Diffusion-Weighted Hyperpolarized 129 Xe MRI in Healthy Volunteers and Subjects with Chronic Obstructive Pulmonary Disease S. Sivaram Kaushik 1,2,* , Zackary I. Cleveland 1,3 , Gary. P Cofer 1,3 , Gregory Metz 3 , Denise Beaver 3 , John Nouls 1,3 , Monica Kraft 4 , William Auffermann 3 , Jan Wolber 5 , H. Page McAdams 3 , and Bastiaan Driehuys 1,3 1 Center for In-Vivo Microscopy, Duke University Medical Center, Durham, NC, USA 2 Department of Biomedical Engineering, Duke University, Durham, NC, USA 3 Department of Radiology, Duke University Medical Center, Durham, NC, USA 4 Department of Pulmonary and Critical Care Medicine, Duke University Medical Center, Durham, NC, USA 5 GE Healthcare, The Grove Center, White Lion Rd, Amersham, UK Abstract 129 Xe apparent diffusion coefficient (ADC) MRI offers an alternative to 3 He ADC MRI, given its greater availability and lower cost. To demonstrate the feasibility of HP 129 Xe ADC MRI, we present results from healthy volunteers (HV), chronic obstructive pulmonary disease (COPD) subjects, and age-matched healthy controls (AMC). The mean parenchymal ADC was 0.036±0.003 cm 2 /s for HV, 0.043±0.006 cm 2 /s for AMC, and 0.056±0.008 cm 2 /s for COPD subjects with emphysema. In healthy individuals, but not the COPD group, ADC decreased significantly in the anterior-posterior direction by ~22% (p = 0.006, AMC; 0.0059, HV), likely due to gravity-induced tissue compression. The COPD group exhibited a significantly larger superior-inferior ADC reduction (~28%) than the healthy groups (~24%) (p = 0.00018 HV; p = 3.45×10 -5 AMC), consistent with smoking-related tissue destruction in the superior lung. Superior-inferior gradients in healthy subjects may result from regional differences in xenon concentration. ADC was significantly correlated with pulmonary function tests (FEV1, r=-0.77, p=0.0002; FEV1/FVC, r=-0.78, p=0.0002; DL CO /V A , r=-0.77, p=0.0002), and in healthy groups, increased with age by 0.0002 cm 2 /s/yr (r=0.56, p=0.02). This study shows 129 Xe ADC MRI is clinically feasible, sufficiently sensitive to distinguish HV from subjects with emphysema, and detects age and posture-dependent changes. Keywords Hyperpolarized 129 Xe MRI; apparent diffusion coefficient; chronic obstructive pulmonary disease; pulmonary function testing Introduction Chronic obstructive pulmonary disease (COPD) is characterized by slowly progressing irreversible airflow limitation (1). COPD affects roughly 12 million patients in the United * Corresponding Author: Bastiaan Driehuys, Center for In Vivo Microscopy, Box 3302, Duke University Medical Center, Durham, NC 27710, Phone (919) 684-7786, Fax (919) 684-7158, [email protected]. NIH Public Access Author Manuscript Magn Reson Med. Author manuscript; available in PMC 2012 May 14. Published in final edited form as: Magn Reson Med. 2011 April ; 65(4): 1154–1165. doi:10.1002/mrm.22697. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diffusion-Weighted Hyperpolarized 129Xe MRI in HealthyVolunteers and Subjects with Chronic Obstructive PulmonaryDisease
S. Sivaram Kaushik1,2,*, Zackary I. Cleveland1,3, Gary. P Cofer1,3, Gregory Metz3, DeniseBeaver3, John Nouls1,3, Monica Kraft4, William Auffermann3, Jan Wolber5, H. PageMcAdams3, and Bastiaan Driehuys1,3
1Center for In-Vivo Microscopy, Duke University Medical Center, Durham, NC, USA2Department of Biomedical Engineering, Duke University, Durham, NC, USA3Department of Radiology, Duke University Medical Center, Durham, NC, USA4Department of Pulmonary and Critical Care Medicine, Duke University Medical Center, Durham,NC, USA5GE Healthcare, The Grove Center, White Lion Rd, Amersham, UK
Abstract129Xe apparent diffusion coefficient (ADC) MRI offers an alternative to 3He ADC MRI, given itsgreater availability and lower cost. To demonstrate the feasibility of HP 129Xe ADC MRI, wepresent results from healthy volunteers (HV), chronic obstructive pulmonary disease (COPD)subjects, and age-matched healthy controls (AMC). The mean parenchymal ADC was0.036±0.003 cm2/s for HV, 0.043±0.006 cm2/s for AMC, and 0.056±0.008 cm2/s for COPDsubjects with emphysema. In healthy individuals, but not the COPD group, ADC decreasedsignificantly in the anterior-posterior direction by ~22% (p = 0.006, AMC; 0.0059, HV), likelydue to gravity-induced tissue compression. The COPD group exhibited a significantly largersuperior-inferior ADC reduction (~28%) than the healthy groups (~24%) (p = 0.00018 HV; p =3.45×10-5 AMC), consistent with smoking-related tissue destruction in the superior lung.Superior-inferior gradients in healthy subjects may result from regional differences in xenonconcentration. ADC was significantly correlated with pulmonary function tests (FEV1, r=-0.77,p=0.0002; FEV1/FVC, r=-0.78, p=0.0002; DLCO/VA, r=-0.77, p=0.0002), and in healthy groups,increased with age by 0.0002 cm2/s/yr (r=0.56, p=0.02). This study shows 129Xe ADC MRI isclinically feasible, sufficiently sensitive to distinguish HV from subjects with emphysema, anddetects age and posture-dependent changes.
KeywordsHyperpolarized 129Xe MRI; apparent diffusion coefficient; chronic obstructive pulmonary disease;pulmonary function testing
IntroductionChronic obstructive pulmonary disease (COPD) is characterized by slowly progressingirreversible airflow limitation (1). COPD affects roughly 12 million patients in the United
*Corresponding Author: Bastiaan Driehuys, Center for In Vivo Microscopy, Box 3302, Duke University Medical Center, Durham, NC27710, Phone (919) 684-7786, Fax (919) 684-7158, [email protected].
NIH Public AccessAuthor ManuscriptMagn Reson Med. Author manuscript; available in PMC 2012 May 14.
Published in final edited form as:Magn Reson Med. 2011 April ; 65(4): 1154–1165. doi:10.1002/mrm.22697.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

States, is the 4th leading cause of death in the United States and Europe (2), and is one of thefew common causes of death that continues to increase in incidence (3). Despite theassociated healthcare and economic burden, little progress has been made toward developingtreatments that significantly slow decline of lung function in COPD patients (3).Additionally, diagnosis is often made too late for simple interventions, such as smokingcessation, to meaningfully impact patient outcomes. This delay in diagnosis may beattributable to a variety of factors, including a) imprecise characterization of the origins ofairflow limitation, b) variable rates of disease progression, and c) the inability to observeand measure subtle changes in disease progression relative to treatment (4).
COPD describes a group of diseases (phenotypes) that include emphysema, bronchitis, andbronchiectasis. Moreover, multiple phenotypes can exist within a single individual. To treatand monitor COPD patients effectively, it will be necessary to assess the regional extent andseverity of each phenotype, and to determine the predominance of one over the others (5).To this end, thin-section computed tomography (CT) has been extensively investigated forthe radiologic evaluation of COPD (6). CT can identify regions of airspace tissue destruction(emphysema) by their low x-ray attenuation, often defined as less than −950 Houndsfieldunits, and CT has shown good correlation to histology (7). CT images acquired at end-expiration can be used to visualize air trapping, and airway wall thickening can be measuredin the first 6 generations (8). However, despite the power and high resolution achievablewith CT, the associated radiation dose constrains its use in asymptomatic patients and inlongitudinal follow-up studies (9), limiting its use for investigational purposes.
