Pathology International 2003; 53 : 204–213 Original Article Blackwell Science, LtdOxford, UK PINPathology International1320-54632003 Japanese Society of Pathology 534April 2003 1456 Retinoid receptors in thyroid carcinoma W. Tang et al . 10.1046/j.1320-5463.2003.01456.x Original Article204213BEES SGML Correspondence: Kennichi Kakudo, MD, PhD, Department of Pathol- ogy, Wakayama Medical University, 811-1 Kimiidera, Wakayama City, Wakayama 641-8509, Japan. Email: [email protected] Received 3 September 2002. Accepted for publication 6 December 2002. Differentiation, proliferation and retinoid receptor status of papillary carcinoma of the thyroid Weihua Tang, 1 Yasushi Nakamura, 1 Hui Zuo, 1 Hironao Yasuoka, 1 Qifeng Yang, 1 Xiaojuan Wang, 1 Misa Nakamura, 1 Ichiro Mori, 1 Akira Miyauchi 2 and Kennichi Kakudo 1 1 Department of Pathology, Wakayama Medical University, Wakayama and 2 Kuma Hospital, Kobe, Japan Messenger RNA expression of retinoic acid receptors (RAR a , RAR b and RAR g ) and retinoid X receptors (RXR a , RXR b and RXR g ) was examined using reverse transcription- polymerase chain reaction in 42 papillary thyroid carcino- mas (PTCs). A loss of mRNA expression was observed in 18 cases of the 42 PTCs, including three cases for RAR a , 14 cases for RAR b , six cases for RXR a and five cases for RXR b . The expressions of RAR g and RXR g were found in all 42 PTCs. Based on Ki 67/MIB1 labeling index (LI), the 42 PTCs were classified into Group A (20 cases; LI = 0–2%), Group B (17 cases; LI = 2–5%) and Group C (5 cases; LI > 5%). The PTCs of groups B and C showed solid, trabe- cular or scirrhous arrangements, infiltrative growth, loss of cellular polarity and cohesiveness more frequently, but cap- sulated growth pattern less frequently, when compared with PTCs of Group A. They also showed more frequent extrathy- roidal extension than Group A. However, no significant dif- ferences were identified in sex, age, nodal status and tumor size. Loss of expression for one or more retinoid receptors frequently occurred in groups B and C. These results sug- gest that the loss of retinoid receptors might occur during the loss of differentiation and tumor progression of PTC. Key words: differentiation, papillary carcinoma, proliferation, retinoic acid, retinoic acid receptor, retinoid X receptor, thyroid gland Retinoic acids (RAs) are biologically active metabolites of vitamin A, and have been shown to mediate a wide spectrum of morphogenesis, proliferation and differentiation processes in vitro and in vivo . 1 Most of the effects of RAs are transduced by nuclear receptors that belong to the steroid hormone receptor superfamily, and have functions as ligand- activated transcription factors. 2 Two different families of the receptors have been identified so far: the retinoic acid recep- tors (RAR a , RAR b and RAR g ) and the retinoid X receptors (RXR a , RXR b and RXR g ). 3 It has been well established that RAR/RXR heterodimers are the functional units that trans- duce the retinoid signal in vivo. 4 These heterodimers activate the transcription by binding to RA response elements located in the promoter region of RA-inducible target genes. 4,5 In experimental and clinical protocols, RAs have been used as anticancer drugs, for example, in cases of acute promye- locytic leukemia, squamous cell carcinomas of the skin, breast cancer and head and neck cancers. 6–9 In these instances, RAs caused the re-differentiation of the cancers and prevented further de-differentiation of the precancerous lesion or cancer. Furthermore, reduced expression of RAR b and RXR b was reported to be associated with poor prognosis of non-small cell lung cancers. 9–11 Clinical pilot studies have indicated that RAs might also be effective in the treatment of de-differentiated thyroid cancer after standard treatment. 12–15 Ligands of the retinoid recep- tors increased thyroid stimulating hormone-binding activity and/or induced 5 ¢ -deiodinase activity, both of which are func- tional differentiation parameters in follicular thyroid carci- noma cell lines. 13,14 Therefore, we might assume that the retinoid receptor status might be correlated to cellular differ- entiation in thyroid carcinomas. Previous immunohistochem- ical studies have reported that RAR b 2 expression was significantly lower in papillary carcinoma than the benign lesions, including goiter, adenoma or normal thyroid, and highly variable in follicular carcinoma. 16 However, only limited information is available about the expression of all six retinoid receptors (RARs and RXRs) in thyroid carcinoma. This study was designed to evaluate the mRNA expression for all six receptors in each of the 42 cases of PTCs.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pathology International
2003;
53
: 204–213
Original Article
Blackwell Science, LtdOxford, UKPINPathology International1320-54632003 Japanese Society of Pathology
534April 20031456
Retinoid receptors in thyroid carcinomaW. Tang
et al.
10.1046/j.1320-5463.2003.01456.xOriginal Article204213BEES SGML
Correspondence: Kennichi Kakudo, MD, PhD, Department of Pathol-ogy, Wakayama Medical University, 811-1 Kimiidera, Wakayama City,Wakayama 641-8509, Japan.Email: [email protected]
Received 3 September 2002. Accepted for publication 6December 2002.
Differentiation, proliferation and retinoid receptor status of papillary carcinoma of the thyroid
Weihua Tang,
1
Yasushi Nakamura,
1
Hui Zuo,
1
Hironao Yasuoka,
1
Qifeng Yang,
1
Xiaojuan Wang,
1
Misa Nakamura,
1
Ichiro Mori,
1
Akira Miyauchi
2
and Kennichi Kakudo
1
1
Department of Pathology, Wakayama Medical University, Wakayama and
2
Kuma Hospital, Kobe, Japan
Messenger RNA expression of retinoic acid receptors(RAR
aaaa
, RAR
bbbb
and RAR
gggg
) and retinoid X receptors (RXR
aaaa
,RXR
bbbb
and RXR
gggg
) was examined using reverse transcription-polymerase chain reaction in 42 papillary thyroid carcino-mas (PTCs). A loss of mRNA expression was observed in 18cases of the 42 PTCs, including three cases for RAR
aaaa
, 14cases for RAR
bbbb
, six cases for RXR
aaaa
and five cases forRXR
bbbb
. The expressions of RAR
gggg
and RXR
gggg
were found in all42 PTCs. Based on Ki 67/MIB1 labeling index (LI), the 42PTCs were classified into Group A (20 cases; LI
====
0–2%),Group B (17 cases; LI
====
2–5%) and Group C (5 cases;LI
>>>>
5%). The PTCs of groups B and C showed solid, trabe-cular or scirrhous arrangements, infiltrative growth, loss ofcellular polarity and cohesiveness more frequently, but cap-sulated growth pattern less frequently, when compared withPTCs of Group A. They also showed more frequent extrathy-roidal extension than Group A. However, no significant dif-ferences were identified in sex, age, nodal status and tumorsize. Loss of expression for one or more retinoid receptorsfrequently occurred in groups B and C. These results sug-gest that the loss of retinoid receptors might occur duringthe loss of differentiation and tumor progression of PTC.
Key words:
differentiation, papillary carcinoma, proliferation,retinoic acid, retinoic acid receptor, retinoid X receptor, thyroidgland
Retinoic acids (RAs) are biologically active metabolites ofvitamin A, and have been shown to mediate a wide spectrumof morphogenesis, proliferation and differentiation processes
in vitro and in vivo
.
