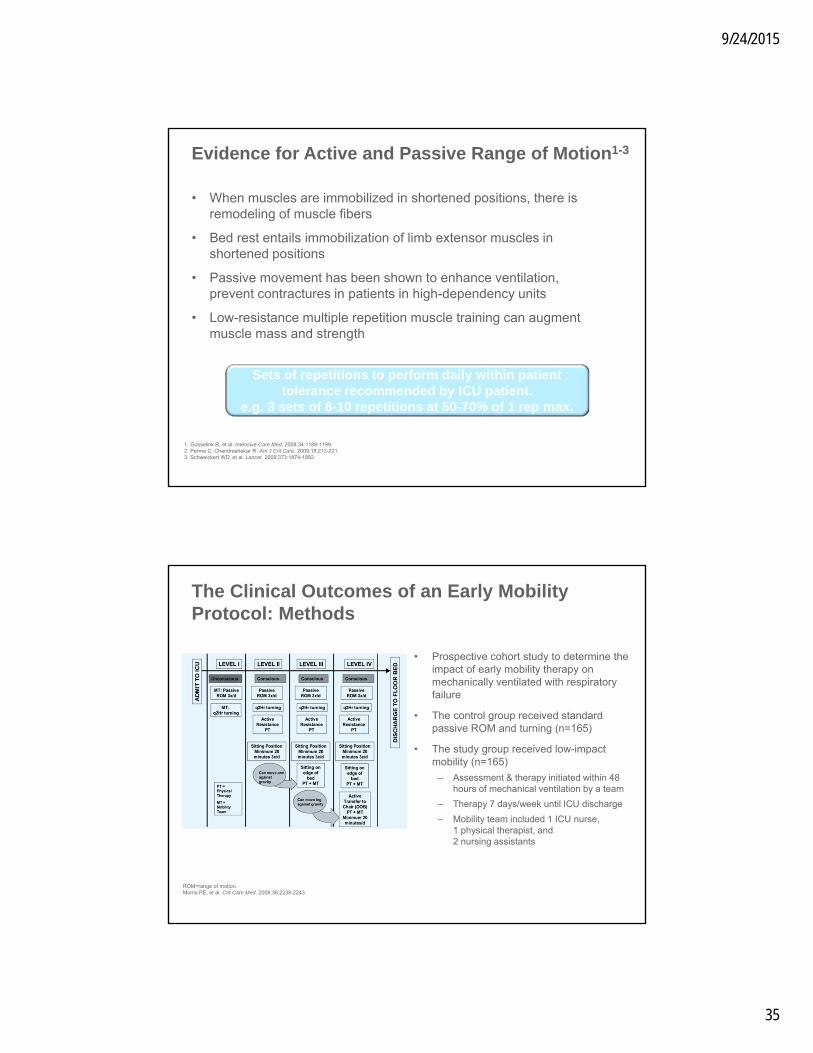
Evidence for Active and Passive Range of Motion1-3
1. Gosselink R, et al. Intensive Care Med. 2008;34:1188-1199.2. Perme C, Chandrashekar R. Am J Crit Care. 2009;18:212-221.3. Schweickert WD, et al. Lancet. 2009;373:1874-1882.
Sets of repetitions to perform daily within patient tolerance recommended by ICU patient.
e.g. 3 sets of 8-10 repetitions at 50-70% of 1 rep max.
• Prospective cohort study to determine the impact of early mobility therapy on mechanically ventilated with respiratory failure
• The control group received standard passive ROM and turning (n=165)
• The study group received low-impact mobility (n=165)
– Assessment & therapy initiated within 48 hours of mechanical ventilation by a team
– Therapy 7 days/week until ICU discharge
– Mobility team included 1 ICU nurse, 1 physical therapist, and 2 nursing assistants
The Clinical Outcomes of an Early Mobility Protocol: Methods
ROM=range of motion.Morris PE, et al. Crit Care Med. 2008;36:2238-2243.
9/24/2015
36
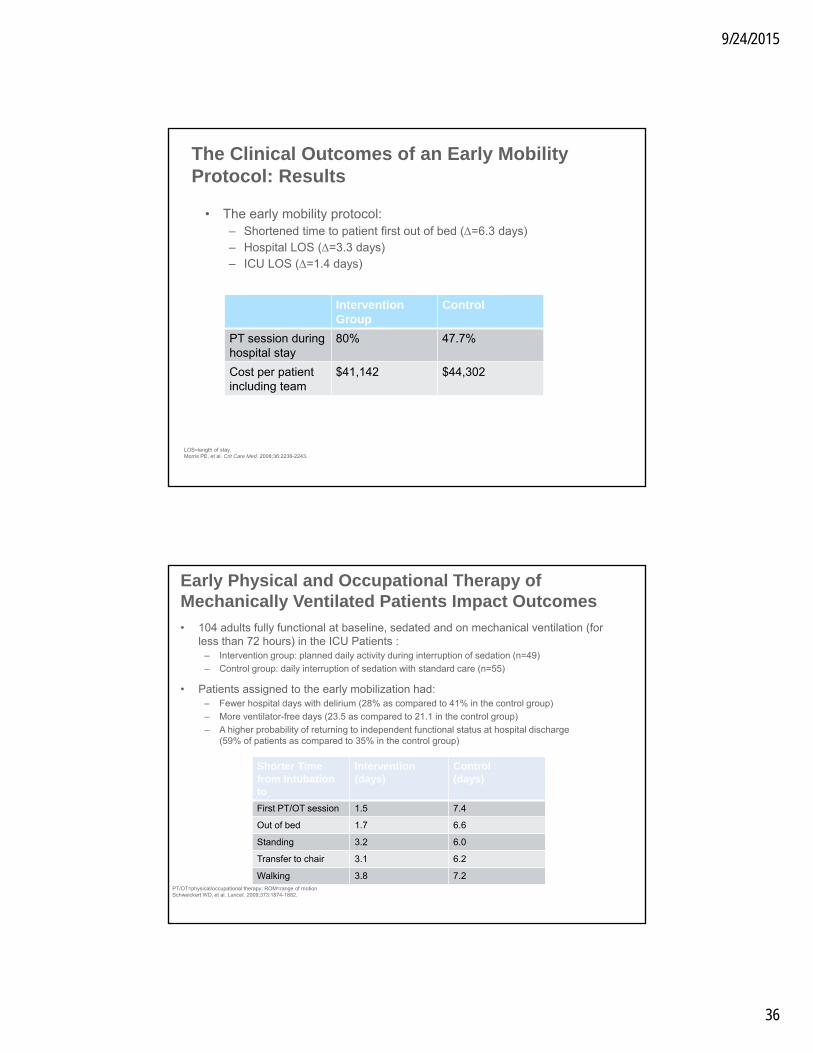
• The early mobility protocol:– Shortened time to patient first out of bed (=6.3 days)– Hospital LOS (=3.3 days)– ICU LOS (=1.4 days)
The Clinical Outcomes of an Early Mobility Protocol: Results
LOS=length of stay.Morris PE, et al. Crit Care Med. 2008;36:2238-2243.
