Disclosures Disclosures D. Ware Branch, MD D. Ware Branch, MD • Nothing to disclose Nothing to disclose

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DisclosuresDisclosuresD. Ware Branch, MDD. Ware Branch, MD
• Nothing to discloseNothing to disclose
Diabetes in PregnancyDiabetes in Pregnancy
An UpdateAn Update
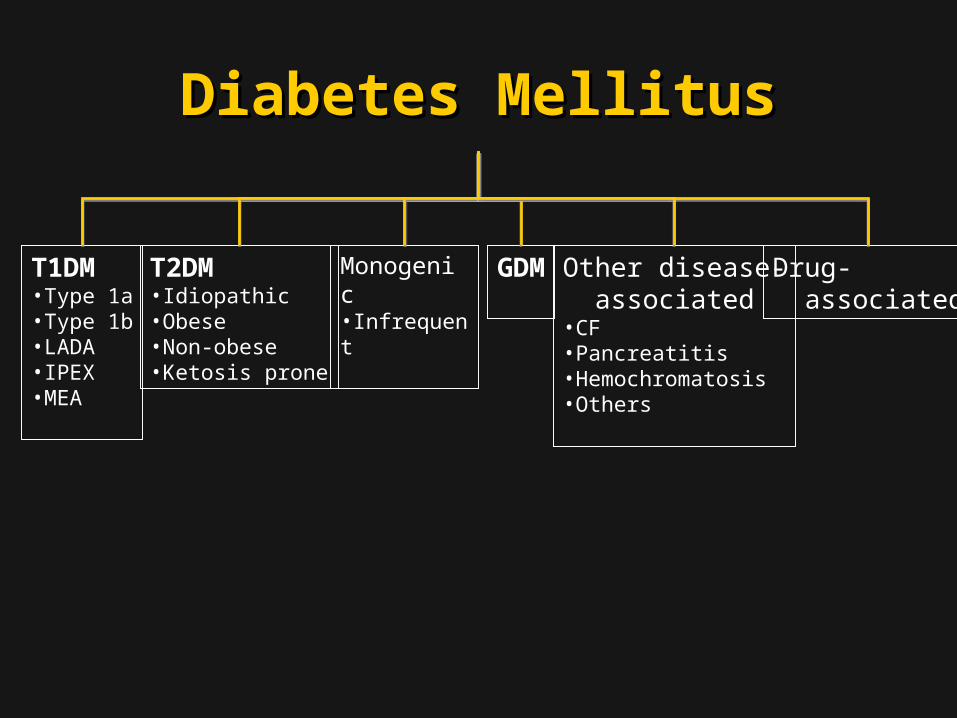
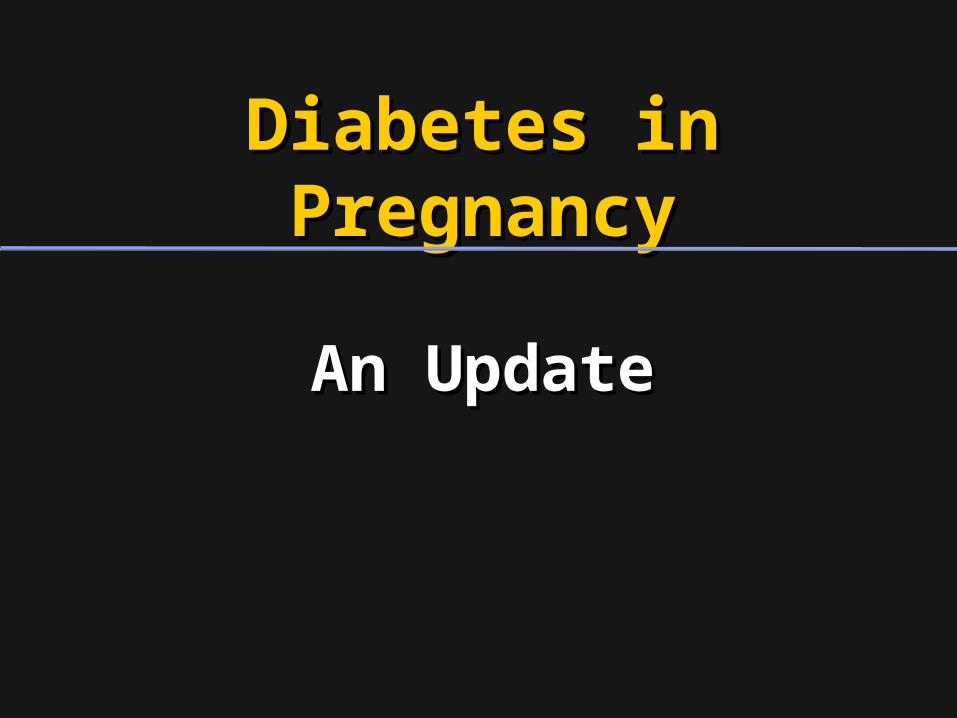
Diabetes MellitusDiabetes Mellitus
T1DM•Type 1a•Type 1b•LADA•IPEX•MEA
T2DM•Idiopathic•Obese•Non-obese•Ketosis prone
Monogenic•Infrequent
GDM Other disease- associated•CF•Pancreatitis•Hemochromatosis•Others
Drug- associated

