Diabetic Foot BY PROF GOUDA ELLABBAN

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diabetic Foot
BYPROF GOUDA ELLABBAN

Definition
A group of disorders in the foot of diabetic patients ranging from ulceration to gangrene.

Causes
1. Hyperglycemia.2. Macroangiopathy.3. Neuropathy.
hyperglycemia
Impairs tissue healing.
Impairs macrophage chemotaxis.
Good medium for bacterial growth.

Macroangiopathy
Impairs tissue healing.
Lead to ischemia and gangrene.
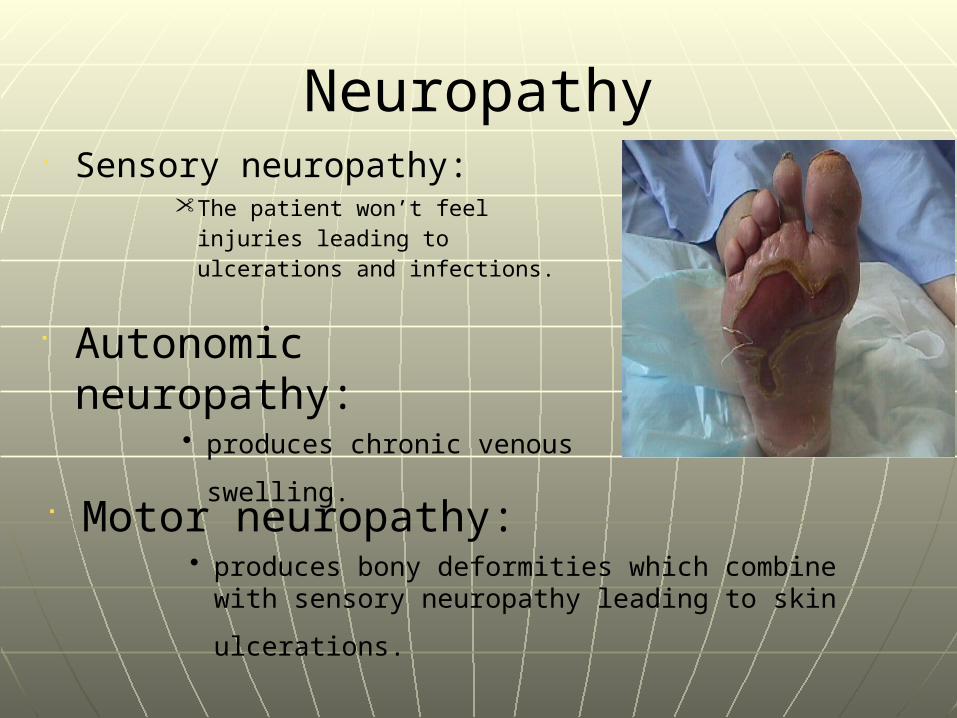
Neuropathy Sensory neuropathy:
• The patient won’t feel injuries leading to ulcerations and infections.
Autonomic neuropathy:• produces chronic venous
swelling.
Motor neuropathy:• produces bony deformities which combine with
sensory neuropathy leading to skin ulcerations.

Clinical presentation
1. Cellulitis:• Redness.• Warm.• Tenderness.• Swelling.
2. Ulcers:• Single or multiple.• May be associated with bleeding.• Thick edges.• Surrounding hyperpigmintation.
3. gangrene:• Arterial block dry gangrene.• Arterial and venous block wet gangrene.
Features of gangrene:• Absence of pulse , sensation , temperature.• Necrotic tissue is a good medium for infections.
4. osteomyelitis:•Spread of infection from a collection of pus in soft tissue to the bone.
5. Joint infection.
6. Bone deformity.

Investigations
1. CBC: leukocytosis.
2. CXR & ECG “ patient > 40 “3. Random and fasting blood sugar.4. X-Ray of the foot:
to role out osteomyelitis and gas gangrene.
5. Swab for culture and sensitivity.

