Differentiating Differentiating Dementia, Mild Dementia, Mild Cognitive Impairment, Cognitive Impairment, and Depression: and Depression: Neuropsychological Neuropsychological Perspective Perspective Emily Trittschuh, PhD Geriatric Research Education and Clinical Center (GRECC) VA Puget Sound Health Care System [email protected] Dept of Psychiatry and Behavioral Sciences University of Washington

Differentiating Dementia, Mild Cognitive Impairment, and Depression: Neuropsychological Perspective Emily Trittschuh, PhD Geriatric Research Education.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Differentiating Differentiating Dementia, Mild Dementia, Mild Cognitive Impairment, Cognitive Impairment, and Depression: and Depression: Neuropsychological PerspectiveNeuropsychological Perspective
Emily Trittschuh, PhDGeriatric Research Education and Clinical Center (GRECC)VA Puget Sound Health Care [email protected]
Dept of Psychiatry and Behavioral SciencesUniversity of Washington

Learning Objectives
Characterize Dementia, Mild Cognitive Impairment, and Depression in Older Adults
Recognize warning signs and initiate diagnostic work-up
Understand components of a Neuropsychological Evaluation
Cognitive Profiles – unique/overlapping features Utilizing this information to guide treatment and care
planning

The Aging Population
Older Americans represent ~12 % of the population. 26% percent of physician office visits A third of all hospital stays and of all prescriptions Almost 40 % of all emergency medical responses 90 % of nursing home residents
In 2011, the first baby boomers will reach their 65th birthdays. By 2029, all baby boomers will be at least 65 years old. This group will join the rest of older adults to total an estimated
70 million people aged 65 and older.
*As reported by the Alzheimer’s Association in 2010

“Typical” Cognitive Aging
Autobiographical memory Recall of well-learned information Procedural and Episodic Memory Emotional processing
Encoding of new memories Slower to learn new tasks
Working memory May need more repetitions to learn new info
Processing speed Slower to respond to novel situations

What you might hear in clinic
I can’t focus She’s not interested in her usual activities I can’t come up with the word I want My energy is low My short-term memory is shot I lost my car in the parking lot My husband’s “selective attention” is worse – he
doesn’t listen to me
Dementia
A decline of cognitive ability and/or comportment . . . primary and progressive due to a structural or chemical brain disease Not secondary to sensory deficits, physical
limitations, or psychiatric symptomatology. to the point that customary social, professional and
recreational activities of daily living become compromised.

Probable Alzheimer’s Disease
NINCDS-ADRDA Criteria from 1984 consensus groupNINCDS-ADRDA Criteria from 1984 consensus group
Dementia established by clinical and neuropsychological examination. Explicit memory impairment plus at least 1 other area of
dysfunction. Activities of daily living have been affected.
Insidious onset and progressive course. Risk increases with age; rare onset before age 60 Other diseases capable of producing a dementia
syndrome have been ruled out.

Causes that Mimic Dementia (*but are treatable)
Toxic/metabolicMedications, B12 deficiency, hypothyroidism
Systemic illnessesInfections, cardiovascular disease, pulmonary
OtherDepression, sleep apnea,psychosocial stressors, drugs
*Treatment may improve, but not fully reverse, symptoms

Mill
ions
of
peop
leM
illio
ns o
f pe
ople
0.01.02.03.04.05.06.07.08.09.0
2000 2010 2020 2030 2040 2050
65-74
75-84
85+
Prevalence of AD in the USPrevalence of AD in the US
Hebert, et al, 2003, Archives of NeurologyHebert, et al, 2003, Archives of Neurology

