Wendie A. Berg, MD, PhD Lorena Gutierrez, MD Moriel S. NessAiver, PhD W. Bradford Carter, MD 2 Mythreyi Bhargavan, PhD Rebecca S. Lewis, MPH Olga B. Ioffe, MD Index terms: Breast, abnormalities Breast, MR, 00.121412, 00.121413, 00.121415, 00.12143 Breast, US, 00.1298 Breast neoplasms, radiography, 00.115 Published online before print 10.1148/radiol.2333031484 Radiology 2004; 233:830 – 849 Abbreviations: DCIS ductal carcinoma in situ EIC extensive intraductal component IDC invasive ductal carcinoma ILC invasive lobular carcinoma MIP maximum intensity projection MLO mediolateral oblique 1 From American College of Radiology Imaging Network, 301 Merrie Hunt Dr, Lutherville, MD 21093 (W.A.B.); Corpo- racion Nacional del Cancer, Santiago, Chile (L.G.); Departments of Radiology (M.S.N.), Surgery (W.B.C.), and Pathol- ogy (O.B.I.), University of Maryland, Bal- timore; and American College of Radi- ology Technology Assessment Studies Assistance Program, Reston, Va (M.B., R.S.L.). From the 2001 RSNA scientific assembly. Received September 15, 2003; revision requested November 28; revision received March 5, 2004; ac- cepted April 12. Supported by a grant from the Society of Breast Imaging. Address correspondence to W.A.B. (e-mail: [email protected]). Current address: 2 Department of Surgical Oncology, Moffitt Cancer Center, Tampa, Fla. Authors stated no financial relation- ship to disclose. Author contributions: Guarantor of integrity of entire study, W.A.B.; study concepts, W.A.B., O.B.I., W.B.C.; study design, W.A.B., L.G.; litera- ture research, W.A.B.; clinical studies, W.A.B., W.B.C., O.B.I.; data acquisition, W.A.B., M.S.N., L.G.; data analysis/inter- pretation, W.A.B., L.G., M.B.; statistical analysis, W.A.B., M.B., R.S.L.; manuscript preparation and definition of intellectual content, W.A.B.; manuscript editing, W.A.B., M.B.; manuscript revision/review, W.A.B., L.G., M.B., R.S.L., O.B.I.; manu- script final version approval, all authors © RSNA, 2004 Diagnostic Accuracy of Mammography, Clinical Examination, US, and MR Imaging in Preoperative Assessment of Breast Cancer 1 PURPOSE: To prospectively assess accuracy of mammography, clinical examina- tion, ultrasonography (US), and magnetic resonance (MR) imaging in preoperative assessment of local extent of breast cancer. MATERIALS AND METHODS: Institutional review board approval and informed patient consent were obtained. Results of bilateral mammography, US, and con- trast-enhanced MR imaging were analyzed from 111 consecutive women with known or suspected invasive breast cancer. Results were correlated with histopatho- logic findings. RESULTS: Analysis included 177 malignant foci in 121 cancerous breasts, of which 89 (50%) foci were palpable. Median size of 139 invasive foci was 18 mm (range, 2–107 mm). Mammographic sensitivity decreased from 100% in fatty breasts to 45% in extremely dense breasts. Mammographic sensitivity was highest for invasive ductal carcinoma (IDC) in 89 of 110 (81%) cases versus 10 of 29 (34%) cases of invasive lobular carcinoma (ILC) (P .001) and 21 of 38 (55%) cases of ductal carcinoma in situ (DCIS) (P .01). US showed higher sensitivity than did mam- mography for IDC, depicting 104 of 110 (94%) cases, and for ILC, depicting 25 of 29 (86%) cases (P .01 for each). US showed higher sensitivity for invasive cancer than DCIS (18 of 38 [47%], P .001). MR showed higher sensitivity than did mammography for all tumor types (P .01) and higher sensitivity than did US for DCIS (P .001), depicting 105 of 110 (95%) cases of IDC, 28 of 29 (96%) cases of ILC, and 34 of 38 (89%) cases of DCIS. In anticipation of conservation or no surgery after mammography and clinical examination in 96 breasts, additional tumor (which altered surgical approach) was present in 30. Additional tumor was depicted in 17 of 96 (18%) breasts at US and in 29 of 96 (30%) at MR, though extent was now overestimated in 12 of 96 (12%) at US and 20 of 96 (21%) at MR imaging. After combined mammography, clinical examination, and US, MR depicted addi- tional tumor in another 12 of 96 (12%) breasts and led to overestimation of extent in another six (6%); US showed no detection benefit after MR imaging. Bilateral cancer was present in 10 of 111 (9%) patients; contralateral tumor was depicted mammographically in six and with both US and MR in an additional three. One contralateral cancer was demonstrated only clinically. CONCLUSION: In nonfatty breasts, US and MR imaging were more sensitive than mammography for invasive cancer, but both MR imaging and US involved risk of overestimation of tumor extent. Combined mammography, clinical examination, and MR imaging were more sensitive than any other individual test or combination of tests. © RSNA, 2004 With increasing use of reliable percutaneous biopsy techniques, a current goal in breast cancer management is accurate pretreatment planning to allow neoadjuvant chemotherapy or a Breast Imaging 830 R adiology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Wendie A. Berg, MD, PhDLorena Gutierrez, MDMoriel S. NessAiver, PhDW. Bradford Carter, MD2
Mythreyi Bhargavan, PhDRebecca S. Lewis, MPHOlga B. Ioffe, MDIndex terms:Breast, abnormalitiesBreast, MR, 00.121412, 00.121413,
00.121415, 00.12143Breast, US, 00.1298Breast neoplasms, radiography,
00.115
Published online before print10.1148/radiol.2333031484
Radiology 2004; 233:830–849
Abbreviations:DCIS � ductal carcinoma in situEIC � extensive intraductal
componentIDC � invasive ductal carcinomaILC � invasive lobular carcinomaMIP � maximum intensity projectionMLO � mediolateral oblique
1 From American College of RadiologyImaging Network, 301 Merrie Hunt Dr,Lutherville, MD 21093 (W.A.B.); Corpo-racion Nacional del Cancer, Santiago,Chile (L.G.); Departments of Radiology(M.S.N.), Surgery (W.B.C.), and Pathol-ogy (O.B.I.), University of Maryland, Bal-timore; and American College of Radi-ology Technology Assessment StudiesAssistance Program, Reston, Va (M.B.,R.S.L.). From the 2001 RSNA scientificassembly. Received September 15,2003; revision requested November 28;revision received March 5, 2004; ac-cepted April 12. Supported by a grantfrom the Society of Breast Imaging.Address correspondence to W.A.B.(e-mail: [email protected]).Current address:2 Department of Surgical Oncology,Moffitt Cancer Center, Tampa, Fla.Authors stated no financial relation-ship to disclose.Author contributions:Guarantor of integrity of entire study,W.A.B.; study concepts, W.A.B., O.B.I.,W.B.C.; study design, W.A.B., L.G.; litera-ture research, W.A.B.; clinical studies,W.A.B., W.B.C., O.B.I.; data acquisition,W.A.B., M.S.N., L.G.; data analysis/inter-pretation, W.A.B., L.G., M.B.; statisticalanalysis, W.A.B., M.B., R.S.L.; manuscriptpreparation and definition of intellectualcontent, W.A.B.; manuscript editing,W.A.B., M.B.; manuscript revision/review,W.A.B., L.G., M.B., R.S.L., O.B.I.; manu-script final version approval, all authors© RSNA, 2004
Diagnostic Accuracy ofMammography, ClinicalExamination, US, and MRImaging in PreoperativeAssessment of Breast Cancer1
PURPOSE: To prospectively assess accuracy of mammography, clinical examina-tion, ultrasonography (US), and magnetic resonance (MR) imaging in preoperativeassessment of local extent of breast cancer.
MATERIALS AND METHODS: Institutional review board approval and informedpatient consent were obtained. Results of bilateral mammography, US, and con-trast-enhanced MR imaging were analyzed from 111 consecutive women withknown or suspected invasive breast cancer. Results were correlated with histopatho-logic findings.
RESULTS: Analysis included 177 malignant foci in 121 cancerous breasts, of which89 (50%) foci were palpable. Median size of 139 invasive foci was 18 mm (range,2–107 mm). Mammographic sensitivity decreased from 100% in fatty breasts to45% in extremely dense breasts. Mammographic sensitivity was highest for invasiveductal carcinoma (IDC) in 89 of 110 (81%) cases versus 10 of 29 (34%) cases ofinvasive lobular carcinoma (ILC) (P � .001) and 21 of 38 (55%) cases of ductalcarcinoma in situ (DCIS) (P � .01). US showed higher sensitivity than did mam-mography for IDC, depicting 104 of 110 (94%) cases, and for ILC, depicting 25 of29 (86%) cases (P � .01 for each). US showed higher sensitivity for invasive cancerthan DCIS (18 of 38 [47%], P � .001). MR showed higher sensitivity than didmammography for all tumor types (P � .01) and higher sensitivity than did US forDCIS (P � .001), depicting 105 of 110 (95%) cases of IDC, 28 of 29 (96%) cases ofILC, and 34 of 38 (89%) cases of DCIS. In anticipation of conservation or no surgeryafter mammography and clinical examination in 96 breasts, additional tumor(which altered surgical approach) was present in 30. Additional tumor was depictedin 17 of 96 (18%) breasts at US and in 29 of 96 (30%) at MR, though extent wasnow overestimated in 12 of 96 (12%) at US and 20 of 96 (21%) at MR imaging.After combined mammography, clinical examination, and US, MR depicted addi-tional tumor in another 12 of 96 (12%) breasts and led to overestimation of extentin another six (6%); US showed no detection benefit after MR imaging. Bilateralcancer was present in 10 of 111 (9%) patients; contralateral tumor was depictedmammographically in six and with both US and MR in an additional three. Onecontralateral cancer was demonstrated only clinically.
CONCLUSION: In nonfatty breasts, US and MR imaging were more sensitive thanmammography for invasive cancer, but both MR imaging and US involved risk ofoverestimation of tumor extent. Combined mammography, clinical examination, andMR imaging were more sensitive than any other individual test or combination of tests.© RSNA, 2004
With increasing use of reliable percutaneous biopsy techniques, a current goal in breast cancermanagement is accurate pretreatment planning to allow neoadjuvant chemotherapy or a
Breast Imaging
830
Ra
dio
logy

single definitive surgical procedure withlymph node sampling, as appropriate.Complete excision of malignant foci is thestandard, with the goal of achieving clearmargins of excision.
The sensitivity of mammography to theindex cancer ranges from 63% to 98% (1–3)and has been reported to be as low as 30%–48% in dense breasts (4,5). Several groupshave evaluated the preoperative use of sup-plemental magnetic resonance (MR) imag-ing (6–8), ultrasonography (US) (9,10), orboth (11,12) after mammography and clini-cal breast examination to assess the extent ofdisease within the breast(s). Across these se-ries, a change in management in 11%–15%of patients resulted from additional imagingafter mammography; 27%–34% of breastshad additional malignant foci not seenmammographically (6–10,12,13). The pur-pose of our study was to prospectively assessthe accuracy of mammography, clinical ex-amination, US, and MR imaging in the pre-operative assessment of the local extent ofbreast cancer. We further sought to deter-mine whether the accuracy of detectionmethods varied with breast density or tumortype.
MATERIALS AND METHODS
Entrance criteria consisted of women olderthan 18 years with newly diagnosed inva-sive breast cancer by means of core biopsyand/or high clinical or mammographicsuspicion of invasive breast cancer. Womenultimately shown to have ductal carci-noma in situ (DCIS) either had a larger areaof calcifications (�2.5 cm) mammographi-cally or a mass (either clinically or at imag-ing) and were therefore suspected of hav-ing an invasive component. Consecutivepatients at the University of Maryland wererecruited from September 1999 throughJanuary 2002. Women had to (a) agree toundergo bilateral mammography, whole-breast US, and contrast material–enhancedMR imaging of the breasts according toan institutional review board–approvedprotocol and (b) provide informed con-sent. Women who were unable to pro-vide consent or undergo MR imaging be-cause of a pacemaker, an aneurysm clip,or a metallic foreign body in or near theeye were excluded, as were patients whohad undergone open biopsy before mam-mography, US, and MR imaging could beperformed.
Imaging and Clinical ExaminationTechniques
Bilateral mammography was per-formed (Lo-Rad MIV unit, Hologic, Dan-
bury, Conn, or DMR Plus, GE MedicalSystems, Milwaukee, Wis) and includedroutine craniocaudal and mediolateraloblique views of the breast(s) and spot- orglobal-magnification views over the areaof the cancer. Findings were recordedprospectively according to the Breast Im-aging Reporting and Data System , or BI-RADS, lexicon (14) by one of several in-terpreting radiologists (including W.A.B.)who were qualified according to theMammography Quality Standards Actand had 2–10 years of experience inmammography. Findings ipsilateral tothe cancer, which were mammographi-cally probably benign, suspicious for can-cer, or highly suggestive of malignancy,were sampled for biopsy if the patientwas a candidate for conservation and ifthe identification of a malignancy at thatsite would change the surgical approach.Contralateral findings suspicious for orhighly suggestive of malignancy weresampled for biopsy. Mammography hadto be performed within 6 weeks of theother imaging studies.
Clinical breast examination was per-formed by one of two radiologists (in-cluding W.A.B.) with 2–10 years of expe-rience in clinical examination at the timeof whole-breast US. Any palpable lumpsin the breast(s) or axilla, skin thickeningor retraction, and nipple discharge or re-traction were noted.
Bilateral whole-breast US was performedwith knowledge of clinical and mammo-graphic findings either prior to MR imag-ing or afterward. US was performed by oneof two radiologists (including W.A.B.) with2–10 years of experience in the perfor-mance and interpretation of breast US,who were blinded to MR imaging results(US results were recorded prospectively).By using a linear-array broadband trans-ducer with a center frequency of 10 MHz,US was performed and supplemented witha linear-array transducer with a center fre-quency of 7.5 MHz as needed to penetratelarger breasts (Acoustic Imaging Performa,Tempe, Ariz, or Elegra, Siemens, Issaquah,Wash). For the inner breast, scanning wasperformed with the patient in the supineposition. For the outer breast, the patientwas placed in the contralateral posterioroblique position with the ipsilateral armraised. Survey scanning was performed intransverse and sagittal planes. Discrete le-sions were measured in both radial andantiradial scanning planes. When multiplesuspicious lesions were identified, pan-oramic display was used whenever possibleto document the distance between lesions.Spatial compounding was intermittentlyused in 20 cases.
Images and perpendicular measure-ments were documented for all discretefindings other than simple cysts. Biopsywas recommended for all palpable solidmasses and for incidental solid massesunless they were (a) circumscribed, oval,uniformly hypoechoic with no posteriorfeatures, and nonpalpable or (b) nonpal-pable complicated cysts. The latter twoclasses of lesions were classified as prob-ably benign at US and were recom-mended for short-interval (6-month) fol-low-up. If such lesions corresponded tosuspicious findings at MR imaging, thenbiopsy was performed, but the US classi-fication remained probably benign forpurposes of analysis. Solid lesions thatwould otherwise have been consideredprobably benign but were ipsilateral tocancers were aspirated or sampled for bi-opsy if a malignant result would changethe surgical approach.
MR imaging was performed with the pa-tient in the prone position in a dedicatedphased-array breast coil. A 1.5-T (n � 30) or1.0-T (n � 81) imager (Philips/MarconiMedical Systems, Cleveland, Ohio) wasused. Transverse T1-weighted MR images(repetition time msec/echo time msec,718/14; two signals acquired; field of view,32–40 cm; section thickness, 5 mm) wereobtained in both breasts, followed by sag-ittal T2-weighted fat-suppressed (6700–7072/68–88; two signals acquired; field ofview, 18 cm; section thickness, 4 mm)images at 1.5 T or inversion-recovery(7100/90/90 [inversion time]; flip angle,90°; one signal acquired; field of view, 18cm; section thickness, 4 mm) images at1.0 T acquired in each breast separately. Acoronal three-dimensional T1-weightedspoiled gradient-echo volume acquisition(10/3.6; flip angle, 30°; field of view, 34–42cm; section thickness, 2.0–2.9 mm; matrix,192 � 256) was then obtained both priorto and then three to six times over a periodof 5–8 minutes after intravenous injectionof 0.1 mmol per kilogram of body weightof gadopentetate dimeglumine (Magnev-ist; Schering, Berlin, Germany) over 20 sec-onds with a power injector.