Hyperpolarized (HP) 3He MRI has emerged as a potentially powerful, noninvasive imagingmodality for diagnosis and evaluation of COPD (10). HP 3He MRI provides high-resolution(~ 3×3×10 mm3) images of ventilation, which permits areas of regional obstruction to bevisualized. Beyond static ventilation imaging, HP 3He MR contrast can be extended toreport on ventilation dynamics (11), regional oxygen partial pressure (12), and the apparentdiffusion coefficient (ADC) (12). Of these contrast mechanisms, the ADC is arguably themost well-developed and straight-forward to interpret. The principle of ADC MRI is thatdiffusion of 3He atoms in the lung is constrained by the size of the alveolar space. Hence,the 3He ADC measured in healthy lung is small [~0.25 cm2/s in healthy humans for typicalprotocols, (13)] compared to a large self-diffusion coefficient of 2 cm2/s. However, inregions of appreciable emphysematous tissue destruction, the ADC becomes elevated,eventually reaching a maximum value consistent with the free-diffusion of 3He in air (~0.8cm2/s). By contrast, ADC would not be expected to increase if airflow limitation was causedby an airway-predominant disease such as bronchitis.
Since the introduction of 3He ADC (14,15) in small animal models of emphysema,considerable progress has been reported. In addition to revealing emphysema in patientswith known COPD, 3He ADC shows early emphysema-like changes in asymptomaticsmokers (16) and in individuals exposed to second-hand smoke (17). The relation of ADC toalveolar size has been demonstrated by its sensitivity to postural gradients (18) and age-related changes in alveolar size (19). 3He ADC MRI has proven highly reproducible inrepeated studies (20) and has shown ability to image disease progression in individualsubjects (21). Recently, 3He ADC was put on a firm theoretical footing by Yablonskiyi etal., who demonstrated the ability to extract accurate airspace dimensions from the ADCmeasurement (22). 3He ADC has been compared clinically to CT, and these studies suggestthat it correlates more strongly with DLCO (Diffusing capacity of carbon monoxide in thelung) than the CT-based metrics (23). Unfortunately, the scarcity of 3He and its rapidlyincreasing cost have severely limited the broader dissemination of HP 3He MRI.
Kaushik et al. Page 2
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
The limitations of 3He have made clear the need to transition to HP 129Xe MRI, the supplyof which is unconstrained. 129Xe MRI has improved considerably (24), since the first humanventilation imaging was demonstrated (25), and additional contrast mechanisms are madepossible by its solubility in tissues and its large (>200 ppm) in vivo chemical shift(24,25). 129Xe MRI has also been implemented with diffusion-weighting (14), and Mugleret al. first demonstrated 129Xe ADC in healthy human volunteers (26), which was followedup by Sindile et al (27). While Mata et al. demonstrated that 129Xe ADC becomes elevatedin an elastase-model of emphysema in rabbits (28), no reports have been published of 129XeADC measurements in patients with COPD. Therefore, the aim of this study was to assessthe clinical feasibility of 129Xe ADC MRI and apply it in a population of healthy volunteers,COPD subjects, and age-matched control subjects. We report a detailed analysis of ADCtrends with disease, age, and posture, and correlate the ADC values with conventionalpulmonary function testing.
MethodsSubject Inclusion/Exclusion Criteria
Studies were conducted under the GE Healthcare Investigational New Drug (IND) as part ofa Phase I clinical trial for hyperpolarized 129Xe MRI, and studies were approved by theDuke University Medical Center (DUMC) Institutional Review Board (IRB). Writteninformed consent was obtained from the volunteers and subjects prior to enrollment.Subjects were excluded if they were pregnant or lactating; had a history of asthma, allergy,or hypersensitivity that affects the pulmonary function; had a history of cardiac arrhythmias;or had a respiratory illness (or exacerbation for COPD subjects) within 30 days of imaging.
The study consisted of a technical run-in phase for pulse-sequence development followed byan efficacy phase using a fixed version of each sequence. During the run-in phase, a groupof healthy volunteers (HV) (3 men, 4 women, mean age = 32.9 ± 11.3 years) underwent thesame version of the 129Xe ADC MRI protocol that was used during the efficacy phase (withminor differences in b-values), and hence, these subjects are included as part of this report.These subjects met the same inclusion/exclusion criteria as the age-matched control subjects(see below), except they did not undergo pulmonary function testing.
For the efficacy phase, 1 subject with GOLD Stage I, 8 subjects with GOLD Stage II, and1 subject with GOLD Stage III COPD were recruited from a population of patients whohad a smoking history of at least 20 pack-years (7 men, 3 women; mean age = 65.9 ± 7.1years). Given the relatively small population, Stage II patients were primarily selected toensure observing a reasonable, but not overly variable, degree of pathology. The Stage IICOPD subjects had a forced expiratory volume in 1 second (FEV1) between 50 and 80%,FEV1/FVC (forced vital capacity) of less than 70%. They had a single-breath carbonmonoxide diffusing capacity (DLCO) of less than 70% of the predicted value. The Stage Isubject had an FEV1 that was 81% of predicted and the Stage III subject had an FEV1 thatwas 35% of predicted, as seen in Table 1. All COPD subjects had a chest x-ray or CT scanon file, with 8 out of 10 exhibiting evidence of emphysema, as determined by a boardcertified radiologist (HPM).
In addition, 10 age-matched healthy controls (AMC) were enrolled (4 men, 6 women,mean age = 62.9 ± 7.6 years). These subjects each had a smoking history of less than 5pack-years and had not smoked for at least 5 years prior to participating in the study.Volunteers typically had an FEV1 and DLCO that were both greater than 80% of thepredicted value and an FEV1/FVC that was greater than 70%. All pulmonary function
Kaushik et al. Page 3
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

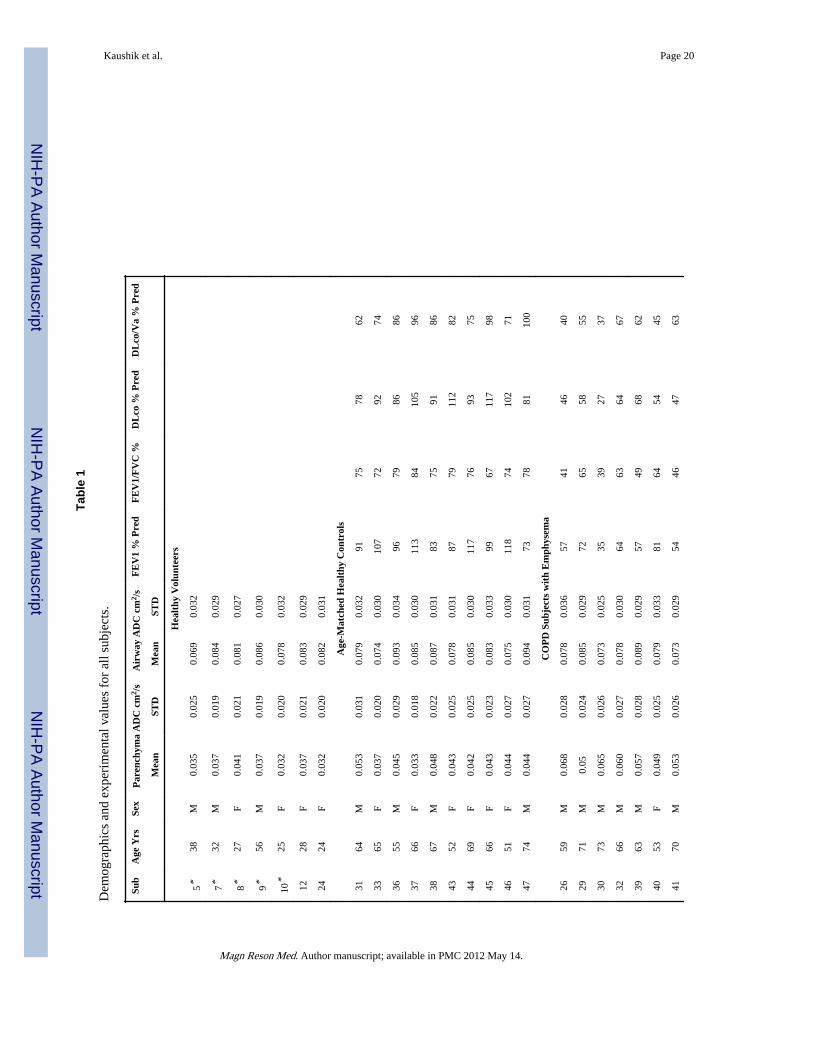
testing was conducted within one week of 129Xe MRI. Table 1 provides a complete list of allthe PFT data for all subjects.