Is it always Alzheimer’s disease?
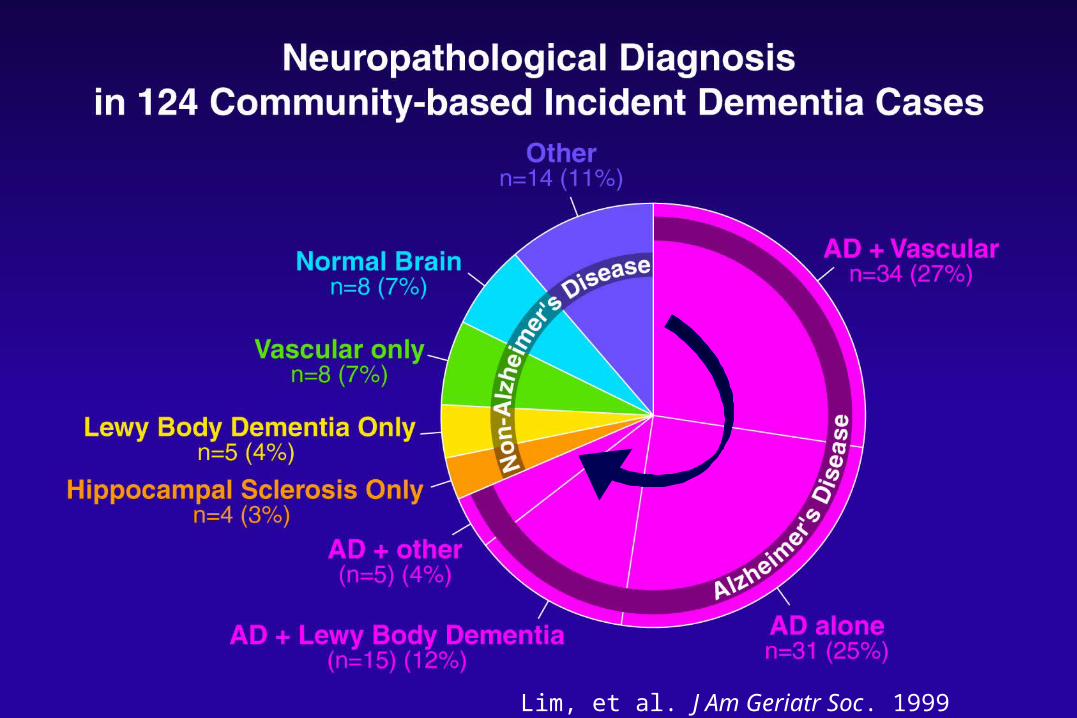
Lim, et al. J Am Geriatr Soc. 1999 May;47(5):564-9.

Objectively measured deficits in memory and/or other thinking abilities
Subjective memory complaint Normal ADLs Prevalence rates vary widely depending on age and community vs clinic
sample
Mild Cognitive Impairment
(Petersen et al., 1999, 2001)(Petersen et al., 1999, 2001)
**** Conversion to dementia is significantly higher in Conversion to dementia is significantly higher in people with MCIpeople with MCI
MCI MCI 12 - 15% per year12 - 15% per yearNormal controlsNormal controls 1 - 2% per year 1 - 2% per year

Depression in Older Adults
Mood disorder characterized by: Sadness Guilt, negative self-regard Apathy – loss of motivation, loss of interest Vegetative Symptoms: sleep, appetite, energy Psychomotor changes – agitation or slowing Trouble thinking, concentrating Loss of interest in life; suicidal ideation
Must occur for at least 2 weeks and interfere with daily living Higher prevalence rates of mood disorder in the elderly
DSM-IV and ICD-10 criteria

Medical EvaluationMedical Evaluation History, physicalHistory, physical
Blood tests, brain scansBlood tests, brain scans
Formal Cognitive TestingFormal Cognitive Testing Evaluate relative to others in Evaluate relative to others in
the same age groupthe same age group
When the Veteran has concerns or When the Veteran has concerns or you notice a change . . .you notice a change . . .

