25 millisieverts (mSv; 1 mSv = 0.001 Sv) for common imaging studies. For example, a conventional anterior–posterior abdominal X-ray examination results in a dose to the stomach of approximately 0.25 mSv, which is at least 50 times less than the corresponding stomach dose from an abdominal CT scan. Table 1 shows average effective doses (mSv) from imaging studies carried out by Mettler FA, Huda W, Yoshizumi TT and Mahesh M in their publication ‘Effective Doses in Radiology 18 and Diagnostic Nuclear Medicine: A Catalogue’ . Table 4 compares findings from our studies with Mettler et. el. Literature Survey Biological effects and risks associated with low doses of ionizing radiation have been discussed in various articles. The organ under study receives typically, an effective radiation dose, depending on the machine settings, in the range of 15 mSv in an adult to 30 mSv in a neonate from a single Pan CT Scan, with an average of 2 to 3 CT scans per study. At these 1 doses , the most likely risks (though small) are for radiation- induced carcinogenesis. Most of our quantitative information regarding radiation induced risks of cancer are derived from studies of the 1945 5 Japanese atomic bomb survivors. The cohorts are large and have been intensively studied over a period of 56 years covering all age groups. Significant subcohort is of 25,000 atom bomb survivors who received radiation doses less than 50 mSv similar to our study. Data from these cohorts of atomic bomb survivors are generally used for predicting risks related to radiation in a population. CT imaging involves localized high exposures in comparison to the uniform dose of radiation fairly distributed throughout the body in the atomic bomb survivors but there is very little evidence to attribute that the risk for a specific organ is influenced significantly due to exposing other organs in the body to radiation. In a subgroup of atomic bomb survivors, receiving radiation in low doses of 5 to 150 mSv and a mean dose of 40 mSv (equates to an organ dose from a typical CT imaging study of 2 to 3 scans in an adult), 7-9 the overall risk of cancer is significantly increased in this subgroup. A large scale study was conducted recently in the 10,11 nuclear industry on 4,00,000 radiation workers who were exposed to an average dose of 20 mSv (comparable to a typical organ dose from a single adult CT Scan). A significant association was identified in this cohort between the radiation dose and mortality from cancer (when workers exposed to doses between 5 to 150 mSv, there was a significant increase in risk of cancer), which were quantitatively consistent with those reported for atomic bomb survivors. In 2005 and 2006, due to the results of further research studies on the 1945 Japanese atomic bomb survivors, the risk estimates were increased in the Biological Effects of Ionizing 24 Abstract Many trauma centers utilize extensive radiological diagnostic tests during acute assessment of seriously injured trauma patients. A point of concern arises about possible biological effects of these cumulative ionizing radiation doses each patient is exposed to, in health care settings. The purpose of this study is to determine the amount of ionizing radiation received by a trauma patient in the Emergency Department (ED) during the first 24 hours of his initial evaluation. In this study, all injured patients who presented to ED of Department of A&E, SRMC in September 2008 and who underwent CT scan and radiographic investigations during first 24 hours of initial evaluation were included. Individual radiation dose from each CT procedure and radiographs was recorded. The median effective dose of radiation received during first 24 hours was observed and reported. A total of 156 trauma patients have been included in the study. Total number of radiographs performed in September 2008 was 863 with a mean of 5.53. Total number of CT Scans performed in September 2008 was 213 with a mean of 1.37. The median dose equivalents for individual CT scan ranged from 0.6 mSv for facial / para nasal sinus to 20 mSv for a head/chest/whole abdomen CT. The mean effective dose of ionizing radiation per patient from CT scan was 4.407 mSv and the median effective dose of ionizing radiation from CT scan was 31.40 mSv. This study clearly demonstrates that trauma patients are exposed to clinically important high doses of radiation during their initial evaluation. Keywords: Diagnostic Radiography, Poly-trauma, Trauma Imaging. Introduction Many trauma centers and EDs utilize extensive radiological diagnostic tests during the acute assessment of seriously injured trauma patients. Patients with a history of trauma commonly receive plain trauma series radiographs shortly after presentation to the ED, followed by computed tomography (CT) of the head, neck, chest, abdomen or the pelvis depending on the injuries sustained. The series of chest, abdomen and pelvis CT imaging studies have been referred as the ‘pan scan’, which is done for poly-trauma. In addition, many other radiographs of the upper or lower limbs and spine may also be done, depending on the injuries sustained by the patient. The radiographic studies, described above, use a form of ionizing radiation that can damage genetic information and induce transformation of biological tissues. A point of concern arises about possible biological effects of these cumulative ionizing radiation doses to which each patient is exposed to, in 1 health care settings. Limited knowledge is available in medical literature that quantifies the dose of ionizing radiation 2-4 delivered in acute assessment of trauma patients. Quantitative Measures of Radiation Doses