Differences in Personality Between Sustained Hypertension, Isolated Clinic Hypertension and Normotension JESU ´ S SANZ * , MARI ´ A PAZ GARCI ´ A-VERA, INE ´ S MAGA ´ N, REGINA ESPINOSA and MARI ´ A FORTU ´ N Department of Clinical Psychology, Universidad Complutense de Madrid, Spain Abstract The aim of this study was to determine whether there are differences in personality between hypertension and normotension. Forty-two male patients with essential hypertension were divided into two groups after self-assessment of blood pressure, 18 with sustained hypertension and 24 with isolated clinic (white coat) hypertension, and were compared with 25 men with normotension on Spielberger’s State-Trait Anxiety Inventory and the Jenkins Activity Survey. In line with hypotheses, the sustained hypertensive group showed higher levels of trait anxiety, Type A behaviour pattern, and hard-driving behaviours/ competitiveness than the normotensive group, whereas isolated clinic hypertensives occupied an intermediate position between those two groups. Results provide support to the hypothesised relationship between personality and hypertension and stress the need of distinguishing sustained hypertension from isolated clinic hypertension. Copyright # 2006 John Wiley & Sons, Ltd. Key words: essential hypertension; isolated clinic hypertension; personality; anxiety; Type A behaviour pattern INTRODUCTION The role of personality in the aetiology of essential hypertension has been a major area of research at least since the 30s–40s of the 20th century (Jorgensen, Johnson, Kolodziej, & Scheer, 1996). Meta-analytic reviews of cross-sectional and prospective studies have supported the hypothesis that some personality traits, such as anxiety, anger, defensiveness, affect expression and depression, are associated with essential hypertension and are European Journal of Personality Eur. J. Pers. 21: 209–224 (2007) Published online 7 September 2006 in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/per.605 *Correspondence to: Dr J. Sanz, Departamento de Personalidad, Evaluacio ´n y Psicologı ´a Clı ´nica, Facultad de Psicologı ´a, Universidad Complutense de Madrid, Campus de Somosaguas, 28223 Madrid, Spain. E-mail: [email protected] Contract/grant sponsor: Community of Madrid; contract/grant number: 06/0028/2002. Contract/grant sponsor: Spanish Ministry of Science and Technology; contract/grant number: BSO2003-08321. Copyright # 2006 John Wiley & Sons, Ltd. Received 11 May 2006 Accepted 11 July 2006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Differences in Personality Between SustainedHypertension, Isolated Clinic Hypertension
and Normotension
JESUS SANZ*, MARIA PAZ GARCIA-VERA, INES MAGAN,REGINA ESPINOSA and MARIA FORTUN
Department of Clinical Psychology, Universidad Complutense de Madrid, Spain
Abstract
The aim of this study was to determine whether there are differences in personality between
hypertension and normotension. Forty-two male patients with essential hypertension were
divided into two groups after self-assessment of blood pressure, 18 with sustained
hypertension and 24 with isolated clinic (white coat) hypertension, and were compared
with 25 men with normotension on Spielberger’s State-Trait Anxiety Inventory and the
Jenkins Activity Survey. In line with hypotheses, the sustained hypertensive group showed
higher levels of trait anxiety, Type A behaviour pattern, and hard-driving behaviours/
competitiveness than the normotensive group, whereas isolated clinic hypertensives
occupied an intermediate position between those two groups. Results provide
support to the hypothesised relationship between personality and hypertension and stress
the need of distinguishing sustained hypertension from isolated clinic hypertension.
Copyright # 2006 John Wiley & Sons, Ltd.
Key words: essential hypertension; isolated clinic hypertension; personality; anxiety;
Type A behaviour pattern
INTRODUCTION
The role of personality in the aetiology of essential hypertension has been a major area of
research at least since the 30s–40s of the 20th century (Jorgensen, Johnson, Kolodziej, &
Scheer, 1996). Meta-analytic reviews of cross-sectional and prospective studies have
supported the hypothesis that some personality traits, such as anxiety, anger, defensiveness,
affect expression and depression, are associated with essential hypertension and are
European Journal of Personality
Eur. J. Pers. 21: 209–224 (2007)
Published online 7 September 2006 in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/per.605
*Correspondence to: Dr J. Sanz, Departamento de Personalidad, Evaluacion y Psicologıa Clınica, Facultad dePsicologıa, Universidad Complutense de Madrid, Campus de Somosaguas, 28223 Madrid, Spain.E-mail: [email protected]
Contract/grant sponsor: Community of Madrid; contract/grant number: 06/0028/2002.Contract/grant sponsor: Spanish Ministry of Science and Technology; contract/grant number: BSO2003-08321.
Copyright # 2006 John Wiley & Sons, Ltd.
Received 11 May 2006
Accepted 11 July 2006
predictors of hypertension development (Jorgensen et al., 1996; Rutledge & Hogan, 2002).
However, such associations are small and highly variable, and further studies are warranted
because inconsistent results have been frequently reported. Thus, after analysing the data
of 83 studies and 25 469 participants, Jorgensen et al. (1996) concluded that their ‘results
empirically substantiate the view that research in the personality correlates of BP (blood
pressure) is marked by substantial amount of inconsistency and confusion’ (p. 310). In fact,
such inconsistencies may easily explain that, in Jorgensen et al.’s meta-analysis,
differences in negative affectivity (including anxiety, anger or depression) between higher
and lower blood pressure groups only reached a mean weighted effect size (d ) of 0.07 that,
although statistically significant, did not meet the standard for a small difference in
function of Cohen’s (1988) conventions for effect sizes (d¼ 0.20).
For example, trait anxiety is one of the personality characteristics most often implicated
as being associated with hypertension, but evidence linking trait anxiety to hypertension
remains ambiguous. Several cross-sectional, case-control studies have found that
hypertensive patients exhibit higher levels of trait anxiety than individuals with normal
BP (Calvo Frances, Dıaz Palarea, Ojeda Ojeda, Ramal, & Aleman, 2001; Cicconetti et al.,
1998); however, other studies have failed to show those differences (Steptoe, Melville, &
Ross, 1982, 1984).
Likewise, the data indicating an association between Type A behaviour pattern and
hypertension are inconsistent. In general, there are as many cross-sectional, case-control
studies indicating that normotensive and hypertensive individuals do not differ
significantly in Type A behaviour pattern (Smyth, Call, Hansell, Sparacino, & Strodtbeck,
1978; Steptoe et al., 1984; Theorell et al., 1985) as there are studies showing that
hypertensives have higher levels of Type A behaviour pattern than normotensives
(Ekeberg, Kjeldsen, Eide, & Leren, 1990; Irvine, Garner, Craig, & Logan, 1991; Steptoe
et al., 1982).
The above-mentioned inconsistencies concerning the role of trait anxiety, Type A
behaviour pattern, and, in general, of personality in hypertension are not surprising since
much of the previous work has been methodologically limited by a number of factors,
including the inherent difficulty in measuring BP and, therefore, the troubles in
categorising individuals as having hypertension, and the difficulty in controlling some
possible confounding variables (e.g. the presence of other cardiovascular disorders).
