Review Different physical treatment modalities for lymphoedema developing after axillary lymph node dissection for breast cancer: A review Nele Devoogdt a,b,c, *, Marijke Van Kampen a,b , Inge Geraerts a,b , Tina Coremans c , Marie-Rose Christiaens d a Department Physiotherapy, University Hospitals Leuven, Belgium b Faculty of Kinesiology and Rehabilitation Sciences, Katholieke Universiteit Leuven, Belgium c Department of Health Care Sciences, University College of Antwerp, Belgium d Multidisciplinary Breast Center, University Hospitals Leuven, Belgium Contents 1. Introduction ....................................................................................................... 4 2. Materials and methods .............................................................................................. 4 3. Results ........................................................................................................... 4 3.1. Combined Physical Therapy ..................................................................................... 4 3.1.1. Skin care ............................................................................................ 7 3.1.2. Manual Lymphatic Drainage ............................................................................. 7 3.1.3. Exercises ............................................................................................ 7 3.1.4. Multi-layer bandaging .................................................................................. 7 3.1.5. Compression sleeve .................................................................................... 7 3.2. Intermittent Pneumatic Compression ............................................................................. 8 European Journal of Obstetrics & Gynecology and Reproductive Biology 149 (2010) 3–9 ARTICLE INFO Article history: Received 8 February 2009 Received in revised form 18 November 2009 Accepted 19 November 2009 Keywords: Breast cancer Lymphoedema Combined Physical Therapy Intermittent Pneumatic Compression Elevation ABSTRACT The purpose of this article is to provide a systematic review of Combined Physical Therapy, Intermittent Pneumatic Compression and arm elevation for the treatment of lymphoedema secondary to an axillary dissection for breast cancer. Combined Physical Therapy starts with an intensive phase consisting of skin care, Manual Lymphatic Drainage, exercises and bandaging and continues with a maintenance phase consisting of skin care, exercises, wearing a compression sleeve and Manual Lymphatic Drainage if needed. We have searched the following databases: PubMed/MEDLINE, CINAHL, EMBASE, PEDro and Cochrane. Only (pseudo-) randomised controlled trials and non-randomised experimental trials investigating the effectiveness of Combined Physical Therapy and its different parts, of Intermittent Pneumatic Compression and of arm elevation were included. These physical treatments had to be applied to patients with arm lymphoedema which developed after axillary dissection for breast cancer. Ten randomised controlled trials, one pseudo-randomised controlled trial and four non-randomised experimental trials were found and analysed. Combined Physical Therapy can be considered as an effective treatment modality for lymphoedema. Bandaging the arm is effective, whether its effectiveness is investigated on a heterogeneous group consisting of patients with upper and lower limb lymphoedema from different causes. There is no consensus on the effectiveness of Manual Lymphatic Drainage. The effectiveness of skin care, exercises, wearing a compression sleeve and arm elevation is not investigated by a controlled trial. Intermittent Pneumatic Compression is effective, but once the treatment is interrupted, the lymphoedema volume increases. In conclusion, Combined Physical Therapy is an effective therapy for lymphoedema. However, the effectiveness of its different components remains uncertain. Furthermore, high-quality studies are warranted. The long-term effect of Intermittent Pneumatic Compression and the effect of elevation on lymphoedema are not yet proven. ß 2009 Elsevier Ireland Ltd. All rights reserved. * Corresponding author at: University Hospitals Leuven, Department Physiotherapy, Herestraat 49, 3000 Leuven, Belgium. Tel.: +32 16 348577; fax: +32 16 342186. E-mail address: [email protected] (N. Devoogdt). Contents lists available at ScienceDirect European Journal of Obstetrics & Gynecology and Reproductive Biology journal homepage: www.elsevier.com/locate/ejogrb 0301-2115/$ – see front matter ß 2009 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejogrb.2009.11.016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

European Journal of Obstetrics & Gynecology and Reproductive Biology 149 (2010) 3–9
Review
Different physical treatment modalities for lymphoedema developing afteraxillary lymph node dissection for breast cancer: A review
Nele Devoogdt a,b,c,*, Marijke Van Kampen a,b, Inge Geraerts a,b, Tina Coremans c, Marie-Rose Christiaens d
a Department Physiotherapy, University Hospitals Leuven, Belgiumb Faculty of Kinesiology and Rehabilitation Sciences, Katholieke Universiteit Leuven, Belgiumc Department of Health Care Sciences, University College of Antwerp, Belgiumd Multidisciplinary Breast Center, University Hospitals Leuven, Belgium
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
2. Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
3.1. Combined Physical Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
3.1.1. Skin care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3.1.2. Manual Lymphatic Drainage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3.1.3. Exercises . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3.1.4. Multi-layer bandaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3.1.5. Compression sleeve . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
3.2. Intermittent Pneumatic Compression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
A R T I C L E I N F O
Article history:
Received 8 February 2009
Received in revised form 18 November 2009
Accepted 19 November 2009
Keywords:
Breast cancer
Lymphoedema
Combined Physical Therapy
Intermittent Pneumatic Compression
Elevation
A B S T R A C T
The purpose of this article is to provide a systematic review of Combined Physical Therapy, Intermittent
Pneumatic Compression and arm elevation for the treatment of lymphoedema secondary to an axillary
dissection for breast cancer. Combined Physical Therapy starts with an intensive phase consisting of skin
care, Manual Lymphatic Drainage, exercises and bandaging and continues with a maintenance phase
consisting of skin care, exercises, wearing a compression sleeve and Manual Lymphatic Drainage if
needed.
We have searched the following databases: PubMed/MEDLINE, CINAHL, EMBASE, PEDro and
Cochrane. Only (pseudo-) randomised controlled trials and non-randomised experimental trials
investigating the effectiveness of Combined Physical Therapy and its different parts, of Intermittent
Pneumatic Compression and of arm elevation were included. These physical treatments had to be
applied to patients with arm lymphoedema which developed after axillary dissection for breast cancer.
Ten randomised controlled trials, one pseudo-randomised controlled trial and four non-randomised
experimental trials were found and analysed. Combined Physical Therapy can be considered as an
effective treatment modality for lymphoedema. Bandaging the arm is effective, whether its effectiveness
is investigated on a heterogeneous group consisting of patients with upper and lower limb
lymphoedema from different causes. There is no consensus on the effectiveness of Manual Lymphatic
Drainage. The effectiveness of skin care, exercises, wearing a compression sleeve and arm elevation is not
investigated by a controlled trial. Intermittent Pneumatic Compression is effective, but once the
treatment is interrupted, the lymphoedema volume increases.