1
Most of the effects of RAs are transduced
by nuclear receptors that belong to the steroid hormonereceptor superfamily, and have functions as ligand-activated transcription factors.
2
Two different families of thereceptors have been identified so far: the retinoic acid recep-tors (RAR
a
, RAR
b
and RAR
g
) and the retinoid X receptors(RXR
a
, RXR
b
and RXR
g
).
3
It has been well established thatRAR/RXR heterodimers are the functional units that trans-duce the retinoid signal
in vivo.
4
These heterodimers activatethe transcription by binding to RA response elements locatedin the promoter region of RA-inducible target genes.
4,5
In experimental and clinical protocols, RAs have been usedas anticancer drugs, for example, in cases of acute promye-locytic leukemia, squamous cell carcinomas of the skin,breast cancer and head and neck cancers.
6–9
In theseinstances, RAs caused the re-differentiation of the cancersand prevented further de-differentiation of the precancerouslesion or cancer. Furthermore, reduced expression of RAR
b
and RXR
b
was reported to be associated with poor prognosisof non-small cell lung cancers.
9–11
Clinical pilot studies have indicated that RAs might also beeffective in the treatment of de-differentiated thyroid cancerafter standard treatment.
12–15
Ligands of the retinoid recep-tors increased thyroid stimulating hormone-binding activityand/or induced 5
¢
-deiodinase activity, both of which are func-tional differentiation parameters in follicular thyroid carci-noma cell lines.
13,14
Therefore, we might assume that theretinoid receptor status might be correlated to cellular differ-entiation in thyroid carcinomas. Previous immunohistochem-ical studies have reported that RAR
b
2 expression wassignificantly lower in papillary carcinoma than the benignlesions, including goiter, adenoma or normal thyroid, andhighly variable in follicular carcinoma.
16
However, only limitedinformation is available about the expression of all six retinoidreceptors (RARs and RXRs) in thyroid carcinoma. This studywas designed to evaluate the mRNA expression for all sixreceptors in each of the 42 cases of PTCs.

Retinoid receptors in thyroid carcinoma 205
MATERIALS AND METHODS
Patients and specimens
Tumor specimens and paired normal thyroid tissue wereobtained from 42 patients with PTC who were surgicallytreated through lobectomy or thyroidectomy at Kuma Hospi-tal, Kobe City, Japan from February to April 2002. There were36 women and six men, with a median age of 50.3 years(range 27–81 years). For the RNA analysis, samples weresnap-frozen immediately after surgical resection. Each tumorspecimen had a slice fixed by methanol in order to confirmthe diagnosis of papillary carcinoma histopathologically andimmunohistochemically.
RNA isolation and reverse transcription-polymerase chain reaction (RT-PCR)
Samples used for RNA isolation contained more than 90%cancer tissue, which was confirmed by frozen section exam-ination. Total RNA was isolated from 50 mg frozen tissue byusing a TRIzol RNA extraction kit (Invitrogen, Carlsbad, CA,USA) according to the manufacturers’ instruction and previ-ous studies from our laboratory.
17–19
First-strand cDNA wassynthesized from 0.5 ìg total RNA in a 20
m
L reaction unit(T
HERMO
S
CRIPT
RT-PCR System, Invitrogen Japan, Tokyo,Japan), and 1
m
L of the cDNA was subjected to PCR, whichwas performed using a thermal cycler (GeneAmp, PCR sys-tem 9700, Tokyo, Japan). The reactions were run at 94
∞
C for2 min, followed by 30 cycles for
b
-actin or 28–32 cycles for allretinoid receptors at 94
∞
C for 30 s, 55–68
∞
C for 30 s and72
∞
C for 45 s, followed by 7 min at 72
∞
C. Sequences of theprimers for RAR and RXR amplification and annealing tem-peratures of PCR are shown in Table 1. Electrophoresis of
the amplification products was performed on 1.5% (weight/volume) agarose gel, and then the gel stained with ethidiumbromide and photographed under ultraviolet light.
The
b
-actin gene was used as an internal control. Whenamplification was observed in normal thyroid tissue and nodetectable band was seen in the corresponding cancer tis-sue, the case was regarded as loss of mRNA expression.
Immunohistochemical staining of Ki-67/MIB1
For the determination of Ki-67/MIB1 labeling index (LI),immunohistochemistry was performed on 5
m
m paraffinembedded sections of the 42 PTCs. In brief, the paraffin-embedded sections were de-waxed and processed in amicrowave with a citrate buffer for 5
¥
3 min for antigenretrieval. Sections were then incubated overnight at 4
∞
C witha 1:100 dilution of anti-Ki-67 monoclonal antibodies (DAKO,Denmark). Tissue sections reacting with mouse IgG wereused instead of primary antibodies as controls. After beingwashed with 1% Tween in Tris-buffered solution, sectionswere incubated with MAX-PO (NICHIREI, Tokyo, Japan) for90 min. A peroxidase substrate, 3,3
¢
-diaminobenzidine tet-rahydrochloride, was then applied to enable visualization,and 0.5% methylgreen at pH 5.0 was used for nuclear stain.
Any follicular epithelial cells with distinct nuclear staining,regardless of staining intensity, were considered positive forKi-67/MIB1, and 2000 tumor cells were counted at a high-power field. The Ki-67/MIB1 LI was expressed as a percent-age of immunoreactive cells to the total counted tumor cells.Three of the investigators (W.T., X.W. and Y.N.) indepen-dently scored the samples. An average of these scores foreach case was used for the analysis.
Statistical analysis was performed on the results using the
c
2
test. A difference was considered to be statistically signif-
Table 1
Primers for the polymerase chain reaction, annealing temperature and length of the products
Sequences of the primers Products Temperature (
∞
C) Reference†
RAR
a
F: 5
¢
-GCATCATCAACAAGGTGAACC-3
¢
262 bp 61 NM000964R: 5
¢
-GTTGTTCTGAGCTGTTGTTCG-3
¢
RAR
b
F: 5
¢
-ATCGATGCCAATACTGTCGA-3
¢
242 bp 55 XM045726R: 5
¢
-GACTCGATGGTCAGCACTG-3
¢
RAR
g
F: 5
¢
-AGCTCATCACCAGGTCAGC-3
¢
421 bp 62 M24857R: 5
¢
-TCTCGGTGTCATCCATCTCC-3
¢
RXR
a
F: 5
¢
-TGATTGACAAGCGGCAGCGGA-3
¢
427 bp 58 NM002957R: 5
¢
-ACGGCGATGGAGCGGTGGGAG-3
¢
RXR
b
F: 5
¢
-CCCACCCCCGATGCCACCAC-3
¢
513 bp 68 BC001167R: 5
¢
-CCCTCCCCATCCCATCCTT-3
¢
RXR
g
F: 5
¢
-CTACCCATCCACCAGCCC-3
¢
551 bp 66 U38480R: 5
¢
-GAGGTCCAGAGAAGTGGGGAA-3
¢b
-actin F: 5
¢
-
TGACGGGGTCACCCACACTGTGCCCATCTA
-3
¢
653 bp 68 M10277R: 5
¢
-
CTAGAAGCATTTGCGGTGGACGATGGAGGG
-3
¢
bp, define; F, forward, R, reverse; RAR, retinoic acid receptor, RXR, retinoid X receptor; Tm, annealing temperature. †Number referring to the GenBankdatabase.
