Diagnosis, Intervention, Evaluation, and Documentation

Diagnosis, intervention, evaluation ncp
May 24, 2015
Diagnosis, intervention, evaluation ncp
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diagnosis, Intervention, Evaluation, and Documentation

Relationship Between
Patient/Client/Group & Dietetics
Professional
-
Nutrition Diagnosis Identify and label problem Determine cause/contributing risk
factors Cluster signs and symptoms/
defining characteristics
Nutrition Assessment Obtain/collect timely and
appropriate data Analyze/interpret with
evidence - based standards
Identify risk factors Use appropriate tools
and methods Involve
interdisciplinary collaboration
Screening & Referral System
Outcomes Management Sys tem
Monitor the success of the Nutrition Care Process implementation
Evaluate the impact with aggregate data Identify and analyze causes of less than
optimal performance and outcomes Refine the use of the Nutrition Care
Process
ADA NUTRITION CARE PROCESS AND MODEL
Document
Nutrition Monitoring and Evaluation Monitor progress Measure outcome indicators Evaluate outcomes Document
Nutrition Intervention Plan nutrition intervention
Formulate goals and determine a plan of action
Implement the nutrition intervention Care is delivered and actions
are carried out Document
Document

Nutrition Assessment Leads to Nutrition Diagnosis
• Nutrition AssessmentNutrition Assessment• Nutrition DiagnosisNutrition Diagnosis• Nutrition Intervention Nutrition Intervention • Nutrition Monitoring and EvaluationNutrition Monitoring and Evaluation

Nutrition vs Medical Dx
Medical Dx Nutrition Diagnosis
Diabetes Excessive CHO intake related to evening visits to Coldstone Creamery as evidenced by diet hx and high hs blood glucose
Trauma and closed head injury
Increased energy expenditure related to multiple trauma as evidenced by results of indirect calorimetry
Liver failure Altered gastrointestinal function related to cirrhosis of the liver as evidenced by steatorrhea and growth failure

Nutritional vs Medical Dx
Medical Dx Nutrition Diagnosis
Obesity Excessive energy intake related to lack of access to healthy food choices (restaurant eating) as evidenced by diet history and BMI of 35.
Dependence mechanical ventilation
Excessive energy intake related to high volume PN as evidenced by RQ >1
Anorexia nervosa
Inappropriate food choices related to history of anorexia nervosa and self-limiting behavior as evidenced by diet history and weight loss of 5 lb

PES Statement
• Problem: nutrition diagnosis labelProblem: nutrition diagnosis label• Etiology: the focus of the interventionEtiology: the focus of the intervention• Signs and symptoms: change when nutrition Signs and symptoms: change when nutrition
problems are successfully treated; the focus problems are successfully treated; the focus of monitoring and evaluationof monitoring and evaluation

Problem (Diagnostic Label)
Falls into three general domains:Falls into three general domains:• Intake (NI)Intake (NI)
• Excessive or Inadequate intake compared Excessive or Inadequate intake compared to requirements to requirements
• Clinical (NC)Clinical (NC)• Medical or physical conditions that are Medical or physical conditions that are
outside normaloutside normal• Behavioral/environmental (NB)Behavioral/environmental (NB)
• Knowledge, attitudes, beliefs, physical Knowledge, attitudes, beliefs, physical environment, access to food, food safetyenvironment, access to food, food safety

Etiology• Etiology (Cause/Contributing Factors)Etiology (Cause/Contributing Factors)
• Related factors that contribute to problemRelated factors that contribute to problem• Identifies cause of the problemIdentifies cause of the problem• Helps determine whether nutrition Helps determine whether nutrition
intervention will improve problemintervention will improve problem• Linked to problem by words “related to” Linked to problem by words “related to”
(RT)(RT)• Note: etiology may not always be clearNote: etiology may not always be clear

Etiology
• Etiology (Cause/Contributing Factors)Etiology (Cause/Contributing Factors)• Excessive energy intake (problem) “related Excessive energy intake (problem) “related
to” regular consumption of large portions of to” regular consumption of large portions of high-fat meals (etiology)…high-fat meals (etiology)…
• Swallowing difficulty (problem) RT recent Swallowing difficulty (problem) RT recent stroke (etiology)…stroke (etiology)…
• Involuntary wt gain RT decrease in Involuntary wt gain RT decrease in exercise…exercise…

Diagnostic Labels Can Be Problems or Etiologies• Inadequate energy intake (NI-1.4) related to food-Inadequate energy intake (NI-1.4) related to food-
nutrition knowledge deficit (NB-1.1)nutrition knowledge deficit (NB-1.1)• Food-nutrition knowledge deficit (NB-1.1) related Food-nutrition knowledge deficit (NB-1.1) related
to lack of previous nutrition educationto lack of previous nutrition education• Involuntary weight loss (NC-3.2) related to Involuntary weight loss (NC-3.2) related to
inadequate energy intake (NI-1.4)inadequate energy intake (NI-1.4)• Inadequate oral food-beverage intake (NI-2.1) Inadequate oral food-beverage intake (NI-2.1)
related to swallowing difficulty (NC-1.1)related to swallowing difficulty (NC-1.1)

