Diagnosis and Management of Sepsis BMC Sepsis Mortality Reduction Initiative Intern Noon Conference 7.2.13 Karin Sloan, MD Director of Quality, Dept of Medicine for the Sepsis Mortality Reduction taskforce

Diagnosis and Management of Sepsis BMC Sepsis Mortality Reduction Initiative Intern Noon Conference 7.2.13 Karin Sloan, MD Director of Quality, Dept of.
Jan 15, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diagnosis and Management of SepsisBMC Sepsis Mortality Reduction Initiative
Intern Noon Conference7.2.13
Karin Sloan, MDDirector of Quality, Dept of Medicinefor the Sepsis Mortality Reduction taskforce
Outline• Sepsis: definitions• Introduce BMC sepsis mortality reduction
initiative– Rationale for sepsis work– Focus on hospital-acquired sepsis
• Stress 2 key areas:– Timely recognition of sepsis– Timely administration of broad-spectrum antibiotic
• Show SCM sepsis order set
Sepsis• Sepsis: a dysregulated inflammatory response
of the body to infection• High mortality rate• More common than MI and stroke• Most common post-op complication• Like MI and stroke, time to treatment saves
lives

2012 BMC Sepsis Patients Expired vs. Discharged
883 sepsis pts in 2012141 sepsis deaths
What is SIRS?
• SIRS “Systemic Inflammatory Response Syndrome”
• Dysregulated inflammatory response • Patients can have SIRS without infection
– PE, acute blood loss, etc
• Sometimes when a patient has SIRS, it is not certain if they have infection

Sepsis: Infection plus some of:• Temperature >38.3 or <36ºC• Heart rate >90 beats/min or more than two standard deviations above the
normal value for age• Tachypnea, respiratory rate >20 breaths/min • **Altered mental status• Hyperglycemia in the absence of diabetes• Leukocytosis (WBC count >12,000 microL–1), greater than 10 percent
immature forms, or leukopenia (WBC count <4000 microL–1) • Hypotension • Hypoxemia• Acute kidney injury • Coagulation abnormalities • Ileus • Thrombocytopenia • Hyperbilirubinemia • Hyperlactatemia
Red: 2/4 = SIRS criteria
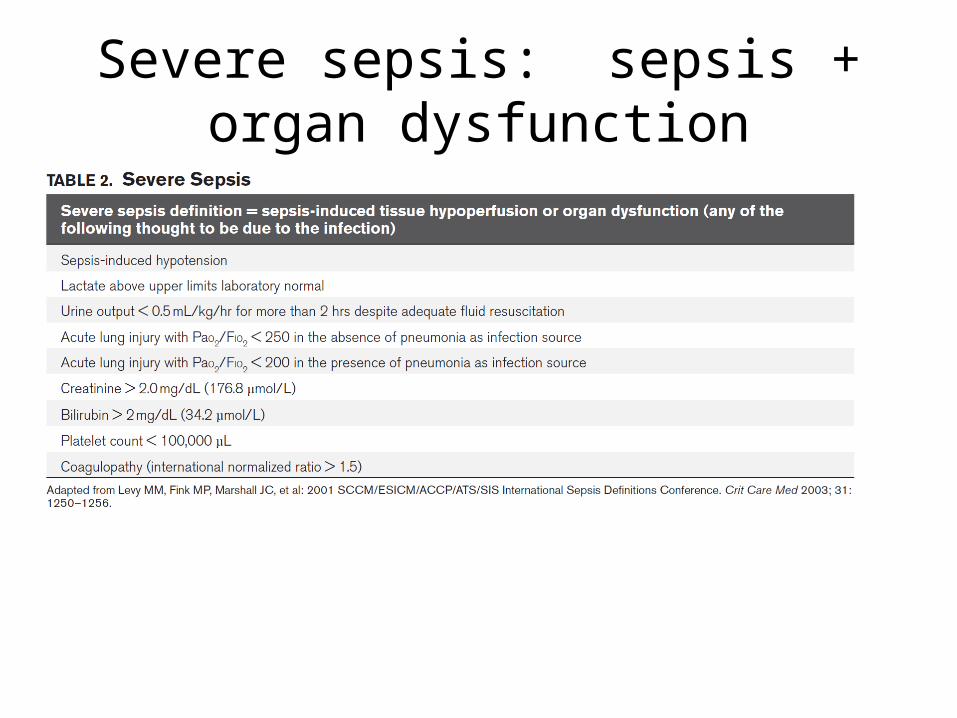
Severe sepsis: sepsis + organ dysfunction

