Digital Hospitals Move Off the Drawing Board Prepared for: CALIFORNIA HE A LT HCARE FOUNDATION Prepared by: First Consulting Group Authors: Erica Drazen and Jason Fortin October 2003

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Digital Hospitals MoveOff the Drawing Board
Pre p a red for:CA L I F O R N I A HE A LT HCA R E FO U N D AT I O N
Pre p a red by :First Consulting Gro u p
Au t h o r s :Erica Dr a zen and Jason Fo rt i n
October 2003

A c k n o w l e d g m e n t sThe authors would like to thank Dr. Tom Lee of the CaliforniaHe a l t h C a re Foundation for his valuable direction. This re p o rtwould not have been possible without the help of the ve n d o r s ,hospitals, and visionary leaders who shared their time and theirexperience.
About the AuthorsFirst Consulting Gro u p p rovides consulting, technology, ando u t s o u rcing services for health care, pharmaceutical, and otherlife sciences organizations in No rth America and Eu rope. Mo re information about FCG is available at: w w w. f c g . c o m.
About the FoundationThe Ca l i f o rnia He a l t h Ca re Fo u n d a t i o n, based in Oakland, is an independent philanthropy committed to improv i n gC a l i f o r n i a’s health care delive ry and financing systems. Formed in 19 9 6, our goal is to ensure that all Californians haveaccess to affordable, quality health care.
The iHealth Re p o rts series focuses on emerging technologyt rends and applications and related policy and re g u l a t o ry d e ve l o p m e n t s .
Additional copies of this re p o rt and other publications can beobtained by visiting us online at w w w. c h c f . o r g.
ISBN 1-9 3 2 0 6 4- 5 0-8Copyright © 2003 California He a l t h C a re Fo u n d a t i o n
C o n t e n t s
4 I. I n t r o d u c t i o nP u r p o s e
7 II. The State of Digital HospitalsDefinition of Digital Hospital
Goals of Making the Digital Tr a n s f o r m a t i o n
Approaches to Making the Digital Tr a n s f o r m a t i o n
16 I I I . Common Themes and Lessons LearnedThe Need for Strong Leadership
Explore the Possibilities
The Importance of Tr a i n i n g
The Value of Vendor Partnerships
The Value of User Partnerships
19 I V. Future of the Digital HospitalE x p e c t a t i o n s
The Bottom Line
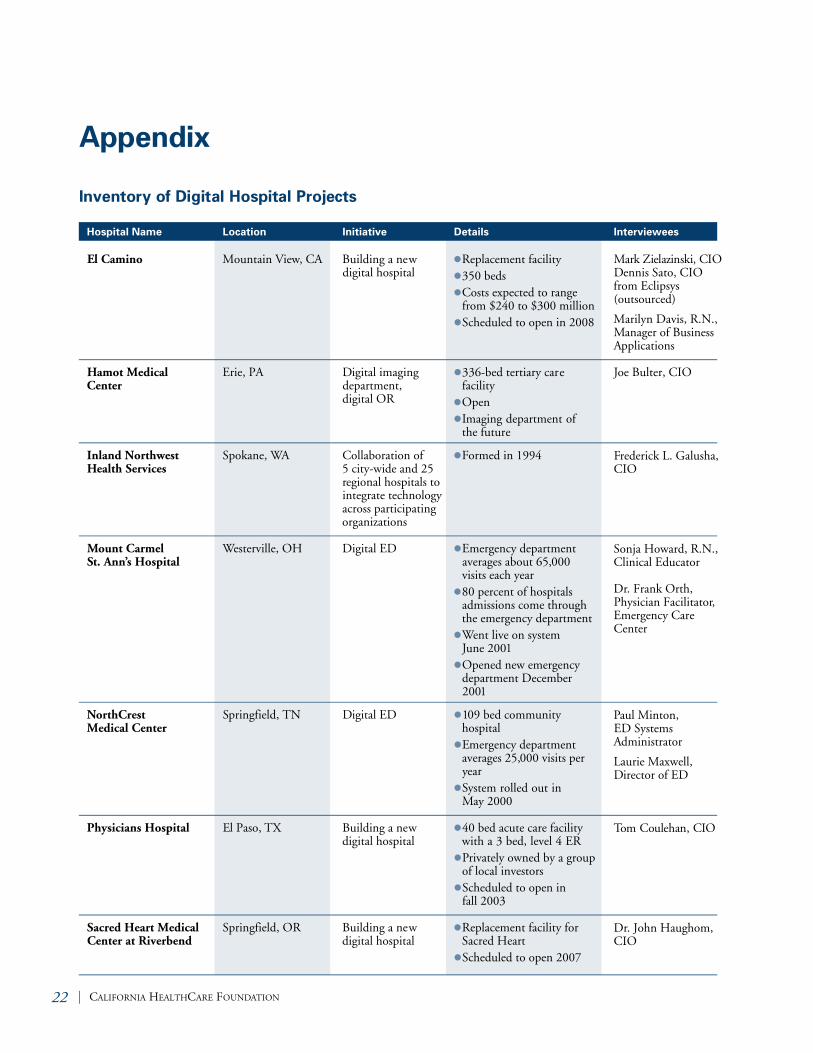
21 Appendix Inventory of Digital Hospital Projects
2 4 E n d n o t e s

4 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
TH E S E A R E C H A L L E N G I N G T I M E S F O R T H Ehospital industry. Ac ross the country, institutions that providemedical and surgical care are facing new pressures on multi-ple fronts. In one particularly vivid example, a 1999 Instituteof Medicine study reported that 98,000 people die in U.S.hospitals each year from preventable medical errors, fueling a justifiable demand from employers, payers, and patients forimproved quality.
Hospital capacity is constrained. In 2001, two thirds of hospi-tals we re forced to dive rt ambulances at some point during theye a r, and one in ten re p o rted dive rting emergency cases 20 p e rcent of the time.1 Fu rt h e r, to meet increasing demand fro mthe elderly population, at least 238,000 new hospital beds willbe needed by 2027.2 With this growing demand, U.S. hospitalsalso have a critical shortage of staff; 90 percent have a short a g eof nurses3 and 15 percent of imaging technician positions inhospitals are va c a n t .4 Declining reimbursements are also a reality at both the federal and state leve l .5
The Institute of Medicine has emphasized that advances intechnology will be vital to “c rossing the quality chasm.”6 Ag rowing number of hospitals are incorporating informationtechnology in the construction and design of new facilities to increase efficiency and ensure that care is provided in a c c o rdance with best practices. Perhaps inevitably, these havecome to be known as digital hospitals.
P u r p o s eThis re p o rt provides an ove rv i ew of digital hospitals in theUnited States. The scope of re s e a rch includes both new digitalhospitals and hospitals that are transforming specific pro c e s s e sor departments using an innova t i ve technological appro a c h .Emphasis has been placed on documenting the results of exist-ing efforts and capturing the lessons that have been learned inplanning and implementation.
I. Introduction
First Consulting Group was retained by theCalifornia He a l t h C a re Foundation to explore ,t h rough interv i ews and site visits, the va r i o u se f f o rts to build the digital hospital. Because ofthe limited number of digital hospitals in opera-tion, the scope of the study was expanded toinclude hospitals that had transformed depart-ments, such as the operating room (OR), theemergency department (ED), and the intensivec a re unit (ICU).
Hospitals currently under construction we reincluded in the re s e a rch to help validate any con-clusions and gain some perspective into what thef u t u re might hold.
When looking for potential sites, the authorsfocused on those that are using technology totransform care as outlined by the ten goals in thesecond Institute of Medicine re p o rt, “Cro s s i n gthe Quality Chasm,” paraphrased below.
■ Patients should re c e i ve care whenever theyneed it and in many forms, not just face-to-face visits.
■ The system of care should have the capabilityto respond to individual patient choices andp re f e re n c e s .
■ Patients should be given the information theyneed to exe rcise control over decisions thataffect them, and the health system should beable to accommodate differences in patientp re f e re n c e s .
■ Patients should have unfettered access to theirown medical information and to clinicalk n owledge; clinicians and patients should alsobe able to communicate effectively and sharei n f o r m a t i o n .
■ Patients should re c e i ve care based on the besta vailable scientific knowledge. Care should notva ry illogically from clinician to clinician orf rom place to place.
■ The health care system should reduce risk ande n s u re safety by paying greater attention tosystems that help pre vent and mitigate erro r s .
■ The health care system should make informa-tion available to patients and to their familiesthat allows them to make informed decisionswhen selecting a health plan, hospital, or clini-cal practice, or choosing among alternativet re a t m e n t s .
■ The health system should anticipate patientneeds, rather than simply reacting to eve n t s .