In conclusion, Combined Physical Therapy is an effective therapy for lymphoedema. However, the
effectiveness of its different components remains uncertain. Furthermore, high-quality studies are
warranted. The long-term effect of Intermittent Pneumatic Compression and the effect of elevation on
lymphoedema are not yet proven.
� 2009 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
journal homepage: www.e lsev ier .com/ locate /e jogrb
* Corresponding author at: University Hospitals Leuven, Department Physiotherapy, Herestraat 49, 3000 Leuven, Belgium. Tel.: +32 16 348577; fax: +32 16 342186.
E-mail address: [email protected] (N. Devoogdt).
0301-2115/$ – see front matter � 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.ejogrb.2009.11.016
N. Devoogdt et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 149 (2010) 3–94
3.3. Elevation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
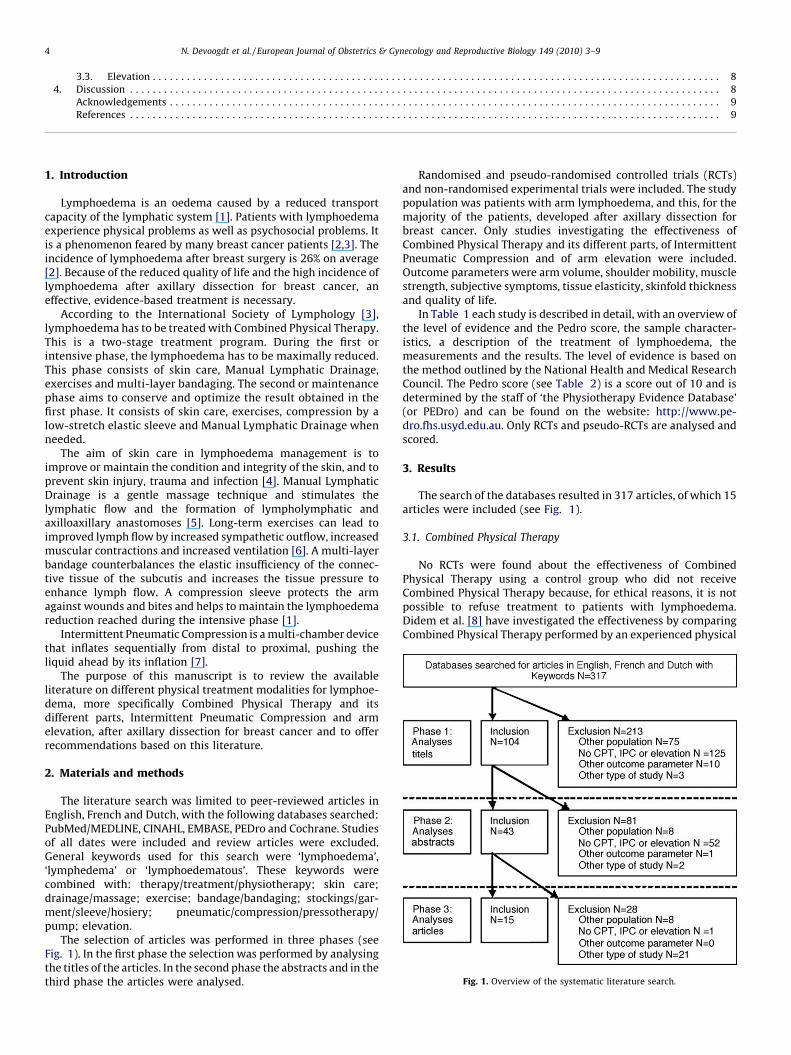
Fig. 1. Overview of the systematic literature search.
1. Introduction
Lymphoedema is an oedema caused by a reduced transportcapacity of the lymphatic system [1]. Patients with lymphoedemaexperience physical problems as well as psychosocial problems. Itis a phenomenon feared by many breast cancer patients [2,3]. Theincidence of lymphoedema after breast surgery is 26% on average[2]. Because of the reduced quality of life and the high incidence oflymphoedema after axillary dissection for breast cancer, aneffective, evidence-based treatment is necessary.
According to the International Society of Lymphology [3],lymphoedema has to be treated with Combined Physical Therapy.This is a two-stage treatment program. During the first orintensive phase, the lymphoedema has to be maximally reduced.This phase consists of skin care, Manual Lymphatic Drainage,exercises and multi-layer bandaging. The second or maintenancephase aims to conserve and optimize the result obtained in thefirst phase. It consists of skin care, exercises, compression by alow-stretch elastic sleeve and Manual Lymphatic Drainage whenneeded.
The aim of skin care in lymphoedema management is toimprove or maintain the condition and integrity of the skin, and toprevent skin injury, trauma and infection [4]. Manual LymphaticDrainage is a gentle massage technique and stimulates thelymphatic flow and the formation of lympholymphatic andaxilloaxillary anastomoses [5]. Long-term exercises can lead toimproved lymph flow by increased sympathetic outflow, increasedmuscular contractions and increased ventilation [6]. A multi-layerbandage counterbalances the elastic insufficiency of the connec-tive tissue of the subcutis and increases the tissue pressure toenhance lymph flow. A compression sleeve protects the armagainst wounds and bites and helps to maintain the lymphoedemareduction reached during the intensive phase [1].
Intermittent Pneumatic Compression is a multi-chamber devicethat inflates sequentially from distal to proximal, pushing theliquid ahead by its inflation [7].
The purpose of this manuscript is to review the availableliterature on different physical treatment modalities for lymphoe-dema, more specifically Combined Physical Therapy and itsdifferent parts, Intermittent Pneumatic Compression and armelevation, after axillary dissection for breast cancer and to offerrecommendations based on this literature.
2. Materials and methods
The literature search was limited to peer-reviewed articles inEnglish, French and Dutch, with the following databases searched:PubMed/MEDLINE, CINAHL, EMBASE, PEDro and Cochrane. Studiesof all dates were included and review articles were excluded.General keywords used for this search were ‘lymphoedema’,‘lymphedema’ or ‘lymphoedematous’. These keywords werecombined with: therapy/treatment/physiotherapy; skin care;drainage/massage; exercise; bandage/bandaging; stockings/gar-ment/sleeve/hosiery; pneumatic/compression/pressotherapy/pump; elevation.
The selection of articles was performed in three phases (seeFig. 1). In the first phase the selection was performed by analysingthe titles of the articles. In the second phase the abstracts and in thethird phase the articles were analysed.
