Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to having your photo taken and allow Project ECHO to use this photo and/or video. If you don’t want your photo taken, please let us know. Thank you! DISCLAIMER

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to having your photo taken and allow Project ECHO to use this photo and/or video. If you don’t want
your photo taken, please let us know.
Thank you!
DISCLAIMER

PHI includes, but is not limited to:- Patient name- Date of birth- Address- Occupation- Name of patient’s friends/family- Other identifiable features, i.e.
scars, tattoos, hair/eye color
Please DO NOT disclose any Protected Health Information (PHI)

Conflicts of Interest
• None related to today’s discussion
Introduction to the Geriatric ECHO Clinic at Project ECHO Nevada
5 minute overview

Outline
• Project ECHO Nevada Overview • Hub and Spoke Model• ECHO clinic anatomy

Project ECHO Nevada
• ECHO stands for: Extensions for Community Healthcare Outcomes
• Project ECHO is a global telehealth platform (you are participating in it right now!)
• Project ECHO Nevada started in 2012
• 4th iteration of Project ECHO model
Current Recurring Clinics (please attend!)1. Antibiotic Stewardship2. Cardiology 3. Complex Pediatrics4. Geriatrics5. Pain Management6. Public Health7. Medication Assisted
Treatment8. Sports Medicine

Hub and Spoke Model
• Hub team includes:• Facilitators (stay consistent across all sessions)• Multidisciplinary team of Subject Matter Experts (SME) (present for
10-15 minutes at one session and attend other sessions)
• Spokes (Target) include:• Multidisciplinary care teams from urban and rural Nevada (sometimes
farther)
• Not a traditional telemedicine model (provider to patient): Increases access to care by facilitating knowledge transfer between health care providers using case-based learning.

Hub and Spoke Model(Clinic Specific)• Hub team includes:
• Patti Swagger – Education/Administrative Partner• Kelley MacMillan – Social Worker/Behavioral Health• Leslie Backer – Pharmacy• Kelly Presser – Nursing• Mordechai Lavi – MD• Umanga Sharma - MD
• Spokes (Target) include:• All of you!
• Not a traditional telemedicine model (provider to patient): Increases access to care by facilitating knowledge transfer between health care providers using case-based learning.

ECHO Clinic Anatomy
Three main sections to an ECHO clinic session1. Introductions
1. Spoke and then hub participants2. 5-10 Minutes
2. Case presentation by 1-2 spoke sites including challenges, questions, etc. 1. Cases submitted ahead of time are preferred (Case Submission Form will be
available on the webpage)2. 20-40 Minutes
3. Didactic presentation by Hub Team/Special Guests 1. 15 - 30 minutes2. Q & A
Dementia ScreeningMordechai Lavi, MDUNR Med Geriatrics
Project ECHO Nevada
Objectives
• To describe different tests that can screen for dementia.• Discuss potential limitations in screening for dementia.

Outline
• Review previous ECHOs on Dementia and their content• Dementia Definition• Who should be screened
• Things to consider
• Screening tools• Mini-Cog• MOCA• 6 CIT
Dementia
Definitions
Dementia - a progressive syndrome characterized by acquired losses in cognition and emotional abilities that are severe enough to interfere with daily functioning and quality of lifeSyndrome – a group of symptoms often seen together or a condition characterized by a set of symptoms seen together
Disease – a process with specific signs and symptoms; it often has a known cause and known consequences

Previous Project ECHO Nevada Didactics on Dementia• Best Practices in Dementia Care July 2018-October 2018
• Polypharmacy• Delirium• Dementia – Neuropsychiatric symptoms• Competence vs Capacity
• Dementia Series April 2019 – October 2019• Creating a person-centered care plan for persons with dementia and
behavioral expressions• Best practices for (De)prescribing medications used to treat dementia• Best Practices to support ADL in persons with dementia• Ethical dilemmas when caring for someone with dementia • Diagnostic criteria for different types of dementia

Who should be screened?
GuidelinesUniversal screening not recommend by USPSTF- Medicare Annual Wellness visit
has you complete a Mini-cog
Clinical Clues- Missed appointments- Medication issues
- Adherence (compliance)- Errors
- Behavioral Concerns- Personal hygiene- Change in personality
- Weight loss- Patient or family mention
concerns