■ The health system should not waste re s o u rc e sor patient time.
■ Clinicians and institutions should actively collaborate and communicate to ensure anda p p ropriate exchange of information andc o o rdination of care .7
The 13 sites that best addressed those goals we reasked to participate. Two of these sites,Oklahoma He a rt Hospital and Indiana He a rtHospital, did not participate in the study.
Be t ween one and four key staff members familiarwith the design and operation of the facility we rei n t e rv i ewed by telephone. In t e rv i ewees includedchief information officers, project managers,d e p a rtment leaders, and end users. Di s c u s s i o nfocused on:
■ Goals of the hospital
■ Ap p roaches to integrating technology into theo r g a n i z a t i o n
■ Lessons learned
■ Results achieve d
Site visits we re then arranged with three of thehospitals to gain a deeper understanding of thedetails around digital hospital planning and operation. Visits included an extensive tour andi n t e rv i ews with the project leaders, hospital exe c-u t i ves, physicians, and nurses who have beend i rectly affected by the effort .
Digital Hospitals Move Off the Drawing Board | 5
6 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
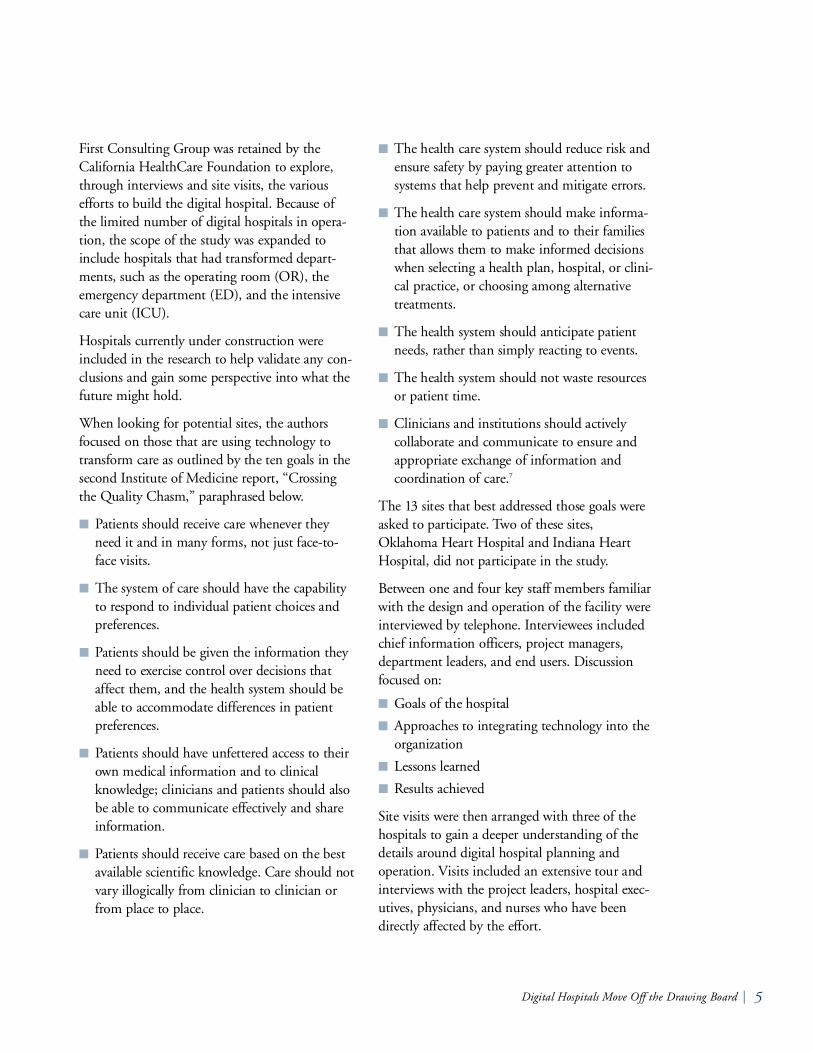
Table 1. Lists of Participating Hospitals
New Hospitals
Hospital Name
El Camino
Physicians Hospital
Sacret Heart Medical Center at Riverbend
Existing Hospitals
Inland Northwest Health Services
St. Vincent’s Hospital
Digital Departments
Hamot Medical Center
Mount Carmel St. Ann’s Hospital
NorthCrest Medical Center
Sentara Norfolk General Hospital
University of Pittsburgh Medical Center
Washington Hospital Center
The following table lists the hospitals that are included in this re p o rt .
Location
Moutain View, CA
El Paso, TX
Springfield, OR
Spokane, WA
Birmingham, AL
Erie, PA
Westerville, OH
Springfield, TN
Norfolk, VA
Pittsburgh, PA
Washington, DC
Project
Replacement facility
New facility
Replacement facility
Collaboration of 5 citywide and 25 regional hospitals to integratetechnology across p a rticipating organizations
Integrating a variety oftechnologies across theorganization
Digital imaging departmentDigital OR
Digital ED
Digital ED
Digital ORDigital ICU
Digital OR
Digital ED
Status
Scheduled to open in 2008
Scheduled to open fall 2003
Scheduled to open in 2007
All hospitals are open
Open
Open
Open
Open
Open
Open
Open
Digital Hospitals Move Off the Drawing Board | 7
Definition of Digital HospitalAlthough the concept of the digital hospital has begun appear-ing in the pre s s ,8,9,10 no accepted definition exists within thei n d u s t ry. T h e re f o re, for the purposes of this re p o rt, the termdigital hospital is defined as: An acute care facility incorpora t i n gthe widespread use of information technology to dra m a t i c a l l yi m p rove the processes and outcomes of care .
Current LandscapeT h e re are 5,8 01 re g i s t e red hospitals in the United St a t e s ,11 a n dmany replacement and new hospitals are under construction tomeet future demand.
The most-publicized digital hospitals are new specialty hospitals—especially the 88-bed Indiana He a rt Hospital inIndianapolis, Indiana; the 80-bed Oklahoma He a rt Hospital in Oklahoma City, Oklahoma; and the planned He a l t h So u t hfacility in Birmingham, Alabama. Smaller acute care digitalhospitals are nearing completion, with Physicians Hospital, a 40-bed facility in El Paso, Texas set to open its doors in fall 2003. The large replacement hospitals at Pe a c e Health in Sp r i n gfield, Oregon and El Camino in Mountain Vi ew,California are not scheduled to open for three or four m o re ye a r s .
With 153 new acute care or specialty hospitals under con-struction now, and 223 in the planning stages,12 it seems likelymany more announcements of new digital hospitals will beforthcoming in the near future.
T h e re are also a growing number of institutions that are trans-forming critical hospital areas. Re s e a rch is being funded onh ow to do it well—for example, in May 2003, a total of 10hospital systems we re selected by the Ro b e rt Wood Jo h n s o nFoundation to participate in a $4.6 million redesign of emer-gency depart m e n t s .13 Fewer institutions that are gradually inte-grating technology across the organization we re identified, butthis may be because these approaches are less publicized ratherthan less pre va l e n t .