Zero-filled interpolation was used for areconstruction matrix of 512 � 512; finalresolution was 1.8–2.2 mm in the phase-encoding direction by 1.5–1.9 mm in thefrequency-encoding direction with 1.0–1.4-mm section thickness. The dynamicacquisition consisted of three volumes at1.5 T and six volumes at 1.0 T obtainedafter administration of contrast material.The dynamic sequence was reviewedwith subtraction technique and maxi-mum intensity projection (MIP) tech-nique.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 831
Ra
dio
logy

Kinetic analysis was performed for re-gions of interest that were either drawnaround the entire lesion (for lesions � 5mm) or based on 4 pixels within the le-sion for lesions larger than 5 mm. Lesionsize was measured on selected MIPs (typ-ically those created from the secondpostinjection subtraction volume) in sag-ittal and transverse planes, and hard cop-ies were generated for clinical use.
Morphology (15) and kinetics (16) at MRimaging were evaluated for all enhancinglesions. Enhancement in contiguity withthe primary tumor was considered suspi-cious, regardless of size or morphology. Iso-lated discrete foci of enhancement thatshowed at least 70% increase in signal in-tensity over background in the first 90 sec-onds after injection and were at least 5 mmin size were considered suspicious unlessthere was (a) a benign correlate at mam-mography, US, or unenhanced MR imag-ing (eg, an intramammary lymph node ofnormal morphology or a fat-containingmass compatible with fat necrosis at T1-weighted MR imaging and/or at mammog-raphy) or (b) a probably benign correlate(such as clustered microcysts at inversion-recovery MR imaging and/or at US).
Lesions smaller than 5 mm with atleast 70% increase in signal intensitywithin the first 90 seconds of injectionwith washout kinetics (16) were also con-sidered suspicious. Regional areas of en-hancement with at least 60% increase insignal intensity within the first 90 sec-onds after contrast material injectionwere considered suspicious for malig-nancy and segmental, or linear clumpedenhancement was considered suspiciousfor DCIS, regardless of kinetics. Lesionsthat did not meet any of these criteriawere considered probably benign, withserial 6-month follow-up MR imagingrecommended. Findings were recordedprospectively.
One radiologist (W.A.B.) with 2 yearsof experience (prior to the study) in con-trast-enhanced breast MR imaging inter-pretation interpreted all MR images; USimages and mammograms were reviewedat the time of MR imaging interpretation,and clinical findings were known. Sec-ond-look US was performed and targetedto areas of concern on MR images whenthe lesion was not believed to have beenidentified at prospective US or mammog-raphy.
Biopsy Technique
Lesions considered suspicious for orhighly suggestive of malignancy withany modality were sampled for biopsy if a
malignant result would change the surgi-cal approach. Lesions considered proba-bly benign with any modality were sam-pled for biopsy if they were ipsilateral tocancer and a malignant result wouldchange the surgical approach. If a lesionwas clearly benign with any modality, itwas not sampled for biopsy. Core biopsyof more than two separate areas in anygiven breast was performed if the lesionshad a different appearance and malig-nant results would change the surgicalapproach.
Preoperative core-needle biopsy wasperformed with US guidance wheneverpossible by one of four radiologists(W.A.B.) or fellows who specialized inbreast imaging and had 6 months to 10years of experience. A 14-gauge automatedbiopsy gun (Monopty; Bard Urological,Covington, Ga) was used to sample lesionswith US guidance with a minimum ofthree passes per lesion. Specimen radiog-raphy was performed according to themethod of Berg et al (17). A clip (Micro-mark II; Biopsys division of Ethicon Endo-Surgery, Cincinnati, Ohio) was placed withUS guidance for lesions 7 mm or smaller,lesions with poor conspicuity, and thosedepicted with only US or MR imaging.The clip was placed via an 11-gauge tro-char (Bard Urological) according to themethod of Kopans (18). When a clip wasplaced, craniocaudal and true lateralmammographic views were acquired af-ter biopsy. Any malignant or atypical re-sult prompted excision, as did any discor-dant result. Follow-up was recommendedafter a benign concordant result.
When a lesion was seen only mammo-graphically and stereotactic biopsy was fea-sible, the patient was positioned prone ona digital stereotactic table (LoRad DSM; Ho-logic, Danbury, Conn). An 11-gauge probe(Biopsys division of Ethicon Endo-Surgery)was inserted, positioning was confirmed,and 12 samples were obtained in circum-ferential fashion with biopsies performedby one of four breast imaging radiologists(W.A.B.) with 2–10 years of experience.Specimen radiography and handling wasperformed as described earlier. A clip (Mi-cromark II; Biopsys division of EthiconEndo-Surgery) was placed in the posterioraspect of the biopsy cavity for all stereotac-tic biopsies.
For lesions first identified at MR imag-ing, mammograms were reevaluated, andsecond-look US was performed as needed.MR imaging–guided biopsy was availableby using a breast biopsy coil (MRI Devices,Waukesha, Wis, supplied by Philips/Mar-coni Medical Systems). During the courseof this study, no MR imaging–guided biop-
sies were required, since (a) the lesioncould be identified with either US or mam-mography or (b) wide excision or mastec-tomy was performed according to patientand physician choice. If the lesion(s) seenonly at MR imaging was not identifiedclearly at initial histopathologic examina-tion, the specimen was resectioned accord-ing to the clockface location and distancefrom the nipple of the MR imaging–de-picted abnormality (or abnormalities) afterdiscussion between the radiologist (W.A.B.)and pathologist (O.B.I.).
Histopathologic Examination
The reference standard was detailed se-rial 5-mm slicing of the surgical speci-men (lumpectomy or mastectomy) perthe method of Egan (19). The histopatho-logic specimen was viewed by one of twopathologists (O.B.I.) with 3–20 years ofexperience in breast pathology. Invasiveductal carcinoma (IDC) was graded ac-cording to the Nottingham system (20).DCIS was graded according to the nucleargrade (20). The number of slides contain-ing DCIS in relation to the total numberof slides was recorded as a surrogate mea-sure of histopathologic size. An extensiveintraductal component (EIC) was definedas tumor with an invasive component,where at least 25% of the tumor wasDCIS and there were additional discretefoci of DCIS outside the main tumormass (21,22).
Analysis
For each imaging modality, a cancerwas considered to be depicted success-fully (true-positive) if it appeared to besuspicious for or highly suggestive of ma-lignancy (14,23,24) with that modality.Lesions considered probably benign thatproved to be malignant at biopsy wereclassified as false-negative findings forthe modality (or modalities) with whichthey appeared probably benign (such as acluster of punctate calcifications or a cir-cumscribed mass at mammography, acomplicated cyst at US, or a round or ovalfocus showing �70% enhancement atMR imaging). If a malignancy was seenonly in retrospect or at repeat scanning(such as those seen at second-look US asdirected by findings at MR imaging), itwas classified as a false-negative findingfor that modality. A modality was creditedwith prompting an additional unnecessarybiopsy if the biopsy sample was not malig-nant and that tissue would otherwise nothave been sampled histologically. Con-tralateral probably benign findings were
832 � Radiology � December 2004 Berg et al
Ra
dio
logy

followed at 6, 12, and 24 months. Therates of additional induced follow-up andcompliance with these recommenda-tions were recorded.
The extent of disease was classified asfollows by using prospectively definedcriteria. Multifocal disease was defined asmultiple discrete discontinuous tumorfoci within 4 cm in one breast. Multicen-tric disease was defined as two or moremalignant foci separated by 4 cm or morein one breast (25). Disease was classifiedas diffuse if more than two quadrants hadmultiple discrete and/or contiguous tu-mor foci. Imaging findings could be alto-gether negative for cancer in that breast.Disease was considered to be underesti-mated with an imaging modality if thesize of the cancer was underestimated byat least 2 cm or if additional malignantfoci were missed that would have re-quired a wider surgical excision. Diseasewas considered to be overestimated if thesize of the primary tumor was overesti-mated by at least 2 cm or if there wereadditional suspicious foci that wouldhave prompted wider surgical excision(or mastectomy) unnecessarily.
In an effort to avoid artificially inflat-ing or deflating the performance of anyimaging modality, we sought practicaldefinitions of disease extent. All suspi-cious findings at imaging were evaluatedhistopathologically. However, since weare unaware of a circumstance whereby abreast with more than four distinct ma-lignant foci separated by more than 5 cmtotal would be recommended for conser-vation, we considered only the perfor-mance of the imaging modality in thedetection of no more than four suspi-cious foci in each breast, even if therewere diffuse foci of tumor. Similarly, wedid not specifically seek to perform corebiopsy in more than four lesions perbreast in any circumstance.
Statistical Methods
The sensitivity and accuracy of extentdetermination with each modality foreach tumor type were compared with thesensitivity and accuracy of extent deter-mination with mammography by usingthe McNemar test and t tests to deter-mine statistical significance. The McNe-mar test was performed for comparisonsof the same group of cases or matchedpairs of patients when comparing howdifferent imaging modalities performedin the same group of cases. t tests wereperformed in separate groups of cases—for example, when comparing across can-
cer types within the same imaging mo-dality.
The corresponding rates for each imag-ing modality combination were comparedwith the rates for mammography and clin-ical examination by using t tests. Indepen-dent comparisons were evaluated with the�2 test. The �2 test was also used to evaluatethe effect of breast density on the sensitiv-ity of imaging modalities.
Multivariate logistic regressions wereperformed with SAS version 8.1 software(SAS Institute, Cary, NC). Logistic multi-ple regression was used to analyze thepossible effect of independent variables,such as modality, tumor type, patientage, and breast density, on (a) accuratedetection of the presence of cancer and(b) accurate depiction of the extent ofcancer (not over- or underestimated). Inaddition to the use of the McNemar testwhen comparing matched pairs of cases,we controlled for cluster and/or depen-dency issues that stemmed from the pres-ence of multiple imaging studies read inthe same patient and the presence ofmultiple lesions by using random-effectslogistic regression. We treated the vari-ability across multiple imaging studiesread in the same patient as a randomeffect.
RESULTS
A total of 120 patients were eligible forthis study. Seven did not participate be-cause of surgeon preference (n � 3, allwith fatty breasts), patient claustropho-bia (n � 3), or scheduling constraints(n � 1). Results from two patients wereexcluded because contrast material injec-tion failed during MR imaging (not rec-ognized by the technologist or patient).In the 111 analyzable women enrolled instudy, the mean age was 48.7 years; me-dian age was 48 years (age range, 26–81years). The presenting (index) lesionproved malignant in 110 of 111 (99.1%)patients (with one focus of architecturaldistortion yielding atypical ductal hyper-plasia at excision); 80 (73%) of these 110lesions were palpable.
A total of 258 discrete lesions, including177 malignancies, were correlated withhistopathologic findings in 121 breastswith cancer. There were 110 foci of inva-sive ductal cancer (including 51 foci withassociated intraductal carcinoma, of which19 had an EIC, and five had mixed IDCand invasive lobular carcinoma [ILC]), 38foci of DCIS (not including EIC cases), 29foci of ILC, 12 atypical lesions (all excisedafter initial diagnosis at core biopsy, with
the same or benign results, including fiveatypical papillomas, three lobular carcino-mas in situ, two cases of atypical lobularhyperplasia, and two cases of atypical duc-tal hyperplasia), and 69 concordant benigndiagnoses (19 fibroadenomas, 19 fibrocys-tic changes, nine cases of sclerosing adeno-sis, seven cases of fibrosis, six papillomas,four ruptured cysts, two lymph nodes, andone case each of foreign body granuloma,chronic inflammatory changes, and lacta-tional changes). One patient presented forevaluation of a new area of architecturaldistortion mammographically in one breast,which proved to be only atypical ductalhyperplasia at excision, with a contralat-eral tubular cancer found only at MR im-aging (Fig 1).
Surgical Approach: Multifocal andMulticentric Disease
Conservation surgery was performed in54 breasts, including 48 breasts with singledefinitive lumpectomy, three with wideexcision (quadrantectomy), and three withdouble lumpectomy. Four of 54 (7%)breasts had positive margins that necessi-tated repeat excision. Mastectomy was per-formed in 67 breasts with cancer, includ-ing 25 recommended on the basis ofcombined mammography and clinical ex-amination. Of 96 breasts in which conser-vation or no surgery was planned aftermammography and clinical examination,(a) 24 (25%) were recommended formastectomy on the basis of MR imagingfindings, in which five cases were overesti-mated, and (b) 19 (20%) were recom-mended for mastectomy on the basis of USfindings, in which four cases were overes-timated. There were no breasts in which USfindings changed the overall managementafter MR imaging (all those converted tomastectomy on the basis of US were alsoconverted on the basis of MR imaging).Fourteen mastectomies were performed ac-cording to patient choice, and anotherfour followed initial lumpectomy withpositive margins.
Of the 121 breasts with cancer, 75(62%) had solitary tumors, of whichseven were classified as “diffuse” becausethey were larger than 7 cm. Eleven (9%)breasts had diffuse foci of cancer in mul-tiple quadrants; 29 (24%) had multifocalcancer within 4 cm surrounding the in-dex lesion, and six (5%) had isolatedmulticentric foci of cancer.
Overall Performance
Table 1 summarizes the overall perfor-mance of each of the imaging modalities
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 833
Ra
dio
logy
and combinations of modalities. Thecombination of mammography, clinicalexamination, and MR imaging was themost sensitive, depicting 176 of 177(99.4%) of all malignant foci. This com-bination was significantly better than thecombination of mammography, clinicalexamination, and US, which depicted165 of 177 (93.2%) foci (P � .001) (Tables1–3). Mammography combined with
clinical examination was more accurateoverall than clinical examination alone(P � .001) or mammography alone (P �.001). With regard to only dense and het-erogeneously dense breasts, however, theaccuracy of mammography and clinicalexamination combined was not signifi-cantly better than that of clinical exami-nation alone (131 of 168 [78.0%] foci vs123 of 168 [73.2%] foci). Because of the
substantial risk of false-positive findingswith both US and MR imaging, the over-all accuracy of US or MR imaging alone orin combination with mammography andclinical examination was no higher thanthe accuracy of mammography alone(Table 1).
For 96 breasts in which conservation orno surgery was planned after mammog-raphy and clinical examination, tumor
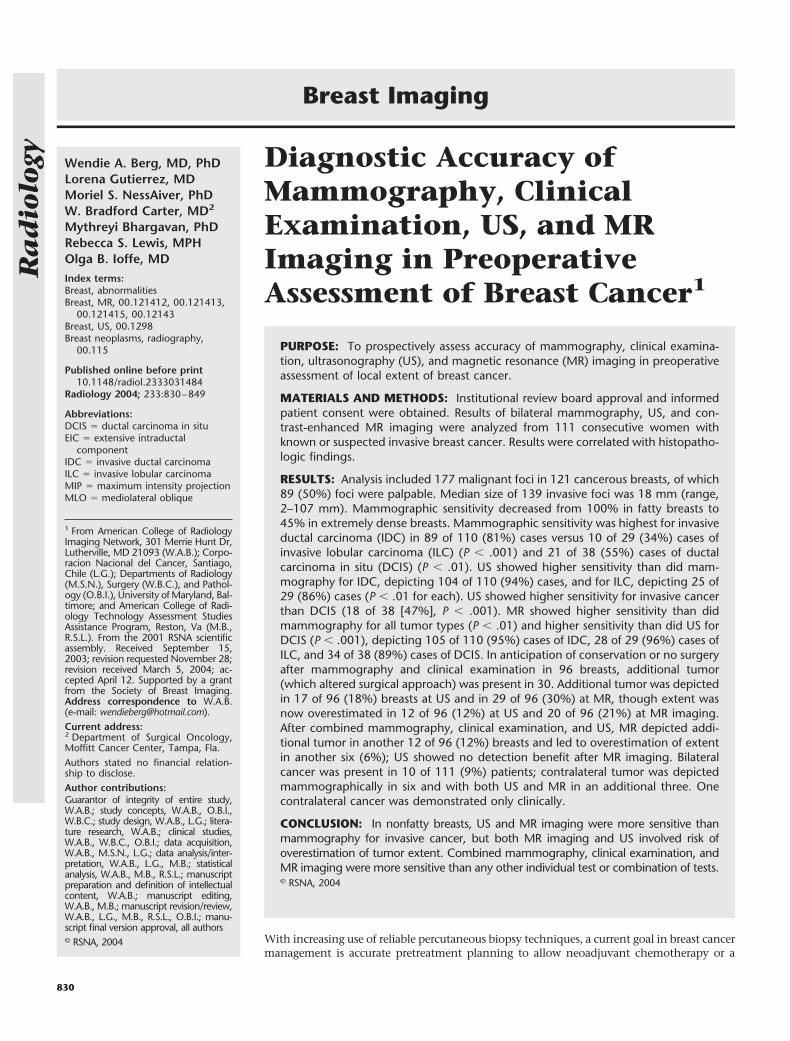
Figure 1. Images in 46-year-old woman with nonpalpable 5-mm tubular carcinoma in left breast seen only at MR imaging. (a) Bilateralmediolateral oblique (MLO) and (b) spot-magnification mediolateral mammograms show subtle architectural distortion (arrow) suspicious forcarcinoma in right breast, which proved to be atypical ductal hyperplasia at excision. (c) Transverse MIP reconstruction of subtracted three-dimensional spoiled gradient-echo coronal volume MR acquisition obtained 90 seconds after intravenous administration of 0.1 mmol/kg gado-pentetate dimeglumine (10/3.6; flip angle, 30°; section thickness, 2.2 mm; field of view, 36 cm; 1.0 T) shows solitary intensely enhancing mass(arrowhead) in upper inner left breast and no abnormal enhancement in right breast. (d) Sagittal second-look US image (L12–7.5-MHz transducer)obtained in 10 o’clock position in left breast demonstrates irregular hypoechoic shadowing mass (arrowhead). US-guided needle localizationrevealed 5-mm (tubular) IDC. Patient underwent lumpectomy with radiation therapy.