Definition: Septic Shock
• Severe sepsis plus hypotension not reversed with adequate fluid resuscitation (30ml/kg crystalloid)– SBP < 90– MAP < 70– SBP > 40 decrease from baseline
• Vasodilatory shock– Low SVR– BP = CO x SVR
• Multiple organ dysfunction syndrome (MODS)
SIRSsepsisMODS continuum• If sepsis is possible, without alternative
explanation, best to treat empirically – Document “SIRS; suspected sepsis or possible
sepsis”
• Can reassess, narrow or discontinue antibiotics later
Sepsis Background
• Patients with positive blood cultures almost always have sepsis, severe sepsis, or septic shock
• Sepsis incidence is increased in older adults, and mortality is higher
• Mortality highest for unknown, GI, or pulmonary source – lower for urinary tract source
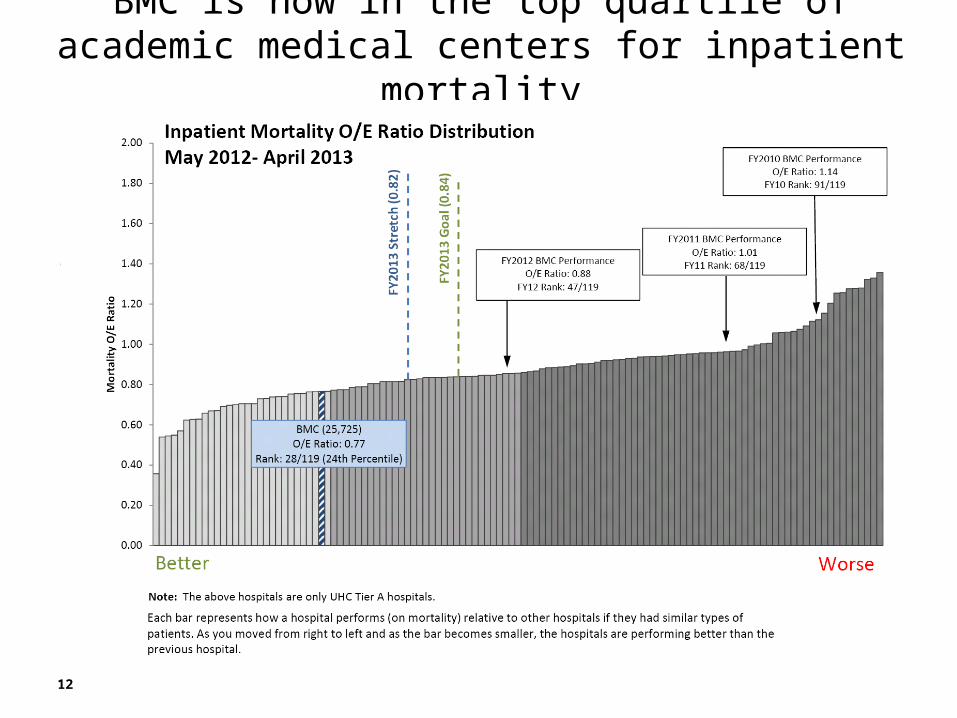
BMC is now in the top quartile of academic medical centers for inpatient mortality
•Slide showing mortality improvements…
12
But…our sepsis mortality lags behind.
• Why work on sepsis at BMC?– Volume of cases
• Top cause of excess deaths at 2013 mortality goal• Of the 444 inpatient deaths in FY12, sepsis was coded in
31%
– Opportunity for improvement• Particularly in hospital-acquired sepsis (65th percentile
performance)– 20% of BMC sepsis cases
• Recognition• Time to antibiotics

Aim Statement
• To improve BMC hospital-acquired sepsis mortality O/E from UHC 65th percentile to 25th percentile by July 2014.– Save 1 hospital-acquired sepsis life/month.– Mortality O/E = Outcome Measure
• Process Measures– Use of sepsis order set (Process)– % with STAT first antibiotic order (Process)– % of patients receiving broad spectrum abx within 60 mins (Process)– Time to broad spectrum abx (Process)– % of pts with 2 blood cxs before abx (Balancing)