II. The State of Digital Hospitals
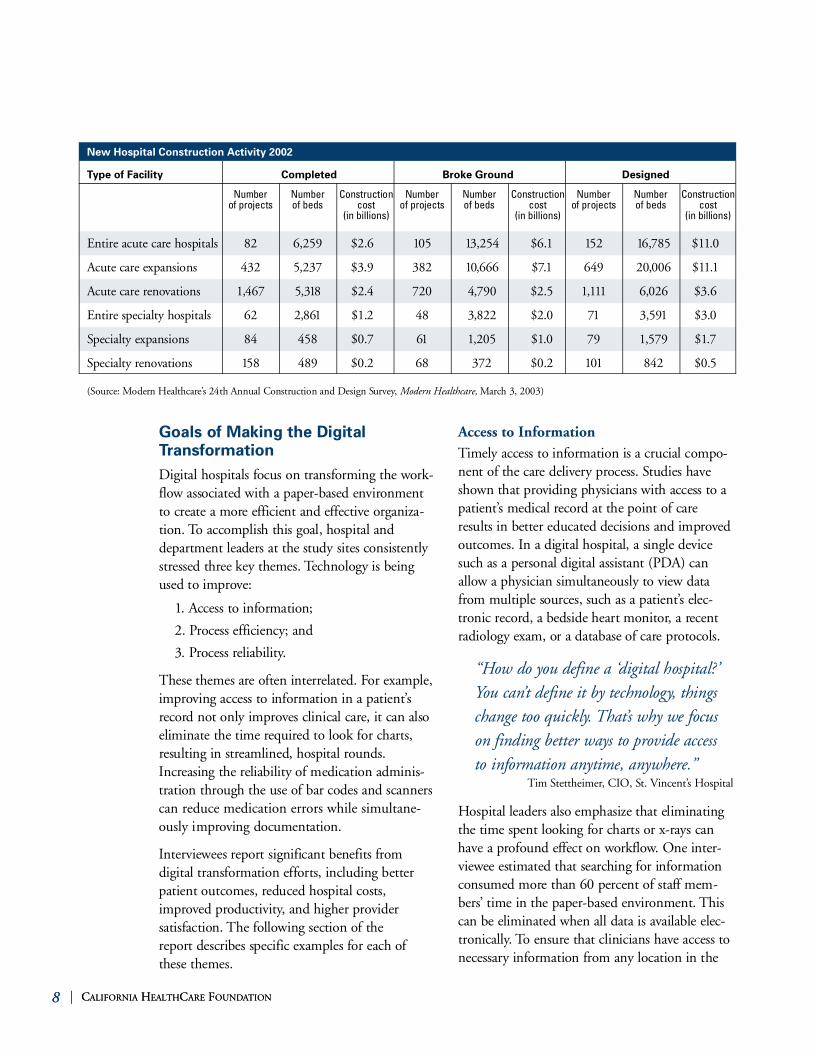
New Hospital Construction Activity 2002
Type of Facility Completed Broke Ground Designed
En t i re acute care hospitals 8 2 6, 2 5 9 $ 2.6 10 5 13, 2 5 4 $ 6.1 15 2 16,7 8 5 $ 11.0
Acute care expansions 4 3 2 5, 2 3 7 $ 3.9 3 8 2 10,6 6 6 $ 7.1 6 4 9 2 0,0 0 6 $ 11.1
Acute care re n ova t i o n s 1,4 6 7 5, 318 $ 2.4 7 2 0 4,7 9 0 $ 2.5 1,111 6,0 2 6 $ 3.6
En t i re specialty hospitals 6 2 2,8 61 $ 1.2 4 8 3,8 2 2 $ 2.0 71 3,5 91 $ 3.0
Specialty expansions 8 4 4 5 8 $ 0 .7 61 1, 2 0 5 $ 1.0 7 9 1,5 7 9 $ 1.7
Specialty re n ova t i o n s 15 8 4 8 9 $ 0 .2 6 8 3 7 2 $ 0 .2 101 8 4 2 $ 0 .5
8 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N8 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Goals of Making the DigitalTr a n s f o r m a t i o nDigital hospitals focus on transforming the work-f l ow associated with a paper-based enviro n m e n tto create a more efficient and effective organiza-tion. To accomplish this goal, hospital andd e p a rtment leaders at the study sites consistentlys t ressed three key themes. Technology is beingused to improve :
1. Access to information;
2. Process efficiency; and
3. Process re l i a b i l i t y.
These themes are often interrelated. For example,i m p roving access to information in a patient’sre c o rd not only improves clinical care, it can alsoeliminate the time re q u i red to look for chart s ,resulting in streamlined, hospital ro u n d s .In c reasing the reliability of medication adminis-tration through the use of bar codes and scannerscan reduce medication errors while simultane-ously im p roving documentation.
In t e rv i ewees re p o rt significant benefits from digital transformation efforts, including betterpatient outcomes, reduced hospital costs,i m p roved pro d u c t i v i t y, and higher provider satisfaction. The following section of the re p o rt describes specific examples for each ofthese themes.
Access to Information Timely access to information is a crucial compo-nent of the care delive ry process. Studies haves h own that providing physicians with access to ap a t i e n t’s medical re c o rd at the point of careresults in better educated decisions and improve doutcomes. In a digital hospital, a single devicesuch as a personal digital assistant (PDA) cana l l ow a physician simultaneously to view dataf rom multiple sources, such as a patient’s elec-t ronic re c o rd, a bedside heart monitor, a re c e n tradiology exam, or a database of care protocols.
“ How do you define a ‘digital hospital?’You can’t define it by technology, thingschange too quickly. T h a t’s why we focuson finding better ways to provide accessto information anytime, anywhere .”
Tim St e t t h e i m e r, CIO, St. Vi n c e n t’s Ho s p i t a l
Hospital leaders also emphasize that eliminatingthe time spent looking for charts or x-rays canh a ve a profound effect on work f l ow. One inter-v i ewee estimated that searching for informationconsumed more than 60 percent of staff mem-b e r s’ time in the paper-based environment. T h i scan be eliminated when all data is available elec-t ro n i c a l l y. To ensure that clinicians have access ton e c e s s a ry information from any location in the
Number of projects
N u m b e rof beds
Construction cost
(in billions)
Number of projects
N u m b e rof beds
Construction cost
(in billions)
Number of projects
N u m b e rof beds
Construction cost
(in billions)
( So u rce: Modern He a l t h c a re’s 24th Annual Construction and Design Su rve y, Mo d e rn He a l t h c a re , Ma rch 3, 2003)
Digital Hospitals Move Off the Drawing Board | 9
hospital, interv i ewees are deploying a variety oftools, including PDAs, tablets, wireless laptops,flat screen televisions, and bedside monitors.Some examples of improved access to clinicalinformation include the following:
■ To eliminate the time-consuming pro c e s s e sassociated with a paper-based enviro n m e n t ,the emergency department at No rt h Cre s tMedical center in Sp r i n gfield, Tennessee hasbecome completely paperless. Do c u m e n t a t i o nand order entry is completed through toolssuch as Pocket PCs, and information can bere t r i e ved from flat touch screens locatedt h roughout the department. Plans are alsou n d e rway to automatically upload data fro memergency medical serv i c e s’ future electro n i cpatient tracking application to No rt h Cre s t’sclinical information system when a patienta r r i ves via ambulance.
Eliminating paper—and the need to search fordocuments—has allowed physicians to focusm o re on administering care. The time patientsspend in the emergency department has beencut by an average of 30 minutes. Despite ani n c rease in volume of 13 to 15 perc e n t ,No rt h Crest has been able to maintain its c u r rent staff level. Clinician satisfaction hasi n c reased, and emergency depart m e n tDi rector Laurie Ma x well notes that thed e p a rtment has not had an open position in more than a ye a r.
■ To ensure that clinicians have immediateaccess to necessary information from any location in the hospital, Drs. Craig Feied andMa rk Smith from Me d Star Health helpeddesign Insight, a fast, compre h e n s i ve clinicalinformation system. De veloped by Ge n e r a lDatomics, Insight re c e i ves and stores real timeinformation from all hospital legacy systems.Clinicians have immediate access to patientdata, including lab tests and images datingback to 19 9 7. In less than five seconds, staffcan view video of previously re c o rded pro c e-
d u res, a full motion cardiac catheterization, ora full motion echocardiogram. First deploye din 1996 in the emergency department atWashington Hospital Center, Insight nowre c e i ves and stores 3 to 4 terabytes of real timedata per year for each of the five Me d St a rHealth hospitals using the system.
Ac c o rding to Dr. Feied, Di rector ofInformatics, Insight is currently the fastestand most extensive clinical information system in the world. Since rolling out thesolution in 19 9 6, the emergency depart m e n tat Washington Hospital Center has been able to double its admissions from 35,000 to 70,0 0 0, without the need for additionalemergency department space.
■ Inland No rt h west Health Se rvices is a collabo-ration of five Washington State hospitals intwo integrated delive ry networks and twe n t y -f i ve regional facilities. In the push to improvethe flow of information across all part i c i p a t i n gfacilities, the nonprofit organization created aunified electronic medical re c o rd (EMR) form o re than two million patients in the re g i o n .Community physicians can access full fidelityclinical imaging, in addition to patient data,f rom their homes, offices, and at the point ofc a re on desktop or laptop computers. Ma n yalso choose to use software provided for theirPDAs that allows them to link wirelessly tothe EMR and gain access to data for all theirh o s p i t a l i zed patients from any hospital.Frederick L. Galusha, CIO, re p o rts that thetool has lead to a decrease of 30 to 45 minutesin daily rounds for each physician.
Inland No rt h west Health Se rvices will soona l l ow patients to download software to theirpersonal PDAs that gives them access to infor-mation from their medical re c o rd when theya re within the hospital’s wireless network .Patients can re v i ew their information priva t e l y,over a secure connection, on their own time.