Gestational DiabetesGestational DiabetesDo we really care?Do we really care?
Most cases identified are mild in naturePatients don’t like the OGCT or 3-hr GTTReally counseling patients is time-consumingPatients are reluctant to check BGsNot sure all of this makes a difference

Gestational DiabetesGestational DiabetesEffect of TreatmentEffect of Treatment
• Randomized clinical trial in 18 Randomized clinical trial in 18 centers (ACHOIS)centers (ACHOIS)
• Women with GDM, 24-34 weeksWomen with GDM, 24-34 weeks’’– Singletons or twinsSingletons or twins– Risk factor(s) for GDM, orRisk factor(s) for GDM, or– Positive 50 g OGCT (Positive 50 g OGCT ( 140 mg/dL), and 140 mg/dL), and– 75 g GTT with FBG 75 g GTT with FBG 140 mg/dL and 2 140 mg/dL and 2
hour BG hour BG 198 mg/dL 198 mg/dL
Crowther et al, N Engl J Med 2005;352:2477

Gestational DiabetesGestational DiabetesEffect of TreatmentEffect of Treatment
OutcomeOutcome
DeathDeath
ShoulderShoulder dystociadystocia
Bone fxBone fx
TreatedTreated(N=506)(N=506)
Routine CareRoutine Care(N= 524)(N= 524)
AdjAdjP valueP value
0.070.07
0.080.08
0.380.38
Crowther et al, N Engl J Med 2005;352:2477Crowther et al, N Engl J Med 2005;352:2477
Nerve palsyNerve palsy 0.110.11
CompositeComposite
00
7 (1%)7 (1%)
00
00
7 (1%)7 (1%)
5 (1%)5 (1%)
16 (3%)16 (3%)
1 (<1%)1 (<1%)
3 (1%)3 (1%)
23 (4%)23 (4%) 0.010.01
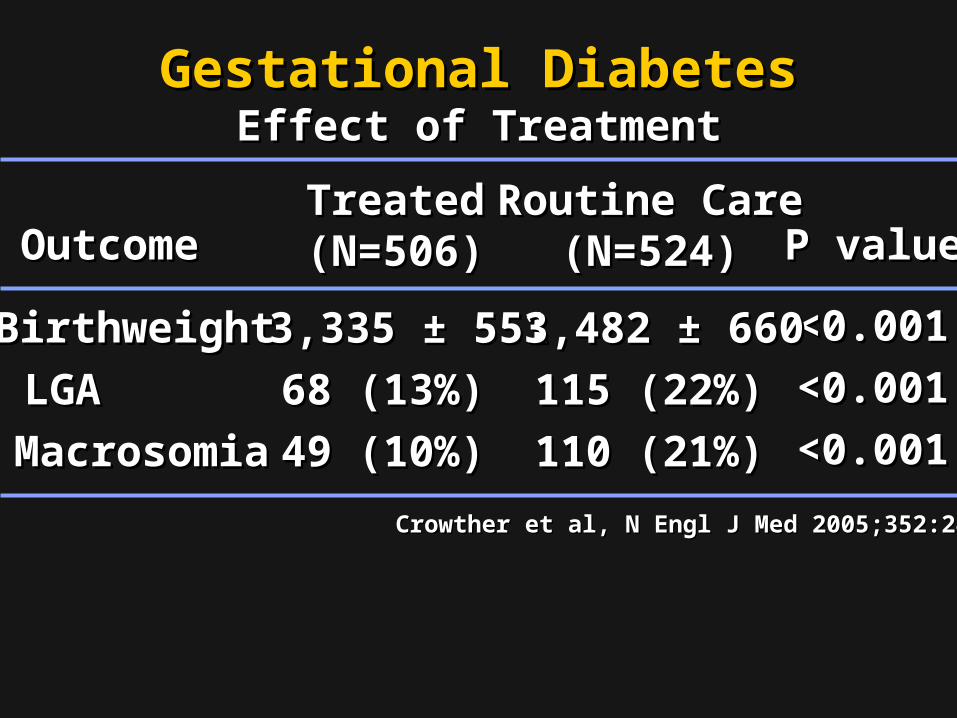
Gestational DiabetesGestational DiabetesEffect of TreatmentEffect of Treatment
OutcomeOutcome
BirthweightBirthweight
LGALGA
MacrosomiaMacrosomia
TreatedTreated(N=506)(N=506)
Routine CareRoutine Care(N=524)(N=524) P valueP value
<0.001<0.001
<0.001<0.0013,335 3,335 ± 551± 551
68 (13%)68 (13%)
49 (10%)49 (10%)
3,482 ± 6603,482 ± 660
115 (22%)115 (22%)
110 (21%)110 (21%) <0.001<0.001
Crowther et al, N Engl J Med 2005;352:2477Crowther et al, N Engl J Med 2005;352:2477

