Renal Disease and Dialysis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Renal Disease and Dialysis

Objectives
CKD
Dialysis
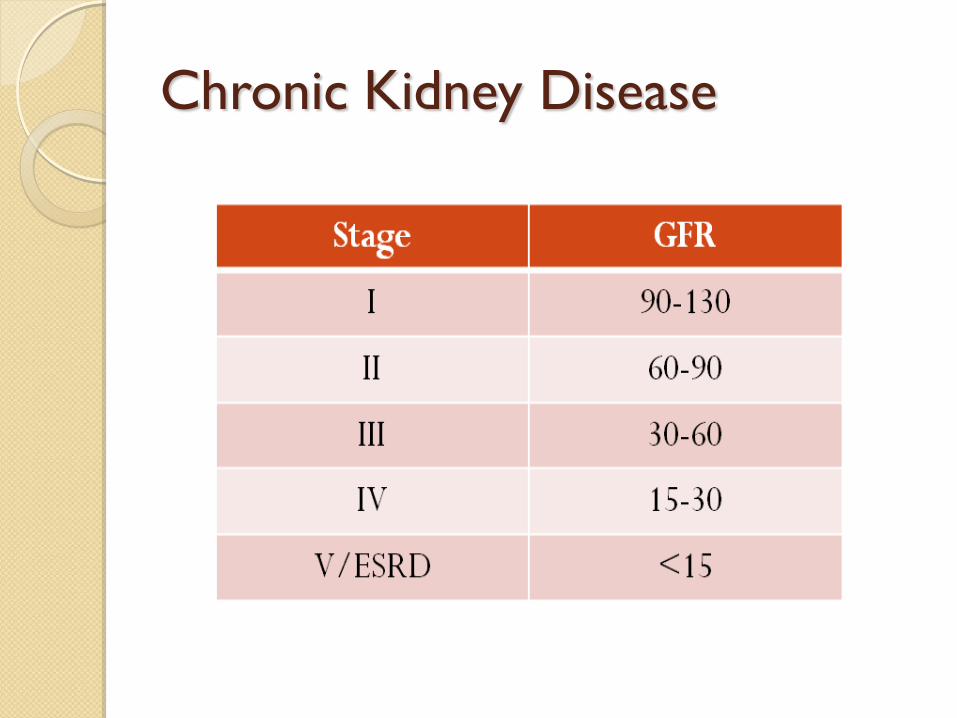
Chronic Kidney Disease

DIALYSIS
HD, PD, CAPD

Common Diagnosis
CKD (ESRD) secondary to hypertensive
nephropathy
Acute gastroenteritis
AKI, Acute gastroenteritis
CKD (ESRD) secondary to chronic
glomerulonephritis
CKD(ESRD) secondary to Diabetic
nephropathy

Indications
End-stage renal failure – GFR less than 5
ml/min( dialysis or renal transplant is
needed).

Contd… Clinical
Fluid overload not responding to diuretics. Uremic convulsion Persistent dyspnea, vomiting and restlessness. Signs of pericarditis, pericardial effusion, pericardial
friction rub. Biochemical
Chemical ARF CRF Normal
Urea >35 mmol/L >40 mmol/L 2.5-6.5 Creatinine >12-14 mg/dl >12-14 mg/dl 0.6-1.3 Potassium >6.5 Meq/L >6.5 Meq/L 3.5-5.5 PH <7.1 <7. 1 7.35-
7.45

Hours for hemodialysis
Hemodialysis usually is done three times a
week.
Each treatment lasts from 2 to 4 hours. During
treatment, patient can read, write, sleep, talk, or
watch TV.

Hemodialysis
Semipermeable membrane
Solute removal via passive diffusion
◦ Inversely proportional to the size (ie effective
removal of K, urea, C; not of PO4)


Ultrafiltration
use of hydrostatic pressure gradient to
induce convection (filtration of water)
solvent drag (pulls dissolved solutes)
across
removal of excess fluid

CVVH
highly permeable membrane
fluid and solute removal via ultrafiltration
filtrate is discarded
replacement fluid is infused similar to
plasma (but no K, urea, Cr, PO4)
used in ICU, runs 12-24h, through double
lumen catheter
less drastic fluid shifts
Preparations for Dialysis
Articles needed for dialysis
i. Arteriovenous fistula : common venous access for HD. Usually radial artery and cephalic vein are anastomosed.
Dialyser set
Arteriovenous set
Fistula needle
Haemodialysis fluid with bicarbonate powder (5 litre)
IV set

…
Inj. 25% Dextrose : If associated with Diabetes,
Diabetic Uropathy , Diabetic Nephropathy.
Inj. Normal Saline(500 ml)
Inj Avil
Inj Heparin
Syringes : 20, 10 & 5 cc.