Randomised and pseudo-randomised controlled trials (RCTs)and non-randomised experimental trials were included. The studypopulation was patients with arm lymphoedema, and this, for themajority of the patients, developed after axillary dissection forbreast cancer. Only studies investigating the effectiveness ofCombined Physical Therapy and its different parts, of IntermittentPneumatic Compression and of arm elevation were included.Outcome parameters were arm volume, shoulder mobility, musclestrength, subjective symptoms, tissue elasticity, skinfold thicknessand quality of life.
In Table 1 each study is described in detail, with an overview ofthe level of evidence and the Pedro score, the sample character-istics, a description of the treatment of lymphoedema, themeasurements and the results. The level of evidence is based onthe method outlined by the National Health and Medical ResearchCouncil. The Pedro score (see Table 2) is a score out of 10 and isdetermined by the staff of ‘the Physiotherapy Evidence Database’(or PEDro) and can be found on the website: http://www.pe-dro.fhs.usyd.edu.au. Only RCTs and pseudo-RCTs are analysed andscored.
3. Results
The search of the databases resulted in 317 articles, of which 15articles were included (see Fig. 1).
3.1. Combined Physical Therapy
No RCTs were found about the effectiveness of CombinedPhysical Therapy using a control group who did not receiveCombined Physical Therapy because, for ethical reasons, it is notpossible to refuse treatment to patients with lymphoedema.Didem et al. [8] have investigated the effectiveness by comparingCombined Physical Therapy performed by an experienced physical
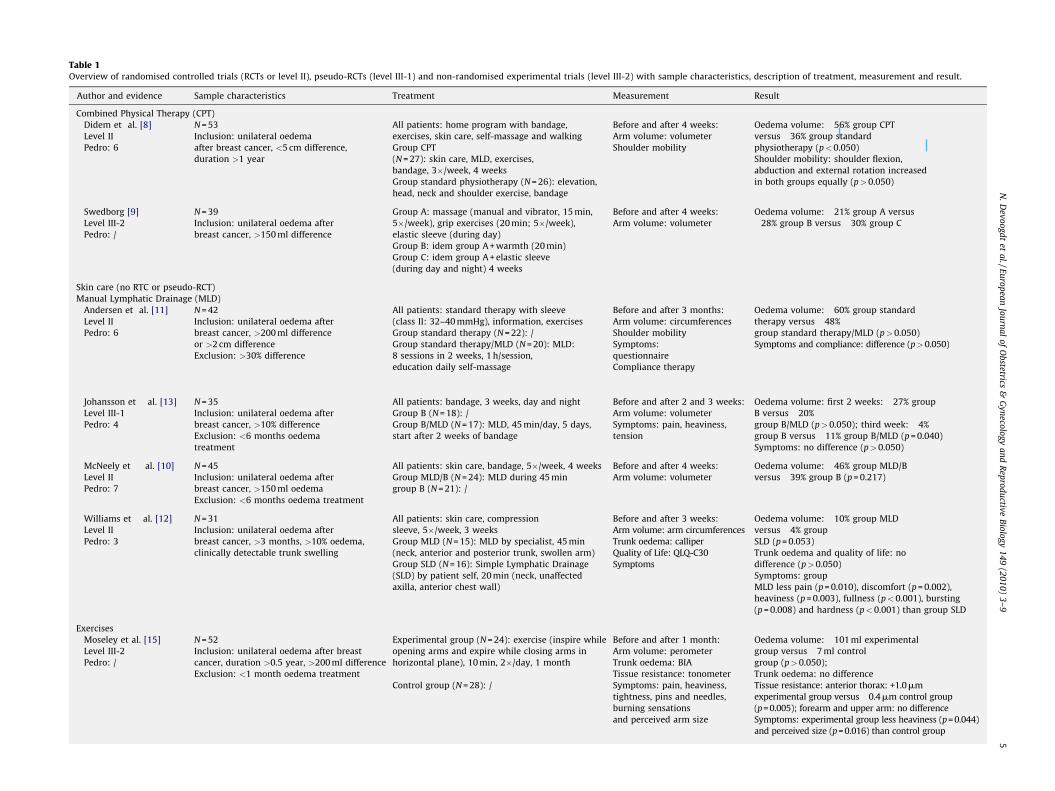
Table 1Overview of randomised controlled trials (RCTs or level II), pseudo-RCTs (level III-1) and non-randomised experimental trials (level III-2) with sample characteristics, description of treatment, measurement and result.
Author and evidence Sample characteristics Treatment Measurement Result
Combined Physical Therapy (CPT)
Didem et al. [8]
Level II
Pedro: 6
N = 53
Inclusion: unilateral oedema
after breast cancer, <5 cm difference,
duration >1 year
All patients: home program with bandage,
exercises, skin care, self-massage and walking
Group CPT
(N = 27): skin care, MLD, exercises,
bandage, 3�/week, 4 weeks
Group standard physiotherapy (N = 26): elevation,
head, neck and shoulder exercise, bandage
Before and after 4 weeks:
Arm volume: volumeter
Shoulder mobility
Oedema volume: �56% group CPT
versus �36% group standard
physiotherapy (p<0.050)
Shoulder mobility: shoulder flexion,
abduction and external rotation increased
in both groups equally (p>0.050)
Swedborg [9]
Level III-2
Pedro: /
N = 39
Inclusion: unilateral oedema after
breast cancer, >150 ml difference
Group A: massage (manual and vibrator, 15 min,
5�/week), grip exercises (20 min; 5�/week),
elastic sleeve (during day)
Group B: idem group A + warmth (20 min)
Group C: idem group A + elastic sleeve
(during day and night) 4 weeks
Before and after 4 weeks:
Arm volume: volumeter
Oedema volume: �21% group A versus
�28% group B versus �30% group C
Skin care (no RTC or pseudo-RCT)
Manual Lymphatic Drainage (MLD)
Andersen et al. [11]
Level II
Pedro: 6
N = 42
Inclusion: unilateral oedema after
breast cancer, >200 ml difference
or >2 cm difference
Exclusion: >30% difference
All patients: standard therapy with sleeve
(class II: 32–40 mmHg), information, exercises
Group standard therapy (N = 22): /
Group standard therapy/MLD (N = 20): MLD:
8 sessions in 2 weeks, 1 h/session,
education daily self-massage
Before and after 3 months:
Arm volume: circumferences