Early Goal-Directed Therapy (EGDT) 30.5% mortality, vs standard therapy 46.5%
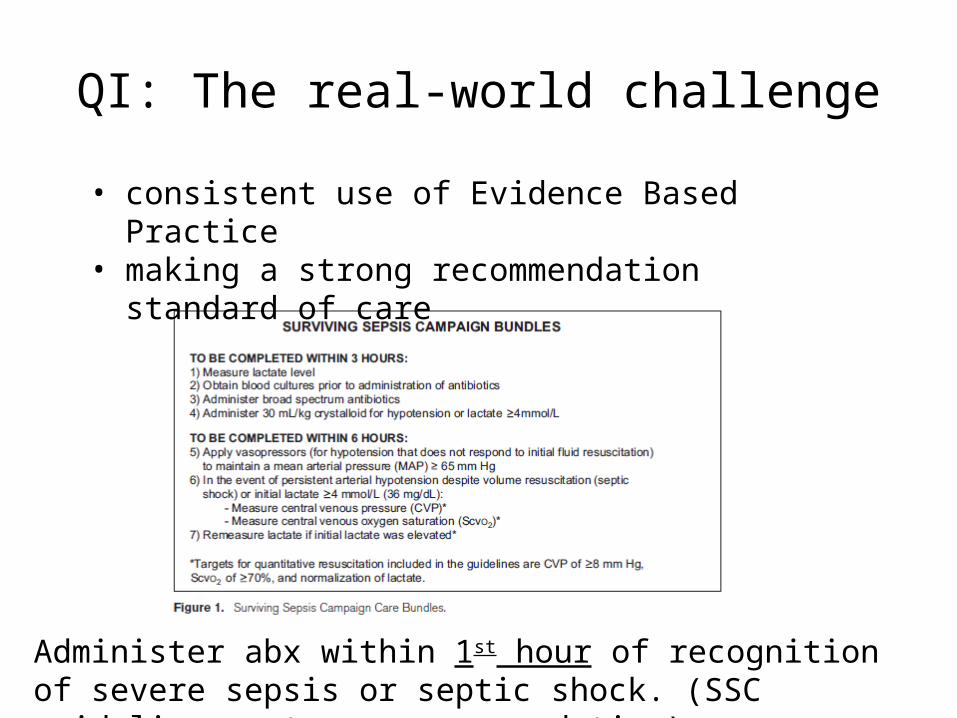
QI: The real-world challenge
• consistent use of Evidence Based Practice• making a strong recommendation standard of
care
Administer abx within 1st hour of recognition of severe sepsis or septic shock. (SSC guidelines: strong recommendation)

Time to Antibiotic and Choice of Antibiotic are key to saving sepsis lives
• Broad spectrum antibiotic or “anchor” antibiotic should always be administered first
– Cefepime 1g, Cetriaxone 2g, or Levofloxacin 750mg• Stocked in all Pyxis machines at BMC
• Vancomycin is not broad spectrum and can lead to delay in getting the most important antibiotic• Anchor Antibiotic
– Effective against rapidly lethal organisms• Gram negative rods• S. pneumoniae
– Long half-life– Can be infused quickly– Low incidence of allergy– Must be premixed or easy-mix, and dosing must not be weight-based
•
Goal 1: Decrease time to antibiotics in BMC hospital-acquired sepsis patients• PI group met• Defined reason for action• Mapped initial & target state
– Current performance: mean time from antibiotic order to administration 200 minutes
• Goal: 60 minutes from order to administration
• Performed gap analysis• Solution approach (to perform P-D-S-A)
– Ordering – changing sepsis order set– RN/MD Education on importance of broad spectrum abx first and time
to abx– Communication