Signs and Symptoms
• Signs/Symptoms (Defining characteristics)Signs/Symptoms (Defining characteristics)• Evidence that problem existsEvidence that problem exists• Linked to etiology by words “as Linked to etiology by words “as
evidenced by”evidenced by”• Evaluation and monitoring of effectiveness Evaluation and monitoring of effectiveness
of intervention is done by reviewing signs of intervention is done by reviewing signs and symptomsand symptoms

Nutrition Dx with S/S• Excessive energy intake (NI-1.5) (P) Excessive energy intake (NI-1.5) (P) • ““related to” regular consumption of large related to” regular consumption of large
portions of high-fat meals (E) portions of high-fat meals (E) • ““as evidenced by” diet history & 12 lb wt as evidenced by” diet history & 12 lb wt
gain over last 18 mo (Signs)gain over last 18 mo (Signs)

Nutrition Assessment Identifies Etiology and S/S• Problem: excessive energy intakeProblem: excessive energy intake• Etiology: reviewing the diet history, we learn Etiology: reviewing the diet history, we learn
thatthat• Patient eats in fast food restaurants 2x dayPatient eats in fast food restaurants 2x day• Patient supersizes portions because it’s a Patient supersizes portions because it’s a
bargainbargain• Patient has only 15 minutes for lunchPatient has only 15 minutes for lunch

PES Statement
Excessive energy intake P
Related to eating frequently in fast food restaurants
E
As evidenced by BMI of 30 and diet history
S

Etiology Guides Intervention!
• The clinician determines what the The clinician determines what the intervention is by looking at the root cause intervention is by looking at the root cause of the nutrition problem. of the nutrition problem.
• If the cause of excessive energy intake is If the cause of excessive energy intake is eating frequently in fast food restaurants, eating frequently in fast food restaurants, how would you intervene?how would you intervene?

Signs and Symptoms Direct Intervention and Evaluation
Intervention/ Eval
P Excessive energy intake
E RT eating frequently in fast food restaurants
Intervention: Counsel patient about best choices in fast food restaurants (C-2.4)
S As evidenced by BMI and diet history
Eval: Recheck weight (S-1.1.4) and diet history (BE-2.1.1.) at next visit

PES Statements
• Excessive fat intake (NI-5.6.2) related to high Excessive fat intake (NI-5.6.2) related to high intake of fried foods and bakery goods as intake of fried foods and bakery goods as evidenced by diet history and hyperlipidemiaevidenced by diet history and hyperlipidemia
• Excessive energy intake (NI-1.5) related to high Excessive energy intake (NI-1.5) related to high intake of fried foods and snack items as evidenced intake of fried foods and snack items as evidenced by diet history and BMIby diet history and BMI
• Food/nutrition related knowledge deficit (NB-1.1)Food/nutrition related knowledge deficit (NB-1.1) related to lack of education on cholesterol related to lack of education on cholesterol lowering diet as evidenced by history and patient lowering diet as evidenced by history and patient self-reportself-report

Nutrition Diagnosis Statement Should Be
• Clear, conciseClear, concise• SpecificSpecific• Related to one problemRelated to one problem• Accurate – related to one etiologyAccurate – related to one etiology• Based on reliable, accurate assessment Based on reliable, accurate assessment
datadata

Evaluating Your PES Statement
• There are no right or wrong PES statementsThere are no right or wrong PES statements• But some are better than othersBut some are better than others

Evaluating Your PES Statement
• Can the RD resolve or improve the nutrition Can the RD resolve or improve the nutrition diagnosis? diagnosis?
• Can your intervention address the etiology Can your intervention address the etiology and thus resolve it or improve the problem?and thus resolve it or improve the problem?
• Or can your intervention address the signs Or can your intervention address the signs and symptoms?and symptoms?
Evaluating Your PES Statement
• Ex: Inadequate energy intake related to Ex: Inadequate energy intake related to decreased taste perception as evidenced by decreased taste perception as evidenced by diet history, medical dx and weight loss of diet history, medical dx and weight loss of 10 lb. during cancer tx10 lb. during cancer tx
• Cannot treat the etiology (decreased taste Cannot treat the etiology (decreased taste perception) but can treat S&S by perception) but can treat S&S by recommending foods with stronger flavorsrecommending foods with stronger flavors

Evaluating Your PES Statement• Altered nutrition-related labs related to GI Altered nutrition-related labs related to GI
bleed as evidenced by medical hx and bleed as evidenced by medical hx and decreased hgb/hct in medical recorddecreased hgb/hct in medical record
• Labs likely won’t improve until GI bleed Labs likely won’t improve until GI bleed is addressed; the etiology is not a is addressed; the etiology is not a nutritional deficitnutritional deficit
• CAN address inadequate intake of iron, CAN address inadequate intake of iron, copper, B12, protein, etc. copper, B12, protein, etc.

