The Journal of Diabetic Foot Complications Open access publishing The Journal of Diabetic Foot Complications Open access publishing Diabetic Ankle Fracture with Distal Tibial and Fibular Varus Corrected Using the Ilizarov Methodology Authors: Sutpal Singh, DPM, FACFAS 1 , Chih-Hui (Jimmy) Tsai, DPM 2 , Albert Kim, DPM 3 Authors: Sutpal Singh, DPM, FACFAS The Journal of Diabetic Foot Complications, Volume 1, Issue 3, No. 2, © All rights reserved. The Journal of Diabetic Foot Complications, Volume 1, Issue 3, No. 2, © All rights reserved. Diabetic Ankle Fracture with Distal Tibial and Fibular Varus Corrected Using the Ilizarov Methodology 1 , Chih-Hui (Jimmy) Tsai, DPM 2 , Albert Kim, DPM 3 57 Abstract: The authors describe a case report of a patient with tibial and fibular fractures with a non- displaced intra-articular fracture that was initially treated in the emergency room unsuccessfully, resulting in a varus deformity. Corrective surgical treatment included the use of an external fixation device using the Ilizarov methodology for several months. After a two- year follow up, there was good alignment of fractured components and the patient is ambulating without any difficulty. The authors recommend reduction of these fractures using the Ilizarov methodology in diabetic patients who meet certain criteria rather than internal fixation. These criteria are discussed. Key words: Diabetes Mellitus, Tibial Fracture, Fibular Fracture, Diabetes with Peripheral Neuropathy and Peripheral Vascular Disease, Ilizarov Methodology Address for Correspondence: Sutpal Singh, DPM. FACFAS. Chief Ilizarov Surgical Instructor at Doctors Hospital West Covina, Fellow of the American College of Foot and Ankle Surgeons. Email: [email protected] 1 Chief Ilizarov Surgical Instructor at Doctors Hospital West Covina, Fellow of the American College of Foot and Ankle Surgeons. 2 Doctor of Podiatric Medicine (R2). Foot and Ankle Medicine and Surgery. Doctors Hospital of West Covina (PM&S-36) 3 Doctor of Podiatric Medicine (R1). Foot and Ankle Medicine and Surgery. Doctors Hospital of West Covina (PM&S-36) ntroduction In this paper, we present a case study of a diabetic patient with an intra-articular distal tibial and fibular fracture that underwent the Ilizarov method of fixation. Due to the complexity of diabetes mellitus, it is important when treating this group of patients to foresee possible complications that can happen and decide upon a course of action that is most beneficial to the patient perioperatively. Currently, the standard of practice for the intra-articular tibial and/or fibular fracture(s) is open reduction and internal fixation (ORIF). 1 However, there are instances, especially in diabetic patient, where performing ORIF is unfavorable. For example, contraindications for ORIF include severe comminution, osteoporosis, peripheral vascular disease, edema and significant soft tissue damage. In these cases, a good alternative to ORIF is using an external fixator. External fixation employing the Ilizarov Methodology has been used for many decades. The multiple advantages of this method include being relatively bloodless and minimally invasive, but disadvantages include a higher learning curve, pin track infection, as well as breakage of pins. In the present case, we believed our patient would benefit the most from circular fixation. In the following paragraphs, we will discuss our surgical approach, results, discussion, and conclusion of using circular frames for a diabetic patient with a long standing history of diabetes mellitus and peripheral vascular disease. I

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Journal of Diabetic Foot Complications Open access publishing The Journal of Diabetic Foot Complications Open access publishing
Diabetic Ankle Fracture with Distal Tibial and Fibular Varus Corrected Using the Ilizarov Methodology Authors: Sutpal Singh, DPM, FACFAS 1, Chih-Hui (Jimmy) Tsai, DPM 2, Albert Kim, DPM 3 Authors: Sutpal Singh, DPM, FACFAS The Journal of Diabetic Foot Complications, Volume 1, Issue 3, No. 2, © All rights reserved. The Journal of Diabetic Foot Complications, Volume 1, Issue 3, No. 2, © All rights reserved.