…
ii. Via Femoral (It is done through through femoral
vein
Dialyser set
Arteriovenous set
Femoral Catheter
Guide Wire Straight tip (70cm)
Haemodialysis fluid with Bicarbonate powder (
5litre)
IV canula
…
IV set
Inj. 25 % Dextrose
Inj 2% Xylocaine
Inj. Normal Saline 500ml
Inj. Avil
Inj. Heparin
Syringes : 20, 10 , 5 cc.

Chemicals Used In Dialysis
Sodium Hypochlorite
Hydrogen Peroxide
Formaldehyde

Part A and part B
i. Part A
Concentrate contains :
Sodium Chloride : 173.65 gm/l
Potassium Chloride : 5.06 gm/l
Calcium Chloride : 8.75 gm/l
Magnesium Chloride : 5.18 gm/l
Glacial Acetic Acid : 8.17gm/l

…
ii. Part B
Sodium Bicarbonate : 626gm
Sodium Chloride : 221 gm
(mixed with 9 litres of Reverse Osmosis water)

Medication used during dialysis
Heparin :6000 IU
Side Effects of Heparin : Pruritus, Allergy
,Osteoporosis, Hyperlipidemia,
Thrombocytopenia
Avil : 1 Ampoule (each ml contains 22.75 mg)
Hydrocortisone :1vial = 100 mg
25% dextrose:
Epofit

Heparin free case
Periodic saline rinse
Every 15-30 minutes , rinse the dialyser rapidly
with 100-250 ml of saline while occluding the
blood inlet line.
The purpose of the periodic rinsing is to allow
inspection of a hollow-fiber dialyser for
evidence of clotting.

Hypoglycemia: It can develop in diabetic patient
treated with either hemodialysis or peritoneal
dialysis and is usually due to reduced insulin
catabolism and to reduce intake and absorption
of food.

In diabetic patients hemodialysis solution should
always contain about 200mg/dl glucose if not
added then severe hypoglycemia during or soon
after hemodialysis can result.

Investigation
Haemoglobin :15 days
Urea, creatinine, Na+, K+ : 1 month
Serology : 2 months

Range of
conductivity:14.7mMho13.2mMho
Normal range of TMP: -100 to 500
The usual flow rate for adult patient is
200-350 ml/min


Financial
Amount of 5 lakhs is provided by the
government for dialysis

Complications Infection
Fever and chills
Catheter clotting
Hypotension
Muscle cramps
Septicemia
Hepatits C

Prognosis(Life expectancy)
2-4 years in haemodialysis
9-10 years in CAPD

Disequilibrium Syndrome : It is the set of
systemic and neurologic symptoms often
associated with characteristic EEG findings that
can occur either during or soon after dialysis .
Early manifestation:nausea ,vomiting
,restlesssness ,headache
Serious manifestation : coma, seizure
Care of vascular access
Check access before each treatment.
Keep access clean at all times. Do not use cream or
lotion over the site.
Use access site only for dialysis.
Be careful not to bump or cut access.
Don’t put a blood pressure cuff on access arm.
Remove jewellary or tight clothes over access site.
Don’t sleep with access arm under your head or
body.
Don’t lift heavy objects or put pressure on access
arm.
Check the pulse in your access every day.

Diet Pattern
Fluid restriction: total intake<1 lit/day in oliguric
ARF and total intake <urine output + extra
renal loss
Total caloric intake– 35~ 50 kcal/kg/day
to avoid catabolism
Salt restriction– 2~4 g/day
Potassium intake– 40 meq/day
Phosphorus intake– 800 mg/day
Daily protein intake of between 0.60 and
0.75gm/kg/day.
The normal level of potassium intake is 3.5-5.0
mEq/l.
2-3g/day of sodium is allowed in CKD patient.
Phosphorus consumption for normal people as well
as people with CKD for non dialysis is 2.7-4.6mg/dl.
For CKD dialysis patients the target range is 3.5-
5.5mg/dl.