MFMU Network Randomized MFMU Network Randomized Treatment Trial of Mild GDM Treatment Trial of Mild GDM
• Multicenter randomized trial of Multicenter randomized trial of women withwomen with– Abnormal 50 g OGCAbnormal 50 g OGC– 3-hr GTT 3-hr GTT GDM, but GDM, but – Normal FBS on 3-hr GTTNormal FBS on 3-hr GTT
• Subjects randomized toSubjects randomized to– Usual care (GTT results not available)Usual care (GTT results not available)– Dietary intervention, SBGM, and Dietary intervention, SBGM, and
insulin if requiredinsulin if required
Landon et al, N Engl J Med 2009; 361:1339Landon et al, N Engl J Med 2009; 361:1339

Gestational DiabetesGestational DiabetesEffect of TreatmentEffect of Treatment
OutcomeOutcomeTreatedTreated(N=485)(N=485)
Routine CareRoutine Care(N= 473)(N= 473) P valueP value
DeathDeath 00 00Hyperbili-Hyperbili- rubinemiarubinemia
0.120.1243 (10%)43 (10%) 54 (13%)54 (13%)
HypoglycemiaHypoglycemia 0.750.7562 (16%)62 (16%) 55 (15%)55 (15%)Elevated cordElevated cord C-peptideC-peptide
0.070.0775 (18%)75 (18%) 92 (23%)92 (23%)
CompositeComposite 149 (32%)149 (32%) 163 (37%)163 (37%) 0.140.143 (<1%)3 (<1%) 6 (1%)6 (1%)Birth traumaBirth trauma 0.330.33
Landon et al, N Engl J Med 2009; 361:1339Landon et al, N Engl J Med 2009; 361:1339

Gestational DiabetesGestational DiabetesEffect of TreatmentEffect of Treatment
OutcomeOutcome
BirthweightBirthweight
LGALGA
MacrosomiaMacrosomia
TreatedTreated(N=485)(N=485)
Routine CareRoutine Care(N=473)(N=473) P valueP value
<0.001<0.001
<0.001<0.0013,302 3,302 ± 502± 502
34 (7.1%)34 (7.1%)
28 (5.9%)28 (5.9%)
3,408 ± 5893,408 ± 589
66 (14.5%)66 (14.5%)
65 (14.3%)65 (14.3%) <0.001<0.001
Landon et al, N Engl J Med 2009; 361:1339Landon et al, N Engl J Med 2009; 361:1339
Fat Mass (g)Fat Mass (g) 427 427 ± 198± 198 464 464 ± 222 ± 222
<0.003<0.003

