Diabetic Ketoacidosis Management Heidi Chamberlain Shea, MD Endocrine Associates of Dallas

Diabetic Ketoacidosis Management Heidi Chamberlain Shea, MD Endocrine Associates of Dallas.
Dec 13, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diabetic Ketoacidosis Management
Heidi Chamberlain Shea, MDEndocrine Associates of Dallas

Goals of Discussion
• Pathophysiology of DKA
• Biochemical criteria for DKA
• Treatment of DKA
• Prevention of DKA
• Hyperosmolar Nonketoic Syndrome

Epidemiology
• Annual incidence in U.S. – 5-8 per 1000 diabetic
subjects
• 2.8% of all diabetic admissions are due to DKA
• Overall mortality rate ranges from 2-10%– Higher is older patients

DKAPrecipitating Factors
• Failure to take insulin• Failure to increase insulin
– Illness/Infection• Pneumonia
• MI
• Stroke
– Acute stress• Trauma
• Emotional
• Medical Stress– Counterregulatory
hormones• Oppose insulin
• Stimulate glucagon release
• Hypovolmemia– Increases glucagon and
catecholamines• Decreased renal blood
flow
• Decreases glucagon degradation by the kidney

Diabetic Ketoacidosis
Due to:
Severe insulin deficiency
Excess counterregulatory hormones
Glucagon
Epinephrine
Cortisol
Growth hormone

Role of Insulin• Required for transport of glucose into
– Muscle– Adipose– Liver
• Inhibits lipolysis• Absence of insulin
– Glucose accumulates in the blood– Liver
• Uses amino acids for gluconeogenesis• Converts fatty acids into ketone bodies
– Acetone, Acetoacetate, β-hydroxybutyrate
– Increased counterregulatory hormones

Counterregulatory Hormones - DKAIncreases
insulin resistance
Activates glycogenolysis
and gluconeogenesis
Activates lipolysis
Inhibits insulin secretion
Epinephrine X X X XGlucagon XCortisol X XGrowth
Hormone X X X

Insulin Deficiency
Glucose uptakeProteolysis
Lipolysis
Amino Acids
Glycerol Free Fatty Acids
GluconeogenesisGlycogenolysisHyperglycemiaHyperglycemia Ketogenesis
AcidosisAcidosisOsmotic diuresis DehydrationDehydration

Signs and Symptoms of DKA
• Polyuria, polydipsia– Enuresis
• Dehydration– Tachycardia– Orthostasis
• Abdominal pain– Nausea– Vomiting
• Fruity breath– Acetone
• Kussmaul breathing• Mental status
changes– Combative– Drunk– Coma

Lab Findings• Hyperglycemia• Anion gap acidosis
– (Na + K) – (Cl + Bicarb) >12
– Bicarbonate <15 mEq/L– pH <7.3
• Urine ketones and serum ketones
• Hyperosmolarity

Differential Diagnosis Anion Gap Acidosis
• Alcoholic ketoacidosis
• Lactic acidosis
• Renal failure
• Ethylene glycol or methyl alcohol poisoning
• Starvation in late pregnancy or lactation (rare)

Atypical Presentations
• DKA can be present with BS <300– Impaired gluconeogenesis
• Liver disease• Acute alcohol ingestion• Prolonged fasting• Insulin-independent glucose is high (pregnancy)
– Chronic poor control but taking insulin
• Bedside urine ketones false negatives– Measure acetoacetate not β-hydroxybutyrate– Send blood to lab

Treatment of DKA• Initial hospital
management– Replace fluid and
electrolytes– IV Insulin therapy– Glucose administration– Watch for complications– Disconnect insulin pump
• Once resolved– Convert to home insulin
regimen– Prevent recurrence

Treatment of DKAFluids and Electrolytes
• Fluid replacement– Restores perfusion of the tissues
• Lowers counterregulatory hormones
– Average fluid deficit 3-5 liters
• Initial resuscitation– 1-2 liters of normal saline over the first 2 hours– Slower rates of 500cc/hr x 4 hrs or 250 cc/hr x 4
hours • When fluid overload is a concern
• If hypernatremia develops ½ NS can be used

Treatment of DKAFluids and Electrolytes
• Hyperkalemia initially present– Resolves quickly with insulin drip– Once urine output is present and K<5.0, add
20-40 meq KCL per liter.
• Phosphate deficit– May want to use Kphos
• Bicarbonate not given unless pH <7 or bicarbonate <5 mmol/L

Treatment of DKAInsulin Therapy
• IV bolus of 0.1-0.2 units/kg (~ 10 units) regular insulin
• Follow with hourly regular insulin infusion
• Glucose levels – Decrease 75-100 mg/dl hour– Minimize rapid fluid shifts
• Continue IV insulin until urine is free of ketones