The classification of participants into hypertensive and normotensive groups is a crucial
aspect of cross-sectional, case-control studies examining the relationship of personality
and hypertension. Most studies have used casual BP measurement taken in the clinic as the
standard for that classification. However, there is ample evidence that this standard may not
be a reliable estimation of individuals’ average level of BP over a prolonged time, and that
pressures measured outside the clinic, either by self-measurement or by ambulatory
monitoring, may improve the reliability and validity of such an estimation (Garcıa-Vera,
Labrador, & Sanz, 1999; O’Brien et al., 2003). Thus, persons categorised as having
hypertension on the basis of casual clinic measurements might not be so classified if BP
readings were obtained outside the clinic. In fact, it has been estimated that as many as
25%–30% of all diagnosed patients with hypertension may have isolated clinic (or office)
hypertension (also known as white-coat hypertension), a clinical condition characterised
by persistently elevated clinic BPs in a patient with normal daytime ambulatory or self-
measured BPs (Garcıa-Vera, Sanz, & Labrador, 2000; O’Brien et al., 2003). Since evidence
to date suggests that the cardiovascular risk associated with isolated clinic hypertension is
lower than that of sustained hypertension and similar, or slightly higher, than that of true
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
210 J. Sanz et al.

normotension (Celis & Fagard, 2004; Pickering, 2005), the potential inclusion of
individuals with isolated clinic hypertension in the comparison between persons with
hypertension and persons with normotension is an important confounding factor that might
obscure their differences in personality, and might explain the inconsistency of previous
studies.
On the other hand, many studies examining the potential relationship between
personality characteristics and hypertension have not carefully excluded participants with
other cardiovascular disorders. There is a wide literature providing evidence that
personality traits such as anxiety, Type A behaviour pattern, depression and anger are also
associated with other cardiovascular disorders, especially with coronary heart disease
(Smith & Ruiz, 2002). Therefore, the presence of persons with coronary heart disease in the
normotension group, in the hypertension group or in both groups, could significantly
confuse the relationship between personality and hypertension, and could also explain the
inconsistency of previous studies on this topic.
The aim of this study was to examine whether there are differences in trait anxiety and
Type A behaviour pattern between patients with hypertension and persons with
normotension, in a manner that addresses the concerns described above. Thus, we used
self-measured BPs to distinguish between sustained hypertension and isolated clinic
hypertension, and, second, participants with other cardiovascular disorders were excluded.
On the other hand, an important line of research that tries to resolve the confusing state of
affairs concerning the relationship between Type A behaviour pattern and cardiovascular
disorders is based on the idea, and related empirical findings, that not all components of the
Type A behaviour pattern may be related to cardiovascular disorders, and perhaps only
some components of the multidimensional Type A behaviour pattern are ‘toxic’ (Booth-
Kewley & Friedman, 1987; Dembroski, MacDougall, Costa, & Grandits, 1989; Lyness,
1993). Therefore, in addition to examine differences in a global measure of Type A
behaviour, a secondary aim of this study was to examine whether there are differences
between hypertensives and normotensives in hard-driving behaviours/competitiveness, the
only Type A component that has been found to discriminate between persons with
cardiovascular disorders and healthy persons in previous studies with Spanish samples
(Jenkins, Zyzanski, & Rosenman, 1992). Based on data from the above-mentioned
literature, we hypothesised that sustained hypertensives would be more anxious, more
Type A, and more hard-driving/competitive than normotensives, whereas patients with
isolated clinic hypertension would occupy an intermediate position between sustained
hypertensives and normotensives.
METHOD
Participants
Forty-three male patients diagnosed as having essential hypertension, by their family
physicians, volunteered to participate in a research on behavioural treatment of essential
hypertension (Garcıa-Vera, Labrador, & Sanz, 1997). Potential patients were considered
for the present study if: (a) the diagnosis was confirmed by three readings of either diastolic
BP above 90 mmHg or systolic BP above 140 during three consecutive casual BP
measurement sessions occurring over a 2- or 3-month period in the clinic; (b) they did not
suffer severe psychiatric disturbances; and (c) they did not have other cardiovascular
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 211
disorders. One patient did not return the personality questionnaires, and therefore the final
patient sample was composed of 42 patients with essential hypertension. Based upon the
average self-measured BPs (see procedure) and the upper limit of normal self-measured
BPs proposed by the European Society of Hypertension (O’Brien et al., 2003), patients
were divided into two groups: an isolated clinic hypertension group (self-measured BPs
<135/85 mmHg and clinic BPs � 140/90 mmHg; n¼ 24) and a sustained hypertension
group (self-measured BPs � 135/85 mmHg and clinic BPs � 140/90 mmHg; n¼ 18).
A group of men with normotension was selected from a larger sample of 268 adults
recruited by a ‘snowball’ technique in which psychology undergraduates invited their
relatives to voluntarily participate in a research on personality and high BP. For the present
study, we selected all men out of that sample that met the following criteria: (a) they
reported not having hypertension, not having a history of hypertension, and not taking
antihypertensive medication; (b) their normotension was confirmed by an average clinic
BP below 140/90 mmHg and an average self-measured BP below 135/85 mmHg (see
procedure); (c) they reported not having heart troubles, atherosclerosis or circulation
troubles, and not having had a stroke and (d) their ages ranged from 26 to 69 years
(precisely the age range of the hypertensive patients). Twenty-five men fulfilled these
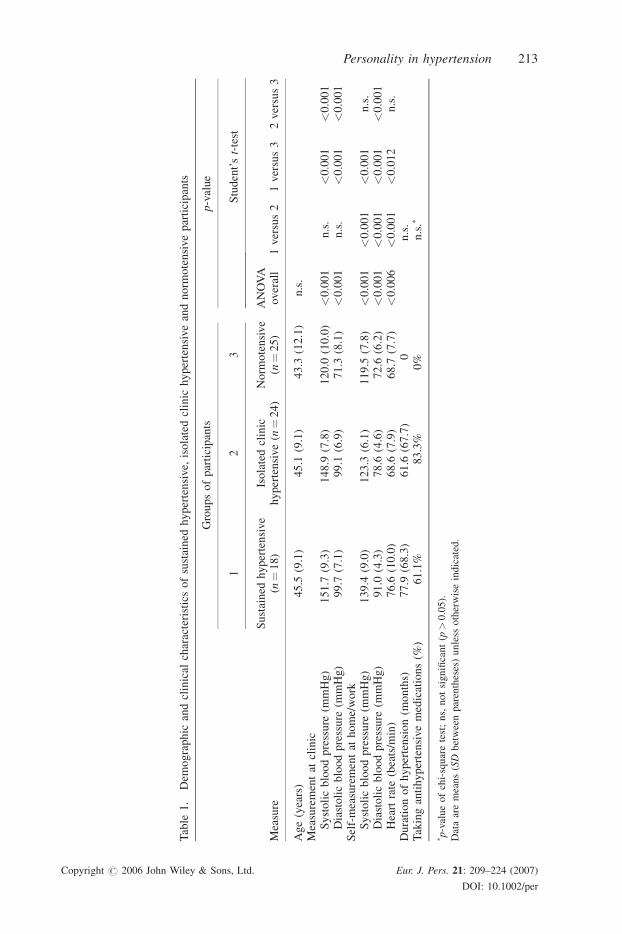
criteria and formed the normotension group. A break down of demographic and clinical
characteristics of the sample of participants for the two hypertension groups and the
normotension group is shown in Table 1.