InterventionGroup
Control
PT session during hospital stay
80% 47.7%
Cost per patient including team
$41,142 $44,302
• 104 adults fully functional at baseline, sedated and on mechanical ventilation (for less than 72 hours) in the ICU Patients :
– Intervention group: planned daily activity during interruption of sedation (n=49)
– Control group: daily interruption of sedation with standard care (n=55)
• Patients assigned to the early mobilization had:– Fewer hospital days with delirium (28% as compared to 41% in the control group)
– More ventilator-free days (23.5 as compared to 21.1 in the control group)
– A higher probability of returning to independent functional status at hospital discharge (59% of patients as compared to 35% in the control group)
Early Physical and Occupational Therapy of Mechanically Ventilated Patients Impact Outcomes
PT/OT=physical/occupational therapy; ROM=range of motion.Schweickert WD, et al. Lancet. 2009;373:1874-1882.
Shorter Time from Intubationto
Intervention (days)
Control (days)
First PT/OT session 1.5 7.4
Out of bed 1.7 6.6
Standing 3.2 6.0
Transfer to chair 3.1 6.2
Walking 3.8 7.2
9/24/2015
37
• Manual turning, 30°-45° head of bed, continuous lateral rotation therapy, passive and active range of motion, as well as sitting in the chair and ambulating are part of early patient mobility
• Early activity is feasible and safe in patients with respiratory failure
Summary: Clinical Evidence for Early Patient Mobility
Overcoming Barriers to
Early Mobility
9/24/2015
38
• Patients noted to be turned less often1:– Heavier patients*
– Patients receiving vasopressors*
– Patients receiving a paralytic agent at least once– Trauma patients with multiple fractures or high intracranial pressure
• Perceived patient and environmental barriers to mobilizing ICU patients2,4:– Fear of line dislodgement– Heavy sedation– Patient comfort– Human and technological resources
• Weaning patients served as their own control.– Out of Bed chair 55-80° vs 40-60 ° : No difference in ABG’s, respiratory or
hemodynamic values3
– Fear of further decreases in oxygenation or hemodynamic parameters
Potential Barriers to Early Mobilization
1. Schallom L, et al. Am J Crit Care. 2005;14:476-478.2. Morris PE. Crit Care Clin. 2007;23:1-20.3. Thomas P, et al. Heart & Lung. 2014;43:105-1114. Jolley SE, et al. BMC Anesthesiology,. 2014;14:1-9* *not statistically significant
• 103 patients who are mechanically ventilated for >4 days
• Mobility team included registered nurse, physical therapist, respiratory therapist, and care technician
• Patients assessed upon admission and daily for readiness
• Activity begins when patient exhibits physiologic stability
• Sedation reduced and oxygen levels supported
• Measures of activity related adverse events Fall to knees, systolic blood pressure >200 or <90 mm Hg, oxygen desaturation <80% and/or extubation, and/or tube removal
Feasibility and Safety of Early Activity in Patients With Acute Respiratory Failure: Methods
Bailey P, et al. Crit Care Med. 2007;35:139-145.

9/24/2015
39
• Measured 1,449 activity events
• Sit on bed (16%), sit in chair (31%), and ambulate (53%)
• Patients with an endotracheal tube in place had 593 activity events– 249 (42%) were ambulated
• 69% survivors ambulated >100 feet at respiratory ICU discharge
• <1% activity-related adverse events
Feasibility and Safety of Early Activity in Patients With Acute Respiratory Failure: Results
Photo courtesy of Bailey P, et al. Crit Care Med. 2007;35:139-145.Bailey P, et al. Crit Care Med. 2007;35:139-145.
• Methods:– Study included 49 ICU patients who had been mechanically ventilated for <72 hours
43% of the patients had ARDS on ICU admission– Patients received daily sedative interruption and were screened for the safety of PT/OT
• PT/OT progressed from passive/active range of motion through bed mobility exercises followed by sitting at the edge of the bed, balance activities, ADLs, transfers, and finally ambulation
• Results:– Average time from intubation to initial therapy was 1.5 days– Therapy occurred on
• 87% of total eligible days on study• 90% of days on mechanical ventilation• 90% of days in the ICU while not on mechanical ventilation
– Patients had ICU delirium during 53% of sessions– Adverse events only occurred during 16% of all PT/OT sessions, including desaturation
≥5%, heart rate increase, ventilator asynchrony/tachypnea, agitation/discomfort, and device removal
Feasibility and Safety of Early Activity in Mechanically Ventilated Patients
ARDS=acute respiratory distress syndrome; PT/OT=physical/occupational therapy.Pohlman MC, et al. Crit Care Med. 2010;38:2089-2094.
9/24/2015
40
• Published literature on safe use of early mobilization with various patient populations
• Continuous renal replacement therapy1,2
• Extracorporeal membrane oxygenation3,4
• Burns5
• Abdominal surgery6
Yes…. They Can Be Mobilized
1. Wang YT, et al. Critical Care. 2014;18:R1612. Talley, et al. Critical Care Nursing Quarterly. 2013 36(1):89-1003. Abrams D, et al. Critical Care. 2014;18:R384. Freeman R, et al. Critical Care Nursing Quarterly. 2013 36(1):73-885. Taylor S, et al. Critical Care Nursing Quarterly. 2013 36(1):56-626. Havey R, et al. Critical Care Nursing Quarterly. 2013 36(1):63-72
• Lateral turn results in a 3%-9% decrease in SVO2, which takes 5-10 minutes to return to baseline
• Appears the act of turning has the greatest impact on any instability seen
• Minimize factors that contribute to imbalances in oxygen supply and demand
The Role of Hemodynamic Instability in Positioning1,2