Shoulder mobility
Symptoms:
questionnaire
Compliance therapy
Oedema volume: �60% group standard
therapy versus �48%
group standard therapy/MLD (p>0.050)
Symptoms and compliance: difference (p>0.050)
Johansson et al. [13]
Level III-1
Pedro: 4
N = 35
Inclusion: unilateral oedema after
breast cancer, >10% difference
Exclusion: <6 months oedema
treatment
All patients: bandage, 3 weeks, day and night
Group B (N = 18): /
Group B/MLD (N = 17): MLD, 45 min/day, 5 days,
start after 2 weeks of bandage
Before and after 2 and 3 weeks:
Arm volume: volumeter
Symptoms: pain, heaviness,
tension
Oedema volume: first 2 weeks: �27% group
B versus �20%
group B/MLD (p>0.050); third week: �4%
group B versus �11% group B/MLD (p = 0.040)
Symptoms: no difference (p>0.050)
McNeely et al. [10]
Level II
Pedro: 7
N = 45
Inclusion: unilateral oedema after
breast cancer, >150 ml oedema
Exclusion: <6 months oedema treatment
All patients: skin care, bandage, 5�/week, 4 weeks
Group MLD/B (N = 24): MLD during 45 min
group B (N = 21): /
Before and after 4 weeks:
Arm volume: volumeter
Oedema volume: �46% group MLD/B
versus �39% group B (p = 0.217)
Williams et al. [12]
Level II
Pedro: 3
N = 31
Inclusion: unilateral oedema after
breast cancer, >3 months, >10% oedema,
clinically detectable trunk swelling
All patients: skin care, compression
sleeve, 5�/week, 3 weeks
Group MLD (N = 15): MLD by specialist, 45 min
(neck, anterior and posterior trunk, swollen arm)
Group SLD (N = 16): Simple Lymphatic Drainage
(SLD) by patient self, 20 min (neck, unaffected
axilla, anterior chest wall)
Before and after 3 weeks:
Arm volume: arm circumferences
Trunk oedema: calliper
Quality of Life: QLQ-C30
Symptoms
Oedema volume: �10% group MLD
versus �4% group
SLD (p = 0.053)
Trunk oedema and quality of life: no
difference (p>0.050)
Symptoms: group
MLD less pain (p = 0.010), discomfort (p = 0.002),
heaviness (p = 0.003), fullness (p<0.001), bursting
(p = 0.008) and hardness (p<0.001) than group SLD
Exercises
Moseley et al. [15]
Level III-2
Pedro: /
N = 52
Inclusion: unilateral oedema after breast
cancer, duration >0.5 year, >200 ml difference
Exclusion: <1 month oedema treatment
Experimental group (N = 24): exercise (inspire while
opening arms and expire while closing arms in
horizontal plane), 10 min, 2�/day, 1 month
Control group (N = 28): /
Before and after 1 month:
Arm volume: perometer
Trunk oedema: BIA
Tissue resistance: tonometer
Symptoms: pain, heaviness,
tightness, pins and needles,
burning sensations
and perceived arm size
Oedema volume: �101 ml experimental
group versus �7 ml control
group (p>0.050);
Trunk oedema: no difference
Tissue resistance: anterior thorax: +1.0mm
experimental group versus �0.4mm control group
(p = 0.005); forearm and upper arm: no difference
Symptoms: experimental group less heaviness (p = 0.044)
and perceived size (p = 0.016) than control group
N.
Dev
oo
gd
tet
al./E
uro
pea
nJo
urn
al
of
Ob
stetrics&
Gy
neco
log
ya
nd
Rep
rod
uctiv
eB
iolo
gy
14
9(2
01
0)
3–
95
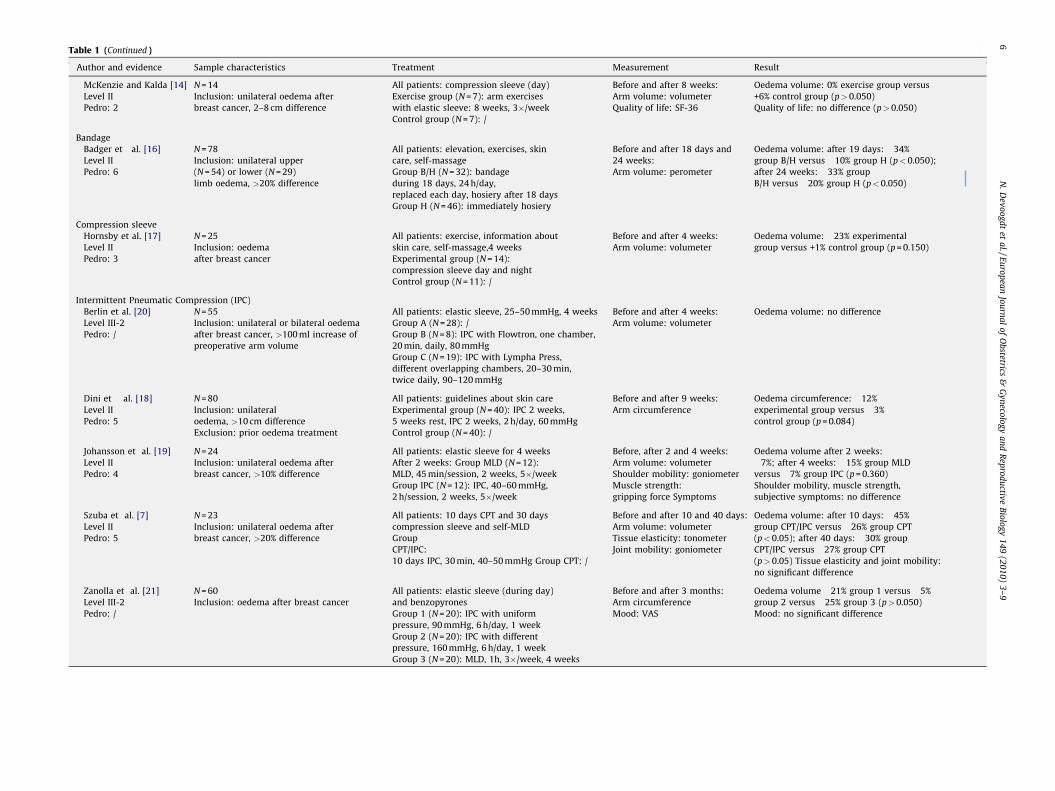
Table 1 (Continued )
Author and evidence Sample characteristics Treatment Measurement Result
McKenzie and Kalda [14]
Level II
Pedro: 2
N = 14
Inclusion: unilateral oedema after
breast cancer, 2–8 cm difference
All patients: compression sleeve (day)
Exercise group (N = 7): arm exercises
with elastic sleeve: 8 weeks, 3�/week
Control group (N = 7): /
Before and after 8 weeks:
Arm volume: volumeter
Quality of life: SF-36
Oedema volume: 0% exercise group versus
+6% control group (p>0.050)
Quality of life: no difference (p>0.050)
Bandage
Badger et al. [16]
Level II
Pedro: 6
N = 78
Inclusion: unilateral upper