834 � Radiology � December 2004 Berg et al
Ra
dio
logy
was missed altogether in eight (8.3%)breasts. In 22 of the 96 (23%) breasts,tumor size was underestimated by at least2 cm, or additional tumor foci were un-derestimated. In another three (3.1%),tumor size was overestimated by at least 2cm, or additional suspicious foci led tooverestimation of disease extent (Tables4–6). Supplemental US after mammogra-phy and clinical examination depictedadditional tumor foci that expanded thesurgical approach in 17 of 96 (18%)breasts. For the 96 breasts, after com-bined mammography, clinical examina-tion, and US, cancer was missed in two(2.1%), underestimated in 15 (16%), andoverestimated in 12 (12%). SupplementalMR imaging after mammography andclinical examination depicted additionaltumor that appropriately expanded thesurgical approach in 29 of 96 (30%)breasts. With mammography, clinical ex-amination, and MR imaging, extent ofdisease was only underestimated in one(1%) breast but was overestimated in 20(21%). The addition of US to this combi-nation of tests provided no additionaldiagnostic yield. After combined mam-mography, clinical examination, and US,MR imaging depicted additional tumorin 12 of 96 (12%) breasts in which con-servation or no surgery had beenplanned. Five of 12 (42%) of the breastswith more extensive tumor only at MRimaging resulted from depiction of anEIC.
Performance as a Function ofTumor Type
IDC.—Of 110 foci of IDC, 73 (66%)were palpable. Mammography was lesssensitive in the depiction of IDC thanwas either US or MR imaging (P � .01 foreach), with no statistically significant dif-ference in sensitivity between US and MRimaging. Specifically, mammography de-picted 89 (81%) foci of IDC, US depicted
104 (94.5%), and MR imaging depicted105 (95.4%) (Table 2). Two small indexIDC foci (one 4-mm colloid IDC and one6-mm grade II IDC with DCIS) were seenonly with mammography, and two (one5-mm tubular IDC [Fig 1] and one 8-mmgrade II IDC) were seen only with MRimaging. The combination of mammog-raphy and clinical examination depicted98 of 110 (89.1%) IDC foci. The combi-nation of mammography, clinical exam-ination, and US depicted 108 (98.2%)IDC foci. The combination of mammog-raphy, clinical examination, and MR im-aging depicted 110 (100%) IDC foci (Ta-ble 2). The addition of either US or MRimaging to mammography and clinicalexamination significantly improved de-tection (P � .005 for each). Of the 21mammographically occult foci of IDC, 18(86%) were depicted at initial US (withanother two at second-look US), and 20(95%) were depicted at MR imaging (Ta-ble 3).
Mammographic sensitivity was in-versely related to breast density (P �.001), with 18 of 30 (60%) foci of IDCdepicted in dense breasts, 31 of 36 (86%)depicted in heterogeneously dense breasts,34 of 38 (89%) depicted in breasts withminimal scattered fibroglandular den-sity, and six of six (100%) depicted infatty breasts (Table 2). Of the 18 foci ofIDC depicted mammographically in densebreasts, 17 (94%) were palpable. Random-effects logistic regression analysis showedthat age did not affect mammographic sen-sitivity independent of density. Breast den-sity did not affect the sensitivity of US orMR imaging.
Ninety-two breasts were found to haveIDC; of these, 43 (47%) had associatedDCIS, including 19 (21%) with EIC. Fourwere mixed IDC and ILC. Of the 92breasts, six (6.5%) had “incidental” IDCat additional imaging that was not de-tected at either mammography or clinical
examination, with two of those occult toinitial US, as well. Of the 92 breasts withIDC, 14 (15%) had diffuse tumor (six ac-cording to primary tumor size larger than7 cm and eight with diffuse foci), four(4.3%) were multicentric, 19 (21%) weremultifocal, and 55 (60%) were solitaryand smaller than 5 cm.
Twenty-one breasts with IDC were rec-ommended for mastectomy on the basisof mammography and clinical examina-tion findings; indeed, the findings in five(24%) of these 21 were ultimately overes-timated not only mammographically butalso on the basis of US and MR imagingfindings.
Among the 72 breasts with IDC forwhich conservation or no surgery wasplanned after mammography and clini-cal examination, the tumor was missedaltogether in six of 72 (8%) breasts, andthe extent of tumor was underestimatedin another 15 (21%) breasts (Table 4). Ofthe 15 underestimates, three (20%) weredue to EIC alone, two (13%) were due tosize, and 10 (67%) were due to discreteadditional foci of tumor (three of whichalso had underestimated EIC). Thus,there were six outright misses and an-other 10 with missed discrete additionaltumor foci, for a total of 16 breasts withmissed tumor after mammography andclinical examination. This number repre-sents 17% of the 92 breasts with IDC withadditional tumor that potentially wouldhave been missed even if clear margins ofexcision had been achieved, had man-agement been based on the combinationof mammography and clinical examina-tion.
US alone (performed with knowledgeof mammographic and clinical findings)was more accurate than mammographyin the depiction of disease extent for IDC(P � .05), but the combination of mam-mography, clinical examination, and USwas not significantly more accurate in
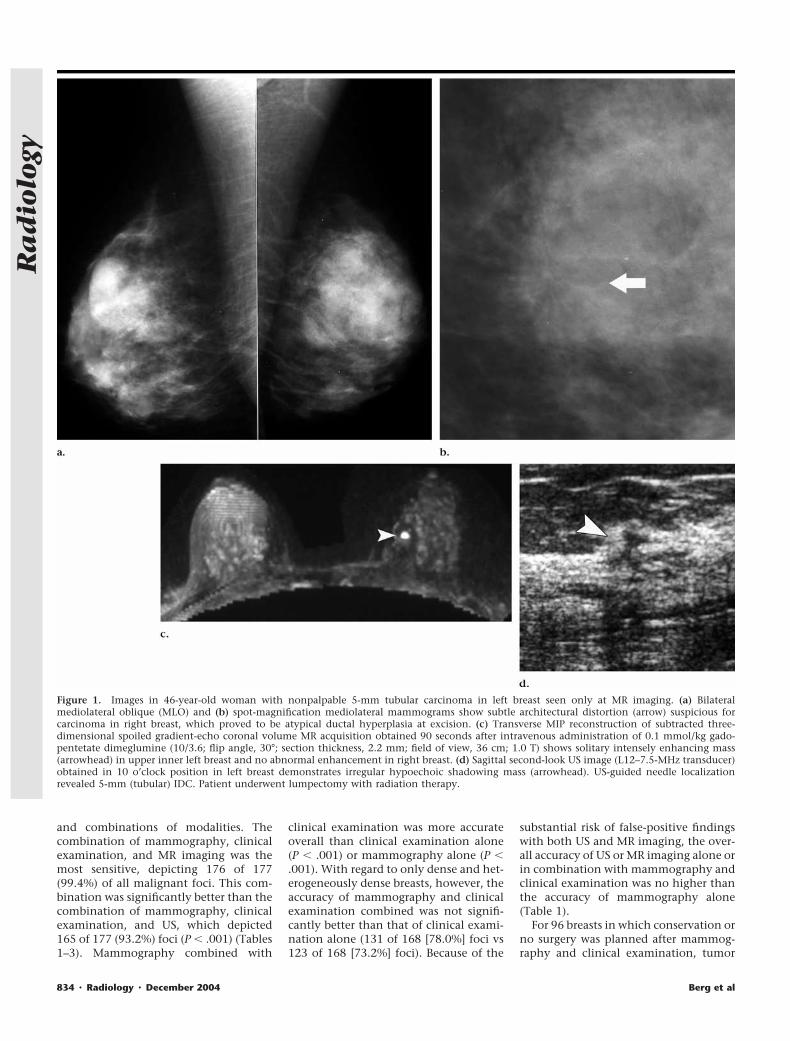
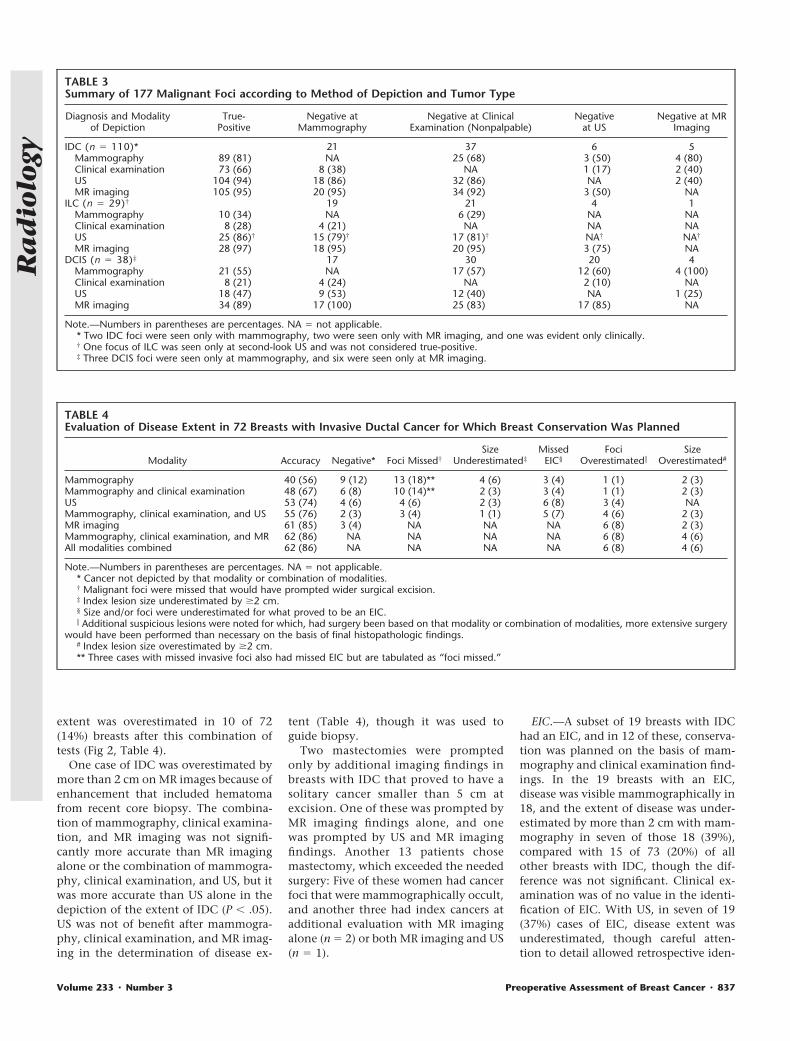
TABLE 1Diagnostic Performance in 258 Proven Lesions (177 Malignancies and 81 Benign Lesions)
Modality Sensitivity Specificity Positive Predictive Value Accuracy
Mammography 120/177 (67.8) 61/81 (75) 120/140 (85.7) 181/258 (70.2)Mammography and clinical examination 137/177 (77.4) 58/81 (72) 137/160 (85.6) 195/258 (75.6)Clinical examination 89/177 (50.3) 75/81 (92) 89/95 (94) 164/258 (63.6)US 147/177 (83.0) 28/81 (34) 147/200 (73.5) 175/258 (67.8)Mammography and US 162/177 (91.5) 19/81 (23) 162/224 (72.3) 181/258 (70.2)Mammography, clinical examination, and US 165/177 (93.2) 18/81 (22) 165/228 (72.4) 183/258 (70.9)MR imaging 167/177 (94.4) 21/81 (26) 167/227 (73.6) 188/258 (72.9)Mammography, clinical examination, and MR 176/177 (99.4) 6/81 (7) 176/251 (70.1) 182/258 (70.5)
NOTE.—Numbers in parentheses are percentages.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 835
Ra
dio
logy
the depiction of disease extent thanmammography and clinical examinationalone. MR imaging alone (interpretedwith knowledge of mammographic andclinical findings) was more accurate than
mammography in the assessment of dis-ease extent (P � .001). The combinationof mammography, clinical examination,and MR imaging provided significantlymore accurate assessment of disease ex-
tent than did mammography and clinicalexamination alone (P � .01). The combi-nation of mammography, clinical exam-ination, and MR imaging left no under-estimates of extent of IDC, but IDC
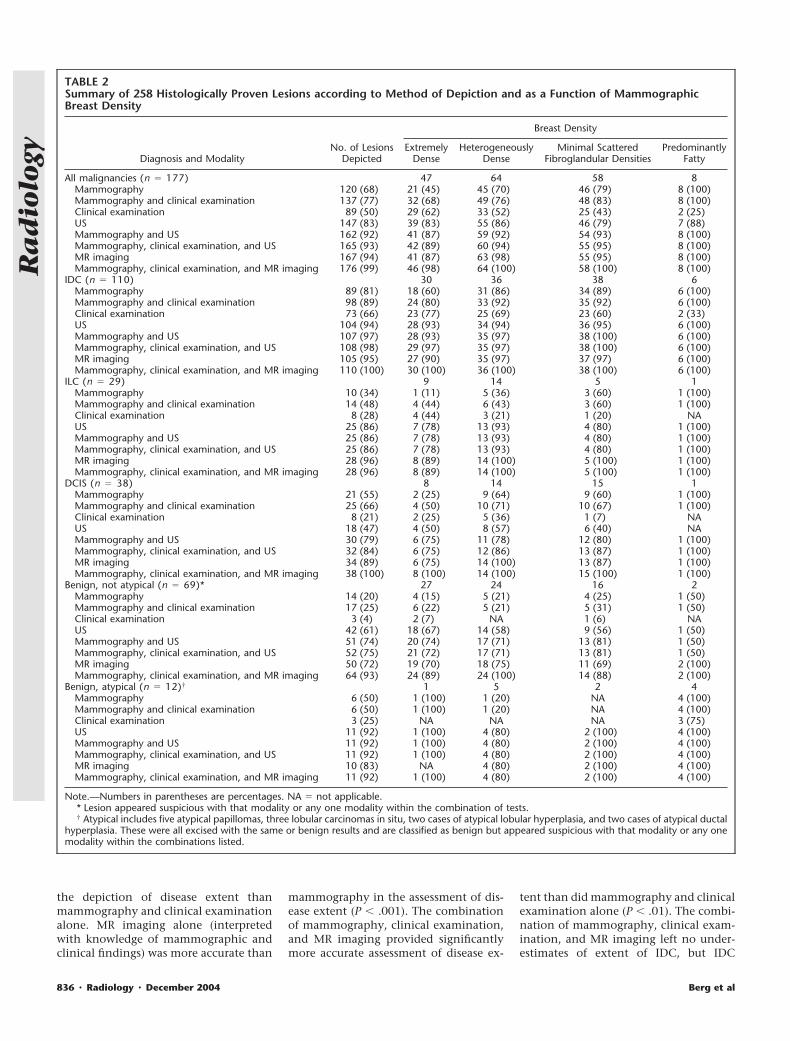
TABLE 2Summary of 258 Histologically Proven Lesions according to Method of Depiction and as a Function of MammographicBreast Density
Diagnosis and ModalityNo. of Lesions
Depicted
Breast Density
ExtremelyDense
HeterogeneouslyDense
Minimal ScatteredFibroglandular Densities
PredominantlyFatty
All malignancies (n � 177) 47 64 58 8Mammography 120 (68) 21 (45) 45 (70) 46 (79) 8 (100)Mammography and clinical examination 137 (77) 32 (68) 49 (76) 48 (83) 8 (100)Clinical examination 89 (50) 29 (62) 33 (52) 25 (43) 2 (25)US 147 (83) 39 (83) 55 (86) 46 (79) 7 (88)Mammography and US 162 (92) 41 (87) 59 (92) 54 (93) 8 (100)Mammography, clinical examination, and US 165 (93) 42 (89) 60 (94) 55 (95) 8 (100)MR imaging 167 (94) 41 (87) 63 (98) 55 (95) 8 (100)Mammography, clinical examination, and MR imaging 176 (99) 46 (98) 64 (100) 58 (100) 8 (100)
IDC (n � 110) 30 36 38 6Mammography 89 (81) 18 (60) 31 (86) 34 (89) 6 (100)Mammography and clinical examination 98 (89) 24 (80) 33 (92) 35 (92) 6 (100)Clinical examination 73 (66) 23 (77) 25 (69) 23 (60) 2 (33)US 104 (94) 28 (93) 34 (94) 36 (95) 6 (100)Mammography and US 107 (97) 28 (93) 35 (97) 38 (100) 6 (100)Mammography, clinical examination, and US 108 (98) 29 (97) 35 (97) 38 (100) 6 (100)MR imaging 105 (95) 27 (90) 35 (97) 37 (97) 6 (100)Mammography, clinical examination, and MR imaging 110 (100) 30 (100) 36 (100) 38 (100) 6 (100)
ILC (n � 29) 9 14 5 1Mammography 10 (34) 1 (11) 5 (36) 3 (60) 1 (100)Mammography and clinical examination 14 (48) 4 (44) 6 (43) 3 (60) 1 (100)Clinical examination 8 (28) 4 (44) 3 (21) 1 (20) NAUS 25 (86) 7 (78) 13 (93) 4 (80) 1 (100)Mammography and US 25 (86) 7 (78) 13 (93) 4 (80) 1 (100)Mammography, clinical examination, and US 25 (86) 7 (78) 13 (93) 4 (80) 1 (100)MR imaging 28 (96) 8 (89) 14 (100) 5 (100) 1 (100)Mammography, clinical examination, and MR imaging 28 (96) 8 (89) 14 (100) 5 (100) 1 (100)
DCIS (n � 38) 8 14 15 1Mammography 21 (55) 2 (25) 9 (64) 9 (60) 1 (100)Mammography and clinical examination 25 (66) 4 (50) 10 (71) 10 (67) 1 (100)Clinical examination 8 (21) 2 (25) 5 (36) 1 (7) NAUS 18 (47) 4 (50) 8 (57) 6 (40) NAMammography and US 30 (79) 6 (75) 11 (78) 12 (80) 1 (100)Mammography, clinical examination, and US 32 (84) 6 (75) 12 (86) 13 (87) 1 (100)MR imaging 34 (89) 6 (75) 14 (100) 13 (87) 1 (100)Mammography, clinical examination, and MR imaging 38 (100) 8 (100) 14 (100) 15 (100) 1 (100)
Benign, not atypical (n � 69)* 27 24 16 2Mammography 14 (20) 4 (15) 5 (21) 4 (25) 1 (50)Mammography and clinical examination 17 (25) 6 (22) 5 (21) 5 (31) 1 (50)Clinical examination 3 (4) 2 (7) NA 1 (6) NAUS 42 (61) 18 (67) 14 (58) 9 (56) 1 (50)Mammography and US 51 (74) 20 (74) 17 (71) 13 (81) 1 (50)Mammography, clinical examination, and US 52 (75) 21 (72) 17 (71) 13 (81) 1 (50)MR imaging 50 (72) 19 (70) 18 (75) 11 (69) 2 (100)Mammography, clinical examination, and MR imaging 64 (93) 24 (89) 24 (100) 14 (88) 2 (100)
Benign, atypical (n � 12)† 1 5 2 4Mammography 6 (50) 1 (100) 1 (20) NA 4 (100)Mammography and clinical examination 6 (50) 1 (100) 1 (20) NA 4 (100)Clinical examination 3 (25) NA NA NA 3 (75)US 11 (92) 1 (100) 4 (80) 2 (100) 4 (100)Mammography and US 11 (92) 1 (100) 4 (80) 2 (100) 4 (100)Mammography, clinical examination, and US 11 (92) 1 (100) 4 (80) 2 (100) 4 (100)MR imaging 10 (83) NA 4 (80) 2 (100) 4 (100)Mammography, clinical examination, and MR imaging 11 (92) 1 (100) 4 (80) 2 (100) 4 (100)
Note.—Numbers in parentheses are percentages. NA � not applicable.* Lesion appeared suspicious with that modality or any one modality within the combination of tests.† Atypical includes five atypical papillomas, three lobular carcinomas in situ, two cases of atypical lobular hyperplasia, and two cases of atypical ductal
hyperplasia. These were all excised with the same or benign results and are classified as benign but appeared suspicious with that modality or any onemodality within the combinations listed.