Diagnostic radiographic imaging studies use quantitative measures for absorbed dose, equivalent dose, effective dose and CT Dose Index (CTDI) to describe radiation doses delivered by diagnostic radiographic imaging studies. These are defined as: l Absorbed Dose: The energy deposited in a small volume of matter like tissues by a radiation beam passing through that matter divided by the mass of the matter is called Absorbed Dose, with Gray (Gy) as its unit. l Equivalent Dose: It is defined as the radiation-weighting factor (a dimensional factor) multiplied by the absorbed dose (in Gy) averaged over an entire organ. Sievert (Sv) is the unit for the equivalent dose. Equivalent dose (Sv) = Absorbed Dose (Gy) x Radiation Factor . l Effective Dose: It is an estimate of the whole-body equivalent dose uniformly that would produce the same level of risk for adverse effect that results from partial body irradiation non-uniformly. Sievert (Sv) is the unit for effective dose. l CTDI: CT Dose Index is defined by US Department of Health and Human Services as the Average Dose imparted by a single axial acquisition to a standard 100 mm pencil chamber dosimeter inside a PMMA phantom over the width of 14 CT slices. Some Common Radiography Dosages Conventional radiography like X-rays has considerable smaller organ doses in comparison to corresponding CT scan imaging. Table 1 shows average effective doses in Diagnostic Radiographic Imaging in Trauma – A Prospective Observational Study Study Effective Dose (mSv) Plain Film (X-rays) Chest (one view) 0.02 Chest (two views) 0.10 Abdomen (one view) 0.70 Acute Abdominal Series 1.50 Hips or Pelvis (one view) 0.70 Cervical Spine Series (Neck) 0.20 Thoracic Spine Series (upper back) 1.00 Lumbar Spine Series (lower back) 1.50 Extermity Series (Arm, leg, hand, foot etc) 0.01 Mammogram series 0.40 Dental (two views) 0.01 Skull (two views) 0.10 CT Scans Brain 2.00 Cervical Spine (Neck) 6.00 Soft Tissue Neck 3.00 Chest (Standard) 7.00 Chest (Pulmonary Angiogram/PE Study) 15.00 Chest (Coronary Angiogram.Cardiac CT) 16.00 Chest (Calcium Scoring) 3.00 Abdomen 8.00 Abdomen (Dedicated 3 Phase Liver) 15.00 Abdomen and Pelvis 14.00 Chest, Abdomen and Pelvis 18.00 Pelvis 6.00 Table 1: Average Effective Radiation Dosage Fig. 1 Estimated Dependence of Lifetime Radiation Induced Risk of Cancer on Age at Exposure 20 for Two Most Common Radiogenic Cancers.

Diagnostic Radiographic Imaging in Trauma – A Prospective Observational Study
Aug 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

25
millisieverts (mSv; 1 mSv = 0.001 Sv) for common imaging studies. For example, a conventional anterior–posterior abdominal X-ray examination results in a dose to the stomach of approximately 0.25 mSv, which is at least 50 times less than the corresponding stomach dose from an abdominal CT scan.
Table 1 shows average effective doses (mSv) from imaging studies carried out by Mettler FA, Huda W, Yoshizumi TT and Mahesh M in their publication ‘Effective Doses in Radiology
18and Diagnostic Nuclear Medicine: A Catalogue’ . Table 4 compares findings from our studies with Mettler et. el.
Literature Survey
Biological effects and risks associated with low doses of ionizing radiation have been discussed in various articles. The organ under study receives typically, an effective radiation dose, depending on the machine settings, in the range of 15 mSv in an adult to 30 mSv in a neonate from a single Pan CT Scan, with an average of 2 to 3 CT scans per study. At these
1doses , the most likely risks (though small) are for radiation-induced carcinogenesis.
Most of our quantitative information regarding radiation induced risks of cancer are derived from studies of the 1945
5Japanese atomic bomb survivors. The cohorts are large and have been intensively studied over a period of 56 years
covering all age groups. Significant subcohort is of 25,000 atom bomb survivors who received radiation doses less than 50 mSv similar to our study. Data from these cohorts of atomic bomb survivors are generally used for predicting risks related to radiation in a population.
CT imaging involves localized high exposures in comparison to the uniform dose of radiation fairly distributed throughout the body in the atomic bomb survivors but there is very little evidence to attribute that the risk for a specific organ is influenced significantly due to exposing other organs in the body to radiation.
In a subgroup of atomic bomb survivors, receiving radiation in low doses of 5 to 150 mSv and a mean dose of 40 mSv (equates to an organ dose from a typical CT imaging study of 2 to 3 scans in an adult),
7-9the overall risk of cancer is significantly increased in this subgroup.
A large scale study was conducted recently in the 10,11 nuclear industry on 4,00,000 radiation workers
who were exposed to an average dose of 20 mSv (comparable to a typical organ dose from a single adult CT Scan).
A significant association was identified in this cohort between the radiation dose and mortality from cancer (when workers exposed to doses between 5 to 150 mSv, there was a significant increase in risk of cancer), which were quantitatively consistent with those reported for atomic bomb survivors.
In 2005 and 2006, due to the results of further research studies on the 1945 Japanese atomic bomb survivors, the risk estimates were increased in the Biological Effects of Ionizing
24
Abstract
Many trauma centers utilize extensive radiological diagnostic tests during acute assessment of seriously injured trauma patients. A point of concern arises about possible biological effects of these cumulative ionizing radiation doses each patient is exposed to, in health care settings.