Dialyzer Re-use
1. Reprocessing technique : The major steps in
dialyzer reuse are rinsing , cleaning,
measurement of dialyzer performance,
disinfection/sterilization and germicide
removal.
a) Rinsing and reverse ultrafiltration
b) Cleaning : Sodium hypochlorite
c) Other cleaning agents : Hydrogen
peroxide,formalin

Nursing consideration
Pre Haemodialysis:
Correct identification of patient, using hospital
number and date of birth
Blood pressure, pulse and temperature
Weight
Blood glucose if diabetic
Observe / assess patient for any other problems
or needs
Observe access site – neckline / fistula / graft

Assess A-B-C
Ambulation, access,
Breathing
Cardiovascular status
Changes
Post Haemodialysis:
After termination of dialysis, record Blood
pressure, pulse and temperature
Blood glucose if diabetic
Weight – assist to scales if necessary
Observe access site to ensure no further
bleeding / dressing secure
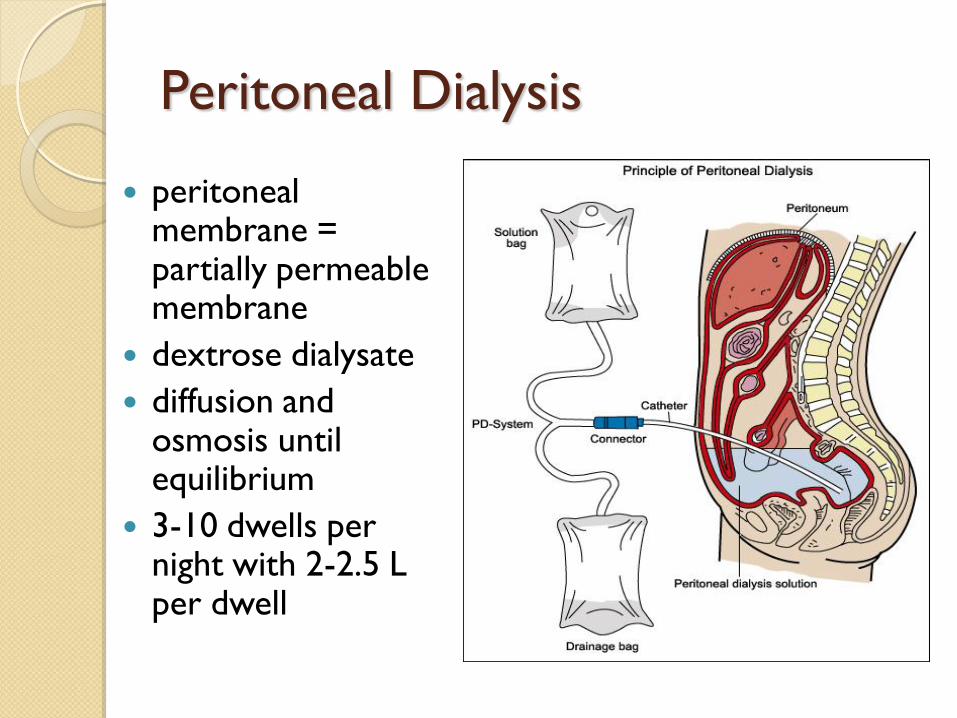
Peritoneal Dialysis
peritoneal membrane = partially permeable membrane
dextrose dialysate
diffusion and osmosis until equilibrium
3-10 dwells per night with 2-2.5 L per dwell

