401 Direct Determination of Vasa Recta Blood Flow in the Rat Renal Papilla Christoph Holliger, Kevin V. Lemley, Susan L. Schmitt, Frances C. Thomas, Channing R. Robertson, and Rex L. Jamison From the Departments of Chemical Engineering Physiology, Biological Sciences, and Medicine, Stanford University, Stanford, California SUMMARY. Blood flow in vasa recta capillaries of the exposed renal papilla of young antidiuretic rats (n = 18) was determined by an adaptation of the video-photometric technique of Intaglietta. The erythrocyte velocity and capillary diameter in vasa recta (« = 97) were measured at the same location by means of fluorescence video microscopy, with fluorescein-labeled bovine 7-globulin as a plasma marker. A factor relating erythrocyte velocity to mean cross-sectional blood velocity was determined in vitro to permit the calculation of single vasa recta blood flows from the measured indices, erythrocyte velocity and capillary diameter. Mean blood flow in descending vasa recta was 8.83 ± 0.96 (SE) nl/min, significantly greater than that in ascending vasa recta, 4.82 ± 0.34 nl/min. The total numbers of ascending and descending vasa recta at the base of the exposed papilla were also determined. Over 1500 vasa recta were identified as ascending vasa recta or descending vasa recta in electron micrographs of three papillas. At this level in the papilla (2 mm from the tip), there were four ascending vasa recta for each descending vas rectum. From the total numbers of ascending vasa recta and descending vas rectum, single vessel blood flows were converted to total blood flow. Total blood outflow in all ascending vasa recta, 11.3 /xl/min, substantially exceeded total blood inflow in all descending vasa recta, 5.2 fil/min. The difference between outflow and inflow (6.1 ^1/min) represents an estimate of water uptake by the papillary microcirculation, and is more than adequate to accommodate the known rate of water reabsorption from the collecting ducts of the exposed papilla. (Circ Res 53: 401-413, 1983) IN addition to supplying oxygen and substrates and removing metabolic wastes, the renal medullary cir- culation performs two other functions. It preserves the axial osmotic gradient of the medulla by coun- tercurrent exchange of water and solutes between descending and ascending vasa recta (DVR and AVR, respectively) (Scholander, 1957; Berliner et al., 1958; Gottschalk, 1961; Gottschalk et al., 1962; U1- rich et al., 1962; Thurau and Levine, 1971; Sanjana et al., 1975, 1976). It also removes water reabsorbed from the descending limb of Henle's loop (including the medullary pars recta) and the medullary collect- ing duct (Ullrich et al., 1962), but the absolute rate at which AVR removes water from the medulla has not been determined (Sanjana et al., 1975, 1976). The issue of water mass balance in the medulla must be investigated further; medullary blood flow should be analyzed quantitatively. Consider fluid balance in the exposed tip of the renal papilla (Fig. 1). Micropuncture experiments in the young rat have shown that approximately 3 ^l/ 1 ™ 11 OI " water is reabsorbed from the collecting ducts of the exposed papilla in antidiuresis (Oliver et al., 1982) and 5 fi\/ min in water diuresis (Jamison et al., 1971). Since the rate of water removal from the descending limb in the papilla is unknown (Gottschalk, 1961; Jami- son et al., 1973), the aforesaid figures underestimate the rate at which water is added to the papillary interstitium. The papillary tip of the young rat weighs about 2 mg (see below); water uptake by the papillary microcirculation is therefore of the order of 1-3 ml/min per g tissue weight in the antidiuretic rat. Estimates of total papillary blood inflow yield values ranging from 0.4 to 0.7 ml/min per g tissue CORTEX I OUTER T MEDULLA u SHORT LOOP OF A <> > HENLE—{; COLLECTING TUBULE INNER MEDULLA t J_ \ -J! 1 \ \ \ 1 \ 1 i \ \r-~\\ ) LONG LOOP OF HENLE V J V y 'rtH M )/, /, /, A \ t, \ 1r VASA RECTA PELVIS y FIGURE 1. Mass balance for water in the renal medulla. The three kinds of structures in the medulla are depicted: short and long loops of Henle, branched collecting ducts, and descending and ascending vasa recta. Arrows indicate direction of fluid flow. Water is added to the medullary interstitium by absorption from the medullary pars recta and descending limb of the loop of Henle, the collecting duct, and the descending vasa recta. Since the epithelium of the thin and thick ascending limbs is water-impermeable, ascending vasa recta represent the only channels by which the added water can be removed from the medulla. by guest on April 5, 2018 http://circres.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

401
Direct Determination of Vasa Recta Blood Flow in theRat Renal Papilla
Christoph Holliger, Kevin V. Lemley, Susan L. Schmitt, Frances C. Thomas,Channing R. Robertson, and Rex L. Jamison
From the Departments of Chemical Engineering Physiology, Biological Sciences, and Medicine, Stanford University, Stanford, California
SUMMARY. Blood flow in vasa recta capillaries of the exposed renal papilla of young antidiureticrats (n = 18) was determined by an adaptation of the video-photometric technique of Intaglietta.The erythrocyte velocity and capillary diameter in vasa recta (« = 97) were measured at the samelocation by means of fluorescence video microscopy, with fluorescein-labeled bovine 7-globulinas a plasma marker. A factor relating erythrocyte velocity to mean cross-sectional blood velocitywas determined in vitro to permit the calculation of single vasa recta blood flows from themeasured indices, erythrocyte velocity and capillary diameter. Mean blood flow in descendingvasa recta was 8.83 ± 0.96 (SE) nl/min, significantly greater than that in ascending vasa recta,4.82 ± 0.34 nl/min. The total numbers of ascending and descending vasa recta at the base of theexposed papilla were also determined. Over 1500 vasa recta were identified as ascending vasarecta or descending vasa recta in electron micrographs of three papillas. At this level in the papilla(2 mm from the tip), there were four ascending vasa recta for each descending vas rectum. Fromthe total numbers of ascending vasa recta and descending vas rectum, single vessel blood flowswere converted to total blood flow. Total blood outflow in all ascending vasa recta, 11.3 /xl/min,substantially exceeded total blood inflow in all descending vasa recta, 5.2 fil/min. The differencebetween outflow and inflow (6.1 ^1/min) represents an estimate of water uptake by the papillarymicrocirculation, and is more than adequate to accommodate the known rate of water reabsorptionfrom the collecting ducts of the exposed papilla. (Circ Res 53: 401-413, 1983)
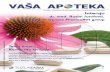
IN addition to supplying oxygen and substrates andremoving metabolic wastes, the renal medullary cir-culation performs two other functions. It preservesthe axial osmotic gradient of the medulla by coun-tercurrent exchange of water and solutes betweendescending and ascending vasa recta (DVR andAVR, respectively) (Scholander, 1957; Berliner et al.,1958; Gottschalk, 1961; Gottschalk et al., 1962; U1-rich et al., 1962; Thurau and Levine, 1971; Sanjanaet al., 1975, 1976). It also removes water reabsorbedfrom the descending limb of Henle's loop (includingthe medullary pars recta) and the medullary collect-ing duct (Ullrich et al., 1962), but the absolute rateat which AVR removes water from the medulla hasnot been determined (Sanjana et al., 1975, 1976).The issue of water mass balance in the medulla mustbe investigated further; medullary blood flowshould be analyzed quantitatively. Consider fluidbalance in the exposed tip of the renal papilla (Fig.1). Micropuncture experiments in the young rat haveshown that approximately 3 ^l/1™11 OI" water isreabsorbed from the collecting ducts of the exposedpapilla in antidiuresis (Oliver et al., 1982) and 5 fi\/min in water diuresis (Jamison et al., 1971). Sincethe rate of water removal from the descending limbin the papilla is unknown (Gottschalk, 1961; Jami-son et al., 1973), the aforesaid figures underestimatethe rate at which water is added to the papillaryinterstitium. The papillary tip of the young ratweighs about 2 mg (see below); water uptake by the
papillary microcirculation is therefore of the orderof 1-3 ml/min per g tissue weight in the antidiureticrat. Estimates of total papillary blood inflow yieldvalues ranging from 0.4 to 0.7 ml/min per g tissue
CORTEX I
OUTER TMEDULLAuSHORTLOOP OF A <> >HENLE—{;
COLLECTINGTUBULE
INNERMEDULLA
t
J_\
- J !