Sepsis Order Set

Sepsis Order set

STAT and continuing dose antibiotic options

Lab, micro, radiology
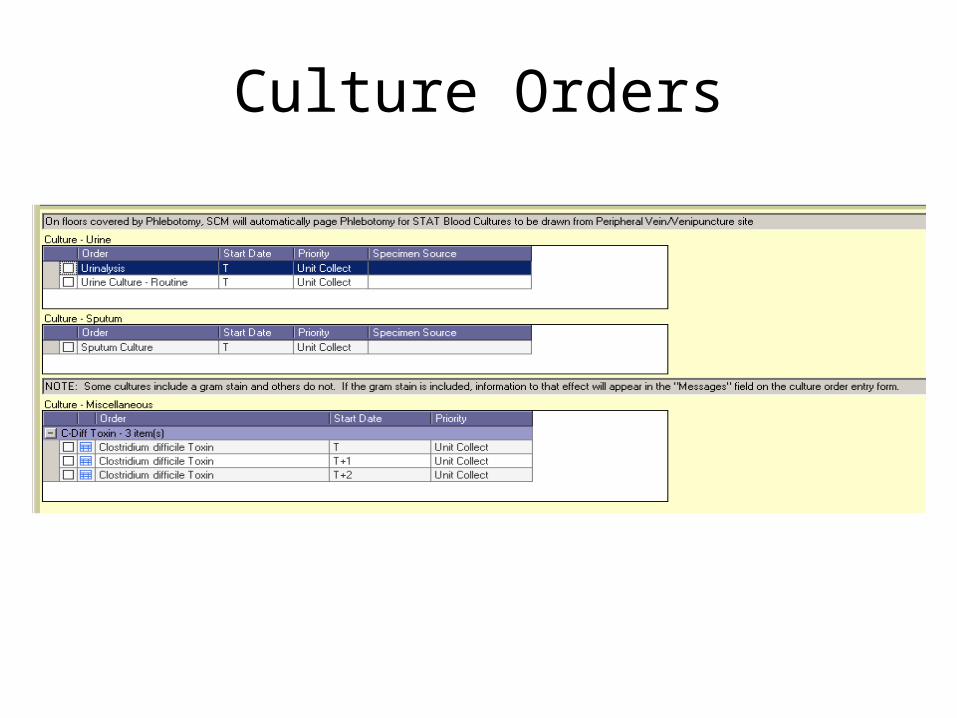
Culture Orders
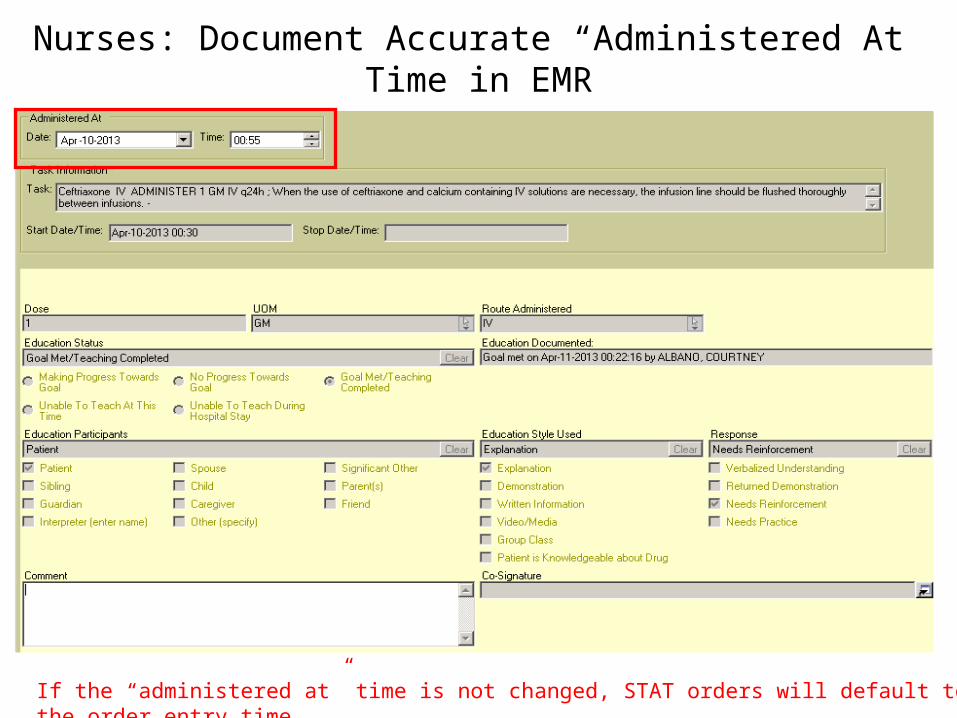
Nurses: Document Accurate “Administered At” Time in EMR
If the “administered at” time is not changed, STAT orders will default to the order entry time.
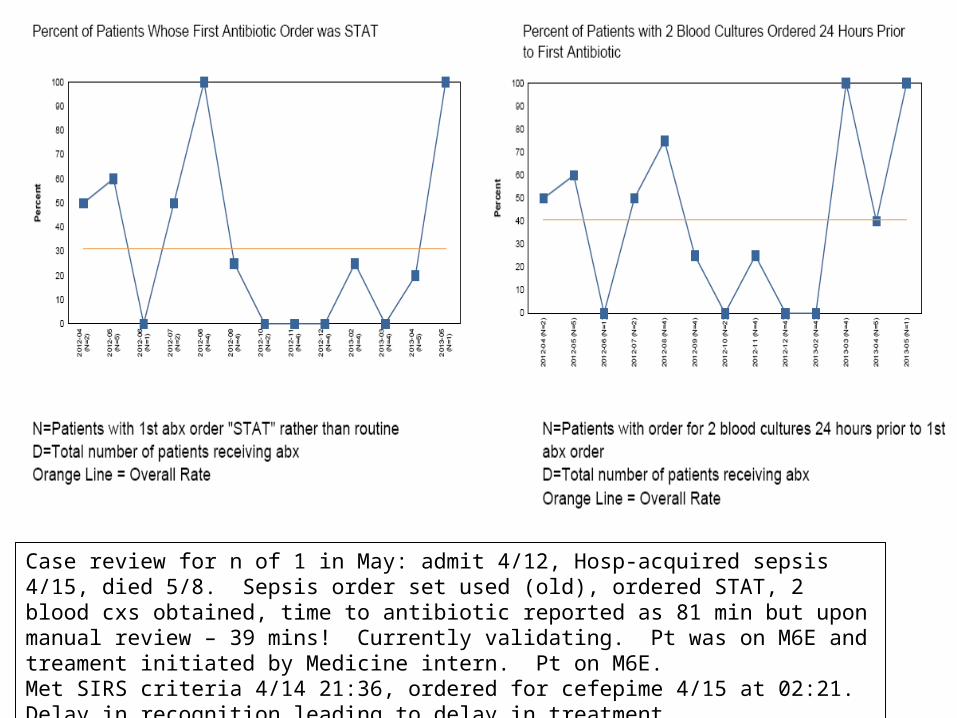
Case review for n of 1 in May: admit 4/12, Hosp-acquired sepsis 4/15, died 5/8. Sepsis order set used (old), ordered STAT, 2 blood cxs obtained, time to antibiotic reported as 81 min but upon manual review – 39 mins! Currently validating. Pt was on M6E and treament initiated by Medicine intern. Pt on M6E.Met SIRS criteria 4/14 21:36, ordered for cefepime 4/15 at 02:21. Delay in recognition leading to delay in treatment.