206 W. Tang
et al
.
icant when the
P
-value was less than 0.05. The computerprogram used for this purpose was StatView 5.0 (SASInstitute, Cary, NC, USA).
RESULTS
RAR and RXR mRNA expression in the 42 PTCs
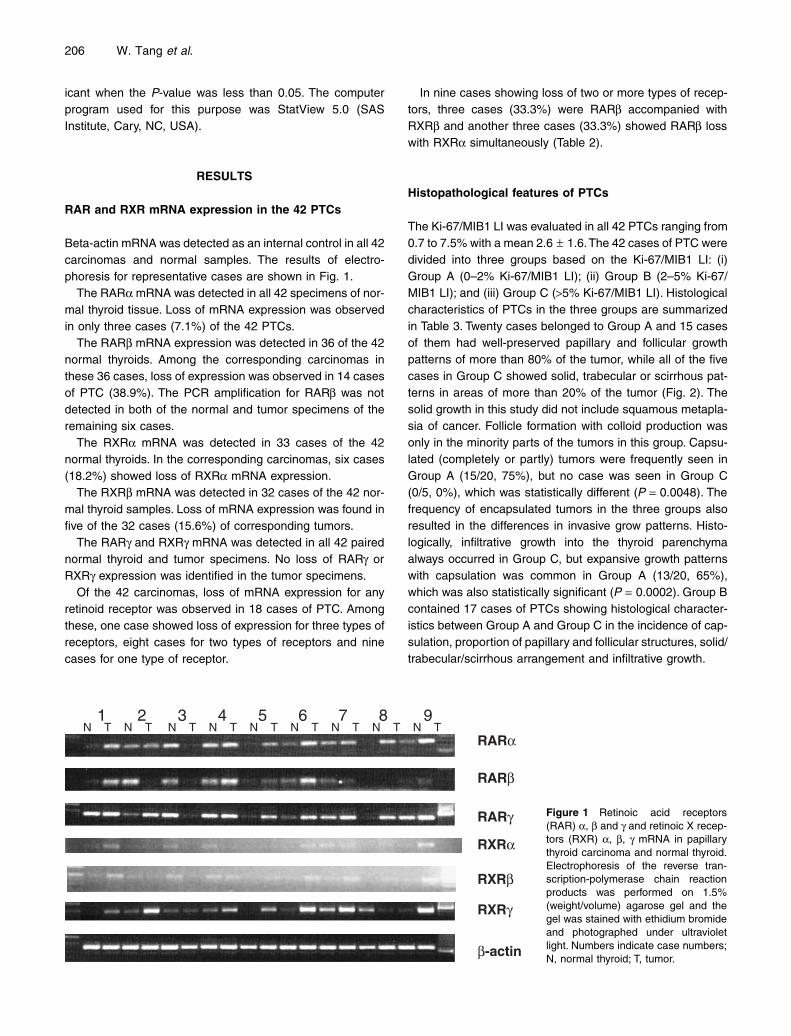
Beta-actin mRNA was detected as an internal control in all 42carcinomas and normal samples. The results of electro-phoresis for representative cases are shown in Fig. 1.
The RAR
a
mRNA was detected in all 42 specimens of nor-mal thyroid tissue. Loss of mRNA expression was observedin only three cases (7.1%) of the 42 PTCs.
The RAR
b
mRNA expression was detected in 36 of the 42normal thyroids. Among the corresponding carcinomas inthese 36 cases, loss of expression was observed in 14 casesof PTC (38.9%). The PCR amplification for RAR
b
was notdetected in both of the normal and tumor specimens of theremaining six cases.
The RXR
a
mRNA was detected in 33 cases of the 42normal thyroids. In the corresponding carcinomas, six cases(18.2%) showed loss of RXR
a
mRNA expression.The RXR
b
mRNA was detected in 32 cases of the 42 nor-mal thyroid samples. Loss of mRNA expression was found infive of the 32 cases (15.6%) of corresponding tumors.
The RAR
g
and RXR
g
mRNA was detected in all 42 pairednormal thyroid and tumor specimens. No loss of RAR
g
orRXR
g
expression was identified in the tumor specimens.Of the 42 carcinomas, loss of mRNA expression for any
retinoid receptor was observed in 18 cases of PTC. Amongthese, one case showed loss of expression for three types ofreceptors, eight cases for two types of receptors and ninecases for one type of receptor.
In nine cases showing loss of two or more types of recep-tors, three cases (33.3%) were RAR
b
accompanied withRXR
b
and another three cases (33.3%) showed RAR
b
losswith RXR
a
simultaneously (Table 2).
Histopathological features of PTCs
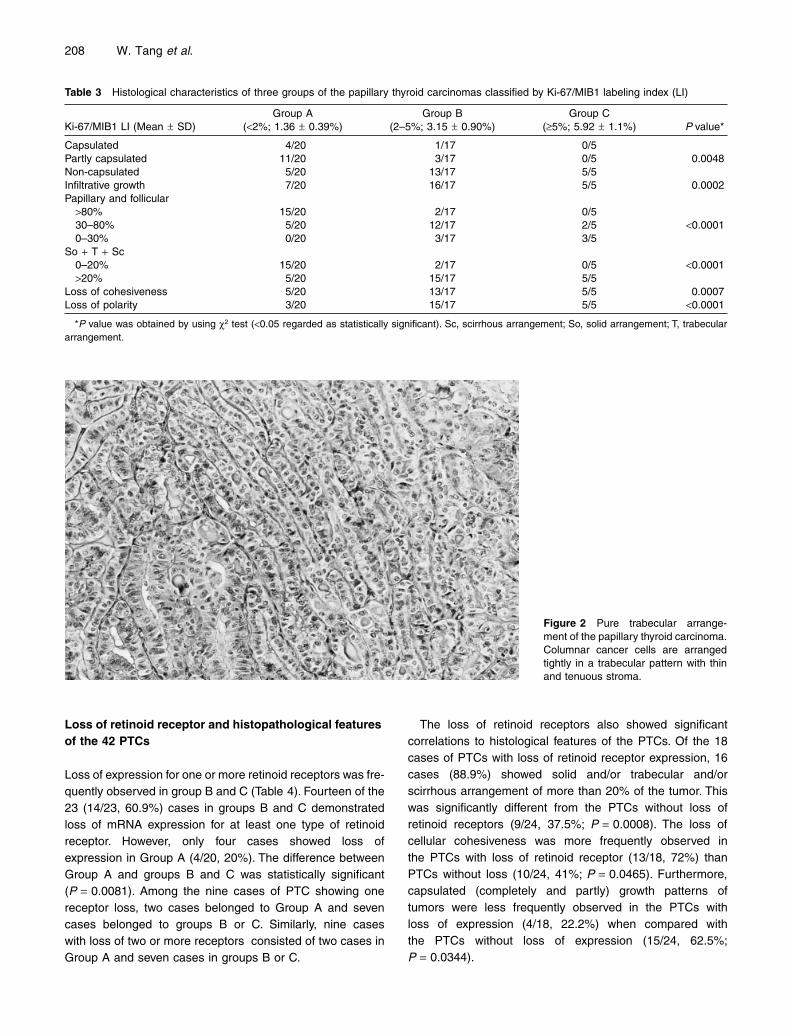
The Ki-67/MIB1 LI was evaluated in all 42 PTCs ranging from0.7 to 7.5% with a mean 2.6 ± 1.6. The 42 cases of PTC weredivided into three groups based on the Ki-67/MIB1 LI: (i)Group A (0–2% Ki-67/MIB1 LI); (ii) Group B (2–5% Ki-67/MIB1 LI); and (iii) Group C (>5% Ki-67/MIB1 LI). Histologicalcharacteristics of PTCs in the three groups are summarizedin Table 3. Twenty cases belonged to Group A and 15 casesof them had well-preserved papillary and follicular growthpatterns of more than 80% of the tumor, while all of the fivecases in Group C showed solid, trabecular or scirrhous pat-terns in areas of more than 20% of the tumor (Fig. 2). Thesolid growth in this study did not include squamous metapla-sia of cancer. Follicle formation with colloid production wasonly in the minority parts of the tumors in this group. Capsu-lated (completely or partly) tumors were frequently seen inGroup A (15/20, 75%), but no case was seen in Group C(0/5, 0%), which was statistically different (P = 0.0048). Thefrequency of encapsulated tumors in the three groups alsoresulted in the differences in invasive grow patterns. Histo-logically, infiltrative growth into the thyroid parenchymaalways occurred in Group C, but expansive growth patternswith capsulation was common in Group A (13/20, 65%),which was also statistically significant (P = 0.0002). Group Bcontained 17 cases of PTCs showing histological character-istics between Group A and Group C in the incidence of cap-sulation, proportion of papillary and follicular structures, solid/trabecular/scirrhous arrangement and infiltrative growth.