1
\
\\
1
\
1
i
\
\r-~\\
)LONGLOOP OFHENLE
V JV y
'rtHM)/,
/,
/,A
\t,
\
1r
VASARECTA
PELVIS y
FIGURE 1. Mass balance for water in the renal medulla. The threekinds of structures in the medulla are depicted: short and long loopsof Henle, branched collecting ducts, and descending and ascendingvasa recta. Arrows indicate direction of fluid flow. Water is added tothe medullary interstitium by absorption from the medullary parsrecta and descending limb of the loop of Henle, the collecting duct,and the descending vasa recta. Since the epithelium of the thin andthick ascending limbs is water-impermeable, ascending vasa rectarepresent the only channels by which the added water can be removedfrom the medulla.
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

402 Circulation Research/Vol. 53, No. 3, September 1983
weight by the isotope-labeled albumin-accumula-tion technique and from 1.0 to 1.8 ml/min per gtissue weight by the isotope-labeled erythrocytemethod (Thurau and Levine, 1971; Wolgast, 1973;Ganguli and Tobian, 1974; Solez et al., 1974; Auk-land, 1976; Chuang et al., 1978; Jamison and Kriz,1982). In other words, the estimated rate of capillarywater uptake exceeds the rate of plasma inflow,which seems inherently unlikely. Apparently, themeasurements of blood flow or protein concentra-tion involve large errors, or water is removed fromthe papilla by an extravascular route (Schmidt-Niel-sen, 1977).
In addition to the likelihood that these indirectmethods for determination of medullary blood flowmay be inaccurate (Aukland, 1976; Jamison andKriz, 1982), they measure either blood inflow oroutflow, but not both, and therefore cannot be usedto determine whether outflow of blood exceeds in-flow by an amount sufficient to satisfy the require-ment of mass balance of water in the renal medulla.The purpose of this study was to determine bothinflow and outflow of blood to the exposed papilla.
Methods
Preparation of AnimalsEighteen young (5-6 weeks) Munich-Wistar rats [108 ±
10 (SD) g body weight] were allowed water ad libitum butwere deprived of food the night before the experiment.They were anesthetized with Inactin (110 mg/kg bodyweight), and the left renal papilla was exposed by excisionof the ureter, as previously described (Battilana et al.,1978). Body temperature was regulated to 37 ± 1°C witha servocontrolled heating table. The animals received anintravenous infusion of normal saline at 2.5-3% of bodyweight per hour throughout the experiment. Blood pres-sure was monitored through a femoral arterial catheter,and urine was collected from the right kidney through abladder catheter for determination of osmolality. Meanarterial blood pressure exceeded 90 mm Hg in all experi-ments used.
Single Vasa Recta Blood Flow, Qv,Single capillary blood flow was calculated according to
the following equation:
Qvr = VbloojA ,jv
where Q^ = single capillary blood flow in a vas rectum(pL/sec); Vbk)od = cross-sectional blood velocity (mm/sec);A = capillary cross-sectional area (/im2); V^ = erythrocytevelocity in a vas rectum (mm/sec); F = V /̂Vbiood (dimen-sionless); D = capillary diameter (Mm).
To determine Q*,, values of V^, D, and F were meas-ured as follows.
Erythrocyte Velocity, V ^Erythrocyte velocities were determined by the video
method of Intaglietta et al. (Tompkins et al., 1974; Intag-lietta et al., 1975), as described previously (Gussis et al.,1979a, 1979b). Briefly, a silicon-intensified target televi-sion camera (COHU 4410 SIT; COHU, Inc.) was mountedon a Leitz intravital microscope (Ernst Leitz GmbH). The
video signal from the camera of the image of the micro-scopic field entered a photoanalyzer (IPM, model 202,Instrumentation for Physiology and Medicine) and a videomonitor (COHU, DM 17/C), where the image was dis-played. Video recordings of capillary blood flow weremade for later analysis. Two electronic 'windows,' sepa-rated by 11-18 ^m and generated by the photoanalyzer,were positioned manually upstream and downstream overa capillary. Fluctuations in light intensity resulting fromthe passage of red blood cells alternating with cell-freeplasma past the windows were monitored electronically.The upstream and downstream 'window' signals pro-duced by the photoanalyzer were cross-correlated to de-termine a transit time for the erythrocytes between thewindows. Erythrocyte velocities were computed by divid-ing the distance between windows by the time delay (redblood cell transit time) which maximized the cross-corre-lation. By replaying the videotape with the windows re-positioned, Vrbc could be measured in several differentvessels. The terms V^ and erythrocyte velocity referstrictly to determinations made using this technique andshould not be interpreted as necessarily indicating individ-ual RBC velocity or the average velocity of all RBC's in agiven capillary cross-section.
Since our initial investigations were published (Gussiset al., 1979a, 1979b), several changes have been incorpo-rated into the system to increase the accuracy of thevelocity measurements. A PDP 11/34 computer (DigitalEquipment Corporation) was employed to sample instan-taneous red cell velocity. Erythrocyte velocity for eachcapillary, V^, was the time average of 100 samples overa total period averaging 3 minutes, which has been pre-viously shown to give reproducible values (Gussis et al.,1979a). The computer also modified the raw velocity datafrom the correlator, using a calibration curve, and cor-rected for local variations in video magnification. Thevelocity calibration curve was determined, using the videomethod, by measurement of apparent velocities of ran-domly placed spots on the rim of a wheel rotating at aknown angular speed. Measurements made by thismethod were reproducible to within 5% between 0.1 and1.6 mm/sec wheel rim velocity for window separationsranging from 11 to 18 jim.
During an experiment, a field of view was selected inwhich several vessels were clearly outlined. AVR consist-ently outnumbered DVR, so fields had to be carefullyselected to include at least one DVR.
Vasa Recta Diameter, DTo permit simultaneous determination of capillary di-
ameters, the incident light illumination system previouslyused was replaced by a Leitz Ploemopak (Ernst Leitz,GmbH) through-the-objective illumination system, em-ploying a double dichroic mirror especially designed forfluorescence microscopy (Ploem, 1967) and a DC HBO200-VV mercury arc lamp (Osram). As described in Appen-dix I, 5-10 mg of fluorescein isothiocyanate (FTTC)-labeled7-globulin, injected intravenously, were employed to en-hance contrast of capillary walls for measurement of vesseldiameters. Diameter measurements were performed on apreviously calibrated video monitor by means of a caliper.Each diameter was measured by two observers, eachobserver making three measurements.
Ratio of Vrt^Vwood, F
As is evident from Equation 1, the measurement of V,^by means of the video microscopy technique is related to
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

HoUiger et al. /Direct Determination of Blood Flow in Vasa Recta 403
iiov AC ;
Parfution Chambar-*-
Quartz Capillary^
Coodaraer
Hg-«rc
To:
VxiecKacordar
Videomonitor
Photoanalyzar
Correlator
Tdevtton Camera
o -*—Microscope
%X-Y Tibk
FIGURE 2. Apparatus designed to determine the factor F. Blood isadded to the perfusion chamber and kept suspended by a stirrer. Therate of blood flow down the quartz capillary is controlled by airpressure. Video microscopy is used to determine red cell velocity, V^.A mercury arc lamp and a condenser provide the source of light.Capillary blood flow is determined by timing the experiment andmeasuring the volume of effluent blood that accumulates on theplexiglass trough.
mean cross-sectional blood velocity through a proportion-ality factor which we designate *F." The range of permis-sible values for F is 1 < F < 2 , the lower bound repre-senting single-file RBC flow (when RBC diameter approx-imates capillary diameter) and the upper bound corre-sponding to Poiseuille flow (a parabolic velocity profile)which occurs when vessel diameter is much greater thanerythrocyte diameter. In addition to capillary diameter, Fmay be a function of mean cross-sectional blood velocity,hematocrit, and the shape, size, and deformability oferythrocytes (Fahraeus, 1928; Barbee and Cokelet, 1971;Gaehtgens et al., 1976). Numerous efforts have been madeto examine this complex relationship (Fahreus, 1928; Bar-bee and Cokelet, 1971; Gaehtgens et al., 1976), yet Fremains ill-defined for the ranges of diameter (8-25 jim)(Jamison and Kriz, 1982), microvessel hematocrit (10-25%) (Ullrich et al., 1961), and V^ (0.1-1.0 mm/sec)(Gussis et al., 1979a, 1979b) which occur in vasa recta.We sought a value of F determined under conditionsapproximating those of our experiments as closely aspossible.
