Disclosures Accreditation and Designation Statements The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The AAP designates this live activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. This activity is acceptable for a maximum of 1 AAP credit. This credit can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Members of the American Academy of Pediatrics. The American Academy of Physician Assistants accepts AMA PRA Category 1 Credits™ from organizations accredited by the ACCME. This program is approved for 1 NAPNAP CE contact hour of which 0 contain pharmacology (Rx) content per the National Association of Pediatric Nurse Practitioners Continuing Education Guidelines. Purpose of Course The American Academy of Pediatrics and National Center for Medical Home Implementation will be hosting a free four-part Webinar series beginning in April 2011. The purpose of the webinar series is to provide child health professionals with practical strategies for implementing medical home in practice. Each webinar will be led by recognized experts with the goal of educating participants about the value of the family-centered primary care medical home for all children and youth, especially in the daily delivery of preventive, acute, and chronic care. Faculty will point participants to practical tools and resources, and will provide strategies for improving quality of care and increasing patient/family partnership and satisfaction. Learning Objectives At the conclusion of this activity, participants should be able to: Describe selected essential clinical and procedural elements needed in medical home practices to deliver chronic care for patients and their families Explain the importance and application of patient population management in the delivery of care for children with a chronic health conditions Explore the delivery of effective chronic care through a case study on pediatric asthma care in the medical home Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities The AAP CME program aims to develop, maintain, and improve the competence, skills, and professional performance of pediatricians and pediatric healthcare professionals by providing quality, relevant, accessible, and effective educational experiences that address gaps in professional practice. The AAP CME program strives to meet participants' educational needs and support their life-long learning with a goal of improving care for children and families. (AAP CME Program Mission Statement, September 2010). The AAP recognizes that there are a variety of financial relationships between individuals and commercial interests that require review to identify possible conflicts of interest in a CME activity. The “AAP Policy on Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities” is designed to ensure quality, objective, balanced, and scientifically rigorous AAP CME activities by identifying and resolving all potential conflicts of interest prior to the confirmation of service of those in a position to influence and/or control CME content. The AAP has taken steps to resolve any potential conflicts of interest. All AAP CME activities will strictly adhere to the Accreditation Council for Continuing Medical Education (ACCME) Standards for Commercial Support: Standards to Ensure the Independence of CME Activities. In accordance with these Standards, the following decisions will be made free of the control of a commercial interest: identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the CME activity. The purpose of this policy is to ensure all potential conflicts of interest are identified and mechanisms to resolve them prior to the CME activity are implemented in ways that are consistent with the public good. The AAP is committed to providing learners with commercially unbiased CME activities.