1. Winslow EH, et al. Heart Lung. 1990;19:557-561.2. Price P. Dynamics. 2006;17:12-19.3. Vollman KM. Crit Care Nurs Q. 2013;36:17-27
• Factors that put patients at risk for intolerance to positioning:3
• Elderly• Diabetes with neuropathy• Prolonged bed rest• Low hemoglobin and cardiovascular reserve• Prolonged gravitational equilibrium
9/24/2015
41
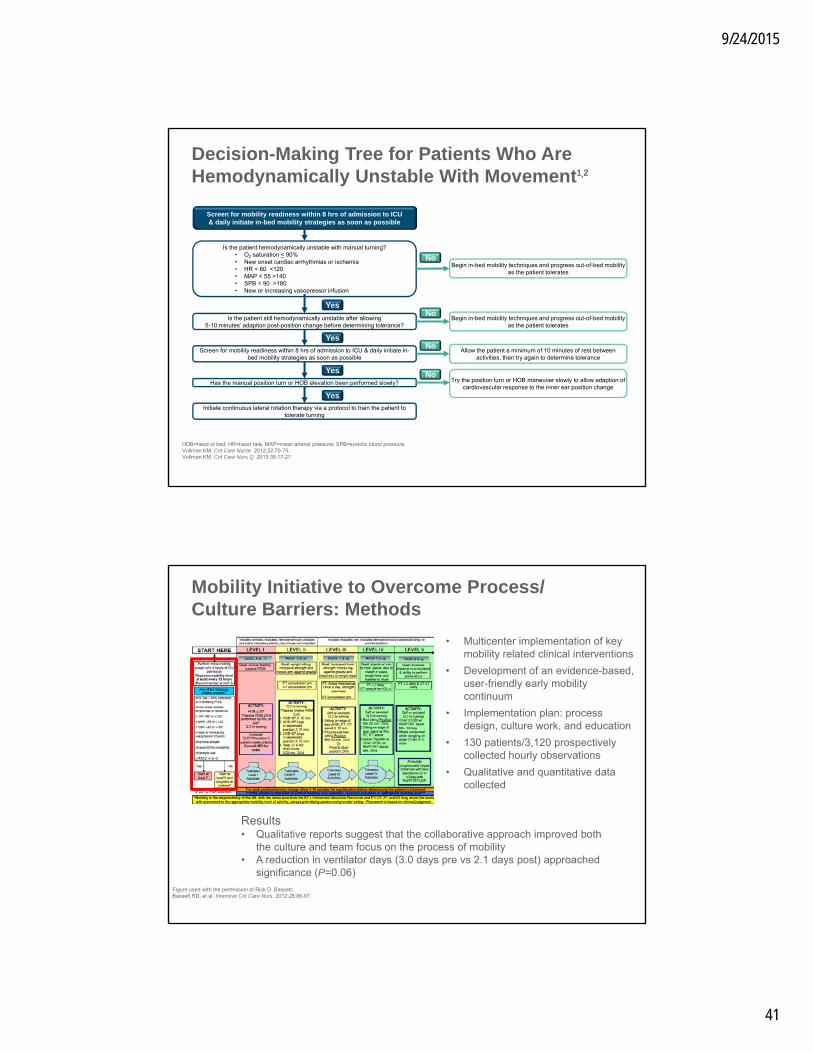
Decision-Making Tree for Patients Who Are Hemodynamically Unstable With Movement1,2
Screen for mobility readiness within 8 hrs of admission to ICU & daily initiate in-bed mobility strategies as soon as possible
Is the patient hemodynamically unstable with manual turning?• O2 saturation < 90%• New onset cardiac arrhythmias or ischemia• HR < 60 <120• MAP < 55 >140• SPB < 90 >180• New or increasing vasopressor infusion
Is the patient still hemodynamically unstable after allowing 5-10 minutes’ adaption post-position change before determining tolerance?
Has the manual position turn or HOB elevation been performed slowly?
Initiate continuous lateral rotation therapy via a protocol to train the patient to tolerate turning
Begin in-bed mobility techniques and progress out-of-bed mobility as the patient tolerates
Allow the patient a minimum of 10 minutes of rest between activities, then try again to determine tolerance
Begin in-bed mobility techniques and progress out-of-bed mobility as the patient tolerates
Try the position turn or HOB maneuver slowly to allow adaption of cardiovascular response to the inner ear position change
No
No
No
No
Screen for mobility readiness within 8 hrs of admission to ICU & daily initiate in-bed mobility strategies as soon as possible
Yes
Yes
Yes
Yes
HOB=head of bed; HR=heart rate; MAP=mean arterial pressure; SPB=systolic blood pressure.Vollman KM. Crit Care Nurse. 2012;32:70-75.Vollman KM. Crit Care Nurs Q. 2013;36:17-27.
Mobility Initiative to Overcome Process/ Culture Barriers: Methods
• Multicenter implementation of key mobility related clinical interventions
• Development of an evidence-based, user-friendly early mobility continuum
• Implementation plan: process design, culture work, and education
• 130 patients/3,120 prospectively collected hourly observations
• Qualitative and quantitative data collected
Figure used with the permission of Rick D. Bassett.Bassett RD, et al. Intensive Crit Care Nurs. 2012;28:88-97.
Results• Qualitative reports suggest that the collaborative approach improved both
the culture and team focus on the process of mobility• A reduction in ventilator days (3.0 days pre vs 2.1 days post) approached
significance (P=0.06)

9/24/2015
42
Cultural Adaptation to Increase Sustainability
Vollman KM, Bassett R. Transforming the Culture: The Key to Hardwiring Early Mobility & Safe Patient Handling. Amer Nurse Today, 2014, September
Early mobility has the potential to help reduce ICU LOS for non-vented and vented patients, creating the potential for significant savings.
Average ICU Costs
Potential Cost Savings if 1 Day ReducedICU LOS (with mechanical ventilation) in
an ICU With an Average of 200 Vent Patients Annually
Reduced ventilator days 1 day
Vent cost/day $3,968
Vent savings/patient $3,968
Annual number of vent patients* 200
Annual ventilator savings $793,600
Potential Cost Savings if 1 Day Reduced ICU LOS (with no mechanical ventilation) in an ICU With an Average of 500 Patients
Annually
ICU reduced LOS 1 day
ICU cost/day $3,184
ICU savings/patient $3,184
Annual number of ICU patients 500
Annual ICU LOS savings $1,592,000
1. Dasta JF, et al. Crit Care Med. 2005;33(6):1266-71.

9/24/2015
43
Financial Model for Cost Effectiveness
Lord R. Crit Care Med, 2013;41:717
Care Bundles and Protocols
9/24/2015
44
• ABCDE bundle = Awakening and Breathing Coordination, Delirium monitoring, and Exercise/early mobility
• ABCDE is designed to:– Promote collaboration among clinical team members– Standardize care– Break the ICU ventilation-sedation-delirium-weakness cycle
ABCDE Bundle to Mitigate ICU-Acquired Delirium and Weakness
Vasilevskis EE, et al. Chest. 2010;138:1224-1233.
National resources materials available to help implement:
• ICU liberation SCCM collaborative at www.iculiberation.org
• AACN CSI Academy & Clinical toolkit: Implementing ABCDE at www.aacn.org
• The ABCDE bundle was evaluated in critically ill patients receiving mechanical ventilation in a prospective before-after study of 186 patients from 5 ICUs (93 patients pre-ABCDE bundle implementation and 94 patients post implementation)
– After ABCDE bundle implementation, patients experienced more days breathing without assistance (average of 24 days without vent assistance vs 21 days in the pre-bundle group) and were less likely to experience ICU delirium (66% vs 75.3% in the pre-bundle group)
• A prospective study evaluated nonventilated patients in the ICU both prior to (n=53) and after (n=56) the implementation of the ABCDE bundle
– ABCDE bundle implementation resulted in a reduction in the overall incidence (19.6% vs 39.6% in the pre-bundle group) and duration of delirium in nonventilated ICU patients
ABCDE Bundle Clinical Evidence
1. Balas M, et al. Crit Care Med. 2014 May;42(5):1024-36.

9/24/2015
45
(Appendix (Appendix A) NeuroIntensiveA) NeuroIntensive Care UnitCare UnitProgressive Upright Mobility Protocol (PUMP) Plus AlgorithmProgressive Upright Mobility Protocol (PUMP) Plus Algorithm
Assess patient (pt.) for the following:•Pt. at risk for/has deconditioning due to immobility? OR•Does pt. require orthostatic training to upright position?