An apparatus was designed to control blood flowthrough a small-bore quartz capillary (Warden Quartz)(Fig. 2).' A reservoir supplied blood to a syringe, in whicha stirrer kept the red cells dispersed. Blood entered thecapillary driven by pressure from a tank of air monitoredby a transducer. V^ in the capillary was determined byvideo microscopy, using a horizontally mounted videomicroscope focused on the capillary, which was transil-luminated by light from a DC mercury arc lamp. Theapparatus was otherwise identical to that described for invivo determination of V^.
A microscope micrometer was recorded on videotapefor calibration of magnification. The blood was pouredinto the reservoir and the chamber pressurized. A pressureof 20-30 mm Hg was used to flush the capillary; it wasthen reduced until the desired V^ was achieved. Duringvideo recordings of velocity, the capillary blood effluentwas collected in a plexiglass trough filled with immersion
* The experiments were done in collaboration with Dr. GeorgeHarrell of the Department of Radiology, Stanford University Schoolof Medicine.
oil. Once a steady state was reached, the capillary wasshifted to allow a new drop of effluent to form, and thevideotape and timer were started. V,^ was measuredduring 3- to 10-minute periods. At the end of the experi-ment, the effluent was aspirated into a calibrated pipetteto determine the volume. The volume divided by collec-tion time and cross-sectional area of the capillary was usedto calculate Vwood- So that the hematocrit within the cap-illary could be determined, the capillary was placed insidea microhematocrit rube, sealed twice with epoxy, andcentrifuged for 5 minutes. The hematocrit of the effluentwas determined in the same way.
Scanning electron microscopy (SEM) was used to meas-ure the capillary diameter for calculation of V ^ ^ fromvolumetric flow rate. Each capillary was glued on a holderwith epoxy, sputtered with gold for 2 minutes, and thenviewed end-on in the scanning electron microscope.
Human blood, with erythrocytes similar in size to thoseof the rat, was drawn into a 7-ml Vacutainer containing10.5 mg ethylenediamine tetraacetic acid (EDTA) (BectenDickinson). (Attempts to use rat blood failed, due to theformation of microthrombi.) After centrifugation for 10minutes, plasma was decanted from erythrocytes and spun12 minutes more to remove platelets. The red cells wereresuspended in the platelet-free plasma to a predeter-mined hematocrit. Capillaries were siliconized with a 7%solution of DRI-Film SC-87 (Pierce), diluted in chloroform,and rinsed twice with toluene and acetone. Just beforeuse, they were checked for patency with saline.
Determination of Number of Ascending andDescending Vasa Recta at the Base of the ExposedPapilla
The measurements described above were used to cal-culate single vessel blood flows, using Equation 1. Toconvert single vessel blood inflow to total inflow andsingle vessel outflow to total outflow of blood from theexposed papilla, the numbers of DVR and AVR, respec-tively, at the base of the exposed papilla were determined.Three specific capabilities were required: (1) distinguishvasa recta from thin loops of Henle, (2) distinguish AVRfrom DVR and determine the ratio of AVR to DVR, and(3) determine the total number of vasa recta.
Preparation of Tissue Sections
The rat was anesthetized, and the left renal artery wascatheterized and perfused at 100-120 mm Hg with pro-caine in 0.1 M phosphate buffer solution (pH = 7.3). Thekidney was prefixed by perfusion with glutaraldehyde-formaldehyde in phosphate buffer (pH = 7.2) and per-fused for 2 minutes with 30% bovine serum albumin in0.1 M Na2HPO«. The renal vein and artery were clamped,and the kidney was removed and immersed immediatelyin a glutaraldehyde-formaldehyde solution and refriger-ated. (The composition of the immersion solution was 1%paraformaldehyde, 0.01% picric acid, 1.1% glutaralde-hyde, and 0.1 M Na2HPO4. The osmolality was 504mOsm/kg H2O. The perfusion solution was composed ofequal volumes of the immersion solution and 0.1 MNa2HPC>4 solution.) After 1 hour, the ureter and cortexwere cut away, and the exposed papilla was returned tothe fixative and refrigerated for 24 hours to completefixation.
The papilla was prepared for ultrathin sectioning byuranyl acetate and osmium tetroxide staining, dehydrationin alcohol, and embedding in epoxy araldite. Severalultrathin sections made 2 mm from the tips of three
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

404
papillas were placed on copper grids for transmissionelectron microscopy. Thick sections from two of thesepapillas were also made at the 2 mm distance from thetip. They were stained with methylene blue, and the totalcross-sectional area of the papilla was determined byplanimetry on light microscopic photographs.
Identification of Vasa Recta
Both peripheral and central regions of the cross-sectionof the papilla were examined in a Hitachi HU-11E-1transmission electron microscope, and as each vessel wasidentifed, it was labeled on a corresponding low-powerelectron micrograph. Blood vessels were differentiatedfrom thin limbs of Henle's loop by their albumin-filledlumens (Fig. 3). Descending vasa recta were differentiatedfrom AVR according to their ultrastructure (Schwartz etal., 1976). AVR were distinguished by fenestrated endoth-elia; DVR had an endotheUum without fenestrae (Fig. 3).In addition, DVR, but not AVR, had abundant pinocytoticvesicles along the basement membrane. Identity of AVRand DVR in representative micrographs was confirmedindependently by Kriz (personal communication). Morethan 500 vasa recta were identified in each of threepapillae.
We next addressed the question of how many capillariesidentified as AVR might actually be communicating cap-illaries, since their ultrastructure is identical to that ofAVR. Communicating capillaries erroneously identified asAVR could spuriously elevate the calculated rate of bloodflow out of the papilla. We determined the proportion oftransverse flowing (functionally communicating) capillar-ies among all vasa recta at the base of the exposed papillafrom videotapes made of four experiments. Of 148 vessels,there were 105 with ascending flow, 40 descending, three
FIGURE 3. Electron micrograph of a section at the base of the exposedpapilla. Two vasa recta can be distinguished from the two Henle'slimbs (L) by their albumin-filled lumens. Note the attenuated endo-thelium of the ascending vas rectum (A) in contrast to the thickerdescending vas rectum (D), the cytoplasm of which has numerousorganelles. 1 = interstitium. 2000X.
Circulation Research/Vol. 53, No. 3, September 1983
capillaries which described a 'loop,' and one clearly trans-verse capillary. We therefore considered the proportion of'AVR' which were actually communicating capillaries tobe negligible.
The number of vasa recta per grid on the electronmicroscope stage was determined for approximately 40-50 grid squares per papilla (corresponding to approxi-mately 500 vasa recta). Using the measured area of thegrids, we converted the number of vasa recta per grid tothe number of vasa recta per unit area. Those vessels ofwhich only a part lay within a grid were counted only ifthe visible portion of the cross-sectional area exceededhalf the area of the average vessel in that particular grid.
The total cross-sectional area of the papilla 2 mm fromthe papillary tip was determined by planimetry, usinglight microscopic photographs of the papilla. The totalnumbers of AVR and DVR were calculated from theAVR:DVR ratio, the capillary density, and the cross-sec-tional area.
Total Papillary Blood FlowTotal inflow of blood to the exposed papilla was cal-
culated as the product of total number of DVR and themean value of Qv, for DVR. Likewise, total outflow ofblood was calculated as the product of total number ofAVR and the mean value of Qv, for AVR. A correctionwhich takes into account the possible elliptical configura-tion of vasa recta in cross-section is discussed in AppendixI.