If dementia, changes can begin up to 20 years before noticeable by self & others importance of prevention …
Is this “normal aging”? Is it a change?
Clinical presentations can be similar may not be detectable using screening tests
Comprehensive assessment is essential rule out other treatable causes
Diagnostic Challenges Diagnostic Challenges

Clinical Neuropsychology
Integrative approach – psychology, psychiatry, and neurology
Record review History is often the most important diagnostic tool Collateral information is helpful Objective cognitive testing to aid in diagnosis
Multiple domains of cognitive function must be evaluated Importance of using appropriate measures and
appropriate normative data
Geriatric Neuropsychology Tests
Consider age of subject and overall health/energy Consider adjusting measures administered based on referral
question (e.g., first diagnosis vs. current function) Normative populations
Limited normative information for 90+ Non-native English speakers Ethnicity/Cultural differences
Premorbid estimates Individualized benchmark

What is “impaired”?What is “impaired”?
““Gold” standard:Gold” standard: premorbid baseline datapremorbid baseline data
Standard benchmark: Standard benchmark: Compare to the average Compare to the average
performance within an age groupperformance within an age group

-2-2 -1.5-1.5 -1-1 -.5-.5 00 .5.5 11 1.51.5 22-2.5-2.5 2.52.5 33-3-3
Standard deviationsStandard deviations

What is “impaired”?What is “impaired”?
““Gold” standard:Gold” standard: premorbid baseline datapremorbid baseline data
Personal benchmark: Personal benchmark: Compare test results to an Compare test results to an
estimate of premorbid abilitiesestimate of premorbid abilities

-2-2 -1.5-1.5 -1-1 -.5-.5 00 .5.5 11 1.51.5 22-2.5-2.5 2.52.5 33-3-3
Standard deviationsStandard deviations

Clinical Symptoms of Cognitive Decline
Memory loss is often the most commonly reported symptom: Forgetfulness Repeats self in conversation Asks the same questions over and over Gets lost in familiar areas Can’t seem to learn new information (routes, tasks,
how to use a new appliance or electronics)

Clinical Symptoms cont . . .
Presenting symptoms can also consist of changes in one or more of these areas: Attention Language Visuospatial abilities Executive function Personality/judgment/behavior
Impairments in Attention
• Starting jobs but not finishing them
• Absentmindedness
• Difficulty following a conversation
• Distractibility
• Losing train of thought

• Problems expressing one’s thoughts in conversation (can’t find the right words)
• Consistently misusing words
• Trouble spelling and/or writing
• Difficulty understanding conversation
Impairments in Language

Impairments in Visuospatial Function
• Getting turned around (even in one’s own home)
• Trouble completing household chores (using knobs or dials)
• Difficulty getting dressed
• Trouble finding items in full view
• Misperceiving visual input

Impairments in Executive Function
• Disorganization
• Poor planning
• Decreased multi-tasking
• Perseveration
• Decreased ability to think abstractly
Changes in Personality or Comportment
Quantitative change in behavior: Increase- disinhibition, impulsivity, poor self-
regulation, socially inappropriate Decrease- flat affect, reduced initiative, lack of
concern, lack of interest in social activities (often initially mistaken for depression)
Behavior not typical of premorbid personality
Case Example: Key Features
68-year-old, r-handed, AA female
Master’s degree; Associate dean
No significant past medical history
Referred from primary care MD for complaints of memory loss
Insidious onset, seems progressive
Symptom History at Initial Visit
2 year decline in memory
Social skills maintained
Living alone, independent in all ADLs
Collateral endorsed a change

MILDMILD
NORMALNORMAL
SEVERESEVERE
AttentionMood Lang Spatial Memory ADLsExecutive
Neurocognitive Profile - MCINeurocognitive Profile - MCI
MODERATEMODERATE
Initial:Initial:(2 yr after onset)(2 yr after onset)
Changes at Second Visit
Sense of progression
Social skills maintained
Still living alone; independent for basic ADLs
Changes in IADLs
Having trouble driving (minor accidents; got lost)
Trouble managing medications

MILDMILD
NORMALNORMAL
SEVERESEVERE
AttentionMood Lang Spatial Memory ADLsExecutive
Neurocognitive Profile - DementiaNeurocognitive Profile - Dementia
MODERATEMODERATE
Initial:Initial:(2 yr after onset)(2 yr after onset)
1st F/U:1st F/U:(3 yr after onset)(3 yr after onset)
2nd F/U:2nd F/U:(5 yr after onset)(5 yr after onset)