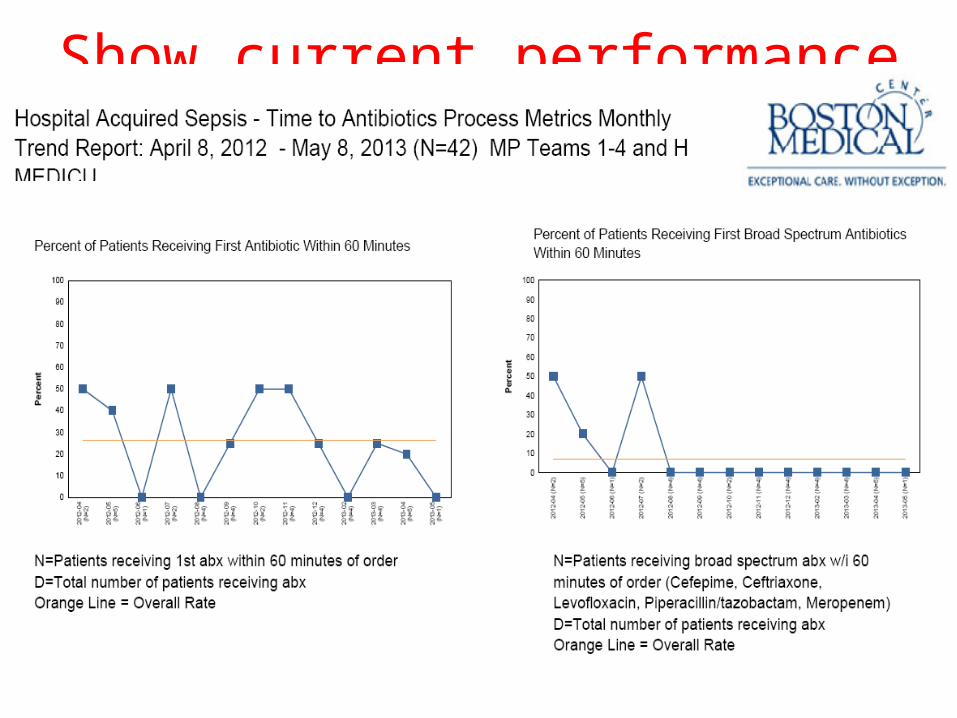
Show current performance data
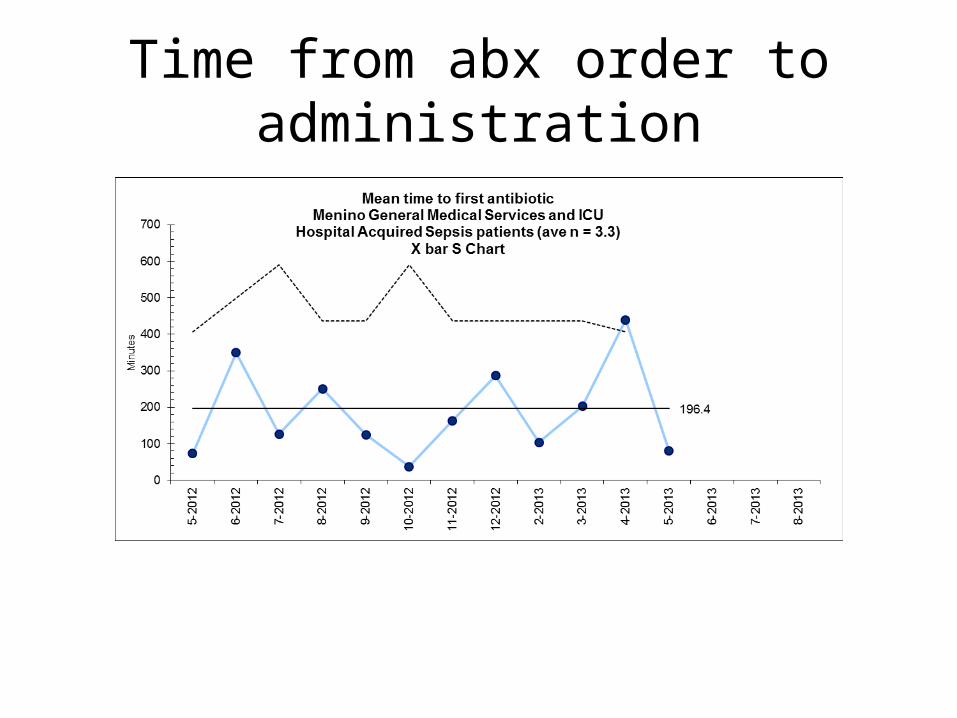
Time from abx order to administration
Goal 2: Improve recognition of hospital-acquired sepsis at BMC
• PI group met• Defined reason for action, mapped initial & target state,
performed gap analysis, and solution approach• Kirkpatrick, Walkey, et al 2013 ATS abstract: Review of 35 BMC
patients from 2008-2010 who died of hospital-acquired sepsis:– 12 (34%) had a greater than 6 hour delay in recognition or treatment of
severe sepsis– 7 patients with delay > 12 hours after the onset of severe sepsis– Patients without tachycardia were statistically more likely to be missed.– Trend towards patients on nodal blockers being more likely to be missed.
Recognition solutions to test