129Xe Polarization and DeliveryIsotopically enriched (83% 129Xe, Spectra Gases Inc., Alpha, NJ) xenon was polarized to5-10% by rubidium vapor spin exchange optical pumping and cryogenically accumulated(29) in 1-L doses over 1 hour using a prototype commercial polarizer (GE Healthcare,Durham NC). Following accumulation, HP 129Xe was immediately thawed into a Tedlar bag(Jensen Inert Products, Coral Springs FL). 129Xe polarization was then measured in aprototype 129Xe polarization measurement station (GE Healthcare). With the subjects lyingsupine, HP 129Xe was then administered from the Tedlar bag through 0.95-cm innerdiameter Tygon tubing (Saint-Gobain Performance Plastics, Akron, OH). Each subjectreceived a 1-L 129Xe dose regardless of lung volume, with inspiration commencing afterexhaling to a lung volume estimated to be between residual volume (RV) and functionalresidual capacity (FRC). Imaging started within 1-2 seconds of the subject inhaling thecontents of the bag. For each 129Xe dose, the subject’s subjects’ blood pressure, heart rate,and oxygen saturation level were continuously measured using a Datex-Ohmeda monitoringsystem (GE Healthcare, Helsinki, Finland).
Hyperpolarized 129Xe ImagingImaging was performed using a 1.5 T Excite 14M5 MRI scanner (GE Healthcare,Milwaukee WI) and a quadrature vest coil (Clinical MR Solutions, Brookfield, WI) tuned tothe 17.66 MHz 129Xe resonance frequency and proton blocked to enable localizing andshimming using the body coil of the scanner. Diffusion-weighted HP 129Xe images wereacquired in the coronal plane using a multi-slice spoiled gradient recalled echo (SPGR)sequence (field of view = 40 cm, slice thickness = 15 mm, matrix = 64×64, bandwidth =15.6 kHz, TE/TR = 9.3/12 ms and flip angle = 5.1°). Diffusion weighting was achievedusing bipolar gradients (amplitude = 3.2 G/cm, ramp time = 500 μs, and pulse width = 2.4ms), having a b-value (30) of 12 s/cm2. This b-value was used for all subjects except for 5healthy volunteers, who received a slightly longer sensitizing gradient pulse width of 2.9 ms,resulting in a b-value of 18.76 s/cm2. For each diffusion-weighted image, an accompanyingunweighted image was acquired in an interleaved fashion to enable pixel-wise ADC valuesto be calculated from the two images. The total acquisition time was limited by the protocolto 16 seconds, thus restricting the number of slices to 10. As a result, the most anterior andmost posterior slices of the lung were generally not scanned.
Source Image ProcessingThe images were interpolated by the reconstruction algorithm of the scanner from a 64×64to a 256×256 matrix and saved in DICOM format. These images were then imported intoMATLAB™ (The MathWorks, Inc., Natick, MA) to generate the ADC maps. To ensure thatADC calculations were made only on pixels corresponding to ventilated lung, severalprocessing steps were applied to the source images. First, the non-diffusion weighted (b = 0)images were used to generate binary masks of each slice, using a threshold derived from themean of the background noise plus twice its standard deviation. The background noise wasdetermined from a 200×50-pixel region outside the lungs, which provided reproduciblenoise measurements regardless of its placement.
The relatively low threshold caused numerous islands of background noise to be retained inthe mask. These islands were removed by an ‘erosion’ operation, which was followed by a‘dilation’ operation to restore mask features belonging to ventilated lung, but lost duringerosion. Erosion (Θ) of a binary image, A, by a smaller structuring element, B, ismathematically defined as (31)
Kaushik et al. Page 4
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

[1]
where z = (z1, z2) is the coordinate within the image space and BZ represents a translation ofa symmetric structuring element across the image by one pixel at a time. B is chosen to besmall compared to the primary image features, but large compared to the spatial scale of theimage noise. Erosion of A by B thus results in the subset of points in A upon which thecenter of B can be placed such that all the pixels in B overlap only with pixels of value 1,thus removing noise of a size smaller than B. Following erosion, dilation (⊕) issubsequently used to restore the size of image A using the same structuring element Baccording to (31)
[2]
If the center of the structuring element falls on top of a pixel with value = 1, the pixel isdilated, meaning that all the neighboring pixels encompassed by the structuring element arereplaced by 1.
To assist in choosing an appropriately sized structuring element for erosion/dilation, thesource images from several representative subjects in the HV, AMC, and COPD groupswere also manually segmented to delineate the ventilated lung from the background. Theresulting masks were applied to the source images and their ADC maps were calculated,along with the mean ADC and its standard deviation. These maps were then compared withthose obtained by automatic segmentation using erosion/dilation with different sizedstructuring elements. These comparisons showed a circular structuring element with a 3-pixel radius to provide results identical to manual segmentation (see Results), and, therefore,this element was used to erode/dilate the masks for all subjects.
ADC CalculationThe ADC value of each pixel was calculated from the segmented source images accordingto
[3]
where S is the signal intensity of the diffusion weighted image pixel, and S0 is the intensityof the pixel without weighting. The resulting ADC maps were further processed by rejectingany pixels with a value outside the interval 0 ≤ ADC ≤ 0.14 cm2/s. The 0.14 cm2/s cutoffwas chosen because it corresponds to the expected free diffusion coefficient of xenon innitrogen at infinite dilution and 37 °C (32). Finally, since 129Xe diffusion in the visibleairways is largely unrestricted (14), the airways were manually segmented out of the maps,such that ADC values for the airways and the distal lung parenchyma were calculatedseparately.
ADC maps were further analyzed for spatial gradients in the anterior-posterior and superior-inferior direction. ADC gradients in the anterior-posterior direction were calculated byplotting the average ADC for each of the ten slices and calculating the slope. ADC gradientsin the superior-inferior direction were calculated by dividing each lung into 3 strips of equalheight and using the mean ADC of each region to derive a corresponding slope.
Statistical AnalysisLinear regression analysis was used to test for correlations between ADC and pulmonaryfunction tests, as well as ADC and age, and these were reported using Pearson’s correlation
Kaushik et al. Page 5
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

coefficient. The mean ADCs of each subject group were tested for statistical significanceusing the Wilcoxon Rank Sum test. This test was chosen rather than the Student’s t-test,because a Bartlett test of our data showed unequal variances between groups. The Wilcoxontest was also used to establish statistical significance of the anterior-posterior and superior-inferior ADC gradients observed in the maps.