Disclosures Accreditation and Designation Statements The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Disclosures
Accreditation and Designation StatementsThe American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The AAP designates this live activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. This activity is acceptable for a maximum of 1 AAP credit. This credit can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Members of the American Academy of Pediatrics. The American Academy of Physician Assistants accepts AMA PRA Category 1 Credits™ from organizations accredited by the ACCME. This program is approved for 1 NAPNAP CE contact hour of which 0 contain pharmacology (Rx) content per the National Association of Pediatric Nurse Practitioners Continuing Education Guidelines.
Purpose of CourseThe American Academy of Pediatrics and National Center for Medical Home Implementation will be hosting a free four-part Webinar series beginning in April 2011. The purpose of the webinar series is to provide child health professionals with practical strategies for implementing medical home in practice. Each webinar will be led by recognized experts with the goal of educating participants about the value of the family-centered primary care medical home for all children and youth, especially in the daily delivery of preventive, acute, and chronic care. Faculty will point participants to practical tools and resources, and will provide strategies for improving quality of care and increasing patient/family partnership and satisfaction.
Learning ObjectivesAt the conclusion of this activity, participants should be able to: Describe selected essential clinical and procedural elements needed in medical home practices to deliver chronic care for patients and their families Explain the importance and application of patient population management in the delivery of care for children with a chronic health conditions Explore the delivery of effective chronic care through a case study on pediatric asthma care in the medical home
Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities The AAP CME program aims to develop, maintain, and improve the competence, skills, and professional performance of pediatricians and pediatric healthcare professionals by providing quality, relevant, accessible, and effective educational experiences that address gaps in professional practice. The AAP CME program strives to meet participants' educational needs and support their life-long learning with a goal of improving care for children and families. (AAP CME Program Mission Statement, September 2010).The AAP recognizes that there are a variety of financial relationships between individuals and commercial interests that require review to identify possible conflicts of interest in a CME activity. The “AAP Policy on Disclosure of Financial Relationships and Resolution of Conflicts of Interest for AAP CME Activities” is designed to ensure quality, objective, balanced, and scientifically rigorous AAP CME activities by identifying and resolving all potential conflicts of interest prior to the confirmation of service of those in a position to influence and/or control CME content. The AAP has taken steps to resolve any potential conflicts of interest.All AAP CME activities will strictly adhere to the Accreditation Council for Continuing Medical Education (ACCME) Standards for Commercial Support: Standards to Ensure the Independence of CME Activities. In accordance with these Standards, the following decisions will be made free of the control of a commercial interest: identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the CME activity.The purpose of this policy is to ensure all potential conflicts of interest are identified and mechanisms to resolve them prior to the CME activity are implemented in ways that are consistent with the public good. The AAP is committed to providing learners with commercially unbiased CME activities.
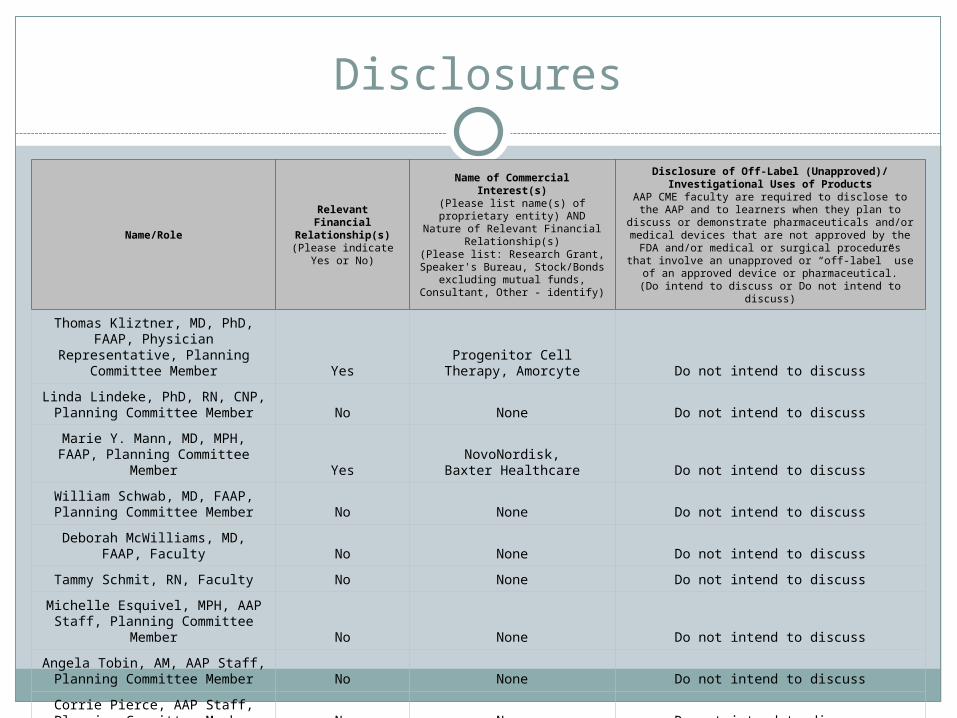
Disclosures
Name/Role
Relevant Financial Relationship(s)
(Please indicate Yes or No)
Name of Commercial Interest(s)
(Please list name(s) of proprietary entity) AND Nature of Relevant
Financial Relationship(s)(Please list: Research Grant,
Speaker's Bureau, Stock/Bonds excluding mutual funds,
Consultant, Other - identify)
Disclosure of Off-Label (Unapproved)/Investigational Uses of Products
AAP CME faculty are required to disclose to the AAP and to learners when they plan to discuss or
demonstrate pharmaceuticals and/or medical devices that are not approved by the FDA and/or medical or surgical procedures that involve an unapproved or
“off-label” use of an approved device or pharmaceutical.
(Do intend to discuss or Do not intend to discuss)
Thomas Kliztner, MD, PhD, FAAP, Physician Representative,
Planning Committee Member YesProgenitor Cell Therapy,
Amorcyte Do not intend to discuss
Linda Lindeke, PhD, RN, CNP, Planning Committee Member No None Do not intend to discuss
Marie Y. Mann, MD, MPH, FAAP, Planning Committee Member Yes
NovoNordisk,Baxter Healthcare Do not intend to discuss
William Schwab, MD, FAAP, Planning Committee Member No None Do not intend to discuss
Deborah McWilliams, MD, FAAP, Faculty No None Do not intend to discuss
Tammy Schmit, RN, Faculty No None Do not intend to discuss
Michelle Esquivel, MPH, AAP Staff, Planning Committee Member No None Do not intend to discuss
Angela Tobin, AM, AAP Staff, Planning Committee Member No None Do not intend to discuss
Corrie Pierce, AAP Staff, Planning Committee Member No None Do not intend to discuss
Disclosures
Commercial Supporters There is no commercial support associated with this course.
Product-Specific Advertising / Links to Product WebsitesNo product-specific advertising of any type appears in this activity. No links to product websites appear in this activity.
List of Principal Faculty and Credentials Deborah McWilliams, MD, FAAPTammy Schmit, RN
Name of Medium or Combination of Media Used Live webinar course
System requirementsPC-based attendeesRequired: Windows® 7, Vista, XP or 2003 ServerMacintosh®-based attendeesRequired: Mac OS® X 10.4.11 (Tiger®) or newer
Questions? Contact Corrie Pierce at [email protected] Privacy and Confidentiality Statement
At the American Academy of Pediatrics (AAP), we take the issue of privacy very seriously. We do not sell, distribute, barter, or transfer personally identifiable information obtained from a user to a third party without your consent. Any information collected on the Web site is only used for the purpose stated.The AAP list is only for important communications, and your e-mail address will not be sold or provided to third parties. You will not receive advertising or promotional materials on this list.The AAP may use “cookie” technology to obtain non-personal information from its online visitors. We do not extract personal information in this process nor do we provide this information to third parties. We also do not contact you based on the information in your cookie file.The AAP has taken steps to make all information received from our online visitors as secure as possible against unauthorized access and use. All information is protected by our security measures, which are periodically reviewed.
© COPYRIGHT AMERICAN ACADEMY OF PEDIATRICS, ALL RIGHTS RESERVED.American Academy of Pediatrics, 141 Northwest Point Blvd., Elk Grove Village, IL, 60007, 847-434-4000
Partnering with Patients and Families
in the Medical Home
2011 CME Webinar Series brought to you by the National Center for Medical Home Implementation
The Role of the Medical Home in Chronic Care Management
Deborah McWilliams, MD, FAAPTammy Schmit, RNMayo Clinic, Minnesota
May 10, 2011

Disclosures
We have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME activity.
I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

Looking Back…
The first webinar of this series:
Medical Home in Preventive and Acute Care (April 27 – archived online) Health care teams, family/professional partnerships History of medical home model The importance of quality improvement
Webinar Objectives
By the end of this webinar, the participant will be able to:
Describe selected essential clinical and procedural elements needed in medical home practices to deliver chronic care for patients and their families
Explain the importance and application of patient population management in the delivery of care for children with a chronic health conditions
Explore the delivery of effective chronic care through a case study on pediatric asthma care in the medical home
1) Changing landscape2) Assessing current needs of our practice3) Putting a structure into place4) Aspects of Spread/Maintenance
Pediatric Asthma Care Management