10 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N10 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Facilities are also using technology to improveaccess to clinical expertise. T h rough videoconfer-encing and remote monitoring equipment, physi-cians can quickly seek the opinion of a specialist,track a patient’s pro g ress, or even administer caref rom a remote location. Some examples include:
■ In an effort to make more efficient use of staffand address capacity problems, Se n t a r aNo rfolk General Hospital in No rfolk, Vi r g i n i amonitors patients in multiple intensive careunits from a remote location. The “v i rt u a l”ICU team—consisting of an ICU physician, acritical care nurse, and associated clericalstaff—can track a patient’s condition thro u g hfour screens that display: video of the patientroom; the patient’s vital signs; the patient’se l e c t ronic medical re c o rd; and alerts to signifi-cant changes in heart rate and other criticalparameters. When intervention becomes nec-e s s a ry, the virtual staff can communicate withon site personnel through the ICU’s video andaudio capabilities.
Remote monitoring of patients in the ICUhas lead to quicker intervention, resulting ini m p roved patient outcomes and reduced costs.A study of Se n t a r a’s first year with the systemin 2001 showed faster intervention lead to a25 percent decrease in hospital mortality ratesfor ICU patients. After subtracting the totalcosts of the project, the hospital was able tore a l i ze a 26 percent savings for ICU patientstay and a 17 percent decrease in ICU lengthof stay. These savings equated to $2,150 perpatient and a total of $3 million per year fortheir two digital ICUs. Use of the system alsomeets the Leapfrog ICU standard for aro u n d -the-clock coverage by an intensivist.
“We’ve learned that remotely monitoringpatients in the ICU does work. T h eresults are there and the skeptics havebeen quieted. Day to day, early interve n-tion saves dollars, saves ICU days, ands a ves live s .”
A n n - Marie Cochran RN, Product Manager for Information Te c h n o l o g y,
Sentara No rfolk General Ho s p i t a l
■ Hamot Medical Center in Erie, Pennsylvania,is making use of real-time network connec-tions and video-conferencing equipment toestablish contact with physicians outside thephysical walls of the hospital. To ensurearound-the-clock radiologist coverage,Hamot has partnered with a site in Australia.The 14-hour time difference allows techni-cians in Erie to send digital images at offhours to an “on-call” Australian radiologistfor rapid diagnosis. The relationship is conveniently reversed half a day later.
Fi n a l l y, some digital hospitals are also focused oni m p roving access to information for patients.
■ The Patient Portal at PeaceHealth’s newhospital in Springfield, Oregon will allowpatients to view a simplified version of theirclinical and financial information, makeappointments, and order prescription re f i l l s .Physicians will be able to view current patientre c o rds and order services for hospitalize dpatients from their offices. T h rough a We b c a min the neonatal intensive care unit, new p a rents will be able to watch their childre nf rom home.
The new hospital will also experiment withd i f f e rent types of patient monitoring technol-ogy that providers and family members canuse to re v i ew a patient’s condition from aremote location. For example, through a “v i rtual waiting ro o m” system, families will beable to get re g u l a r, real-time updates through a mobile device, rather than keeping a vigil atthe bedside.
Digital Hospitals Move Off the Drawing Board | 11
■ Physicians Hospital in El Paso, Texas is plan-ning to install patient entertainment systemsin its new hospital. T h rough bedside devices,patients will be able to view movies, access theInternet, watch educational films, and eve no rder meals. Physicians will be able to sit withpatients and families to re v i ew the patient’sown digital images and clinical informationf rom a touch screen at the bedside. All thesef e a t u res are designed to play a significant ro l ein improving the patient experience.
Process Efficiency In t e rv i ewees also relied on new technology toautomate existing processes and streamline work-f l ow. By improving process efficiency, hospitalscan increase throughput and capacity. Ph y s i c i a n sand nurses spend more time with patients, con-tributing to a rise in satisfaction. Also, by study-ing the data on process performance, sites we reable to identify and address potential pro b l e m searly on.
“Without enough data to evaluate something, what is the point? If you c a n’t effectively measure a process, yo uc a n’t improve it.”
Dr. Frank Orth, Mount Carmel St. Ann's Ho s p i t a l
■ The system from A4 Health Systems selectedfor the new emergency department at Mo u n tCarmel St. Ann's Hospital in Ohio automatesall aspects of patient data collection and cared e l i ve ry from initial check-in—which takesless than two minutes—to final disposition.Using color coding and a compre h e n s i ve set of icons (currently about 110), the system isable to drive workflow and alert clinicians to critical values and outstanding tasks.Clinicians can view the condition, location,and admission time of all patients in thedepartment through an electronic “grease-board” available on mobile devices and computers throughout the department.
The system allows staff to track the ave r a g etime that patients are spending in the EDf rom admission to discharge, and determine ifspecific clinical complaints are causing bottle-necks in flow. Overall, in the first year of oper-ation, the department saved more than $1.5million from improved process efficiencies.
■ St. Vi n c e n t’s Hospital in Bi r m i n g h a m ,Alabama is engaged in a pilot project to testVocera communication badges. Using a small,one-button device worn around the neck, staffcan immediately contact a specific clinician, ag roup of clinicians, or a type of specialist. Byp ressing the button and saying, “Call Ja n eJo n e s” or “Find neurologist,” a connection isestablished to the nearest contact who is in thehospital and not in a pro c e d u re room. St a f foutside the walls of the hospital can access thesystem by calling an 800 number and usingthe same verbal commands used to operate the device.
Since deploying the communication badges inMay 2003 across the neurology unit, Vo c e r are p o rts that nurses at St. Vi n c e n t’s have beenable to save up to 30 minutes each day thatwould have been spent finding a clinician.
■ The digital operating rooms at the Un i ve r s i t yof Pittsburgh Medical Center have integratedn ew technology with physical design changesto streamline surgeries. HERMES vo i c e - c o n-t rolled software allows the surgeon to makesmall, precise adjustments to the operatingtable camera or lights using only voice com-mands. In traditional surgeries, a nurse wouldh a ve to be interrupted each time a changeneeded to be made. Most of the new equip-ment is mobile or fixed to the ceiling onbooms, and can be quickly rolled out of thew a y, making clean-up between cases faster.

12 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N12 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
In the first year of operation, executives atUPMC believe the new operating roomswere able to save as much as $400,000 byreducing time between cases and cuttingclean up time in half. Overall, the new tech-nology lead to a reduction in actual casetimes of 5 to 8 percent.
In a randomized trial, re s e a rchers at UPMCfound that physician and nurse satisfactionrose significantly after introducing the speechrecognition system used by the surgeons toc o n t rol a number of operating room devices.Asked to rate their satisfaction with the systemon a ten-point scale, nurses assisting with surgeries returned and average score of 9.2,c o m p a red to 5.3 for those in traditional siteswho had used the technology in the past. The response from physicians was just as p o s i t i ve (9.0 vs.5.1 ) .14
Process Reliability Un n e c e s s a ry variables in the delive ry of care can lead to medical errors. Computers allow tasksto be performed exactly the same way for eve rypatient. With sophisticated decision support, the systems can check for potential errors, remind about ove rdue tests, and support pro t o-cols for care .
■ When it opens in fall 2003, Ph y s i c i a n sHospital in El Paso, TX, will promote patientsafety by linking bar-coded medications with ap a t i e n t’s electronic medical re c o rd. Nurses willdocument medication administration thro u g ha handheld device. Be f o re a drug is given to apatient, the bar code on the dru g’s packagingwill be scanned and compared with a bar codeon the patient’s wrist. An alert will be generat-ed if the medication has not been ord e red or ifa potentially dangerous drug interaction isfound or an allergy exists.
■ In a paper-based world, ensuring that all carerelated charges are accurately captured andassociated with a specific patient can be timeconsuming and inaccurate. St. Vi n c e n t’sHospital, which tags IV drugs administere dduring surgery with bar codes, is using theDo c u Jet system from Do c u Sys to re c o rd med-ication administration. When a syringe isloaded into the device, the system displays thed rug and concentration level. The bar code isverified against the patient’s electronic re c o rdto check for allergies, drug interactions, ande ven recent doses. Any potential pro b l e mp rompts an alert—both on the device’s smalls c reen and on the monitor in front of thephysician. As the drug is administered, a cam-era inside re c o rds the total amount dispensed.All information is stored in the patient’sre c o rd, ensuring that the hospital can trackand account for all IV medications and billa c c o rd i n g l y.
■ Ad vances in robotics in the minimally inva s i veendoscopic suites at Sentara No rfolk Ge n e r a lHospital are designed to increase safety of sur-gical pro c e d u res. Instead of relying on ascalpel or probe, the surgeon sits at a consoleaway from the operating table, viewing thes u r g e ry from a monitor. Using hand contro l s ,the surgeon can remotely pilot the ro b o t’s twosurgical arms. Endoscope position, light inten-s i t y, and table height are manipulated by thep h y s i c i a n’s voice. Any movement of the ro b o tor adjustment to the table is precise and exact,g reatly reducing the risk of erro r. The OR atSentara recently became one of the first in thec o u n t ry to perform a laparoscopic radicalp rostatectomy with ro b o t i c s .