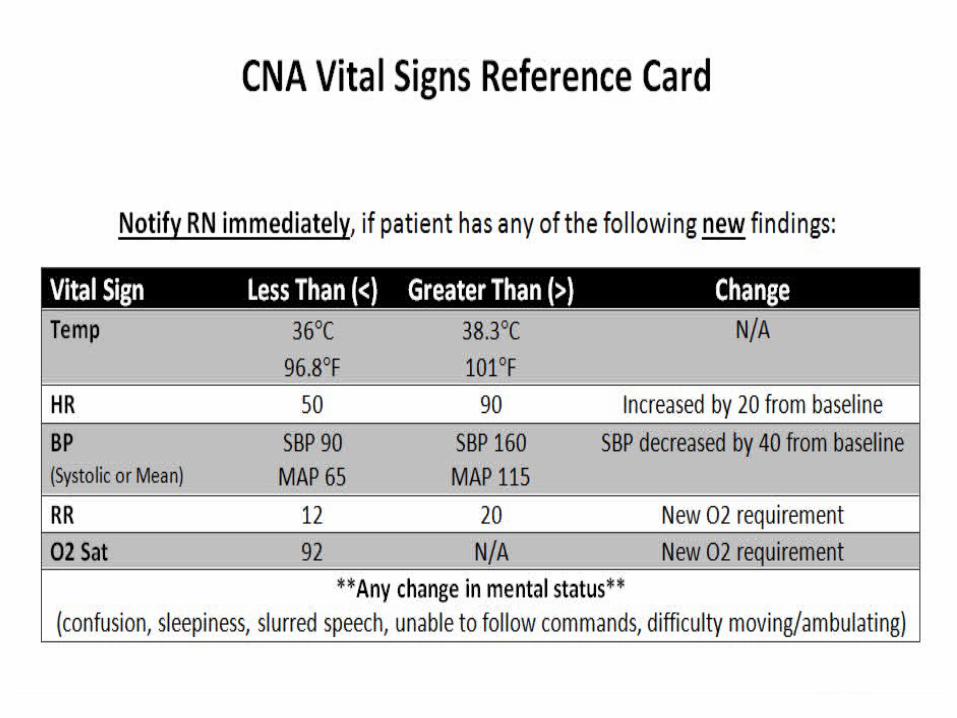
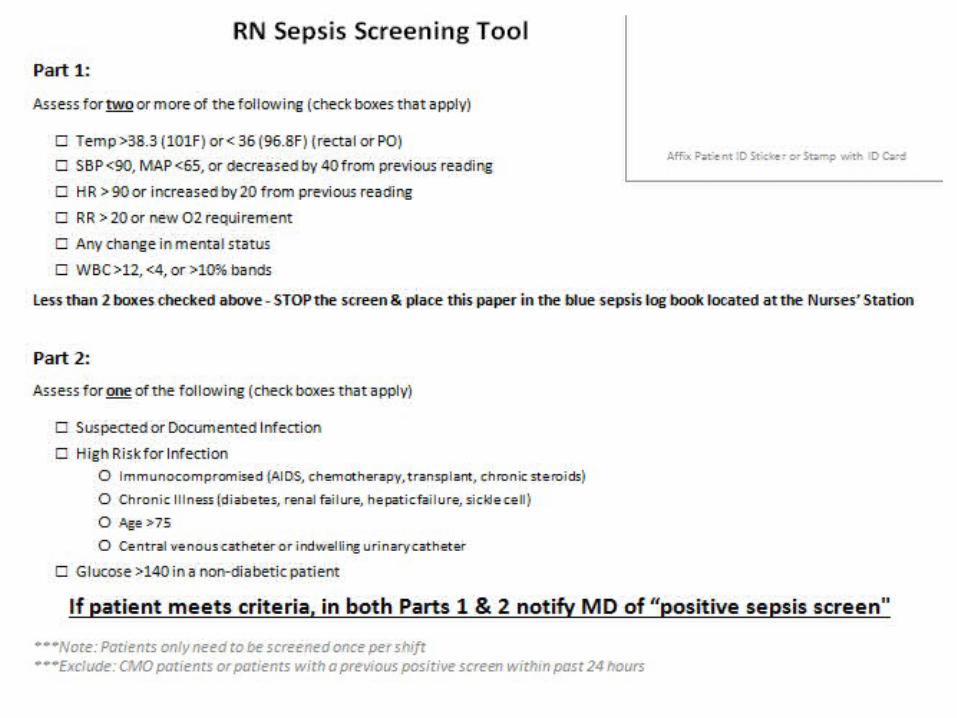
• Pilot on Menino 6W began end of April– Education – CNA RN notification parameters– RN paper screening tool
• v1: identified many patients already on abx• v2: exclude patients on abx.
– Without prompts, difficult for nurses to remember to complete.
– Changing flowsheet visual cues
• MD Notification – always text page• Helps providers know the urgency of the page• Patient name• Patient location• RN name• Call back number• Concern (sepsis)
• If RN does not reach someone, they have been instructed to go up the chain (call resident, attending if no one can be reached)
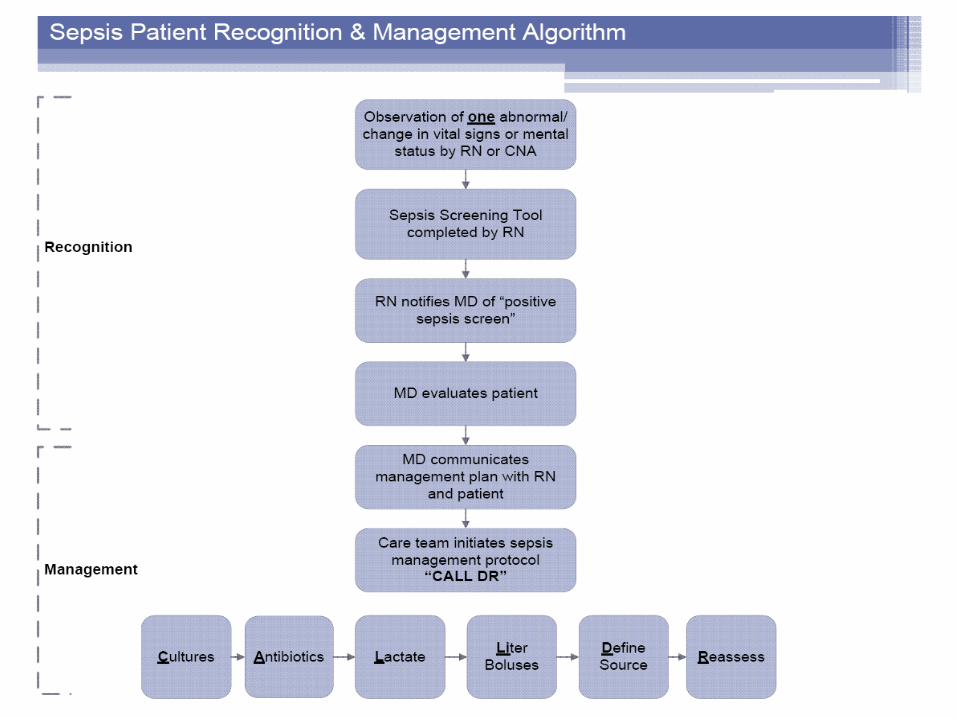
Nurses: “CALL DR”
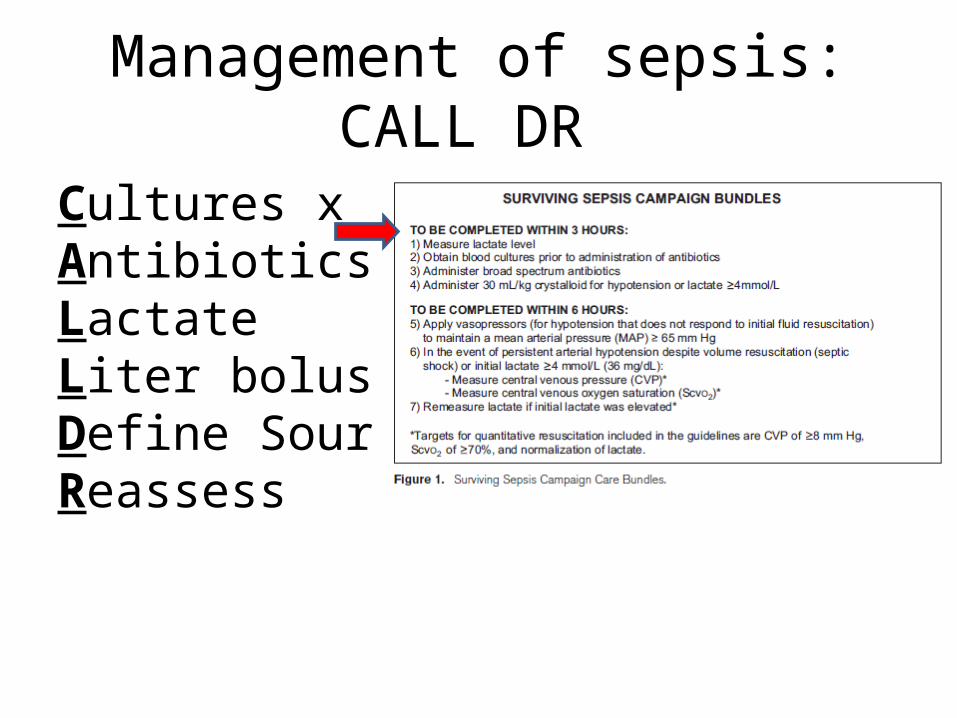
Management of sepsis: CALL DR
Cultures x 2AntibioticsLactate Liter bolusesDefine SourceReassess
• Goal to draw 2 sets prior to antibiotic administration• Do not delay antibiotics – most important sepsis goal is to
administer broad spectrum antibiotics within 60 minutes – Draw blood cultures as soon as possible– Have a charcoal additive to remove antibiotics, if drawn after antibiotic
administration
• 2 sets and 2 separate peripheral venipuncture sites (per BMC policy 3.76)
• BC Bottles:– Should be labeled with source (peripheral, central line, etc.)– Are plastic and should be sent to the lab via P-tube
Cultures x 2
Antibiotics (Broad Spectrum in < 60 mins)
Lactate
• Measure of tissue hypoperfusion• Stratify severity of sepsis, severe sepsis• Follow value with resussitation, goal to
normalize