(N = 54) or lower (N = 29)
limb oedema, >20% difference
All patients: elevation, exercises, skin
care, self-massage
Group B/H (N = 32): bandage
during 18 days, 24 h/day,
replaced each day, hosiery after 18 days
Group H (N = 46): immediately hosiery
Before and after 18 days and
24 weeks:
Arm volume: perometer
Oedema volume: after 19 days: �34%
group B/H versus �10% group H (p<0.050);
after 24 weeks: �33% group
B/H versus �20% group H (p<0.050)
Compression sleeve
Hornsby et al. [17]
Level II
Pedro: 3
N = 25
Inclusion: oedema
after breast cancer
All patients: exercise, information about
skin care, self-massage,4 weeks
Experimental group (N = 14):
compression sleeve day and night
Control group (N = 11): /
Before and after 4 weeks:
Arm volume: volumeter
Oedema volume: �23% experimental
group versus +1% control group (p = 0.150)
Intermittent Pneumatic Compression (IPC)
Berlin et al. [20]
Level III-2
Pedro: /
N = 55
Inclusion: unilateral or bilateral oedema
after breast cancer, >100 ml increase of
preoperative arm volume
All patients: elastic sleeve, 25–50 mmHg, 4 weeks
Group A (N = 28): /
Group B (N = 8): IPC with Flowtron, one chamber,
20 min, daily, 80 mmHg
Group C (N = 19): IPC with Lympha Press,
different overlapping chambers, 20–30 min,
twice daily, 90–120 mmHg
Before and after 4 weeks:
Arm volume: volumeter
Oedema volume: no difference
Dini et al. [18]
Level II
Pedro: 5
N = 80
Inclusion: unilateral
oedema, >10 cm difference
Exclusion: prior oedema treatment
All patients: guidelines about skin care
Experimental group (N = 40): IPC 2 weeks,
5 weeks rest, IPC 2 weeks, 2 h/day, 60 mmHg
Control group (N = 40): /
Before and after 9 weeks:
Arm circumference
Oedema circumference: �12%
experimental group versus �3%
control group (p = 0.084)
Johansson et al. [19]
Level II
Pedro: 4
N = 24
Inclusion: unilateral oedema after
breast cancer, >10% difference
All patients: elastic sleeve for 4 weeks
After 2 weeks: Group MLD (N = 12):
MLD, 45 min/session, 2 weeks, 5�/week
Group IPC (N = 12): IPC, 40–60 mmHg,
2 h/session, 2 weeks, 5�/week
Before, after 2 and 4 weeks:
Arm volume: volumeter
Shoulder mobility: goniometer
Muscle strength:
gripping force Symptoms
Oedema volume after 2 weeks:
�7%; after 4 weeks: �15% group MLD
versus �7% group IPC (p = 0.360)
Shoulder mobility, muscle strength,
subjective symptoms: no difference
Szuba et al. [7]
Level II
Pedro: 5
N = 23
Inclusion: unilateral oedema after
breast cancer, >20% difference
All patients: 10 days CPT and 30 days
compression sleeve and self-MLD
Group
CPT/IPC:
10 days IPC, 30 min, 40–50 mmHg Group CPT: /
Before and after 10 and 40 days:
Arm volume: volumeter
Tissue elasticity: tonometer
Joint mobility: goniometer
Oedema volume: after 10 days: �45%
group CPT/IPC versus �26% group CPT
(p<0.05); after 40 days: �30% group
CPT/IPC versus �27% group CPT
(p>0.05) Tissue elasticity and joint mobility:
no significant difference
Zanolla et al. [21]
Level III-2
Pedro: /
N = 60
Inclusion: oedema after breast cancer
All patients: elastic sleeve (during day)
and benzopyrones
Group 1 (N = 20): IPC with uniform
pressure, 90 mmHg, 6 h/day, 1 week
Group 2 (N = 20): IPC with different
pressure, 160 mmHg, 6 h/day, 1 week
Group 3 (N = 20): MLD, 1h, 3�/week, 4 weeks
Before and after 3 months:
Arm circumference
Mood: VAS
Oedema volume �21% group 1 versus �5%
group 2 versus �25% group 3 (p>0.050)
Mood: no significant difference
N.
Dev
oo
gd
tet
al./E
uro
pea
nJo
urn
al
of
Ob
stetrics&
Gy
neco
log
ya
nd
Rep
rod
uctiv
eB
iolo
gy
14
9(2
01
0)
3–
96
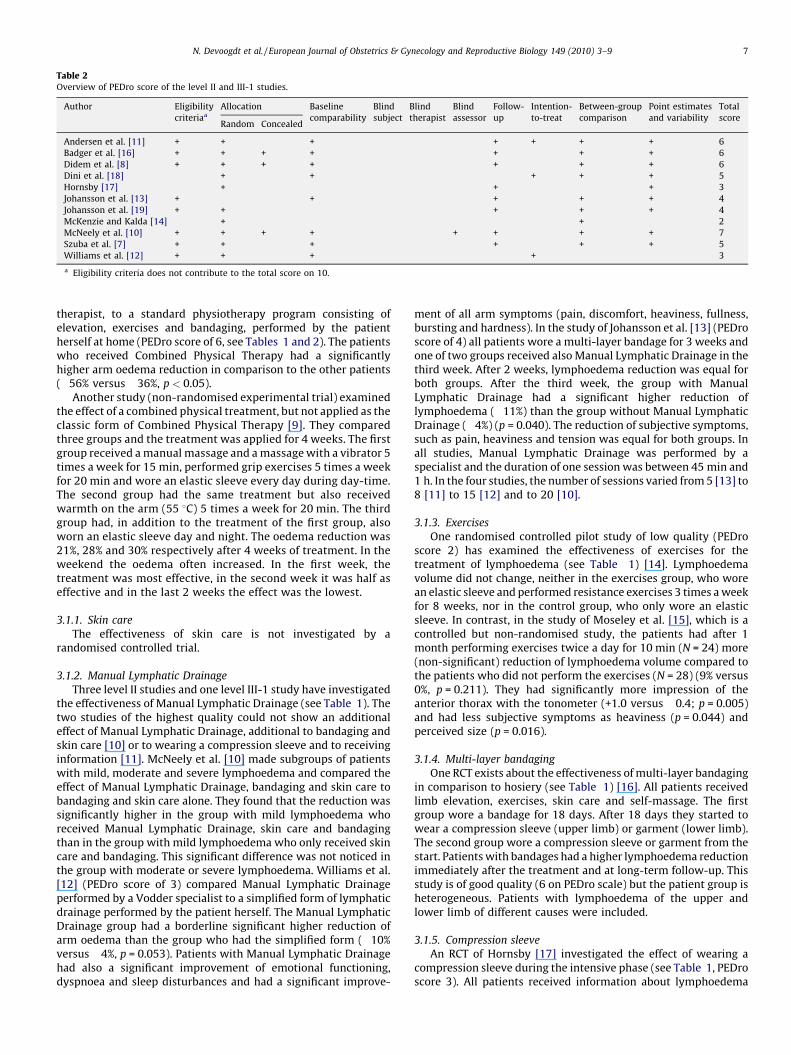
Table 2Overview of PEDro score of the level II and III-1 studies.