Apparatus and materials
BP measurement
For patients, clinic BP readings were taken with a RIESTER NOVA mercury
sphygmomanometer. On the other hand, each patient was given an OMRON HEM-
403C digital BP monitor to self-record his/her BP and heart rate. This semi-automatic
device uses an oscillometric method to measure both BP and heart rate. For normal
participants, clinic BP readings were taken with an OMRON 705IT digital BP monitor, and
this same device was given to them to self-record their BP and heart rate. The OMRON
705IT is an automatic device that also uses an oscillometric method to measure both BP
and heart rate. A number of studies support the accuracy of these two digital devices to
measure BP (El Assaad, Topouchian, & Asmar, 2003; Imai et al., 1989; Garcıa-Vera et al.,
1999).
Psychological measurements
State-Trait Anxiety Scale (STAI; Spielberger, Gorsuch, & Lushene, 1970). The STAI
comprises separate 20-item self-report scales for measurement of two distinct anxiety
concepts: trait anxiety and state anxiety. In the present study, we used the trait anxiety
scale. High scores in this scale indicate a greater tendency to respond to situations
perceived as threatening with anxiety. We used the Spanish version of the STAI
(Spielberger, Gorsuch, & Lushene, 1988). Although this version uses for each item a 0–3
response scale instead of the 1–4 response scale of the original, this change does not affect
the reliability or validity of the STAI. For example, with adult samples from the Spanish
general population, Cronbach’s alpha coefficients ranging between 0.84 and 0.86 have
been reported for the Trait Anxiety scale, indicating adequate internal consistency
(Spielberger et al., 1988). In the present sample of participants, the Cronbach’s alpha
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
212 J. Sanz et al.
Tab
le1
.D
emo
gra
ph
ican
dcl
inic
alch
arac
teri
stic
so
fsu
stai
ned
hy
per
ten
sive,
iso
late
dcl
inic
hy
per
ten
sive
and
no
rmo
ten
sive
par
tici
pan
ts
Mea
sure
Gro
up
so
fp
arti
cip
ants
p-v
alu
e
12
3
AN
OV
Aover
all
Stu
den
t’st-
test
Su
stai
ned
hy
per
ten
sive
(n¼
18
)Is
ola
ted
clin
ich
yp
erte
nsi
ve
(n¼
24
)N
orm
ote
nsi
ve
(n¼
25
)1
ver
sus
21
ver
sus
32
ver
sus
3
Ag
e(y
ears
)4
5.5
(9.1
)4
5.1
(9.1
)4
3.3
(12
.1)
n.s
.M
easu
rem
ent
atcl
inic
Sy
sto
lic
blo
od
pre
ssu
re(m
mH
g)
15
1.7
(9.3
)1
48
.9(7
.8)
12
0.0
(10
.0)
<0
.00
1n
.s.
<0
.00
1<
0.0
01
Dia
sto
lic
blo
od
pre
ssu
re(m
mH
g)
99
.7(7
.1)
99
.1(6
.9)
71
.3(8
.1)
<0
.00
1n
.s.
<0
.00
1<
0.0
01
Sel
f-m
easu
rem
ent
ath
om
e/w
ork
Sy
sto
lic
blo
od
pre
ssu
re(m
mH
g)
13
9.4
(9.0
)1
23
.3(6
.1)
11
9.5
(7.8
)<
0.0
01
<0
.00
1<
0.0
01
n.s
.D
iast
oli
cb
loo
dp
ress
ure
(mm
Hg
)9
1.0
(4.3
)7
8.6
(4.6
)7
2.6
(6.2
)<
0.0
01
<0
.00
1<
0.0
01
<0
.00
1H
eart
rate
(bea
ts/m
in)
76
.6(1
0.0
)6
8.6
(7.9
)6
8.7
(7.7
)<
0.0
06
<0
.00
1<
0.0
12
n.s
.D
ura
tio
no
fh
yp
erte
nsi
on
(mo
nth
s)7
7.9
(68
.3)
61
.6(6
7.7
)0
n.s
.T
akin
gan
tihyper
tensi
ve
med
icat
ions
(%)
61.1
%83.3
%0%
n.s
.�
� p-v
alu
eo
fch
i-sq
uar
ete
st;
ns,
no
tsi
gn
ifica
nt
(p>
0.0
5).
Dat
aar
em
ean
s(SD
bet
wee
npar
enth
eses
)unle
ssoth
erw
ise
indic
ated
.
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 213
coefficient for the STAI was 0.87, similar to those obtained in the Spanish normative
samples.
Jenkins Activity Survey, Form C (JAS; Jenkins, Zyzanski, & Rosenman, 1979). The JAS
is a 52-item multiple-choice indicator of Type A-related behaviours. Its four scales give an
overall measurement of Type A behaviour pattern and specific measurements of three of its
components (hard-driving behaviours/competitiveness, speed and impatience and job
involvement), although we only used the Type A behaviour pattern scale (Type A-JAS) and
the hard-driving behaviours/competitiveness scale (Factor H-JAS). We used the Spanish
version of the JAS (Jenkins et al., 1992) whose psychometric properties are similar to those
showed by the original one, with Cronbach’s alpha coefficients of internal consistency of
0.86 for the Type A-JAS scale and of 0.87 for Factor H-JAS scale (Jenkins et al., 1992).
Surprisingly, in the participant sample of this study, the Cronbach’s alpha coefficients of
the Factor H-JAS and Type A-JAS scales were low (0.46 and 0.61, respectively), although
the latter exceeded the threshold of 0.60 proposed by Nunnally (1978) as an acceptable
reliability level for research purposes.
Procedure
Before a patient was referred to Garcıa-Vera et al.’s (1997) study and over a 2- or 3-month
period, three clinic measurements of BP (each measurement being the average of 2–3 clinic
BP readings) were taken by two experienced nurses in the health centre that patients
attended regularly. For patients, clinic BP was the average of those three measurements.
After being referred by their physicians, patients were invited to a two-session individual
assessment of their hypertension. After giving written informed consent for participation,
in the first session patients completed an interview that assessed several variables related to
their hypertension problem (e.g. duration of hypertension, previous treatments). Then,
patients were carefully instructed on how to self-measure and self-record BP readings
correctly, and carried out several practice trials. Patients were given self-recording sheets
that included reminders on how to carry out self-measurement of BP correctly. Patients
were asked to self-measure their BP and heart rate on three occasions per day for 16 days:
two times at home (when getting up in the morning and before bedtime) and one at work. In
each occasion, they obtained one reading. For patients, self-measured BP was the average
of those 48 home and work BP readings. This average allowed to obtain reliable estimates
of BP, with dependability coefficients (G�, analogous to reliability coefficients) higher than
0.90 (Garcıa-Vera & Sanz, 1999). In fact, in this sample, the intra-class correlations (ICC)
for a one-way random effects model (McGraw & Wong, 1996) were 0.98 both for systolic
and for diastolic BP self-measurements. Finally, patients received the JAS to be completed
at home. The study therapist reviewed the specific instructions of the JAS with patients, and
these were asked to schedule a time during the following week to complete the instrument
in a quiet room, free from interruption, ‘so that you can give your entire concentration to fill
out the questionnaire’. The second session of assessment was held 8 days after the first one.