Gestational DiabetesGestational DiabetesEffect of TreatmentEffect of Treatment
OutcomeOutcomeTreatedTreated(N=485)(N=485)
Routine CareRoutine Care(N= 473)(N= 473) P valueP value
CesareanCesarean 0.020.02128 (27%)128 (27%) 154 (34%)154 (34%)
ShoulderShoulder dystocia dystocia
0.020.027 (1.5%)7 (1.5%) 18 (4%)18 (4%)
Landon et al, N Engl J Med 2009; 361:1339Landon et al, N Engl J Med 2009; 361:1339
GHTN - PEGHTN - PE 41 (9%)41 (9%) 62 (14%)62 (14%) 0.010.01
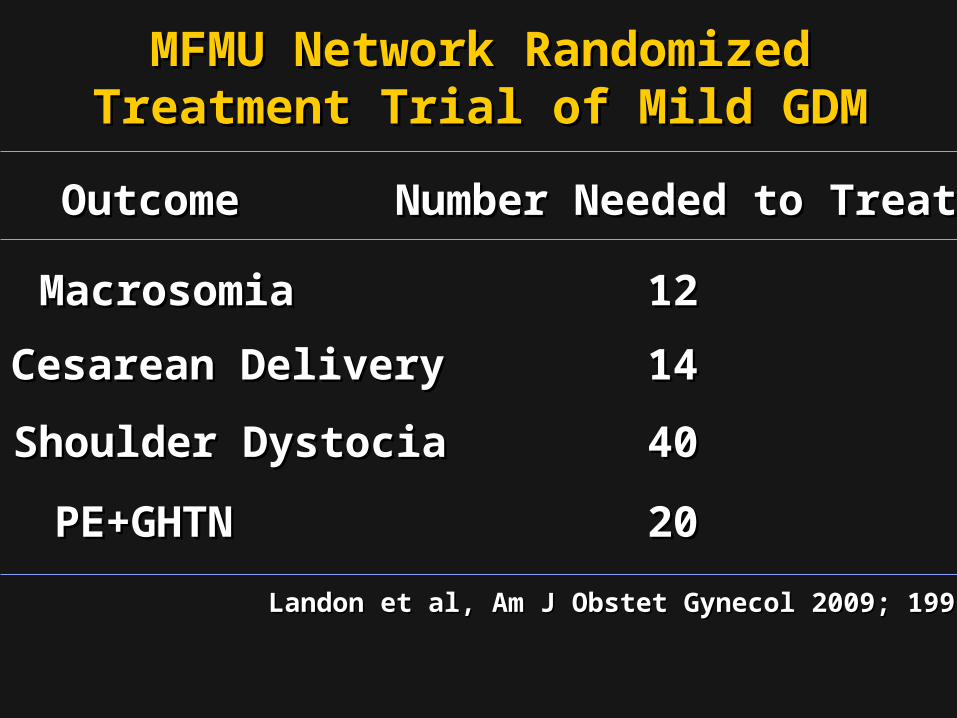
MFMU Network Randomized MFMU Network Randomized Treatment Trial of Mild GDM Treatment Trial of Mild GDM
Landon et al, Am J Obstet Gynecol 2009; 199:S2Landon et al, Am J Obstet Gynecol 2009; 199:S2
OutcomeOutcome Number Needed to TreatNumber Needed to Treat
MacrosomiaMacrosomia
Cesarean DeliveryCesarean Delivery
Shoulder DystociaShoulder Dystocia
PE+GHTNPE+GHTN
1212
1414
4040
2020

Diabetes in PregnancyDiabetes in PregnancyDo we really care?Do we really care?
Offspring childhood obesity and DMMothers type 2 DM

MFMU Network Treatment Trial of MFMU Network Treatment Trial of Mild GDMMild GDM
Childhood Follow-upChildhood Follow-up
• Follow-up of 500 (55%) children Follow-up of 500 (55%) children (ages 5-10) from MFMUN treatment (ages 5-10) from MFMUN treatment trialtrial– Physical parameters and BPPhysical parameters and BP– Fasting glucose and insulinFasting glucose and insulin– TriglyceridesTriglycerides– HDL cholesterolHDL cholesterol
Landon et al. Diab Care 2014Landon et al. Diab Care 2014
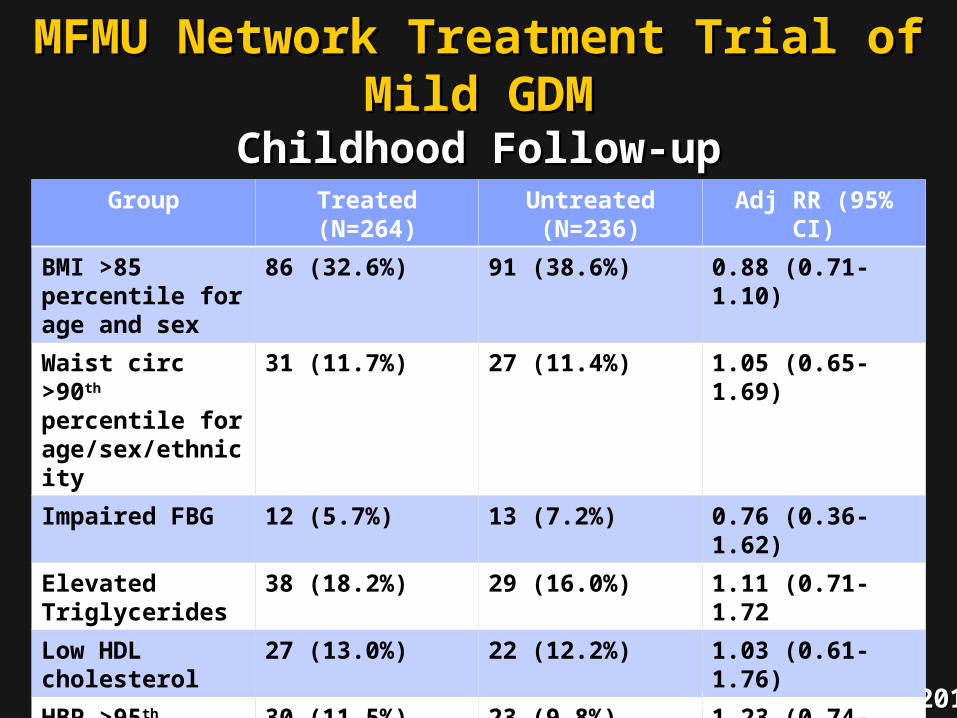
MFMU Network Treatment Trial of Mild MFMU Network Treatment Trial of Mild GDMGDM
Childhood Follow-upChildhood Follow-up
Landon et al. Diab Care 2014Landon et al. Diab Care 2014
Group Treated(N=264)
Untreated(N=236)
Adj RR (95% CI)
BMI >85 percentile for age and sex
86 (32.6%) 91 (38.6%) 0.88 (0.71-1.10)
Waist circ >90th percentile for age/sex/ethnicity
31 (11.7%) 27 (11.4%) 1.05 (0.65-1.69)
Impaired FBG 12 (5.7%) 13 (7.2%) 0.76 (0.36-1.62)
Elevated Triglycerides
38 (18.2%) 29 (16.0%) 1.11 (0.71-1.72
Low HDL cholesterol
27 (13.0%) 22 (12.2%) 1.03 (0.61-1.76)
HBP >95th percentile for age/sex/height
30 (11.5%) 23 (9.8%) 1.23 (0.74-2.05)