ResultsSubject Response to HP 129Xe
The 129Xe ADC imaging procedure was well-tolerated and the exam was completed by allsubjects without incident. No clinically significant changes in vital signs were observedduring the imaging exam. However, a large fraction of subjects (91%) did report transientxenon-related effects for at least one xenon dose, including dizziness, paraesthesia, andeuphoria, all of which resolved within 2-3 minutes without clinical intervention. A detailedreport documenting all the xenon safety testing, vital signs monitoring, and laboratorytesting conducted will be presented in a forthcoming manuscript.
Effect of Image ProcessingThe signal-to-noise ratio (SNR) in 129Xe MRI is generally lower than that achieved for 3HeMRI. In this work, the unweighted images had a mean SNR of 15.21±4.74 versus 9.41±2.98for the weighted images. Therefore, several imaging processing steps were employed toeliminate noise in regions of the image outside the lungs. Figure 1A shows the maskobtained using a simple thresholding procedure that retains much of the background noise,which, if propagated, would contribute meaningless values to the ADC maps. When thismask was eroded with a circular structuring element of 3-pixel radius (Figure 1B), most ofthe discontinuous noise was eliminated, but some structural features in the mask were alsolost, particularly the major airways. However, as is seen in Figure 1C, subsequent dilationrestores most of these structural features. The choice of a structuring element with 3-pixelradius was established because the resulting ADC maps provided the best correspondence tothose obtained with masks derived by manual segmentation as illustrated in Figure 2. Forthis example, the mean parenchymal ADC of a healthy subject obtained using a thresholdmask without erosion/dilation or further manual segmentation was 0.041±0.026 cm2/s. Bycontrast, manual segmentation reduced the mean parenchymal ADC to 0.037±0.021 cm2/swhile erosion/dilation using a 3-pixel radius structuring element generated the same result(ADC = 0.037±0.021 cm2/s).
129Xe ADC in the Three Subject GroupsFigure 3 displays representative ADC maps from individuals in each of the three subjectgroups. Figure 3A shows the ADC map from a HV (age = 28 years) with a meanparenchymal ADC of 0.037±0.021 cm2/s, which is significantly smaller than the self-diffusion coefficient of pure xenon (0.06 cm2/s) (14), indicating that confinement by thelung microstructure restricts the diffusion of xenon. In this healthy volunteer, the mean ADCin the airways, where 129Xe experiences nearly free diffusion (14), was 0.083±0.029 cm2/s.This value actually exceeds the self-diffusion coefficient of pure xenon, indicating somedegree of dilution with the lighter pulmonary gases such as nitrogen and oxygen occurred.The ADC values in this subject exhibit a narrow distribution, as seen in the correspondinghistogram. Figure 3B shows the ADC map of an older AMC subject (age = 69 years), with aslightly higher, but still relatively low, mean parenchymal ADC (0.042±0.025 cm2/s) and anarrow ADC distribution in the histogram. By contrast, Figure 3C shows the ADC map of aStage II COPD subject (age = 59 years) with a substantially higher mean (0.068±0.028 cm2/s), reflecting enlarged airspaces. The ADC measurements for all subjects in this study aresummarized in Table 1.
Kaushik et al. Page 6
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

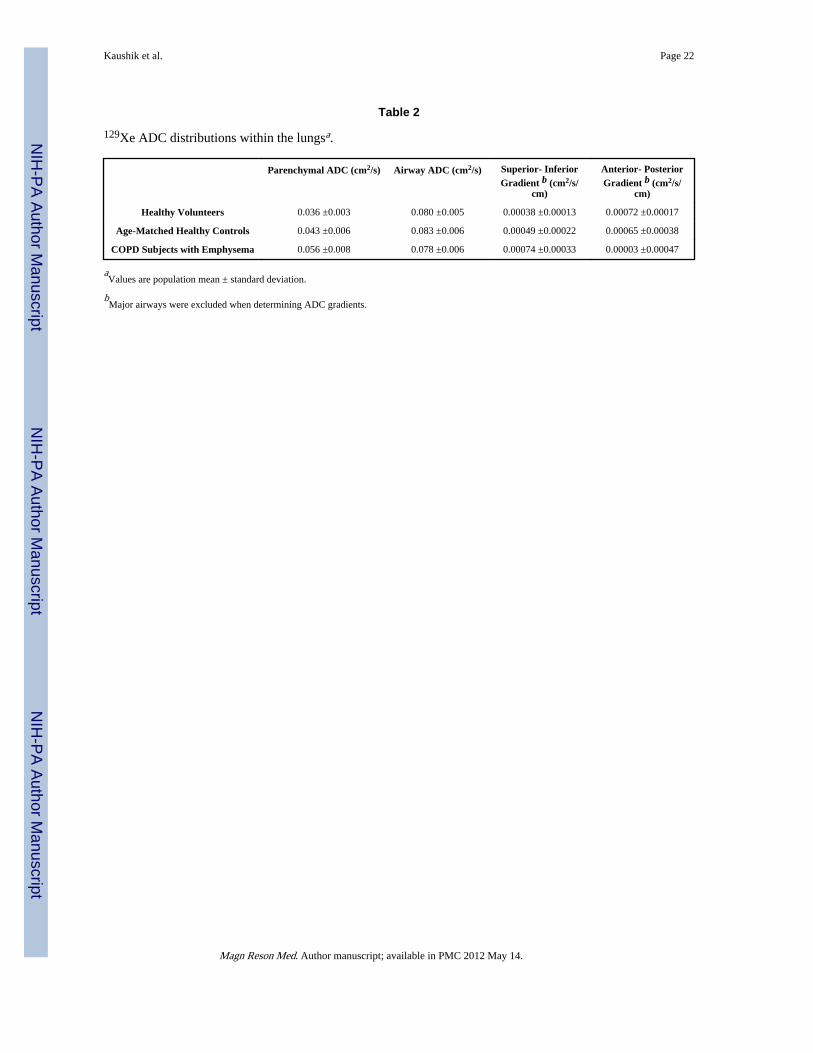
The mean parenchymal ADC from each of the three subject groups is summarized in Table2 and graphed in Figure 4. As a group, the HVs had a mean ADC of 0.036±0.003 cm2/s,which is significantly lower than that of the AMC (0.043±0.006 cm2/s; p = 0.0046), whichin turn was significantly lower than that of the COPD subjects (0.056±0.008 cm2/s, p =0.0021). Additionally, the mean ADC of the COPD subjects with emphysema wassignificantly elevated compared to that of the HV (p = 0.0003). Note that this mean for theCOPD group excludes the two COPD patients who had no evidence of emphysema on theirCT scans. Indeed, these two subjects showed mean parenchymal ADCs of 0.036±0.021 cm2/s and 0.039±0.022 cm2/s, which are below the mean ADC for the AMC and the subjectswith emphysema. For all three groups, the mean airway ADC was ~0.08 cm2/s, and asexpected for a gases experiencing nearly free diffusion, there was no significant differencein airway ADC between the three groups.
ADC Gradients and CorrelationsEach of the subjects depicted in Figure 3 exhibit noticeable gradients in the ADC valueswith higher ADC observed in the apex relative to the base of the lungs. These superior-inferior gradients are well illustrated in the full ADC maps of a healthy volunteer depicted inFigure 5. These gradients, which produced a ~24% higher ADC in the apex relative to thebase for the two healthy groups (p = 0.00018, HV; p = 3.45×10-5, AMC), are consistent withthose observed for all the groups as shown in Figure 6A.
The superior-inferior gradient was larger (p = 0.024) for the COPD subjects withemphysema (0.00074±0.00033 cm2/s/cm) than for the AMCs (0.00049±0.00022 cm2/s/cm),which in turn was larger, though not significantly larger (p = 0.09), than the HVs(0.00038±0.00013 cm2/s/cm). The strong superior-inferior ADC gradient in the COPDsubjects is indicative of greater smoking-induced tissue destruction in the upper lobes of thelung, which has also been reported in the CT (33), pathology (34), and 3He MRI literature(13).