The purpose of this study is to determine the amount of ionizing radiation received by a trauma patient in the Emergency Department (ED) during the first 24 hours of his initial evaluation.
In this study, all injured patients who presented to ED of Department of A&E, SRMC in September 2008 and who underwent CT scan and radiographic investigations during first 24 hours of initial evaluation were included. Individual radiation dose from each CT procedure and radiographs was recorded. The median effective dose of radiation received during first 24 hours was observed and reported.
A total of 156 trauma patients have been included in the study. Total number of radiographs performed in September 2008 was 863 with a mean of 5.53. Total number of CT Scans performed in September 2008 was 213 with a mean of 1.37. The median dose equivalents for individual CT scan ranged from 0.6 mSv for facial / para nasal sinus to 20 mSv for a head/chest/whole abdomen CT.
The mean effective dose of ionizing radiation per patient from CT scan was 4.407 mSv and the median effective dose of ionizing radiation from CT scan was 31.40 mSv.
This study clearly demonstrates that trauma patients are exposed to clinically important high doses of radiation during their initial evaluation.
Keywords: Diagnostic Radiography, Poly-trauma, Trauma Imaging.
Introduction
Many trauma centers and EDs utilize extensive radiological diagnostic tests during the acute assessment of seriously injured trauma patients. Patients with a history of trauma commonly receive plain trauma series radiographs shortly after presentation to the ED, followed by computed tomography (CT) of the head, neck, chest, abdomen or the pelvis depending on the injuries sustained. The series of chest, abdomen and pelvis CT imaging studies have been referred as
the ‘pan scan’, which is done for poly-trauma. In addition, many other radiographs of the upper or lower limbs and spine may also be done, depending on the injuries sustained by the patient.
The radiographic studies, described above, use a form of ionizing radiation that can damage genetic information and induce transformation of biological tissues. A point of concern arises about possible biological effects of these cumulative ionizing radiation doses to which each patient is exposed to, in
1health care settings. Limited knowledge is available in medical literature that quantifies the dose of ionizing radiation
2-4delivered in acute assessment of trauma patients.
Quantitative Measures of Radiation Doses
Diagnostic radiographic imaging studies use quantitative measures for absorbed dose, equivalent dose, effective dose and CT Dose Index (CTDI) to describe radiation doses delivered by diagnostic radiographic imaging studies. These are defined as:
l Absorbed Dose: The energy deposited in a small volume of matter like tissues by a radiation beam passing through that matter divided by the mass of the matter is called Absorbed Dose, with Gray (Gy) as its unit.
l Equivalent Dose: It is defined as the radiation-weighting factor (a dimensional factor) multiplied by the absorbed dose (in Gy) averaged over an entire organ. Sievert (Sv) is the unit for the equivalent dose. Equivalent dose (Sv) = Absorbed Dose (Gy) x Radiation Factor .
l Effective Dose: It is an estimate of the whole-body equivalent dose uniformly that would produce the same level of risk for adverse effect that results from partial body irradiation non-uniformly. Sievert (Sv) is the unit for effective dose.
l CTDI: CT Dose Index is defined by US Department of Health and Human Services as the Average Dose imparted by a single axial acquisition to a standard 100 mm pencil chamber dosimeter inside a PMMA phantom over the width of 14 CT slices.
Some Common Radiography Dosages
Conventional radiography like X-rays has considerable smaller organ doses in comparison to corresponding CT scan imaging. Table 1 shows average effective doses in
Diagnostic Radiographic Imaging in Trauma – A Prospective Observational Study
Study Effective Dose (mSv)
Plain Film (X-rays)
Chest (one view) 0.02
Chest (two views) 0.10
Abdomen (one view) 0.70
Acute Abdominal Series 1.50
Hips or Pelvis (one view) 0.70
Cervical Spine Series (Neck) 0.20
Thoracic Spine Series (upper back) 1.00
Lumbar Spine Series (lower back) 1.50
Extermity Series (Arm, leg, hand, foot etc) 0.01
Mammogram series 0.40
Dental (two views) 0.01
Skull (two views) 0.10
CT Scans
Brain 2.00
Cervical Spine (Neck) 6.00
Soft Tissue Neck 3.00
Chest (Standard) 7.00
Chest (Pulmonary Angiogram/PE Study) 15.00
Chest (Coronary Angiogram.Cardiac CT) 16.00
Chest (Calcium Scoring) 3.00
Abdomen 8.00
Abdomen (Dedicated 3 Phase Liver) 15.00
Abdomen and Pelvis 14.00
Chest, Abdomen and Pelvis 18.00
Pelvis 6.00Table 1: Average Effective Radiation Dosage
Fig. 1 Estimated Dependence of Lifetime Radiation Induced Risk of Cancer on Age at Exposure
20for Two Most Common Radiogenic Cancers.