After a psychophysiological assessment, patients received the STAI, and instructions for
BP self-measurement and for completing questionnaires at home were reviewed.
Data from normotensive participants were taken from a larger research on personality
and hypertension. After giving written informed consent for participation, participants
completed an interview that assessed their cardiovascular health and several risk factors
associated with hypertension, and also filled out several personality questionnaires,
including the trait scale of the STAI and the Type A behaviour pattern and hard-driving
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
214 J. Sanz et al.
behaviours/competitiveness scales of the JAS. In addition, six clinic BP readings were
taken by the experimenter with a 2-minute interval between readings. For normotensive
participants, clinic BP was the average of those six BP readings. The ICCs for systolic and
diastolic clinic BP readings were 0.95 and 0.97, respectively. Then, participants were
carefully instructed on how to self-measure and self-record BP readings correctly, and they
carried out several practice trials. These participants were asked to self-measure their BP
two consecutive times (with a 2-minute interval between measurements) on three
occasions per day (on the same occasions as the self-measurement of the patients) for
6 days (36 BP measures in total). In addition, participants were also given self-recording
sheets that included reminders on how to carry out self-measurement of BP correctly. For
normotensive participants, self-measured BP was the average of those 36 home and work
BP readings. This average allowed to obtain reliable estimates of BP, with G� coefficients
higher than 0.90 (Sanz, Garcıa-Vera, Risco, & Magan, 2006). In fact, in this normotensive
sample, the ICCs were 0.97 and 0.98 for systolic and diastolic BP self-measurements,
respectively.
Statistical analyses
Demographic, clinic and personality variables were analysed by one-way ANOVAs with
participant group (sustained hypertensives, isolated clinic hypertensives and normoten-
sives) as between-subjects factor, except for the percentage of medicated patients that was
analysed by Pearson chi-square. When the variances of the dependent variables were not
equal across groups, we used the Welch test as a more robust and conservative alternative to
the usual F-test. When the ANOVA F-tests (or the Welch tests) revealed statistically
significant differences between groups, pairwise comparisons of the group means were
conducted by Student’s t-tests. For personality variables, those t-tests were computed with
Bonferroni adjusted p-values, and effect sizes for pairwise comparisons were measured by
Cohen’s d statistic (the difference between the means divided by the pooled standard
deviation).
RESULTS
Demographic and clinical characteristics
The demographic and clinical characteristics of the three participant groups (sustained
hypertensives, isolated clinic hypertensives and normotensives) are displayed in Table 1.
There were no significant differences between the three participant groups in age (Welch
statistic (2, 40.6)¼ 0.25, n.s.), but, as expected, the three groups significantly differed in
their BP and heart rate measures (all F-tests with p< 0.05). The subsequent t-tests revealed
that sustained and isolated clinic hypertensives did not significantly differ in clinic systolic
and diastolic BPs (both t-tests n.s.), but that both hypertensive groups showed higher levels
of clinic systolic and diastolic BPs than did the normotensive group (all t-tests with
p< 0.05). In contrast, the t-tests also revealed that the sustained hypertensive patients
showed higher levels of self-measured systolic and diastolic BPs and of self-measured
heart rate than did isolated clinic hypertensive and normotensive groups (all t-tests with
p< 0.05), and that these latter groups did not significantly differ in self-measured systolic
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 215

BP and heart rate (all t-tests n.s.), but they significantly differed in self-measured diastolic
BP [t (47)¼ 3.82, p< 0.001].
On the other hand, there were no significant differences between the sustained
hypertensive and the isolated clinic hypertensive groups in such clinical variables as
duration of hypertension [t (40)¼ 0.77, ns] or percentage of patients taking
antihypertensive medication [chi-square (1, N¼ 42)¼ 2.63, ns].
Personality characteristics
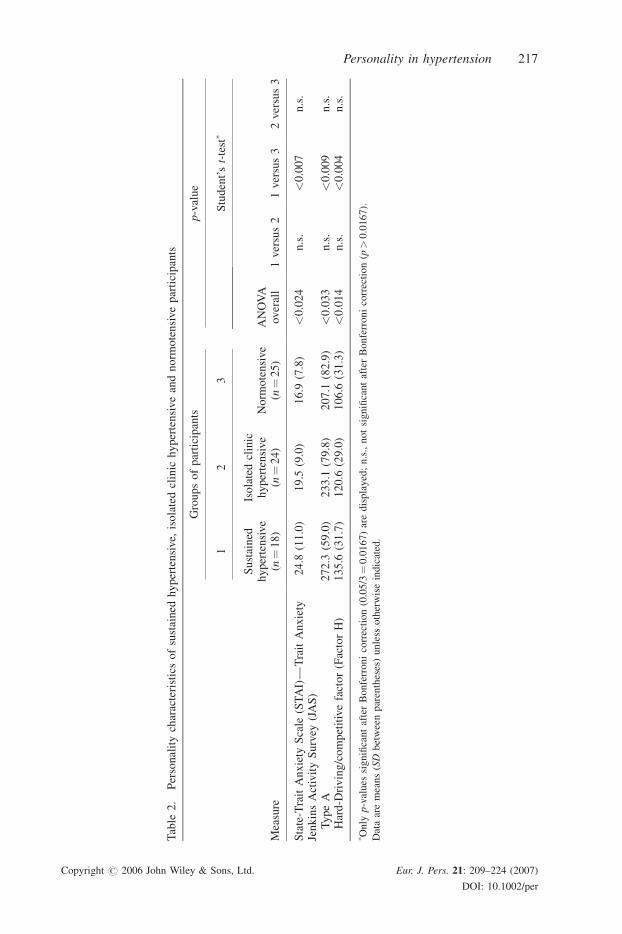
The personality test score means of the three participant groups are presented in Table 2.
Given that the presence of outliers can lead to errors and distortions when using either
parametric or nonparametric tests, we checked for the presence of personality scores
deviated three or more standard deviations from the mean. We did not found any outliers
and, therefore, we conducted one-way ANOVAs for each personality variable. Group
differences on all personality variables were statistically significant (all F-tests with
p< 0.05). Using Bonferroni adjusted p-values, the subsequent t-tests revealed a same
pattern of differences between groups for all personality measures: sustained hypertensives
significantly showed higher levels of trait anxiety, Type A behaviour pattern and hard-
driving behaviours/competitiveness than did the normotensives (all t-tests with p< 0.05),
but both participant groups did not significantly differ from the isolated clinic hypertensive
group. Thus, although isolated clinic hypertensives tended to show lower levels of trait
anxiety, Type A behaviour pattern and hard-driving behaviours/competitiveness than did
the sustained hypertensives (see Table 2), these differences did not reach statistical
significance (all t-tests n.s.). Likewise, although isolated clinic hypertensives tended to
show higher levels of the above-mentioned personality characteristics than did the
normotensives (see Table 2), these differences did not also reach statistical significance (all
t-tests n.s.).