CONTRAINDICATIONS?Include but are not limited to unstable spine, active stroke alerts and/or up to 24hours after receiving tPA or endovascular intervention, increased intracranial HTN, active resuscitation for life-threatening hemodynamicinstability, femoral sheaths, traction, CRRT, aggressivemodes of ventilation and palliative care.
Is the pt. immobile or have ineffective mobility plus one or more of:•Lobar collapse, atelectasis, excessive secretions?•P/F Ratio < 300?•Hemodynamic instability with manual turning (↓O2Sat; ↓BP, ↑HR)?
Assess skin q2hours. Temporarily offload Pressure areas for circulatory recovery. Do not use turning wedges during rotation.
Q shift: assess pt. progress towards expected outcomes; adherence to rotation goals; tolerance to therapy; clinical contra-indications (listed above)…Does the pt. meet CLRT discontinuation criteria:•CXR improved/resolving infiltrates; P/F ratio> 300; stable hemodynamically; improved secretion mgmt; pt. turns self?
PUMP STEPS: Progress each step from 30-60 minutes. Each step must be implemented at least three times/day and more frequently as tolerated. Repeat each step until patient demonstrates clinical tolerance to stated activity/position, then advance to next step, at the next activity period opportunity.* It is highly recommended to coordinate pt. mealtime with mobility steps whenever possible.STEP 1: HOB elevated at 45°STEP 2: HOB elevated at 45°plus legs in dependent position (partial chair mode or cardiac chair)STEP 3: HOB elevated at 45°plus legs in full dependent position (full bed chair mode/cardiac chair)STEP 4: HOB elevated at 65°plus legs in full dependent position & feet on floor & standing in place*If cardiopulmonary intolerance develops, use reverse T-Berg for orthostatic training TID, until resolved.STEP 5: Initiate stand position/pivot and into chairSTEP 6: (PLUS) Transfer standing from bed to chair for 2-3 meals with sitting time not to exceed 45min.STEP 7 (PLUS): Ambulate within room using assistive devices & extra personnel PRN (goal = 20 feet)STEP 8 (PLUS): Ambulate within hallway using assistive devices & extra personnel PRN (goal = 50 feet)STEP 9 (PLUS): Ambulate within hallway using assistive devices & extra personnel PRN (goal = 100 feet)STEP 10 (PLUS): Ambulates 150 ft with contact guard (hands on only for balance) or personnel supervision/assistance (coaching only).STEP 11: (PLUS): Ambulates without coaching or supervision, may use device if necessary.
Initiate/continueCont. Lateral
RotationTherapy (CLRT)
Initiate orcontinue
PUMP Steps
Pt. able toambulate at all?
START HERESTART HERE……
N Y
Y
Proceed to PUMP PLUS
Steps 6 through 11
N
N
Y
N
Y
N
Notify primary MDto prescribe appropriateactivity orders for pt.
Y
Use of a of a Mobility Bundle Toolkit and Technology in a Neurointensive Care Unit
• All patient admitted over 16 month period
• 10 month pre-obs- 6 month post
• 100% Nurse-driven protocol
• One protocol for nurses to follow; all patients
• Mobility goals for patients with or without deconditioning
• Defined steps beyond “chair” to better prepare patients for discharge, earlier
• End point mobility goals similar to outpatient PT goals
Modified from The University of Kansas Hospital Progressive Mobility Algorithm for Critically Ill Patients (http://www.aacn.org/wd/nti2009/nti_cd/data/papers/main31710.pdf© Shands at the University of Florida, 2010Courtesy of J Hester.
Titsworth WL. J Neurosurg, 2012 116:1379-1388
Use of a of a Mobility Bundle Toolkit and Technology in a Neurointensive Care Unit (NICU)
Titsworth WL. J Neurosurg, 2012 116:1379-1388
Mobility was increased among the NICU care patients by 300%

9/24/2015
46
Protocol Driven Mobility Program: Impacting NICU Outcomes
• Pre-post intervention study
• Large academic NICU
• 637 patients
– 260 pre
– 377 post
• Intervention: Early Progressive Mobility Protocol
– Exclusion criteria
– Readiness criteria
– Started on admission
– Encourage to use ICU bed features & lifts to assist
– Protocol place at bedside
Klein K, et al. Crit care Med, 2015, epub
Protocol Driven Mobility Program: Impacting NICU OutcomesMultivariate analysis done to control for group differences:
K, et al. Crit care Med, 2015, epub
9/24/2015
47
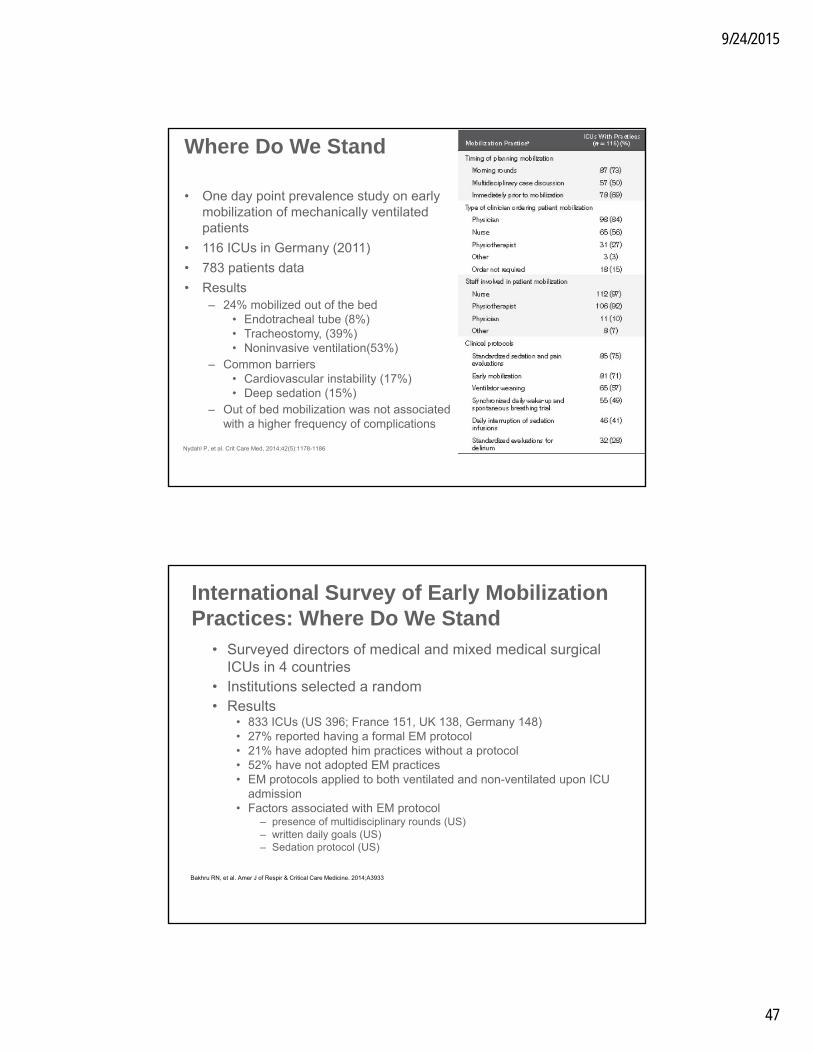
• One day point prevalence study on early mobilization of mechanically ventilated patients
• 116 ICUs in Germany (2011)
• 783 patients data
• Results– 24% mobilized out of the bed
• Endotracheal tube (8%)• Tracheostomy, (39%)• Noninvasive ventilation(53%)
– Common barriers• Cardiovascular instability (17%)• Deep sedation (15%)
– Out of bed mobilization was not associated with a higher frequency of complications
Where Do We Stand
Nydahl P, et al. Crit Care Med, 2014;42(5):1178-1186
• Surveyed directors of medical and mixed medical surgical ICUs in 4 countries
• Institutions selected a random• Results
• 833 ICUs (US 396; France 151, UK 138, Germany 148)• 27% reported having a formal EM protocol• 21% have adopted him practices without a protocol• 52% have not adopted EM practices• EM protocols applied to both ventilated and non-ventilated upon ICU
admission• Factors associated with EM protocol
– presence of multidisciplinary rounds (US)– written daily goals (US)– Sedation protocol (US)
International Survey of Early Mobilization Practices: Where Do We Stand
Bakhru RN, et al. Amer J of Respir & Critical Care Medicine. 2014;A3933
9/24/2015
48
How Can We Implement a
Program to Help Patients Achieve
Early Mobility and Potentially
Reduce Organizational Costs?