Digital Hospitals Move Off the Drawing Board | 13
Approaches to Making the Digital Tr a n s f o r m a t i o nOrganizations have taken two approaches tointegrating technology into the operationalmodel of the hospital. Some are building a newfacility and incorporating technology into thehospital design. These can be completely newhospitals, like the 40-bed acute care PhysiciansHospital in El Paso, Texas, or replacement sites,like the facilities under construction at ElCamino and PeaceHealth. Other hospitals,already in operation, are working to make thetransition to a digital environment by integrat-ing technology in stages, either across theorganization or within a specific department.
Integrating Technology in New HospitalsMost organizations building a new facility startby establishing a vision. The vision includes goalsfor the future as well as descriptions of the futuree n v i ronment and how the application of technol-ogy will enable better care.
In determining the goals for El Camino Ho s p i t a l ,for example, CEO Lee Dominico and his col-leagues we re responding to a number of trends in health care, including the transition:
■ From exc l u s i vely selling large blocks of serv i c e sat low prices to third party payers to sellingindividual services to patients who are takingan active role in their health care .
■ From a “no questions asked, physician-drive ne n v i ro n m e n t” to shared decision makingb e t ween the patient and the family and thedoctor and nurses, accelerated by advances int e c h n o l o g y, such as the In t e r n e t .
■ From human intervention at all times toincreased technology substitution for humancapital, lowering cost and improving per-formance.
■ From “episodic, hospital-centered, one-size -fits-all care” to administering care on multipled e l i ve ry platforms beyond the physical walls
of the facility, including the internet, at homeclinics, and partner hospitals.15
El Camino then set three goals for the new h o s p i t a l :
■ Build the “s m a rt” hospital of Silicon Va l l e y.
■ Create the health care destination of Si l i c o nVa l l e y.
■ Create a care system based on individualpatient needs and va l u e s .
Pe a c e Health built their vision around achievingthe goals laid out in the IOM re p o rt “Cro s s i n gthe Quality Chasm.” To convey their vision tothe entire enterprise, they created a documentthat describes the future health care experiencef rom a patient, nurse, and physician perspective .
Approaches to Planning New HospitalsAt the drawing-board stage, digital hospitalsgenerally had a planning team that includedoperational staff and members of the IT depart-ment. In the case of new hospitals, this team wassmall, but dedicated all their time to planningthe facility. Replacement hospitals often hadonly one or two staff people assigned to thep roject, but invo l ved many others in planningcommittees for specific processes (access to care ,supply chain management) or operational are a s( l a b o r a t o ry, ED, etc). Almost all hospital designteams had members of the architectural designfirm as well as outside technology consultants askey part i c i p a n t s .
The planning was typically stru c t u red based onthe lead-time re q u i red to implement decisions.The teams started with design of the physicalplant, then identified technology that would beneeded, and finally designed the operationalmodel. This approach is not always effective ,h owe ve r. Admitting can be in a centralize dd e p a rtment or at the bedside; documentation ata central nursing station or via mobile technologya n y w h e re in the hospital. The operational modelaffects the arc h i t e c t u re design.

14 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N14 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
“ In planning for the new hospital, themost important thing is to determ i n eh ow you are going to do business in thef u t u re. We’re trying to predict what thehospital will look like years from now.”
Dennis Sato, El Camino Ho s p i t a l
Planning teams re a l i zed that while plans fora rc h i t e c t u re, technology, and operations shouldideally be done in parallel, the logistics of thechanges may not allow for such an appro a c h .One hospital assessed what technologies had theg reatest potential impact on the facility designand focused on those considerations first.Technology standards we re adopted—consistentwith the anticipated national standards thre eyears into the future—so that all equipment p u rchased would fit with the new facility’s tech-nology arc h i t e c t u re.
“ It’s not so much about what we want to do in 2008 when our new hospitalopens. It’s about the changes we are mak-ing to our practices today. For example,one of our goals is to be completely film-less by 2008 and we are not planning to build a film room in the new hospital.Waiting until then to incorporate changesto the associated processes would be disas-t ro u s — we need to start doing businessd i f f e rently today.”
Ma rk Zielazinski, CIO, El Camino Ho s p i t a l
Most hospitals do not have a single person whois responsible for both clinical and informationt e c h n o l o g y, which makes integrated planning achallenge. Likewise, overall responsibility forfacility construction and IT planning was splitb e t ween two people at eve ry study site. Often the responsibility for operational planning wasd e c e n t r a l i zed, with separate teams focused on the
design of nursing care, supply management, thel a b o r a t o ry, etc. Planning for clinical technologieswas always decentralized, with each depart m e n tchoosing its technology. All participating sitesre c o g n i zed the need to have more coord i n a t i o namong these groups. Se veral recommended cre a t-ing a program management office to take re s p o n-sibility for integrating the planning for IT andoperations with the design of the facility.
Integrating Technology in Existing HospitalsBuilding a new or replacement hospital from theg round up is not a viable option for most sites.In fact, while there are almost 6,000 hospitals inthe United States, only 105 new entire acute carehospitals broke ground in 2002.16 Planning andc o n s t ruction re q u i res hundreds of millions ofdollars and a significant investment of time andre s o u rces—for example, El Camino estimatescosts approaching $300 million for their newf a c i l i t y. In light of practical and financial limita-tions, many existing sites are taking a stageda p p roach to building the digital hospital.
Some of these sites are focused on incorporatinga number of technologies across the enterprise.Others have identified a specific problem withina department and are looking for the right tech-nology to solve it.
“We tried to gradually integrate new tech-n o l o gy. By putting an electronic wra p p e ra round all existing processes, our hopewas to make all old processes go away. Wewant old systems to die a natural death.”
Dr. Craig Feied, Di rector of Informatics, Me d Star Health Sy s t e m

Digital Hospitals Move Off the Drawing Board | 15
St. Vi n c e n t’s Hospital in Birmingham, Alabamais integrating a variety of technologies across theorganization. The site is the designated digitalhospital for Ascension Health System and isintended to serve as a model facility, show i n gother hospitals in the system and the countrywhat can be accomplished with informationt e c h n o l o g y. Leaders at the hospital are alwayslooking for new, innova t i ve technology solutions.Decisions are driven by determining which newp roducts can fill the gaps in supporting carep rocesses. For example, in assessing software fro mAdobe, the hospital re a l i zed they could integratec e rtain components of the paper-based re c o rd(such as documents requiring signatures) intothe electronic medical record. The hospital hassince entered into a partnership with the com-pany to use its workflow tools and eliminate allremaining paper.
Inland No rt h west Health Se rvices is a collabora-tion of two competing Spokane, Wa s h i n g t o n -a rea health systems that strives to become a re c o g n i zed national leader in innova t i ve healthc a re solutions. In addition to creating an inte-grated information system for the part i c i p a t i n ghospitals, the nonprofit organization has spon-s o red initiatives like Inland No rt h we s tTe l e H E A LTH Se rvices, a network that allow srural physicians to communicate with specialistsin city hospitals through real-time video andaudio conferencing capabilities. This technology,in combination with the integrated clinical infor-mation system, has also been applied to create adigital, paperless Te l e PH A R M ACY networkb e t ween larger Spokane hospitals and rural hospi-tals where pharmacists are in short supply. Ke ydecisions on technology projects and initiative sa re determined by which new solutions can besta d d ress the strategic plans for hospitals, depart-ments, physicians, and consumers.
Sometimes efforts to integrate technology acro s sthe enterprise start by optimizing a single depart-ment. Many efforts are underway nationally toc reate the OR of the future, the ED of the
f u t u re, and the ICU of the future. Some are driv-en by a vision of the way care will be delive re d .Others are the result of a specific operational cri-sis. Either way, these departments are high stre s spoints in the current health care system and cans e rve as a proving ground for the entire hospital.For example,
■ The digital ORs at University of PittsburghMedical Center (UPMC) are the vision ofsurgeons Jim Luketich and Phil Schauer.Although no operational crisis existed atUPMC, the surgeons believed that minimal-ly-invasive surgery was going to growdramatically and that it could be done mosteffectively in a specially equipped operatingroom. The two physicians began by sellingtheir vision to the executive team, and lead-ing a number of meetings between surgeons,department heads, and industry leaders. Thefirst two operating rooms were built in 2001,three additional rooms were reconfiguredshortly thereafter.
“Ad m i n i s t ra t i ve support is essential, andto keep that support for a long period oftime, you need to be using the technology,driving re venue, publishing papers, andteaching residents. You need clinicianswith a passion – their energy will carrythe whole project forw a rd .”