Interestingly, the personality differences between sustained hypertensives and
normotensives not only were statistically significant, but also they were large in terms
of effect size, with d statistics ranged from 0.83 for trait anxiety to 0.90 and 0.92 for Type A
behaviour pattern and hard-driving behaviours/competitiveness, respectively.
Given that isolated clinic hypertensives and normotensives significantly differed in self-
measured diastolic BP, we carried out ANCOVAs with isolated clinic hypertensives versus
normotensives as between-subjects factor and self-measured diastolic BP as covariate, for
each personality variable. The ANCOVAs revealed similar results to those obtained with
the t-tests.
Both JAS scales (Type A-JAS and Factor H-JAS) were significantly intercorrelated
(r¼ 0.60, p< 0.001), whereas the trait anxiety subscale of the STAI did not correlate
significantly with the Type A-JAS (r¼�0.05, n.s.), but it did with the Factor H-JAS
(r¼ 0.25, p< 0.04). Given these significant correlations, to determine whether the
differences in trait anxiety, Type A behaviour pattern and hard-driving behaviours/
competitiveness found in the comparison of sustained hypertensives with normotensives
could be explained by only a subset of these variables, a stepwise discriminant analysis was
conducted. The stepwise discriminant analysis selects the variable that accounts for the
largest amount of variance in defining group membership and, then, includes in the
discriminant function each subsequent variable only if it contributes to additional unique
variance between groups. The stepwise discriminant analysis provided a canonical
discriminant function that significantly distinguished between sustained hypertensives and
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
216 J. Sanz et al.
Tab
le2
.P
erso
nal
ity
char
acte
rist
ics
of
sust
ain
edh
yp
erte
nsi
ve,
iso
late
dcl
inic
hy
per
ten
sive
and
no
rmo
ten
sive
par
tici
pan
ts
Mea
sure
Gro
up
so
fp
arti
cip
ants
p-v
alu
e
12
3
AN
OV
Aover
all
Stu
den
t’st-
test�
Su
stai
ned
hy
per
ten
sive
(n¼
18
)
Iso
late
dcl
inic
hy
per
ten
sive
(n¼
24
)N
orm
ote
nsi
ve
(n¼
25
)1
ver
sus
21
ver
sus
32
ver
sus
3
Sta
te-T
rait
An
xie
tyS
cale
(ST
AI)
—T
rait
An
xie
ty2
4.8
(11
.0)
19
.5(9
.0)
16
.9(7
.8)
<0
.02
4n
.s.
<0
.00
7n
.s.
Jen
kin
sA
ctiv
ity
Su
rvey
(JA
S)
Ty
pe
A2
72
.3(5
9.0
)2
33
.1(7
9.8
)2
07
.1(8
2.9
)<
0.0
33
n.s
.<
0.0
09
n.s
.H
ard
-Dri
vin
g/c
om
pet
itiv
efa
cto
r(F
acto
rH
)1
35
.6(3
1.7
)1
20
.6(2
9.0
)1
06
.6(3
1.3
)<
0.0
14
n.s
.<
0.0
04
n.s
.
� On
lyp-v
alu
essi
gn
ifica
nt
afte
rB
on
ferr
on
ico
rrec
tio
n(0
.05
/3¼
0.0
16
7)
are
dis
pla
yed
;n
.s.,
no
tsi
gn
ifica
nt
afte
rB
on
ferr
on
ico
rrec
tio
n(p>
0.0
16
7).
Dat
aar
em
ean
s(SD
bet
wee
np
aren
thes
es)
un
less
oth
erw
ise
ind
icat
ed.
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 217
nomortensives (Wilks’ lambda¼ 0.63; chi-square¼ 16.48, p< 0.001), allowed one to
correctly classified the 75.6% of the cases, and only included two variables: hard-driving
behaviours/competitiveness and trait anxiety. The standardised coefficients of the
canonical discriminant function indicated that hard-driving behaviours/competitiveness
(0.81) accounted for larger proportion of the variance than trait anxiety (0.58). The fact that
the second variable selected for entry was trait anxiety indicated that the association of
higher trait anxiety with sustained hypertension was not entirely explained by the
significant but weak correlation between the trait anxiety scores and the hard-driving
behaviours/competitiveness scores (r¼ 0.25).
On the other hand, we found low internal consistency indices for the two JAS scales.
Therefore, it may be that the observed between-group differences in these scales provides a
misestimation of the true association of hypertension with Type A behaviour pattern and
hard-driving behaviours/competitiveness. To obtain more reliable measures, we eliminated
the JAS items with low correlations with the total adjusted score of the corresponding scale,
and created two measures of Type A behaviour pattern and hard-driving behaviours/
competitiveness with good internal consistency indices (equal or above the standard of
0.70 for good internal consistency; Nunnally, 1978). Thus, four items from the original
Type A-JAS and nine items from the original Factor H-JAS were eliminated, and both the
resultant 17-item Type A scale and the resultant 11-item Factor H scale reached Cronbach’s
alpha coefficients of 0.70. With these two new scales, we repeated all the statistical
analyses. The results were almost identical to those obtained with the original JAS scales.
DISCUSSION
The aim of this study was to examine whether there are differences in trait anxiety, Type A
behaviour pattern and hard-driving behaviours/competitiveness (a component of Type A
behaviour pattern), between hypertension and normotension, especially when hyperten-
sion is diagnosed based on both clinic and self-measured BPs and, therefore, isolated clinic
hypertension can be detected and controlled. Our first hypothesis was that, in comparison
with normotensives, true hypertensives (sustained hypertensives) could be characterised by
higher levels of those personality traits. Our results revealed statistically significant
differences between sustained hypertensives and normotensives in trait anxiety, Type A
behaviour pattern and hard-driving behaviours/competitiveness, with higher scores in these
personality traits for sustained hypertensives. In fact, these differences in personality
between normotensives and sustained hypertensives were large in function of Cohen’s
(1988) conventions for effect sizes (d> 0.80).
Based on data that indicate that persons with isolated clinic hypertension have a worse or
equal cardiovascular prognosis than normotensives, but a better one than those with
sustained hypertension (Celis & Fagard, 2004; Pickering, 2005), we also hypothesised that
isolated clinic hypertensives would occupy an intermediate position between sustained
hypertensives and normotensives in trait anxiety, Type A behaviour pattern and hard-
driving behaviours/competitiveness. However, this hypothesis was not fully supported by
our results. Although, isolated clinic hypertensives showed higher levels of those
personality characteristics than normotensives, and they also showed lower levels of those
personality characteristics than sustained hypertensives, all these between-group
differences were not statistically significant.
