PBL

Diabetic Ketoacidosis
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PBL
CASE
An 18-year-old female was taken to the
emergency room in coma
Her parents noticed that she had polydipsia,
polyuria, and rapid weight loss which started
approximately 1 month ago and had worsened
in the last week
She had not been taking any medications and
the clinical history was otherwise unremarkable
On examination
breathing was deep and rapid (Kussmaul respiration),
pulse rate was 100 beats per minute, and
blood pressure 110/70 mmHg;
she also had signs of dehydration
CNS - She was drowsy and confused, no FND
CVS – S1 and S2 heard
RS – NVBS, No added sounds
INVESTIGATIONS
hematocrit 44%,
hemoglobin 13 g/dl
white blood cell count 12,000/ μl,
glucose 520 mg/dl
urea 50 mg/dl creatinine 1.0 mg/dl
Na+ 130 mEq/L K+ 4.6 mEq/L, PO4 2.0 mEq/L Cl− 112 mmol/L Mg 1.6
Arterial pH was 7.0, PO 98 mmHg, PCO 25 mmHg, HCO 12 mEq/L AG 16
O 2 sat 98%.
Serum Osmolality 306
What is your diagnosis?
Which additional biochemical tests are
required to confirm the diagnosis?
Precipitating events?
Inadequate insulin administration
Infection (pneumonia/UTI/gastroenteritis/sepsis)
Infarction (cerebral, coronary, mesenteric, peripheral)
Drugs (cocaine)
Pregnancy
Symptoms and signs

Polyuria, thirst
Weight loss
Weakness
Nausea, vomiting
Leg cramps
Blurred vision
Abdominal pain
Dehydration
Hypotension (postural or supine)
Cold extremities/peripheral cyanosis
Tachycardia
Air hunger (Kussmaul breathing)
Smell of acetone
Hypothermia
Confusion, drowsiness, coma (10%)