Dr. James Luketich, Un i versity of Pi t t s b u r g hMedical Center
In other cases, the departmental transformationresults from solving a specific operational pro b-lem, as the following examples describe.
■ The intensive care units at Sentara No rf o l kGeneral Hospital we re suffering from capacityp roblems, high costs, and inconsistent carep rocesses. As an organization accustomed toexploring new technology, Sentara selected theeICU product from Visicu to maximize the
use of intensivists and facilitate fast interve n-tions when patients are in need of care. T h etechnology has been so successful that Se n t a r ahas rolled it out to three of the six hospitals inthe system and will expand to a fourth sitethis ye a r.
■ Be f o re opening their new emergency depart-ment two years ago, Mount Carmel St. Ann’sHospital in Ohio was struggling with capacityp roblems. The decision was made to designthe facility with the assumption that the tech-nology would make it paperless.
“You need to examine eve ry aspect ofe ve ry process, thinking about screens inthe context of hospital work f l ow.Sometimes you need to make adjustmentsto the system, sometimes you need to fixthe process. It’s the hardest thing I’ve e ver done.”
Sonja How a rd, Clinical Ed u c a t o r, Mount CarmelSt. Ann’s Ho s p i t a l
While phasing technology in at a measured pacea l l ows hospitals to focus on specific areas of oper-ational excellence, challenges still exist. For sitesi n t roducing technology into a department with a high number of patient transfers, just one are ain the facility may be affected. New informationneeds to be integrated with existing systems toc reate a complete medical re c o rd. The location ordesign of the existing space may also limit whatcan be done.
16 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Digital Hospitals Move Off the Drawing Board | 17
THE DIGITAL HOSPITAL IS NOT YET A REALITY.The early state of current efforts makes it impossible to definebest practices for achieving the digital transformation and whatresults can be expected. In spite of the limited experiencenationwide, interv i ews with those at the study sites did re ve a lsome common themes on the barriers that must be ove rc o m eand the practices that contribute to success. Fi ve themes we res t ressed consistently:
The Need for Strong LeadershipAll study participants cited leadership and vision as keys tosuccess. Se veral sites had a CEO who believed that technologywas the key to the future. Cu rtis James at St. Vi n c e n t’sHospital has long been a technology advocate within bothAscension Health and one of its predecessor organizations,Daughters of Charity. John Haywood at Pe a c e Health canclearly articulate his vision for the role of technology in nextgeneration health care. His predecessor was of the same mind,a d vocating the purchase of the PHAMIS system (now IDXC a re C a s t ) .
“The administration needs to fully understand the depth of commitment that is re q u i red, and bep re p a red to take the appropriate action to ensure s u c c e s s .”
Sonja How a rd, Clinical Ed u c a t o r, Mount Carmel St. Ann’s Ho s p i t a l
Howe ve r, the drive to go digital does not have to come fro mthe top. At the Un i versity of Pittsburgh Medical Center, Dr s .Luketich and Schauer came to the hospital to lead a pro g r a mof minimally inva s i ve surgery with the vision that the ORswould be optimized to conduct what was then a new appro a c hto surgery. While they have full support from administration,their COO, John Innocenti, characterizes his role as “m a k i n gs u re nothing gets in their way.”
Washington Hospital Center re a l i zed that performance of theemergency department needed to be dramatically improve d .Drs. Craig Feied and Ma rk Smith we re hired to lead the trans-formation. One of their first interventions was to develop aninformation system that would ensure timely and accurateinformation from all sources was available in the ED.
III. Common Themes and Lessons Learned

18 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Explore the PossibilitiesHospitals we re asked about strategies for obtain-ing and evaluating new operational designs orn ew technologies. Se veral organizations hire dleaders who could show them what needed to bedone. Within departments, ideas sometimescame from canvassing the exhibits at trade show sand talking with colleagues at professional meet-ings. Hospitals that had reputations as technolo-gy advocates had less of a problem finding tech-nology; their challenge was efficiently scre e n i n gsolutions that we re brought to them by entre p re-neurs and salespeople for technology firms.
All of these approaches proved to have disadva n-tages. They we re hard to sustain across an entirehospital, and the people advocating part i c u l a rsolutions often lacked any data to support theirchoice, nor could they act as good sources ofinformation about the re l a t i ve benefits of alterna-t i ve technologies.
Other study sites took a different approach. T h eUn i versity of Pittsburgh Medical Center selectedSt ryker as a vendor partner for their digital ORsto not only provide equipment, but to serve asthe general contractor. If St ryker did not manu-f a c t u re a needed product (such as the vo i c erecognition software that controls the lights,table, and cameras), they found another supplier.St ryker was responsible for ensuring that thee n t i re solution would work together to create theideal minimally inva s i ve OR.
“ It is essential to pre-sell the concepts andbenefits to the physicians and other clini-cal staff. The biggest learning curve is thefear of the unknow n .”
A n n - Marie Cochran, R.N., Product Manager forInformation Te c h n o l o g y, Sentara No rfolk
General Ho s p i t a l
Pe a c e Health is a member of He a l t h Tech (T h eHealth Technology Center). He a l t h Tech pro-duces re p o rts on emerging technologies thata d d ress the current state of the technology and
its likely evolution. These re p o rt s p redict thelikely impact of technology on staffing, ITneeds, reimbursement, and hospital utilization.Pe a c e Health used these as one source of infor-mation on what clinical technologies theyshould use in their new facility. They also s u m m a r i zed the re p o rts to educate the entireleadership team about how technology couldhelp achieve their plan for a next-generationhealth care facility.
The Importance of Tr a i n i n gTraining is probably the most overlooked compo-nent of introducing new processes and new tech-nology into any setting. Howe ve r, health carep resents special challenges. Hospitals must trainstaff that work 24 hours a day and 7 days a we e k .Training typically needs to be available on thesame schedule, unless the hospital is willing topay staff to attend training in off-work hours. Inmost hospitals the physicians are not employe e s ,and time spent in training detracts from theirability to see patients and generate re ve n u e .
One goal in the study sites was to minimize theneed for training by selecting systems that aresimple to use and guide the user from one activi-ty to the next. Built-in safety features to pre ve n tusers form making serious errors are also impor-tant. At St. Vi n c e n t’s Hospital the OR documen-tation system takes the user through a task listthat automatically moves to the next task whenone is completed.
“The technology needs to be user friendly,fast and reliable. If physicians can writeit down faster than they can enter it inthe system, you are going to have pro b-lems. Once the choice has been narrowe dd own, take the most ave rage user you canfind and measure their success with thes y s t e m .”
Paul Minton, ED System Ad m i n i s t r a t o r,No rt h Crest Medical Center

Digital Hospitals Move Off the Drawing Board | 19
One-on-one training and demonstrations arereplacing classroom training in many settings.The objective is to tailor training to the needs ofthe user and to confirm mastery of the know l-edge as training is delive red. The Un i versity ofPittsburgh Medical Center has the mosta d vanced training capabilities of all part i c i p a t i n ghospitals (and one that might not be cost effec-t i ve outside of a major teaching hospital). T h en ew digital ORs are equipped to transmit imagesof the OR, the patient’s data, and the internalimage of what the surgeon is seeing and doing.While observers can follow the pro c e d u re from av i ewing room next to the OR, they can also seethe same images in an upstairs conference ro o mor at a remote facility.
The Un i versity of Pittsburgh Medical Center alsohas a large simulation laboratory. The trainingcenter can be used to train and certify people onn ew technology and new pro c e d u res using simu-lated patients in hospital rooms, the ED, and theOR. They have a an extensive curriculum deve l-oped by hospital staff that is used for vo l u n t a ryand mandatory training. The students can trackthe results of specific actions and re v i ew thescripts of virtual encounters to learn from mistakes. The video of each simulation can bereviewed at a later time by students and profes-sors through the center’s Web portal.
“ Our training labora t o ry can simulateany kind of potential disaster and pre p a restaff for once in a lifetime situations.Ph y s i c i a n’s reaction to what happens onep e rcent of the time saves live s .”
Dr. John Williams, Chair, Dept of Anesthesiology,Un i versity of Pittsburgh Medical Center
The Value of Vendor Part n e r s h i p sPa rticipating hospitals stressed the importance of partnering with vendors. At a minimum, thep a rtnership invo l ved an agreement from the vendor to modify or develop a product to meetp re-defined needs, and re q u i red an exchange ofk n owledge from both sides to be effective. Insome partnerships, such as the one between St .Vi n c e n t’s and Do c u Sys to develop an OR system,both parties collaborated to create the pro d u c t .Others, such as the relationship between St ry k e rand the Un i versity of Pittsburgh Medical Center,m o re closely resembled standard contractor/pur-chaser arrangements. In some instances the ve n-dor also provided funding for re s e a rch at theinstitution or for learning centers, but in manycases the only direct monetary benefit to the hospital was free equipment for the initial test.