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
218 J. Sanz et al.
In sum, our results support our first hypothesis concerning differences in personality
between normotension and hypertension, and are consistent with those obtained in
previous studies that also support the role of trait anxiety and Type A behaviour pattern in
hypertension (Calvo Frances et al., 2001; Cicconetti et al., 1998; Ekeberg et al., 1990;
Irvine et al., 1991; Steptoe et al., 1982).
Of course, as mentioned in the introduction of this article, there are studies that have
failed to show differences in trait anxiety and Type A behaviour pattern between persons
with normotension and patients with essential hypertension (Smyth et al., 1978; Steptoe
et al., 1982, 1984; Theorell et al., 1985). However, most of these studies (Smyth et al.,
1978; Steptoe et al., 1982, 1984; Theorell et al., 1985) did not used, along with clinic BPs,
out-of-clinic BPs (self-measured or ambulatory BPs) to diagnose hypertension and,
therefore, they were not able to detect and control isolated clinic hypertension. As our
results indicate, the levels of trait anxiety and Type A behaviour pattern of isolated clinic
hypertensives are not statistically distinguishable from those of sustained hypertensives
and normotensives, occupying an intermediate position between these latter groups.
Therefore, the differences in personality between normotension and hypertension could be
obscured by the unnoticed inclusion of isolated clinic hypertensives in the sustained
hypertensive group.
Although sustained hypertensives significantly differed from normotensives on all
personality variables examined in the present study, the results of the discriminant analysis
indicated that trait anxiety and hard-driving behaviours/competitiveness (a component of
Type A behaviour pattern) were the most important personality characteristics to
discriminate between sustained hypertension and normotension, and even though there was
some correlation between the measures of both personality traits, these contributed
independently to that discrimination.
In sum, our results suggest that sustained hypertensives are more prototypical of the
‘hypertensive personality’ than patients whose BP is different in different settings (isolated
clinic hypertension). This difference could explain why research literature on the relations
between personality and hypertension has yielded mixed findings and, although suggestive,
it is far from conclusive. Further studies on this issue should, therefore, distinguish
different types of hypertensive patients based on the observed discrepancies between clinic
and nonclinic measures of BP, and examine differentially not only patients with isolated
clinic and sustained hypertension, but also subjects with normal clinic BP but high self-
measured or ambulatory BPs (which has been termed ‘isolated clinic normotension’,
‘white coat normotension’ or ‘masked hypertension’).
Furthermore, from a clinical viewpoint, there is the need for taking BP readings away
from the medical environment, by self-measurement of BP in the home or work place or by
ambulatory BP measurement using automated devices, in order to identify isolated clinic
hypertension, especially in those cases where the probability of isolated clinic hypertension
is high (clinic systolic BP 140–159 mmHg or diastolic BP 90–99 mmHg, female sex, non-
smokers, hypertension of recent onset, limited number of clinic BP measurements;
O’Brien et al., 2003). Given the high incidence and low risk profile of isolated clinic
hypertension, the consequences of failing to identify this condition are considerable,
because life-long treatment may be prescribed unnecessarily, and if antihypertensive
medication is given to people whose usual BP is normal, they may be made unwell by the
adverse effects of medication. Moreover, given that our results suggest that ‘toxic’
personality traits are more present in sustained hypertension than in isolated clinic
hypertension, it may be that antihypertensive psychological treatments aimed to change
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 219
those personality traits could only benefit to sustained hypertensives, and could be
unnecessary for isolated clinic hypertensives.
On the other hand, it has been hypothesised that patients with isolated clinic
hypertension would be generally more anxious and that it would be their anxiety associated
with clinic visit that would be responsible for elevated clinic BPs (Pickering & Friedman,
1991). We found that isolated clinic hypertensives and sustained hypertensives did not
differ significantly in scores on a well-standardised, widely-used, psychometric test
measuring trait anxiety (the trait anxiety scale of the STAI; see Table 2). Although a
nonsignificant trend was found among isolated clinic hypertensives to show higher levels
of trait anxiety than normotensives, a nonsignificant trend was also found among isolated
clinic hypertensives to show lower levels of trait anxiety than sustained hypertensives.
Therefore, it is clearly safest to conclude that trait anxiety does not play a major role in the
phenomenon of isolated clinic hypertension in light of previous literature showing no
group differences on different anxiety measures (Schneider, Egan, Johnson, Drobny, &
Julius, 1986), including the measure employed in the present study (Gerardi, Blanchard,
Andrasik, & McCoy, 1985; Siegel, Blumenthal, & Divine, 1990).
In conclusion, our results do not support the hypothesis that isolated clinic hypertension
is related to trait anxiety. However, our data do not preclude the possibility that trait anxiety
is related to the white-coat effect. Although isolated clinic hypertension is frequently
confounded with the white-coat effect, they are different phenomena. The white-coat effect
refers to an alerting reaction of the patient to the measurement of BP in the clinic
environment that can be quantified by continuous BP monitoring before and during the
physician’s visit. On the other hand, isolated clinic hypertension is a clinical condition
characterised by persistently elevated clinic BP and normal daytime ambulatory or self-
measured BPs. For a long time, it was assumed that this condition could reflect the
persistence over time of an alerting reaction to the physician’s visit. However, results from
several studies indicate that the difference between office and ambulatory or self-measured
BP values does not correlate with the BP rise induced in the patient by the physician’s visit
(Lantelme, Milon, Vernet, & Gayet, 2000; Palatini et al., 2003). In fact, these results are the
reason for the recommendation, given by the World Health Organization-International
Society of Hypertension (1999), that the condition characterised by persistently high clinic
BP and by persistently normal daytime ambulatory or self-measured BP values should be
named ‘isolated clinic (or office) hypertension’ instead of using the appealing, but
misleading, term ‘white coat hypertension’ (see also Garcıa-Vera et al., 2000). Therefore, it
may be that the white-coat effect could be partially explained by an exaggerated pattern of
anxiety (trait anxiety) to novel or stressful stimuli, whereas isolated clinic hypertension
could be explained by other multiple factors including, for example, factors affecting both
the BP measured in the physician’s office and the BP recorded in real-life conditions.
Future studies should test those hypotheses to determine the conditions and mechanisms
underlying the white-coat effect and isolated clinic hypertension, and, in any case, these
two conditions need to be separately considered to avoid further misunderstandings that
have often occurred in previous literature.