Author Eligibility
criteriaa
Allocation Baseline
comparability
Blind
subject
Blind
therapist
Blind
assessor
Follow-
up
Intention-
to-treat
Between-group
comparison
Point estimates
and variability
Total
scoreRandom Concealed
Andersen et al. [11] + + � + � � � + + + + 6
Badger et al. [16] + + + + � � � + � + + 6
Didem et al. [8] + + + + � � � + � + + 6
Dini et al. [18] � + � + � � � � + + + 5
Hornsby [17] � + � � � � � + � � + 3
Johansson et al. [13] + � � + � � � + � + + 4
Johansson et al. [19] + + � � � � � + � + + 4
McKenzie and Kalda [14] � + � � � � � � � + � 2
McNeely et al. [10] + + + + � � + + � + + 7
Szuba et al. [7] + + � + � � � + � + + 5
Williams et al. [12] + + � + � � � � + � � 3
a Eligibility criteria does not contribute to the total score on 10.
N. Devoogdt et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 149 (2010) 3–9 7
therapist, to a standard physiotherapy program consisting ofelevation, exercises and bandaging, performed by the patientherself at home (PEDro score of 6, see Tables 1 and 2). The patientswho received Combined Physical Therapy had a significantlyhigher arm oedema reduction in comparison to the other patients(�56% versus �36%, p < 0.05).
Another study (non-randomised experimental trial) examinedthe effect of a combined physical treatment, but not applied as theclassic form of Combined Physical Therapy [9]. They comparedthree groups and the treatment was applied for 4 weeks. The firstgroup received a manual massage and a massage with a vibrator 5times a week for 15 min, performed grip exercises 5 times a weekfor 20 min and wore an elastic sleeve every day during day-time.The second group had the same treatment but also receivedwarmth on the arm (55 8C) 5 times a week for 20 min. The thirdgroup had, in addition to the treatment of the first group, alsoworn an elastic sleeve day and night. The oedema reduction was21%, 28% and 30% respectively after 4 weeks of treatment. In theweekend the oedema often increased. In the first week, thetreatment was most effective, in the second week it was half aseffective and in the last 2 weeks the effect was the lowest.
3.1.1. Skin care
The effectiveness of skin care is not investigated by arandomised controlled trial.
3.1.2. Manual Lymphatic Drainage
Three level II studies and one level III-1 study have investigatedthe effectiveness of Manual Lymphatic Drainage (see Table 1). Thetwo studies of the highest quality could not show an additionaleffect of Manual Lymphatic Drainage, additional to bandaging andskin care [10] or to wearing a compression sleeve and to receivinginformation [11]. McNeely et al. [10] made subgroups of patientswith mild, moderate and severe lymphoedema and compared theeffect of Manual Lymphatic Drainage, bandaging and skin care tobandaging and skin care alone. They found that the reduction wassignificantly higher in the group with mild lymphoedema whoreceived Manual Lymphatic Drainage, skin care and bandagingthan in the group with mild lymphoedema who only received skincare and bandaging. This significant difference was not noticed inthe group with moderate or severe lymphoedema. Williams et al.[12] (PEDro score of 3) compared Manual Lymphatic Drainageperformed by a Vodder specialist to a simplified form of lymphaticdrainage performed by the patient herself. The Manual LymphaticDrainage group had a borderline significant higher reduction ofarm oedema than the group who had the simplified form (�10%versus �4%, p = 0.053). Patients with Manual Lymphatic Drainagehad also a significant improvement of emotional functioning,dyspnoea and sleep disturbances and had a significant improve-
ment of all arm symptoms (pain, discomfort, heaviness, fullness,bursting and hardness). In the study of Johansson et al. [13] (PEDroscore of 4) all patients wore a multi-layer bandage for 3 weeks andone of two groups received also Manual Lymphatic Drainage in thethird week. After 2 weeks, lymphoedema reduction was equal forboth groups. After the third week, the group with ManualLymphatic Drainage had a significant higher reduction oflymphoedema (�11%) than the group without Manual LymphaticDrainage (�4%) (p = 0.040). The reduction of subjective symptoms,such as pain, heaviness and tension was equal for both groups. Inall studies, Manual Lymphatic Drainage was performed by aspecialist and the duration of one session was between 45 min and1 h. In the four studies, the number of sessions varied from 5 [13] to8 [11] to 15 [12] and to 20 [10].
3.1.3. Exercises
One randomised controlled pilot study of low quality (PEDroscore 2) has examined the effectiveness of exercises for thetreatment of lymphoedema (see Table 1) [14]. Lymphoedemavolume did not change, neither in the exercises group, who worean elastic sleeve and performed resistance exercises 3 times a weekfor 8 weeks, nor in the control group, who only wore an elasticsleeve. In contrast, in the study of Moseley et al. [15], which is acontrolled but non-randomised study, the patients had after 1month performing exercises twice a day for 10 min (N = 24) more(non-significant) reduction of lymphoedema volume compared tothe patients who did not perform the exercises (N = 28) (9% versus0%, p = 0.211). They had significantly more impression of theanterior thorax with the tonometer (+1.0 versus �0.4; p = 0.005)and had less subjective symptoms as heaviness (p = 0.044) andperceived size (p = 0.016).