Gestational DiabetesGestational Diabetes
• DiagnosisDiagnosis– Controversy in adopting Controversy in adopting
IADPSG/ADA guidelines for IADPSG/ADA guidelines for diagnosis of GDMdiagnosis of GDM
– Why experts, including ACOG, Why experts, including ACOG, hesitatehesitate

HAPO StudyHAPO Study
• Prospective, observational study of Prospective, observational study of 23,316 pregnant women23,316 pregnant women
• 75 g OGTT75 g OGTT7 glucose categories7 glucose categories• Primary outcomesPrimary outcomes
– LGALGA– CSCS– Neonatal hypoglycemiaNeonatal hypoglycemia– Cord C-peptideCord C-peptide

Frequency of Primary Outcomes across the Glucose Categories
The HAPO Study Cooperative Research Group. N Engl J Med 2008;358:1991-2002

IADPSG Screening Strategy IADPSG Screening Strategy for Diabetes in Pregnancyfor Diabetes in Pregnancy
• FBG or HgbA1c at first prenatal visitFBG or HgbA1c at first prenatal visit– ≥≥126 or 6.5% 126 or 6.5% overt diabetes overt diabetes
– 92-125 92-125 GDM GDM
– <92 <92 75 g OGTT at 24-28 weeks 75 g OGTT at 24-28 weeks

IADPSG Screening Strategy IADPSG Screening Strategy for GDMfor GDM
• One-step approach One-step approach – 75 g, 2 hour OGTT75 g, 2 hour OGTT
• GDM diagnosis if any one threshold met GDM diagnosis if any one threshold met or exceededor exceeded
Status Threshold Glucose
Fasting 92
1 hour 180
2 hour 153
Based on glucose levels associated with 1.75-fold increased risk of LGA, neonatal body fat >90th%tile, & cord insulin

ImplicationImplication
• HAPOHAPOIADPSG recommendation IADPSG recommendation would result in nearly 20% of the would result in nearly 20% of the population being diagnosed with population being diagnosed with GDM!GDM!

Pros for IADPSG Pros for IADPSG RecommendationsRecommendations
• Based on 2 randomized trialsBased on 2 randomized trials– ~30% to 60% reduction in adverse ~30% to 60% reduction in adverse
outcomesoutcomes
• In HAPO (23,316 pregnancies), dx In HAPO (23,316 pregnancies), dx and treatment wouldand treatment would
• Prevent 140 cases of LGA, 21 SDs, and 16 Prevent 140 cases of LGA, 21 SDs, and 16 birth injuriesbirth injuries
• Potential for long-term health Potential for long-term health improvements related to patient improvements related to patient education in pregnancyeducation in pregnancy

Cons for IADPSG Cons for IADPSG RecommendationsRecommendations
• High percentage of population diagnosed High percentage of population diagnosed with GDMwith GDM• But would But would onlyonly prevent 140 cases of LGA, 21 SDs, prevent 140 cases of LGA, 21 SDs,
and 16 birth injuriesand 16 birth injuries
• Reproducibility of 75 g OGTT poor – 25% Reproducibility of 75 g OGTT poor – 25% could be reclassifiedcould be reclassified
• ““Treatment” in real-world may not be Treatment” in real-world may not be practical or effectivepractical or effective