Evaluating Your PES Statement
• When all things are equal and there is a choice When all things are equal and there is a choice between two nutrition diagnoses from different between two nutrition diagnoses from different domains, consider the Intake domain diagnosis as domains, consider the Intake domain diagnosis as the one more specific to the role of the RDthe one more specific to the role of the RD
• Instead of Altered nutrition-related labs related to Instead of Altered nutrition-related labs related to GI bleed as evidenced by medical hx and GI bleed as evidenced by medical hx and decreased hgb/hct in medical record decreased hgb/hct in medical record
• Consider Inadequate intake of iron (NI-5.10.1) Consider Inadequate intake of iron (NI-5.10.1) related to increased needs due to GI bleed as related to increased needs due to GI bleed as evidenced by medical history, blood count, diet evidenced by medical history, blood count, diet history, and serum ferritinhistory, and serum ferritin

Evaluating Your PES Statement
• Will measuring the signs and symptoms tell Will measuring the signs and symptoms tell you if the problem is resolved or improved? you if the problem is resolved or improved?
• Ex: If nutrition dx is excessive energy Ex: If nutrition dx is excessive energy intake, can do another diet history at next intake, can do another diet history at next visit and see if intake has changed; can also visit and see if intake has changed; can also check weightcheck weight

NCP Example: Long Term Care
• 85 y.o. resident of LTC facility has lost 85 y.o. resident of LTC facility has lost >10% weight in the last 6 months>10% weight in the last 6 months
• Medical workup negativeMedical workup negative• Oral supplement is ordered but patient Oral supplement is ordered but patient
continues to lose weightcontinues to lose weight• Nutrition professional is consulted for Nutrition professional is consulted for
enteral feeding recommendationsenteral feeding recommendations

NCP Example: LTC
• On assessment, it is found that patient’s On assessment, it is found that patient’s teeth no longer fit and she cannot chew teeth no longer fit and she cannot chew regular meats and vegetables; patient is regular meats and vegetables; patient is storing oral supplement in drawer as she storing oral supplement in drawer as she worries about the costworries about the cost

Write a PES statement for this patient!

NCP Example: LTC
• Diagnosis: Inadequate energy intake (NI-Diagnosis: Inadequate energy intake (NI-1.4) related to poorly fitting dentures and 1.4) related to poorly fitting dentures and hoarding of oral supplement as evidenced hoarding of oral supplement as evidenced by observation and pt interviewby observation and pt interview

Etiology Guides Intervention
• Intervention: Nutrition professional orders Intervention: Nutrition professional orders dental consult (RC-1.3) to reline dentures dental consult (RC-1.3) to reline dentures and chopped diet (ND-1.2); puts resident on and chopped diet (ND-1.2); puts resident on Medpass supplement (ND-3.1.1)Medpass supplement (ND-3.1.1)

Diagnoses Apply to All Settings
Long term care
Inadequate energy intake (NI-1.4) related to patient refusal of pureed diet as evidenced by intake records, pt self-report and 8% weight loss/3 months
Long term care
Inadequate fiber intake (NI-5.8.5) related to patient avoidance of fruits and vegetables as evidenced by chronic constipation and diet history
Ambulatory Care
Not ready for diet/lifestyle change (NB-1.4) related to social/environmental issues as evidenced by pt verbalization and continued weight gain

ADA’s Nutrition Care Process Steps
• Nutrition AssessmentNutrition Assessment• Nutrition DiagnosisNutrition Diagnosis• Nutrition Intervention Nutrition Intervention • Nutrition Monitoring and EvaluationNutrition Monitoring and Evaluation

Nutrition Intervention
• Should be targeted at etiologyShould be targeted at etiology• If not etiology, then signs and symptomsIf not etiology, then signs and symptoms

Nutrition Interventions
Four categories of nutrition interventions:Four categories of nutrition interventions:• Food and/or nutrient delivery (ND)Food and/or nutrient delivery (ND)• Nutrition education (E)Nutrition education (E)• Nutrition counseling (C)Nutrition counseling (C)• Coordination of nutrition care (RC)Coordination of nutrition care (RC)
Food and/or Nutrient Delivery
• Meals and snacks (ND-1)Meals and snacks (ND-1)• Enteral/parenteral nutrition (ND-2)Enteral/parenteral nutrition (ND-2)• Medical food supplements (ND-3.1)Medical food supplements (ND-3.1)• Vitamin and mineral supplement (ND-3.2)Vitamin and mineral supplement (ND-3.2)• Bioactive substance supplement (ND-3.3)Bioactive substance supplement (ND-3.3)• Feeding assistance (ND-4)Feeding assistance (ND-4)• Feeding environment (ND-5)Feeding environment (ND-5)• Nutrition-related medication management (ND-6)Nutrition-related medication management (ND-6)

Nutrition Education (E)
• Initial/brief nutrition education (E-1)Initial/brief nutrition education (E-1)• E.g. survival skills on dischargeE.g. survival skills on discharge
• Comprehensive nutrition education (E-2)Comprehensive nutrition education (E-2)• PurposePurpose• Recommended modificationsRecommended modifications• Result interpretationResult interpretation• OtherOther
Note: Education is appropriate for food and nutrition-related knowledge deficit. If the client knows the content, more education probably won’t help

Nutrition Counseling (C)
• Theory or approachTheory or approach• StrategiesStrategies• PhasePhase