n = 156
Fig. 2 Age and Gender Distribution of Trauma Patients Included in Study
2726
Materials and Methods
Study Design and SettingThis is a prospective, observational study based on the data of the Accident and Emergency Department of Sri Ramachandra Medical College & Research Institute, a 1,500 bedded tertiary care university hospital and a level I Trauma Center in the South Indian metropolitan city of Chennai. The Institute receives 4000 trauma patients per year on an average in the Emergency Department, making it ideal for a study of this nature.
Inclusion CriteriaAll consecutive injured patients irrespective of age, who were registered in the ED in the month of September 2008, with history of trauma and who underwent CT scan imaging during the first 24 hours of initial evaluation were included in the study. These patients were entered in our trauma registry.
Exclusion CriteriaTrauma patients without CT scan imaging were excluded from the study.
Operational DefinitionsFor this study, following definitions are used:
l Trauma: It is defined as a bodily lesion at the organic level, resulting from acute exposure to physical energy in amounts that exceed the threshold of physiological tolerance.
l Triage Priorities: Following criteria were used for prioritization of patients.
Priority 1: Immediate life threatening condition Priority 2: Potential life threatening conditionPriority 3:Non-life threatening condition or minor injuries
Methods of MeasurementIn this prospective observational study the effective dose for the entire body is measured in mSv, which is the standard unit used very commonly to compare radiation exposure received during different imaging procedures. Standardized radiography radiation tables were also used to calculate
18exposure dose.
12Radiation (BEIR) VII report , and several important conclusions were drawn from this report. Exposure to 100 mSv would cause leukaemia or solid organ cancer in 1 in 100 persons (0.01/mSv). This is the principal finding of the BEIR VII report.
thThe National Academy of Sciences 7 report on biological effects of ionizing radiation in 2005 states that out of 1,00,000 people exposed to a dose of 100 mSv, there would be an
12additional 800 cases of cancer.
In children, the situation is clearer and they are at higher risk than adults from a given dose of ionizing radiation (Fig. 1), both because they are inherently more radiosensitive and because they have more remaining years of life during which a
13,14radiation-induced cancer could develop.
Cancer risks decrease with increasing age, both because children have more years of life during which a potential cancer can be expressed (latency periods for solid tumours are typically decades) and because growing children are inheritently more radiosensitive, since they have a larger proportion of dividing cells.
In 2005, the National Academy of 12Sciences tabled a report on the 1945
Japanese atomic bombings survivors and from this report the risk estimates applicable to other populations are ultimately derived and the data have been averaged according to sex.
In short, there is proven evidence from recent epidemiologic studies that the organ doses in relation to a common CT study (two or three scans, leading to a dose in the range of 30 to 90 mSv)
12result in an increased risk of cancer . The evidence is reasonably convincing for adults and very convincing for children.
Report on BEIR VII published by Board on Radiation Effects Research finds that the risk estimates allow an estimation of relative risk of cancer.
Risk of cancer occurrence due to radiation is related to a number of factors like age, sex, race, duration of exposure, as well as exposure to environmental agents like ionizing
12radiations . Relative risk of cancer describes the multiplicative increase in risk of cancer associated with exposure
12to a radiation dose .
The report estimates that the relative risk of lifetime cancer after exposure to
100 mSv would be 1.024. The relative risk in the University of Pennsylvania series was 1.025 and that in the Sunnybrook series was 1.005 (1.037 in the high exposure subgroup). For a single 4.55 mSv CT imaging, the relative risk would be 1.001. The risk per CT imaging is roughly 1 fatal cancer per 2000 CT scans, although this varies substantially with the age of the patient. The risk of fatal malignancies is 5% per sievert.
Aims and Objectives
The purpose of this study is to determine the amount of ionizing radiation received by a trauma patient in the ED during the first 24 hours of their initial evaluation. We used estimated radiation doses calculated by the CT scans and radiographs performed for each trauma patient during their initial 24 hours of assessment.
Data Collection and Processing
A single investigator, who was not involved with the management and disposition of the trauma patient's was included in the study, collected the data. The data was entered directly into a preformatted questionnaire, the instrument used in the study. Data obtained included demographics, date of admission, mechanism of injury, injury severity score, triage priorities, initial disposition from the emergency department (including intensive care unit, wards, morgue, home, and discharge against medical advice or operating room). Radiographic studies included in the study were CT scans and plain radiographs. Individual radiation dose from each CT procedure and radiograph was recorded. A 24-hour period was selected because the investigators were interested in the immediate post-trauma assessment.
The investigator chose not to follow the patient for the entire hospitalization because there is likelihood that a wide range in injury severity, comorbidities and length of stay can confound the data. Also the types of studies carried out during a patient's initial assessment are likely to be less variable during the first 24 hours versus the entire hospitalization.
All CT scans were performed with a General Electric Light Speed VCT 64 slice scanner and a General Electric Light Speed Ultra 8 slice scanner (General Electric Company, Fairfield, CT) with dose modulation capabilities to decrease radiation exposure. All X-rays were performed using a General Electric Light Speed HF Advantage X-ray machine (General Electric Company, Fairfield, CT). Reports of individual doses from each X-ray and CT imaging were obtained and reviewed. The dose report displays the integrated radiation dose of a specific CT scan imaging that is the dose length product index.