What do you do when you decide to screen someone?Get a good history:
• Onset, duration, and course of symptoms• Progressive – months to years• Acute – hours to days• Subacute – days to weeks
• Associated events (e.g. stroke, hospital stay, medication changes)• PMH, FH, PSH, medications (OTC, supplements, herbs, recreational drugs)
Assess to see if this could be another disease process- Psychiatric Disease
- Depression (Personal Health Questionnaire (PHQ) 2 or PHQ 9)- Delirium
- Acute confusion (3-minute diagnostic assay - Confusion Assessment Method)- Delirium is almost always caused by an acute medical issue (infection, constipation, pain,
over/under medicating)
Labs to consider: CBC, CMP, B12, TSH/fT4

What to do once you decide you are not dealing with depression or delirium
Choose your screening method of choice (next slide)There are multiple considerations when choosing a screening test including:- primary language- literacy (both reading and health)- education level
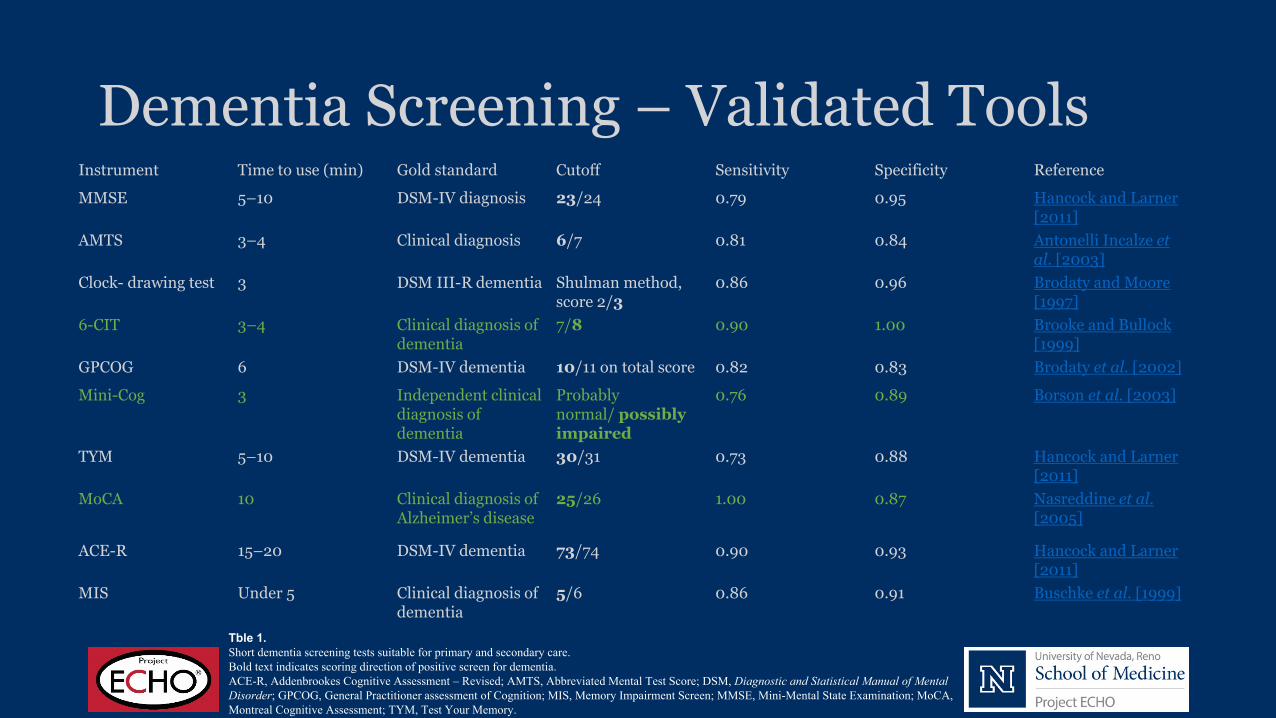
Dementia Screening – Validated Tools Instrument Time to use (min) Gold standard Cutoff Sensitivity Specificity Reference
MMSE 5–10 DSM-IV diagnosis 23/24 0.79 0.95 Hancock and Larner [2011]
AMTS 3–4 Clinical diagnosis 6/7 0.81 0.84 Antonelli Incalze et al. [2003]
Clock- drawing test 3 DSM III-R dementia Shulman method, score 2/3
0.86 0.96 Brodaty and Moore [1997]
6-CIT 3–4 Clinical diagnosis of dementia
7/8 0.90 1.00 Brooke and Bullock [1999]
GPCOG 6 DSM-IV dementia 10/11 on total score 0.82 0.83 Brodaty et al. [2002]
Mini-Cog 3 Independent clinical diagnosis of dementia
Probably normal/ possibly impaired
0.76 0.89 Borson et al. [2003]
TYM 5–10 DSM-IV dementia 30/31 0.73 0.88 Hancock and Larner[2011]
MoCA 10 Clinical diagnosis of Alzheimer’s disease
25/26 1.00 0.87 Nasreddine et al. [2005]
ACE-R 15–20 DSM-IV dementia 73/74 0.90 0.93 Hancock and Larner [2011]
MIS Under 5 Clinical diagnosis of dementia
5/6 0.86 0.91 Buschke et al. [1999]
Tble 1.Short dementia screening tests suitable for primary and secondary care.Bold text indicates scoring direction of positive screen for dementia.ACE-R, Addenbrookes Cognitive Assessment – Revised; AMTS, Abbreviated Mental Test Score; DSM, Diagnostic and Statistical Manual of Mental Disorder; GPCOG, General Practitioner assessment of Cognition; MIS, Memory Impairment Screen; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; TYM, Test Your Memory.
Mini-Cog
1. Screens for dementia (almost always followed by another test) 2. Multiple languages3. Three-minute, two-item test 4. Scored on a five-point scale
• Three points per word remembered• Two points for a correct clock• Universal Mini-Cog© Instrument
Mini-Cog Step 1
Make sure you have the patient’s attention.
Instruct the patient to listen carefully to and remember three unrelated words, and then to repeat the words back to you so you know they heard the words correctly. You may want to say something like, “What we’re going to do next will take some concentration. Ready?”
Mini-Cog Step 2
Ask the patient to repeat the words to ensure understanding.
Once you are sure the patient is paying attention, say, “I am going to say three words that I want you to remember now and later. The words are banana, sunrise, chair. Please say them now.” Give the patient three tries to repeat the words. You may repeat the words to them for each try. If they are unable to repeat the words back to you after three tries, go directly to the clock drawing.