The Value of User Part n e r s h i p sHospitals that we re selected for site visits cre a t e ds t rong partnerships between the end users andthe IT experts to design and implement theirdigital services. W h e re the focus was on re d e s i g n-ing departments, a user typically led the effort. Inthose sites investigating how technology could beapplied across the hospital, the IT depart m e n tstaff we re often in the lead. In all cases a personwho understood both the clinical use and thetechnology played a key role. These people we resometimes formally trained in clinical informat-ics, but often we re nurses who worked in the ITd e p a rtment or physicians who had pursued ani n t e rest in technology. In all the study sites thee f f o rts we re sanctioned by the institution, whichmade staff available to work on the pro j e c t .
“A large part of our success stemmed fro mthe fact that the system was designed andd r i ven by people who are experts in bothmedicine and technology.”
Dr. Craig Feied, Di rector of Informatics at Me d Star He a l t h
20 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
E x p e c t a t i o n sIn talking with the people who are planning new facilities, itbecame clear that the benefits of incorporating digital technol-ogy into hospital operations extend far beyond the installationof new equipment. Many of the institutions being conceive dtoday are truly health systems that integrate information acro s sthe continuum of care, including hospitals, physician practices,and long-term care, and can even extend into a patient’s home.The participants in this study of digital hospitals re c o g n i ze dthat access to information was the first key barrier to ove rc o m ewithin the hospital. Providing access to information amongsettings is even more challenging, and these connections bare l yexist today.
For example, how does the hospital know what medicationsthe patient is taking on an ambulatory basis so they can avo i dd rug interactions with medications being given in the hospital?How does the emergency department know whether an abnor-mal EKG pattern is new or has been there for years? When apatient appears in a physician’s office two days after dischargef rom the hospital, what will they know about the course oft reatment? Providing a seamless, instant flow of informationb e t ween all authorized care g i vers is the digital hospital’s ulti-mate goal.
The institutions invo l ved in this re s e a rch stated that they we red e voting more than half of their efforts to changing pro c e s s e sas opposed to implementing new technology. Hospitals on thedrawing board seem to be weighted more heavily tow a rd thep rocess end of the spectrum. For instance, at Pe a c e Health, then ew design was framed around the ten principles outlined inthe Institute of Medicine Re p o rt “Crossing the Qu a l i t yChasm.” Their goal is not paperless or digital but transformingtheir entire operation to meet the IOM goals.
I V. Future of the Digital Hospital

Digital Hospitals Move Off the Drawing Board | 21
The Bottom LineThe reality of the digital hospital is still two tof i ve years away. While most institutions planningnext-generation health care want to learn fro mpast experimenters, access to that experience isve ry limited. Few sites are operational and haveresults to show; fewer still have done formal eva l-uations of their digital experience or even docu-mented their lessons learned. This re p o rt is onestep tow a rd filling that knowledge gap.
A dispro p o rtionate share of the current andplanned digital hospitals are specialty institutions,and many invo l ve opening new facilities, ratherthan replacing existing ones. The specialty hospi-tals often have different business models, andn ew facilities have staff dedicated to planning the new facility. Since most U.S. hospitals aren o n p rofit, acute care general hospitals, many arewaiting to see whether this model proves to beboth broadly applicable and afford a b l e .T h e re f o re, projects such as the new El CaminoHospital and Pe a c e He a l t h’s new Sa c red He a rtMedical Center at Riverbend will be ve ry impor-tant for the advancement of next generationhealth care .
Based on the findings of this re s e a rch, theauthors recommend that all organizations adoptsome sort of “technology watch” function bycreating a formal process for educating the lead-ership about emerging technologies. They mightalso consider adopting a formal technologyadvocacy program to evaluate the potential benefits of new technologies. All of these stepswould help prepare the organization to makeintegrated decisions about how facility designs,clinical technologies, IT, and operational modelscan help to implement their vision of next-gen-eration health care.
22 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
El Camino
Hamot Medical Center
Inland Northwest Health Services
Mount Carmel St. Ann’s Hospital
NorthCrest Medical Center
Physicians Hospital
Sacred Heart Medical Center at Riverbend
Inventory of Digital Hospital Projects
Appendix
Mountain View, CA
Erie, PA
Spokane, WA
Westerville, OH
Springfield, TN
El Paso, TX
Springfield, OR
Building a newdigital hospital
Digital imagingdepartment, digital OR
Collaboration of 5 city-wide and 25regional hospitals tointegrate technologyacross participatingorganizations
Digital ED
Digital ED
Building a newdigital hospital
Building a newdigital hospital
● Replacement facility● 350 beds● Costs expected to range
from $240 to $300 million● Scheduled to open in 2008
● 336-bed tertiary carefacility
● Open● Imaging department of
the future
● Formed in 1994