The effective dose, the entire body is exposed to in milli-sieverts, is arrived by multiplying the conversion factors for a
19,20specific area of the body with the dose length product index.
Data AnalysisThe primary outcome of this prospective observational study was the median effective dose of radiation received by an adult poly-trauma patient during the first 24 hours. Data were collected in a pre-formatted questionnaire and compiled into a
Patients Characteristics
Demographics Number Remarks
Registered 289 Trauma cases in Sep 2008
Less Excluded 133 No CT Scan Indicated
Admitted and Studied 156
Males 136
Females 20
Age Group Distribution M F T %
<10 2 6 8 5.13
10-19 15 1 16 10.26
20-19 42 1 43 27.56
30-39 28 6 34 21.79
40-49 15 4 19 12.18
50-59 24 0 24 15.38
60-69 5 1 6 3.85
70-79 4 0 4 2.56
>80 1 1 2 1.28
136 20 156 100.00
Injury
Road accidents 64.0
Industrial Accidents 17.3
Fall 5.0
Assault 4.7
Other Injuries 9.0
Injury Severity
Priority I 24.0
Priority II 48.7
Priority III 27.3
Disposition
Admitted to ward 76 48.72
Admitted to ICU 16 10.26
Discharged to Home 23 14.74
Expired in ED 2 1.28
Left treatment (AMA) 39 25.00 Could not afford treatment
Table 2: Demographic Summary
Fig. 3 Disposition of Patients from ED
2928
spreadsheet (Microsoft Office Excel 2007; Microsoft Corporation, Redmond, WA) and descriptive analysis was
thperformed using statistical software (SPSS Release 15.0.0 [6 September 2006]; SPSS Inc., Chicago, Illinois).
Demographic Analysis
A total of 289 patients were registered with trauma in the month of September 2008, out of which 156 patients have been included in this study. One hundred thirty three patients, who did not undergo CT scan imaging as it was not indicated, were excluded from the study. The patient characteristics and demographic details are summarized in Table 2.
Age and Gender ProfileAmong them, 136 were males and 20 were females, and 61% of them were 20 to 49 years of age (Fig. 2 - previous page).
Mechanism of InjuryMechanism of injury included road traffic accident (64%), industrial accidents (17.3%), fall related injuries (5%), assault (4.7%) and other injuries (9%). The median injury severity score was 19 with a range of 6 to 46.
Severity of Injury Among these patients, 26% belonged to priority 2 and priority 3 triage categories and 24% were triage priority 1 patients. Disposition of PatientsOut of 156 trauma patients, 76 were admitted to ward (48.7%), 16 admitted to intensive care unit (10.2%), 23 were discharged
(14.7%), and 2 expired in ED (1.2%) (Fig.3- on previous page). There were 39 patients who were discharged against medical advice (25%), since they could not afford high costs involved in intensive care unit or surgical intervention, etc.
Radiologic Analysis
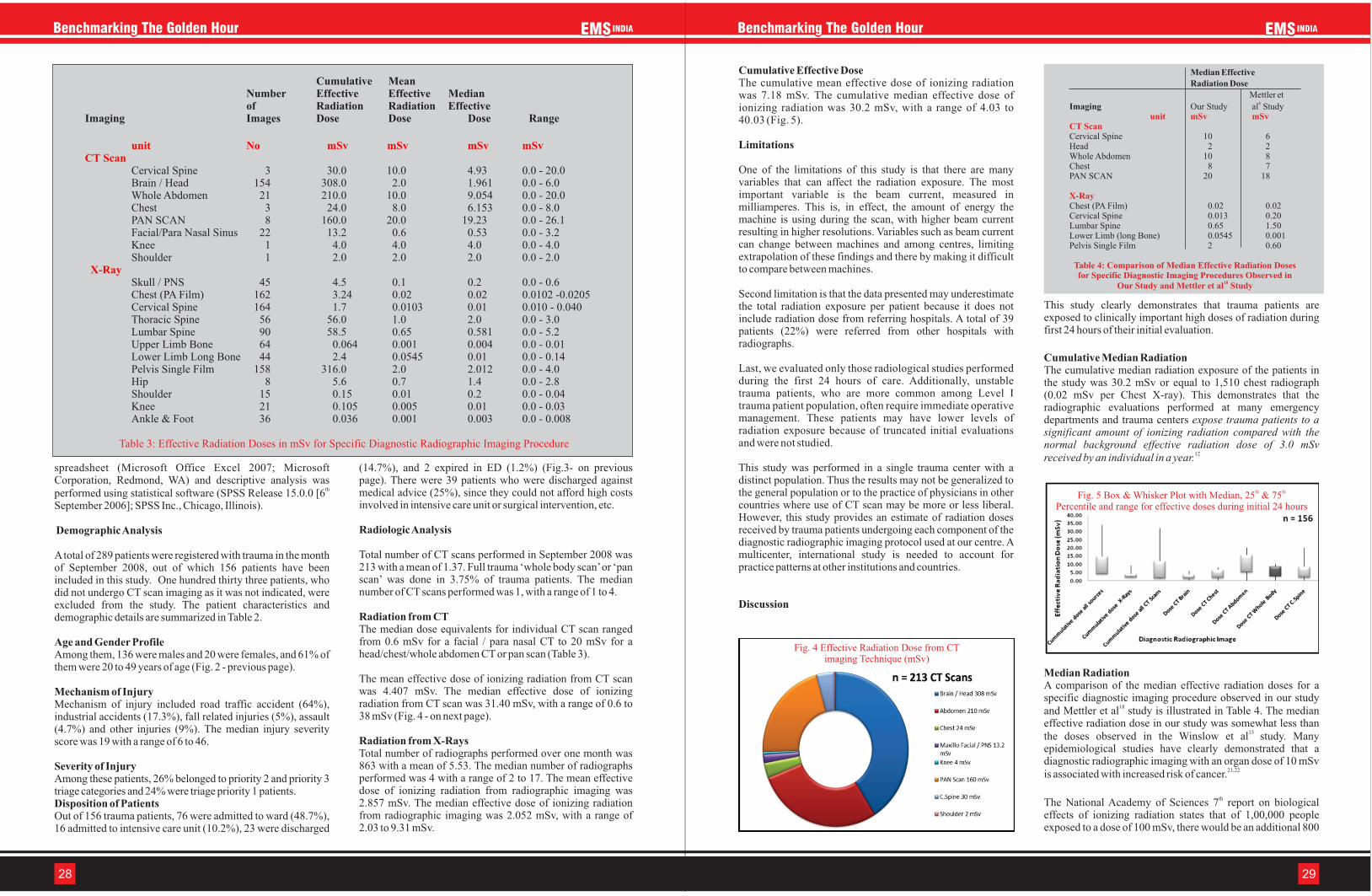
Total number of CT scans performed in September 2008 was 213 with a mean of 1.37. Full trauma ‘whole body scan’ or ‘pan scan’ was done in 3.75% of trauma patients. The median number of CT scans performed was 1, with a range of 1 to 4.
Radiation from CTThe median dose equivalents for individual CT scan ranged from 0.6 mSv for a facial / para nasal CT to 20 mSv for a head/chest/whole abdomen CT or pan scan (Table 3).