Utilizing bed systems combined with lifts and a early mobility protocol,caregivers can progress patients from the flat/supine position throughexiting the bed safely, easily, and more often.
This early mobility protocol is a simplified process of small,interventional activities that can be easily accomplished at the bed sidewith a minimum number of caregivers.

9/24/2015
49
Initial Patient Assessment
Mobility Level Criteria Start at Level 1 if:
PaO2/FiO2 <250
Positive end-expiratory pressure (PEEP) ≥10 cm H2O
O2 saturation <90%
Respiratory rate (RR) Not within 10-30 per min.
Cardiac arrhythmias or ischemia New onset
Heart rate (HR) <60 or >120 beats per min.
Mean arterial pressure (MAP) <55 or >140 mm Hg
Systolic blood pressure (SBP) <90 or >180 mm Hg
Vasopressor infusion New or increasing
Richmond agitation sedation scale (RASS) <–3
Riker sedation-agitation scale (SAS) <3
• Assess patients’ mobility levels within 8 hours of admission to the ICU and reassess at least every 24 hours
Adapted from Bassett RD, et al. Intensive Crit Care Nurs. 2012;28:88-97.
HOB angle – improve VAP protocol compliance• The Centers for Disease Control and
Prevention recommends an HOB angle of 30°-45°, unless contraindicated1
• Visually confirm the HOB is elevated ≥30°to comply with VAP prevention protocols
Activities• Every-2-hour turning• Passive range of motion• 20° Reverse Trendelenburg/Tilt Table with
lower extremity exercises/retracting footboard
Breathe
1. Tablan OC, et al. MMWR Recomm Rep. 2004;53:1-36.
RASS –5 to –3; SAS 1-2 (eg, cannot participate)Patient Assessment
Early Mobility Protocol Level 1: Breathe

9/24/2015
50
• Continuous lateral rotation therapy (CLRT) can be considered part of early mobility therapy in patients who are at high risk for pulmonary complications1
• CLRT provides side-to-side rotation to help facilitate gravitational effects on pulmonary secretions and blood flow
• Consult the CLRT Quick Reference Guide for additional information
– The CLRT QRG provides information regarding patient assessments and activities to be implemented in both hemodynamically stable and hemodynamically unstable patients
Early Mobility Protocol Level 1: Breathe (Cont.)
1. Swadener-Culpepper L, et al. Crit Care Nurs Q. 2008;31:270-279.
Breathe
Where Does CLRT Fit Into a Early Mobility Program?
CLRT=continuous lateral rotation therapy; PEEP=positive end-expiratory pressure.

9/24/2015
51
Activities Activities Activities Activities
Where Does CLRT Fit Into a Early Mobility Program? (Cont.)
CLRT=continuous lateral rotation therapy; PEEP=positive end-expiratory pressure.
CLRT Protocol for HemodynamicallyStable Patients
CLRT Quick Reference Guide
CLRT=continuous lateral rotation therapy.* This tool is provided for education and discussion only. Each facility is responsibility for the development, adoption and implementation of its own protocols. Follow protocols and rules adoptedby your facility.

9/24/2015
52
CLRT Protocol for HemodynamicallyUnstable Patients
CLRT Quick Reference Guide
CLRT=continuous lateral rotation therapy.* This tool is provided for education and discussion only. Each facility is responsibility for the development, adoption and implementation of its own protocols. Follow protocols and rules adopted by your facility.
Early Mobility Program Protocol Level 1: Breathe (Cont.)
• Move to Level 2 when the patient…– Has acceptable
oxygenation/hemodynamics
– Tolerates every-2-hour turning
– Tolerates HOB>30° or Reverse Trendelenburg 20°
Breathe

9/24/2015
53
20° Reverse Trendelenburg/Tilt Table position• Tilt Table positioning allows for orthostatic
training in fragile patients1
• If available, use in conjunction with retracting foot section to allow for partial weight bearing prior to sitting up in bed or getting out of bed
Activities• Maintain head of bed ≥30°• Every-2-hour turning• Passive/active range of motion• Legs dependent (partial chair)• PT consultation
Early Mobility Program Protocol Level 2: Tilt
Tilt
1. Trees D, Coale N. Acute Care Perspect. 2007;16:6-9.
RASS >–3; SAS >3 (eg, opens eyes; may have profound weakness)Patient Assessment
Early Mobility Protocol Level 2: Tilt (Cont.)