5. Check blood vessels:Doppler waveform assessment; loss of tri phasic
pattern and increased vel.Duplex scan; increased vel.Arteriography: stop metforminMagnetic resonance angiography MRAIntravenous ultrasound IVUS
Severity of the disease with ankle to brachial pressure index ABPI
ABPI norm 09-102, ABPI claudication <0.9, critical ischemia ABPI <0.4-0.5
Pre operative care
- Restore Hg & electrolyte- DM control & hold and type blood- Pain relief & CXR- Treat CHF & arrhythmia- Antiseptic - Cephalosporin/flagyl in mixed injection
intravenously, w/Pen. If moist gangrene for 2d.

Management
1. Control of blood sugar.2. IV antibiotics. “for cellulitis and abscess”
3. Abscess incision and drinage.4. Dry gangrene “follow up autoamputation”
5. Wet gangrene “amputation”
Amputation
Approximately 60% are for vascular disease. 22% for diabetic 9% for trauma. Amputation should not be regarded as an indication of failure, and is frequently a beneficial procedure to relieve pain restore mobility( prosthesis) or rarely to save life. The aim is to achieve a healthy stump for a suitable prosthesis and successful rehabilitation depends upon a team approach, including surgeons prosthetist physiotherapist occupational therapist and counselors.

Indications
Life savingRarely, moist gangrene spreading infection to viable tissue
leading to systemic infectionExtensive tissue necrosis following trauma Uncontrolled sepsis(DF) resulting in systemic infection VascularRest pain/ non healing ulceration in non constructible diseae or
extensive gangrene with loss of function.
HealingPatient selection and level of amputation is important:Above knee 85-90% healing with 40% achieving walking Through knee 50-90% healing but 28% achieve walkingBelow knee 63-95% achieve healing and 75% achieve walking
Levels of amputation: Amputation at a level where there is sufficient tissue
perfusion to allow healing ( arteriograghy to establish the level). The level is improved by treating reconstructible lesion by angioplasty/arterial bypass/profundaplasty/sympathectomy.
Below knee amputation has a reasonable chance of healing if Doppler ACP >50mmhg. Transcutaneous oxygen tension measurement may aid in selection of the appropriate level. If there is reduced sensation diminished skin temperature or muscle tenderness. Amputation should be carried at a higher level.

Hip disarticulation hindquarter amputation\few pts require but needed in pts w/ necrosis
infection malignancy and trauma above the level for AKA
Above knee AKA\ transaction at junction of upper 2/3 & 1/3, 12-15cm
above knee. Fish mouth flaps fashioned Myodesis minimizes bone dislocating within stump &
improve healing Gritti-stokes at the knee\. Long stump with alonger
lever suitable for wheelchair dependent. Less muscles removed and femur transected at 30
degree at the level of adductor tubercle.
Types of Amputation

Through knee\ lower healing rate than Gritti stokes produces a wide stump, cosmetically ugly and prosthesis fitment difficult.
Below knee Wt bearing on patellar tendon with PTB prosthesis.Good knee function is essential. Not to pts w/ flexion
contracture Skew flap method is the best technique rounder more
cosmetic & shorter time for rehab. Tibia is transected 10cm distal to tibial tuberosity and
the fibula 2cm proximally.
Symes 1ry for diabetic the heal pad is spared and its suitability is debatable often it is loose on the tibia. Prosthesis is difficult and a BKA provides greater mobility.

TransmetatarsalUseful in diabetics Essential control of sepsis Long plantarflap essential for good healing w/ transaction at
mid-tarsal level.
RayDistal localized gangrene extending into forefootUseful in diabetic when infection tracks up a tendon sheath.
Digital Dry demarcated localized gangrene w/ auto amputationDivision is through a healthy tissue.

Post operative care
- Control pain w/ opiate PCA or sciatic/femoral nerve infusional block. Careful attention to pressure area.
- Regular Physiotherapy to prevent muscle contracture/atrophy
- Early rehabilitation on temporary limb aid.
ComplicationsEarlyhemorrhage ,Hematoma ,abscess ,gas gangrene ,wound dehiscence ,ischemic flaps and fat embolism. Latepain ,sinus formation, osteomyelitis, Stump pain / phantom pain regular dose of
diazepam or combination. TENS ( transcutaneous nerve stimulation)
machine or sympathetic nerve block. If persistent exclude neuromata.

Thank you
Related Documents