Diabetic Ankle Fracture with Distal Tibial and Fibular Varus Corrected Using the Ilizarov Methodology
1, Chih-Hui (Jimmy) Tsai, DPM 2, Albert Kim, DPM 3
57
Abstract: The authors describe a case report of a patient with tibial and fibular fractures with a non-displaced intra-articular fracture that was initially treated in the emergency room unsuccessfully, resulting in a varus deformity. Corrective surgical treatment included the use of an external fixation device using the Ilizarov methodology for several months. After a two-year follow up, there was good alignment of fractured components and the patient is ambulating without any difficulty. The authors recommend reduction of these fractures using the Ilizarov methodology in diabetic patients who meet certain criteria rather than internal fixation. These criteria are discussed. Key words: Diabetes Mellitus, Tibial Fracture, Fibular Fracture, Diabetes with Peripheral Neuropathy and Peripheral Vascular Disease, Ilizarov Methodology
Address for Correspondence: Sutpal Singh, DPM. FACFAS. Chief Ilizarov Surgical Instructor at Doctors Hospital West Covina, Fellow of the American College of Foot and Ankle Surgeons. Email: [email protected] 1 Chief Ilizarov Surgical Instructor at Doctors Hospital West Covina, Fellow of the American College of Foot and Ankle Surgeons. 2 Doctor of Podiatric Medicine (R2). Foot and Ankle Medicine and Surgery. Doctors Hospital of West Covina (PM&S-36) 3 Doctor of Podiatric Medicine (R1). Foot and Ankle Medicine and Surgery. Doctors Hospital of West Covina (PM&S-36)
ntroduction In this paper, we present a case study of a diabetic patient with an intra-articular distal
tibial and fibular fracture that underwent the Ilizarov method of fixation. Due to the complexity of diabetes mellitus, it is important when treating this group of patients to foresee possible complications that can happen and decide upon a course of action that is most beneficial to the patient perioperatively. Currently, the standard of practice for the intra-articular tibial and/or fibular fracture(s) is open reduction and internal fixation (ORIF).1 However, there are instances, especially in diabetic patient, where performing ORIF is unfavorable. For example, contraindications for ORIF include severe comminution, osteoporosis, peripheral vascular disease, edema and significant soft tissue damage. In these cases, a good alternative to ORIF is using an external fixator. External fixation employing the Ilizarov Methodology has been used for many decades. The multiple advantages of this method include being relatively bloodless and minimally invasive, but disadvantages include a higher learning curve, pin track infection, as well as breakage of pins. In the present case, we believed our patient would benefit the most from circular fixation. In the following paragraphs, we will discuss our surgical approach, results, discussion, and conclusion of using circular frames for a diabetic patient with a long standing history of diabetes mellitus and peripheral vascular disease.
I
The Journal of Diabetic Foot Complications Open access publishing
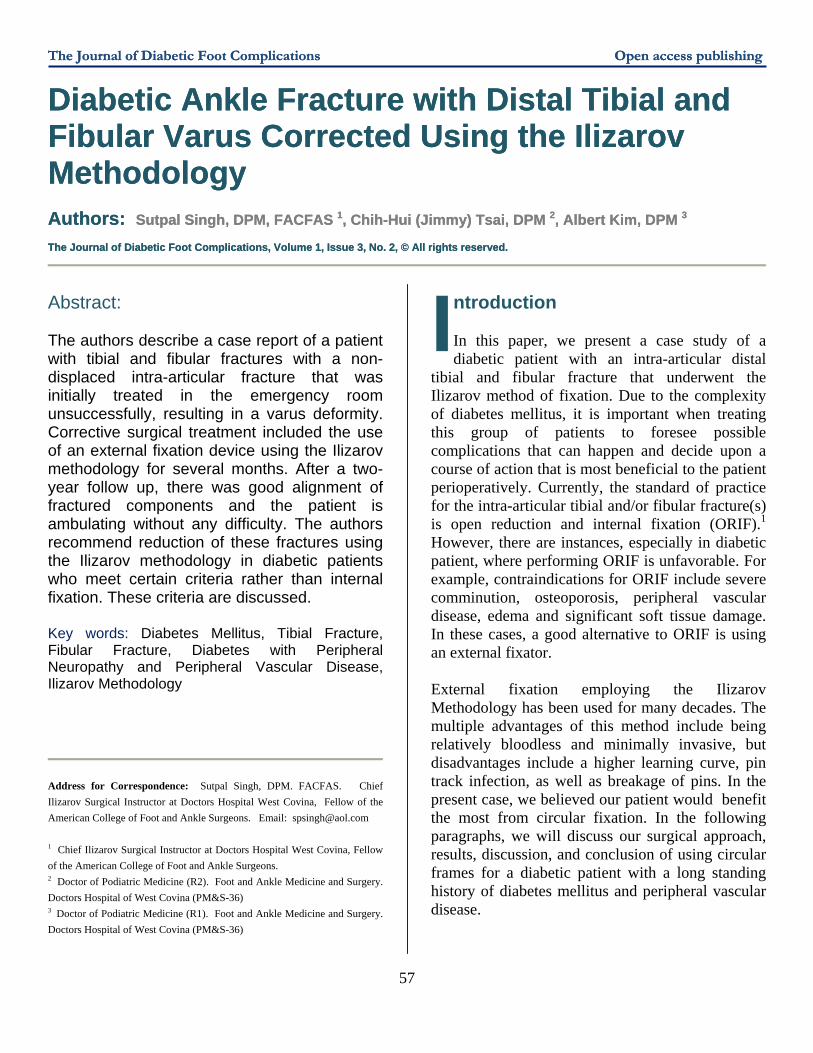
Figure 1 Distal Tibial Varus Ankle Fracture.