• Move to Level 3 when the patient…– Tolerates active-assistance exercises 2 times a day
– Tolerates lower extremity exercises against footboard/20° Reverse Trendelenburg
– Tolerates partial chair position (legs dependent/HOB ≥30°)
– Can move arms against gravity
Tilt
9/24/2015
54
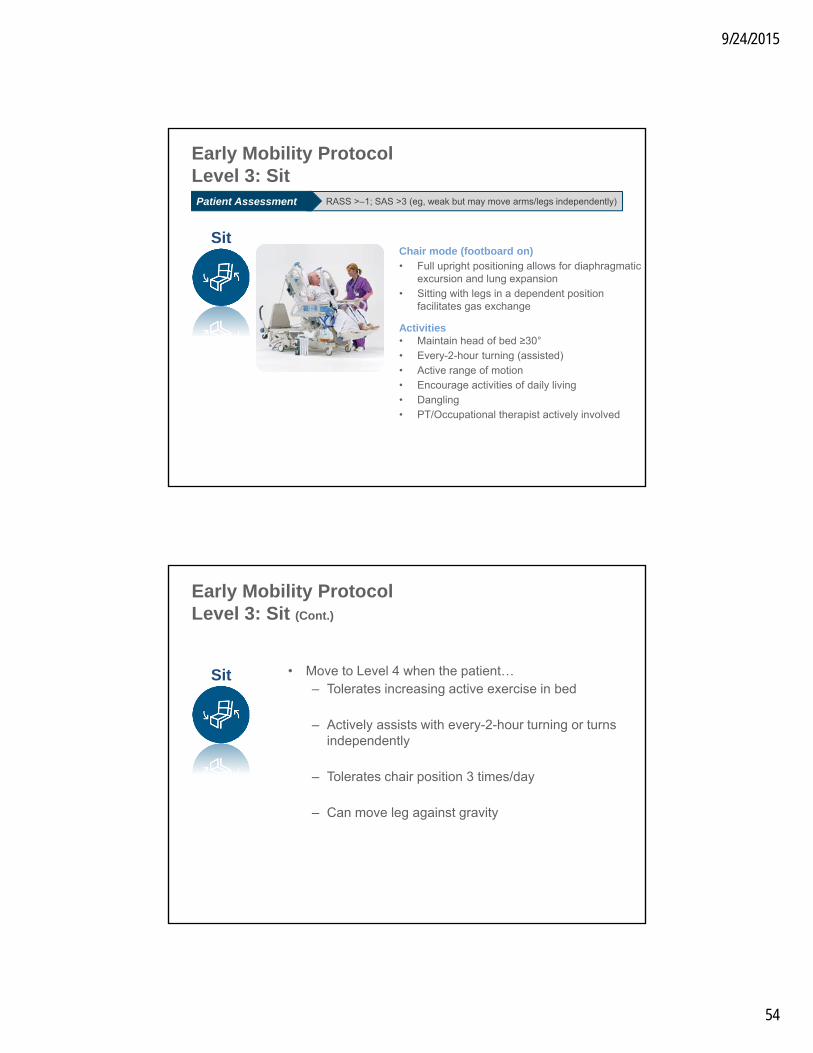
Chair mode (footboard on)• Full upright positioning allows for diaphragmatic
excursion and lung expansion• Sitting with legs in a dependent position
facilitates gas exchange
Activities• Maintain head of bed ≥30°• Every-2-hour turning (assisted)• Active range of motion• Encourage activities of daily living• Dangling• PT/Occupational therapist actively involved
Early Mobility Protocol Level 3: Sit
Sit
RASS >–1; SAS >3 (eg, weak but may move arms/legs independently)Patient Assessment
Early Mobility Protocol Level 3: Sit (Cont.)
• Move to Level 4 when the patient…– Tolerates increasing active exercise in bed
– Actively assists with every-2-hour turning or turns independently
– Tolerates chair position 3 times/day
– Can move leg against gravity
Sit
9/24/2015
55
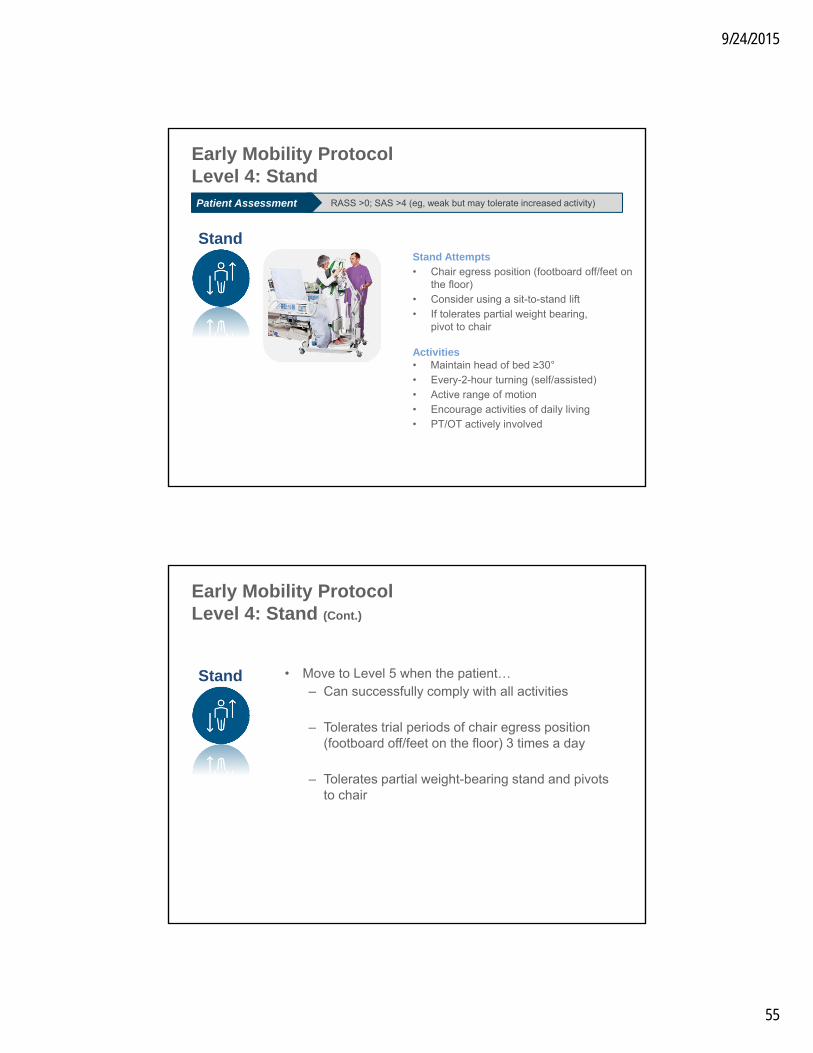
Stand Attempts• Chair egress position (footboard off/feet on
the floor)• Consider using a sit-to-stand lift• If tolerates partial weight bearing,
pivot to chair
Activities • Maintain head of bed ≥30°• Every-2-hour turning (self/assisted)• Active range of motion• Encourage activities of daily living• PT/OT actively involved
Stand
Early Mobility Protocol Level 4: Stand
RASS >0; SAS >4 (eg, weak but may tolerate increased activity)Patient Assessment
Early Mobility Protocol Level 4: Stand (Cont.)