Indications for Dialysis
Acidosis
Electrolytes
Ingestions
Overload
Uremia

Access
Arteriovenous fistula (AVF)
Graft
Tunneled catheter
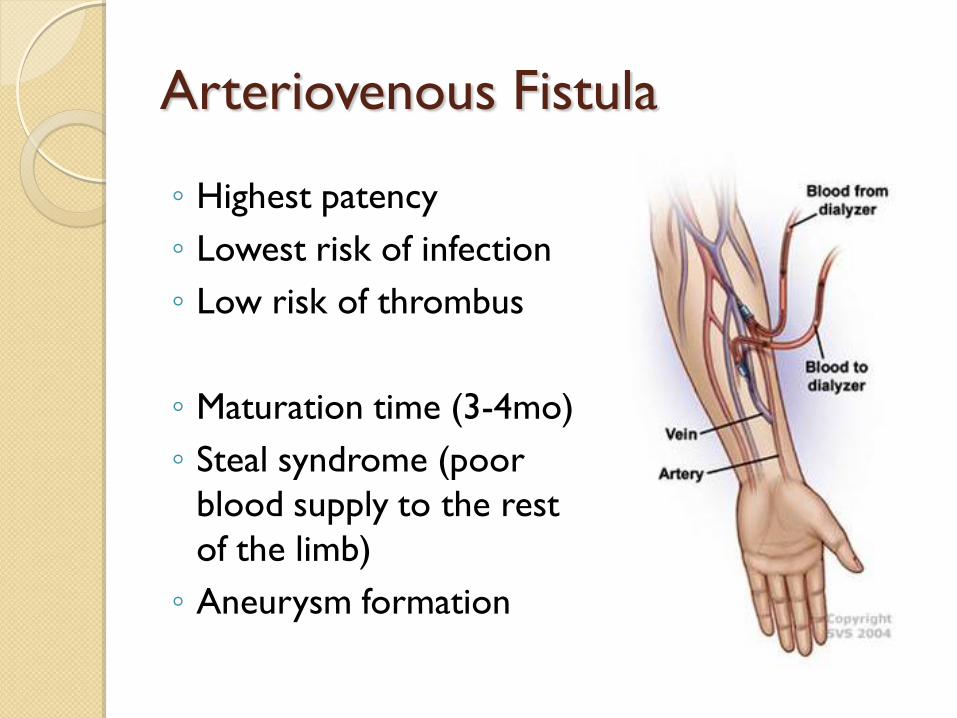
Arteriovenous Fistula
◦ Highest patency
◦ Lowest risk of infection
◦ Low risk of thrombus
◦ Maturation time (3-4mo)
◦ Steal syndrome (poor
blood supply to the rest
of the limb)
◦ Aneurysm formation

Arteriovenous Graft
Easier to create
Maturation time 3-6 weeks
Poor patency (often requires thrombectomy or angioplasty)
Infection
Aneurysms
Steal syndrome

Tunneled Catheter
Immediate use
Bridge to AVF/AVG
Poor flow (decreased HD efficiency)
High infection risk
Venous stenosis
Thrombosis

Dialysis Rx:
Time: 2-5 hours
Bath
Blood flow rate: 400-450cc/min
Dialysate flow rate: 500-800cc/min
Anticoagulant
Additives:
◦ Anemia (EPO, blood)
◦ Bone metabolism (vit D, calcitriol, etc)
◦ Meds (antibiotics)

Dialysate Bath

Common Admissions on Eckel
Complications of missed HD
◦ SOB from fluid overload
◦ HTN crisis
◦ Hyperkalemia
Line infections
Access issues
And everything else…

Eckel Pearls: presentation
75 yo AAM with ESRD 2/2 DM (HD MWF
via RUE AVF, at CDC East, nephrologist
Dr. Wish, dry weight 82kg, oligouric)

Eckel Pearls: history
how did the last HD session go?
complications since being started on HD?
◦ infections?
◦ multiple access points?
medically compliant?
get run sheets from dialysis center
Eckel Pearls: physical exam
Vitals: no BP in the arm of the access
Volume status
Access:
◦ Infection?
◦ Aneurysms
◦ Bruits/thrills


Page 1
RN LK50: OMG’s K is 3.1. Can we
replete?
•Had dialysis 3rd shift. Finished 2hrs ago

Labs in ESRD
Get labs before or 4h after HD
Only the H/H is accurate
Floor RNs can’t use HD lines
Can ask to have cultures drawn at HD
from the line

Page 2
RN LK20: New admit AMS on floor. Hard to arouse. Please eval
ED presentation with abd pain
Workup initiated since there are no beds…
Pain meds: morphine 1mg, then 1mg, then 2 mg, then 3mg IVP
Sent to the floor