ase Report A trau
tibial and
62 year old diabetic male had a matic right ankle, intra-articular distal fibular fracture for several weeks
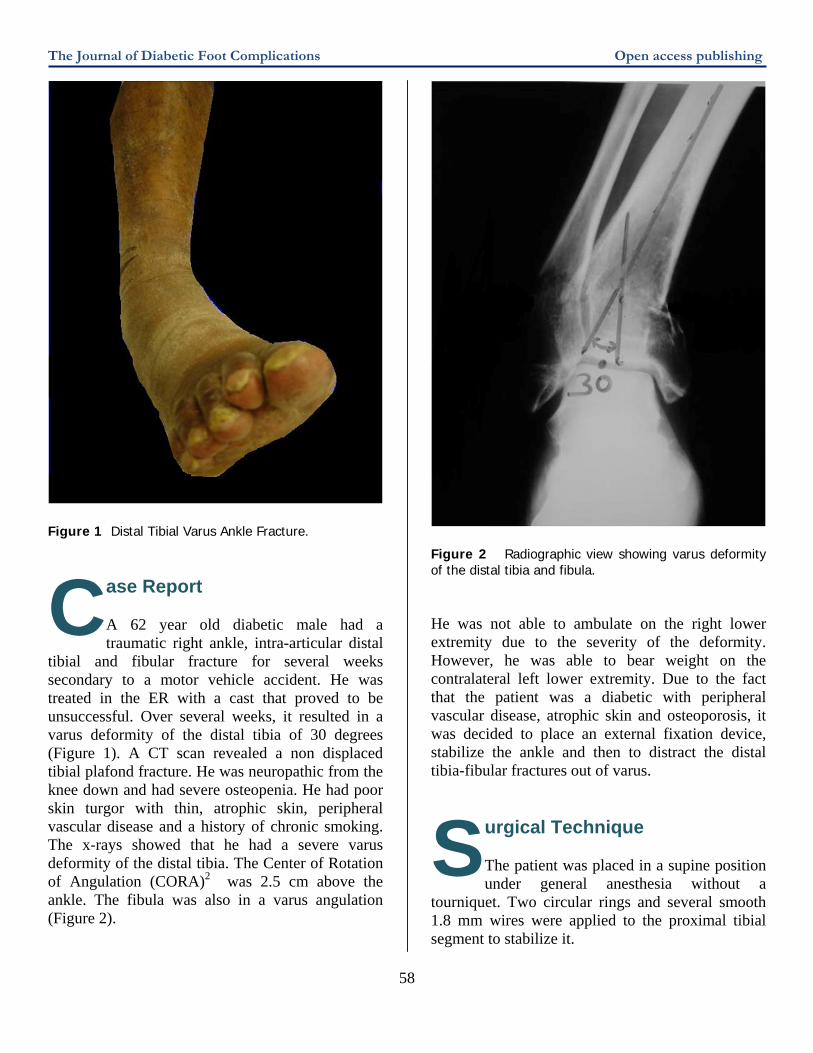
secondary to a motor vehicle accident. He was treated in the ER with a cast that proved to be unsuccessful. Over several weeks, it resulted in a varus deformity of the distal tibia of 30 degrees (Figure 1). A CT scan revealed a non displaced tibial plafond fracture. He was neuropathic from the knee down and had severe osteopenia. He had poor skin turgor with thin, atrophic skin, peripheral vascular disease and a history of chronic smoking. The x-rays showed that he had a severe varus deformity of the distal tibia. The Center of Rotation of Angulation (CORA)2 was 2.5 cm above the ankle. The fibula was also in a varus angulation (Figure 2).