MILDMILD
NORMALNORMAL
SEVERESEVERE
AttentionMood Lang Spatial Memory ADLsExecutive
Neurocognitive Profile - MCINeurocognitive Profile - MCI
MODERATEMODERATE
Initial:Initial:(2 yr after onset)(2 yr after onset)
1st F/U:1st F/U:(3 yr after onset)(3 yr after onset)
2nd F/U:2nd F/U:(5 yr after onset)(5 yr after onset)

Symptom History at Initial Visit 2 year decline in memory; collateral notes change
Affective Changes
Loss of interest in normal activities
Sadness and decreased social network
Living alone, independent in basic ADLs
IADLs
Sometimes forgets medication dosages
a few examples of inattention while driving

MILDMILD
NORMALNORMAL
SEVERESEVERE
AttentionMood Lang Spatial Memory ADLsExecutive
Neurocognitive Profile - DepressionNeurocognitive Profile - Depression
MODERATEMODERATE
Initial:Initial:(2 yr after onset)(2 yr after onset)
Tx x 1 yr:Tx x 1 yr:(Incomplete remission)(Incomplete remission)
Tx x 1 yr:Tx x 1 yr:(Effective)(Effective)

Complicating issues
Chronic depression is a risk factor for dementia Reported rates of depression in dementia range from
0-86% of cases Recent meta-analysis found 50% prevalence Discriminating depression from dementia is even more
challenging in non-AD dementias With the trajectory of MCI unknown, the relationship to
depression is less clear Depression may indicate prodromal dementia

Treatment and Care Planning
DementiaNo cure and the causes are not entirely
understoodEffective intervention = improve functional
status to a degree discernable to caregivers or health care providers
In the case of a progressive disorder, “improvement” = slower decline

Current FDA-Approved Medications Acetylcholinesterase Inhibitors
tacrine Cognex® hepatotoxic
donepezil Aricept® 1 month
galantamine Razadyne® 4 months
rivastigmine Exelon® 4 months; patch
NMDA receptor antagonist
memantine Namenda® 1 month; approved for mod-severe AD
Adjunct Therapies (off label) Antidepressants
Antipsychotics
SSRIs, mirtazapine
risperidone, quetiapine

Environment Genetic
AGEAGE
Neuronal and Synaptic dysfunction
Cognitive DeclineAlzheimer’s Disease Diagnosis
Alzheimer’s pathology NFTs
Amyloid Plaques
Head Injury, Depression, Female,
Presence of APOE e4 allele Chronic Illness
Risk
Factors

NormalNormal MCIMCI DementiaDementia
An ideal point of An ideal point of intervention?intervention?
Mild Cognitive ImpairmentMild Cognitive Impairment

Risk Factors that can be Managed or Risk Factors that can be Managed or AvoidedAvoided
Medical ConditionsMedical Conditions
High Blood PressureHigh Blood Pressure
High CholesterolHigh Cholesterol
Type II DiabetesType II Diabetes
Nutrition/DietNutrition/Diet
Alcohol / TobaccoAlcohol / Tobacco
ExerciseExercise
StressStress
SocializationSocialization
Behavioral FactorsBehavioral Factors

Older adults (>55 yrs) with diabetes have a 65% increased risk of developing Alzheimer’s disease (compared to those without diabetes)
Adults with diabetes havelower scores on cognitive tests
Type II Diabetes
Bennett, et al. Religious Orders Study. Archives of Neurology, 2004
Depression in the Elderly
Depression is not a normal part of aging Estimated that only 10% of Older Adults with
depression receive treatment Suicide rates – higher in the elderly and higher
in Veteran populations Risk of cognitive decline should be monitored

Dementia?
Mild Cognitive Impairment?
Depression?
Superman in his later years
Dang! . . . Now where
was I going?

Related Documents