Unique aspects of our clinic
Large subspecialty clinicPrimary care
55% patients/dependents (self-insured) Pediatricians + Family Medicine (5 sites)
16 Pediatricians, 7 PNP, residency program 49 Fam Med, 11 FNP/PA’s, residency program
Issues with appointment access Prevalence of current pediatric asthma = 12%
Relatively low ER/Hosp utilization for asthma Hosp 0.2/1000 Healthy People 2010 Target
0.8/1000 ER 0.8/1000 Healthy People 2010 Target 1.7/1000

Pediatric Asthma Care Management
1) Changing landscape2) Assessing current needs of our
practice3) Putting a structure into place4) Aspects of Spread/Maintenance

Pediatric Asthma Care Management
1) Changing landscape MN Baskets of Care Healthcare Home MN Community Measurement
2) Assessing current needs of our practice3) Putting a structure into place4) Aspects of Spread/Maintenance
Baskets of Care Proposed Plan MN legislature
Classify severity onceAssess control twice a yearSpirometry min once a year
Once every 2 yrs for intermittent asthma
Peak flow monitoring (when spirometry not available)
Home assessment when neededFlu shots yearly, pneumococcal q 5 yrsIdentify/treat comorbid conditionsWritten Asthma Action PlansSpecific Education

“Healthcare/Medical Home” Certification
(Mayo Clinic, certified Feb 2011)
These 2 slides adapted from FAQ sheet developed by Steve Hagedorn, MD
The core principle is the same: The needs of the patient come first. The way we define and address our patient’s needs is changing. We use a team approach, with all team members working to the full extent of their licensure. We assess and address our patient’s needs beyond their chief complaint. We address the needs of our patient population whether they are seeing us in the office or not. We work more closely to coordinate care with the ED, hospital, care facilities and community partners.
The traditional paradigm we use to care for our patients is unsustainable. We are responsible for ever increasing numbers of patients. Advances in medicine and public health have resulted in a much older and medically complex patient population. We are expected to effectively deliver a broad range of preventive and chronic care services to our patients … A physician does not have time, resources or energy during a face-to-face office visit to accomplish this work. A new approach is needed.© 2011 Mayo Clinic

Tier Approach
Is it ethical to “tier” our patients?Our goal is to provide the right care, at the right time, in the right location, with the right provider. In our traditional model, we frequently provide unnecessary care to our healthy patients, and inadequate care to our sickest patients.
We need to develop systems to remain engaged with those patients and respond to their needs in a timely fashion to the best of our ability. By tiering our patients, based on their medical and psychosocial complexity, we are able to design and apply systems of care to better meet their needs.
© 2011 Mayo Clinic

MN Community Measurement

MN Community Measurement
Asthma well controlled (symptom questionnaire)
Not at increased risk of exacerbations Pt reported ER Visits + Hosp util < 2 in last yr
Current written asthma action plan
Ages 5-50. Pts trigger reporting via billing after 2 visits.

MN Community Measurement
Empower patients … but
Potential concerns: Systems issues … “Pullable” info system, searchable
registry External quality metrics “Exceptionism” “Not fair” = Not all asthmatics (visit driven) … for us =
35% = inclusion of subspecialty patients Potentially large impact …estimated 3188 pts at our sites Philosophical decisions

Pediatric Asthma Care Management
1) Changing landscape2) Assessing current needs of our
practice3) Putting a structure into place4) Aspects of Spread/Maintenance
Pediatric Asthma Care Management
1) Changing landscape2) Assessing current needs of our practice
Checking our assumptions Critical self-assessment New Rules
3) Putting a structure into place4) Aspects of Spread
Future steps Cost justification
Assessing our Needs
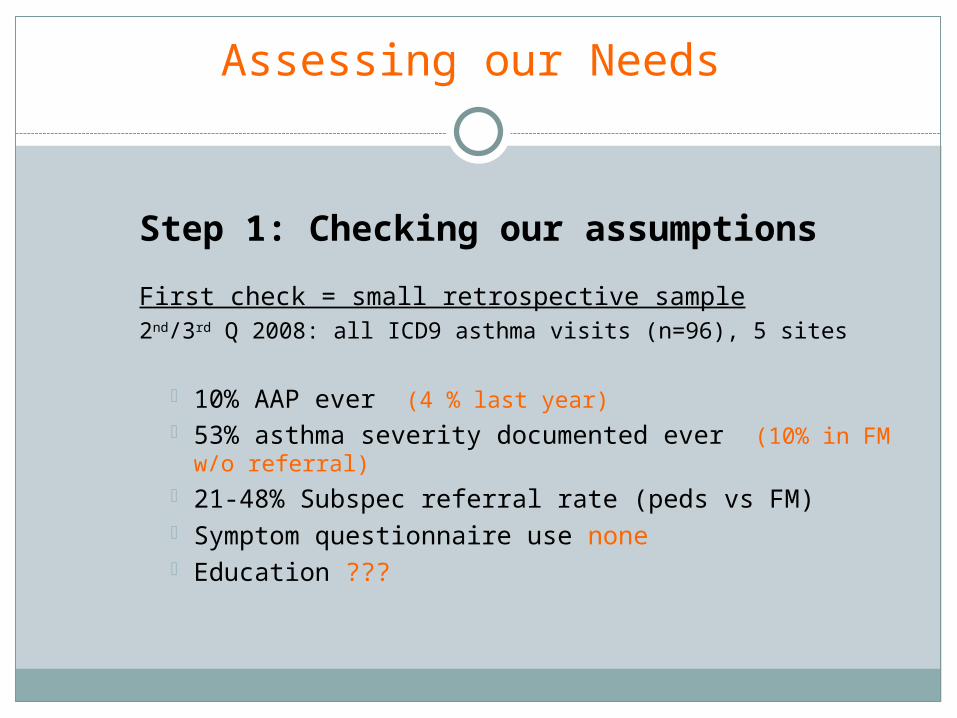
Step 1: Checking our assumptions
First check = small retrospective sample2nd/3rd Q 2008: all ICD9 asthma visits (n=96), 5 sites
10% AAP ever (4 % last year) 53% asthma severity documented ever (10% in FM
w/o referral) 21-48% Subspec referral rate (peds vs FM) Symptom questionnaire use none Education ???