These calculations were performed for the region 2 mmfrom the papillary tip. To convert absolute flows to flowsper tissue mass, 19 rats (9 male, 10 female), averaging 110g, were anesthetized, and the left kidney was removedand weighed. The papilla was quickly excised and thepapillary tip severed 2 mm from the tip. The whole kidneyand both portions of the papilla were weighed in pre-weighed capped microcentrifuge tubes.
StatisticsUnless stated otherwise, the data are presented as
means ± SE. Paired determinations were tested for signif-icance by Student's t-test (Snedecor, 1966).
Results
Urinary OsmolalityThe mean osmolality was 1250 ±190 mOsm/kg
H2O.
Erythrocyte Velocity, V ^Individual values are illustrated in Figure 4 and
summarized in Table 1. In 25 DVR from 18 rats,mean V ^ was 1.04 ± 0.10 mm/sec. In 72 AVR fromthe same 18 rats, mean V^ was 0.38 ± 0.03 mm/sec, significantly lower than in DVR (P < 0.001).
Vasa Recta Diameter, DIndividual values are illustrated in Figure 5 and
summarized in Table 1. The DVR (mean diameter15.6 ± 0.5 fim) were narrower than AVR (20.0 ±0.4 Mm) (P < 0.001).
Ratio of Vrt^Vb,,,,,,,, F
Table 2 presents the results of the determinationof F, and Figure 6 illustrates V ^ as a function of
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

HoUiger et al./Direct Determination of Blood Flow in Vasa Recta 405
DVR AVRFIGURE 4. Vasa recta erythrocyte velocity, V^. Individual determi-nations of Vr*,. in vasa recta were averaged and treated as one valuefor DVR and AVR per animal. Lines connect the average V^ for DVR(left) and AVR (right) in the same animal The average value for the18 animals ± 1 SE IS depicted for DVR (left) and AVR (right) by thevertical lines.
Vbiood- In 25 separate determinations in which Vbioodranged from 0.14 to 1.70 mm/sec, V^ varied from0.18 ± 0.08 to 2.05 ± 0.10 mm/sec, duration ofcollection ranged from 2.5 to 11 minutes, 'feed*
TABLE 1
Erythrocyte Velocity, Capillary Diameter, and Blood Flow inIndividual Vasa Recta
(mm/sec) D(Mm) Qv, (nl/min)
DVRJ AVRJ DVR AVR DVR AVR
Mean
SE
P
n'
"t
1.04
0.10
0.38
0.03
<0.001
25
18
72
18
15.6
0.5
<0
20.0
0.4
.001
8.83 4.82
0.96 0 34
<0.001
hematocrit ranged from 9 to 21%, and capillarydiameters ranged from 12.5 to 28.4 fim; the meanvalue for F is 1.4 ± 0.3 SD. We were unable to finda significant dependence of F on V ^ ^ , hematocrit,or capillary diameter for the range of values for eachvariable selected in the experiments, a fact that maybe attributed to the actual variabilitity of flow in thisregime where the transition from single (one red cellper cross-section) to multiple file flow (several redcells per cross-section) takes place, and to unavoid-able imprecision inherent in the techniques.
Single Vasa Recta Blood Flow, Qv,Individual values are illustrated in Figure 7 and
summarized in Table 1. Blood flow in DVR (8.83 ±0.96 nl/min) was almost twice that in AVR (4.82 ±0.34 nl/min) (P < 0.001).
AVR:DVR Ratio and Total Numbers of AVR andDVR
The AVR:DVR ratio and the total numbers of AVRand DVR are summarized in Table 3. The total
VASARECTA
DIAMETER
• Number of vasa recta; -(number of animalsJ DVR = descending vasa recta; AVR = ascending vasa recta.
DVR AVRFIGURE 5. Vast recta diameter, D. See legend to Figure 4 for furtherexplanation.
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

406 Circulation Research/Vo/. 53, No. 3, September 1983
TABLE 2
Determination of F*
Experimentno.
12345678910111213141516171819202122232425
D(Mm)
13131315562725252626272626282526252526272320212020
(sec)
400505457646719439457548513584646390414340595644450338514384315134143142136
(mm/sec)
0.46 ± 0.040.43 ± 0.050.95 ± 0.420.30 ± 0.010.40 ± 0.040.35 ± 0.020.18 ±0.080.27 ±0.010.24 ± 0.010.21 ±0.010.21 ± 0.010.38 ± 0.020.31 ± 0.030.45 ± 0.020.26 ± 0.010.48 ± 0.040.72 ± 0.030.21 ±0.010.44 ± 0.040.46 ± 0.071.37 ± 0.301.80 ±0.102.05 ±0.101.73 ± 0.201.71 ± 0.10
20.520.520.519.319.318.018020.020.020.020.06.09.011.211.210 010.010.010.010.013.013.013.013.013 0
FU,
——14.712.713.3——14 014.0—
15.07.413.013.58.65.74.9—
333.1——
6.06.98.7
—
22.016.7——————
19.0—
18.7—
13.8———
959.7—
6.06.99.713.6
(mm/sec)
0.2990.3500.5590.1600.2250.2080.1400.2010.2200.1710.1650.3620.2330.4790.2050.2730.3670.1680.3380 2711.0701.1041.3211 6961.629
F
1541.231.701 881.781.681.291 341 091.231.271.051.330.941.271.761.961.251.301.701.281.631.541.021.05
*F = V.tciVbtood; D, diameter of glass capillary; T^n, duration of collection;blood velocity. — = not determined, n = 25; F = 1.4 ± 0.3 SD.
, RBC velocity; H, hematocrit; V i ^ j , mean cross-sectional
vblood(mm/sec)
0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0 2.2 2.4
Vrfjc (mm/sec)
FIGURE 6. Determination of F = V^:Vu^. The results of 25 experiments performed using the apparatus depicted in Figure 2 are illustrated. Theslope of the line is 1/1.4 (= r1).
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

HoUiger et al. /Direct Determination of Blood Flow in Vasa Recta
18
407
16 -
14 -
12 -
VASA 1 0
RECTABLOODFLOW 8
(nl/min)
DVRFIGURE 7. Single vasa recta blood flow,for further explanation.
AVR2w- See legend to Figure 4
number of vasa recta was the product of the averagenumber of vessels per unit area (1436 mm"2) mul-tiplied by the average papillary cross-sectional areaat the base determined by light microscopy (2.20mm2). This was converted to total number of AVRand DVR with the aid of the AVR:DVR ratio estab-lished from all grids. More than 1500 individualcapillaries were identified in three papillas. Thenumber of AVR exceeded that of DVR by approxi-mately 4:1. As shown in Table 3, there were 593DVR and 2351 AVR at the base of the exposedpapilla 2 mm from the tip.
Total Papillary Tip Blood FlowMultiplying the number of DVR (593) times the
mean Q^ for the DVR (8.83 nl/min) yielded a value
TABLE 3Number of Vasa Recta at Base of Exposed Papilla
Papilla
1 Mean
No. of VR countedVR per grid*VR per mm2
AVR:DVR ratioCross-sectional area of pa-
pilla base (mm2)
563 50212.1 11.91420 13974.26 4.071.97 1.53t
53713.61490 14363 55 3.962 65 2.05
Total number of VR at base = (1436 mm"2) X (2.05 mm2) =2994. For an AVR:DVR ratio of 3.96: 593 DVR; 2351 AVR.
' Area of electron microscope grid: papillas 1 and 2, 0.00852mm2; papilla 3, 0.00913 mm2.
f A portion of papilla 2, at 2 mm from the tip, was inadvert-ently cut during sectioning. To determine total cross-sectionalarea of the base at 2 mm, the cross-sectiona] areas of the papillaat 1.8 mm and 1 9 mm from the tip were determined and thecross-sectional area of the papilla 2.0 mm from the tip wasdetermined assuming a cone shape.
for blood flow entering the exposed papilla of 5.2jil/min. The corresponding calculation of blood flowleaving the exposed papilla in AVR was 11.3 ^ 1 /min. Extrapolated values for total blood flows inindividual papillas, calculated using the averagenumber of DVR and AVR, are illustrated in Figure8. In each case, total AVR flow exceeded total DVRflow (mean difference = 6.1 jtl/min; range, 1.0-11.9^1/min).