836 � Radiology � December 2004 Berg et al
Ra
dio
logy
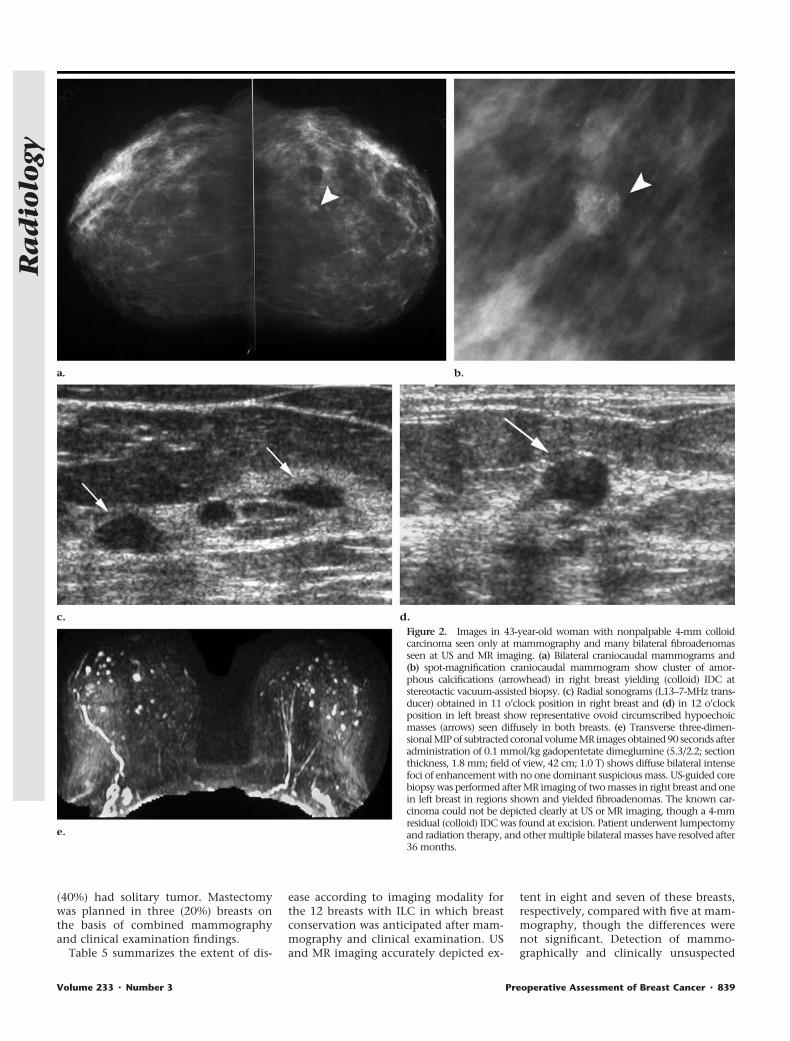
extent was overestimated in 10 of 72(14%) breasts after this combination oftests (Fig 2, Table 4).
One case of IDC was overestimated bymore than 2 cm on MR images because ofenhancement that included hematomafrom recent core biopsy. The combina-tion of mammography, clinical examina-tion, and MR imaging was not signifi-cantly more accurate than MR imagingalone or the combination of mammogra-phy, clinical examination, and US, but itwas more accurate than US alone in thedepiction of the extent of IDC (P � .05).US was not of benefit after mammogra-phy, clinical examination, and MR imag-ing in the determination of disease ex-
tent (Table 4), though it was used toguide biopsy.
Two mastectomies were promptedonly by additional imaging findings inbreasts with IDC that proved to have asolitary cancer smaller than 5 cm atexcision. One of these was prompted byMR imaging findings alone, and onewas prompted by US and MR imagingfindings. Another 13 patients chosemastectomy, which exceeded the neededsurgery: Five of these women had cancerfoci that were mammographically occult,and another three had index cancers atadditional evaluation with MR imagingalone (n � 2) or both MR imaging and US(n � 1).
EIC.—A subset of 19 breasts with IDChad an EIC, and in 12 of these, conserva-tion was planned on the basis of mam-mography and clinical examination find-ings. In the 19 breasts with an EIC,disease was visible mammographically in18, and the extent of disease was under-estimated by more than 2 cm with mam-mography in seven of those 18 (39%),compared with 15 of 73 (20%) of allother breasts with IDC, though the dif-ference was not significant. Clinical ex-amination was of no value in the identi-fication of EIC. With US, in seven of 19(37%) cases of EIC, disease extent wasunderestimated, though careful atten-tion to detail allowed retrospective iden-
TABLE 3Summary of 177 Malignant Foci according to Method of Depiction and Tumor Type
Diagnosis and Modalityof Depiction
True-Positive
Negative atMammography
Negative at ClinicalExamination (Nonpalpable)
Negativeat US
Negative at MRImaging
IDC (n � 110)* 21 37 6 5Mammography 89 (81) NA 25 (68) 3 (50) 4 (80)Clinical examination 73 (66) 8 (38) NA 1 (17) 2 (40)US 104 (94) 18 (86) 32 (86) NA 2 (40)MR imaging 105 (95) 20 (95) 34 (92) 3 (50) NA
ILC (n � 29)† 19 21 4 1Mammography 10 (34) NA 6 (29) NA NAClinical examination 8 (28) 4 (21) NA NA NAUS 25 (86)† 15 (79)† 17 (81)† NA† NA†
MR imaging 28 (97) 18 (95) 20 (95) 3 (75) NADCIS (n � 38)‡ 17 30 20 4
Mammography 21 (55) NA 17 (57) 12 (60) 4 (100)Clinical examination 8 (21) 4 (24) NA 2 (10) NAUS 18 (47) 9 (53) 12 (40) NA 1 (25)MR imaging 34 (89) 17 (100) 25 (83) 17 (85) NA
Note.—Numbers in parentheses are percentages. NA � not applicable.* Two IDC foci were seen only with mammography, two were seen only with MR imaging, and one was evident only clinically.† One focus of ILC was seen only at second-look US and was not considered true-positive.‡ Three DCIS foci were seen only at mammography, and six were seen only at MR imaging.
TABLE 4Evaluation of Disease Extent in 72 Breasts with Invasive Ductal Cancer for Which Breast Conservation Was Planned
Modality Accuracy Negative* Foci Missed†Size
Underestimated‡Missed
EIC§Foci
Overestimated�Size
Overestimated#
Mammography 40 (56) 9 (12) 13 (18)** 4 (6) 3 (4) 1 (1) 2 (3)Mammography and clinical examination 48 (67) 6 (8) 10 (14)** 2 (3) 3 (4) 1 (1) 2 (3)US 53 (74) 4 (6) 4 (6) 2 (3) 6 (8) 3 (4) NAMammography, clinical examination, and US 55 (76) 2 (3) 3 (4) 1 (1) 5 (7) 4 (6) 2 (3)MR imaging 61 (85) 3 (4) NA NA NA 6 (8) 2 (3)Mammography, clinical examination, and MR 62 (86) NA NA NA NA 6 (8) 4 (6)All modalities combined 62 (86) NA NA NA NA 6 (8) 4 (6)
Note.—Numbers in parentheses are percentages. NA � not applicable.* Cancer not depicted by that modality or combination of modalities.† Malignant foci were missed that would have prompted wider surgical excision.‡ Index lesion size underestimated by �2 cm.§ Size and/or foci were underestimated for what proved to be an EIC.� Additional suspicious lesions were noted for which, had surgery been based on that modality or combination of modalities, more extensive surgery
would have been performed than necessary on the basis of final histopathologic findings.# Index lesion size overestimated by �2 cm.** Three cases with missed invasive foci also had missed EIC but are tabulated as “foci missed.”
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 837
Ra
dio
logy

tification in five cases in which second-look US was performed (Fig 3). In six of19 (32%) breasts with EIC, only MR im-aging depicted the EIC; five of those sixEIC cases seen only at MR imaging werein breasts in which conservation was an-ticipated. Findings in only one (5%)breast with EIC were underestimated atMR imaging, with the EIC seen at bothmammography and US in that breast.
ILC.—Twenty-nine foci of ILC wereevaluated, of which eight (28%) were pal-pable. Mammography was less sensitiveto ILC than IDC (P � .001). Mammogra-phy was less sensitive to ILC than wereUS or MR imaging (P � .001 for eachcomparison), with no statistically signif-icant difference in sensitivity between USand MR imaging. Specifically, mammog-
raphy depicted 10 of 29 (34%) foci of ILC,US depicted 25 (86%), and MR imagingdepicted 28 (96%) (Table 2). Two foci ofILC were depicted only at MR imaging,and one was depicted only at second-look US. The combination of mammog-raphy and clinical examination allowedidentification of 14 of 29 (48%) cases ofILC. Mammography and US with orwithout clinical examination depicted 25of 29 (86%) cases; mammography, clini-cal examination, and MR imaging de-picted 28 of 29 (96%) cases. The additionof either US or MR imaging to mammog-raphy and clinical examination signifi-cantly improved detection of ILC (P �.001 each for US and MR imaging) (Ta-bles 2, 3).
As with IDC, mammographic sensitiv-
ity to ILC was again inversely related tobreast density, with one of nine (11%)cases of ILC depicted in dense breasts,five of 14 (36%) depicted in heteroge-neously dense breasts, three of five (60%)depicted in breasts with minimal scat-tered fibroglandular density, and one ofone (100%) depicted in fatty breasts (P �.001) (Table 2). Of the nine foci of ILC indense breasts, all had palpable index le-sions. As with IDC, breast density did notaffect US or MR imaging sensitivity.
The management of 15 breasts wasbased on presence of ILC. Of the 15breasts with ILC, three (20%) had diffusetumor (one according to tumor size largerthan 7 cm and two according to diffusefoci), one (6.7%) had multicentric tumor,five (33%) had multifocal tumor, and six
TABLE 5Evaluation of Disease Extent in 12 Breasts with Invasive Lobular Cancer for Which Breast Conservation Was Planned
Modality Accuracy Negative* Foci Missed†Size
Underestimated‡Foci
Overestimated§Size
Overestimated�
Mammography 5 (42) 4 (33) 3 (25) NA NA NAMammography and clinical examination 5 (42) 2 (17) 5 (42) NA NA NAUS 8 (67) NA 2 (17) NA 2 (17) NAMammography, clinical examination, and US 8 (67) NA 2 (17) NA 2 (17) NAMR imaging 7 (58) NA 1 (8)# NA 4 (33) NAMammography, clinical examination, and MR 7 (58) NA 1 (8) NA 4 (33) NAAll modalities combined 7 (58) NA 1 (8) NA 4 (33) NA
Note.—Numbers in parentheses are percentages. NA � not applicable.* Cancer not depicted by that modality or combination of modalities.† Malignant foci were missed that would have prompted wider surgical excision.‡ Index lesion size underestimated by �2 cm.§ Additional suspicious lesions were noted for which, had surgery been based on that modality or combination of modalities, more extensive surgery
would have been performed than necessary on the basis of final histopathologic findings. All breasts with overestimated foci of tumor were due to fociof lobular carcinoma in situ.
� Index lesion size overestimated by �2 cm.# In one breast with ILC, additional tumor was found only at second-look US.
TABLE 6Evaluation of Disease Extent in 12 Breasts with DCIS for Which Breast Conservation Was Planned
Modality Accuracy Negative* Foci Missed†Size
Underestimated‡Foci
Overestimated§Size
Overestimated�
Mammography 6 (50) 4 (33) 1 (8) 1 (8) NA NAMammography and clinical examination 10 (83) NA 1 (8) 1 (8) NA NAUS 4 (33) 4 (33)# NA NA 4 (33)# NAMammography, clinical examination, and US 8 (75) NA NA NA 4 (33)# NAMR imaging 5 (42) 1 (8)# NA NA 5 (42)#,** 1 (8)**Mammography, clinical examination, and MR 6 (50) NA NA NA 5 (42)** 1 (8)**All modalities combined 6 (50) NA NA NA 5 (42)** 1 (8)**
Note.—Numbers in parentheses are percentages. NA � not applicable.* Cancer not depicted by that modality or combination of modalities.† Malignant foci were missed that would have prompted wider surgical excision.‡ Index lesion size underestimated by �2 cm.§ Additional suspicious lesions were noted for which, had surgery been based on that modality or combination of modalities, more extensive surgery
would have been performed than necessary on the basis of final histopathologic findings.� Index lesion size overestimated by �2 cm.# In two breasts with DCIS, there were multiple false-positive findings at both US and MR imaging, though the index DCIS was occult. When
combined with mammography, disease extent appeared overestimated. These are listed as “overestimated foci,” though they could have been listedas “negative” for each of US and MR imaging.