Treatment of DKAGlucose Administration
• Supplemental glucose– Hypoglycemia occurs
• Insulin has restored glucose uptake • Suppressed glucagon
– Prevents rapid decline in plasma osmolality• Rapid decrease in insulin could lead to cerebral
edema
• Glucose decreases before ketone levels decrease
• Start glucose when plasma glucose <300 mg/dl

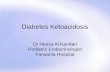
Insulin-Glucose Infusion for DKABlood glucose Insulin Infusion D5W Infusion
<70 0.5 units/hr 150 cc/hr
70-100 1.0 125
101-150 2.0 100
151-200 3.0 100
201-250 4.0 75
251-300 6.0 50
301-350 8.0 0
351-400 10.0 0
401-450 12.0 0
451-500 15.0 0
>500 20.0 0

Complications of DKA• Infection
– Precipitates DKA– Fever– Leukocytosis can be secondary
to acidosis
• Shock– If not improving with fluids
r/o MI
• Vascular thrombosis– Severe dehydration– Cerebral vessels– Occurs hours to days after
DKA
• Pulmonary Edema– Result of aggressive fluid
resuscitation
• Cerebral Edema– First 24 hours– Mental status changes– Tx: Mannitol– May require intubation with
hyperventilation

Once DKA ResolvedTreatment
• Most patients require 0.5-0.6 units/kg/day• Pubertal or highly insulin resistant patients
– 0.8-1.0 units/kg/day• Long acting insulin
– 1/2-2/3 daily requirement– NPH, Levemir or Lantus
• Short acting insulin– 1/3-1/2 given at meals– Regular, Humalog, Novolog or Apidra
• Give insulin at least 2 hours prior to weaning insulin infusion.

Prevention of DKASick Day Rules
• Never omit insulin– Cut long acting in half
• Prevent dehydration and hypoglycemia
• Monitor blood sugars frequently
• Monitor for ketosis• Provide supplemental fast
acting insulin• Treat underlying triggers• Maintain contact with
medical team

Goals of Discussion
• Pathophysiology of DKA
• Biochemical criteria for DKA
• Treatment of DKA
• Prevention of DKA
• Hyperosmolar Nonketoic Syndrome

Hyperosmolar Nonketotic Syndrome
• Extreme hyperglycemia and dehydration– Unable to excrete glucose as quickly as it
enters the extracellular space– Maximum hepatic glucose output results in a
plateau of plasma glucose no higher than 300-500 mg/dl
– When sum of glucose excretion plus metabolism is less than the rate which glucose enters extracellular space.

Hyperosmolar Nonketotic Syndrome
• Extreme hyperglycemia and hyperosmolarity• High mortality (12-46%)• At risk
– Older patients with intercurrent illness– Impaired ability to ingest fluids
• Urine volume falls– Decreased glucose excretion
• Elevated glucose causes CNS dysfunction and fluid intake impaired
• No ketones– Some insulin may be present– Extreme hyperglycemia inhibits lipolysis

Hyperosmolar Nonketotic Syndrome Presentation
• Extreme dehydration
• Supine or orthostatic hypotension
• Confusion coma
• Neurological findings– Seizures– Transient hemiparesis– Hyperreflexia– Generalized areflexia

Hyperosmolar Nonketotic Syndrome Presentation
• Glucose >600 mg/dl
• Sodium– Normal, elevated or low
• Potassium– Normal or elevated
• Bicarbonate >15 mEq/L
• Osmolality >320 mOsm/L

Hyperosmolar Nonketotic Syndrome Treatment
• Fluid repletion– NS 2-3 liters rapidly– Total deficit = 10 liters
• Replete ½ in first 6 hours
• Insulin– Make sure perfusion is adequate – Insulin drip 0.1U/kg/hr
• Treat underlying precipitating illness

Clinical Errors• Fluid shift and shock
– Giving insulin without sufficient fluids– Using hypertonic glucose solutions
• Hyperkalemia– Premature potassium administration before insulin has begun to
act
• Hypokalemia– Failure to administer potassium once levels falling
• Recurrent ketoacidosis – Premature discontinuation of insulin and fluids
when ketones still present
• Hypoglycemia– Insufficient glucose administration

Conclusion• Successful management
requires– Judicious use of fluids
• Establish good perfusion
– Insulin drip• Steady decline
• Complete resolution of ketosis
– Electrolyte replacement– Frequent neurological
evaluations – High suspicion for complications
• Determine etiology to avoid recurrent episodes
Related Documents