Nutrition Counseling: Theory or ApproachThe theories or models used to design and The theories or models used to design and
implement an intervention; provide a research-implement an intervention; provide a research-based rationale for designing and tailoring based rationale for designing and tailoring nutrition interventionsnutrition interventions
• Cognitive-behavioral therapy (C-1.2)Cognitive-behavioral therapy (C-1.2)• Health belief model (C-1.3)Health belief model (C-1.3)• Social learning theory (C-1.4)Social learning theory (C-1.4)• Transtheoretical Model/Stages Transtheoretical Model/Stages of Change (C-1.5)of Change (C-1.5)• Other (C-1.6) Other (C-1.6)

Nutrition Counseling: Strategies*
• Motivational Motivational interviewing (C-2.1)interviewing (C-2.1)
• Goal setting (C-2.2)Goal setting (C-2.2)• Self-monitoring (C-2.3) Self-monitoring (C-2.3) • Problem solving (C-2.4)Problem solving (C-2.4)• Social support (C-2.5)Social support (C-2.5)• Stress management (C-Stress management (C-
2.6)2.6)• Stimulus control (C-2.7)Stimulus control (C-2.7)
• Cognitive Cognitive restructuring (C-2.8)restructuring (C-2.8)
• Relapse prevention Relapse prevention (C-2.9)(C-2.9)
• Rewards/contingency Rewards/contingency mgt (C-2.10)mgt (C-2.10)
• OtherOther
*Selectively applied evidence-based method or plan of action designed to achieve a particular goal

Coordination of Care (RC)
• Coordination of other care during nutrition care Coordination of other care during nutrition care (RC-1)(RC-1)• Team meetingTeam meeting• Referral to RDReferral to RD• Collaboration with other providersCollaboration with other providers• Referral to community agencies/programsReferral to community agencies/programs
• Discharge and transfer of nutrition care to new Discharge and transfer of nutrition care to new setting/provider (RC-2)setting/provider (RC-2)• CollaborationCollaboration• Referral to community agencies/programsReferral to community agencies/programs

ADA’s Nutrition Care Process Steps
• Nutrition AssessmentNutrition Assessment• Nutrition DiagnosisNutrition Diagnosis• Nutrition InterventionNutrition Intervention • Nutrition Monitoring and EvaluationNutrition Monitoring and Evaluation

Nutrition Monitoring and Evaluation
• Monitor progress and determine if goals are Monitor progress and determine if goals are metmet
• Identifies patient/client outcomes relevant Identifies patient/client outcomes relevant to the nutrition diagnosis and intervention to the nutrition diagnosis and intervention plans and goalsplans and goals
• Measure and compare to client’s previous Measure and compare to client’s previous status, nutrition goals, or reference status, nutrition goals, or reference standardsstandards

Nutrition Outcomes – 4 Categories• Nutrition-Related Behavioral and Environmental Nutrition-Related Behavioral and Environmental
Outcomes (BE)—Nutrition-related knowledge, Outcomes (BE)—Nutrition-related knowledge, behavior, access, and ability that impact food and behavior, access, and ability that impact food and nutrient intakenutrient intake
• Food and Nutrient Intake Outcomes (FI)—Food Food and Nutrient Intake Outcomes (FI)—Food and/or nutrient intake from all sourcesand/or nutrient intake from all sources
• Nutrition-Related Physical Signs and Symptom Nutrition-Related Physical Signs and Symptom Outcomes (S)—Anthropomorphic, biochemical, Outcomes (S)—Anthropomorphic, biochemical, and physical exam parametersand physical exam parameters
• Nutrition-Related Patient/client centered Nutrition-Related Patient/client centered Outcomes (PC)—perception of patient/client’s Outcomes (PC)—perception of patient/client’s nutrition intervention and its impactnutrition intervention and its impact

Nutrition-Related Behavioral and Environmental Outcomes (BE)• Knowledge/beliefs (1)Knowledge/beliefs (1)• Behavior (2)Behavior (2)• Access (3)Access (3)• Physical activity and function (4)Physical activity and function (4)

Behavior-Environmental Outcomes Domain: Beliefs and Attitudes (BE-1.1)
Definition: beliefs/attitudes about and/or readiness to Definition: beliefs/attitudes about and/or readiness to change food, nutrition, or nutrition-related change food, nutrition, or nutrition-related behaviorsbehaviors
Potential indicators (BE-1.1)Potential indicators (BE-1.1)• Readiness to changeReadiness to change• Perceived consequences of changePerceived consequences of change• Perceived costs versus benefits of changePerceived costs versus benefits of change• Perceived riskPerceived risk• Outcome expectancyOutcome expectancy• Conflict with patient/family value systemConflict with patient/family value system• Self efficacySelf efficacy

Beliefs and Attitudes (BE-1.1)
Measurement methods or data sourcesMeasurement methods or data sources• Patient self-report, client/patient Patient self-report, client/patient
assessment questionnaire or interviewassessment questionnaire or interview
Typically used to monitor and evaluate Typically used to monitor and evaluate change in the following domains of change in the following domains of nutrition intervention:nutrition intervention:• Nutrition education, nutrition counselingNutrition education, nutrition counseling