** Both size and foci were overestimated at MR imaging in one breast, listed as “size overestimated.”
838 � Radiology � December 2004 Berg et al
Ra
dio
logy
(40%) had solitary tumor. Mastectomywas planned in three (20%) breasts onthe basis of combined mammographyand clinical examination findings.
Table 5 summarizes the extent of dis-
ease according to imaging modality forthe 12 breasts with ILC in which breastconservation was anticipated after mam-mography and clinical examination. USand MR imaging accurately depicted ex-
tent in eight and seven of these breasts,respectively, compared with five at mam-mography, though the differences werenot significant. Detection of mammo-graphically and clinically unsuspected
Figure 2. Images in 43-year-old woman with nonpalpable 4-mm colloidcarcinoma seen only at mammography and many bilateral fibroadenomasseen at US and MR imaging. (a) Bilateral craniocaudal mammograms and(b) spot-magnification craniocaudal mammogram show cluster of amor-phous calcifications (arrowhead) in right breast yielding (colloid) IDC atstereotactic vacuum-assisted biopsy. (c) Radial sonograms (L13–7-MHz trans-ducer) obtained in 11 o’clock position in right breast and (d) in 12 o’clockposition in left breast show representative ovoid circumscribed hypoechoicmasses (arrows) seen diffusely in both breasts. (e) Transverse three-dimen-sional MIP of subtracted coronal volume MR images obtained 90 seconds afteradministration of 0.1 mmol/kg gadopentetate dimeglumine (5.3/2.2; sectionthickness, 1.8 mm; field of view, 42 cm; 1.0 T) shows diffuse bilateral intensefoci of enhancement with no one dominant suspicious mass. US-guided corebiopsy was performed after MR imaging of two masses in right breast and onein left breast in regions shown and yielded fibroadenomas. The known car-cinoma could not be depicted clearly at US or MR imaging, though a 4-mmresidual (colloid) IDC was found at excision. Patient underwent lumpectomyand radiation therapy, and other multiple bilateral masses have resolved after36 months.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 839
Ra
dio
logy
contralateral ILC occurred in two breastson the basis of additional imaging withUS and MR imaging (Fig 4). US and MRimaging were both hampered by false-positive findings due to lobular carci-noma in situ (Fig 5). Two patients hadpotentially unnecessary mastectomy onthe basis of US and MR imaging findings(Fig 5).
DCIS.—Of 38 foci of DCIS evaluated,21 (55%) were depicted mammographi-cally, and eight of 38 (21%) were clini-cally evident (six foci were palpable, andtwo breasts had Paget disease of the nip-ple). Three (8%) DCIS foci were seen onlymammographically. US was less sensitivefor DCIS than for IDC or ILC (P � .001),with 18 of 38 (47%) foci identified ini-
tially and another three (8%) seen at sec-ond-look US. MR imaging depicted 34 of38 (89%) DCIS foci, which was signifi-cantly more than that depicted with US(P � .001) or mammography (P � .01)(Table 2). Six foci of DCIS were seen onlyat MR imaging.
The foci of DCIS depicted mammo-graphically included two of eight (25%)in dense breasts, nine of 14 (64%) inbreasts with heterogeneously dense pa-renchyma, nine of 15 (60%) in breastswith minimal scattered fibroglandulardensity, and one of one (100%) in fattybreasts. Another focus of low-grade DCISwas initially considered probably benignat mammography and manifested as agrouping of four punctate calcifications
at stereotactic biopsy performed after in-tense progressive enhancement seen atMR imaging.
The management of 14 breasts waspredicated on DCIS (six high-grade, fourintermediate-grade, and four low-gradeDCIS). Of the 14 breasts, one (7.1%)showed diffuse foci of DCIS, one (7.1%)had multicentric foci, five (36%) hadmultifocal disease, and seven (50%) hadsolitary tumor foci. Of the six with mul-tifocal or multicentric disease, three(50%) were micropapillary DCIS.
Table 6 summarizes the extent of dis-ease according to imaging modality forthe 12 breasts with DCIS for which breastconservation was anticipated on the basisof clinical examination and mammo-
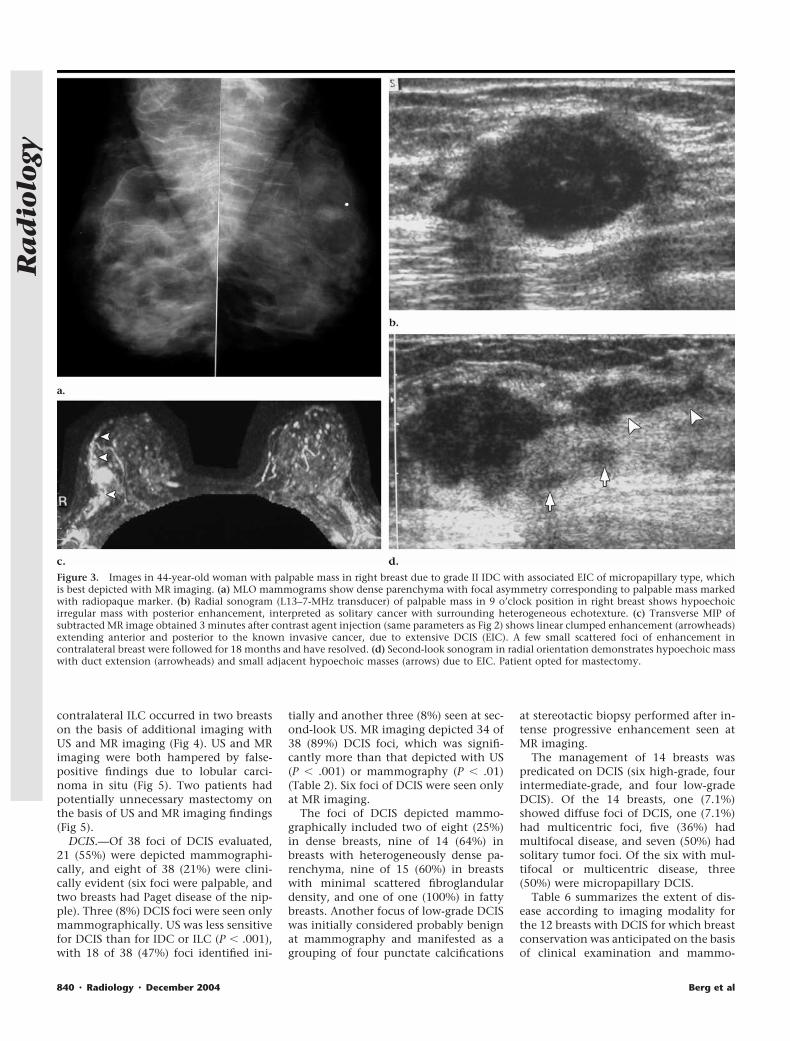
Figure 3. Images in 44-year-old woman with palpable mass in right breast due to grade II IDC with associated EIC of micropapillary type, whichis best depicted with MR imaging. (a) MLO mammograms show dense parenchyma with focal asymmetry corresponding to palpable mass markedwith radiopaque marker. (b) Radial sonogram (L13–7-MHz transducer) of palpable mass in 9 o’clock position in right breast shows hypoechoicirregular mass with posterior enhancement, interpreted as solitary cancer with surrounding heterogeneous echotexture. (c) Transverse MIP ofsubtracted MR image obtained 3 minutes after contrast agent injection (same parameters as Fig 2) shows linear clumped enhancement (arrowheads)extending anterior and posterior to the known invasive cancer, due to extensive DCIS (EIC). A few small scattered foci of enhancement incontralateral breast were followed for 18 months and have resolved. (d) Second-look sonogram in radial orientation demonstrates hypoechoic masswith duct extension (arrowheads) and small adjacent hypoechoic masses (arrows) due to EIC. Patient opted for mastectomy.
840 � Radiology � December 2004 Berg et al
Ra
dio
logy
graphic findings. Combined mammogra-phy and clinical examination depictedextent of DCIS well, but differences com-pared with other modalities alone or incombination were not significant, likelyas a result of the small number of cases.The extent of disease was overestimatedwith US in four of 12 (33%) breasts andwith MR imaging in six of 12 (50%). Onemastectomy was prompted by the find-ing of multiple scattered suspicious fociat both US and MR imaging, with twoadditional core biopsy results indicatingatypical ductal hyperplasia. This caseproved to be a solitary 25-mm mass ofintermediate-grade DCIS. Another fourof 12 (33%) breasts with DCIS for which
conservation was planned were negativeat US. Two breasts were appropriatelyconverted from planned lumpectomy tomastectomy on the basis of more exten-sive disease at US and MR imaging (Fig 6).
Contralateral Cancer
Of the 111 patients, 10 (9.0%) wereshown to have synchronous bilateral can-cer, with an 11th patient found to havecancer in the breast opposite a benign pre-senting lesion (Fig 1) at MR imaging only.Six of the 10 with synchronous contralat-eral cancers were suspected mammo-graphically, eight were suspected at US,and nine were suspected at MR imaging.
One 7-cm recurrent contralateral grade IIIIDC was only evident clinically 2 monthsafter study evaluation; findings from an-other US examination and mammogramremained negative at the time of diagnosis.Three of the contralateral cancers seen atUS were not seen at mammography (Fig 7).The presenting lesion proved to be IDC inseven patients, ILC in two, and DCIS inone with synchronous bilateral cancer.Histologic examination of the contralat-eral cancers revealed five IDCs, five ILCs(including diffuse ILC in one [Fig 4], mul-tifocal ILC in another, separate foci of ILCand DCIS in another, separate foci of ILCand IDC in another, and one case of mixedIDC and ILC), and one case of DCIS.
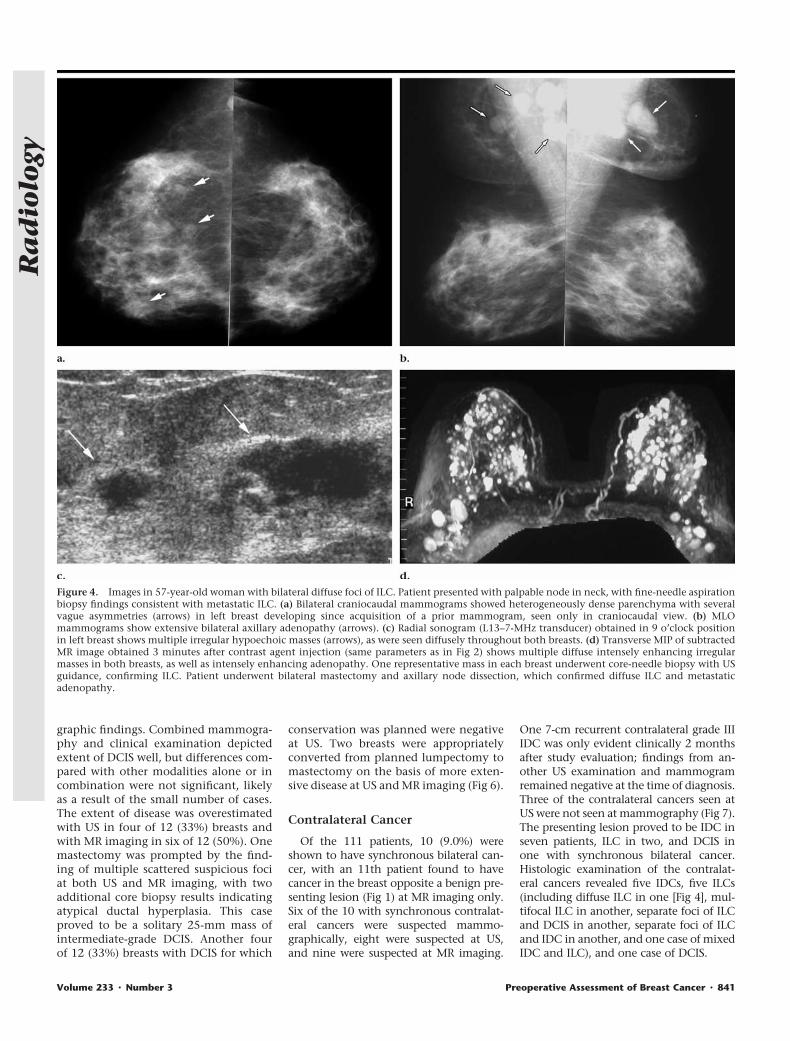
Figure 4. Images in 57-year-old woman with bilateral diffuse foci of ILC. Patient presented with palpable node in neck, with fine-needle aspirationbiopsy findings consistent with metastatic ILC. (a) Bilateral craniocaudal mammograms showed heterogeneously dense parenchyma with severalvague asymmetries (arrows) in left breast developing since acquisition of a prior mammogram, seen only in craniocaudal view. (b) MLOmammograms show extensive bilateral axillary adenopathy (arrows). (c) Radial sonogram (L13–7-MHz transducer) obtained in 9 o’clock positionin left breast shows multiple irregular hypoechoic masses (arrows), as were seen diffusely throughout both breasts. (d) Transverse MIP of subtractedMR image obtained 3 minutes after contrast agent injection (same parameters as in Fig 2) shows multiple diffuse intensely enhancing irregularmasses in both breasts, as well as intensely enhancing adenopathy. One representative mass in each breast underwent core-needle biopsy with USguidance, confirming ILC. Patient underwent bilateral mastectomy and axillary node dissection, which confirmed diffuse ILC and metastaticadenopathy.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 841
Ra
dio
logy
Additional Biopsies
An additional 145 biopsies were per-formed in tissue beyond the presentinglesion, of which 67 (46%) findingsproved malignant and 12 (8.3%) provedatypical (Table 2). Nine of the 67 (13%)additional cancers were palpable. Beyondthe presenting lesion, mammographicfindings prompted 43 biopsies, of which23 (53%) findings were malignant and six(14%) were atypical. Findings at USprompted 93 additional biopsies, ofwhich 40 (43%) findings were malignant
and 11 (12%) were atypical. There wereno cancers seen only at initial US (ie, allcancers were also found at clinical exam-ination, mammography, or MR imag-ing), though one ILC was seen only atsecond-look US. Findings at MR imaginghelped prompt 115 additional biopsies,of which 54 (47%) findings were malig-nant and 10 (8.7%) were atypical.
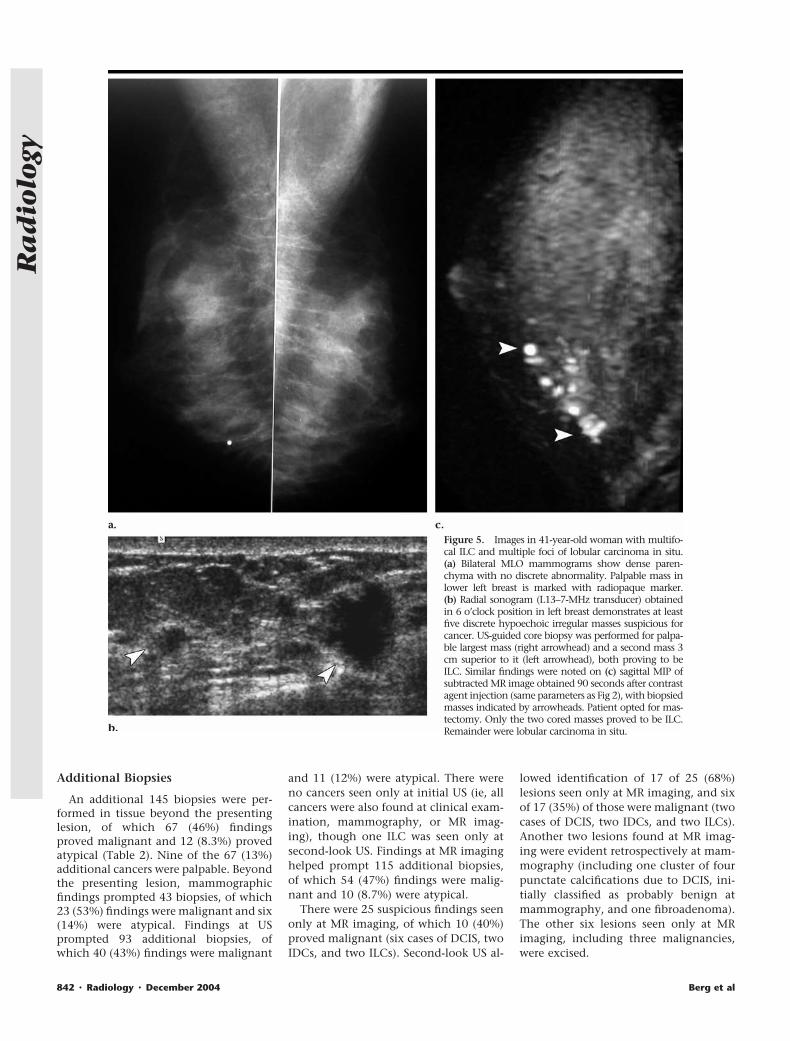
There were 25 suspicious findings seenonly at MR imaging, of which 10 (40%)proved malignant (six cases of DCIS, twoIDCs, and two ILCs). Second-look US al-
lowed identification of 17 of 25 (68%)lesions seen only at MR imaging, and sixof 17 (35%) of those were malignant (twocases of DCIS, two IDCs, and two ILCs).Another two lesions found at MR imag-ing were evident retrospectively at mam-mography (including one cluster of fourpunctate calcifications due to DCIS, ini-tially classified as probably benign atmammography, and one fibroadenoma).The other six lesions seen only at MRimaging, including three malignancies,were excised.