Figure 5 also shows a clear trend towards higher ADC values in the more anterior imageslices. Such anterior-posterior ADC gradients are clearly present in both of the healthygroups, but this gradient was negligible in the COPD subjects with emphysema. Asillustrated in Figure 6B, the average anterior-posterior ADC gradients for the HVs were0.00072±0.00017 cm2/s/cm and 0.00065±0.00038 cm2/s/cm for the AMCs, but were nearlyabsent (0.00003±0.00047 cm2/s/cm) for the COPD subjects with emphysema. Thisdifference was statistically significant relative to both the HV group (p = 0.014) and theAMC group (p = 0.0085).
For the COPD and AMC subjects, the mean parenchymal ADC was correlated with threepulmonary function metrics — DLCO/VA, FEV1, and FEV1/FVC. As illustrated in Figure7A-C, the mean parenchyma ADC was moderately, yet significantly, correlated with allthree metrics (FEV1 and DLCO/VA expressed as percent predicted values). The meanparenchyma ADC also showed a significant correlation with the absolute DLCO/VA (mL/mHg/min/L) values (r = -0.77, p = 0.0002) but not with the absolute FEV1. As shown inFigure 7D, the mean ADC for the HVs and AMCs also increased with age (r = 0.56, p =0.02), with a slope of 0.0002 cm2/s per year.
DiscussionDiffusion-weighted MRI using 129Xe MRI poses numerous challenges compared tousing 3He. The nearly three-fold lower gyromagnetic ratio (γ) of 129Xe and lowerpolarization achieved in our setting contributed to the low image SNR. Moreover, the lowerdiffusivity of 129Xe relative to 3He requires that a larger b-value be applied to achieve
Kaushik et al. Page 7
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

sufficient weighting to derive meaningful ADC calculations. Because the b-value also scaleswith γ2 (30), sufficiently large b-values could only be attained using relatively longdiffusion weighting pulses. For this study, the 2.4 ms pulse durations required, resulted inminimum echo times of 8.3 ms, which contributes unwanted T2*-weighting. These factorscombined to create a significant SNR challenge and led us to introduce several processingsteps to calculate 129Xe ADC values only for pixels belonging to ventilated lung. Thisinvolved first creating a rough lung mask by applying a relatively low threshold, andrefining the mask using erosion/dilation to remove residual background noise. This approachgave similar ADC results as when masks were generated by manual segmentation and havethe advantage of being objective and fast. However, a disadvantage of the erosion/dilationtechnique is that it could erroneously remove isolated areas of ventilation smaller than thestructuring element. Of course, the need for image processing would be substantiallyreduced by improving the relatively modest 129Xe polarization (5-10%) available in thisstudy. Considering that liter-quantities of HP 129Xe with polarizations approaching 50%have recently been demonstrated (35), achieving better ADC map fidelity through improvedimage SNR appears promising.
Besides lower SNR, 129Xe differs from 3He in that xenon diffuses into the capillary blood-stream (24), which could decrease 129Xe concentration during imaging. Assuming an initialalveolar xenon concentration of 20% after inhalation, its solubility of ~15% in the blood,combined with a cardiac output of ~80 ml/sec would reduce the alveolar concentration toabout 19.2% during a 16 second breath-hold. This change in concentration is expected toincrease the xenon self-diffusion coefficient by only 0.9%. Given that any difference indiffusion will be further reduced by confinement, the influence of xenon solubility on theADC is expected to be negligible.
The mean parenchymal 129Xe ADC values of 0.036 cm2/s for HVs agrees well with thepreliminary values of 0.039 and 0.036 cm2/s reported by Mugler et al. (26) and 0.04 cm2/sreported by Sindile et al. (27). Even with this relatively small sample of 17 healthy subjects(7 HVs and 10 AMCs), 129Xe ADC shows an increase with age. The age-related change canbe compared to the annual 3He ADC change of 0.0015 cm2/s/yr reported by Fain et al. (19)by considering the predicted ADC for a single subject age. The predicted 3He ADC at for ahealthy subject at age 25 is 0.1875 cm2/s, which gives a 3He ADC slope of 0.8% per year.From our data, the predicted 129Xe ADC at age 25 is 0.0363 cm2/s, giving a 129Xe ADCslope of 0.6% per year. Moreover, the mean 129Xe ADC correlates relatively well withpulmonary function testing, which is again similar to the trend seen for the 3He ADC (13).The correlation of 129Xe ADC with FEV1/FVC (r = -0.78) is slightly weaker than thatreported for 3He ADC [r = -0.97, (13)]. Additionally, the standard deviation of the 129XeADC did not correlate well with pulmonary function metrics, whereas such correlationshave been reported for 3He ADC (13). This difference may be attributable to the substantialsuperior-inferior ADC gradients seen with 129Xe, which broadens the ADC distribution evenin the absence of disease.
Although the mean ADC metric was effective in separating the three subject groups inaggregate, there was some overlap between the subjects with emphysema and the healthyvolunteers. These deviations could result from different degrees of 129Xe dilution into lungvolumes (discussed below). However, similarly overlapping mean ADC data have beenreported in asymptomatic smokers (16) and emphysema patients (13,36) in the 3He MRIliterature, suggesting that natural individual-to-individual variations in lung microstructurecould also play a role.
The ADC gradients seen in the anterior-posterior direction in healthy subjects areattributable to gravity-dependent compression of the lung airspaces (37). Compression in the
Kaushik et al. Page 8
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

dependent lung is caused by the weight of the lung itself (37), with additional contributionsfrom the weight of the heart (38). Thus, in the healthy lung smaller ADC values (smalleralveolar size) are expected in the dependent lung compared to the non-dependent lung. Thisobserved trend is similar to that reported by Fichele et al. using 3He ADC (39). However,the near absence of anterior-posterior ADC gradients in the COPD subjects with emphysemamay suggest that the heterogeneity of emphysematous tissue destruction could negate theinfluence of gravity. The reduction of the anterior-posterior gradient has also been attributedto a decrease in the compressibility of the lung tissue due to COPD (18). A similarly smallanterior-posterior gradient was seen by Diaz et al., using 3He ADC (36). The superior-inferior gradient we observed in the HVs and AMCs corresponded to an average ADCreduction of 23.5%, which is significantly smaller (p = 0.00018, HV; p=3.45×10-5, AMC)than the 28.1% observed in the COPD subjects with emphysema, but still quite substantial.
We suggest that the higher 129Xe ADC we observed in the superior lung may resultfrom 129Xe dilution effects. This conclusion is driven by reports suggesting that supinesubjects exhibit a larger functional residual capacity (FRC) in the superior lung relative tothe inferior lung (40). This greater residual volume will more fully dilute the inhaled 129Xein the superior lung, thereby producing larger xenon diffusion constants in this region. Thissuperior-inferior gradient, which we note is the opposite of that reported by Sindile et al.(27), cautions that 129Xe ADC, while sensitive to microstructure, is also affected by 129Xedilution in lighter alveolar gases. 129Xe dilution could lead to erroneously high ADC valuesin regions of air trapping, which would admit very little xenon per breath. Such regions ofhigh dilution could potentially be identified as those with very low SNR on the b = 0images. Alternatively, the effect of 129Xe dilution on 129Xe ADC could provide a novelmeans to quantify regional fractional ventilation.