Figure 1 Retinoic acid receptors(RAR) a, b and g and retinoic X recep-tors (RXR) a, b, g mRNA in papillarythyroid carcinoma and normal thyroid.Electrophoresis of the reverse tran-scription-polymerase chain reactionproducts was performed on 1.5%(weight/volume) agarose gel and thegel was stained with ethidium bromideand photographed under ultravioletlight. Numbers indicate case numbers;N, normal thyroid; T, tumor.
RXRb
RXRa
RARg
RARb
RARa
RXRg
b-actin
1 2 3 4 5 6 7 8 9 N T N T N T N T N T N T N T N T N T
T
Retinoid receptors in thyroid carcinoma 207
The loss of cohesiveness was often seen in the peripheryof the tumor, where cancer cells were loosely or individuallyarranged with no papillary or follicular formation (Fig. 3).This feature occurred in 18 cases (78.3%) out of the 23cases of groups B and C, and the frequency was signifi-cantly different from cases in Group A (5/20, 25%;P = 0.0007). The features of loss of cellular polarity in thisstudy were defined as follows: the nuclei of the epitheliumwas located in the middle or on top of the cells, simulating ahob-nail appearance (Fig. 4) or of a papillary structure withelevated nuclear positions in cancer glandular (papillary)cells (Fig. 5). In other cases, the epithelial cells werearranged in irregular shaped tubular structures without col-loid (Fig. 6). The hob-nail appearance was found in three
cases in Group B and three cases in Group A, and the irreg-ular tubular arrangement was seen in five cases in Group B.Another four cases in Group B showed the elevated nucleiand foci of hob-nail appearance in the same tumor. In addi-tion, papillary structures covered with low, flattened or smallround cells (Fig. 7) were observed in three cases in GroupB and two cases in Group C, which were also included asan expression of the loss of cellular polarity in this study. Inthe remaining two cases in Group C, the tubular arrange-ment, hob-nail appearance and elevated nuclei were allobserved in the same tumor. The features of the loss of cel-lular polarity in groups B and C are summarized in Table 3,and were more frequently found than in Group A(P < 0.0001).
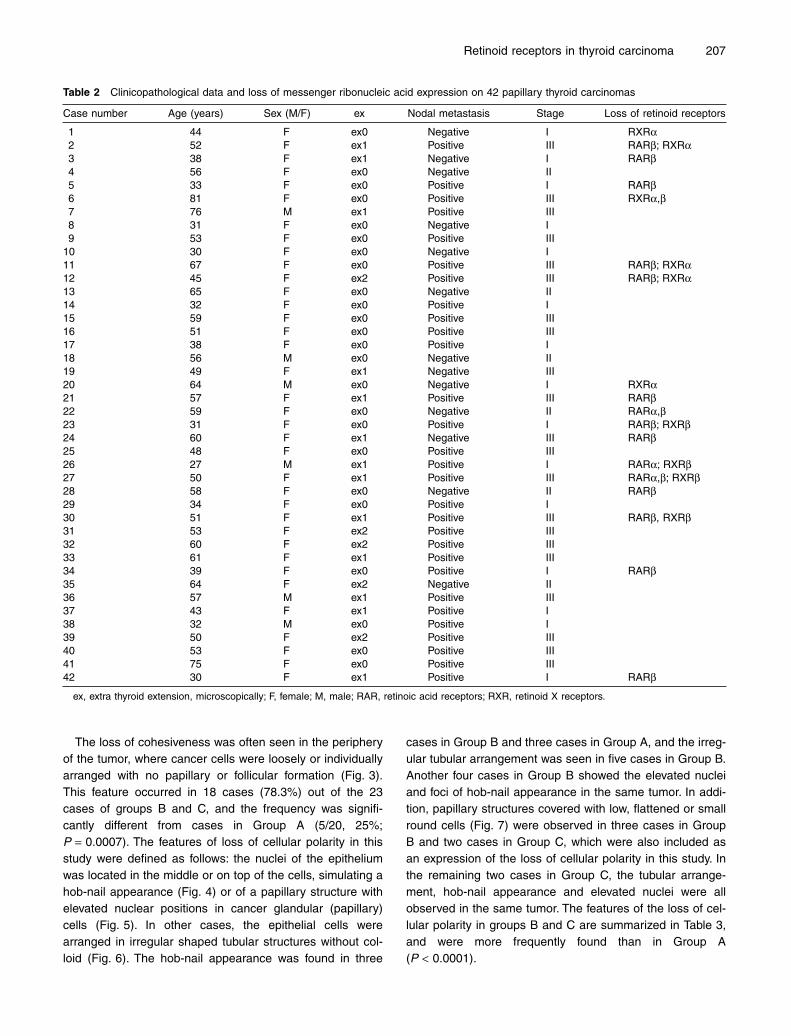
Table 2 Clinicopathological data and loss of messenger ribonucleic acid expression on 42 papillary thyroid carcinomas
Case number Age (years) Sex (M/F) ex Nodal metastasis Stage Loss of retinoid receptors
1 44 F ex0 Negative I RXRa2 52 F ex1 Positive III RARb; RXRa3 38 F ex1 Negative I RARb4 56 F ex0 Negative II5 33 F ex0 Positive I RARb6 81 F ex0 Positive III RXRa,b7 76 M ex1 Positive III8 31 F ex0 Negative I9 53 F ex0 Positive III
10 30 F ex0 Negative I11 67 F ex0 Positive III RARb; RXRa12 45 F ex2 Positive III RARb; RXRa13 65 F ex0 Negative II14 32 F ex0 Positive I15 59 F ex0 Positive III16 51 F ex0 Positive III17 38 F ex0 Positive I18 56 M ex0 Negative II19 49 F ex1 Negative III20 64 M ex0 Negative I RXRa21 57 F ex1 Positive III RARb22 59 F ex0 Negative II RARa,b23 31 F ex0 Positive I RARb; RXRb24 60 F ex1 Negative III RARb25 48 F ex0 Positive III26 27 M ex1 Positive I RARa; RXRb27 50 F ex1 Positive III RARa,b; RXRb28 58 F ex0 Negative II RARb29 34 F ex0 Positive I30 51 F ex1 Positive III RARb, RXRb31 53 F ex2 Positive III32 60 F ex2 Positive III33 61 F ex1 Positive III34 39 F ex0 Positive I RARb35 64 F ex2 Negative II36 57 M ex1 Positive III37 43 F ex1 Positive I38 32 M ex0 Positive I39 50 F ex2 Positive III40 53 F ex0 Positive III41 75 F ex0 Positive III42 30 F ex1 Positive I RARb
ex, extra thyroid extension, microscopically; F, female; M, male; RAR, retinoic acid receptors; RXR, retinoid X receptors.