Beliefs and Attitudes (BE-1.1)
Typically used to monitor and evaluate change in the Typically used to monitor and evaluate change in the following nutrition diagnosesfollowing nutrition diagnoses• Harmful beliefs/attitudes about food- or Harmful beliefs/attitudes about food- or
nutrition-related topicsnutrition-related topics• Not ready for diet/lifestyle changeNot ready for diet/lifestyle change• Inability to manage self-careInability to manage self-care• Excess or inadequate oral food/beverage, Excess or inadequate oral food/beverage,
energy, macronutrient, micronutrient, or energy, macronutrient, micronutrient, or bioactive substance intakebioactive substance intake
• Imbalance of nutrientsImbalance of nutrients• Inappropriate fat foodsInappropriate fat foods

Beliefs and Attitudes (BE-1.1)
Typically used to monitor/evaluate change in the Typically used to monitor/evaluate change in the following nutrition diagnoses (cont)following nutrition diagnoses (cont)• Inappropriate intake of amino acidsInappropriate intake of amino acids• UnderweightUnderweight• Overweight/obesityOverweight/obesity• Disordered eating patternDisordered eating pattern• Physical inactivityPhysical inactivity• Excess exerciseExcess exercise

Behavior-Environmental Outcomes Domain: Food and Nutrition Knowledge (BE-1.2)
Definition: Level of knowledge about food, Definition: Level of knowledge about food, nutrition and health, or nutrition-related nutrition and health, or nutrition-related information and guidelines relevant to information and guidelines relevant to patient/client needspatient/client needs

Food and Nutrition Knowledge (BE-1.2) Potential Indicators
• Level of knowledge (e.g. none, limited, minimal, Level of knowledge (e.g. none, limited, minimal, substantial, and extensivesubstantial, and extensive
• Areas of knowledge:Areas of knowledge:• Food/nutrient requirementsFood/nutrient requirements• Physiological functionsPhysiological functions• Disease/conditionDisease/condition• Nutrition recommendationsNutrition recommendations• Food productsFood products• Consequences of food behaviorConsequences of food behavior• Food label understanding/knowledgeFood label understanding/knowledge• Self-management parametersSelf-management parameters

Food and Nutrition Knowledge (BE-1.2)
Measurement methods or data sourcesMeasurement methods or data sources• Pre and post-tests administered orally, on paper, or Pre and post-tests administered orally, on paper, or
by computerby computer• Scenario discussionsScenario discussions• Patient/client restate key informationPatient/client restate key information• Review of food recordsReview of food records• Practical demonstration/testPractical demonstration/testTypically used to monitor and evaluate change in the Typically used to monitor and evaluate change in the
following domains of nutrition intervention:following domains of nutrition intervention:• Nutrition education, nutrition counselingNutrition education, nutrition counseling

Food and Nutrition Knowledge (BE-1.2)
Typically used to monitor and evaluate Typically used to monitor and evaluate change in the following nutrition diagnoses:change in the following nutrition diagnoses:
• Food- and nutrition-related knowledge Food- and nutrition-related knowledge deficitdeficit
• Limited adherence to nutrition-related Limited adherence to nutrition-related recommendationsrecommendations
• Intake domainIntake domain

Ability to Plan Meals/Snacks (BE-2.1)
• Definition: Patient/client ability related to Definition: Patient/client ability related to planning healthy meals and snacks, which planning healthy meals and snacks, which are compatible with dietary goalsare compatible with dietary goals
• Potential indicator: Meal/snack planning Potential indicator: Meal/snack planning ability (e.g. may include ability to use ability (e.g. may include ability to use planning tools, plan a menu, create/tailor a planning tools, plan a menu, create/tailor a meal plan, create/use a shopping listmeal plan, create/use a shopping list

Ability to Plan Meals/Snacks (BE-2.1)
• Measurement methods/data sources: food Measurement methods/data sources: food intake records, self-report or caregiver intake records, self-report or caregiver report, 24-hour recall, menu review, report, 24-hour recall, menu review, targeted questionnairetargeted questionnaire
• Typically used to measure outcomes for Typically used to measure outcomes for these domains of nutrition interventions:these domains of nutrition interventions:• Nutrition educationNutrition education• Nutrition counselingNutrition counseling

Ability to Plan Meals/Snacks (BE-2.1)
Typically used to monitor and evaluate change in the Typically used to monitor and evaluate change in the following nutrition diagnoses:following nutrition diagnoses:
• Excessive or inadequate oral food/beverage intakeExcessive or inadequate oral food/beverage intake• UnderweightUnderweight• Overweight/obesityOverweight/obesity• Limited adherence to nutrition-related Limited adherence to nutrition-related
recommendationsrecommendations• Inability or lack of desire to manage self-careInability or lack of desire to manage self-care