• Move to Level 5 when the patient…– Can successfully comply with all activities
– Tolerates trial periods of chair egress position (footboard off/feet on the floor) 3 times a day
– Tolerates partial weight-bearing stand and pivots to chair
Stand
9/24/2015
56
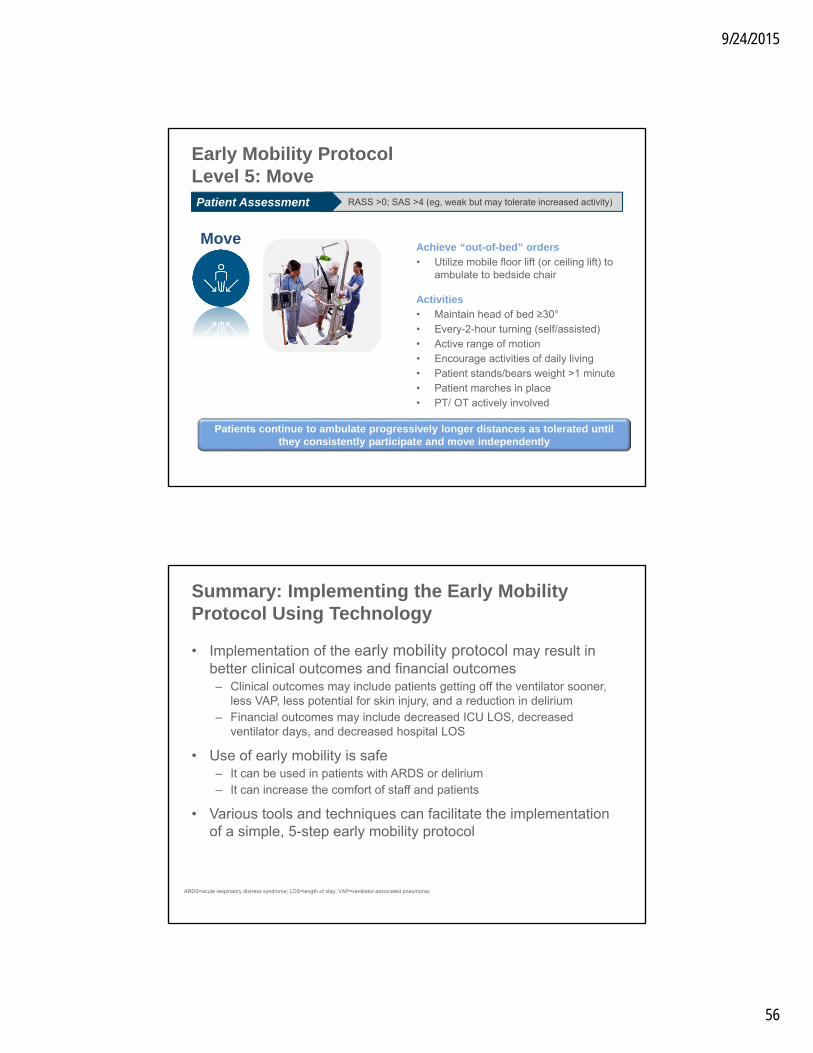
Early Mobility Protocol Level 5: Move
MoveAchieve “out-of-bed” orders• Utilize mobile floor lift (or ceiling lift) to
ambulate to bedside chair
Activities• Maintain head of bed ≥30°• Every-2-hour turning (self/assisted)• Active range of motion• Encourage activities of daily living• Patient stands/bears weight >1 minute• Patient marches in place• PT/ OT actively involved
RASS >0; SAS >4 (eg, weak but may tolerate increased activity)Patient Assessment
Patients continue to ambulate progressively longer distances as tolerated until they consistently participate and move independently
• Implementation of the early mobility protocol may result in better clinical outcomes and financial outcomes– Clinical outcomes may include patients getting off the ventilator sooner,
less VAP, less potential for skin injury, and a reduction in delirium– Financial outcomes may include decreased ICU LOS, decreased
ventilator days, and decreased hospital LOS
• Use of early mobility is safe– It can be used in patients with ARDS or delirium– It can increase the comfort of staff and patients
• Various tools and techniques can facilitate the implementation of a simple, 5-step early mobility protocol
Summary: Implementing the Early Mobility Protocol Using Technology
ARDS=acute respiratory distress syndrome; LOS=length of stay; VAP=ventilator-associated pneumonia.
9/24/2015
57
Questions?
2013 hospital national patient safety goals. Joint Commission website. http://www.jointcommission.org/assets/1/6/2013_HAP_NPSG_final_10-23.pdf. Accessed 02/26/13.
2014 clinical quality measures tipsheet. CMS website. http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/ClinicalQualityMeasuresTipsheet.pdf. Accessed 02/26/13.
AACN practice alert: delirium assessment and management. http://www.aacn.org/WD/practice/docs/practicealerts/delirium-practice-alert-2011.pdf. Accessed 02/25/13.
Barr J, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263-306.
Bennett G, et al. The cost of pressure ulcers in the UK. Age Ageing. 2004;33(3):230-235.
CMS. Fed Regist. 2008;73:48433-49084.
CMS Office of Public Affairs. Fact sheet: CMS proposes additions to list of hospital-acquired conditions for fiscal year 2009. Baltimore, MD: Centers for Medicare & Medicaid Services; 4/14/08.
CMS quality measurement programs characteristics. CMS website. http://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/qualitymeasures/downloads/cmsqualitymeasurementprogramscharacteristics.pdf. Accessed 02/26/13.
Courtney BA, et al. Save our skin: initiative cuts pressure ulcer incidence in half. Nurs Manage. 2006;37:36,38,40.
Dasta JF, et al. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005;33(6):1266-71.
De Jonghe B, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288:2859-2867.
De Jonghe B, et al. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness. Crit Care Med. 2007;35(9):2007-2015.
Device-associated module: ventilator-associated event protocol. NHSN website. http://www.cdc.gov/nhsn/PDFs/pscManual/10-VAE_FINAL.pdf. Accessed 02/22/13.
References
9/24/2015
58
Dudeck MA, et al. National Healthcare Safety Network (NHSN) report, data summary for 2010, device-associated module. http://www.cdc.gov/nhsn/PDFs/dataStat/2010NHSNReport.pdf. Accessed 12/19/12;17.
Edbrooke DL, et al. Implications of ICU triage decisions on patient mortality: a cost-effectiveness analysis. Crit Care. 2011;15:R56.
Elward AM, et al. Ventilator-associated pneumonia in pediatric intensive care unit patients: risk factors and outcomes. Pediatrics. 2002;109:758-764.
Fiscal year 2009 quality measure reporting for 2010 payment update. CMS website. http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Downloads/HospitalRHQDAPU200808.pdf. Accessed 02/26/13.
Goldhill DR, et al. A prospective observational study of ICU patient position and frequency of turning. Anaesthesia. 2008;63(5):509-515.
Harms MP, et al. Postural effects on cardiac output and mixed venous oxygen saturation in humans. Exp Physiol. 2003;88:611-616.
Hermans G, et al. Clinical review: critical illness polyneuropathy and myopathy. Crit Care. 2008;12:238.
Herridge MS, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. New Engl J Med. 2003;348:683-693.
Hopkins RO, Jackson JC. Long-term neurocognitive function after critical illness. Chest. 2006;130:869-878.
Hospital-acquired conditions. Centers for Medicare & Medicaid Services website. http://www.cms.gov/HospitalAcqCond/06_Hospital-Acquired_Conditions.asp. Accessed 1/3/12.
Hospital value-based purchasing program. CMS website. http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/Hospital_VBPurchasing_Fact_Sheet_ICN907664.pdf. Accessed 02/26/13.
Jankowski IM, Nadzam DM. Identifying gaps, barriers, and solutions in implementing pressure ulcer prevention programs. Jt Comm J Qual Patient Saf. 2011;37:253-264.
References (Cont.)
Knight, et al. Effects of bedrest 1: cardiovascular, respiratory and haematological systems. Nurs Times. 2009;105(21):16-20.
Knight, et al. Effects of bedrest 2: gastrointestinal, endocrine, renal, reproductive and nervous systems. Nurs Times. 2009;105(22):24-27.
Krishnagopalan S. Body positioning of intensive care patients: clinical practice versus standards. Crit Care Med. 2002;30:2588-2592
Lachenbruch C, et al. Presented at WOCN. 2011.