Liter boluses
• For severe sepsis: 30ml/kg bolus Normal Saline or Lactated Ringers– 70kg patient = 2L bolus
• Goals in first 6 hours (early goal-directed therapy):– CVP 8-12 mmHg– MAP ≥ 65 mmHg– UOP ≥ 0.5ml/kg/hr– SVC sat ≥ 70%
Define Source
• As directed by patient signs and symptoms, in addition to blood cultures, may order UA, urine culture, CXR, imaging

Reassess
• Follow heart rate, blood pressure, urine output, lactate to determine whether patient is improving or worsening
• Consinder whether patient may need to be transferred to IMCU or ICU
• Follow up cultures and narrow or discontinue antibiotics if appropriate

In Summary…• Have a heightened suspicion for sepsis• Respond to RN notification in a timely manner• Document SIRS and sepsis• Treat aggressively and empirically for possible sepsis
– Can always peel back later
• Use the SCM “sepsis order set” to initiate early goal-directed therapy
• Communicate that timely orders were placed– Stress importance of broad spectrum within 60 minutes
• Notify the attending of a change in patient’s clinical status– Involve the MICU if necessary

Future Directions
• Nursing floor spread • Spread to ICU, Surgical services, ultimately
medical specialty services• Possible simulation teams training• Feedback welcome on the sepsis initiative
overall• Potential for resident involvement
Acknowledgements• Steering Committee• Stephanie Martinez• Willie Baker• James Murphy• Kate Mandell• Tamar Barlam• Kevin Horbowicz• Jennifer Ellingwood• Jane Jansen• Patty Covelle• George Barth• Louise Vecchio
• Roshan Hussain• Paul Kelley• Tom Lau• Kevin Guy• Nahid Bhadelia• Morsal Tahouni• Jim Meisel• Jake Feldman• Allan Walkey• Don Johnstone and 6W staff• Ann Woolley, Stephanie Maximous, Morgan
Richards, Jeff Jenks• YOU!!• Surgery residents and PA• Eric Poon• Stan Hochberg• Laura Harrington
Related Documents