Other BE Nutrition Outcomes
Behavior (2)Behavior (2)• Ability to select healthful Ability to select healthful
food/mealsfood/meals• Ability to prepare Ability to prepare
food/mealsfood/meals• AdherenceAdherence• Goal settingGoal setting• Portion controlPortion control• Self-care managementSelf-care management• Self-monitoringSelf-monitoring• Social supportSocial support• Stimulus controlStimulus control
Access (3)Access (3)• Access to foodAccess to foodPhysical activity and Physical activity and
function (4) function (4) • Breastfeeding successBreastfeeding success• Nutrition-related ADLs Nutrition-related ADLs
and IADLsand IADLs• Physical activityPhysical activity

Other Outcomes
Food and Nutrient Intake Food and Nutrient Intake (FI)(FI)
• Energy intake (1)Energy intake (1)• Food and Beverage (2)Food and Beverage (2)• Enteral and parenteral (3)Enteral and parenteral (3)• Bioactive substances (4)Bioactive substances (4)• Macronutrients (5)Macronutrients (5)• Micronutrients (6)Micronutrients (6)
Physical Signs/Symptoms Physical Signs/Symptoms (S)(S)
• Anthropometric (1)Anthropometric (1)• Biochemical and medical Biochemical and medical
tests (2)tests (2)
• Physical examination (3)Physical examination (3)
Patient-Client Centered Patient-Client Centered Outcomes (PC)Outcomes (PC)

Outcomes Based Practice• Underlays Performance Improvement Underlays Performance Improvement
and Managementand Management• Meets accreditation standards (TJC, Meets accreditation standards (TJC,
American Diabetes Association)American Diabetes Association)• Supports value of nutrition providers in Supports value of nutrition providers in
health delivery systemhealth delivery system• Enhances reputation/ties with medical Enhances reputation/ties with medical
staff and other colleaguesstaff and other colleagues

NCP Example: Acute Care
• Mr. D. is a 73 y.o. white male admitted with L leg Mr. D. is a 73 y.o. white male admitted with L leg fx after fall. He lives with his son and daughter in fx after fall. He lives with his son and daughter in law. Per his son, Mr. D’s appetite has been poor law. Per his son, Mr. D’s appetite has been poor the past 6 months, his dentures are very loose and the past 6 months, his dentures are very loose and he refuses to wear them. He also refuses pureed he refuses to wear them. He also refuses pureed foods. Ht: 6 ft.; weight 133 lb; usual weight 1 year foods. Ht: 6 ft.; weight 133 lb; usual weight 1 year ago 165 lb. Meds: milk of magnesia, Pepcid, Di-ago 165 lb. Meds: milk of magnesia, Pepcid, Di-Gel. No significant medical hx save progressive Gel. No significant medical hx save progressive dementia;labs after hydration serum alb 2.4 g/dL; dementia;labs after hydration serum alb 2.4 g/dL; Hgb 10.6 g/dL; HCT 35.3%; BUN, Cr, liver fxn Hgb 10.6 g/dL; HCT 35.3%; BUN, Cr, liver fxn tests WNLtests WNL

Write a PES statement for this patient!

NCP Example: Acute CareNutrition DiagnosisNutrition Diagnosis• Inadequate energy intake (NI-1.4) related to Inadequate energy intake (NI-1.4) related to
dementia and poor appetite as evidenced by dementia and poor appetite as evidenced by diet history and recent unintentional weight diet history and recent unintentional weight lossloss
• Chewing difficulty (NC-1.2) related to ill-Chewing difficulty (NC-1.2) related to ill-fitting dentures as evidenced by diet history fitting dentures as evidenced by diet history
• Increased energy expenditure (NI-1.2) Increased energy expenditure (NI-1.2) related to long bone fx as evidenced by related to long bone fx as evidenced by medical historymedical history

How would you intervene with this patient?

Intervention
• Dental consult to have dentures relined for better Dental consult to have dentures relined for better fit (RC - coordination of care)fit (RC - coordination of care)
• Try oral supplements to determine patient Try oral supplements to determine patient preference and evaluate acceptance (ND-3.1.1 preference and evaluate acceptance (ND-3.1.1 food-nutrient delivery)food-nutrient delivery)
• Consider move to assisted living (RC - Consider move to assisted living (RC - coordination of care)coordination of care)
• Educate patient’s family on nutrient-dense choices Educate patient’s family on nutrient-dense choices for supplemental feedings (E - nutrition education)for supplemental feedings (E - nutrition education)

Monitoring and Evaluation
• Initiate calorie count while patient is Initiate calorie count while patient is hospitalized to evaluate acceptance of oral hospitalized to evaluate acceptance of oral supplementssupplements
• Weigh patient weekly after discharge Weigh patient weekly after discharge • Evaluate patient’s ability to chew textured Evaluate patient’s ability to chew textured
foods after dentures are replacedfoods after dentures are replaced• Evaluate patient in Geriatric Clinic in one Evaluate patient in Geriatric Clinic in one
monthmonth

The Diet Prescription
• Designates type, amount, frequency of Designates type, amount, frequency of feeding based on pt’s needs, care goalsfeeding based on pt’s needs, care goals
• May specify calorie goalMay specify calorie goal• May limit or increase various components May limit or increase various components
of the dietof the diet• Each institution usually has specific diets Each institution usually has specific diets
that have been approved by committee that that have been approved by committee that are used at that institutionare used at that institution