This study did have several limitations that could affect the precision of the results. First, theneed for simplified logistics in this first clinical trial required that the inhaled 129Xe volumeremain fixed at 1 liter for all subjects regardless of their total lung capacity. Hence, subjectswith smaller resting lung volumes would experience more alveolar expansion, perhapsslightly elevating the resulting 129Xe ADC (36). However, smaller residual volumes ofalveolar gas will result in less dilution of the inhaled 129Xe, which will have the oppositeeffect on the ADC. Further work, in which inhaled volume is adjusted to the subject totallung capacity (TLC) (36), will be required to fully elucidate the interplay of these twoeffects. Also, the starting lung volume for subjects was only loosely controlled to liebetween RV and FRC. Better control of initial lung volume, would likely improvereproducibility, particularly of the ADC gradients, which may be eliminated when lungvolumes reach closer to TLC (41). Similarly future 129Xe studies will use a consistent b-value for all subjects, rather than the two that were used here. Hence, while this small trialhad certain limitations, and does not definitively cement the diagnostic utility of 129XeADC, the preliminary results are encouraging.
ConclusionsThis work showed that despite the lower gyromagnetic ratio, polarization, and free-diffusionof 129Xe relative to 3He, hyperpolarized 129Xe ADC maps can be obtained in humansubjects in a clinically feasible manner. The associated lower SNR of 129Xe images requirescareful segmentation of the lung from background noise, which we have accomplished usinga thresholded mask in conjunction with erosion/dilation operations. The resulting 129XeADC maps exhibit sufficient dynamic range to distinguish subjects with emphysema fromage-matched control subjects, and younger healthy subjects. The mean ADC exhibits amoderate, yet significant correlation with pulmonary function tests, similar to what has been
Kaushik et al. Page 9
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
reported for 3He ADC. Moreover, the 129Xe ADC is sufficiently sensitive to reveal itsdependence on changes in pulmonary microstructure due to subject age.
Taken together, the results reported in this work indicate that 129Xe holds promise forreplacing the scarcely available 3He for generating pulmonary ADC measurements. 129XeADC holds promise for the detection and characterization of early emphysematous changesin the lung, and in conjunction with ventilation analysis (5) could serve as a means to non-invasively phenotype and monitor the treatment of subjects with COPD.
AcknowledgmentsThe authors wish to thank Jerry Dahlke (GE Healthcare) for assistance with the MR hardware; Kevin Kelly(Radiation Oncology, Duke University) for performing proton imaging; Sean Fain (University of Wisconsin-Madison) for supplying the SPGRE sequence used in this work; Christine Willis and Rafael Firszt (Duke UniversityMedical Center) for subject monitoring; and from the Center for In Vivo Microscopy, Alexandra Badea for thehelpful discussion regarding the image processing and statistics; and Sally Zimney for carefully proofreading themanuscript. This work was funded by GE Healthcare, with additional support from the Duke Center for In VivoMicroscopy, an NIH/NCRR National Biomedical Technology Research Center (P41 RR005959), and NHLBI R21HL087094.
References1. Celli BR, Macnee W. Standards for the diagnosis and treatment of patients with COPD: A summary
of the ATS/ERS position paper. Eur Resp J. 2004; 23:932–946.
2. Makita H, Nasuhara Y, Nagai K, Ito Y, Hasegawa M, Betsuyaku T, Onodera Y, Hizawa N,Nishimura M. Characterisation of phenotypes based on severity of emphysema in chronicobstructive pulmonary disease. Thorax. 2007; 62:932–937. [PubMed: 17573447]
3. Hurd S. The impact of COPD on lung health worldwide - Epidemiology and incidence. Chest. 2000;117:1S–4S. [PubMed: 10673465]
4. Cazzola M, MacNee W, Martinez FJ, Rabe KF, Franciosi LG, Barnes PJ, Brusasco V, Burge PS,Calverley PMA, Celli BR, Jones PW, Mahler DA, Make B, Miravitlles M, Page CP, Palange P, ParrD, Pistolesi M, Rennard SI, Molken M, Stockley R, Sullivan SD, Wedzicha JA, Wouters EF.Outcomes for COPD pharmacological trials: From lung function to biomarkers. Eur Resp J. 2008;31:416–468.
5. Mathew L, Kirby M, Etemad-Rezai R, Wheatley A, McCormack DG, Parraga G. Hyperpolarized3He Magnetic Resonance imaging: Preliminary evaluation of phenotyping potential in chronicobstructive pulmonary disease. Eur J Radiol. 2009 In press.
6. Park KJ, Bergin CJ, Clausen JL. Quantitation of emphysema with three-dimensional CTdensitometry: Comparison with two-dimensional analysis, visual emphysema scores, andpulmonary function test results. Radiology. 1999; 211:541–547. [PubMed: 10228540]
7. Thurlbeck WM, Muller NL. Emphysema - Definition, imaging and quantification. Am JRoentgenol. 1994; 163:1017–1025. [PubMed: 7976869]
8. Lee YK, Oh YM, Lee JH, Kim EK, Kim N, Seo JB, Do Lee S. Quantitative assessment ofemphysema, air trapping, and airway thickening on computed tomography. Lung. 2008; 186:157–165. [PubMed: 18351420]
9. Smith-Bindman R, Lipson J, Marcus R, Kim KP, Mahesh M, Gould R, de Gonzalez AB, MigliorettiDL. Radiation dose associated with common computed tomography examinations and theassociated lifetime attributable risk of cancer. Arch Intern Med. 2009; 169:2078–2086. [PubMed:20008690]
10. Kauczor HU, Ebert M, Kreitner KF, Nilgens H, Surkau R, Heil W, Hofmann D, Otten EW, ThelenM. Imaging of the lungs using 3He MRI: Preliminary clinical experience in 18 patients with andwithout lung disease. J Magn Reson Imaging. 1997; 7:538–543. [PubMed: 9170039]
11. Holmes JH, O’Halloran RL, Brodsky EK, Jung Y, Block WF, Fain SB. 3D hyperpolarized He-3MRI of ventilation using a multi-echo projection acquisition. Magn Reson Med. 2008; 59:1062–1071. [PubMed: 18429034]
Kaushik et al. Page 10
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

12. Yu JS, Law M, Kadlecek S, Emami K, Ishii M, Stephen M, Woodburn JM, Vahdat V, Rizi RR.Simultaneous measurement of pulmonary partial pressure of oxygen and apparent diffusioncoefficient by hyperpolarized He-3 MRI. Magn Reson Med. 2009; 61:1015–1021. [PubMed:19230017]
13. Salerno M, de Lange EE, Altes TA, Truwit JD, Brookeman JR, Mugler JP. Emphysema:Hyperpolarized helium 3 diffusion MR imaging of the lungs compared with spirometric indexes -Initial experience. Radiology. 2002; 222:252–260. [PubMed: 11756734]
14. Chen XJ, Moller HE, Chawla MS, Cofer GP, Driehuys B, Hedlund LW, Johnson GA. Spatiallyresolved measurements of hyperpolarized gas properties in the lung in vivo. Part I: Diffusioncoefficient. Magn Reson Med. 1999; 42:721–728. [PubMed: 10502761]
15. Chen XJ, Hedlund LW, Moller HE, Chawla MS, Maronpot RR, Johnson GA. Detection ofemphysema in rat lungs by using magnetic resonance measurements of He-3 diffusion. Proc NatlAcad Sci U S A. 2000; 97:11478–11481. [PubMed: 11027348]
16. Fain SB, Panth SR, Evans MD, Wentland AL, Holmes JH, Korosec FR, O’Brien MJ, Fountaine H,Grist TM. Early emphysematous changes in asymptomatic smokers: Detection with He-3 MRimaging. Radiology. 2006; 239:875–883. [PubMed: 16714465]
17. Wang C, Mugler JP, De Lange EE, Shim Y, Altes TA. Healthy nonsmokers exposed regularly tosecondhand smoke have evidence of lung injury detected by hyperpolarized-3 diffusion MRI. AmJ Respir Crit Care Med. 2010; 181:A5438.