3.1.4. Multi-layer bandaging
One RCT exists about the effectiveness of multi-layer bandagingin comparison to hosiery (see Table 1) [16]. All patients receivedlimb elevation, exercises, skin care and self-massage. The firstgroup wore a bandage for 18 days. After 18 days they started towear a compression sleeve (upper limb) or garment (lower limb).The second group wore a compression sleeve or garment from thestart. Patients with bandages had a higher lymphoedema reductionimmediately after the treatment and at long-term follow-up. Thisstudy is of good quality (6 on PEDro scale) but the patient group isheterogeneous. Patients with lymphoedema of the upper andlower limb of different causes were included.
3.1.5. Compression sleeve
An RCT of Hornsby [17] investigated the effect of wearing acompression sleeve during the intensive phase (see Table 1, PEDroscore 3). All patients received information about lymphoedema

N. Devoogdt et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 149 (2010) 3–98
and performed exercises, self-massage and skin care during 4weeks. One group also wore a compression sleeve. Lymphoedemareduction was (not significantly) higher in the patient group whowore a compression sleeve compared with the other group (�23%versus +1%, p = 0.150).
No RCT exists about the effectiveness of wearing a compressionsleeve during the maintenance phase.
3.2. Intermittent Pneumatic Compression
Three level II studies exist about the effectiveness of Intermit-tent Pneumatic Compression (see Table 1). In the study of Szubaet al. [7] (PEDro score of 5) all patients received Combined PhysicalTherapy for 10 days. One group also received IntermittentPneumatic Compression for 30 min a day. For the next 30 days,the reduction of lymphoedema was maintained by wearing acompression sleeve and self-drainage for both groups. After 10days, patients with Combined Physical Therapy and IntermittentPneumatic Compression had a significantly higher reduction oflymphoedema volume (�45%) compared to patients who had onlyCombined Physical Therapy (�26%) (p < 0.050). In the mainte-nance phase, the additional effect of Intermittent PneumaticCompression disappeared and after 30 days both groups had equalamount of lymphoedema reduction (�30% versus �27%,p > 0.050). Dini et al. [18] (PEDro score of 5) examined theadditional effect of 20 sessions Intermittent Pneumatic Compres-sion for 2 h a day on skin care. After 9 weeks, patients who hadIntermittent Pneumatic Compression and skin care had a border-line significantly higher lymphoedema reduction (�12%) com-pared to patients who only had skin care (�3%) (p = 0.084). Theydid not follow up their patients further. The third RCT (PEDro scoreof 4) compared the effectiveness of Manual Lymphatic Drainageand wearing a compression sleeve to Intermittent PneumaticCompression and wearing a compression sleeve [19]. After 2weeks, patients with Manual Lymphatic Drainage had anadditional reduction of lymphoedema volume of 15% and patientswith Intermittent Pneumatic Compression had an additionalreduction of 7% (p = 0.360). Furthermore, Berlin et al. [20]performed a non-randomised experimental trial. All patientsreceived a compression sleeve; one group received additionallyone-chamber Intermittent Pneumatic Compression, a secondgroup received multi-chamber Intermittent Pneumatic Compres-sion and these two groups were compared to a third group who didnot receive Intermittent Pneumatic Compression. There was nosignificant difference in lymphoedema reduction between thethree groups. Another non-randomised experimental trial wasperformed by Zanolla et al. [21]. The oedema circumference wassignificantly decreased by 21% in the group with uniformcompression therapy with lower pressure (90 mmHg) and non-significantly decreased by 5% in the group with differentcompression therapy with higher pressure (160 mmHg). Thetherapy was applied during 1 week for 6 h a day. Pressure ofIntermittent Pneumatic Compression ranged between 40 mmHgand 60 mmHg for the level II studies [7,18,19] and between80 mmHg and 160 mmHg for the other studies [20,21].
3.3. Elevation
No controlled study exists about the effectiveness of armelevation for the treatment of lymphoedema.
4. Discussion
This review article gives an overview of the effectiveness of thephysical treatment, i.e. Combined Physical Therapy and itsdifferent parts, Intermittent Pneumatic Compression and arm
elevation, of lymphoedema developing after axillary dissection forbreast cancer.
From 15 studies meeting the inclusion and exclusion criteria,only 11 studies were (pseudo-) randomised controlled trials(RCTs). Moreover, the quality of the major part of the (pseudo-)RCTs was poor. Only 4 of 11 studies had a score of 6 or 7 on thePEDro scale. In none of the studies was the subject or the therapistblinded to the type of treatment. In only one study was the assessorblinded. In addition, in only 3 of 11 studies was the allocation to thetreatment group concealed and in only 3 of 11 studies wereintention-to-treat analyses applied.
It can be supposed that Combined Physical Therapy is aneffective treatment modality for arm lymphoedema developingafter axillary dissection. Patients with Combined Physical Therapyperformed by a specialist had 20% higher reduction of lymphoe-dema volume compared to a placebo Combined Physical Therapyperformed by the patient herself [8]. The quality of this study wasacceptable. According to Swedborg [9] Combined Physical Therapywas most effective the first week and the oedema volumedecreased less towards the end of the fourth week of the intensivetreatment. They also concluded that the treatment sessions shouldpreferably be given daily and breaks at weekends should beavoided. These are findings from only one older study and have tobe confirmed by other studies.
The effectiveness of the different parts of Combined PhysicalTherapy will be successively discussed. The effectiveness of skincare has not been examined by controlled studies. The effect ofexercise on the lymphoedema volume is not obvious. Firstly, a highqualitative RCT is missing. Secondly, the results of two studies withlow quality are conflicting. The effectiveness of Manual LymphaticDrainage is well investigated but there is conflicting evidence. TwoRCTs [10,11] of moderate to high quality do not show an effect ofManual Lymphatic Drainage, whereas results from one RCT [12]and one pseudo-RCT [13], both of low quality, show an additionalbeneficial effect from Manual Lymphatic Drainage on lymphoe-dema volume reduction. McNeely et al. [10], although finding nooverall beneficial effect from Manual Lymphatic Drainage,analysed subgroups of patients and found that patients with mildlymphoedema in the group with Manual Lymphatic Drainage had alarger reduction than patients with mild lymphoedema in thegroup without Manual Lymphatic Drainage. So, based on theconflicting findings among these studies, further study iswarranted to determine the relative benefit of Manual LymphaticDrainage. Hornsby [17] could not statistically prove the effective-ness of a compression sleeve for the treatment of lymphoedema.The study was of low quality and they included a limited number ofpatients (N = 25). Badger et al. [16] have proven in a moderatequality study the effectiveness of bandaging and this in compari-son with hosiery. This study included patients with all differentcauses of lymphoedema of both the lower and the upper limb. So,the exact effect of bandaging on lymphoedema developing afteraxillary dissection for breast cancer is not known. There exists noscientific evidence to support or refute the use of a compressionsleeve during the maintenance phase of Combined PhysicalTherapy.