Figure 5. Images in 41-year-old woman with multifo-cal ILC and multiple foci of lobular carcinoma in situ.(a) Bilateral MLO mammograms show dense paren-chyma with no discrete abnormality. Palpable mass inlower left breast is marked with radiopaque marker.(b) Radial sonogram (L13–7-MHz transducer) obtainedin 6 o’clock position in left breast demonstrates at leastfive discrete hypoechoic irregular masses suspicious forcancer. US-guided core biopsy was performed for palpa-ble largest mass (right arrowhead) and a second mass 3cm superior to it (left arrowhead), both proving to beILC. Similar findings were noted on (c) sagittal MIP ofsubtracted MR image obtained 90 seconds after contrastagent injection (same parameters as Fig 2), with biopsiedmasses indicated by arrowheads. Patient opted for mas-tectomy. Only the two cored masses proved to be ILC.Remainder were lobular carcinoma in situ.
842 � Radiology � December 2004 Berg et al
Ra
dio
logy
False-Negative Findings
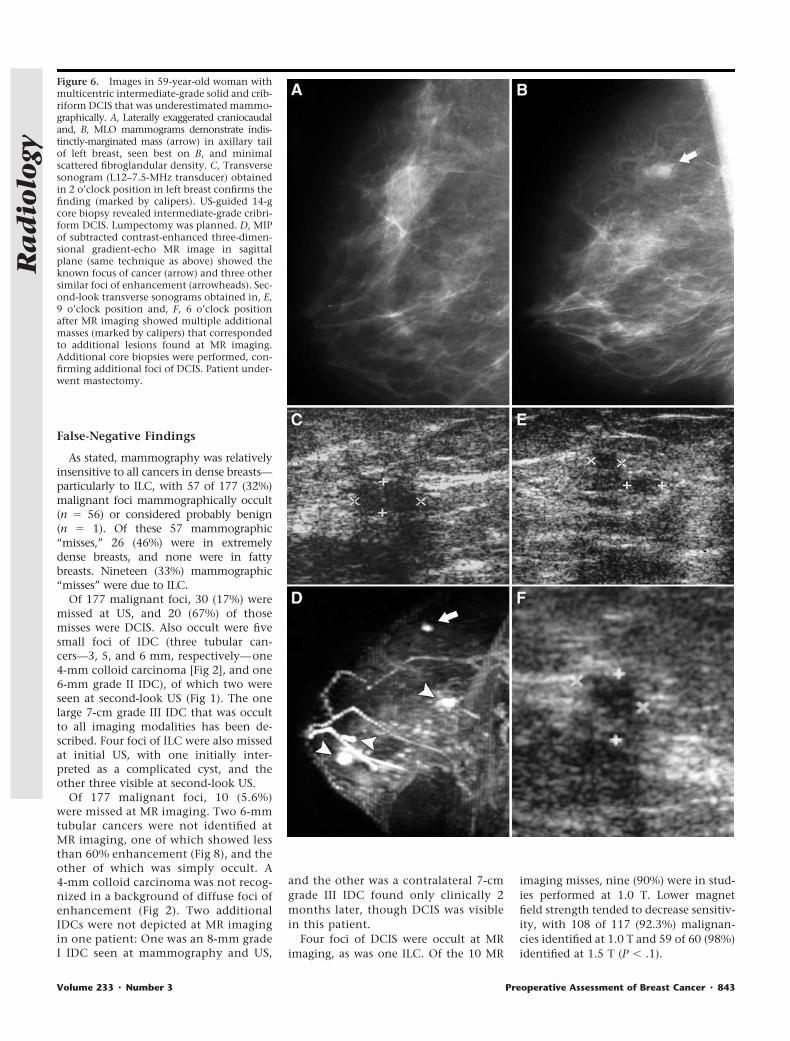
As stated, mammography was relativelyinsensitive to all cancers in dense breasts—particularly to ILC, with 57 of 177 (32%)malignant foci mammographically occult(n � 56) or considered probably benign(n � 1). Of these 57 mammographic“misses,” 26 (46%) were in extremelydense breasts, and none were in fattybreasts. Nineteen (33%) mammographic“misses” were due to ILC.
Of 177 malignant foci, 30 (17%) weremissed at US, and 20 (67%) of thosemisses were DCIS. Also occult were fivesmall foci of IDC (three tubular can-cers—3, 5, and 6 mm, respectively—one4-mm colloid carcinoma [Fig 2], and one6-mm grade II IDC), of which two wereseen at second-look US (Fig 1). The onelarge 7-cm grade III IDC that was occultto all imaging modalities has been de-scribed. Four foci of ILC were also missedat initial US, with one initially inter-preted as a complicated cyst, and theother three visible at second-look US.
Of 177 malignant foci, 10 (5.6%)were missed at MR imaging. Two 6-mmtubular cancers were not identified atMR imaging, one of which showed lessthan 60% enhancement (Fig 8), and theother of which was simply occult. A4-mm colloid carcinoma was not recog-nized in a background of diffuse foci ofenhancement (Fig 2). Two additionalIDCs were not depicted at MR imagingin one patient: One was an 8-mm gradeI IDC seen at mammography and US,
and the other was a contralateral 7-cmgrade III IDC found only clinically 2months later, though DCIS was visiblein this patient.
Four foci of DCIS were occult at MRimaging, as was one ILC. Of the 10 MR
imaging misses, nine (90%) were in stud-ies performed at 1.0 T. Lower magnetfield strength tended to decrease sensitiv-ity, with 108 of 117 (92.3%) malignan-cies identified at 1.0 T and 59 of 60 (98%)identified at 1.5 T (P � .1).
Figure 6. Images in 59-year-old woman withmulticentric intermediate-grade solid and crib-riform DCIS that was underestimated mammo-graphically. A, Laterally exaggerated craniocaudaland, B, MLO mammograms demonstrate indis-tinctly-marginated mass (arrow) in axillary tailof left breast, seen best on B, and minimalscattered fibroglandular density. C, Transversesonogram (L12–7.5-MHz transducer) obtainedin 2 o’clock position in left breast confirms thefinding (marked by calipers). US-guided 14-gcore biopsy revealed intermediate-grade cribri-form DCIS. Lumpectomy was planned. D, MIPof subtracted contrast-enhanced three-dimen-sional gradient-echo MR image in sagittalplane (same technique as above) showed theknown focus of cancer (arrow) and three othersimilar foci of enhancement (arrowheads). Sec-ond-look transverse sonograms obtained in, E,9 o’clock position and, F, 6 o’clock positionafter MR imaging showed multiple additionalmasses (marked by calipers) that correspondedto additional lesions found at MR imaging.Additional core biopsies were performed, con-firming additional foci of DCIS. Patient under-went mastectomy.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 843
Ra
dio
logy
Additional Short-Interval Follow-up
Additional probably benign foci of en-hancement in the contralateral breastwere common at MR imaging, seen in 54of 111 (49%) patients, with 25 of theparticipants requiring follow-up for find-ings seen only at MR imaging. Probablybenign findings were noted mammo-graphically in the contralateral breast in19 of 111 (17%) patients (seen only atmammography in four of these) and atUS in 21 of 111 (19%) patients (seen onlyat US in three of these). After all threeimaging modalities were performed, 64of 111 (58%) patients had probably be-nign findings in the contralateral breast.Adequate follow-up was performed for 55of 64 (86%) of these: Six of these breastsunderwent biopsy (or removal) with be-nign results, and 49 breasts had lesions
that were stable, decreasing, or gone. In-deed, three patients opted for contralat-eral mastectomy on the basis of probablybenign findings at MR imaging, whichproved benign.
With a median of 24 months (range,13–60 months) of follow-up when avail-able for patients in this series, there havebeen no local recurrences. However, fiveof the 111 (4.5%) patients died of theirdisease, and another five (4.5%) had dis-tant metastases.
DISCUSSION
Detection of Cancer
Detection of breast cancer is the pri-mary goal of breast imaging. Mammog-raphy has proved effective as a screeningtest for the early detection of breast can-
cer. In dense and heterogeneously densebreasts, mammographic sensitivity is de-creased, with as few as 30%–48% of can-cers depicted in extremely dense breasts(4,5). Indeed, in this series, where 50% ofcancers were palpable, mammographicsensitivity was 45% (21 of 47 foci) inextremely dense breasts and 70% (45 of64 foci) in heterogeneously dense breastsand was lower for ILC than for IDC acrossall grades of breast density. Only one of19 (5%) invasive cancers depicted mam-mographically in dense breasts was non-palpable, which further suggests thatscreening mammography is of limitedvalue in dense breasts.
In this series, cancer was nearly twiceas prevalent in dense or heterogeneouslydense breasts than in nondense breasts(111 of 177 [62.7%] malignant foci vs 66
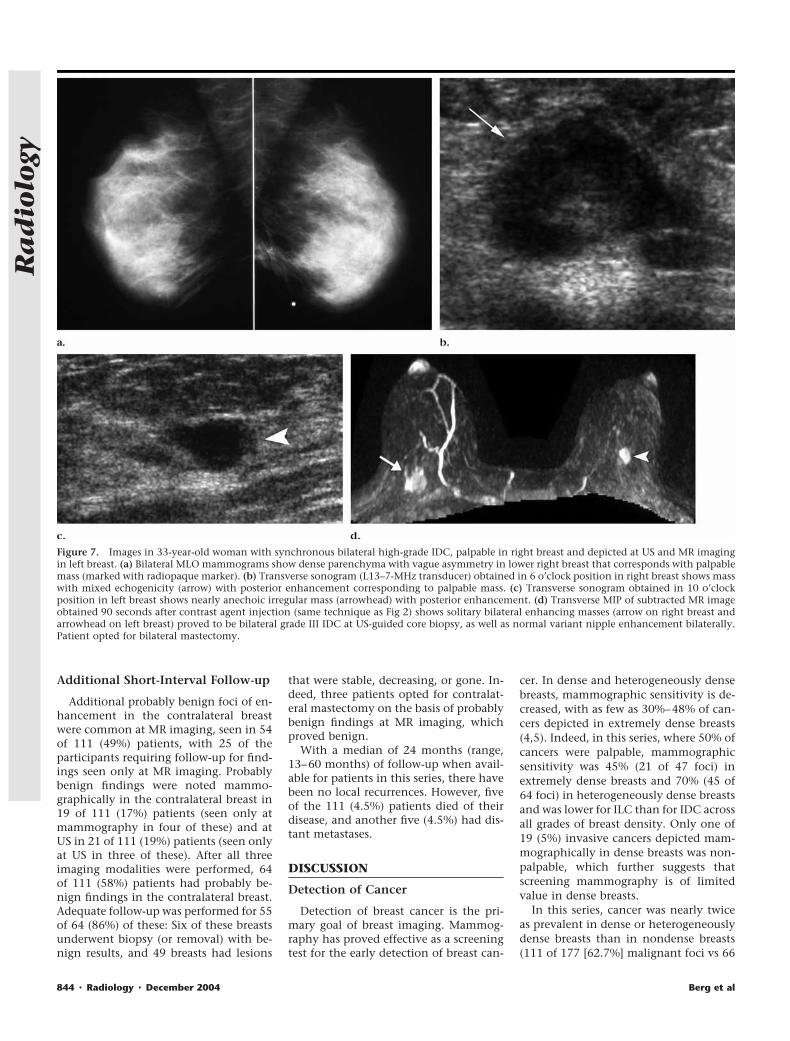
Figure 7. Images in 33-year-old woman with synchronous bilateral high-grade IDC, palpable in right breast and depicted at US and MR imagingin left breast. (a) Bilateral MLO mammograms show dense parenchyma with vague asymmetry in lower right breast that corresponds with palpablemass (marked with radiopaque marker). (b) Transverse sonogram (L13–7-MHz transducer) obtained in 6 o’clock position in right breast shows masswith mixed echogenicity (arrow) with posterior enhancement corresponding to palpable mass. (c) Transverse sonogram obtained in 10 o’clockposition in left breast shows nearly anechoic irregular mass (arrowhead) with posterior enhancement. (d) Transverse MIP of subtracted MR imageobtained 90 seconds after contrast agent injection (same technique as Fig 2) shows solitary bilateral enhancing masses (arrow on right breast andarrowhead on left breast) proved to be bilateral grade III IDC at US-guided core biopsy, as well as normal variant nipple enhancement bilaterally.Patient opted for bilateral mastectomy.
844 � Radiology � December 2004 Berg et al
Ra
dio
logy
of 177 [37.3%] malignant foci, P � .001).Increased breast density has been shownto increase the risk of breast cancer from2.2- to fivefold when breasts with densestgrades are compared with fatty breasts(26,27). The combination of decreasedmammographic sensitivity and increasedprevalence of cancer in denser breasts hasprompted interest in the investigation ofsupplemental screening with US (28) oreven MR imaging.
Stomper et al (29) reported that thefrequency of dense breasts decreases withincreasing age, with 62% of women intheir 30s having more than 50% breastdensity compared with 27% of women intheir 60s. Several studies (3,30) haveshown decreased mammographic sensi-tivity in younger women, even after cor-recting for breast density.
Mammographically occult tumor mayhelp explain the observations that (a)
women younger than 40 years with pos-itive margins are at increased risk of hav-ing residual tumor in their breasts com-pared with older women (31) and that (b)women younger than 40 years experi-ence a much higher rate of local recur-rence after radiation therapy than doolder women, even with a boost to thelumpectomy site (32). We did not findyounger age to be an independent pre-dictor of decreased mammographic sen-sitivity or increased risk of multifocalityper se.