Finally, there are some limitations of this study that should be considered. First, this is a
cross-sectional study and, therefore, its design does not allow to decide whether trait
anxiety, Type A behaviour pattern and hard-driving behaviours/competitiveness are
causing hypertension or vice versa. Further studies should use prospective designs to test
whether, in normotensives, high levels of trait anxiety, Type A behaviour pattern and hard-
driving behaviour/competitiveness predict later incidence of hypertension. Second, this
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
220 J. Sanz et al.
study focused on men and, obviously, this may limit the generalisation of our findings to
women. Therefore, further research is needed to replicate our findings with samples of
hypertensive women. This need is more apparent in the light of findings suggesting that: (1)
hypertension is a growing problem in women, particularly after the fifth to sixth decade of
life (Oparil & Miller, 2005); (2), although no one group seems to be exempt from isolated
clinic hypertension, the probability increases in women (O’Brien et al., 2003) and (3) the
personality traits may be differently related to hypertension in men and women. For
example, although Type A males show fairly consistent cardiovascular responsiveness to
stressful challenges or competition, the findings in women are more equivocal (Matthews
& Haynes, 1986). In a related vein, Type A men, but not women, show elevated
cardiovascular responses during a challenging reaction time test; however, Type A women
show greater cardiovascular increases during a verbally challenging interaction
(MacDougall, Dembroski, & Krantz, 1981). Finally, Type A seems to have different
personality correlates in men and women. For example, women show higher correlation
between Type A and guilt, and men between Type A and suspiciousness (McCann,
Woolfolk, Lehrer, & Schwarcz, 1987). However, there are also a number of empirical
reasons to suppose that personality traits are not differently related to hypertension in men
and women. Perhaps, the most compelling reason is that previous meta-analytic studies on
the relationship between personality and hypertension have found that gender was
unrelated to the magnitude and direction of effect sizes reflecting the association between
personality traits and blood pressure (Jorgensen et al., 1996; Rutledge & Hogan, 2002).
Third, for some comparisons (between sustained hypertensives and isolated clinic
hypertensives, and between isolated clinic hypertensives and normotensives), it may be
that the present study had low statistical power since the three participant groups were
relatively small. Post-hoc analysis of statistical power revealed that, for the
comparisons between sustained hypertensives and isolated clinic hypertensives,
statistical power indices were 0.45 for hard-driving behaviour/competitiveness, 0.51
for trait anxiety, and 0.55 for Type A behaviour pattern. For comparisons between
isolated clinic hypertensives and normotensives, statistical power indices were 0.28 for
trait anxiety, 0.29 for Type A behaviour pattern, and 0.46 for hard-driving behaviour/
competitiveness. These data suggest that further studies should recruit between 84
and 124 participants to have a probability of 80% of correctly rejecting the null
hypothesis of absence of personality differences between sustained hypertensives and
isolated clinic hypertensives, whereas they should recruit between 120 and 318
participants for having a probability of 80% of correctly rejecting the null hypothesis
of absence of personality differences between isolated clinic hypertensives and
normotensives.
On the other hand, further studies would also benefit from the use of a more
comprehensive overarching theoretical framework in conceptualising the relationship
between psychological traits and hypertension. This meta-model would provide a matrix of
interrelated conceptual personality domains to guide research on the relationships between
personality traits and hypertension and to improve conceptual clarity. One such promising
framework is the five-factor model (or Big Five), arguably the most popular and influential
contemporary taxonomy of personality traits. This model suggest that the five dimensions
of neuroticism or emotional stability, extraversion, openness to experience or culture,
agreeableness and conscientiousness summarise and integrate the majority of personality
traits (McCrae & Costa, 1997; Sanz, Silva, & Avia, 1999). Interestingly enough, a number
of studies have already tested the personality dimensions of neuroticism and extraversion
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 221
for association with hypertension (Hozawa et al., 2002; Kohler, Scherbaum, Richter, &
Bottcher, 1993).
ACKNOWLEDGEMENTS
Preliminary analyses based on a subsample of participants of this study were presented as a
poster in the 17th Annual Conference of the European Health Psychology Society (Kos,
Greece; September 24–27, 2003). We thank the other members of the Complutense
University research group on personality and hypertension (Francisco Calabozo, Drissa
Delkader, Marıa Esther Garcıa, Almudena Gomez, Marıa Gomez, Beatriz Huertas, Amaia
Izquierdo, Jose Enrique Lopez, Carolina Munoz, Patricia Pastor, Carolina Perandones,
Elvira Polo, Mercedes Risco and Coral Rojo) for their assistance on the assessment of
normotensive participants.
REFERENCES
Booth-Kewley, S., & Friedman, H. S. (1987). Psychological predictors of heart disease: Aquantitative review. Psychological Bulletin, 101, 343–362.
Calvo Frances, F., Dıaz Palarea, D., Ojeda Ojeda, B., Ramal, J., & Aleman, S. (2001). Diferencias enansiedad, depresion, estres y apoyo social entre sujetos hipertensos y normotensos [Differences inanxiety, depression, stress, and social support between hypertensive and normotensive subjects].Ansiedad y Estres, 7, 203–213.
Celis, H., Fagard, R. H., (2004). White-coat hypertension: A clinical review. European Journal ofInternal Medicine, 15, 348–357.
Cicconetti, P., Thau, F., Bauco, C., Bianchi, A., Fidente, D., Vetta, F., Ettorre, E., & Marigliano, V.(1998). Psychological assessment in the elderly with new mild systolic hypertension. Archives ofGerontology and Geriatrics Suppl., 6, 79–82.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: LawrenceErlbaum Associates.
Dembroski, T. M., MacDougall, J. M., Costa, P. T., & Grandits, G. A. (1989). Components of hostilityas predictors of sudden death and myocardial infarction in the multiple risk factor interventiontrial. Psychosomatic Medicine, 51, 514–522.
Ekeberg, O., Kjeldsen, S. E., Eide, I., & Leren, P. (1990). Childhood traumas and psychosocialcharacteristics of 50-year-old men with essential hypertension. Journal of PsychosomaticResearch, 34, 643–649.
El Assaad, M. A., Topouchian, J. A., & Asmar, R. G. (2003). Evaluation of two devices for self-measurement of blood pressure according to the international protocol: The Omron M5-I and theOmron 705IT. Blood Pressure Monitoring, 8, 127–133.
Garcıa-Vera, M. P., Labrador, F., & Sanz, J. (1997). Stress management training for essentialhypertension:a controlled study. Applied Psychophysiology and Biofeedback, 22, 261–283.
Garcıa-Vera, M. P., Labrador, F., & Sanz, J. (1999). Comparison of clinic, home self-measured, andwork self-measured blood pressures. Behavioral Medicine, 25, 13–22.
Garcıa-Vera, M. P., & Sanz, J. (1999). How many self-measured blood pressure readings are neededto estimate hypertensive patients’ ‘‘true’’ blood pressure? Journal of Behavioral Medicine, 22, 93–113.
Garcıa-Vera, M. P., Sanz, J., & Labrador, F. J. (2000). Proposal for a system of assessment anddiagnosis of essential hypertension in primary health services. Psychology in Spain, 4, 35–54.
Gerardi, R. J., Blanchard, E. B., Andrasik, F., & McCoy, G. C. (1985). Psychological dimensions of’office hypertension’. Behaviour Research and Therapy, 23, 609–612.
Hozawa, A., Ohkubo, T., Tsuji, I., Kikuya, M., Matsubara, M., Suzuki, T., Nagai, K., Kitaoka, H.,Arai, Y., Hosokawa, T., Satoh, H., Hisamichi, S., & Imai, Y. (2002). Relationship between
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
222 J. Sanz et al.
personality and self-measured blood pressure value at home: The Ohasama study. ClinicalExperimental Hypertension, 24, 115–123.