Morris PE. Moving our critically ill patients: mobility barriers and benefits. Crit Care Clin. 2007;23:1-20.
Nigam Y, et al. Effects of bedrest 3: musculoskeletal and immune systems, skin and self-perception. Nurs Times. 2009;105(23):18-22.
Pendergraft TB, et al. Rates and characteristics of intensive care unit admissions and intubations among asthma-related hospitalizations. Ann Allergy Asthma Immunol. 2004;93:29-35.
Phillips L, Buttery J. Exploring pressure ulcer prevalence and preventative care. Nurs Times. 2009;105(16):34-36.
Readmissions reduction program. CMS website. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed 02/26/13.
Reddy M, et al. Preventing pressure ulcers: a systematic review. JAMA. 2006;296:974-984.
Restrepo MI, et al. Economic burden of ventilator-associated pneumonia based on total resource utilization. Infect Control Hosp Epidemiol. 2010;31(5):509-515.
Rhodes A, et al. The variability of critical care bed numbers in Europe. Intensive Care Med. 2012;38:1647-1653.
Rosenberg AL, Watts C. Patients readmitted to ICUs*: a systematic review of risk factors and outcomes. Chest. 2000;118:492-502.
Rosenthal VD, et al. International Nosocomial Infection Control Consortium (INICC) report, data summary of 36 countries, for 2004-2009. Am J Infect Control. 2012;40(5):396-407.
References (Cont.)
9/24/2015
59
Schallom L, et al. Effect of frequency of manual turning on pneumonia. Am J Crit Care. 2005;14:476-478.
Sjostrand T. Volume and distribution of blood and their significance in regulating the circulation. Physiol Rev. 1953;33:202-228.
Society of Critical Care Medicine. Critical care statistics in the United States. Mount Pleasant, IL: Society of Critical Care Medicine; 2012. http://www.sccm.org/SiteCollectionDocuments/StatisticsBroch_d4.pdf. Accessed 7/27/12.
Topp R, et al. The effect of bed rest and potential of prehabilitation on patients in the intensive care unit. AACN Clin Issues. 2002;13(2):263-276.
Torres A, et al. Re-intubation increases the risk of nosocomial pneumonia in patients needing mechanical ventilation. Am J Respir Crit Care Med. 1995;152:137-141.
VanGilder C, et al. Poster. WOCN. 2012 (abstr 6007).
VanGilder C, et al. Presented at: Symposium on the Advances of Skin and Wound Care. 2010.
Knight, et al. Effects of bedrest 1: cardiovascular, respiratory and haematological systems. Nurs Times. 2009;105(21):16-20.
Knight, et al. Effects of bedrest 2: gastrointestinal, endocrine, renal, reproductive and nervous systems. Nurs Times. 2009;105(22):24-27.
Vasilevskis EE, et al. Reducing iatrogenic risks: ICU-acquired delirium and weakness--crossing the quality chasm. Chest. 2010;138:1224-1233.
Vincent J, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34(2):344-353.
Vollman KM. Introduction to progressive mobility. Crit Care Nurse. 2010;30:S3-S5.
Winkelman C. Bed rest in health and critical illness: a body systems approach. AACN Adv Crit Care. 2009;20:254-266.
References (Cont.)
Bailey P, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med. 2007;35:139-145.
Balas M, et al. Safety and efficacy of the ABCDE bundle in critically-ill patients receiving mechanical ventilation. Crit Care Med. 2012;40(suppl)(abstr 1).
Bassett RD, et al. Integrating a multidisciplinary mobility programme into intensive care practice (IMMPTP): a multicentre collaborative. Intensive Crit Care Nurs. 2012;28:88-97.
Dasta JF, et al. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005;33(6):1266-71.
Drakulovic MB, et al. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354:1851-1858.
Garcia R. Presented at: APIC. 2004. “Reduction of microbial colonization in the oropharynx and dental plaque reduces ventilator-associated pneumonia”. http://www.sageproducts.com/education/oral-hygiene/vSymposiaPres.cfm
Goldhill DR, et al. Rotational bed therapy to prevent and treat respiratory complications: a review and meta-analysis. Am J Crit Care. 2007;16:50-61.
Gosselink R, et al. Physiotherapy for adult patients with critical illness: recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically Ill Patients. Intensive Care Med. 2008;34:1188-1199.
Herridge MS. Legacy of intensive care unit–acquired weakness. Crit Care Med. 2009;37:S457-S461.
Morris PE. Moving our critically ill patients: mobility barriers and benefits. Crit Care Clin. 2007;23:1-20.
Morris PE, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 2008;36:2238-2243.
Olsen K, et al. The ABCDE bundle reduces the incidence of delirium in non-mechanically ventilated patients. Crit Care Med. 2012:40(suppl)(abstr 5).
Perme C, Chandrashekar R. Early mobility and walking program for patients in intensive care units: creating a standard of care.Am J Crit Care. 2009;18:212-221.
Pohlman MC, et al. Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation. Crit Care Med. 2010;38:2089-2094.
Price P. Physiologic effects of first-time sitting among male patients after coronary artery bypass graft surgery. Dynamics. 2006;17:12-19.
Schallom L, et al. Effect of frequency of manual turning on pneumonia. Am J Crit Care. 2005;14:476-478.
Schweickert WD, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373:1874-1882.
References
9/24/2015
60
Staudinger T, et al. Continuous lateral rotation therapy to prevent ventilator-associated pneumonia. Crit Care Med. 2010;38:486-490.
Swadener-Culpepper L, et al. The impact of continuous lateral rotation in overall clinical and financial outcomes of critically ill patients. Crit Care Nurs Q. 2008;31:270-279.
Tablan OC, et al. Guidelines for preventing health-care–associated pneumonia, 2003. MMWR Recomm Rep. 2004;53:1-36.
Titsworth WL, et al. The effect of increased mobility on morbidity in the neurointensive care unit. J Neurosurg. 2012;116:1379-1388.
Trees D, Coale N. Use of a dynamic tilt table for preambulation strength training of severely deconditioned patients. Acute Care Perspect. 2007;16:6-9.
van Nieuwenhoven CA, et al. Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Crit Care Med. 2006;34:396-402.
Vasilevskis EE, et al. Reducing the iatrogenic risks: ICU-acquired delirium and weakness—crossing the quality chasm. Chest. 2010;138:1224-1233.
Vollman KM. Introduction to progressive mobility. Crit Care Nurse. 2010;30:S3-S5.
Vollman KM. Hemodynamic instability: is it really a barrier to turning critically ill patients? Crit Care Nurse. 2012;32:70-75.
Vollman KM. Understanding critically ill patients hemodynamic response to mobilization: using the evidence to make it safe and feasible. Crit Care Nurs Q. 2013;36:17-27
Winkelman C. Poster. AANP. 2009. “Early Therapeutic Mobility in ICU: Patient Responses”
Winslow EH, et al. Effects of a lateral turn on mixed venous oxygen saturation and heart rate in critically ill adults. Heart Lung. 1990;19:557-561.
.
References (Cont.)
Related Documents