Figure 2 Radiographic view showing varus deformity of the distal tibia and fibula. He was not able to ambulate on the right lower extremity due to the severity of the deformity. However, he was able to bear weight on the contralateral left lower extremity. Due to the fact that the patient was a diabetic with peripheral vascular disease, atrophic skin and osteoporosis, it was decided to place an external fixation device, stabilize the ankle and then to distract the distal tibia-fibular fractures out of varus.
urgical Technique The patient was placed in a supine position under general anesthesia without a
tourniquet. Two circular rings and several smooth 1.8 mm wires were applied to the proximal tibial segment to stabilize it.
C
S58
The Journal of Diabetic Foot Complications Open access publishing
59
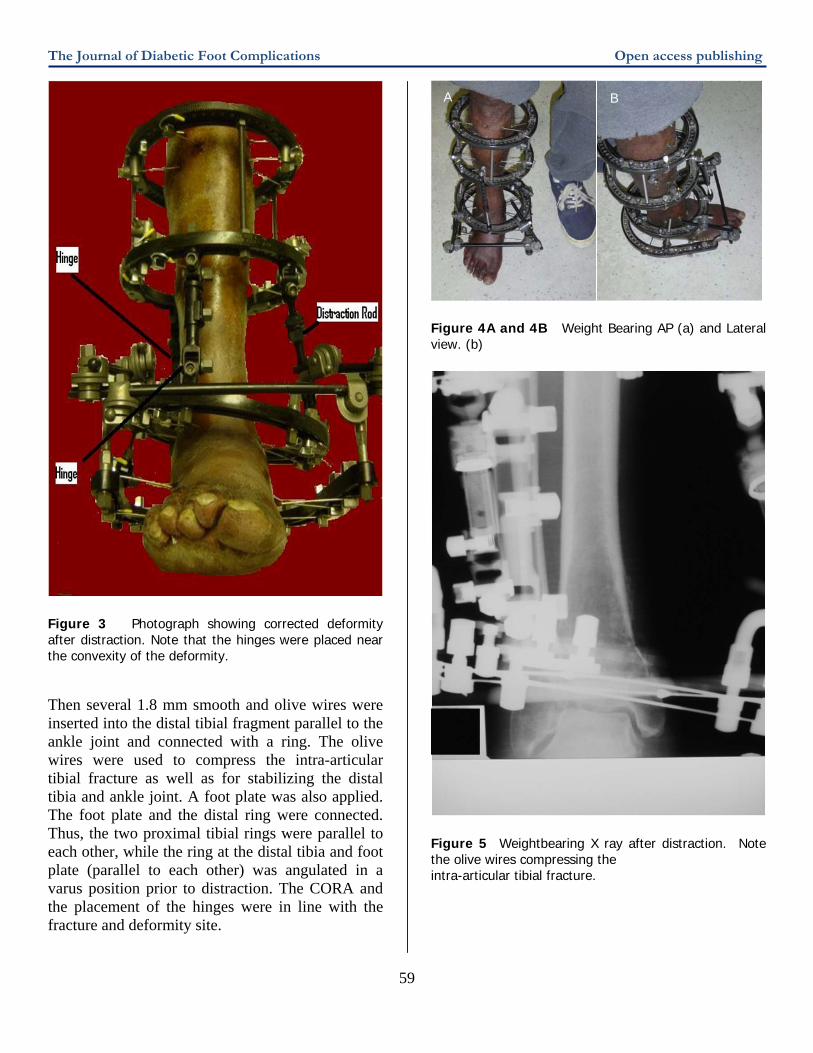
Figure 3 Photograph showing corrected deformity after distraction. Note that the hinges were placed near the convexity of the deformity. Then several 1.8 mm smooth and olive wires were inserted into the distal tibial fragment parallel to the ankle joint and connected with a ring. The olive wires were used to compress the intra-articular tibial fracture as well as for stabilizing the distal tibia and ankle joint. A foot plate was also applied. The foot plate and the distal ring were connected. Thus, the two proximal tibial rings were parallel to each other, while the ring at the distal tibia and foot plate (parallel to each other) was angulated in a varus position prior to distraction. The CORA and the placement of the hinges were in line with the fracture and deformity site.
A B
Figure 4A and 4B Weight Bearing AP (a) and Lateral view. (b)
Figure 5 Weightbearing X ray after distraction. Note the olive wires compressing the intra-articular tibial fracture.