208 W. Tang et al.
Loss of retinoid receptor and histopathological features of the 42 PTCs
Loss of expression for one or more retinoid receptors was fre-quently observed in group B and C (Table 4). Fourteen of the23 (14/23, 60.9%) cases in groups B and C demonstratedloss of mRNA expression for at least one type of retinoidreceptor. However, only four cases showed loss ofexpression in Group A (4/20, 20%). The difference betweenGroup A and groups B and C was statistically significant(P = 0.0081). Among the nine cases of PTC showing onereceptor loss, two cases belonged to Group A and sevencases belonged to groups B or C. Similarly, nine caseswith loss of two or more receptors consisted of two cases inGroup A and seven cases in groups B or C.
The loss of retinoid receptors also showed significantcorrelations to histological features of the PTCs. Of the 18cases of PTCs with loss of retinoid receptor expression, 16cases (88.9%) showed solid and/or trabecular and/orscirrhous arrangement of more than 20% of the tumor. Thiswas significantly different from the PTCs without loss ofretinoid receptors (9/24, 37.5%; P = 0.0008). The loss ofcellular cohesiveness was more frequently observed inthe PTCs with loss of retinoid receptor (13/18, 72%) thanPTCs without loss (10/24, 41%; P = 0.0465). Furthermore,capsulated (completely and partly) growth patterns oftumors were less frequently observed in the PTCs withloss of expression (4/18, 22.2%) when compared withthe PTCs without loss of expression (15/24, 62.5%;P = 0.0344).
Table 3 Histological characteristics of three groups of the papillary thyroid carcinomas classified by Ki-67/MIB1 labeling index (LI)
Ki-67/MIB1 LI (Mean ± SD)Group A
(<2%; 1.36 ± 0.39%)Group B
(2–5%; 3.15 ± 0.90%)Group C
(≥5%; 5.92 ± 1.1%) P value*
Capsulated 4/20 1/17 0/5Partly capsulated 11/20 3/17 0/5 0.0048Non-capsulated 5/20 13/17 5/5Infiltrative growth 7/20 16/17 5/5 0.0002Papillary and follicular
>80% 15/20 2/17 0/530–80% 5/20 12/17 2/5 <0.00010–30% 0/20 3/17 3/5
So + T + Sc0–20% 15/20 2/17 0/5 <0.0001>20% 5/20 15/17 5/5
Loss of cohesiveness 5/20 13/17 5/5 0.0007Loss of polarity 3/20 15/17 5/5 <0.0001
*P value was obtained by using c2 test (<0.05 regarded as statistically significant). Sc, scirrhous arrangement; So, solid arrangement; T, trabeculararrangement.
Figure 2 Pure trabecular arrange-ment of the papillary thyroid carcinoma.Columnar cancer cells are arrangedtightly in a trabecular pattern with thinand tenuous stroma.
Retinoid receptors in thyroid carcinoma 209
Stage and clinicopathological parameters
The cases of groups B and C showed more frequent extrathy-roidal extension (14/22, 63.6%) than Group A (4/20, 20%;P = 0.0120). The cases in tumor node metastasis stage IIIwere more frequently observed in groups B and C (14/22,63.6%) when compared with Group A (7/20, 35%), althoughno statistical significance was established (P = 0.1003). Fivecases of encapsulated variant were observed in the 42cases, and four of them belonged to Group A (Table 5). Nosignificant difference was identified between men andwomen, patients aged more than 45 years and those less
than 45 years, and positive and negative nodal metastasisamong the groups.
DISCUSSION
In this study, mRNA expressions of six retinoid receptorswere investigated in 42 cases of PTC. Loss of the expressionfor one or more retinoid receptors was observed in 18 casesof PTC, including three cases for RARa, 14 for RARb, six forRXRa and five for RXRb. These results did not conflict withprevious reports on thyroid tissue and/or thyroid carcinoma
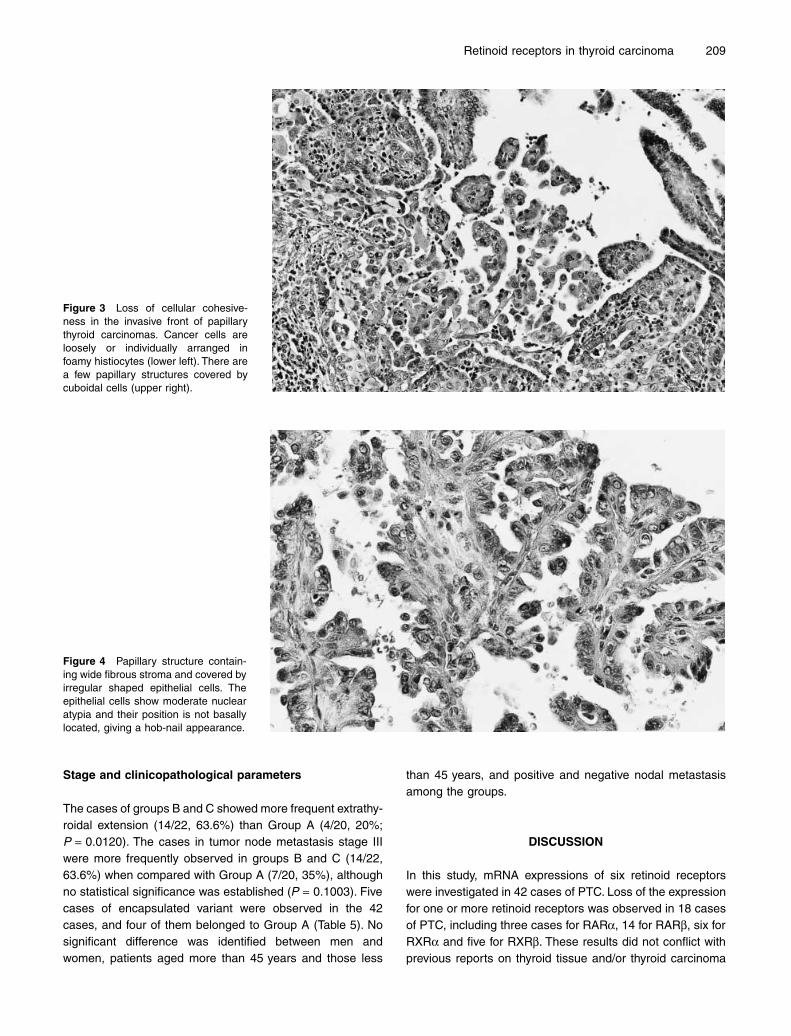
Figure 3 Loss of cellular cohesive-ness in the invasive front of papillarythyroid carcinomas. Cancer cells areloosely or individually arranged infoamy histiocytes (lower left). There area few papillary structures covered bycuboidal cells (upper right).