Modifications of the Normal Diet• Normal nutrition is foundation of Normal nutrition is foundation of
therapeutic diet modificationstherapeutic diet modifications• Based on DRIsBased on DRIs• Based on Food Guide PyramidBased on Food Guide Pyramid
• Purpose of diet is to supply needed Purpose of diet is to supply needed nutrientsnutrients

Modifications of the Normal Diet
• Change in consistencyChange in consistency• Increase/decrease energy value of dietIncrease/decrease energy value of diet• Increase/decrease type of food or nutrient Increase/decrease type of food or nutrient
consumedconsumed• Elimination of specific foods or componentsElimination of specific foods or components• Adjustment in level, ratio, balance of protein, Adjustment in level, ratio, balance of protein,
fat, CHOfat, CHO• Change in number, frequency of mealsChange in number, frequency of meals• Change in route of delivery of nutrientsChange in route of delivery of nutrients

Basic Hospital Diets
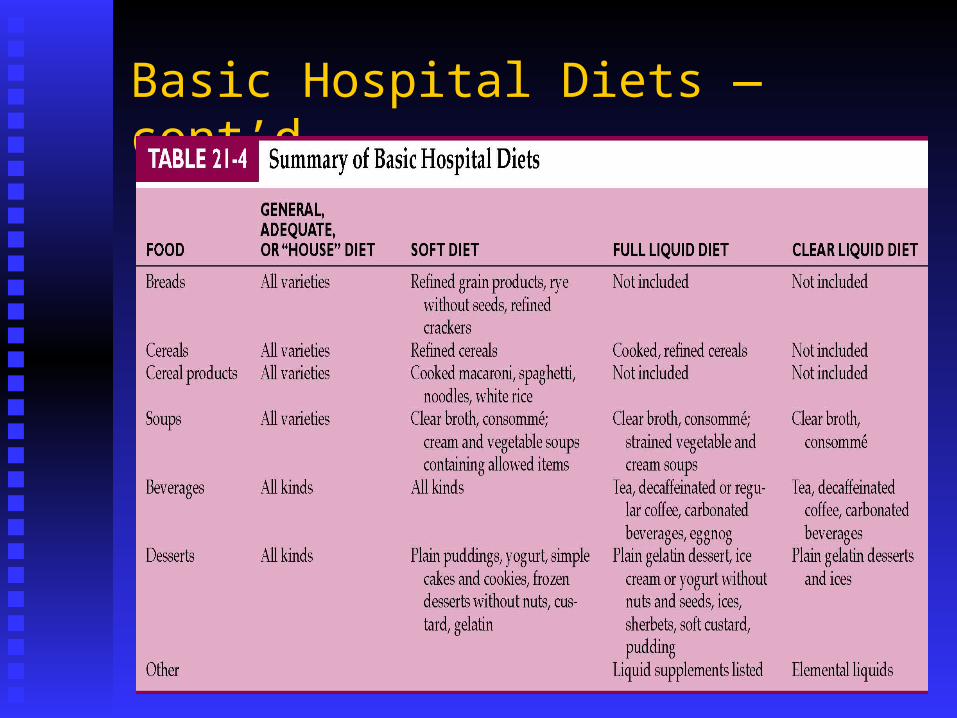
Basic Hospital Diets —cont’d

“Surgical” Soft Diet

Clear Liquid Diet

Full Liquid Diet
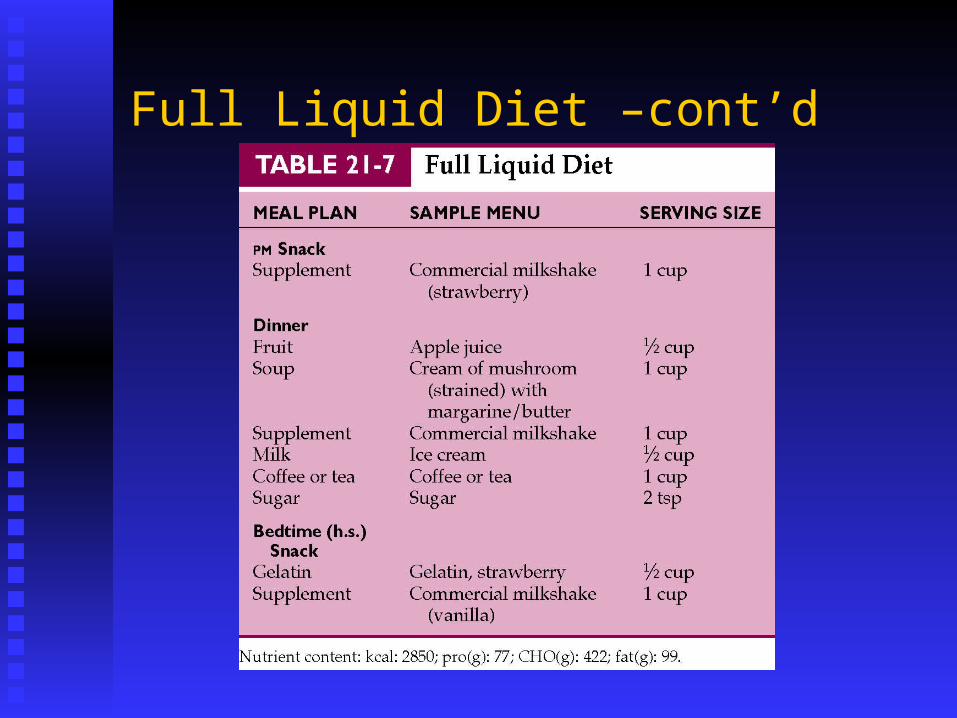
Full Liquid Diet –cont’d