Imai, Y., Abe, K., Sasaki, S., Minami, N., Munakata, M., Sakuma, H., Hashimoto, J., Sekino, H.,Imai, K., & Yoshinaga, K. (1989). Clinical evaluation of semiautomatic and automatic devices forhome blood pressure measurement: Comparison between cuff-oscillometric and microphonemethods. Journal of Hypertension, 7, 983–990.
Irvine, J., Garner, D. M., Craig, H. M., & Logan, A. G. (1991). Prevalence of type A behavior inuntreated hypertensive individuals. Hypertension, 18, 72–78.
Jenkins, C. D., Zyzanski, S. J., & Rosenman, R. H. (1979). Jenkins Activity Survey. New York: ThePsychological Corporation.
Jenkins, C. D., Zyzanski, S. J., & Rosenman, R. H. (1992). Inventario de Actividad de Jenkins (FormaC) [Jenkins Activity Survey, Form C]. Madrid: TEA.
Jorgensen, R. S., Johnson, B. T., Kolodziej, M. E., & Scheer, G. E. (1996). Elevated blood pressureand personality: A meta-analytic review. Psychological Bulletin, 120, 293–320.
Kohler, T., Scherbaum, N., Richter, R., & Bottcher, S. (1993). The relationship between neuroticismand blood pressure reexamined: An investigation of a nonclinical sample of military conscripts.Psychotherapy and Psychosomatics, 60, 100–105.
Lantelme, P., Milon, H., Vernet, M., & Gayet, C. (2000). Difference between office and ambulatoryblood pressure or real white coat effect: Does it matter in term of prognosis? Journal ofHypertension, 18, 383–389.
Lyness, S. A. (1993). Predictors of differences between Type A and B individuals in heart rate andblood pressure reactivity. Psychological Bulletin, 114, 266–295.
MacDougall, J. M., Dembroski, T. M., & Krantz, D. S. (1981). Effects of types of challenge onpressor and heart rate responses in Type A and Type B women. Psychophysiology, 18, 1–9.
Matthews, K. A., & Haynes, S. G. (1986). Type A behavior pattern and coronary disease risk. Updateand critical evaluation. American Journal of Epidemiology, 123, 923–960.
McCann, B. S., Woolfolk, R. L., Lehrer, P. M., & Schwarcz, L. (1987). Gender differences in therelationship between hostility and the type A behavior pattern. Journal of Personality Assessment,51, 355–366.
McCrae, R. R., & Costa, P. T., Jr. (1997). Personality trait structure as a human universal. AmericanPsychologist, 52, 509–516.
McGraw, K. O., & Wong, S. P. (1996). Forming inferences about some intraclass correlationcoefficients. Psychological Methods, 1, 30–46.
Nunnally, J. C. (1978). Psychometric theory. New York: McGraw-Hill.O’Brien, E., Asmar, R., Beilin, L., Imai, Y., Mallion, J.-M., Mancia, G., Mengden, T., Myers, M.,
Padfield, P., Palatinin, P., Parati, G., Pickering, T., Redon, J., Staessen, J., Stergiou, G., &Verdecchia, P. on behalf of the European Society of Hypertension Working Group on BloodPressure Monitoring (2003). European Society of Hypertension recommendations for conven-tional, ambulatory and home blood pressure measurement. Journal of Hypertension, 21, 821–848.
Oparil, S., & Miller, A. P. (2005). Gender and blood pressure. Journal of Clinical Hypertension, 7,300–309.
Palatini, P., Palomba, D., Bertolo, O., Minghetti, R., Longo, D., Sarlo, M., & Pessina, A. C. (2003).The white-coat effect is unrelated to the difference between clinic and daytime blood pressure andis associated with greater reactivity to public speaking. Journal of Hypertension, 21, 545–553.
Pickering, T. G. (2005). Should white coat hypertension be treated? The Journal of ClinicalHypertension, 7, 550–553.
Pickering, T. G., & Friedman, R. (1991). The white coat effect: A neglected role for behavioral factorsin hypertension. In P. M. Mccabe, N. Schneiderman, T. M. Field, & J. S. Skyler (Eds.), Stress,coping and disease (pp. 35–49). Hillsdale, NJ: LEA.
Rutledge, T., & Hogan, B. E. (2002). A quantitative review of prospective evidence linkingpsychological factors with hypertension development. Psychosomatic Medicine, 64, 758–766.
Sanz, J., Garcıa-Vera, M. P., Risco, M., & Magan, I. (2006). How many self-measured blood pressurereadings are needed to estimate adults’ ‘‘true’’ blood pressure? manuscript submitted forpublication.
Sanz, J., Silva, F., & Avia, M. D. (1999). La evaluacion de la personalidad desde el modelo de los«Cinco Grandes»: El Inventario de Cinco Factores NEO de Costa y McCrae [Personalityassessment from the Big Five model: Costa and McCrae’s NEO Five Factor Inventory].
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
Personality in hypertension 223

In F. Silva (Ed.), Avances en Evaluacion Psicologica [Advances in Psychological Assessment](pp. 171–234). Valencia: Promolibro.
Schneider, R. H., Egan, B. M., Johnson, E. H., Drobny, H., & Julius, S. (1986). Anger and anxiety inborderline hypertension. Psychosomatic Medicine, 48, 242–248.
Siegel, W. C., Blumenthal, J. A., & Divine, G. W. (1990). Physiological, psychological, andbehavioral factors and white coat hypertension. Hypertension, 16, 140–146.
Smith, T. W., & Ruiz, J. M. (2002). Psychosocial influences on the development and course ofcoronary heart disease: current status and implications for research and practice. Journal ofConsulting and Clinical Psychology, 70, 548–568.
Smyth, K., Call, J., Hansell, S., Sparacino, J., & Strodtbeck, F. L. (1978). Type A behavior pattern andhypertension among inner-city black women. Nursing Research, 27, 30–35.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970). STAI. Manual for the State-Trait AnxietyInventory. Palo Alto, CA: Consulting Psychologist Press.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1988). STAI. Cuestionario de Ansiedad Estado-Rasgo: manual [STAI. Manual for the State-Trait Anxiety Inventory]. Madrid: TEA.
Steptoe, A., Melville, D., & Ross, A. (1982). Essential hypertension and psychological functioning:A study of factory workers. British Journal of Clinical Psychology, 21, 303–311.
Steptoe, A., Melville, D., & Ross, A. (1984). Behavioral response demands, cardiovascular reactivity,and essential hypertension. Psychosomatic Medicine, 46, 33–48.
Theorell, T., Hjindahl, P., Eriesson, F., Kallner, A., Knox, S., Perski, A., Svensson, J., Tidgren, B., &Waller, D. (1985). Psychosocial and physiological factors in relation to blood pressure at rest—astudy of Swedish men in their upper twenties. Journal of Hypertension, 3, 591–600.
World Health Organization-International Society of Hypertension Guidelines Subcommittee. (1999).1999 World Health Organization-International Society of Hypertension guidelines for the manage-ment of hypertension. Journal of Hypertension, 17, 151–183.
Copyright # 2006 John Wiley & Sons, Ltd. Eur. J. Pers. 21: 209–224 (2007)
DOI: 10.1002/per
224 J. Sanz et al.

Related Documents