As time has passed …. has this held true?
Intake of 1444 (25% subspecialty rate)
ER/Hosp < 2/year Meet MNCM goal 1395 (96.6%) Do not meet goal 49 (3.4%)
Current AAP Within last year 161 (11.2%) > 1 year ago 90 (6.2%) Never 1193 (82.6%)
As time has passed …. has this held true?
Intake of 818 (at first site)
Asthma Questionnaires Well controlled 509 (62.2%) Not well controlled 216 (26.4%) Poorly controlled 93 (11.4%)
Influenza vaccine 61%
Assessing our Needs
Step 2: Critical Self-Assessment (Where are we?)
No registry“Soft” diagnosisVariable nursing involvement Variable pt education availability Information not pull-able Inconsistent documentationNo “standard” of care (NAEPP/NHLBI)Minimal use of Asthma Action PlansMinimal (no?) support to school system
Critical self-assessment

Assessing our Needs
Step 3: New Rules (2009) Registry Agree to agree
“MDs prefer to practice alone together” Evidenced based care
Meet patient in a different way Right Care, right time, right place More longitudinal, less reactive
Care team model Less hierarchical, trust in others Work to full level of licensure
Need metrics for assessment Need admin support for forms “Cocoon of Support” = school system, family
Medical Home
Build an environment that values … Pt engagement/centeredness MD engagement Teamwork Evidenced based medicine Transparency – measurement and decision
making Continuous improvement – striving for excellence Systems approach – focus on efficiency

New Rules: Addition of RN Care Managers

Addition of RN Care Managers
New role not used in our practices before
How do systems match with their job role and the role of others
Always kept in mind the team effort
What things needed to change?
How could this role enhance care?
What might the barriers be?
© 2011 Mayo Clinic

Addition of RN Care Manager
Sneak peak to the future
(i.e…. Did it work ????)
Note: in the following slides, it will become evident what outcomes were most important to us by what metrics we followed (i.e., you might pick something different) …

Addition of RN Care Manager
Sneak peak to the future
(i.e…. Did it work ????)
Note: in the following slides, it will become evident what outcomes were most important to us by what metrics we followed (i.e., you might pick something different) … however, we hope their might be some general learnings from our experience that can be shared with others.

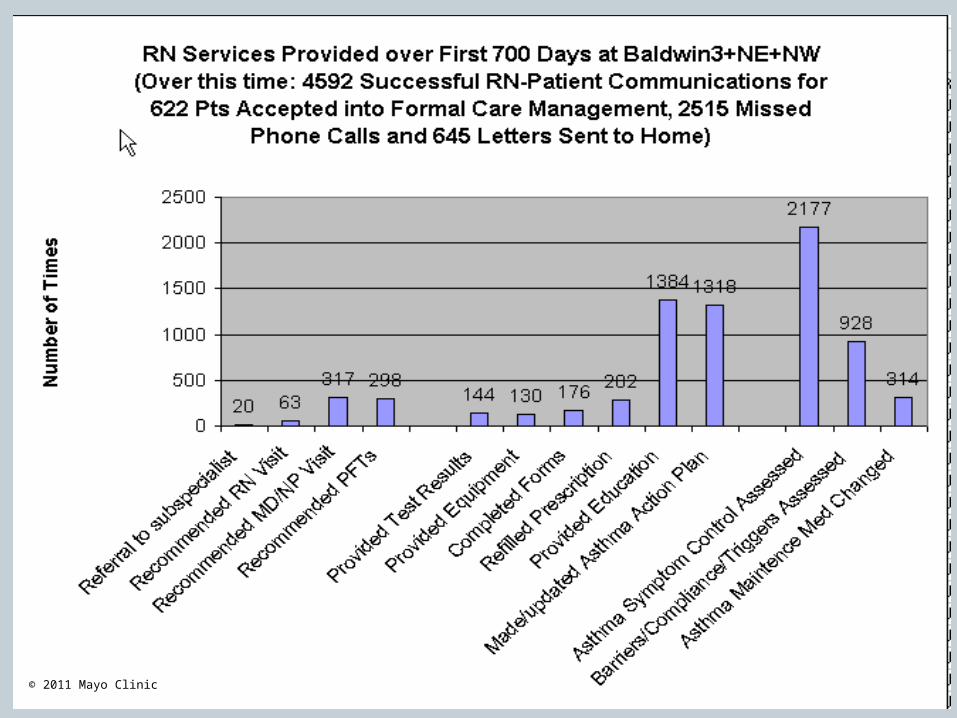
Results of Asthma Symptom Questionnaire
Notes: This includes ALL questionnaires (ex: handed out by care team, admin by CM, etc) New patients are being identified continually throughout this timeframe
© 2011 Mayo Clinic

Over past month: How much did Asthma impact activity?
(for all responses answered at First Site, N=2289)
0: Not at all
1: Almost Never
2: A little
3: Moderate
4: A lot
© 2011 Mayo Clinic