ILC presents particular dilemmas inthe detection and evaluation of diseaseextent. ILC tends to be mammographi-cally subtle if it is seen at all. In one series(33), more than one of three mammo-
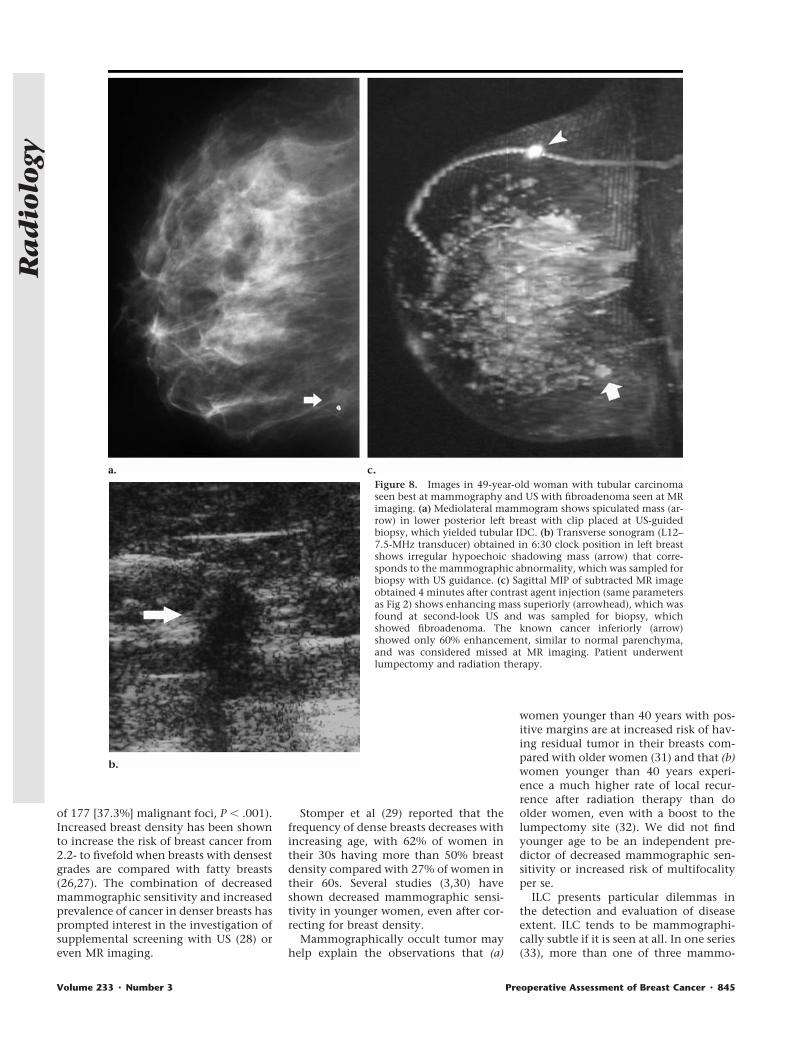
Figure 8. Images in 49-year-old woman with tubular carcinomaseen best at mammography and US with fibroadenoma seen at MRimaging. (a) Mediolateral mammogram shows spiculated mass (ar-row) in lower posterior left breast with clip placed at US-guidedbiopsy, which yielded tubular IDC. (b) Transverse sonogram (L12–7.5-MHz transducer) obtained in 6:30 clock position in left breastshows irregular hypoechoic shadowing mass (arrow) that corre-sponds to the mammographic abnormality, which was sampled forbiopsy with US guidance. (c) Sagittal MIP of subtracted MR imageobtained 4 minutes after contrast agent injection (same parametersas Fig 2) shows enhancing mass superiorly (arrowhead), which wasfound at second-look US and was sampled for biopsy, whichshowed fibroadenoma. The known cancer inferiorly (arrow)showed only 60% enhancement, similar to normal parenchyma,and was considered missed at MR imaging. Patient underwentlumpectomy and radiation therapy.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 845
Ra
dio
logy

graphically depicted ILCs was seen as avague asymmetry, poorly defined opac-ity, or area of possible architectural dis-tortion. US is beneficial in the identifica-tion of ILC. In the series of Butler et al(34), 81 of 208 (39%) ILCs were mammo-graphically subtle or occult, and 71 ofthose 81 (88%) were depicted at US. Inthis series, 19 of 29 (66%) ILCs weremammographically occult (comparedwith 21 of 110 [19%] IDCs [P � .001]),with 15 of these 19 (79%) seen at US.
In this series, the combination ofmammography, clinical examination,and US depicted 165 of 177 (93.2%) ma-lignant foci, with the remainder seenonly at MR imaging. The sensitivity ofcombined mammography and US was96% each in the screening series of Kolbet al (5) and in the series of 480 symp-tomatic patients reported by Houssami etal (35). Moy et al (36) reported that 97%of palpable cancers were depicted with acombination of US and mammography.
MR imaging alone depicted 167 of 177(94.4%) malignant foci. MR imaging sen-sitivity at 1.0 T tended to be lower thanthat at 1.5 T. Heywang-Kobrunner et al(37) found equivalent sensitivity at thetwo field strengths, with improved spec-ificity at 1.0 T. We found no difference inthe rate of false-positive findings as afunction of field strength.
Of the 17 malignancies seen with onlyone modality, five (29%) were seen onlymammographically, 10 (59%) only at MRimaging, and one (6%) only at second-look US. One (6%) was only clinicallyevident. This suggests that additional im-aging should be considered a supplementto mammography, not a replacement. USprovided no benefit over and above com-bined MR imaging, mammography, andclinical examination in the identificationof tumor foci, though US was used toguide biopsy whenever possible.
In this series, 47% of DCIS foci wereidentified at US. In the series of Moon et al(10), 56 of 76 (74%) DCIS foci were identi-fied. In both the study of Moon et al (10)and the present series, US was performedwithout being blinded to mammographicfindings, and its independent performancemay be substantially less. When seenmammographically, 73%–98% of DCIS ismanifest as microcalcifications (38–40).Despite spatial compounding, speckle ar-tifact present in breast tissue hampersidentification of microcalcifications, asdoes resolution.
Yang and Tse (41) reported that US wasnot helpful in the characterization ofmorphology or extent of calcifications insymptomatic DCIS. Soo et al (42) de-
scribe that in their experience with US oflesions manifested as suspicious mam-mographic microcalcifications, only 26of 111 (23%) lesions could be identifiedwith US. Importantly, lesions seen at USwere more likely to be malignant (69% vs21%) and invasive (72% vs 28%), withunderestimation of an invasive compo-nent less likely when biopsy was per-formed sonographically than stereotacti-cally (42). On the basis of our experiencewith false-positive and false-negativefindings, we would not encourage the useof US in the evaluation of the extent ofDCIS per se but would reserve its use forbiopsy guidance when possible.
As with US, MR imaging proved prob-lematic in cases of DCIS in this series andwas more likely to result in unnecessarybiopsy or surgery than to improve treat-ment planning. MR imaging has proveduseful in the evaluation of extent of DCISin patients with more than focally posi-tive margins of excision (43,44), thoughthat was not the focus of the present se-ries.
Extent of Disease
As summarized in the study of Libermanet al (8), across multiple series totaling1280 breasts with detailed histopathologicevaluation after a preoperative diagnosis ofunifocal cancer, 619 (48%) were found tohave additional tumor foci unsuspected atmammography. In this series, among 96breasts in which conservation or no sur-gery was anticipated after mammographyand clinical examination, 30 (31%) hadadditional mammographically occult tu-mor foci. Supplemental US more accu-rately depicted extent, which necessitatedwider excision in 17 of 96 (18%) breasts forwhich conservation was anticipated, corre-sponding to 17 of 30 (57%) breasts withmammographically or clinically occult tu-mor (though four remained underesti-mated). In an earlier nonoverlapping series(9), we found that US depicted additionaltumor, which altered the surgical approachin 15% of breasts.
Supplemental MR imaging depictedadditional tumor that necessitated widerexcision in 29 of 96 (30%) breasts forwhich conservation was anticipated, cor-responding to 29 of 30 (97%) breasts withmammographically or clinically occulttumor. Liberman et al (8) reported addi-tional tumor depiction with MR imagingin 27% of ipsilateral breasts. Orel et al (7)reported additional tumor depiction withMR imaging in 34% of patients.
As stated earlier, the vast majority ofadditional tumor foci are found in the
same quadrant as the index lesion. In thisseries, in 40 of 46 (87%) breasts with ad-ditional foci of tumor, the foci were mul-tifocal in the immediate 4 cm of tissuesurrounding the index lesion; 92% ofbreasts with additional tumor were mul-tifocal in the series of Liberman et al (8).In the present series, 11 of 46 (24%)breasts with additional tumor were bothmultifocal and multicentric, with diffusetumor foci involving multiple quadrants.In only six of 121 (5%) breasts were thereisolated multicentric foci of tumor. Thus,the vast majority of additional tumor fociare in the same quadrant and within 4cm of the index cancer: At a minimum,when performing US in a patient knownor suspected to have cancer, thoroughevaluation of at least that quadrant of thebreast is recommended.
Evaluation of the contralateral breastdeserves discussion. On the basis of clin-ical or mammographic evaluation orboth, 2%–3% of patients are found tohave synchronous bilateral cancer (45).Invasive lobular histologic findings (46)and age younger than 55 years (46,47)increase the risk of contralateral breastcancer. In the present series, 9% of pa-tients had synchronous bilateral cancer,with 3% of patients identified as havingunsuspected contralateral cancer at USand MR imaging that was occult at mam-mography and clinical examination.Similar rates of 4%–6% of unsuspectedcontralateral breast cancer have beenseen in other series (10,11,48–50) on thebasis of supplemental imaging beyondmammography.
We found a benefit of MR imagingover and above combined mammogra-phy, clinical examination, and US in 12of 96 (12%) breasts for which conserva-tion (or no surgery) had been planned,similar to the 7% (seven of 104) addi-tional benefit of MR imaging in the seriesof Hlawatsch et al (12). In five of the 12(42%) breasts with an additional MR im-aging benefit, MR imaging depicted anextensive intraductal component thatwas otherwise occult; presumably, thesepatients would have had positive mar-gins at lumpectomy. Ideally, patientswith an EIC could be selected to undergopreoperative MR imaging. Mai et al (51)found that EIC could be predicted on thebasis of core biopsy findings. If at leastthree cores had low-grade DCIS or at leasttwo cores had high-grade DCIS, 20 of 23(87%) patients with IDC had EIC at exci-sion (51). Importantly, nine of 15 (60%)lumpectomies in the group with core bi-opsy findings suggestive of EIC (accord-ing to the criteria of Mai et al) had posi-
846 � Radiology � December 2004 Berg et al
Ra
dio
logy

tive margins or margins less than 1 mm(51). Further validation of this approachis needed.
In the patient with newly diagnosedILC, MR imaging was particularly helpfulin the assessment of disease extent. Ro-denko et al (52) showed correlation withpathologic extent of disease in 17 of 20(85%) MR evaluations, compared withonly 32% correlation with mammo-graphic studies. In the series of Weinsteinet al (53), MR imaging changed clinicalmanagement in 50% of patients withILC. In this series, US was as accurate asMR imaging in the evaluation of the ex-tent of ILC. Liberman et al (8) found thatadditional sites of cancer were more com-mon with lobular than ductal histologicfindings and in women with a family his-tory of breast cancer. We did not evaluatethe latter. We found that eight of 15(53%) breasts with ILC had multiple tu-mor foci compared with 31 of 92 (34%)with IDC, but the difference was not sig-nificant. Contralateral breast cancer ismore common with lobular histologicfindings than IDC (46,54). Indeed, two ofour 15 patients with index ILC had un-suspected contralateral ILC found only atMR imaging and US, and five of 10 (50%)patients with bilateral cancer had ILC inat least one breast, though ILC repre-sented only 29 of 177 (16%) of all cancersin this series.
The 25%–36% rate of local recurrencein the absence of radiation or chemother-apy (55,56) parallels the frequency ofmultifocal and multicentric tumor foundonly at US and/or MR imaging evalua-tion. This suggests the potential for theseadditional tumor foci to be clinically rel-evant and may also suggest that com-plete excision directed by multimodalitypretreatment imaging may decrease theneed for radiation therapy, though suchstudies have not yet been performed.
Much of the additional tumor that isoccult at mammography would be iden-tified at surgery. Tumor size can be un-derestimated, but this is often evident atthe time of surgery or would certainlyyield positive margins. With an EIC, asstated earlier, positive margins are com-mon, and repeat excision or mastectomywould be performed. With IDC, wefound that 16 of 92 (17%) breasts hadtumor that would have been missed atmammography and clinical examinationif clear margins had been achieved. Inanother five of 15 (33%) breasts with ILC,foci were missed at mammography andclinical examination in the present se-ries. IDC represents 85%–90% of all inva-sive carcinoma, and ILC represents 10%–
15% of invasive breast cancer (57). Fromthis, we would expect residual tumor inapproximately 19% of patients with in-vasive carcinoma ([0.9 � 17%] � [0.1 �33%] � 19%) if management proceededonly on the basis of mammography andclinical examination with standard surgi-cal management (ie, repeat excision ormastectomy if margins are positive). Onthe basis of the observations of Broet et al(46), chemotherapy may “sanitize” ap-proximately half of tumor foci. Thus, wewould expect that if all residual tumorwere of clinical importance, the recur-rence rate would be 9%–10% after stan-dard treatments. Indeed, the risk of recur-rence after lumpectomy and radiation isgenerally 1%–2% per year for the first 5years, averaging 5%–13% at 5 years(32,56,58). The prognosis of women withlocal recurrence within the first 5 years isworse than that with late recurrence,with 61% subsequent 5-year survival ver-sus 84% in one series (59). Presumably,the identification of multiple tumor focipreoperatively and the complete excisionof them will decrease the rate of localrecurrence, but this has not been shown.
Decreasing the theoretical risk of localrecurrence comes at the price of in-creased risk of unnecessary wider exci-sion or mastectomy. For breasts with can-cer in this series, 67 of 121 (55%)underwent mastectomy, with only 23 of67 (34%) of these recommended on thebasis of mammography and clinical ex-amination alone. Fifteen mastectomieswere deemed potentially excessive. Infive of 15 (33%) of those breasts, atypicallesions had been sampled for biopsy per-cutaneously and required excision in ad-dition to the known cancer, which inthese patients proved problematic in thatpoor cosmetic results were then antici-pated if lumpectomy and separate surgi-cal biopsy (or biopsies) were performed.Three patients opted for bilateral mastec-tomy because of findings consideredprobably benign in the contralateralbreast at MR imaging (with all provingbenign), and another three patientsopted for mastectomy (for tumor thatcould have been removed by means oflumpectomy) because their cancer wasseen only at MR imaging (n � 2) or atboth US and MR imaging (n � 1) andthey lacked confidence in standard imag-ing follow-up. It is imperative that his-topathologic proof of disease extent beobtained preoperatively whenever possi-ble to assist in proper surgical planning,though atypical results and multiplicityof additional suspicious findings (Fig 5)can make this task problematic.
It should be recognized that lack of aUS correlate for an abnormality at MRimaging should not deter biopsy of a sus-picious finding. In the experience of LaTrenta et al (60), lesions found at second-look US were more likely malignant, but14% of lesions seen only at MR imagingwere malignant and required MR imag-ing–guided biopsy. In the present series,25 suspicious findings were evident atMR only, and 10 (40%) of these provedmalignant. Integration of breast MR im-aging interpretation with other breastimaging is critical. Of the 25 suspiciousfindings at MR imaging, 17 (68%) wereidentified at second-look US and weresampled for biopsy, including six of 10(60%) malignancies identified only withMR imaging.
Another malignancy (DCIS) first seenat MR imaging was evident at mammog-raphy retrospectively as a group of fourpunctate microcalcifications, as was a be-nign fibroadenoma. Of six suspiciousfindings seen only at MR imaging evenafter second-look US and review of mam-mograms, three (50%) proved malignantin the present series. Capability of MRimaging–guided core biopsy is critical tothe widespread use of breast MR imaging.Commercially available methods are indevelopment (61) and are to be encour-aged.
In addition to the risk of potentiallyunnecessary wide excision or mastec-tomy, additional imaging follow-up wasrequired in 48% of patients because ofincidental findings at MR imaging.Brown et al (62) reported that 29% of MRimaging studies showed incidental en-hancing lesions. Teifke et al (63) foundincidental enhancing lesions in 16% ofpatients. The criteria for classification ofenhancing lesions found at MR imagingas benign or probably benign are not wellestablished. When contrast material con-tinues to accumulate within the lesionover time (ie, progressive or persistentkinetics), this tends to correlate with be-nignancy. Kuhl et al (16) found that nineof 146 (6%) lesions with progressive orinitially progressive then delayed plateauenhancement were malignant, and thisrepresented 9% of malignant lesions intheir series.
Detailed morphologic analysis is notreadily performed for very small lesions(smaller than 5 mm) when bilateralbreast MR imaging is performed becauseof the requirement for imaging bothbreasts within the first 1–2 minutes aftercontrast material injection and resultinglimited resolution. Experimental contrastagents with prolonged intravascular
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 847
Ra
dio
logy

phase may facilitate detailed morpho-logic analysis and biopsy of lesions seenonly at MR imaging (64). Importantly,Liberman et al (65) found that nine of 89(10%) women with lesions consideredprobably benign at MR imaging provedto have malignancy at a median fol-low-up of 11 months, though three ofnine (33%) of the malignancies were atother sites. Prognosis was not likely ad-versely affected by short-interval fol-low-up in that series, as five of nine(56%) cancers were DCIS, and the me-dian size of the IDCs was 6 mm (thoughtwo had micrometastases) (65).
One of the limitations of our study wasthat US was performed without beingblinded to mammographic or clinicalfindings, and MR imaging was performedwithout being blinded to mammo-graphic, clinical, or US findings. This ar-tificially inflates the performance of sup-plemental imaging, since findings thatmight otherwise be dismissed will be tar-geted specifically. Importantly, US wasperformed independent of MR imagingresults, and we found no supplementalindependent benefit of US after mam-mography and MR imaging, except toguide biopsy.