House or Standard Diet Controversies
• Should the house diet be low in fat, Should the house diet be low in fat, saturated fat, sodium, and sugar to conform saturated fat, sodium, and sugar to conform with the U.S. dietary guidelines?with the U.S. dietary guidelines?
• Should the house diet be intended to Should the house diet be intended to maximize the nutritional intake of sick maximize the nutritional intake of sick people, featuring familiar, comfort foods people, featuring familiar, comfort foods and fulfilling patient preferences and and fulfilling patient preferences and expectations, regardless of conformity to expectations, regardless of conformity to dietary guidelines designed for healthy dietary guidelines designed for healthy people?people?

Consistency Diet Controversies
• Soft Diet: what should be included or excluded? Is Soft Diet: what should be included or excluded? Is the diet ‘dental” soft, “surgical” soft, mechanical the diet ‘dental” soft, “surgical” soft, mechanical soft; the needs of dysphagia patients and dental soft; the needs of dysphagia patients and dental patients are differentpatients are different
• Full liquid diet: there is no evidence that it has a role Full liquid diet: there is no evidence that it has a role as part of a surgical progression; many of the foods as part of a surgical progression; many of the foods included are poorly tolerated by persons included are poorly tolerated by persons immediately post GI surgery (dairy products, fats, immediately post GI surgery (dairy products, fats, etc.) May be useful as a source of nutrition for etc.) May be useful as a source of nutrition for persons with mouth pain or dental surgerypersons with mouth pain or dental surgery

Consistency Diet Controversies
• Thickened liquids: when speech Thickened liquids: when speech pathologists recommend specific liquid pathologists recommend specific liquid consistencies, they may be using a consistencies, they may be using a different standard than is used in the food different standard than is used in the food and nutrition departmentand nutrition department
• There is no generally-accepted standard for There is no generally-accepted standard for nectar thick, honey thick, etc. Often these nectar thick, honey thick, etc. Often these foods vary greatly among and within foods vary greatly among and within institutions and depending on where and institutions and depending on where and by whom the thickening is doneby whom the thickening is done

Therapeutic Diet Controversies
• Should patients with Should patients with chronic diseases who chronic diseases who are hospitalized with are hospitalized with acute illnesses be acute illnesses be placed on the placed on the restricted diet that is restricted diet that is appropriate for them appropriate for them long term? long term?

Therapeutic Diet Controversies• Should residents in Should residents in
long term care long term care facilities have the facilities have the same right as home-same right as home-based clients to decide based clients to decide whether or not to whether or not to follow a restricted follow a restricted diet?diet?

Nutritional Care of the Terminally Ill Patient• Maintenance of comfort and quality of life Maintenance of comfort and quality of life
are the main goals of nutritional care for are the main goals of nutritional care for terminally ill patients = “palliative care”terminally ill patients = “palliative care”
• Dietary restrictions and aggressive nutrition Dietary restrictions and aggressive nutrition care that negatively impacts quality of life care that negatively impacts quality of life are rarely appropriate.are rarely appropriate.

Palliative Care• Encourages the alleviation of physical Encourages the alleviation of physical
symptoms, anxiety, and fear while symptoms, anxiety, and fear while attempting to maintain the patient’s ability attempting to maintain the patient’s ability to function independentlyto function independently

Continuity of Care• Due to shortened length of stay, more nutritional Due to shortened length of stay, more nutritional
care is being provided in alternative settings (long care is being provided in alternative settings (long term care, home care, ambulatory clinics and term care, home care, ambulatory clinics and community programs)community programs)
• Nutrition counseling and education in acute care is Nutrition counseling and education in acute care is often limited to survival skillsoften limited to survival skills
• Nutritional counseling should be provided in a Nutritional counseling should be provided in a setting conducive to long term behavior changesetting conducive to long term behavior change
• The acute care stay can be an opportunity to The acute care stay can be an opportunity to identify nutritional problems and devise a plan for identify nutritional problems and devise a plan for follow-up carefollow-up care

Discharge PlanningDischarge documentation includesDischarge documentation includes• Summary of nutritional therapies and Summary of nutritional therapies and
outcomesoutcomes• Pertinent information such as weight, lab Pertinent information such as weight, lab
results, dietary intakeresults, dietary intake• Potential drug-nutrient interactionsPotential drug-nutrient interactions• Expected progress or prognosisExpected progress or prognosis• Recommendations for follow-up servicesRecommendations for follow-up services

Discharge Planning
Courtesy University of Washington Medical Centers, Seattle.
Related Documents