Medications in ESRD
Antibiotics
◦ Renally dose
◦ Loading dose, then maintenance dose
No lovenox dvt ppx, use heparin
No morphine
◦ Hepatic metabolism – but active metabolites
◦ Limit the other opioids
Dilaudid: hepatic metabolism – but metabolites can cause neuroexcitiation
constipation/GERD : avoid magnesium/phosphate containing agents

Page 3
RN: new admit OK. Called wound care for
leg.
After lunch you walk on over to the patient
room. ESRD admitted for access.
OK is doing ok. Vitals stable. Comfortable.


Calciphylaxis
Calcinosis cutis

Page 4
RN LK20: Code white, WAA is hypoxic, 83% on RA. Now 92% on VM.
Acutely SOB. Looks uncomfortable.
Your co-NF points that one leg is bigger than the other.
You ask, “have you had a blood clot before?”
WAA nods yes.
Hmmm….amongst other things, CTPE?
Imaging in CKD
Avoid contrast in CKD patients
If you have to, prep
◦ volume expansion: isotonic IVFs
3 cc/kg x 1h before
1cc/kg x 6h after
◦ ? alkalinization: sodium bicarbonate
◦ ? acetylcysteine
◦ radiology can give you the protocol
(treat empirically)

Imaging in ESRD
CT with contrast is ok
MRI with gadolinium is NOT:
◦ Nephrogenic Systemic Fibrosis (NSF)
◦ IF you must: HD x 3 over 3 consecutive days,
with the first right after

Page 5
RN LK20: Lost access on GRR. Can you order a PICC?
Finally, an easy question.
CKD. Sure, why not?

Access in CKD
Avoid PICC/midlines in CKD stage 4-5
Try to preserve access
Try for the feet/EJ
But if you need to, order a midline
PCP should refer CKD stage IV to nephrologists in anticipation of HD

Don’t treat them lightly

The end.

Dialysis Patients at Risk
for Infection

Why are Dialysis Patients at Risk for
Infection?
◦ Frequent use of catheters or insertion of needles
to access the bloodstream
◦ Weakened immune systems
◦ Frequent hospital stays and surgery

Dialysis patients are at risk of getting hepatitis B
and C infections and bloodstream infections
◦ Hepatitis B and C are bloodborne
viral infections that can cause chronic
(life-long) disease involving
inflammation (swelling) of the liver Hepatitis B and C viruses can live on
surfaces and be spread without visible blood
◦ A bloodstream infection is a serious infection that can
occur when bacteria or other germs get into the blood
One way bacteria can enter the bloodstream is through a vascular
access (catheter, fistula, or graft)
Infections in Dialysis Patients

• Advise patients to inform you if they notice any of the following
possible signs of infection:
– Fever
– The access site is:
• Swollen (bulging),
• red,
• warm, or
• has pus
– Severe pain at the access site
Remember: infections of the vascular
access site can be life threatening
How to Recognize an Infection

Bloodstream infections are a dangerous complication of
dialysis
1 in 4 patients who get a
bloodstream infection caused by
S. aureus (staph) bacteria can face
complications such as:
◦ Endocarditis (infected heart valve)
◦ Osteomyelitis (infected bone)
Total costs for each infection can be more than $20,000
Bloodstream infections can cause sepsis (a potentially deadly
condition)
Up to 1 in 5 patients with an infection die within 12 weeks
Infections in Dialysis Patients

Basic Steps in Fistula/Graft Care
Cannulation Procedure:
1. Wash the site
2. Perform hand hygiene
3. Put on a new, clean pair of gloves
4. Wear proper face protection
5. Apply skin antiseptic and allow it
to dry
6. Insert needle using aseptic
technique
7. Remove gloves and perform hand
hygiene
Aseptic technique means taking great care to not contaminate the fistula
or graft site before or during the cannulation or decannulation procedure
Photo provided by Stephanie Booth, used with permission
Basic Steps in Catheter Care
Catheter Connection Procedure:
1. Perform hand hygiene
2. Put on a new, clean pair of gloves
3. Wear proper face protection
4. Apply antiseptic to catheter hub and allow it to dry
5. Connect the catheter to blood lines using aseptic technique
6. Unclamp the catheter
7. Remove gloves and perform hand hygiene