The mean effective dose of ionizing radiation from CT scan was 4.407 mSv. The median effective dose of ionizing radiation from CT scan was 31.40 mSv, with a range of 0.6 to 38 mSv (Fig. 4 - on next page).
Radiation from X-RaysTotal number of radiographs performed over one month was 863 with a mean of 5.53. The median number of radiographs performed was 4 with a range of 2 to 17. The mean effective dose of ionizing radiation from radiographic imaging was 2.857 mSv. The median effective dose of ionizing radiation from radiographic imaging was 2.052 mSv, with a range of 2.03 to 9.31 mSv.
Cumulative Effective DoseThe cumulative mean effective dose of ionizing radiation was 7.18 mSv. The cumulative median effective dose of ionizing radiation was 30.2 mSv, with a range of 4.03 to 40.03 (Fig. 5).
Limitations
One of the limitations of this study is that there are many variables that can affect the radiation exposure. The most important variable is the beam current, measured in milliamperes. This is, in effect, the amount of energy the machine is using during the scan, with higher beam current resulting in higher resolutions. Variables such as beam current can change between machines and among centres, limiting extrapolation of these findings and there by making it difficult to compare between machines.
Second limitation is that the data presented may underestimate the total radiation exposure per patient because it does not include radiation dose from referring hospitals. A total of 39 patients (22%) were referred from other hospitals with radiographs.
Last, we evaluated only those radiological studies performed during the first 24 hours of care. Additionally, unstable trauma patients, who are more common among Level I trauma patient population, often require immediate operative management. These patients may have lower levels of radiation exposure because of truncated initial evaluations and were not studied.
This study was performed in a single trauma center with a distinct population. Thus the results may not be generalized to the general population or to the practice of physicians in other countries where use of CT scan may be more or less liberal. However, this study provides an estimate of radiation doses received by trauma patients undergoing each component of the diagnostic radiographic imaging protocol used at our centre. A multicenter, international study is needed to account for practice patterns at other institutions and countries.
Discussion
This study clearly demonstrates that trauma patients are exposed to clinically important high doses of radiation during first 24 hours of their initial evaluation.
Cumulative Median RadiationThe cumulative median radiation exposure of the patients in the study was 30.2 mSv or equal to 1,510 chest radiograph (0.02 mSv per Chest X-ray). This demonstrates that the radiographic evaluations performed at many emergency departments and trauma centers expose trauma patients to a significant amount of ionizing radiation compared with the normal background effective radiation dose of 3.0 mSv
12received by an individual in a year.