Work/School days missed = our “financial payoff”
© 2011 Mayo Clinic
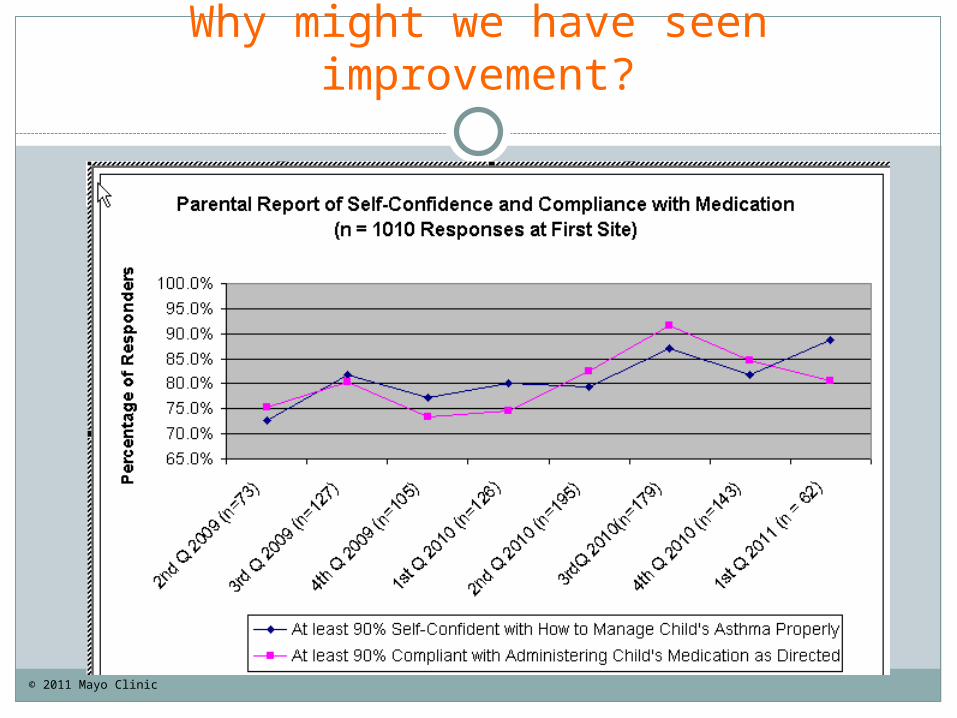
Why might we have seen improvement?
© 2011 Mayo Clinic

Pediatric Asthma Care Management
1) Changing landscape2) Assessing current needs of our practice3) Putting a structure into place4) Aspects of Spread/Maintenance

Pediatric Asthma Care Management
1) Changing landscape2) Assessing current needs of our practice3) Putting a structure into place
Enrollment Criteria Competencies Define RN “actions” Medical Rule Set Communication Plan Metric Development
4) Aspects of Spread/Maintenance
Putting a Structure into Place
Looking back, what was important? Enrollment/Graduation Criteria Competencies Expectations of RN “action”
Symptom assessment Needs assessment (barriers/technique/equipment) Form completion
Medical Rule set (NAEPP/NHLBI Guidelines) Develop tools
Questionnaires Database
Communication with rest of care team Metrics (outcomes and cost/effort)

Structure: Enrollment
Enrollment Criteria Ages 5-18, current primary care patient “Persistent” Asthma Asthma not under Good Sx Control (Red, Yellow) Active Health-care Utilizers (ER/Hosp)
Graduation: “Green” (well controlled) for a year
No maintenance med No ER/Hosp use
CM is also a resource for general asthma questions
Need IT tools … but process must be done first
Structure: Competencies
Triage/assessment Knowledge Documentation Pt Education Facilitator Communication
© 2011 Mayo Clinic
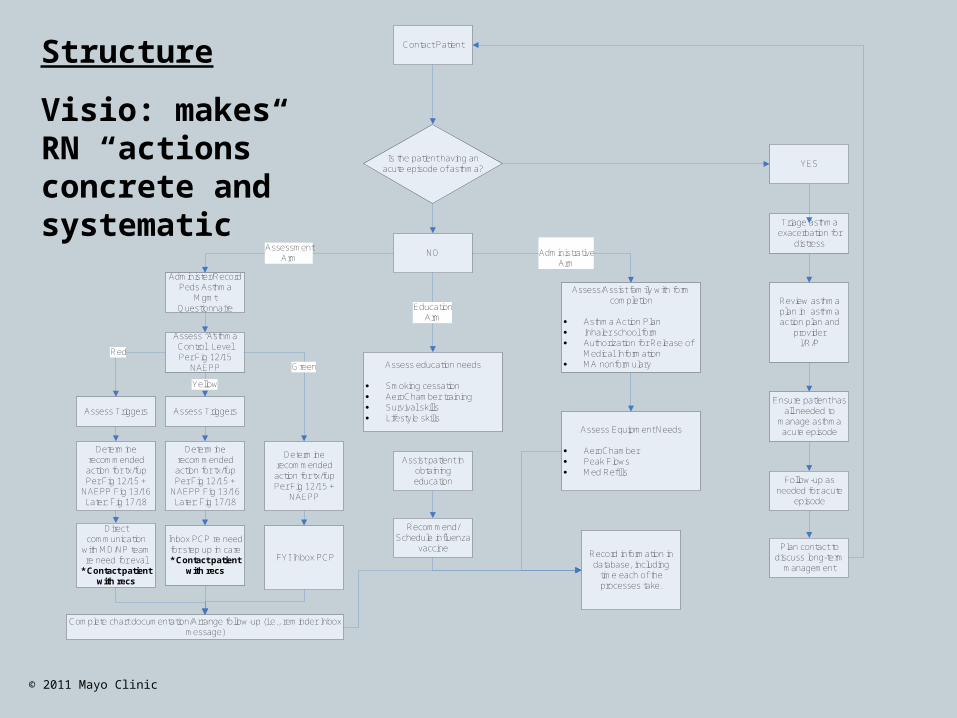
NO
Administer/Record Peds Asthma
Mgmt Questionnaire
Assess Triggers Assess Triggers
Determine recommended action for tx/fup Per Fig 12/15 +
NAEPP
Determine recommended action for tx/fup Per Fig 12/15 +
NAEPP Fig 13/16Later: Fig 17/18
Determine recommended action for tx/fup Per Fig 12/15 +
NAEPP Fig 13/16Later: Fig 17/18
Assess education needs
· Smoking cessation· AeroChamber training· Survival skills· Lifestyle skills
Assist patient in obtaining education
Recommend/Schedule influenza
vaccine
Assess/Assist family with form completion
· Asthma Action Plan· Inhaler school form· Authorization for Release of
Medical Information· MA nonformulary
Assess Equipment Needs
· AeroChamber· Peak Flows· Med Refills
AssessmentArm
EducationArm
AdministrativeArm
Record information in database, including
time each of the processes take.
Assess “Asthma Control” Level Per Fig 12/15
NAEPP
Red
Yellow
Green
FYI Inbox PCP
Inbox PCP re need for step up in care* Contact patient
with recs
Direct communication
with MD/NP team re need for eval
* Contact patient with recs
Complete chart documentation/Arrange follow-up (i.e., reminder Inbox message)
Contact Patient
Is the patient having an acute episode of asthma?
YES
Triage asthma exacerbation for
distress
Review asthma plan in asthma action plan and
providerI/R/P
Ensure patient has all needed to
manage asthma acute episode
Follow-up as needed for acute
episode
Plan contact to discuss long-term
management
Structure
Visio: makes RN “actions” concrete and systematic
© 2011 Mayo Clinic