Figure 4 Papillary structure contain-ing wide fibrous stroma and covered byirregular shaped epithelial cells. Theepithelial cells show moderate nuclearatypia and their position is not basallylocated, giving a hob-nail appearance.
210 W. Tang et al.
cell lines. Rochaix et al. reported that a decrease in RARbimmunostaining was observed in all 16 cases of PTC thatthey investigated.16 In addition to loss of RARb mRNA in38.9% of our 36 cases of PTC, decreased mRNA levels lessthan 50% of normal thyroid were observed in three cases, inline with previous research. Schmutzler et al. demonstratedmultiple loss of mRNA expression in nine of 12 thyroid tumorsfor one or more retinoid receptor, except for RXRg.20 Similarresults were reported for malignant lesions of otherorgans.21–24 Our report on thyroid cancer is the first that suc-cessfully showed the status of all 6 retinoid receptors in PTC.
The histopathological characteristics of the 42 PTCs werealso analyzed, and they were classified into three groupsbased on Ki-67/MIB1 LI. The characteristic histological fea-tures, such as trabecular, solid or scirrhous arrangement,were frequently observed in groups B and C, which had highproliferation indexes. These histological features were alsodescribed in the other previous reports on ‘poorly differenti-ated carcinoma’ of the thyroid.25–31 Although the term ‘poorlydifferentiated carcinoma’ of the thyroid was introduced bytwo separate sources almost simultaneously in the early1980s,25,26 the morphological criteria used were not always
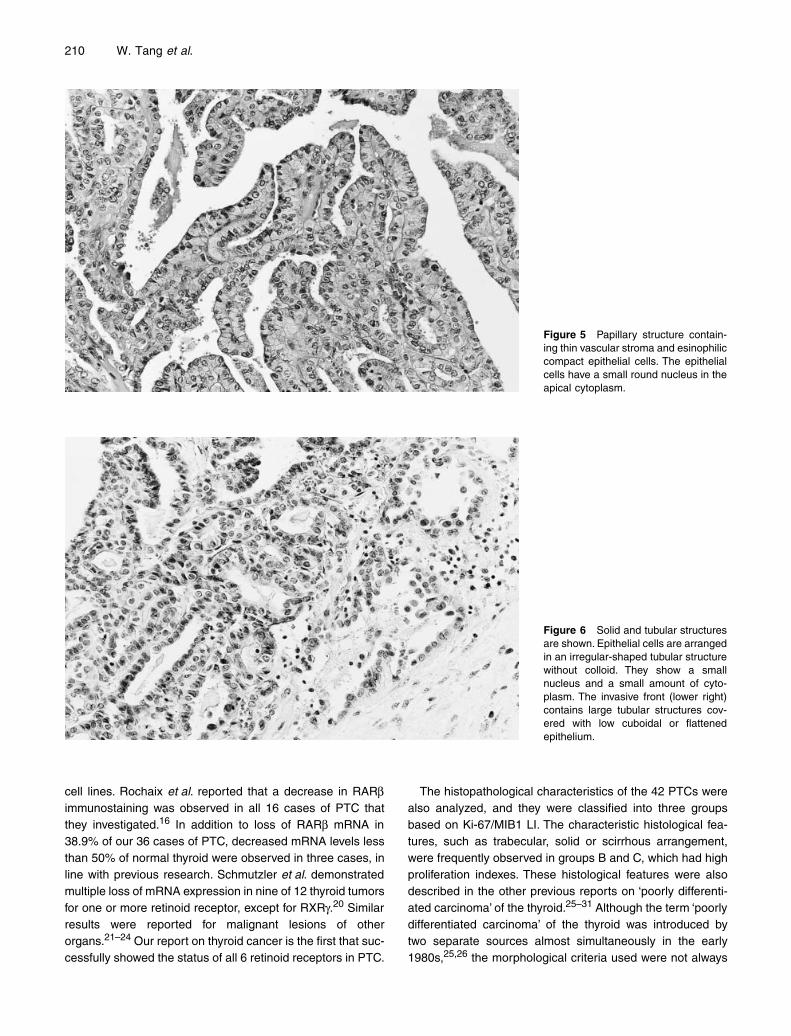
Figure 5 Papillary structure contain-ing thin vascular stroma and esinophiliccompact epithelial cells. The epithelialcells have a small round nucleus in theapical cytoplasm.
Figure 6 Solid and tubular structuresare shown. Epithelial cells are arrangedin an irregular-shaped tubular structurewithout colloid. They show a smallnucleus and a small amount of cyto-plasm. The invasive front (lower right)contains large tubular structures cov-ered with low cuboidal or flattenedepithelium.
Retinoid receptors in thyroid carcinoma 211
comparable.25–31 Our grouping of PTCs linking a proliferationpotential of poorly differentiated characteristics was morecommon in groups B and C. In order to avoid confusion withprevious classifications, we did not use the terminology of the‘poorly differentiated’ PTCs in this paper. The tall cell orcolumnar cell variants were not included in this analysis.30,32
Certain histological features in PTCs, such as loss of cellularpolarity and loss of cellular cohesiveness, were described inthis study in addition to solid/trabecular/scirrhous growth pat-tern, frequently observed in groups B and C. These histolog-ical features showed a link to high Ki-67/MIB1 proliferationindex. Loss of cellular attachment is an important finding invarious malignant tumors, as previously reported using dif-ferent methods and organs.33 The description about the loss
of polarity and loss of cellular cohesiveness defined in thisstudy has not been introduced to describe the more progres-sive type of PTC.25–32
The Ki-67/MIB1 LI is a well-established proliferation markerand is associated with the progression of a variety of malig-nant tumors, including thyroid carcinomas.34–36 Tallini et al.reported that the Ki-67/MIB1 index showed a strong correla-tion with the subclassification of the thyroid carcinomas inthree prognostic groups, well-differentiated papillary or follic-ular carcinomas (group 1), poorly differentiated carcinomasand tall cell variant PTC (group 2) and undifferentiated
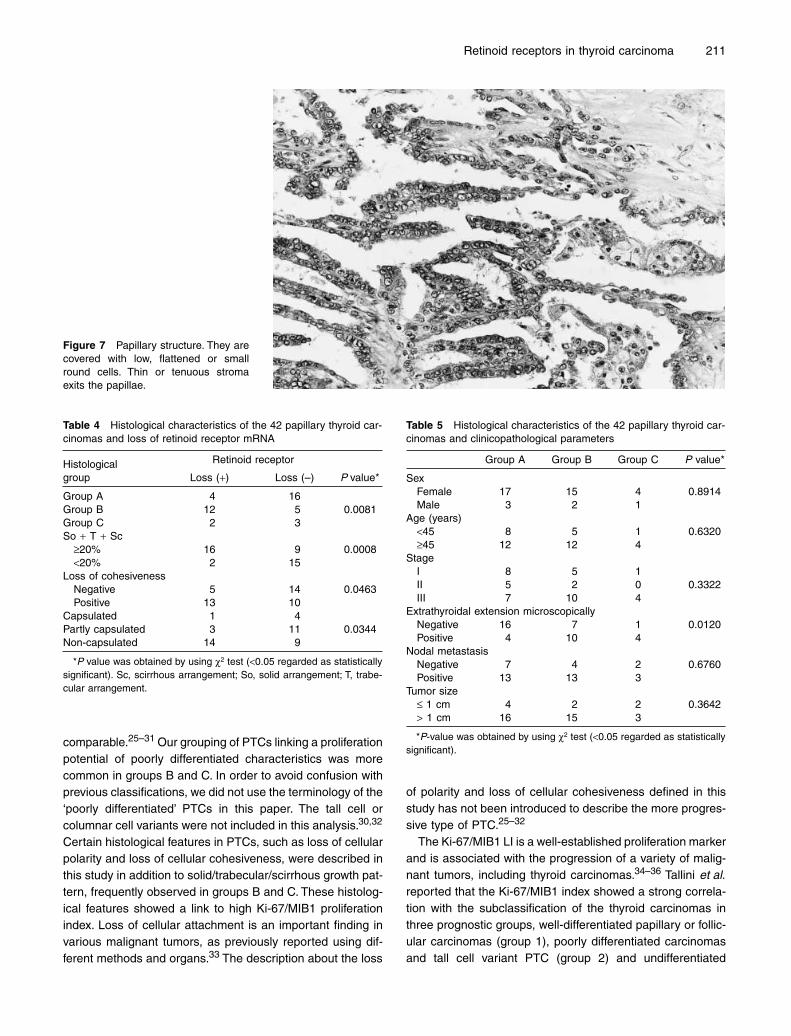
Figure 7 Papillary structure. They arecovered with low, flattened or smallround cells. Thin or tenuous stromaexits the papillae.