Papillary WeightThe mean weight of the left kidney was 465 ± 34
SD mg. The mean weights of the papilla and thepapillary tip were 4.93 mg ± 1.48 and 1.8 ± 0.66mg, respectively. Thus, the blood inflow to theexposed papilla averaged 5.2 jtl/min per 1.81 mgpapillary tip, or 2.9 ml/min per g tissue, and theblood outflow from the exposed papilla averaged11.3 jil/min per 1.81 mg papillary tip, or 6.2 ml/min per g tissue.
Discussion
We found that at the base of the exposed renalpapilla of the rat, blood flow leaving in the AVR,11.3 /al/min, is twice as great as that entering in theDVR, 5.2 jtl/min. The difference, 6.1 /xl/min, rep-resents an estimate of net capillary uptake of water.These values were calculated from the total numberof AVR and DVR multiplied by mean single vasarecta blood flow (Qw) of AVR and DVR, respectively.Mean Qvr was 4.8 nl/min in AVR and 8.8 nl/minin DVR, but AVR outnumbered DVR by a ratio ofapproximately 4:1. In each vas rectum, Q^ wascalculated from V^, D, and F, according to Equation1. Our findings and conclusions are based on severalmethods with their specific accuracies and certainassumptions, as follows.
The rats were anesthetized with Inactin, which,as recently emphasized (De Lano and Zweifach,1981), can cause fluctuations in blood pressure. Ex-
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

408
20
18 "
16
14
TOTALPAPILLARY 1 2
TIPBLOODFLOW 1 0
(ul/min)
8
DVR AVRFIGURE 8. Total papillary tip blood flow. The values were determinedby multiplying the number of DVR times mean Q^ for DVR (left)and number of AVR times the mean Q ^ for AVR (right). For furtherexplanation, see legend to Figure 4.
posure of the papilla impairs urinary concentratingability (Jamison, 1970), and may stimulate the re-lease of vasoactive prostaglandins (Chuang et al.,1978).
Erythrocyte Velocity, VH*The techniques used to determine V ^ and their
limitations have been discussed previously (Holligeret al., 1975; Gussis et al., 1979a). In brief, the presenttechnique is a substantial improvement over othertechniques employed to determine V^ , in our opin-ion. Marsh and Segel (1971) viewed red cells flowingin a vas recta in vivo through a microscope. Theanimal lay on a movable stage. V ^ was determinedas that velocity at which the stage was moved man-ually to maintain the red cells immobile. This rela-tively crude technique has been abandoned byMarsh in favor of the present video technique.Bottcher and Steinhausen (1976) used a microcine-
Circulation Research/Vol. 53, No. 3, September 1983
matic technique in which the film ran across theobjective in an axis perpendicular to that of illumi-nated red cells flowing in a vas rectum. Images ofthe red cells in a vas rectum traced parallel lines atan angle to the film centerline. From the angle ofthe lines and the film speed, V ^ was calculated.Variability of Vrbc during short time intervals wouldnot be easily detected. Another limitation is that thecontrast between capillary wall and flowing bloodwas not enhanced by a plasma marker (like FITC-labeled 7-globulin) to increase the accuracy of thediameter measurements. Because of the improvedprecision in our methodology, a substantial differ-ence was detected between V ^ in DVR and thelower V^ in AVR. Bottcher and Steinhausen (1976)previously reported that erythrocyte velocity islower in AVR than in DVR.
Our value for V,^ in DVR, 1.04 ± 0.10 mm/sec,is higher than that found by Bottcher and Steinhau-sen (1976) in rats (0.64 ± 0.05 mm/sec) and Marshand Segel (1971) in hamsters (0.50 ± 0.03 mm/sec).These differences may be attributable to differencesin experimental conditions, or to technical improve-ments in the present study. The latter is suggestedby the fact that the value 1.04 mm/sec representsan increase from our own earlier determinations(Gussis et al., 1979a, 1979b), presumably due to anincrease in measurable range of V^. The value forVrt* in AVR, 0.38 ± 0.03 mm/sec, compares reason-ably well with Bottcher and Seinhausen's 0.49 ±0.04 mm/sec (1976), but is higher than Marsh andSegel's value in the hamster, 0.18 ± 0.04 mm/sec(1971).
Vasa Recta and Quartz Tube Diameters, DThe accuracy of Qv, also depends on the precision
of the capillary diameter measurements, especiallysince the square of the diameter is used (Eq. 1). Thedata in Table 4 indicate a small (<3%) error whenthe video system is used to measure quartz capillar-ies of known diameter. Capillary wall contrast wasenhanced by the injection of FITC-labeled 7-glob-ulin, together with a Ploemopak fluorescence micro-scope. We previously tried FITC-labeled high-mo-lecular-weight dextran, but the rats often becamehypotensive and edematous. Injection of FITC-la-beled albumin was followed by a progressive accu-mulation of fluorescence in the papillary intersti-tium. Whether this represents capillary leakage ofFITC-albumin (Moffat, 1969; Venkatachalam andKamovsky, 1972), or of the FTTC moiety, alone, is
Quartz Capillary
Observer 1Observer 2SEMf
TABLE 4Diameter Measurements
Capillary 1
8.4 ±0.2*8.6 ± 0.38.6 ± 0.3
Capillary
16.8 ±0 .17.1 ±0 .17.4 ±0 .
2
223
* Values in /im; meqan ± SD.•f SEM, scanning electron microscopy; values in
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

Holliger el al. /Direct Determination of Blood Flow in Vasa Recta 409
unknown. Injection of FITC-labeled 7-globulin wasfound to be a much improved method for outliningcapillary lumina. Not only was the interface betweenplasma and capillary walls well demarcated, but thecross-correlation of the upstream and downstreamvideo signals was improved, due to the sharpercontrast between erythrocytes and plasma.
The use of fluorescent 7-globulin made it possibleto measure the capillary diameter at the same site atwhich V ^ was measured. Previous methods in-volved measurement by microscopic ocular of thesame vessel (Bottcher and Steinhausen, 1976) ordetermination from photographs of a separate groupof vasa recta (Marsh and Segel, 1971).
Two limitations to this method of determiningcapillary diameters persist. First, the image qualityor sharpness of the contrast between the plasmaand the capillary wall decreases with time. At pres-ent, this restricts measurements to a period 30-60minutes after infusion of the FITC-labeled 7-glob-ulin. The second limitation is the assumption thatvasa recta in vivo have circular cross-sections (seeAppendix I). Capillary diameters determined fromour videotapes necessarily are those of an imagethrough a single plane. If the elongate or roughlyelliptical configuration of vasa recta suggested inFigure 3 and elsewhere (Jamison and Kriz, 1982) isverified by a morphological study, then true capil-lary cross-sectional areas, especially of the moreelongate AVR, are overestimated using the formula,A = irD2/4. We calculated that the single vesselflows would be reduced in DVR by 9.5%, from 8.8to 8.0 nl/min, and in AVR by 15.8%, from 4.8 to4.1 nl/min (see Eq. 1 and Appendix I). These num-bers should be considered preliminary, subject tocorrection later on the basis of a more extensivemorphological study.
Ratio of Vrt«:Vblood, F
Despite several attempts to define the ratio be-tween red cell velocity, V^ , and mean cross-sec-tional blood velocity, V ^ ^ (Barbee and Cokelet,1971; Gaehtgens et al., 1976), F remains ill-definedfor the composite range of diameter, microvesselhematocrit, and blood velocity encountered in vasarecta. For that reason, we determined F for this rangein in vitro experiments.