Cons for IADPSG Cons for IADPSG RecommendationsRecommendations
• Unintended consequences of Unintended consequences of “overmedicalization”“overmedicalization”– Inductions and early deliveryInductions and early delivery
• Costs > benefits?Costs > benefits?
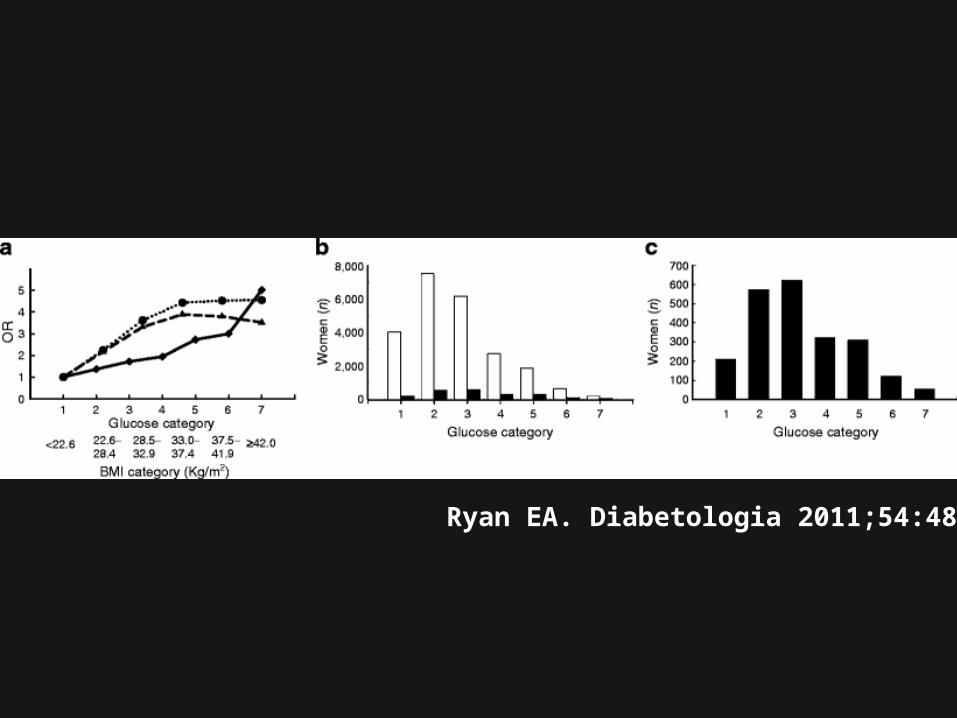
Ryan EA. Diabetologia 2011;54:480

Diagnosing GDM?Diagnosing GDM?
• Both glucose and BMI predict LGABoth glucose and BMI predict LGA
• In HAPO, 78% of LGA infants were In HAPO, 78% of LGA infants were born of women without IADPSG GDM born of women without IADPSG GDM diagnosis!diagnosis!
• BMI is more relevant except at BMI is more relevant except at highest glucose levelshighest glucose levels
Ryan EA. Diabetologia 2011;54:480
Obesity?
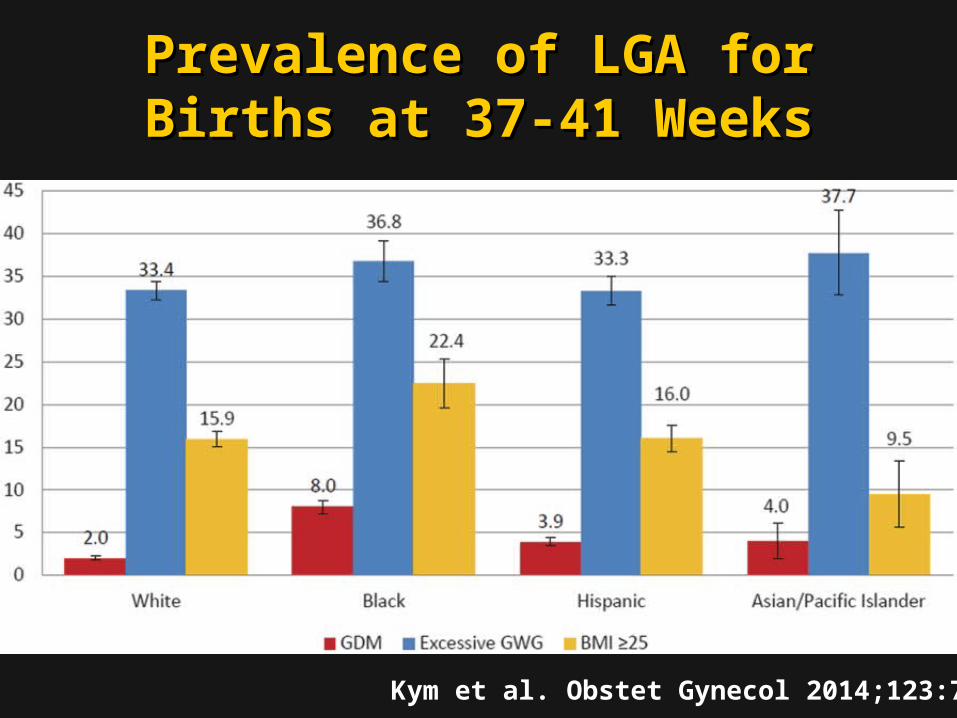
Prevalence of LGA for Births at Prevalence of LGA for Births at 37-41 Weeks37-41 Weeks
Kym et al. Obstet Gynecol 2014;123:737