Median RadiationA comparison of the median effective radiation doses for a specific diagnostic imaging procedure observed in our study
18and Mettler et al study is illustrated in Table 4. The median effective radiation dose in our study was somewhat less than
15 the doses observed in the Winslow et al study. Many epidemiological studies have clearly demonstrated that a diagnostic radiographic imaging with an organ dose of 10 mSv
21,22 is associated with increased risk of cancer.
thThe National Academy of Sciences 7 report on biological effects of ionizing radiation states that of 1,00,000 people exposed to a dose of 100 mSv, there would be an additional 800
Cumulative MeanNumber Effective Effective Medianof Radiation Radiation Effective
Imaging Images Dose Dose Dose Range
Cervical Spine 3 30.0 10.0 4.93 0.0 - 20.0Brain / Head 154 308.0 2.0 1.961 0.0 - 6.0Whole Abdomen 21 210.0 10.0 9.054 0.0 - 20.0Chest 3 24.0 8.0 6.153 0.0 - 8.0PAN SCAN 8 160.0 20.0 19.23 0.0 - 26.1Facial/Para Nasal Sinus 22 13.2 0.6 0.53 0.0 - 3.2Knee 1 4.0 4.0 4.0 0.0 - 4.0Shoulder 1 2.0 2.0 2.0 0.0 - 2.0
Skull / PNS 45 4.5 0.1 0.2 0.0 - 0.6Chest (PA Film) 162 3.24 0.02 0.02 0.0102 -0.0205 Cervical Spine 164 1.7 0.0103 0.01 0.010 - 0.040Thoracic Spine 56 56.0 1.0 2.0 0.0 - 3.0Lumbar Spine 90 58.5 0.65 0.581 0.0 - 5.2Upper Limb Bone 64 0.064 0.001 0.004 0.0 - 0.01Lower Limb Long Bone 44 2.4 0.0545 0.01 0.0 - 0.14Pelvis Single Film 158 316.0 2.0 2.012 0.0 - 4.0Hip 8 5.6 0.7 1.4 0.0 - 2.8Shoulder 15 0.15 0.01 0.2 0.0 - 0.04Knee 21 0.105 0.005 0.01 0.0 - 0.03Ankle & Foot 36 0.036 0.001 0.003 0.0 - 0.008
unit No mSv mSv mSv mSvCT Scan
X-Ray
Table 3: Effective Radiation Doses in mSv for Specific Diagnostic Radiographic Imaging Procedure
Fig. 4 Effective Radiation Dose from CTimaging Technique (mSv)
Median Effective Radiation Dose
Mettler et8Imaging Our Study al Study
Cervical Spine 10 6Head 2 2Whole Abdomen 10 8Chest 8 7PAN SCAN 20 18
Chest (PA Film) 0.02 0.02Cervical Spine 0.013 0.20Lumbar Spine 0.65 1.50Lower Limb (long Bone) 0.0545 0.001Pelvis Single Film 2 0.60
unit mSv mSvCT Scan
X-Ray
Table 4: Comparison of Median Effective Radiation Doses for Specific Diagnostic Imaging Procedures Observed in
18Our Study and Mettler et al Study
th thFig. 5 Box & Whisker Plot with Median, 25 & 75Percentile and range for effective doses during initial 24 hours

3130
19. Jessen KA, Shrimpton PC, Geleijns J, et al. Dosimetry for optimisation of patient protection in computed tomography. Appl Radiat Isot. 1999; 50:165-172
20.McCollough CH, Schueler BA. Calculation of effective dose. Med Phys. 2000; 27:828-837
21.Doll R, Wakeford R. Risk of childhood cancer from foetal irradiation. Br. J. Radiol. 1997; 70:130-139
22.Mole R. H. Childhood cancer after prenatal exposure to diagnostic X-ray examinations in Britain. Br. J. Cancer. 1990; 62:152-168
Dr Srihari Cattamanchi, The Author is Disaster Medicine Fellow
Harvard Affiliated Disaster Medicine Fellowship, Harvard Medical School,
USA
Co-authored ByProf T V Ramakrishnan,
Professor & Head of Clinical Services, Dept. of Accident & Emergency Medicine,
Sri Ramachandra Medical College & Research Institute,Chennai
This article has been peer reviewed.
12cases of cancer. This risk is linear, suggesting that the median dose of 30.2 mSv observed in this study would contribute to an additional 241 cancer cases per 1,00,000 subjects exposed.
Cases of PolytraumaIt is widely accepted that poly-trauma patients (triage 1) are at high risk of life-threatening injuries and this clearly justifies aggressive investigation to identify and intervene in such injuries, even if the investigation entails some risk. But most of the patients in the study were in triage priority 2 & 3 (76%), who are not in immediate life threatening condition and where diagnostic radiographic imaging should be used judiciously after thorough clinical examination and evaluating pros and cons of each radiographic imaging, with goal of minimizing patient's exposure to ionizing radiation.
Our data gives us an insight into the amount of ionizing radiation exposure occurring among trauma patients at one large academic center during their initial assessment.