● Emergency departmentaverages about 65,000 visits each year
● 80 percent of hospitalsadmissions come throughthe emergency department
● Went live on system June 2001
● Opened new emergencydepartment December2001
● 109 bed community hospital
● Emergency departmentaverages 25,000 visits peryear
● System rolled out in May 2000
● 40 bed acute care facilitywith a 3 bed, level 4 ER
● Privately owned by a groupof local investors
● Scheduled to open in fall 2003
● Replacement facility forSacred Heart
● Scheduled to open 2007
Ma rk Zielazinski, CIODennis Sato, CIOfrom Eclipsys (outsourced)
Marilyn Davis, R.N.,Manager of BusinessApplications
Joe Bulter, CIO
Frederick L. Galusha,CIO
Sonja Howard, R.N.,Clinical Educator
Dr. Frank Orth,Physician Facilitator,Emergency CareCenter
Paul Minton, ED SystemsAdministrator
Laurie Maxwell,Director of ED
Tom Coulehan, CIO
Dr. John Haughom,CIO
Hospital Name Location Initiative Details Interviewees
Digital Hospitals Move Off the Drawing Board | 23
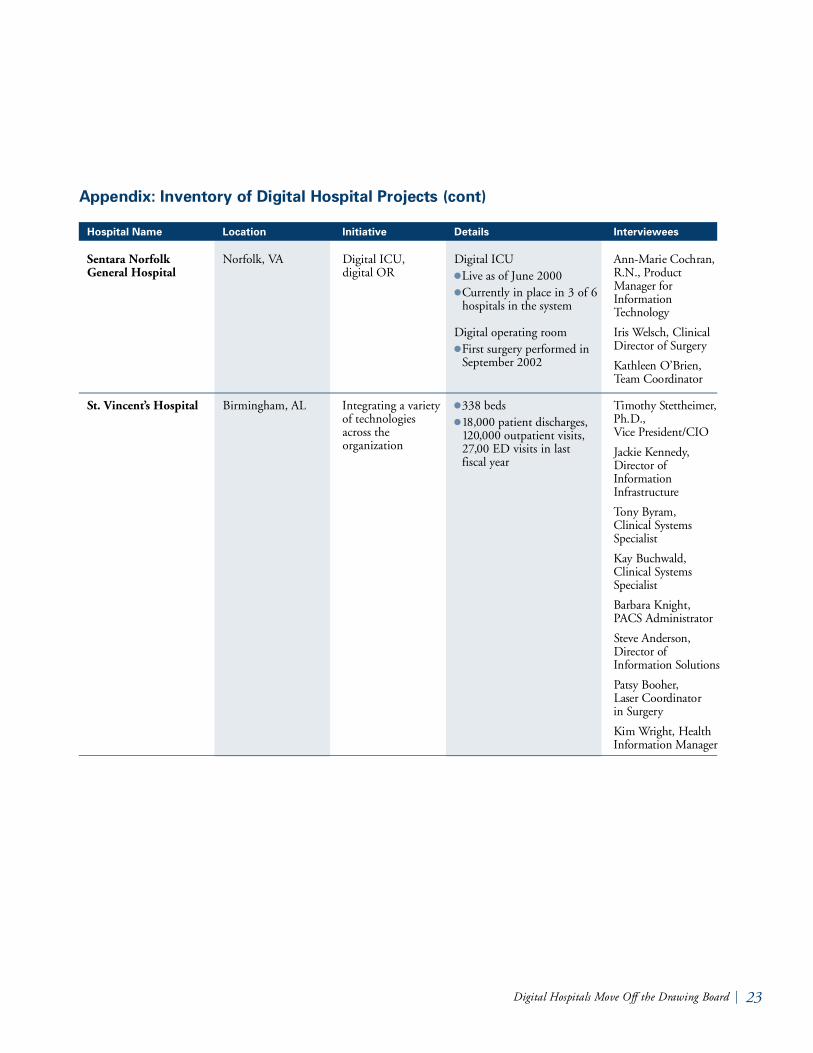
Sentara Norfolk General Hospital
St. Vincent’s Hospital
Appendix: Inventory of Digital Hospital Projects (cont)
Norfolk, VA
Birmingham, AL
Digital ICU,digital OR
Integrating a varietyof technologiesacross the organization
Hospital Name Location Initiative Details Interviewees
Digital ICU● Live as of June 2000● Currently in place in 3 of 6
hospitals in the system
Digital operating room● First surgery performed in
September 2002
● 338 beds● 18,000 patient discharges,
120,000 outpatient visits,27,00 ED visits in last fiscal year
A n n - Marie Cochran,R.N., Pro d u c tMa n a g e r f o rIn f o r m a t i o nTe c h n o l o g y
Iris Welsch, ClinicalDi rector of Su r g e ry
Kathleen O’Br i e n ,Team Coord i n a t o r
Timothy St e t t h e i m e r,Ph.D., Vice Pre s i d e n t / C I O
Jackie Ke n n e d y,Di rector ofIn f o r m a t i o nIn f r a s t ru c t u re
Tony Byram, Clinical Sy s t e m sSp e c i a l i s t
Kay Bu c h w a l d ,Clinical Sy s t e m sSp e c i a l i s t
Barbara Knight, PACS Ad m i n i s t r a t o r
St e ve Anderson,Di rector ofInformation So l u t i o n s
Patsy Booher, Laser Coordinator in Su r g e ry
Kim Wright, He a l t hInformation Ma n a g e r
24 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
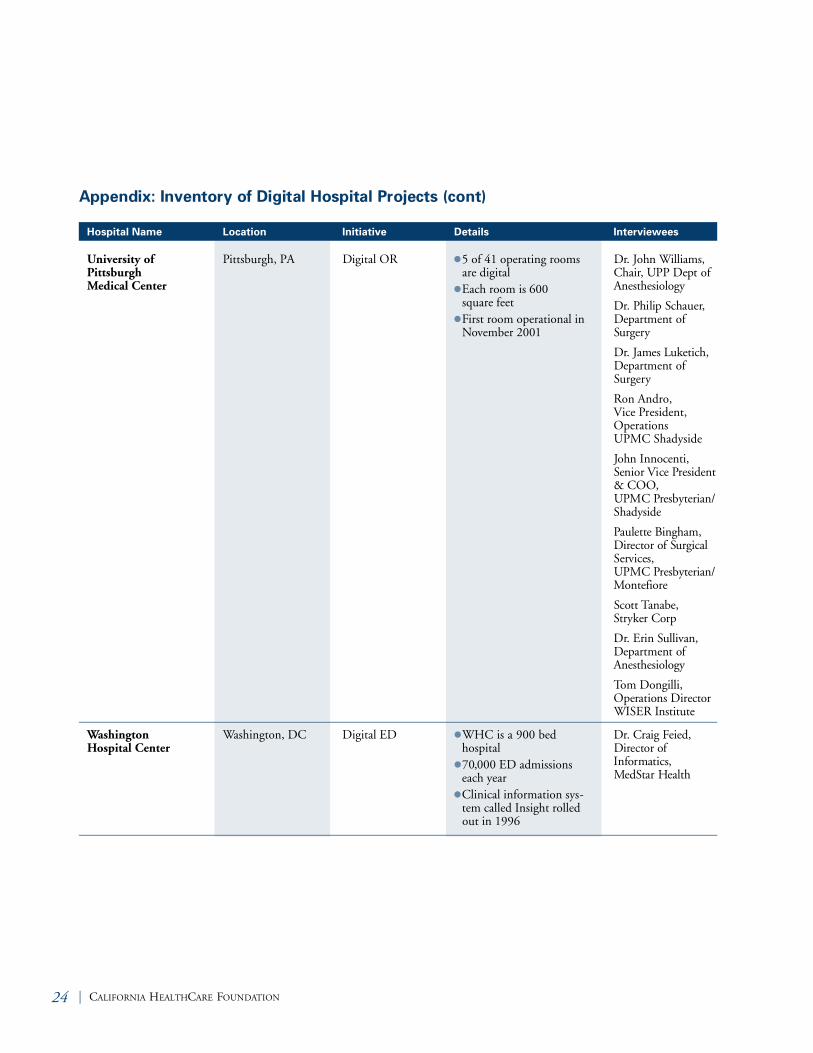
Appendix: Inventory of Digital Hospital Projects (cont)
Hospital Name Location Initiative Details Interviewees
University of Pittsburgh Medical Center
Washington Hospital Center
Pittsburgh, PA
Washington, DC
● 5 of 41 operating roomsare digital
● Each room is 600 square feet
● First room operational inNovember 2001
● WHC is a 900 bed hospital
● 70,000 ED admissionseach year
● Clinical information sys-tem called Insight rolledout in 1996
Digital OR
Digital ED
Dr. John Wi l l i a m s ,C h a i r, UPP Dept ofA n e s t h e s i o l o g y
Dr. Philip Schauer,De p a rtment ofSu r g e ry
Dr. James Lu k e t i c h ,De p a rtment ofSurgery
Ron Andro,Vice President,OperationsUPMC Shadyside
John In n o c e n t i ,Senior Vice Pre s i d e n t& COO, UPMC Pre s by t e r i a n /Sh a d y s i d e
Paulette Bi n g h a m ,Di rector of Su r g i c a lSe rvices, UPMC Pre s by t e r i a n /Mo n t e f i o re
Scott Ta n a b e ,St ryker Corp
Dr. Erin Su l l i va n ,De p a rtment ofA n e s t h e s i o l o g y
Tom Do n g i l l i ,Operations Di re c t o rWISER In s t i t u t e
Dr. Craig Fe i e d ,Di rector ofInformatics, Me d Star He a l t h
Digital Hospitals Move Off the Drawing Board | 25
1. Hospital Emergency De p a rtments: Crowd e dConditions Va ry Among Hospitals and Communities.G AO, Ma rch 2003.
2. “ National and Local Impact of Long-termDemographic Change on Inpatient Acute Care . ”Solucient, November 2002.
3. 2002 AHA En v i ronmental Assessment.
4. The He a l t h c a re Wo rk f o rce Sh o rtage and It sImplications for American Ho s p i t a l s , AHA 2001.
5. “ Hospitals Face a Challenging Op e r a t i n gEn v i ronment.” Statement of the AmericanHospital Association before the Federal Tr a d eCommission, September 2002.
6. Institute of Medicine. Crossing the Quality Chasm:A New Health System for the 21st Ce n t u ry. Na t i o n a land Academic Press, Washington D.C., 2001.
7. Ib i d .
8. “ Sp e c i a l i zed Digital Hospitals Take Of fNationwide.” He a l t h c a re In f o rm a t i c s , June 2003.
9. “ New Indianapolis He a rt Center Offers Latest inHi g h - Tech He a l t h c a re.” Indianapolis St a r,Fe b ru a ry 14, 2003.
10 .“ He a l t h South Pre vails in Suit over Di g i t a lHospital.” Bi rmingham Business Jo u rn a l ,Fe b ru a ry 7, 2003.
11.AHA Hospital Statistics, 2002.
12.“ Projects by Construction Phase in 2002.” Mo d e rn He a l t h c a re , Ma rch 3, 2003.
13.“ Regional Medical Center To Try Tr a c k i n gTechnology For Emergency Room Ef f i c i e n c y. ”Memphis Commercial Appeal, June 11, 2003
14.Luketich J.D., Fernando H.C., Bu e n a ventura P. O . ,Christie N.A., Grondin S.C., Schauer P.R. “Re s u l t sof a Randomized Trial of HERMES-assisted Ve r s u sNon-HERMES-assisted Laparoscopic Antire f l u xSu r g e ry.” Surgical En d o s c o py. September 2002.
15. “ El Camino Hospital 30 Years Later.” HIMSS2003 Pro c e e d i n g s .
16.“ Projects by Construction Phase in 2002.” Mo d e rn He a l t h c a re , Ma rch 2003.
E n d n o t e s
Related Documents










![The Drawing Tools (Level 2)the Drawing Tools Format tab is added to the Ribbon. 1. Move to the Insert tab and, in the Illustrations group, click on [Shapes] (in PowerPoint this button](https://static.cupdf.com/doc/110x72/5f782264933bb910d43c30e9/the-drawing-tools-level-2-the-drawing-tools-format-tab-is-added-to-the-ribbon.jpg)