Full assessment of the local extent ofbreast cancer also includes the axilla. Wedid not specifically evaluate the axillaprospectively with US or MR imaging inthese patients, though enhancement oflymph nodes in the axilla and even(rarely) internal mammary chain wasseen at MR imaging. We have found thatwhen a node is identified at MR imagingthat enhances more intensely or is visu-ally strikingly larger than adjacent nodesor has lost its fatty hilum, that subse-quent US identification and US-guidedfine-needle aspiration biopsy (66) can fa-cilitate surgical planning. If a nodal me-tastasis is confirmed, the patient will typ-ically proceed straight to full axillarydissection rather than initial sentinelnode biopsy and second axillary surgeryif the sentinel node is positive. Refine-ment of criteria and further validation ofthis approach are warranted.
In summary, US and MR imaging wereeach more sensitive than mammographyfor invasive cancer, particularly in hetero-geneously dense or extremely dense breasts.Supplemental imaging beyond mammog-raphy was problematic for most cases ofDCIS and of no value in fatty breasts. Of 96breasts in which conservation or no sur-gery was planned after mammography andclinical examination, 30 (31%) were ulti-mately found to have additional foci ofcancer that would change the surgical ap-
proach. After combined mammographyand clinical examination, US depictedadditional tumor foci that changed thesurgical approach in 17 of 96 (18%)breasts, and MR imaging depicted addi-tional tumor foci that changed the surgi-cal approach in 29 of 96 (30%) breasts.After combined mammography, clinicalexamination, and US, MR imaging de-picted additional cancer in 12 of 96(12%) breasts for which conservation wasanticipated (with five of 12 [42%] ofthese due to depiction of an EIC); addi-tion of MR imaging carried a substantialrisk of false-positive findings, with extentof disease overestimated in 20 of 96(21%) breasts (compared with three of 96[3.1%] overestimated at mammographyand clinical examination alone and 12 of96 [12%] overestimated after mammog-raphy, clinical examination, and US).
Combined mammography, clinical ex-amination, and MR imaging were moresensitive to malignancy than any othertest alone or in combination, depictingall 177 malignancies. The use of com-bined US and mammography was nearlyas effective as MR imaging, except whenan EIC was present, and was equivalentto MR imaging in the assessment of ILC.While useful in guiding biopsy of lesionsseen at MR imaging, US had no role inthe detection of disease after MR imagingin this series. Bilateral whole-breast US orcontrast-enhanced MR imaging was ofvalue in the depiction of mammographi-cally and clinically occult synchronouscontralateral cancer in three (3%) pa-tients.
References1. Burhenne HJ, Burhenne LW, Goldberg F,
et al. Interval breast cancers in the Screen-ing Mammography Program of BritishColumbia: analysis and classification. AJRAm J Roentgenol 1994; 162:1067–1071;discussion, 1072–1075.
2. Robertson CL. A private breast imagingpractice: medical audit of 25,788 screen-ing and 1,077 diagnostic examinations.Radiology 1993; 187:75–79.
3. Kerlikowske K, Grady D, Barclay J, SicklesEA, Ernster V. Effect of age, breast density,and family history on the sensitivity offirst screening mammography. JAMA1996; 276:33–38.
4. Mandelson MT, Oestreicher N, Porter PL,et al. Breast density as a predictor of mam-mographic detection: comparison of in-terval- and screen-detected cancers. J NatlCancer Inst 2000; 92:1081–1087.
5. Kolb TM, Lichy J, Newhouse JH. Compar-ison of the performance of screeningmammography, physical examination,and breast US and evaluation of factorsthat influence them: an analysis of 27,825patient evaluations. Radiology 2002; 225:165–175.
6. Harms SE, Flamig DP, Hesley KL, et al. MR
imaging of the breast with rotating deliv-ery of excitation off resonance: clinicalexperience with pathologic correlation.Radiology 1993; 187:493–501.
7. Orel SG, Schnall MD, Powell CM, et al.Staging of suspected breast cancer: effectof MR imaging and MR-guided biopsy.Radiology 1995; 196:115–122.
8. Liberman L, Morris EA, Dershaw DD,Abramson AF, Tan LK. MR imaging of theipsilateral breast in women with percuta-neously proven breast cancer. AJR Am JRoentgenol 2003; 180:901–910.
9. Berg WA, Gilbreath PL. Multicentric andmultifocal cancer: whole-breast US in pre-operative evaluation. Radiology 2000;214:59–66.
10. Moon WK, Noh DY, Im JG. Multifocal,multicentric, and contralateral breastcancers: bilateral whole-breast US in thepreoperative evaluation of patients. Radi-ology 2002; 224:569–576.
11. Fischer U, Kopka L, Grabbe E. Breast car-cinoma: effect of preoperative contrast-enhanced MR imaging on the therapeuticapproach. Radiology 1999; 213:881–888.
12. Hlawatsch A, Teifke A, Schmidt M,Thelen M. Preoperative assessment ofbreast cancer: sonography versus MR im-aging. AJR Am J Roentgenol 2002; 179:1493–1501.
13. Fischer U, Kopka L, Brinck U, Korabiow-ska M, Schauer A, Grabbe E. Prognosticvalue of contrast-enhanced MR mam-mography in patients with breast cancer.Eur Radiol 1997; 7:1002–1005.
14. American College of Radiology. Breastimaging reporting and data system. 3rded. Reston, Va: American College of Ra-diology, 1998.
15. Nunes LW, Schnall MD, Orel SG, et al.Correlation of lesion appearance and his-tologic findings for the nodes of a breastMR imaging interpretation model. Radio-Graphics 1999; 19:79–92.
16. Kuhl CK, Mielcareck P, Klaschik S, et al.Dynamic breast MR imaging: are signalintensity time course data useful for dif-ferential diagnosis of enhancing lesions?Radiology 1999; 211:101–110.
17. Berg WA, Jaeger B, Campassi C, Kumar D.Predictive value of specimen radiographyfor core needle biopsy of noncalcifiedbreast masses. AJR Am J Roentgenol 1998;171:1671–1678.
18. Kopans DB. Clip placement during sono-graphically guided breast biopsy. AJRAm J Roentgenol 2001; 176:1076–1077.
19. Egan RL. Multicentric breast carcinomas:clinical-radiographic-pathologic whole or-gan studies and 10-year survival. Cancer1982; 49:1123–1130.
20. Ellis IO, Pinder SE, Lee AH, Elston CW. Acritical appraisal of existing classificationsystems of epithelial hyperplasia and insitu neoplasia of the breast with propos-als for future methods of categorization:where are we going? Semin Diagn Pathol1999; 16:202–208.
21. Schnitt SJ, Connolly JL, Harris JR, Hell-man S, Cohen RB. Pathologic predictorsof early local recurrence in stage I and IIbreast cancer treated by primary radia-tion therapy. Cancer 1984; 53:1049–1057.
22. Connolly JL, Boyages J, Nixon AJ, et al.Predictors of breast recurrence after con-servative surgery and radiation therapy
848 � Radiology � December 2004 Berg et al
Ra
dio
logy
for invasive breast cancer. Mod Pathol1998; 11:134–139.
23. Ikeda DM, Baker DR, Daniel BL. Magneticresonance imaging of breast cancer: clin-ical indications and breast MRI reportingsystem. J Magn Reson Imaging 2000; 12:975–983.
24. Mendelson EB, Berg WA, Merritt CR. To-ward a standardized breast ultrasound lex-icon, BI-RADS: ultrasound. Semin Roentge-nol 2001; 36:217–225.
25. Fisher ER, Sass R, Fisher B. Pathologicfindings from the National Surgical Adju-vant Project for Breast Cancers (protocolno. 4). X. Discriminants for tenth yeartreatment failure. Cancer 1984; 53(suppl3):712–723.
26. Nagao Y, Kawaguchi Y, Sugiyama Y, SajiS, Kashiki Y. Relationship between mam-mographic density and the risk of breastcancer in Japanese women: a case-controlstudy. Breast Cancer 2003; 10:228–233.
27. Ursin G, Ma H, Wu AH, et al. Mammo-graphic density and breast cancer in threeethnic groups. Cancer Epidemiol Biomar-kers Prev 2003; 12:332–338.
28. Berg WA. Rationale for a trial of screeningbreast ultrasound: American College ofRadiology Imaging Network (ACRIN)6666. AJR Am J Roentgenol 2003; 180:1225–1228.
29. Stomper PC, D’Souza DJ, DiNitto PA,Arredondo MA. Analysis of parenchymaldensity on mammograms in 1353women 25–79 years old. AJR Am J Roent-genol 1996; 167:1261–1265.
30. Carney PA, Miglioretti DL, Yankaskas BC,et al. Individual and combined effects ofage, breast density, and hormone replace-ment therapy use on the accuracy ofscreening mammography. Ann InternMed 2003; 138:168–175.
31. Wazer DE, Schmidt-Ullrich RK, RuthazerR, et al. The influence of age and exten-sive intraductal component histologyupon breast lumpectomy margin assess-ment as a predictor of residual tumor. IntJ Radiat Oncol Biol Phys 1999; 45:885–891.
32. Bartelink H, Horiot JC, Poortmans P. Re-currence rates after treatment of breastcancer with standard radiotherapy withor without additional radiation. N EnglJ Med 2001; 345:1378–1387.
33. Hilleren DJ, Andersson IT, Lindholm K,Linnell FS. Invasive lobular carcinoma:mammographic findings in a 10-year ex-perience. Radiology 1991; 178:149–154.
34. Butler RS, Venta LA, Wiley EL, Ellis RL,Dempsey PJ, Rubin E. Sonographic eval-uation of infiltrating lobular carcinoma.AJR Am J Roentgenol 1999; 172:325–330.
35. Houssami N, Irwig L, Simpson JM,McKessar M, Blome S, Noakes J. SydneyBreast Imaging Accuracy Study: compar-ative sensitivity and specificity of mam-mography and sonography in youngwomen with symptoms. AJR Am J Roent-genol 2003; 180:935–940.
36. Moy L, Slanetz PJ, Moore R, et al. Speci-ficity of mammography and US in theevaluation of a palpable abnormality: ret-rospective review. Radiology 2002; 225:176–181.
37. Heywang-Kobrunner SH, Bick U, BradleyWG Jr, et al. International investigationof breast MRI: results of a multicentrestudy (11 sites) concerning diagnostic pa-rameters for contrast-enhanced MRIbased on 519 histopathologically corre-lated lesions. Eur Radiol 2001; 11:531–546.
38. Ikeda DM, Andersson I. Ductal carcinomain situ: atypical mammographic appear-ances. Radiology 1989; 172:661–666.
39. Dershaw DD, Abramson A, Kinne DW.Ductal carcinoma in situ: mammographicfindings and clinical implications. Radiol-ogy 1989; 170:411–415.
40. Stomper PC, Margolin FR. Ductal carci-noma in situ: the mammographer’s per-spective. AJR Am J Roentgenol 1994; 162:585–591.
41. Yang WT, Tse GM. Sonographic, mam-mographic, and histopathologic correla-tion of symptomatic ductal carcinoma insitu. AJR Am J Roentgenol 2004; 182:101–110.
42. Soo MS, Baker JA, Rosen EL. Sonographicdetection and sonographically guided bi-opsy of breast microcalcifications. AJRAm J Roentgenol 2003; 180:941–948.
43. Soderstrom CE, Harms SE, Farrell RS Jr,Pruneda JM, Flamig DP. Detection withMR imaging of residual tumor in thebreast soon after surgery. AJR Am J Roent-genol 1997; 168:485–488.
44. Orel SG, Reynolds C, Schnall MD, SolinLJ, Fraker DL, Sullivan DC. Breast carci-noma: MR imaging before re-excisionalbiopsy. Radiology 1997; 205:429–436.
45. Hungness ES, Safa M, Shaughnessy EA, etal. Bilateral synchronous breast cancer:mode of detection and comparison ofhistologic features between the 2 breasts.Surgery 2000; 128:702–707.
46. Broet P, de la Rochefordiere A, Scholl SM,et al. Contralateral breast cancer: annualincidence and risk parameters. J Clin On-col 1995; 13:1578–1583.
47. Healey EA, Cook EF, Orav EJ, Schnitt SJ,Connolly JL, Harris JR. Contralateralbreast cancer: clinical characteristics andimpact on prognosis. J Clin Oncol 1993;11:1545–1552.
48. Rieber A, Merkle E, Bohm W, Brambs HJ,Tomczak R. MRI of histologically con-firmed mammary carcinoma: clinical rel-evance of diagnostic procedures for de-tection of multifocal or contralateralsecondary carcinoma. J Comput AssistTomogr 1997; 21:773–779.
49. Liberman L, Morris EA, Kim CM, et al. MRimaging findings in the contralateralbreast of women with recently diagnosedbreast cancer. AJR Am J Roentgenol 2003;180:333–341.
50. Lee SG, Orel SG, Woo IJ, et al. MR imag-ing screening of the contralateral breastin patients with newly diagnosed breastcancer: preliminary results. Radiology2003; 226:773–778.
51. Mai KT, Yazdi HM, Ford JC, Matzinger FR.Predictive value of extent and grade ofductal carcinoma in situ in radiologicallyguided core biopsy for the status of mar-gins in lumpectomy specimens. Eur J SurgOncol 2000; 26:646–651.
52. Rodenko GN, Harms SE, Pruneda JM, etal. MR imaging in the management be-fore surgery of lobular carcinoma of thebreast: correlation with pathology. AJRAm J Roentgenol 1996; 167:1415–1419.
53. Weinstein SP, Orel SG, Heller R, et al. MRimaging of the breast in patients withinvasive lobular carcinoma. AJR Am JRoentgenol 2001; 176:399–406.
54. Fisher ER, Fisher B, Sass R, Wickerham L.Pathologic findings from the NationalSurgical Adjuvant Breast Project (ProtocolNo. 4). XI. Bilateral breast cancer. Cancer1984; 54:3002–3011.
55. Dawson PJ. What is new in our under-standing of multifocal breast cancer.Pathol Res Pract 1993; 189:111–116.
56. Fisher ER, Anderson S, Tan-Chiu E, FisherB, Eaton L, Wolmark N. Fifteen-year prog-nostic discriminants for invasive breastcarcinoma. Cancer 2001; 91:1679–1687.
57. Li CI, Anderson BO, Daling JR, Moe RE.Trends in incidence rates of invasive lob-ular and ductal breast carcinoma. JAMA2003; 289:1421–1424.
58. Fisher B, Dignam J, Wolmark N, et al.Lumpectomy and radiation therapy forthe treatment of intraductal breast can-cer: findings from National Surgical Ad-juvant Breast and Bowel Project B-17.J Clin Oncol 1998; 16:441–452.
59. Kurtz JM, Spitalier JM, Amalric R, et al.The prognostic significance of late localrecurrence after breast-conserving ther-apy. Int J Radiat Oncol Biol Phys 1990;18:87–93.
60. La Trenta LR, Menell JH, Morris EA, Der-shaw DD, Abramson AF, Liberman L. His-topathologic significance of sonographicidentification of MRI-detected breast le-sions (abstr). Radiology 2001; 221(P):232.
61. Liberman L, Morris EA, Dershaw DD,Thornton CM, Van Zee KJ, Tan LK. FastMRI-guided vacuum-assisted breast bi-opsy: initial experience. AJR Am J Roentge-nol 2003; 181:1283–1293.
62. Brown J, Smith RC, Lee CH. Incidentalenhancing lesions found on MR imagingof the breast. AJR Am J Roentgenol 2001;176:1249–1254.
63. Teifke A, Lehr HA, Vomweg TW, Hla-watsch A, Thelen M. Outcome analysisand rational management of enhancinglesions incidentally detected on contrast-enhanced MRI of the breast. AJR Am JRoentgenol 2003; 181:655–662.
64. Kuhl CK, Simon B, Sondermann E, Leut-ner CC, Shamsi K, Schild HH. Ultra-highresolution breast MR imaging using intra-vascular contrast agent (Gadomer17) (ab-str). Radiology 2002; 225(P):652.
65. Liberman L, Morris EA, Benton CL,Abramson AF, Dershaw DD. Probably be-nign lesions at breast magnetic resonanceimaging: preliminary experience in high-risk women. Cancer 2003; 98:377–388.
66. Krishnamurthy S, Sneige N, Bedi DG, etal. Role of ultrasound-guided fine-needleaspiration of indeterminate and suspi-cious axillary lymph nodes in the initialstaging of breast carcinoma. Cancer 2002;95:982–988.
Volume 233 � Number 3 Preoperative Assessment of Breast Cancer � 849
Ra
dio
logy
Related Documents