15This study confirms similar findings found by Winslow et al at Wake Forest University, Winston-Salem, NC. So approaches should be designed to minimize the risks as much as possible. These approaches include reducing the number of repeated imaging studies, using low dose imaging techniques, using alternative imaging methods that do not use ionizing radiation (ultrasonography or magnetic resonance imaging) and an increased reliance on primary and secondary survey, clinical examinations and repeated assessment of the patient for making a diagnosis.
Yes, diagnostic radiographic imaging is very useful in immediate life threatening poly-trauma patients (triage priority 1).
CT scan has transformed trauma management such that most injuries are now managed non-operatively and also allows early recognition of injuries such as bowel perforation that needs surgery and active arterial extravasation that needs interventional angiography. The treating physician should consider the risks and benefits of exposure to these levels of ionizing radiation before ordering diagnostic imaging radiographs in potential life threatening and minor trauma patients (triage priority 2 and 3).
As most patients are in triage priority 2 and 3, decision to take diagnostic imaging studies have to be made after weighing the benefits and risks in order to prevent high equivalent doses of ionizing radiation. If not used judiciously, diagnostic imaging radiography would be really harmful in triage priority 2 and 3 patients.
Conclusion
This study clearly demonstrates that trauma patients are exposed to potentially significant doses of radiation during their initial evaluation. Although radiographic studies are an important part of poly-trauma assessment, they should be used judiciously with the aim of reducing the patient's exposure to ionizing radiation, particularly for cases of triage priority 2 and 3. Physicians should consider the risks and benefits of exposure to these levels of ionizing radiation before ordering diagnostic radiographic imaging of trauma patients.
References
1. Brenner DJ, Doll R, Goodhead DT, et al. Cancer risks attributable to low doses of ionizing radiation: assessing
what we really know. Proc Natl Acad Sci USA. 2003; 100:13761-13766
2. Boffard KD, Goosen J, Plani F, et al. The use of low dosage x-ray (Lodox/Statscan) in major trauma: comparison between low dose x-ray and conventional x-ray techniques. J Trauma. 2006; 60:1175-1181. Discussion 1181-1183
3. Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from paediatric CT. AJR Am J Roentgenol. 2001; 176:289-296
4. Kim PK, Zho X, Houseknecht E, et al. Effective radiation dose from radiologic studies in paediatric trauma patients. World J Surg. 2005; 29:1557-1562
5. BEIR VII. Health risks from exposure to low levels of ionizing radiation. Washington, DC: National Academies Press; 2005
6. Preston DL, Pierce DA, Shimizu Y, et al. Effect of recent changes in atomic bomb survivor dosimetry on cancer mortality risk estimates. Radiat Res. 2004; 162:377-389
7. Preston DL, Shimizu Y, Pierce DA, Suyama A, Mabuchi K. Studies of mortality of atomic bomb survivors. Report 13: Solid cancer and noncancer disease mortality: 1950-1997. Radiat Res. 2003; 160:381-407
8. Pierce DA, Preston DL. Radiation related cancer risks at low doses among atomic bomb survivors. Radiat Res. 2000; 154:178-186
9. Preston DL, Ron E, Tokuoka S, et al. Solid cancer incidence in atomic bomb survivors: 1958-1998. Radiat Res. 2007; 168;1-64
10.Cardis E, Vrijheid M, Blettner M, et al. The 15-country collaborative study of cancer risk among radiation workers in the nuclear industry: estimates of radiation related cancer risks. Radiat Res. 2007; 167:396-416
11. Idem. Risk of cancer after low doses of ionising radiation: retrospective cohort study in 15 countries. BMJ. 2005; 331-377
12.NRC. Health Risks From Exposure to Low Levels of Ionizing Radiation—BEIR VII Phase 2. N.R.C.o.t.N. Academies, ed. Washington DC: National Academies Press; 2006
13.Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med. 2007; 357:2277-2284
14.Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from paediatric CT. AJR Am J Roentgenol. 2001; 176:289-96
15.Winslow JE, Hinshaw JW, Hughes MJ, et al. Quantitative assessment of diagnostic radiation doses in adult blunt trauma patients. Ann Emerg Med. 2008; 52:93-97
16.William R. Mower, et al. Radiation Doses Among Blunt Trauma Patients: Assessing Risks and Benefits of Computed Tomographic Imaging. Ann Emerg Med. 2008; 52:99-100
17.Tien HC, Tremblay LN, Rizoli SB. Radiation exposure from diagnostic imaging in severely injured trauma patients. J.Trauma. 2007; 62:151-156
18.Mettler FA, Huda W, Yoshizumi TT, Mahesh M. Effective Doses in Radiology and Diagnostic Nuclear Medicine: A Catalogue. Radiology. 2008; 248:254-263
Fig. 6 Mean Effective Ionizing Radiation Dose per Patient for each Group
Figure 6c: Median effective does of ionizing radiation duringinitial 24 hours according to mechanism of injury
Figure 6d: Mean effective dose of ionizing radiation duringinitial 24 hours according to Disposition of Patient
Figure 6a: Mean effective dose of ionizing radiation duringinitial 24 hours according to patient’s age
Figure 6b: Mean effective dose of ionizing radiation duringinitial 24 hours according to Triage Priority
Related Documents