The effectiveness of Intermittent Pneumatic Compression iswell investigated. Two RCTs, both of moderate quality, showed asignificant short-term effect of Intermittent Pneumatic Compres-sion on lymphoedema reduction [7,18] but in the long term, theeffect could not be maintained [7]. Another study concluded thatIntermittent Pneumatic Compression is as effective as ManualLymphatic Drainage [19].
Due to a lack of high-quality studies it is difficult to makeconclusions and offer recommendations about the differentphysical treatment modalities discussed in this review. Oneplacebo-controlled study of moderate quality has proven that

N. Devoogdt et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 149 (2010) 3–9 9
Combined Physical Therapy is effective for the treatment oflymphoedema after axillary dissection for breast cancer. This hasto be further confirmed by other high-quality studies. Scientificevidence on bandaging exists, although the study was of moderatequality and the study group consisted of patients with upper andlower lymphoedema. The effect of bandaging has to be furtherexamined on only breast cancer patients with arm lymphoedema.Further research on the effectiveness of skin care, exercises andwearing an elastic sleeve is necessary. Two studies with acceptablequality could not prove the effectiveness of Manual LymphaticDrainage, so this treatment modality also has to be furtherinvestigated. Intermittent Pneumatic Compression is an effectivetreatment modality for lymphoedema at short term. These studieswere of moderate quality. High-quality studies with long-termapplication of Intermittent Pneumatic Compression at lowerpressures are needed.
Requirements for new studies are high-quality randomisedcontrolled trials in which enough patients are included, in which apower analysis is performed, in which besides the lymphoedemavolume the arm symptoms and quality of life are also analysed andin which subgroups of patients with lymphoedema are analysed.
Acknowledgements
None.
References
[1] Foldi E, Foldi M, Clodius L. The lymphedema chaos: a lancet. Ann Plast Surg1989;22:505–15.
[2] Erickson VS, Pearson ML, Ganz PA, Adams J, Kahn KL. Arm edema in breastcancer patients. J Natl Cancer Inst 2001;93:96–111.
[3] The diagnosis and treatment of peripheral lymphedema. Consensus documentof the International Society of Lymphology. Lymphology 2003;36:84–91.
[4] MacLaren JA. Skin changes in lymphoedema: pathophysiology and manage-ment options. Int J Palliat Nurs 2001;7:381–8.
[5] Ferrandez JC, Laroche JP, Serin D, Felix-Faure C, Vinot JM. Lymphoscintigraphicaspects of the effects of manual lymphatic drainage. J Mal Vasc 1996;21:283–9.
[6] Lane K, Worsley D, McKenzie D. Exercise and the lymphatic system: implica-tions for breast-cancer survivors. Sports Med 2005;35:461–71.
[7] Szuba A, Achalu R, Rockson SG. Decongestive lymphatic therapy for patientswith breast carcinoma-associated lymphedema. A randomized, prospectivestudy of a role for adjunctive intermittent pneumatic compression. Cancer2002;95:2260–7.
[8] Didem K, Ufuk YS, Serdar S, Zumre A. The comparison of two differentphysiotherapy methods in treatment of lymphedema after breast surgery.Breast Cancer Res Treat 2005;93:49–54.
[9] Swedborg I. Effectiveness of combined methods of physiotherapy for post-mastectomy lymphoedema. Scand J Rehabil Med 1980;12:77–85.
[10] McNeely ML, Magee DJ, Lees AW, Bagnall KM, Haykowsky M, Hanson J. Theaddition of manual lymph drainage to compression therapy for breast cancerrelated lymphedema: a randomized controlled trial. Breast Cancer Res Treat2004;86:95–106.
[11] Andersen L, Hojris I, Erlandsen M, Andersen J. Treatment of breast-cancer-related lymphedema with or without manual lymphatic drainage—a random-ized study. Acta Oncol 2000;39:399–405.
[12] Williams AF, Vadgama A, Franks PJ, Mortimer PS. A randomized controlledcrossover study of manual lymphatic drainage therapy in women with breastcancer-related lymphoedema. Eur J Cancer Care (Engl) 2002;11:254–61.
[13] Johansson K, Albertsson M, Ingvar C, Ekdahl C. Effects of compression bandag-ing with or without manual lymph drainage treatment in patients withpostoperative arm lymphedema. Lymphology 1999;32:103–10.
[14] McKenzie DC, Kalda AL. Effect of upper extremity exercise on secondarylymphedema in breast cancer patients: a pilot study. J Clin Oncol 2003;21:463–6.
[15] Moseley AL, Piller NB, Carati CJ. The effect of gentle arm exercise and deepbreathing on secondary arm lymphedema. Lymphology 2005;38:136–45.
[16] Badger CM, Peacock JL, Mortimer PS. A randomized, controlled, parallel-groupclinical trial comparing multilayer bandaging followed by hosiery versushosiery alone in the treatment of patients with lymphedema of the limb.Cancer 2000;88:2832–7.
[17] Hornsby R. The use of compression to treat lymphoedema. Prof Nurse 1995;11:127–8.
[18] Dini D, Del Mastro L, Gozza A, et al. The role of pneumatic compression in thetreatment of postmastectomy lymphedema. A randomized phase III study.Ann Oncol 1998;9:187–90.
[19] Johansson K, Lie E, Ekdahl C, Lindfeldt J. A randomized study comparingmanual lymph drainage with sequential pneumatic compression for treat-ment of postoperative arm lymphedema. Lymphology 1998;31:56–64.
[20] Berlin E, Gjores JE, Ivarsson C, Palmqvist I, Thagg G, Thulesius O. Postmastec-tomy lymphoedema. Treatment and a five-year follow-up study. Int Angiol1999;18:294–8.
[21] Zanolla R, Monzeglio C, Balzarini A, Martino G. Evaluation of the results ofthree different methods of postmastectomy lymphedema treatment. J SurgOncol 1984;26:210–3.
Related Documents