Table 4 Histological characteristics of the 42 papillary thyroid car-cinomas and loss of retinoid receptor mRNA
Histological group
Retinoid receptor
P value* Loss (+) Loss (–)
Group A 4 16Group B 12 5 0.0081Group C 2 3So + T + Sc
≥20% 16 9 0.0008<20% 2 15
Loss of cohesivenessNegative 5 14 0.0463Positive 13 10
Capsulated 1 4Partly capsulated 3 11 0.0344Non-capsulated 14 9
*P value was obtained by using c2 test (<0.05 regarded as statisticallysignificant). Sc, scirrhous arrangement; So, solid arrangement; T, trabe-cular arrangement.
Table 5 Histological characteristics of the 42 papillary thyroid car-cinomas and clinicopathological parameters
Group A Group B Group C P value*
SexFemale 17 15 4 0.8914Male 3 2 1
Age (years)<45 8 5 1 0.6320≥45 12 12 4
StageI 8 5 1II 5 2 0 0.3322III 7 10 4
Extrathyroidal extension microscopicallyNegative 16 7 1 0.0120Positive 4 10 4
Nodal metastasisNegative 7 4 2 0.6760Positive 13 13 3
Tumor size£ 1 cm 4 2 2 0.3642> 1 cm 16 15 3
*P-value was obtained by using c2 test (<0.05 regarded as statisticallysignificant).
212 W. Tang et al.
carcinomas (group 3).34 Cancers with a trabecular or solidgrowth pattern were included in group 2, with a relatively highKi-67/MIB1 LI. They also included follicular carcinoma ingroup 1 and insular or tall cell variant in group 2. Togetherwith the observation by Tallini et al., poorly differentiated typePTCs under various histological definitions have a high Ki-67/MIB1 LI and might be a predictive parameter for patient prog-nosis. In this paper, only papillary carcinomas were analyzed,and unfortunately, no prognostic data was provided. The Ki-67/MIB1 LI of PTC was previously reported as 1.1 ± 0.7%(Yoshida et al.),36 but a higher percentage was also reportedin the other reports.36,37 The Ki-67/MIB1 LI (0.6–7.5,2.6 ± 1.6%) in this paper might be a little bit higher than thatreported previously.34,36–38 This might be caused by a differ-ent method of fixation and/or antigen retrieval applied to oursamples. A comparison with formalin-fixed paraffin embed-ded routinely processed section and decalcified samplesmight be necessary before making a firm conclusion on howto classify PTCs by Ki-67/MIB1 LI. The loss of expression ofretinoid receptors frequently occurred in the PTCs of groupsB and C, in which the Ki-67/MIB1 was higher than Group A.The information of loss of retinoid receptors might be usefulto pick up PTCs with high Ki-67/MIB1 proliferation indexesand cases with loss of cellular differentiation from commonPTCs that might be biologically more aggressive than ordi-nary PTCs.
The stage of the PTCs did not have a significant correlationto mRNA expression of retinoid receptor. This result mightprovide a conclusion that loss of retinoid receptors mightoccur even in early stages of PTC, and could be no changein tumor progression from stage I to stage III. Therefore, theretinoid receptor status might be important in characterizingtumor aggressiveness in any stage of the disease.
The underlying mechanism, responsible for the loss of ret-inoid receptors in PTC, is not clear. The observations onbreast cancer from our previous study implied that epigeneticchanges such as methylation based on LOH contribute to theloss of RARb2.39,40 We might be able to assume that anygenetic or epigenetic changes that occur during the develop-ment of thyroid carcinomas induce a loss of RAR and RXRexpression.
Previous reports have indicated the efficacy of RA in re-differentiation therapy for thyroid cancer after standard treat-ment. Approximately 40% of the patients responded to RAapplication with an increased radioiodide uptake.12–15 Ourstudy successfully demonstrated a high incidence of retinoidreceptor loss as well as amplification in PTCs. Thus, evalu-ation of the receptor status might be necessary when treat-ment is applied for the purpose of finding more effectivecases from non-responder.
We observed that the loss of mRNA expression of retinoidreceptors frequently occurred in PTCs of groups B and C thathad higher Ki-67/MIB1 LIs. From these observations, we
might conclude that the status of retinoid receptor expressioncould be one of the molecular markers involved in tumor pro-liferation and differentiation of thyroid papillary carcinomas.
ACKNOWLEDGMENTS
We thank Mr Hiroshi Yoshida, Kuma Hospital, for his help inpreparing tissue samples for this study, and Emiko Taniguchi,Tomoko Kagiya, Miyoko Maekawa and Tomoko Ohue for his-topathological examination. Dr Weihua Tang was supportedby Rotary Yoneyama Memorial Foundation and by a For-eigner’s Research Grant from Wakayama foundation for thePromotion of Medicine (scholarships awarded by NORIT-SUKOKI, Wakayama, Japan). This study was supported inpart by a Grant-in-aid for Scientific Research C (No.14570155).
REFERENCES
1 Pfahl M, Chytil F. Regulation of metabolism by retinoic acid andits nuclear receptors. Ann Rev Nutr 1996; 16: 257–83.
2 Mangelsdrff DJ, Evans RE. The RXR heterodimers and orphanreceptors. Cell 1995; 86: 841–50.
3 Chambon P. A decade of molecular biology of retinoic acidreceptors. Fed Am Soc Exp Biol J 1996; 10: 940–54.
4 Kastner P, Mark M, Chambon P. Nonsteroid nuclear receptors:What are genetic studies telling us about their role in real life?Cell 1995; 83: 859–69.
5 Leid N, Kastner P, Chambon P. Multiplicity generates diversityin the retinoic acid signaling pathways. Trends Biochem Sci1992; 17: 427–33.
6 Lotan R. Retinoids in cancer chemoprevention. Fed Am SocExp Biol J 1996; 10: 1031–9.
7 Hong WK, Sporn MB. Recent advances in chemoprevention ofcancer. Science 1997; 278: 1073–7.
8 Crowe DL. Retinoic acid receptor, induces terminal differentia-tion of squamous cell carcinoma lines in the absence of cyclin-dependent kinase inhibitor expression. Cancer Res 1998; 58:142–8.