The in vitro experiments, which represent, to ourknowledge, the first attempt to estimate F for capil-laries in the 15-25 fim diameter range, had severallimitations. First, we used quartz capillaries, notmammalian capillaries. However, Fenton et al.(19821), in experiments in which monolayers of hu-man endothelial cells were grown over the innersurface of glass tubes, demonstrated that (comparedwith unlined tubes) the presence of an endotheliallining had no effect on the flow of either plasma orred cells suspended in plasma. Second, we usedplatelet-free EDTA-treated human blood, not ratwhole blood. Under normal conditions, however,
platelets or EDTA are unlikely to affect F in flowingblood, and human red cells are nearly the same sizeas rat red cells. Third, we used isotonic, not hyper-tonic fluid; whether hypertonicity might have stiff-ened red cells and possibly reduced F remains spec-ulative. Fourth, there was considerable scatter insome individual determinations, as can be seen byinspecting Table 2. Nevertheless, the individual de-terminations do not exceed the theoretical limits of1 < F < 2 (actual range, 0.94 < F < 1.96), andrepresent a normal distribution about the mean of1.4. Moreover, we were able to encompass the rangeof values of capillary diameter (13-56 fim), eryth-rocyte velocity (0.18 to 2.05 mm/sec), and hemato-crit (6-21%) known for vasa recta in vivo. Thevalues obtained for V^iV^cd in 25 experiments (Fig.6; Table 2) suggest that 1.4 is a reasonable estimatein this range of values for these variables, but, forany experiment considered separately, this ratio mayvary from 0.7 to 1.41 times the mean value given.As mentioned above, an important point is that thisvalue of F is a calibrating parameter that permitsmeasurements made, using our video microscopytechniques, to be converted into estimates of capil-lary blood flow; i.e., this value of F is specific forthese techniques and may not be applicable to ex-periments employing other means to determine V^ .
AVR:DVR Ratio
The principal assumption in determining the ratioof AVR to DVR is that ultrastructural differences ofcapillary endothelia correspond to differences indirection of blood flow. Only two types of bloodvessels exist in the medulla (Kriz et al., 1976;Schwartz et al., 1976): one type has a relatively thickcontinuous nonfenestrated endothelium, whereasthe other possesses a thin attenuated endotheliumwith numerous fenestrae (Schwartz et al., 1976).Schwartz et al. (1976) were able to distinguish AVRfrom DVR by partial injection of carbon, or bytracing individual vasa recta from their origins. Theendothelium of DVR was found to be continuous,whereas AVR had fenestrated endothelium like theperirubular capillaries of the renal cortex.
We considered the possibility that some vesselscounted as AVR were actually "communicating" cap-illaries between AVR and DVR. Determination ofdirection of blood flow in 148 capillaries from 60Mm-wide strips of the papillary surface on the videomonitor revealed only four vessels that were notunambiguously ascending or descending. Assumingthe papillary surface is representative of the under-lying papilla, the number of connecting capillariesin a histological section 12 times thinner (<5 nm)probably can be neglected. This neglect does notmean that the medulla contains no communicatingcapillaries—only that, in a section less than 5-^mthick, their frequency is probably very low. In fact,Jamison and Kriz (1982) have suggested that AVRoriginate very near DVR, without a large intervening
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

410
segment of connecting capillaries.From 200 capillaries on the surface of the exposed
rat papilla in vivo, Bottcher and Steinhausen (1976)determined the ratio of AVR to DVR to be 2.2, lowerthan the ratio of 4 in the present study. Aside fromdifferences in methods employed, the main differ-ence between their study and ours is that theydetermined the ratio 0.5 mm from the tip of thepapilla, while we determined the ratio 2 mm fromthe tip. In light of the implication that the ratio ofAVR to DVR approaches unity toward the tip of thepapilla (Jamison and Kriz, 1982), the difference be-tween our results and theirs is perhaps not surpris-ing.
Total Papillary Tip Blood FlowTotal blood flow was calculated by multiplying
Qvr by the number of AVR or DVR. Two implicitassumptions are that Qvr was determined exactly 2mm from the tip of the papilla in every vessel, andthat the number of AVR and DVR 2 mm from thetip of the papilla is reasonably constant. A definitivetest of the latter assumption awaits a systematicstudy of the number of AVR and DVR in a largerseries of animals.
Taking the physiological variability and the tech-nical limitations together, we estimated the possiblerange of these determinations for single vessel flowand total blood flow. Based on confidence limits of95.4% (given by mean ± 2 SE) for each contributingparameter, we obtain a worst case range for singlevessel flows in DVR of 5.6-12.4 nl/min and in AVRof 3.6-6.8 nl/min. The true variability of numbersof AVR and DVR 2 mm from the tip of the papillais difficult to estimate; if the whole range of actualnumbers determined is used, the number of DVRranged from 0.71 to 1.46 of the mean value, and thenumber of AVR ranged from 0.73 to 1.31 of themean value. Combining these limits with those forsingle vessel flow yields the following worst casebounds; for inflow, 2.4-10.7 jtl/min; for outflow,6.2-20.9 /il/min. Corrected for the weight of theexposed papillary tip, these values convert to 1.3-5.9 ml/min per g tissue weight inflow and 3.4-11.6ml/min per g tissue weight outflow.
Comparison with Other Measurements ofPapillary Blood Flow
Plasma flow entering the renal papilla determinedby the Lilienfield 131I-labeled albumin-accumulationtechnique (Lilienfield et al., 1961) ranges from 0.29to 0.38 ml/min per g tissue weight (Solez et al.,1974; Chuang et al., 1978; Buerkert et al., 1981), or,in terms of blood flow, 0.39-0.51 ml/min per gtissue weight, assuming a capillary hematocrit of25%. This is lower than our estimated lower boundof 1.3 ml/min per g tissue weight. The recent mod-ification of the albumin-accumulation technique(Rasmussen, 1978) also yields values lower thanours, 0.44-0.72 ml/min per g tissue weight.
Circulation Research/Vo/. 53, No. 3, September 1983
As Chuang et al. (1978) have noted, exposure ofthe papilla may increase blood inflow by as muchas 40%. Using this figure to adjust for papillaryexposure, our values would correspond to 0.8-3.5ml/min per g tissue weight with the ureter intact.Blood flow per gram of tissue to the extrarenalpapilla may be greater than to the papilla as a whole,because it is more vascular than the rest of thepapilla (Knepper et al., 1977).
Since the Lilienfield technique requires severalassumptions that may be incorrect (Aukland, 1976;Rasmussen, 1978; Jamison and Kriz, 1982), a fun-damentally different method for measuring papil-lary blood flow is useful. The concentration profileof I-labeled albumin in the plasma entering vasarecta is assumed to be the same as that in systemicplasma, whereas a more plausible assumption is thatthe radioactivity profile of plasma by the time itarrives at the papilla is considerably dispersed com-pared with the radioactivity profile in systemicplasma. The technique assumes no loss of labeledalbumin from the papilla during the accumulationperiod. Within an accumulation time even as shortas 10 seconds, however, labeled albumin may al-ready begin to be carried out by AVR, judging fromthe time course of disappearance of lissamine greenfrom the papilla (unpublished observations). In viewof these considerations, the Lilienfield techniquemay underestimate true plasma flow to the papilla.A more rigorous comparison of values obtained byour method with those obtained by the Lilienfieldmethod must await the performance of experimentsin which both techniques are used simultaneously.
Values obtained for inner medullary and papillaryblood flow rate by other methods, such as the dyedilution technique and diffusive isotopes [summa-rized by Thurau and Levine (1971) and Jamison andKriz (1982)], are also lower than the flow ratesreported herein. Recently, however, using an isotopeof rubidium, Hermansson and Wolgast found valuesreasonably close to our inflow values (Wolgast, per-sonal communication). The findings of Meier et al.(1964) are of particular interest. They determinedmedullary blood flow by inserting the photoelectri-cal cells directly into the renal medulla of anesthe-tized dogs. Average plasma velocity was 2 mm/sec.On the basis of differences between transit timesdetermined by diffuse illumination of the medullaand that determined by local illumination, Meier etal. concluded that the velocity of blood in AVR islower than that of DVR, that the blood volume ofAVR is 1.7 times that of DVR, and that the higherAVR volume reflects net fluid uptake.