Improved Outcomes After Improved Outcomes After Use of IADPSG Criteria?Use of IADPSG Criteria?
• Retrospective comparison of two Retrospective comparison of two cohorts:cohorts:– 1750 women in 2011-12 using 1750 women in 2011-12 using
conventional criteria (CC)conventional criteria (CC)– 1526 women in 2012-13 using IADPSG1526 women in 2012-13 using IADPSG– Both group treated similarly after dx of Both group treated similarly after dx of
GDMGDM
• Dx of GDM in 10.6% using CC, 35.5% Dx of GDM in 10.6% using CC, 35.5% using IADPSG!using IADPSG!
Duran et al. Diab Care 2014;37:2442

Improved Outcomes After Improved Outcomes After Use of IADPSG Criteria?Use of IADPSG Criteria?
• Using IADPSG,Using IADPSG,
Increased use of insulinIncreased use of insulin
Estimated cost savings!Estimated cost savings!
Duran et al. Diab Care 2014;37:2442
Outcome CC Criteria IADPSG Criteria
P Value
GHTN 4.1% 3.5% <0.021
Cesarean 25.4% 19.7% <0.002
LGA 4.6% 3.7% <0.004
NICU adm 8.2% 6.2% <0.001

Screening Strategy for GDMScreening Strategy for GDM
• All women “whether by …medical history, All women “whether by …medical history, clinical risk factors, or laboratory clinical risk factors, or laboratory screening test….”screening test….”
• Laboratory screeningLaboratory screening– 50 g glucose challenge 50 g glucose challenge 1 hour venous 1 hour venous
glucoseglucose• Threshold of 135 or 140Threshold of 135 or 140• 3 hour diagnostic OGTT3 hour diagnostic OGTT
ACOG Practice Bulletin 137, August 2013ACOG Practice Bulletin 137, August 2013
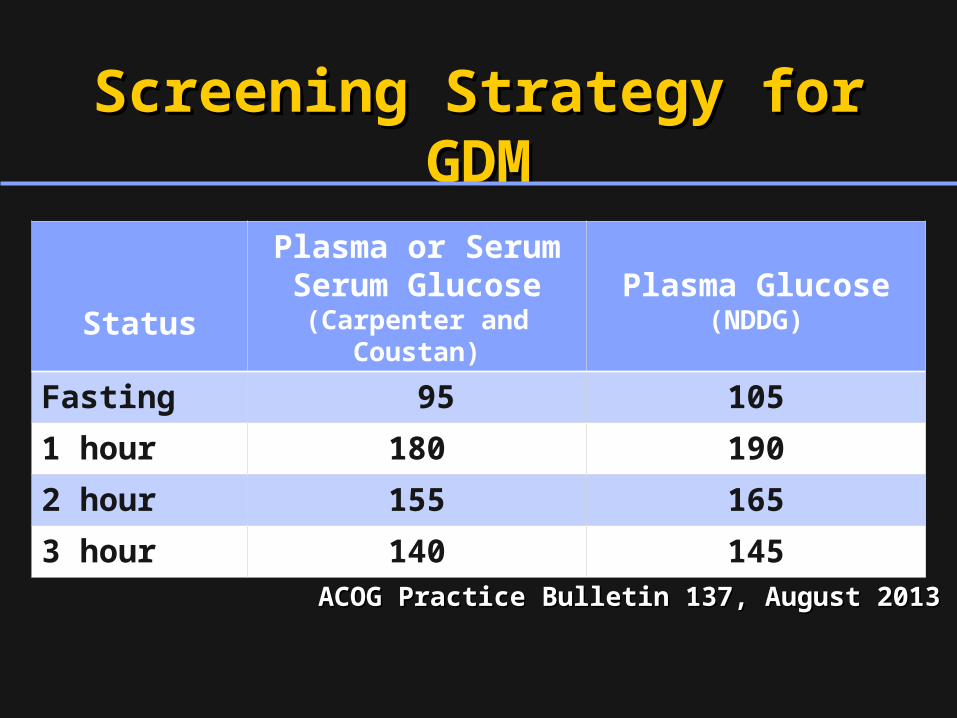
Screening Strategy for GDMScreening Strategy for GDM
Status
Plasma or Serum Serum Glucose
(Carpenter and Coustan)Plasma Glucose
(NDDG)
Fasting 95 105
1 hour 180 190
2 hour 155 165
3 hour 140 145
ACOG Practice Bulletin 137, August 2013ACOG Practice Bulletin 137, August 2013