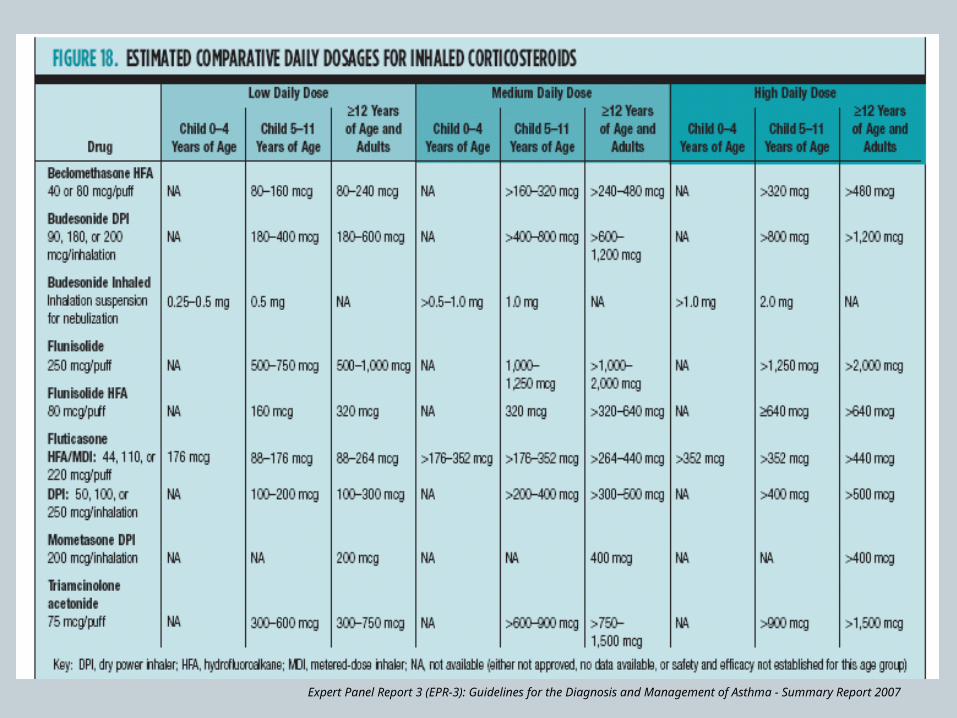
Structure: Medical Rule set (NAEPP/NHLBI)allows RNs to perform full assessment w/
recommendations
Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma - Summary Report 2007

Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma - Summary Report 2007
Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma - Summary Report 2007

Structure: Tools
Other tools: EMR Hot buttons for ordering
Meds Spirometry
EMR Flowsheets Track pts longitudinally over time
Website information/links Standard Asthma Action Plan Educational flow sheet/ patient education
materials Questionnaires Database
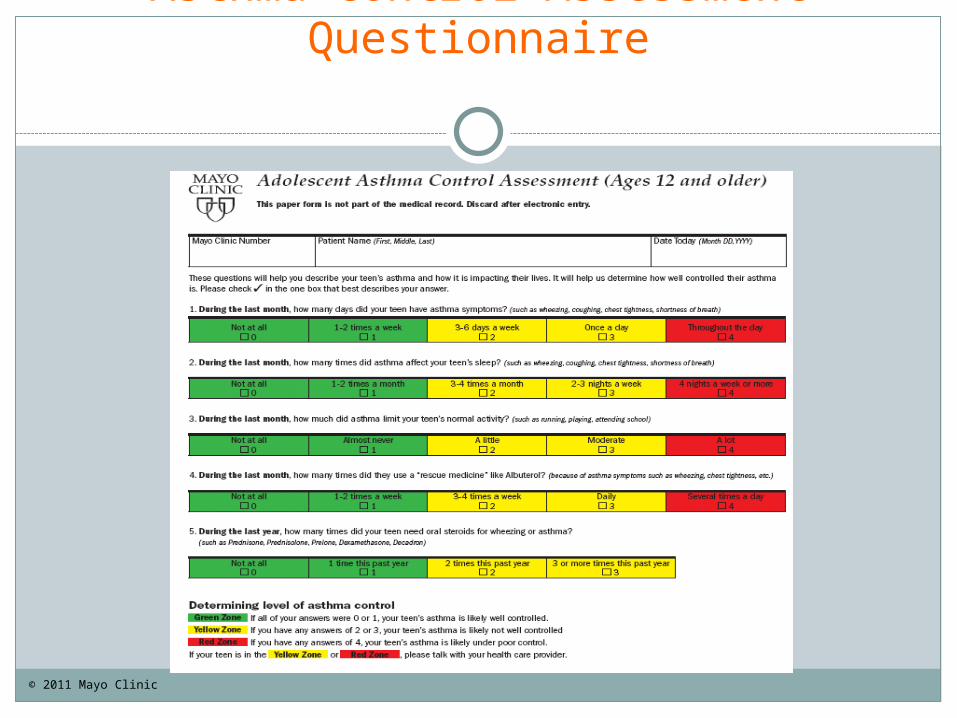
Asthma Control Assessment Questionnaire
© 2011 Mayo Clinic