18. Evans A, McCormack D, Ouriadov A, Etemad-Rezai R, Santyr G, Parraga G. Anatomicaldistribution of He-3 apparent diffusion coefficients in severe chronic obstructive pulmonarydisease. J Magn Reson Imaging. 2007; 26:1537–1547. [PubMed: 17968961]
19. Fain SB, Altes TA, Panth SR, Evans MD, Waters B, Mugler JP, Korosec FR, Grist TM, SilvermanM, Salerno M, Owers-Bradley J. Detection of age-dependent changes in healthy adult lungs withdiffusion-weighted He-3 MRI. Acad Radiol. 2005; 12:1385–1393. [PubMed: 16253850]
20. Stavngaard T, Sogaard LV, Batz M, Schreiber LM, Dirksen A. Progression of emphysemaevaluated by MRI using hyperpolarized He-3 (Hp He-3) measurements in patients with alpha-1-antitrypsin (A1AT) deficiency compared with CT and lung function tests. Acta Radiol. 2009;50:1019–1026. [PubMed: 19863412]
21. Kirby M, Mathew L, Wheatley A, Santyr GE, McCormack DG, Parraga G. Chronic obstructivepulmonary disease: Longitudinal hyperpolarized He-3 MR imaging. Radiology. 2010; 256:280–289. [PubMed: 20574101]
22. Yablonskiy DA, Sukstanskii AL, Woods JC, Gierada DS, Quirk JD, Hogg JC, Cooper JD, ConradiMS. Quantification of lung microstructure with hyperpolarized He-3 diffusion MRI. J ApplPhysiol. 2009; 107:1258–1265. [PubMed: 19661452]
23. Diaz S, Casselbrant I, Piitulainen E, Magnusson P, Peterson B, Wollmer P, Leander P, Ekberg O,Akeson P. Validity of apparent diffusion coefficient hyperpolarized He-3-MRI using MSCT andpulmonary function tests as references. Eur J Radiol. 2009; 71:257–263. [PubMed: 18514455]
24. Cleveland ZI, Cofer GP, Metz G, Beaver D, Nouls JC, Kaushik SS, Kraft M, Wolber J, Kelly KT,McAdams HP, Driehuys B. Hyperpolarized 129Xe MR imaging of alveolar gas uptake in humans.PLoS ONE. 2010; 5:e12192. [PubMed: 20808950]
25. Mugler JP, Driehuys B, Brookeman JR, Cates GD, Berr SS, Bryant RG, Daniel TM, deLange EE,Downs JH, Erickson CJ, Happer W, Hinton DP, Kassel NF, Maier T, Phillips CD, Saam BT, SauerKL, Wagshul ME. MR imaging and spectroscopy using hyperpolarized Xe-129 gas: Preliminaryhuman results. Magn Reson Med. 1997; 37:809–815. [PubMed: 9178229]
26. Mugler, JP.; Mata, JF.; Wang, HTJ.; Tobias, WA.; Cates, GD.; Christopher, JM.; Missel, JL.;Reish, AG.; Ruppert, K.; Brookeman, JR.; Hagspiel, KD. The apparent diffusion coefficient of129-Xe in the lung: Preliminary human results. Proceedings of the 12th Annual Meeting ofISMRM; Kyoto, Japan. 2004.
27. Sindile, A.; Muradian, I.; Hrovat, MI.; Johnson, DC.; Hersman, FW.; Patz, S. Human pulmonarydiffusion weighted imaging at 0.2T with hyperpolarized 129Xe. Proceedings of 15th AnnualMeeting of the ISMRM; Berlin, Germany. 2007. p. 1290
28. Mata JF, Altes TA, Cai J, Ruppert K, Mitzner W, Hagspiel KD, Patel B, Salerno M, BrookemanJR, de Lange EE, Tobias WA, Wang HTJ, Cates GD, Mugler JP. Evaluation of emphysema
Kaushik et al. Page 11
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

severity and progression in a rabbit model: Comparison of hyperpolarized He-3 and Xe-129diffusion MRI with lung morphometry. J Appl Physiol. 2007; 102:1273–1280. [PubMed:17110518]
29. Driehuys B, Cates GD, Miron E, Sauer K, Walter DK, Happer W. High-volume production oflaser-polarized Xe-129. Appl Phys Lett. 1996; 69:1668–1670.
30. Yablonskiy DA, Sukstanskii AL, Leawoods JC, Gierada DS, Bretthorst GL, Lefrak SS, Cooper JD,Conradi MS. Quantitative in vivo assessment of lung microstructure at the alveolar level withhyperpolarized He-3 diffusion MRI. Proc Natl Acad Sci U S A. 2002; 99:3111–3116. [PubMed:11867733]
31. Gonzalez RC, Woods RE. Digital Image Processing: Pearson Education. 2004
32. Trengove RD, Dunlop PJ. Diffusion coefficients and thermal diffusion factors for 5 binary systemsof nitrogen and a noble gas. Physica A. 1982; 115:339–352.
33. Stern EJ, Frank MS. CT of the lung in patients with pulmonary emphysema - Diagnosis,quantification, and correlation with pathological and physiological findings. Am J Roentgenol.1994; 162:791–798. [PubMed: 8140992]
34. Tuder RM, Yoshida T, Fijalkowka I, Biswal S, Petrache I. Role of lung maintenance program inthe heterogeneity of lung destruction in emphysema. Proc Am Thorac Soc. 2006; 3:673–679.[PubMed: 17065372]
35. Ruset IC, Ketel S, Hersman FW. Optical pumping system design for large production ofhyperpolarized Xe-129. Phys Rev Lett. 2006; 96:053002-1–053002-4. [PubMed: 16486926]
36. Diaz S, Casselbrant I, Piitulainen E, Pettersson G, Magnusson P, Peterson B, Wollmer P, LeanderP, Ekberg O, Akeson P. Hyperpolarized He-3 apparent diffusion coefficient MRI of the lung:Reproducibility and volume dependency in healthy volunteers and patients with emphysema. JMagn Reson Imaging. 2008; 27:763–770. [PubMed: 18344208]
37. Kaneko K, Milicemi J, Dolovich MB, Dawson A, Bates DV. Regional distribution of ventilationand perfusion as a function of body position. J Appl Physiol. 1966; 21:767–777. [PubMed:5912746]
38. Albert RK, Hubmayr RD. The prone position eliminates compression of the lungs by the heart. AmJ Respir Crit Care Med. 2000; 161:1660–1665. [PubMed: 10806172]
39. Fichele S, Woodhouse N, Swift AJ, Said Z, Paley MNJ, Kasuboski L, Mills GH, van Beek EJR,Wild JM. MRI of helium-3 gas in healthy lungs: Posture related variations of alveolar size. J MagnReson Imaging. 2004; 20:331–335. [PubMed: 15269962]
40. Amis TC, Jones HA, Hughes JMB. Effect of posture on inter-regional distribution of pulmonaryventilation in man. Respir Physiol. 1984; 56:145–167. [PubMed: 6463423]
41. Halaweish AF, Thedens DR, Sieren JP, Hoffman EA, Van Beek EJR. Volume-controlledhyperpolarized 3He ADC measurements across multiple lung volumes in human subjects. Am JRespir Crit Care Med. 2010; 181:A5521.
Kaushik et al. Page 12
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Erosion and dilation of binary masks. A: Binary mask generated from a representative, non-diffusion weighted image (b = 0) of a COPD subject with emphysema. The mask wasgenerated using a threshold obtained using the mean background intensity mean plus twiceits standard deviation. B: Mask from A after erosion using a circular structuring element(radius = 3 pixels), showing that the majority of the background noise has been removed C:Mask from B after dilation with the same structuring element showing the restoration ofsubtle image features.