Mini-Cog – Step 3Ask the patient to draw a clock.
Provide the patient with page 2 of the Universal Mini-Cog© Instrument. Say all the following phrases in the order indicated below:1. “Please draw a clock in the circle.” It is acceptable to provide a sheet of
paper with the circle already drawn for the patient, as depicted on the standardized Mini-Cog©
2. “Put all the numbers in the circle”3. When #2 is completed, say, “Now set the hand to show ten past eleven.”4. If the patient has not finished the clock drawing in 3 minutes,
discontinue and ask for the word recall items.

Mini-Cog – Step 4
Ask patient to recall the 3 words.You will be asking the patient to recall the set of 3 words you gave them at the beginning of the test. Say, “What were the three words I asked you to remember?” Administer this portion of the test even if the patient did not accurately repeat the 3 words earlier.

Montreal Cognitive Assessment (MoCA)
• 7-10 minute test• Multiple languages• MoCA Test Basic• MoCA Test Blind• 12 items – score out of 30 points• Official training offered by mocatest.org
• Hour-long training• Cost - $125 for two-year certification
• Half off future tests• Group Rates

Six-Item Cognitive Impairment Test (6 CIT)• 2-3 minute test• 7 steps (6 questions)• 28 total points• Multiple languages• International

6- CIT (points associated with wrong answer)1. What year is it? (4)2. What month is it? (3)3. Provide address to memorize 4. About what time is it? (3)5. Count backwards from 20-1 (4)6. Say the months of the year in reverse (4)7. Repeat Address (10)
Limitations to screening
Only a clinic tool, not a diagnostic instrument • Limiting factors include:
• Language barriers• Education level• Functional assessment• Acute or chronic medical conditions• Cultural traditions

References
1. Medina-Walpole A, Pacala JT, Potter JF, eds. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine. 9th ed. New York: American Geriatrics Society; 2016.
2. Sheehan, Bart. “Assessment Scales in Dementia.” Therapeutic Advances in Neurological Disorders 5.6 (2012): 349–358. PMC. Web. 17 Sept. 2018.
Accessed 10/14/20191. https://mini-cog.com/2. https://www.mocatest.org/3. http://www.wales.nhs.uk/sitesplus/documents/862/FOI-286g-
13.pdf
Thank youQuestions?
Related Documents