© 2011 Mayo Clinic
Structure: Communication within the Care Team
Goals:
1) Develop processes
ex: phone calls, electronic communication
2) Way to identify asthmatics
ICD9 codes poor way to identify asthmatics
1531 pts: 785 from ICD9s
27 from ER/Hosp use
644 Albuterol on med list (LPN)
75 Med refill/form requests, triage call (RN/Sec)
3) Shift “spirit” of team work Engage the whole team, including the “front line” with concrete processes
Structure: Communication within the Care Team
Tools to improve communication SBAR
Situation, Background, Assessment, Recommendation Coaching sessions/ access to medical expert Debriefing Group meetings Feedback from the practice –Ask, ask, ask
Decrease the sense of hierarchy … everyone has valuable input

Structure … Results of increased communication with Care Team (PDSA
cycles)
© 2011 Mayo Clinic
© 2011 Mayo Clinic

© 2011 Mayo Clinic
© 2011 Mayo Clinic

Structure: Gather Metrics that you need719 days of experience (484 pts in CM)
Total (%) Non visit
RN time MD/NP involved
Initial full asthma CM
assess
484(15.1%)
86% 35.7 min 73% (7.1 min, 5.2 min )
Partial Asthma Control assess
1516(47.3%)
94% 27.8 min 55%(4.9 min, 2.7 min)
Twice/year Full assessment
172(5.4%)
92% 39.4 min 76%(5.0 min, 3.8 min)
Provider f/u visit 203(6.3%)
65% 21.2 min 43%(6.8 min, 2.9 min)
F/u re: med change, acute
620(19.4%)
84 % 22.9 min 40 %(6.5 min, 2.5 min)
Education 208(6.5%)
77% 33.5 min 60%(7.5 min, 2.6 min)
Total 3203 88% 28.6 avg 3.4 min avg © 2011 Mayo Clinic

Structure: Gather Metrics that you need
719 days of experience (484 pts in CM)
Total (%) Non visit
RN time MD/NP involved
Initial full asthma CM
assess
484(15.1%)
86% 35.7 min 73% (7.1 min, 5.2 min
)
Partial Asthma Control assess
1516(47.3%)
94% 27.8 min 55%(4.9 min, 2.7
min)
Twice/year Full assessment
172(5.4%)
92% 39.4 min 76%(5.0 min, 3.8
min)
Provider f/u visit
203(6.3%)
65% 21.2 min 43%(6.8 min, 2.9
min)
F/u re: med change, acute
620(19.4%)
84 % 22.9 min 40 %(6.5 min, 2.5
min)
Education 208(6.5%)
77% 33.5 min 60%(7.5 min, 2.6
min)
Total 3203 88% 28.6 avg 3.4 min avg
Average 4.0 contacts/yrAverage 4.0 contacts/yr
For those in Care ManagementFor those in Care Management
1.8 hr/pt/year RN1.8 hr/pt/year RN13.6 min/pt/yr MD/PNP13.6 min/pt/yr MD/PNP
This allows us to justify FTE needs This allows us to justify FTE needs and plan better over time, including and plan better over time, including need for blocked “nonvisit” time for need for blocked “nonvisit” time for
MD/NPsMD/NPs© 2011 Mayo Clinic
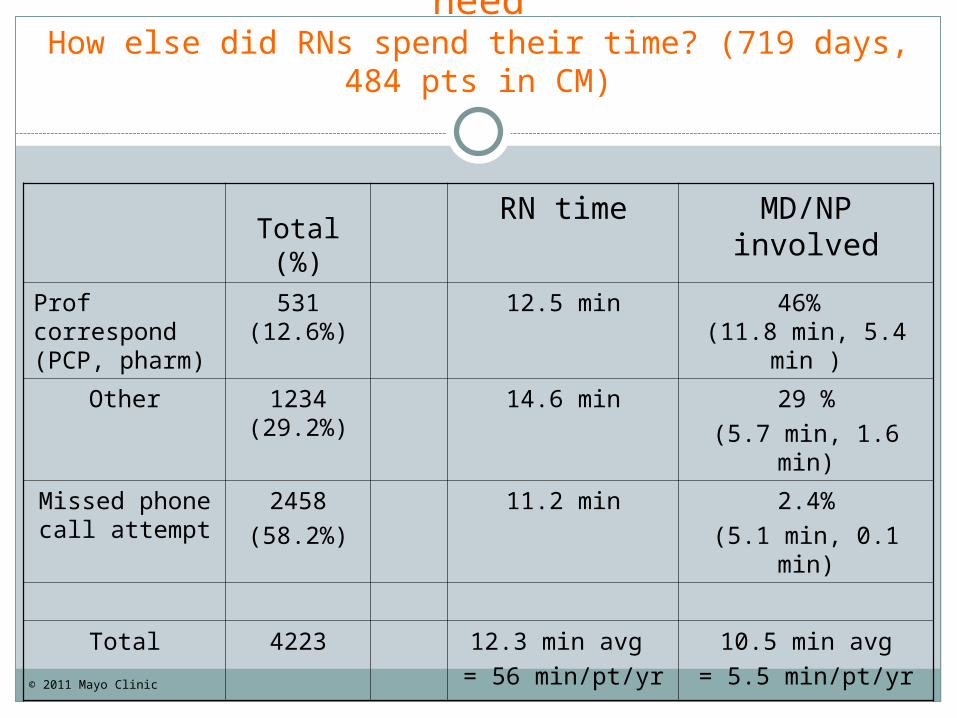
Structure: Gather Metrics that you needHow else did RNs spend their time? (719 days, 484
pts in CM)
Total (%)
RN time MD/NP involved
Prof correspond(PCP, pharm)
531(12.6%)
12.5 min 46% (11.8 min, 5.4
min )
Other 1234(29.2%)
14.6 min 29 %(5.7 min, 1.6 min)
Missed phone call attempt
2458(58.2%)
11.2 min 2.4%(5.1 min, 0.1 min)
Total 4223 12.3 min avg = 56 min/pt/yr
10.5 min avg= 5.5 min/pt/yr
© 2011 Mayo Clinic