Kaushik et al. Page 13
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Effect of masking on the ADC map generation. Separate masks were generated for a healthyvolunteer using only a threshold, a threshold followed by erosion/dilation, and manualsegmentation. The top row shows the masks and the bottom row shows the correspondingADC map obtained after application of the mask. With a threshold mask, the mean ADC ofthe healthy subject was 0.041±0.026 cm2/s. This mean ADC reduced to 0.037±0.021 cm2/swith a mask that underwent erosion/dilation with a circular structuring element with a radiusof 3-pixels. With a manually segmented mask, the mean ADC was the same as that obtainedusing erosion/dilation.
Kaushik et al. Page 14
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Representative slices from 129Xe ADC maps and corresponding whole-lung ADChistograms. A: Healthy volunteer (age = 28 years) with a low mean ADC of 0.037±0.021cm2/s indicating normal alveolar microstructure. The ADC values in the airways are higher(0.083±0.029 cm2/s) and reflect nearly free diffusion. B: Age matched healthy controldisplaying similarly low parenchymal ADC values (0.042±0.025 cm2/s). C: COPD subjectwith emphysema shows high ADC values (0.068±0.028 cm2/s) in the parenchyma,indicating alveolar destruction. D: Whole-lung histogram for the healthy volunteer in panelA showing narrow ADC distribution. E: Whole-lung histogram for the age-matched controlin panel B, exhibits a similarly homogenous distribution. F: Whole-lung histogramcorresponding to the COPD subject with emphysema in panel C, exhibiting a moderatelybroader distribution.
Kaushik et al. Page 15
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 4.Mean parenchyma ADC values for each subject group. The mean ADC of the COPDsubjects with emphysema (0.056±0.008 cm2/s) was significantly higher than that of the age-matched controls (0.043± 0.006 cm2/s, p = 0.0021), which in turn was significantly higherthan that of the healthy volunteers (0.036±0.003 cm2/s, p = 0.0046).
Kaushik et al. Page 16
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 5.A complete ADC map for a healthy volunteer. The map shows clear ADC gradients in boththe superior-inferior and anterior-posterior directions.
Kaushik et al. Page 17
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 6.ADC gradients. (A) Mean ADC gradients in the superior-inferior direction. This gradientwas significantly larger in the COPD subjects with emphysema (0.00074 cm2/s/cm) than inthe age matched healthy controls (0.00049 cm2/s/cm, p = 0.024), and was also larger thanthat of the healthy volunteers (0.00038 cm2/s/cm, p = 0.0017). There was no significantdifference between the superior-inferior gradients observed in the two groups of healthysubjects (p = 0.09). (B) Mean ADC gradients in the anterior-posterior direction. The meanADC gradient from the COPD subjects with emphysema (3.05×10-5 cm2/s/cm) issignificantly smaller than that of either the healthy volunteers (0.00072 cm2/s/cm, p = 0.014)or the age matched healthy controls (0.00065 cm2/s/cm, p = 0.0085). The ADC gradientsfrom the two groups of two healthy subjects were not significantly different (p = 0.81) fromone another.
Kaushik et al. Page 18
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 7.Correlation of mean parenchymal ADC with pulmonary function metrics and age. (A)Correlation with percentage of predicted FEV1. r = −0.77, p = 0.0002. (B) Correlation withpercentage of predicted FEV1/FVC. r = -0.78, p = 0.0002. (C) Correlation with percentageof predicted DLCO/VA. r = −0.77, p = 0.0002. (D) Correlation with age (healthy subjectsonly). r = 0.56, p = 0.02.
Kaushik et al. Page 19
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kaushik et al. Page 20
Tabl
e 1
Dem
ogra
phic
s an
d ex
peri
men
tal v
alue
s fo
r al
l sub
ject
s.
Sub
Age
Yrs
Sex
Par
ench
yma
AD
C c
m2 /
sA
irw
ay A
DC
cm
2 /s
FE
V1
% P
red
FE
V1/
FV
C %
DL
co %
Pre
dD
Lco
/Va
% P
red
Mea
nST
DM
ean
STD
Hea
lthy
Vol
unte
ers
5*38
M0.
035
0.02
50.
069
0.03
2
7*32
M0.
037
0.01
90.
084
0.02
9
8*27
F0.
041
0.02
10.
081
0.02
7
9*56
M0.
037
0.01
90.
086
0.03
0
10*
25F
0.03
20.
020
0.07
80.
032
1228
F0.
037
0.02
10.
083
0.02
9
2424
F0.
032
0.02
00.
082
0.03
1
Age
-Mat
ched
Hea
lthy
Con
trol
s
3164
M0.
053
0.03
10.
079
0.03
291
7578
62
3365
F0.
037
0.02
00.
074
0.03
010
772
9274
3655
M0.
045
0.02
90.
093
0.03
496
7986
86
3766
F0.
033
0.01
80.
085
0.03
011
384
105
96
3867
M0.
048
0.02
20.
087
0.03
183
7591
86
4352
F0.
043
0.02
50.
078
0.03
187
7911
282
4469
F0.
042
0.02
50.
085
0.03
011
776
9375
4566
F0.
043
0.02
30.
083
0.03
399
6711
798
4651
F0.
044
0.02
70.
075
0.03
011
874
102
71
4774
M0.
044
0.02
70.
094
0.03
173
7881
100
CO
PD
Sub
ject
s w
ith
Em
phys
ema
2659
M0.
068
0.02
80.
078
0.03
657
4146
40
2971
M0.
050.
024
0.08
50.
029
7265
5855
3073
M0.
065
0.02
60.
073
0.02
535
3927
37
3266
M0.
060
0.02
70.
078
0.03
064
6364
67
3963
M0.
057
0.02
80.
089
0.02
957
4968
62
4053
F0.
049
0.02
50.
079
0.03
381
6454
45
4170
M0.
053
0.02
60.
073
0.02
954
4647
63
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kaushik et al. Page 21
Sub
Age
Yrs
Sex
Par
ench
yma
AD
C c
m2 /
sA
irw
ay A
DC
cm
2 /s
FE
V1
% P
red
FE
V1/
FV
C %
DL
co %
Pre
dD
Lco
/Va
% P
red
Mea
nST
DM
ean
STD
4272
F0.
044
0.02
50.
073
0.02
854
5273
83
CO
PD
Sub
ject
s w
itho
ut E
mph
ysem
a
2563
F0.
036
0.02
10.
075
0.02
878
6961
76
2868
M0.
039
0.02
20.
093
0.03
379
6666
55
* b =
18.
76 s
/cm
2 ra
ther
than
b =
12
s/cm
2 us
ed f
or a
ll ot
her
subj
ects
.
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kaushik et al. Page 22
Table 2
129Xe ADC distributions within the lungsa.
Parenchymal ADC (cm2/s) Airway ADC (cm2/s) Superior- InferiorGradient b (cm2/s/
cm)
Anterior- PosteriorGradient b (cm2/s/
cm)
Healthy Volunteers 0.036 ±0.003 0.080 ±0.005 0.00038 ±0.00013 0.00072 ±0.00017
Age-Matched Healthy Controls 0.043 ±0.006 0.083 ±0.006 0.00049 ±0.00022 0.00065 ±0.00038
COPD Subjects with Emphysema 0.056 ±0.008 0.078 ±0.006 0.00074 ±0.00033 0.00003 ±0.00047
aValues are population mean ± standard deviation.
bMajor airways were excluded when determining ADC gradients.
Magn Reson Med. Author manuscript; available in PMC 2012 May 14.
Related Documents