Our findings indicate that the rate of blood flowto the exposed papilla is about 2.9 ml/min per gtissue weight (DVR) (range 1.3-5.9), whereas out-flow in AVR is about 6.2 ml/min per g tissue weight(range 3.4-11.6). Thus, the estimated capacity forwater uptake of 3.3 ml/min per g tissue weight(range 2.1-5.7) is adequate to account for the re-
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

Holliger et al. /Direct Determination of Blood Flow in Vasa Recta 411
moval of water reabsorbed from the papillary col-lecting duct (1.5-2.6 ml/min per g) (Oliver et al.,1982).
Appendix I
Cross-sectional Area of Vasa Recta
Introduction
To convert mean cross-sectional blood velocity, Vtnooi,to single vasa recta blood flow, Q^, we need to determinethe cross-sectional area, A, of the vas rectum. True vasarecta diameter, D, often exceeds the diameter of the redblood cell column because of the existence of a peripherallayer of cell-free plasma (Holliger et al., in press). Theinterface between cell-free plasma and capillary endothe-lium is not visible by ordinary video microscopy. There-fore, our intention was to enhance the contrast betweenplasma and the capillary endothelium/interstitial back-ground. Fluorescein isothiocyanate (FITC)-labeled high-molecular-weight dextrans have been used previously asa plasma marker. Intravenous FTTC-dextran administra-tion, however, caused acute hypotension and edema. Wetried FITC-labeled bovine serum albumin (66,000 daltons).Unexpectedly, the FITC-albumin seemed to extravasateinto the interstitium within about 15 minutes. To avoidextravasation, we next used bovine 7-globulin (150,000daltons). The plasma contrast enhancement achieved wasstable over the measurement period, and intravenous ad-ministration was not associated with visible edema or witha change in systemic blood pressure (105 ± 3 mm Hgbefore, vs. 106 ± 4 mm Hg 15-20 minutes after).
Preparation of FITC-Labeled y-Globulin
Sixty milligrams of bovine 7-globulin (Cohn FractionII, Sigma Chemical Company) were dissolved in 5 ml ofcarbonate-buffered saline at pH 9.9 (Rasmussen, 1978).After the protein dissolved, 40 mg of 10% fluoresceinisothiocyanate (FITC) on celite (Sigma) were added andswirled gently. After 2 hours of reaction at room temper-ature, the solution was centrifuged at 5000 rpm for 10minutes to remove the celite. The supernatant was passedthrough a 23-cm Bio-Gel P-4 (Bio-Rad Laboratories) col-umn to remove free, unreacted FITC. The elution fluid forthe column was phosphate-buffered saline (0.1 M, 0.85%at pH 7.4). The labeled 7-globulin (approximately 1%solution) was collected and stored at 4°C. An aliquot ofthe solution (0.5-1 ml) was warmed to room temperatureand injected intravenously 30-60 minutes before velocityand capillary diameter determinations.
Measurement of Vasa Recta Diameter, D
Vessel dimension (Vs) were determined directly fromthe frozen-frame capillary image on the television moni-tor. Owing to the inhomogeneity inherent in video sys-tems, the measurements were converted to absolute cap-illary dimensions in terms of local magnification. Themonitor was partitioned into 20 regions in which localhorizontal and vertical magnifications were establishedwith a Leitz stage micrometer. The accuracy and reprod-ucibility of measurements of vessel diameters were inves-tigated using FITC-filled quartz capillaries. Diameters de-termined with a scanning electron microscope were thestandard with which the video measurements were com-pared. Table 4 summarizes the results, where the standard
deviation of the much more accurate SEM method docu-ments the variability of inner diameters along the testcapillary; mean values from the video system agreed withthe electron microscope values to within 3%.
As shown in Figure 3, vasa recta may be more accuratelyregarded as elliptical in cross-section. [Please see also, forexample, Figure 16-3, p. 238, in Jamison and Kriz (1982).]Therefore, capillary dimensions measured using the videomonitor are not necessarily the diameters of circular vasarecta.
Assuming a uniform distribution of ellipse orientations,an average capillary cross-sectional area A for the purposeof blood flow calculations can be computed according tothe formula j :
A'-
• \ir Vl + (/32 - l)sin20 d0(2)
where A' is the apparent cross-sectional area as deter-mined by video microscopy (A' = irD2/4), /S is the ellipseaspect ratio (ratio of major axis length to minor axislength), N is a normalized AVR- or DVR-specific distribu-tion function for /3, and 6 is an angle that is zero when Dequals the minor axis length, and is 90° when D equalsthe major axis length.
The elliptical model itself is a simplification of the actualshapes of the vasa recta cross-sections suggested by Figure3. Its main advantage lies in the fact that it can accomodatea continuum of vessel shapes without becoming mathe-matically intractable. Still unresolved is the question ofwhether or not the noncircular shapes of the vasa rectacross-sections in the electron micrographs are artifacts orreflect the true state of affairs in vivo. We know of no apriori reason that the vasa recta should be cylindricaltubes, although it is conceivable that DVR—with theirthicker endothelium—may tend to be more nearly cylin-drical than AVR.
It is unlikely that the angle of sectioning of the papillacould account for the eccentric shapes of vasa recta cross-sections. The chance of fixation artifact is more trouble-some, and will require further morphological studies. Be-cause of the possibility that vasa recta are elliptical, ratherthan circular, the 'corrected" values for blood flow givenbelow represent possible lower bounds set by this uncer-tainty.
Aspect ratios were determined for AVR and DVR fromelectron micrographs of two papillas. Ellipses were hand-drawn to approximate capillary cross-sections for all thosevasa recta which lay entirely within electron microscopegrids in which no fixation distortion was evident. Themajor and minor axes then were measured, and /? calcu-lated as their ratio. A total of 143 AVR and 63 DVR wereanalyzed. The median value for jS in the AVR was 1.9;that in the DVR was 1.6. Replacing the continuous distri-bution of /3 in Equation 2 by a discrete, step-functiondistribution, the following "corrected" values were ob-tained: single vasa recta blood flow in AVR is 4.06 nl/min (compared to 4.82 nl/min), in DVR 7.99 nl/min(compared to 8.83 nl/min). Total blood flow into theexposed papilla in DVR is 4.7 jjl/min (compared to 5.2Ml/min), and from the exposed papilla in AVR 9.6 /xl/min(compared to 11.3 /il/min); the difference (which is a
t The authors will provide a complete derivation of Equation 2,upon request.
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

412 Circulation Research/Vo/. 53, No. 3, September 1983
revised estimate of water uptake by the vasa recta) is 4.9jtl/min (compared to 6.1 ^1/min).
We are grateful to Kristina Blouch and Jim Knapp for technicalassistance and Ditter Peschcke-Kocdt for secretarial assistance.
This research was supported by National Institutes of HealthGrants 5-RO1-AM 18077, 2-R01-AM 18910, and 5-T32-AM 07357,by American Heart Association Grant-in-Aid 81 712, and by grantsfrom Mr. George Kwong, Dr. and Mrs. Rachford Harris, and Merckand Co., Inc.
This work was presented in preliminary form to the AmericanPhysiological Society April 22, 1982, and appears in abstract form inFed. Proc. 41: x 1982.
Dr. Holliger's present address is: Hohere Techmsche Lehranstalt,CH-5200 Brugg, Switzerland.
Dr. Schmitt's present address is: Standard Oil of Indiana, 200 EastRandolph Drive, Chicago, Illinois 60601.
Address for reprints: Dr. R.L. Jamison, Division of Nephrology,Stanford University School of Medicine, Stanford, California 94305.
Received March 3, 1983; accepted for publication July 13, 1983.