Screening Strategy for Screening Strategy for GDM?GDM?
• Retrospective cohort study of women Retrospective cohort study of women without DM and with HgbA1c ≤ 20 weeks without DM and with HgbA1c ≤ 20 weeks in a single practicein a single practice
• Compared those with A1c 5.7-6.4% to Compared those with A1c 5.7-6.4% to those with A1c <5.7%those with A1c <5.7%
• Primary outcomePrimary outcomeGDMGDM
Fong et al, AJOG 2014;211:641Fong et al, AJOG 2014;211:641

Maternal Outcomes HgbA1c <5.7% vs 5.7% to 6.4%Outcome HA1c <5.7%
(N=471)HA1c 5.7-6.4%
(N=55)Adj OR (95% CI)
Development of GDM 41 (8.7%) 15 (27.3%) 2.38 (1.01-5.63)
Non-elective CS 107/443 (24.2%) 14/52 (26.9%) 0.94 (0.43-2.06)Wt gain, lb 29.7 ± 17.0 27.2 ± 15.1 --
Wt gain > IOM 228/465 (49%) 24/55 (43.6%) 0.90 (0.48-1.70)
1-hr OGCT 114.5 ± 30.3 128.9 ± 28.9 --
FBG on 3-hr GTT
81.2 ± 11.1 89.1± 19.4 --
Screening Strategy for Screening Strategy for GDM?GDM?
Fong et al, AJOG 2014;211:641Fong et al, AJOG 2014;211:641
Timing of Delivery in GDMTiming of Delivery in GDM• Women with good glycemic control who are Women with good glycemic control who are
receiving medical therapy do not require receiving medical therapy do not require delivery before 39 weeksdelivery before 39 weeks
• In insulin treated casesIn insulin treated cases– Delivery at 38-39 weeks may be associated with Delivery at 38-39 weeks may be associated with
fewer cases of LGA infantsfewer cases of LGA infants– Delivery at or beyond 40 weeks may be associated Delivery at or beyond 40 weeks may be associated
with more cases of shoulder dystociawith more cases of shoulder dystocia
• There is no evidence-based recommendation There is no evidence-based recommendation regarding timing of delivery (diet or medical regarding timing of delivery (diet or medical therapy)therapy)
ACOG Practice Bulletin 137, August 2013

Diet and Activity in GDMDiet and Activity in GDM
• Carbohydrate intake [should] be limited to 33–40% of calories, with the remaining calories divided between protein (20%) and fat (40%)
• A moderate exercise program as part of the treatment plan for women with GDM is recommended
ACOG Practice Bulletin 137, August 2013

Diet and Carbs in GDMDiet and Carbs in GDM
Total Calories Carbohydrate Calories (@40% of total) / g of carbs
Examples of Daily Carbohydrate Selection
2000 calories per day (1st 6 months of pregnancy)
800 calories200 g carbohydrates
1 medium fruit, 1 average bread, 1 ½-⅔ cup cereals/grains/potatoes per meal, along with assorted other carbs
2200 calories per day (last 3 months of pregnancy)
880 calories220 g carbohydrates
Add 1-2 carb servings per day

Activity in GDMActivity in GDM
• 30 minutes of moderate-to-vigorous intensity aerobic exercise at least 5 days a week (150 min per week)– You can talk but not sing– You cannot say more than a few words
without pausing for a breath
ADA, 2013http://www.diabetes.org/food-and-fitness/fitness/types-of-activity/?loc=DropDownFF-typesofactivity


Tools for DM CareTools for DM Care
• Glucose monitorsGlucose monitors
• Ultrashort acting insulinUltrashort acting insulin
• Insulin pumpsInsulin pumps
• ““Peakless” insulinsPeakless” insulins
• Continuous glucose monitorsContinuous glucose monitors
• Linked CGM-Pump systemsLinked CGM-Pump systems



Diabetes Management 101Diabetes Management 101(aka “Coaching”)(aka “Coaching”)
• Insist on patient self blood glucose Insist on patient self blood glucose monitoring - monitoring - ““you manage what you you manage what you measuremeasure””
• Review the results at every patient Review the results at every patient visitvisit
• Suggest ways to improve – coach!Suggest ways to improve – coach!
• Establish reliable, outcome-oriented Establish reliable, outcome-oriented referral servicesreferral services
Related Documents