Structure: Gather Metrics that you needHow else did RNs spend their time? (719 days, 484
pts in CM)
Total (%)
RN time MD/NP involved
Prof correspond(PCP, pharm)
531(12.6%)
12.5 min 46% (11.8 min, 5.4 min )
Other 1234(29.2%)
14.6 min 29 %(5.7 min, 1.6 min)
Missed phone call attempt
2458(58.2%)
11.2 min 2.4%(5.1 min, 0.1 min)
Total 4223 12.3 min avg = 56 min/pt/yr
10.5 min avg= 5.5 min/pt/yr
Hmmm…Hmmm…
11.2 min/missed phone call11.2 min/missed phone call
= 0.15 FTE !! (for 484 pts)= 0.15 FTE !! (for 484 pts)
(Also 0.1 FTE making letters)(Also 0.1 FTE making letters)
This allows us to look for areas to This allows us to look for areas to increase efficiencies, including increase efficiencies, including
involvement of others in care team involvement of others in care team and other technology than just and other technology than just
telephone usetelephone use© 2011 Mayo Clinic

Pediatric Asthma Care Management
1) Changing landscape2) Assessing current needs of our practice3) Putting a structure into place4) Aspects of Spread/Maintenance
Keep It Real Start small…build on success Measure what you need Change in culture occurs over time

Aspects of Spread/Maintenance
If I could give you a hug over the phone, I would this is the first time I have felt like someone cares for my daughter.
The other day when picking him up school he was playing dodge ball and running with the other kids and was doing great, I thought “sweet"!!!!
Motivation …Keep it real
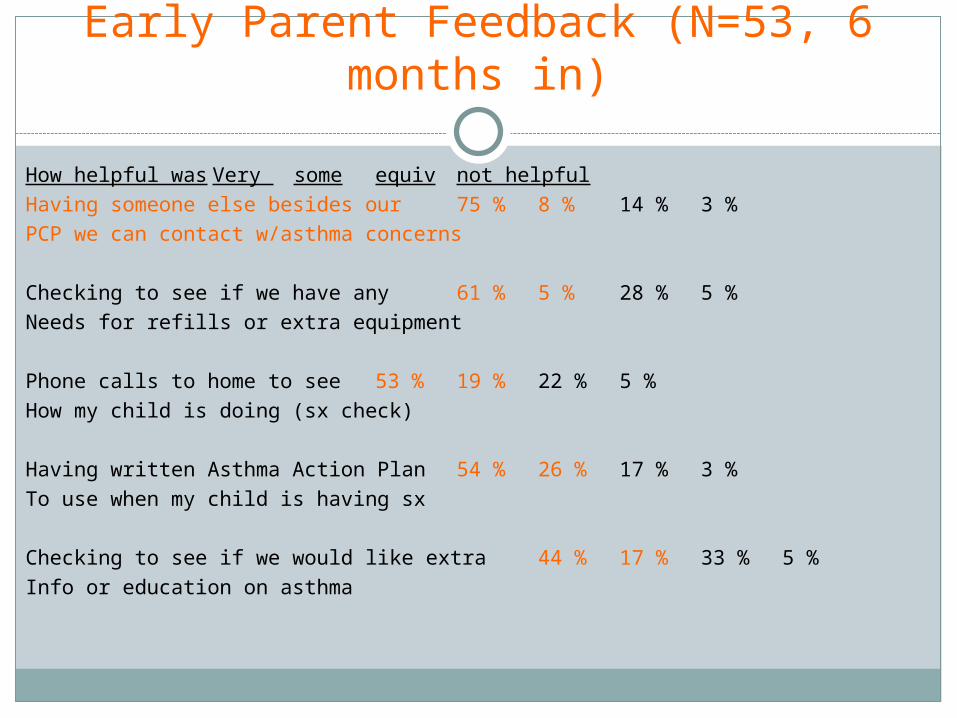
Early Parent Feedback (N=53, 6 months in)
How helpful was Very some equiv not helpfulHaving someone else besides our 75 % 8 % 14 % 3 %PCP we can contact w/asthma concerns
Checking to see if we have any 61 % 5 % 28 % 5 %Needs for refills or extra equipment
Phone calls to home to see 53 % 19 % 22 % 5 %How my child is doing (sx check)
Having written Asthma Action Plan 54 % 26 % 17 % 3 %To use when my child is having sx
Checking to see if we would like extra 44 % 17 % 33 % 5 %Info or education on asthma

Early Parent Feedback (N=53, 6 months in)
Before CM After CM
Comfort level managing asthma = E/VG 46.1% 88.9%Rate child’s asthma care = E/VG 80.5% 86.1%Would definitely recommend care here 80.6% 86.1%
(to others with asthma)
E = ExcellentVG = Very Good

Maintenance: Start Small with Attainable Victories
First 6 months of Care Management, Site 1 (start Mar 2009)
2nd-3rd Q’08 Goal (n=180)
Current AAP 2% 20% Current Severity 41% 60%

Maintenance: Start Small with Attainable Victories
First 6 months of Care Management, Site 1 (start Mar 2009)
2nd-3rd Q’08 Goal 2nd-3rd Q’09 (n=180) (n=234) Current AAP 2% 20% 48.1% Current Severity 41% 60% 75.3%

Maintenance: Start Small with Attainable Victories
First 6 months of Care Management, Site 1 (start Mar 2009)
2nd-3rd Q’08 Goal 2nd-3rd Q’09 2nd-3rd Q’10 (n=180) (n=234)(n=213) Current AAP 2% 20% 48.1% 73.7%Current Severity 41% 60% 75.3% 92.5%

Aspects of Spread/Maintenance
Metrics, metrics, metrics What are we accomplishing? What are we doing (task-wise)?
What would have been done by MDs What would have not been done otherwise
What does this “cost”? $$ RN/MD times
What might we assume will change over time?
Where are areas for improved efficiencies? IT improvements Use of other care team members

Spread/Maintenance = Gradual Change in Culture
© 2011 Mayo Clinic

Got Medical Home?
Have a specific question or need regarding medical home?
Contact us!
[email protected]/433-9016 ext 7605
Related Documents