The Journal of Diabetic Foot Complications Open access publishing
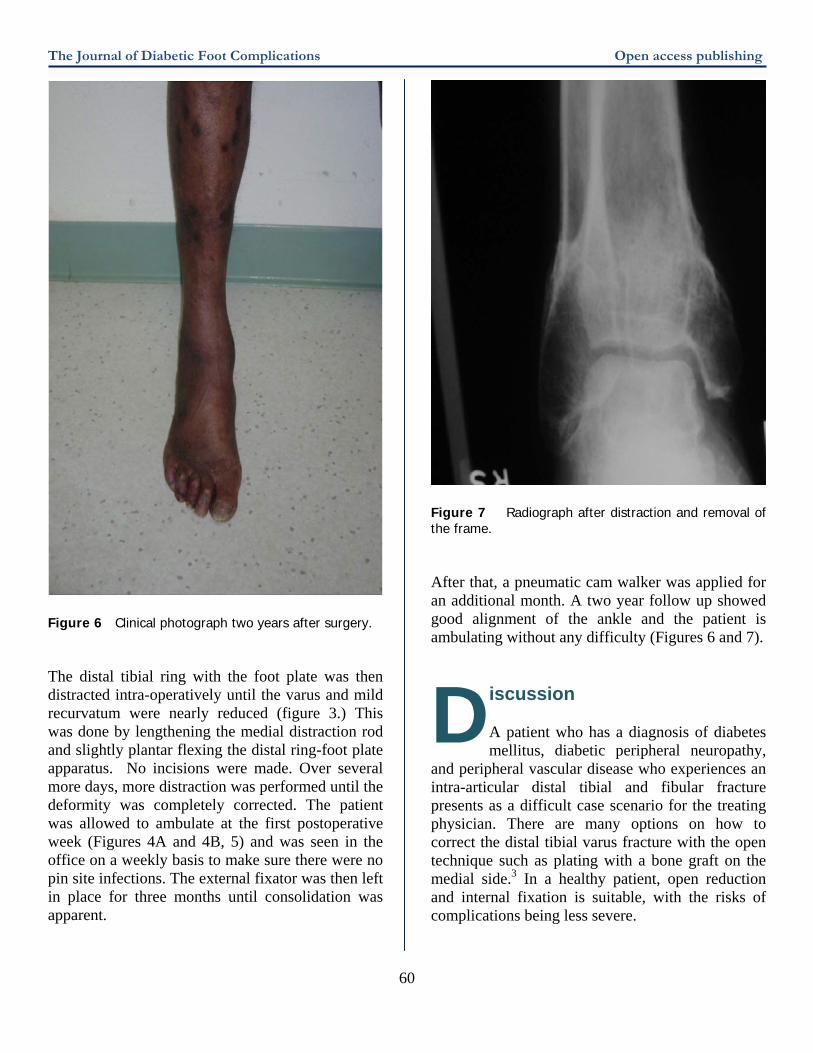
Figure 6 Clinical photograph two years after surgery. The distal tibial ring with the foot plate was then distracted intra-operatively until the varus and mild recurvatum were nearly reduced (figure 3.) This was done by lengthening the medial distraction rod and slightly plantar flexing the distal ring-foot plate apparatus. No incisions were made. Over several more days, more distraction was performed until the deformity was completely corrected. The patient was allowed to ambulate at the first postoperative week (Figures 4A and 4B, 5) and was seen in the office on a weekly basis to make sure there were no pin site infections. The external fixator was then left in place for three months until consolidation was apparent.
Figure 7 Radiograph after distraction and removal of the frame. After that, a pneumatic cam walker was applied for an additional month. A two year follow up showed good alignment of the ankle and the patient is ambulating without any difficulty (Figures 6 and 7).
iscussion A patient who has a diagnosis of diabetes mellitus, diabetic peripheral neuropathy,
and peripheral vascular disease who experiences an intra-articular distal tibial and fibular fracture presents as a difficult case scenario for the treating physician. There are many options on how to correct the distal tibial varus fracture with the open technique such as plating with a bone graft on the medial side.3 In a healthy patient, open reduction and internal fixation is suitable, with the risks of complications being less severe.