ReferencesAukland K (1976) Renal blood flow. In Kidney and Urinary Tract
Physiology, II, volume 11, edited by K. Thurau. Baltimore,University Park Press, pp 23-79
Barbee JH, Cokelet GR (1971) The Fahraeus effect. Microvasc Res3: 6-16
Bartilana CA, Dobyan DC, Lacy FB, Bhattacharya J, Johnston PA,Jamison RL (1978) Effect of chronic potassium loading onpotassium secretion by the pars recta or descending limb of thejuxtamedullary nephron in the rat. J Clin Invest 62; 1093-1103
Berliner RW, Levinsky NG, Davidson DG, Eden M (1958) Dilutionand concentration of the urine and the action of antidiuretichormone. Am J Med 24: 730-744
Bottcher W, Steinhausen M (1976) Microcirculation of the renalpapilla under control conditions and after temporary ischemia.Kidney Int 10: S76-S80
Buerkert J, Martin D, Prasad J, Trigg D (1981) Role of deepnephrons and the terminal collecting duct in a mannitol-in-duced diuresis Am J Physiol 240: F411-F422
Chuang EL, Reineck HJ, Osgood RW, Kunau RT, Jr, Stein JH(1978) Studies on the mechanism of reduced urinary osmolalityafter exposure of the renal papilla. Clin Invest 61: 633-639
De Lano FA, Zweifach BW (1981). Anesthesia and microvasculardynamics in spontaneously hypertensive rats. Am J Physiol241: H821-H828
Fahraeus R (1928) Die Stromungsverhaltnisse und die Verteilungder Blutzellen im Gefassystem. Klin Wochenschr 7: 100-106
Fenton BM, Cokelet GR, LaCelle PL (1982) Influence of wallsurface on the flow of blood through endothelial-lined glasstubes. Int J Microcirc Clin Exp 1: 157-162
Gaehtgens P, Benner KU, Schickendantz S, Albrecht KH (1976)Method for simultaneous determination of red cell and plasmaflow velocity in vitro and in vivo. PfluegeTS Arch 361: 191-195
Ganguli M, Tobian L, (1974) Does the kidney autoregulate pap-illary plasma flow in chronic 'post-salt" hypertension? Am JPhysiol 226: 330-333
Gottschalk CW (1961) Osmotic concentration and dilution of theurine. Am J Med 36: 670-685
Gottschalk CW, Lassiter WE, Mylle M (1962) Studies of thecomposition of vasa recta plasma in the hamster kidney. Ex-cerpta Med 47: 375-376
Gussis GL, Jamison RL, Robertson CR (1979a) Determination oferythrocyte velocities in the mammalian inner renal medullaby a video velocity-tracking system. Microvasc Res 18: 370-383
Gussis GL, Robertson CR, Jamison RL (1979b) Erythrocyte veloc-ity in vasa recta. Effect of antidiuretic hormone and salineloading. Am J Physiol 237: F326-F332
Holliger C, Anliker M, Klingler D, Bollinger A (1975) Evaluationof an on-bne videodensitimetric measurement of the RBCvelocity in the capillaries of the human nailfold. Biomed Eng20: 187-192
Holliger C, Radzyner M, Knoblauch M, (in press) Effects ofglucagon, VIP and vasopressin on villous microarculation andsuperior mesenteric artery blood flow of the rat. Gastroenter-ology
Intaglietta M, Silverman NR, Tompkins WR (1975) Capillary flowvelocity measurements in vivo and in situ by television meth-ods. Microvasc Res 10: 165-179
Jamison RL (1970) Micropuncture study of superficial and juxta-medullary nephrons in the rat. Am J Physiol 218: 46-55
Jamison RL, Kriz W (1982) Urinary Concentrating Mechanism:Structure and Function. New York, Oxford University Press,pp 233-242
Jamison RL, Buerkert J, Lacy FB (1971) A micropuncture study ofcollecting tubule function in rats with hereditary diabetes msi-pidus. J Clin Invest 50: 2444-2452
Jamison RL, Buerkert J, Lacy FB (1973) A micropuncture study ofHenle's thin loop in Brattleboro rats. Am J Physiol 224: 180-185
Knepper MA, Danielson RA, Saidel GM, Post RS (1977) Quanti-tative analysis of renal medullary anatomy in rats and rabbits.Kidney Int 12: 313-323
Kriz W, Barrett JM, Peter S (1976) The renal vasculature: Anatom-ical-functional aspects. In Kidney and Urinary Tract Physiol-ogy, II, volume 11, edited by K Thurau. Baltimore, UniversityPark Press, pp 1-21
Lilienfield LS, Maganzini HC, Bauer MH (1961) Blood flow inthe renal medulla. Circ Res 9: 614-617
Marsh DJ, Segel LA (1971) Analysis of countercurrent diffusionexchange in blood vessels of the renal medulla. Am J Physiol221:817-828
Meier M, Brechtelsbauer H, Kramer K (1964) Hamodynamik desNierenmarks. IV. Mitteilung Fabstoffvrdnnungskurven in ver-schiedenen Abschnitten des Nierenmarks. Pfluegers Arch 279:294-304
Moffat DB (1969) Extravascular protein in the renal medulla. JExp Physiol 54: 60-67
Oliver RE, Roy DR, Jamison RL (1982) Urinary concentration inthe papillary collecting duct of the rat. Role of the ureter. J ClinInvest 69: 157-164
Ploem JS (1967) The use of a vertical illuminator with inter-changeable dichroic mirrors for fluorescence microscopy withincident light. Mikrosk Technik 68: 129-142
Rasmussen SN (1978) Red cell and plasma volume flows to theinner medulla of the right kidney. Pfluegers Arch 373: 153-159
Sanjana V, Johnston PA, Troy JL, Deen WM, Robertson CR,Brenner BM, Jamison RL (1975) Hydraulic and oncotic pressuremeasurements in the mammalian kidney Am J Physiol 228:1921-1926
Sanjana VM, Johnston PA, Robertson CR, Jamison RL (1976) Anexamination of the transcapillary water flux in the renal innermedulla. Am J Physiol 231: 313-318
Schmidt-Nielsen B (1977) Excretion in mammals: Role of therenal pelvis in the modification of the urinary concentrationand composition. Fed Proc 36: 2493-2503
Scholander PF (1957) The wonderful net. Sci Am 1%: 96-107Schwartz MM, Kamovsky MA, Venkatachalam MA (1976) Ultra-
stnictural differences between rat inner medullary descendingand ascending vasa recta. Lab Invest 35: 161-170
Snedecor GW (1966) Statistical Methods. Ames, Iowa, Iowa StateUniversity Press, pp 35-64
Solez K, Kramer EC, Fox JA, Heptinstall RH (1974) Medullaryplasma flow and intravascular leukocyte accumulation in acuterenal failure. Kidney Int 6: 24-37
Thurau K, Levine DZ (1971) The renal circulation. In The Kidney.Morphology, Biochemistry, Physiology, edited by C Rouiller,AF Muller. New York, Academic Press, pp 1-70
Tompkins WR, Monti R, Intaglietta M (1974) Velocity measure-ment of self-tracking correlator. Rev Sci Instrum 45: 647-649
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

Holliger et al. /Direct Determination of Blood Flow in Vasa Recta 413
Ullrich KJ, Pehling G, Stockle W (1961) Hamoglobinkonzentra- peritubular capillary permeability using protein tracers. Labtion, Erythrocytenzahl und Hamatokrit im Vasa Recta Blut. Invest 27: 435-444Pfluegers Arch 273: 573-578 Wolgast M (1973) Renal medullary red cell and plasma How as
Ullrich KJ, Kramer K, BoylanJW (1962) Present knowledge of the studied with labelled indicators and internal detection. Actacountercurrent system in the mammalian kidney. In Heart, Physiol Scand 88: 215-225Kidney and Electrolytes, edited by CK Friedberg. New York,Grune & Stratton, pp 1-37 INDEX TERMS: Vas recta blood flow • Renal medulla • Papilla
Venkatachalam MA, Karnovsky MJ (1972) Extravascular protein • Fluorescence video microscopyin the kidney. An ultrasrructural study of its relation to renal
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from

C Holliger, K V Lemley, S L Schmitt, F C Thomas, C R Robertson and R L JamisonDirect determination of vasa recta blood flow in the rat renal papilla.
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1983 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.53.3.4011983;53:401-413Circ Res.
http://circres.ahajournals.org/content/53/3/401World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on April 5, 2018
http://circres.ahajournals.org/D
ownloaded from
Related Documents