9 Lawrence JA, Adamson PC, Caruso R et al. Phase I clinical trialof alitretinoin and tamoxifen in breast cancer patients: toxicity,parmacokinetic, and biomarker evaluations. J Clin Oncol 2001;19: 2754–63.
10 Khuri FR, Lotan R, Kemp BL et al. Retinoic acid receptor-b asa prognostic indicator in stage I non-small cell lung cancer. JClin Oncol 2000; 18: 2798–804.
11 Brabender J, Danenberg KD, Metzger R et al. The role of ret-inoid X receptor messenger RNA expression in curativelyresected Non-small cell lung cancer. Clin Cancer Res 2002; 8:438–43.
12 Schmutzler C, Köhrle J. Retinoic acid redifferentiation therapyfor thyroid cancer. Thyroid 2000; 10: 393–406.
13 Schreck R, Schnieders F, Schmutzler C, Köhrle J. Retinoidsstimulate type-I iodothyronine 5¢-deiodinase activity in humanfollicular thyroid-carcinoma cell lines. J Clin Endocrinol Metab1994; 78: 791–8.
14 Simon D, Köhrle J, Reiners C et al. Redifferentiation therapywith retinoids: therapeutic option for advanced follicular andpapillary thyroid carcinoma. World J Surg 1998; 22: 569–74.
Retinoid receptors in thyroid carcinoma 213
15 Grunwald F, Menzel C, Bender H et al. Redifferentiation ther-apy-induced radioiodine uptake in thyroid cancer. J Nucl Med1998; 39: 1903–6.
16 Rochaix P, Monteil-Onteniente S, Rochette-Egly C, Caratero C,Voigt JJ, Jozan S. Reduced expression of retinoic acid receptorbeta protein (RAR beta) in human papillary thyroid carcinoma:immunohistochemical and western blot study. Histopathology1998; 33: 337–43.
17 Tang W, Nakamura Y, Tsujimoto M et al. Heparanase: a keyenzyme in invasion and metastasis of gastric carcinoma. ModPathol 2002; 15: 593–8.
18 Nakamura M, Hashimoto T, Nakajima T et al. A new type ofhuman calcitonin receptor isoform generated by alternativesplicing. Biochem Biophys Res Commun 1995; 209: 744–51.
19 Nakamura M, Yang Q, Gouda T et al. Loss of calcitonin bindingin rat is not related to calcitonin receptor gene abnormality. Bio-chem Biophys Res Commun 2001; 284: 1184–8.
20 Schmuzler C, Brtko J, Winzer R et al. Functional retinoid andthyroid hormone receptors in human thyroid-carcinoma celllines and tissues. Int J Cancer 1998; 76: 368–76.
21 Lord RV, Tsai PI, Danenberg KD et al. Retinoic acid receptor-alpha messenger RNA expression is increased and retinoicacid receptor-gamma expression is decreased in Barrett’sintestinal metaplasia, dysplasia, adenocarcinoma sequence.Surgery 2001; 129: 267–76.
22 Xu XC, Wong WY, Goldberg L et al. Progressive decreases innuclear retinoid receptors during skin squamous carcinogene-sis. Cancer Res 2001; 61: 4306–10.
23 Ariga N, Moriya T, Suzuki T, Kimura M, Ohuchi N, Sasano H.Retinoic acid receptor and retinoid X receptor in ductal carci-noma in situ and intraductal proliferative lesions of the humanbreast. Jpn J Cancer Res 2000; 91: 1169–76.
24 Picard E, Seguin C, Monhoven N et al. Expression of retinoidreceptor genes and protein in non-small-cell Lung cancer. JNatl Cancer Inst 1999; 91: 1059–66.
25 Sakamoto A, Kasai N, Sugano H. Poorly differentiated carci-noma of the thyroid. A clinicopathologic entity for a high-riskgroup of papillary and follicular carcinomas. Cancer 1983; 52:1849–55.
26 Carcangiu ML, Zampi G, Rosai J. Poorly differentiated(‘insular’) thyroid carcinoma. A reinterpretation of ‘Langhans’‘wuchernde struma’. Am J Surg Pathol 1984; 8: 655–68.
27 Papotti M, Botto Micca F, Favero A, Palestini N, Bussolati G.Poorly differentiated thyroid carcinomas with primordial cellcomponent: a group of aggressive lesions sharing insular,
trabecular, and solid pattern. Am J Surg Pathol 1993; 17: 291–301.
28 Pilotti S, Collini P, Manzari A, Marubini E, Rilke F. Poorly dif-ferentiated forms of papillary thyroid carcinoma: distinctive enti-ties or morphological patterns? Sem Diagn Pathol 1995; 12:249–55.
29 Sasaki A, Tsutomu D, Kashima K, Yokoyama S, Nakayama I,Noguchi S. Insular component as a risk factor of thyroid carci-noma. Pathol Int 1996; 46: 939–46.
30 Sobrinho-Simoes M, Nesland JM, Johannessen JV. Columnar-cell carcinoma. Another variant of poorly differentiated carci-noma of the thyroid. Am J Clin Pathol 1998; 89: 264–7.
31 Sobrinho-Simoes M. Poorly differentiated carcinomas of thethyroid. Endocr Pathol 1996; 7: 99–102.
32 Van den Brekel MWM, Hekkenberg RJ, Asa SL, Tomlinson G,Rosen IB, Freeman JL. Prognostic features in tall cell papillarycarcinoma and insular thyroid carcinoma. Laryngoscope 1997;107: 254–9.
33 Kakudo K, Itatani H, Uematsu K. Non-papillary carcinoma insitu of the urinary bladder. An electron microscopic study. ActaPathol Jpn 1984; 34: 345–54.
34 Tallini G, Garcia-Rostan G, Herrero A et al. Downregulation ofp27KIP1 and Ki-67/Mib1 labeling index support the classifica-tion of thyroid carcinoma into prognostically relevant categories.Am J Surg Pathol 1999; 23: 678–85.
35 Gerdes J, Lemke H, Baisch H, Wacker H, Schwab U, Stein H.Cell cycle analysis of a cell proliferation-associated humannuclear antigen defined by the monoclonal antibody Ki-67. JImmunol 1985; 133: 1710–15.
36 Yoshida A, Nakamura Y, Imada T, Asaga T, Shimizu A, HaradaM. Apoptosis and proliferative activity in thyroid tumors. SurgToday 1999; 29: 204–8.
37 Terada T, Maeta H, Endo K, Ohta T. Protein expression of dou-ble-stranded RNA-activated protein kinase in thyroid carcino-mas: correlation with histological types, and Ki-67 labeling.Hum Pathol 2000; 31: 817–21.
38 Erickson LA, Yousef OM, Jin L, Lohse CM, Pankratz VS, LloydRV. p27kip1 expression distinguishes papillary hyperplasia inGrave’s diseases from papillary thyroid carcinoma. Mod Pathol2000; 13: 1014–19.
39 Yang Q, Mori I, Shan L et al. Biallalic Inactivation of retinoic acidreceptor,2 gene by epigenetic change in breast cancer. Am JPathol 2001; 158: 299–303.
40 Mori I, Yang Q, Kakudo K. Predictive and prognostic markers forinvasive breast cancer. Pathol Int 2002; 52: 186–94.
Related Documents