Management?
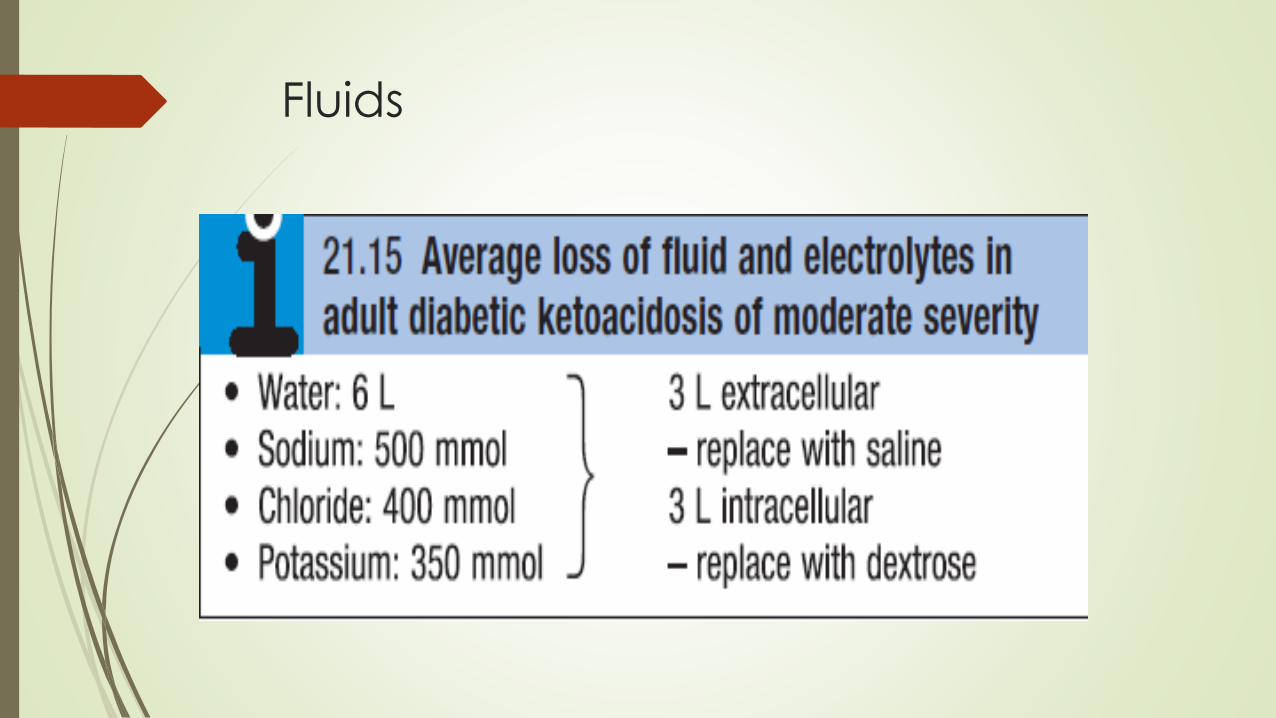
Fluids
Fluid replacement
Time: 0–60 mins
Commence 0.9% sodium chloride
If systolic BP > 90 mmHg, give 1 L over 60 mins
If systolic BP < 90 mmHg, give 500 mL over 10–15 mins,
then re-assess
60 mins to 12 hrs
IV infusion of 0.9% sodium chloride with 40 mmol/L potassium chloride
added as indicated below
1 L over 2 hrs
1 L over 4 hrs
1 L over 6 hrs
If plasma sodium is > 155 mmol/L, 0.45% sodium chloride maybe used
When hemodynamic stability and adequate urine output are achieved, IV
fluids should be switched to 0.45% saline at 250–500 mL/h
Insulin
If the initial serum potassium is <3.3 mmol/L, do not administer insulin until
the potassium is corrected.
0.1 units/kg bolus
intravenous insulin infusion of 0.1 U/kg body weight/hr is recommended
Continue with SC basal insulin analogue if usually taken by patient
glucose concentration should fall by approximately 55–110 mg/dL per hour
Failure of blood glucose to fall within 1 hour of commencing insulin infusion
should lead to a re-assessment of insulin dose
5% glucose and 0.45% saline at 150–250 mL/h when plasma glucose
reaches 200 mg/dL
Potassium
Plasma potassium Potassium replacement
> 5.5 Nil
3.5–5.5 40
< 3.5 additional potassium required
Cardiac rhythm should be monitored in severe DKA because of the risk of
electrolyte-induced cardiac arrhythmia.
Bicarbonate, Mg, Po4
Adequate fluid and insulin replacement should resolve the acidosis.
The use of intravenous bicarbonate therapy is currently not recommended
severe acidosis (arterial pH <6.9), the ADA advises bicarbonate
50 mmol/L of sodium bicarbonate in 200 mL of sterile water with 10 meq/L
KCl per hour for 2 h until the pH is >7.0
Hypomagnesemia may develop during DKA therapy and may also require
supplementation.
serum phosphate < 1 mg/dL, then phosphate supplement should be
considered and the serum calcium monitored
Monitoring
Hourly capillary blood glucose testing
Venous bicarbonate and potassium after 1 and 2 hrs, then
every 2 hrs
Plasma electrolytes every 4 hrs
Clinical monitoring of O2 saturation, pulse, BP, respiratory rate and urine
output every hour
If ketoacidosis has resolved and patient is able to eat and drink
Re-initiate SC insulin
Do not discontinue IV insulin until 30 mins after SC short-acting insulin
injection
Hyperglycaemic hyperosmolar state
severe hyperglycaemia >600 mg/dL
hyperosmolality serum osmolality > 320 mOsm/kg
Dehydration
in the absence of significant hyperketonaemia(< 3 mmol/L) or acidosis (pH
> 7.3, bicarbonate> 15 mmol/L).
hyperglycaemia usually develops over a longer period, causing more
profound hyperglycaemia and dehydration
fluid loss may be 10–22 litres in a person weighing 100 kg
typically occurs in the elderly
Common precipitating factors include
infection,
myocardial infarction,
cerebrovascular events
drug therapy (e.g. corticosteroids).
Give fluid replacement with 0.9% sodium chloride (IV)
Use 0.45% sodium chloride only if osmolality is increasing, despite positive
fluid balance
Target fall in plasma sodium is ≤ 10 mmol/L at 24 hrs
Aim for positive fluid balance of 3–6 L by 12 hrs
replacement of remaining estimated loss over next 12 hrs
Initiate insulin IV infusion (0.05 U/kg body weight/hr) only when blood
glucose is not falling with 0.9% sodium chloride
Reduce blood glucose by no more than 5 mmol/L/hr
Related Documents