Basic Steps in Catheter Care
Catheter Disconnection Procedure:
1. Perform hand hygiene
2. Put on a new, clean pair of gloves
3. Wear proper face protection
4. Disconnect the catheter from blood lines using aseptic technique
5. Apply antiseptic to catheter hub and allow it to dry
6. Replace caps using aseptic technique
7. Make sure the catheter remains clamped
8. Remove gloves and perform hand hygiene

Catheter Exit Site Care
1. Perform hand hygiene
2. Put on a new, clean pair of gloves
3. Wear a face mask if required
4. Apply antiseptic to catheter exit
site and allow it to dry
5. Apply antimicrobial ointment
6. Apply clean dressing to exit site
7. Remove gloves and perform hand
hygiene
Photo provided by Stephanie Booth, used with permission

Separate Clean Areas from Contaminated
Areas
• Clean areas should be used for the
preparation, handling and storage of
medications and unused supplies and equipment
– Your center should have clean medication and
clean supply areas
• Contaminated areas are where used
supplies and equipment are handled
• Do not handle or store medications or clean
supplies in the same area as where used
equipment or blood samples are handled
Remember: Treatment stations are contaminated areas!
Clean area
Photo provided by Stephanie Booth, used with permission

Dedicate Supplies to a Single Patient
• Any item taken to a patient’s dialysis
station could become contaminated
• Items taken into the dialysis station should either be:
– Disposed of, or
– Cleaned and disinfected before being taken to a common clean area or used on another patient
• Unused medications or supplies taken to the patient’s station should not be returned to a common clean area (e.g., medication vials, syringes, alcohol swabs)
Photo provided by Marshia Coe and Teresa Hoosier, used with permission

Safe Use of Medication Vials
• Prepare all individual patient doses in a
clean area away from dialysis stations
• Prepare doses as close as possible to the
time of use
• Do not carry medications from station
to station
• Do not prepare or store medications at
patient stations
• CDC recommends that dialysis facilities:
– Use single-dose vials whenever possible and
dispose of them immediately after use

Guidelines for Carrying Medications
Do not use the same medication cart to deliver
medications to multiple patients
Do not carry medication vials, syringes, alcohol swabs, or
supplies in pockets
Be sure to prepare the medication in a clean area away
from the patient station and bring it to the patient station
for that patient only at the time of use

Cleaning and disinfection reduce the risk of spreading an
infection
Cleaning is done using cleaning detergent,
water and friction, and is intended to
remove blood, body fluids, and other
contaminants from objects and surfaces
Disinfection is a process that kills many
or all remaining infection-causing
germs on clean objects and surfaces
◦ Use an EPA-registered hospital disinfectant
◦ Follow label instructions for proper dilution
Wear gloves during the cleaning/disinfection process
Cleaning and Disinfecting the
Dialysis Station

All equipment and surfaces are considered to be
contaminated after a dialysis session and therefore must be
disinfected
After the patient leaves the station,
disinfect the dialysis station
(including chairs, trays, countertops,
and machines) after each patient
treatment
◦ Wipe all surfaces
◦ Surfaces should be wet with disinfectant and allowed to air dry
◦ Give special attention to cleaning control panels on the dialysis
machines and other commonly touched surfaces
◦ Empty and disinfect all surfaces of prime waste containers
Disinfecting the Dialysis Station
Photo provided by Stephanie Booth, used with permission

Safe Handling of Dialyzers and
Blood Tubing
• Before removing or transporting used
dialyzers and blood tubing, cap dialyzer
ports and clamp tubing
• Place all used dialyzers and tubing in
leak-proof containers for transport
from station to reprocessing or
disposal area
• If dialyzers are reused, follow
published methods (e.g., AAMI
standards) for reprocessing
AAMI is the Association for the Advancement of Medical
Instrumentation
Photo provided by Stephanie Booth, used with permission

Conclusion
Infections that patients can get while receiving dialysis are
serious and preventable!
Healthcare workers like you following infection control
precautions and other safe care practices are the key to
prevention
Infection prevention is everyone’s responsibility
Related Documents