D
60

The Journal of Diabetic Foot Complications Open access publishing However, in a diabetic patient with peripheral vascular disease, osteopenia, and poor skin turgor, opening up the ankle may be detrimental. In the present case, the tibia and fibula were both very osteopenic and the patient had severe peripheral vascular disease, thin shinny atrophic skin and diabetes. Because of the osteopenia, the fracture fragments were malleable enough to allow for the distraction over several days. Severe complications were avoided by proper pin tract care and avoidance of any incisions. It is important to also note that the hinges were placed as close to the convexity of the deformity to prevent any over lengthening of the fractured fragments. In other words, as the hinges move further away from the convexity of the deformity, there is over distraction and lengthening of bones as the angular deformity is corrected. Complications in diabetic patients could include a compromise in wound healing, infections (superficial or deep), loss of fixation, and even amputations.4 In fact, the corrected deformity in the traditional open technique in neuropathic patients may enhance the development of Charcot arthropathy and severely compromise the limb.5 Thus, in a compromised diabetic patient with or without other co-morbidities, it is very important to preserve the periosteum and blood supply of the patient. In addition to good surgical technique, an even tighter control on blood glucose levels should decrease the risks for diabetic complications following surgery.6
61
onclusion In bloo
Ilizarov M
conclusion, a less invasive, minimal d loss type of surgery using the
ethodology mitigates the risk of complications in the high-risk diabetic patient with severe deformity.7 This type of surgery has its own inherent type of complications including, but not limited to pin/wire site infections, dehiscence, and breakage. Also, non-unions may arise if the distraction rate is too rapid. If that happens, the rate of distraction is slowed down; however, if the distraction rate is too slow, a resultant premature consolidation may arise. In this situation the patient will need to have the consolidated site re-fractured
in order to continue distraction osteogenesis.8 In a diabetic patient these risks and complications are increased.9 In order to reduce and minimize such risks it is recommended that such high-risk patients be monitored closely for glycemic control, operated on in such a way as to minimize tourniquet time, and to use the Ilizarov Method of fixation.10 It is also very important to have the patient followed every week to clean the skin and pin/wire site interface to prevent any type of infections that may arise. The Ilizarov Methodology coupled with good surgical technique and tight glycemic control is a beneficial and effective methodology in treating diabetic ankle fractures. Also, this allows for better healing while reducing the risk of infection in an effort to help preserve the limb and prevent serious complications.
eferences 1. Banks A, Downey M, Martin D, Miller S. McGlamry’s Comprehensive Textbook of Foot and
Ankle Surgery. Third Edition:1897-1926, 2001. 2. Paley, Dror. Osteotomy Concepts and Frontal Plane Realignment. Principles of Deformity Correction, Springer-Verlag Berlin Heidelberg, New York 2002: 99-104. 3. Hansen, Sigvard T. Functional Reconstruction of the Foot and Ankle. Lippincott Williams & Wilkins, 361-362, 2000. 4. Blotter RH, Connolly E, Wasan A, Chapman MW. Acute complications in the operative treatment of isolated ankle fractures in patients with diabetes mellitus. Foot Ankle Int. Nov;20(11):687-94, 1999. 5. Fishco W. Surgically Induced Charcot’s Foot. Journal of the American Podiatric Medical Association Volume 91 Number 8 388-393, 2001. 6. McMahon MM, Bistrian BR. Host defenses and susceptibility to infection in patients with diabetes mellitus. Infect Dis Clin North Am 9:1–9, 1995. 7. DiDomenico L, Brown D, Zgonis T. The Use of Ilizarov Technique as a Definitive Percutaneous Reduction for Ankle Fractures in Patients Who Have Diabetes Mellitus and Peripheral Vascular Disease. Clinics in Podiatric Medicine and Surgery Volume 26, Issue 1, January 2009, Pages 141-148, 2009. 8. Catagni, M.A. Treatment of Tibial Nonunions. Treatment of Fractures, Nonunions and Bone Loss of the Tibia with the Ilizarov Method. Smith and Nephew INC. 97-103, 1998.
C
R

The Journal of Diabetic Foot Complications Open access publishing 9. Wukich DK, Belczyk RJ, Burns PR, Frykberg RG. Complications encountered with circular ring fixation in persons with diabetes mellitus. Foot Ankle Int. 2008 Oct;29(10):994-1000, 2008. 10. Rogers L, Bevilacqua N, Frykberg R, Armstrong D. Predictors of Postoperative Complications of Ilizarov External Ring Fixators in the Foot and Ankle. The Journal of Foot & Ankle Surgery 46(5):372–375, 2007.
62
Related Documents











