[email protected] 3. Kölner Kardio-Diabetes Symposium 27. September 2012 Diabetes und Herzinsuffizienz die Sicht des Kardiologen 1. Epidemiologie 2. Diabe=sche Kardiomyopathie 3. Therapie des Diabetes 4. Therapie der Herzinsuffizienz 5. Guidelines 6. Fazit

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

3. Kölner Kardio-Diabetes Symposium 27. September 2012
Diabetes und Herzinsuffizienz die Sicht des Kardiologen
1. Epidemiologie 2. Diabe=sche Kardiomyopathie 3. Therapie des Diabetes 4. Therapie der Herzinsuffizienz 5. Guidelines 6. Fazit
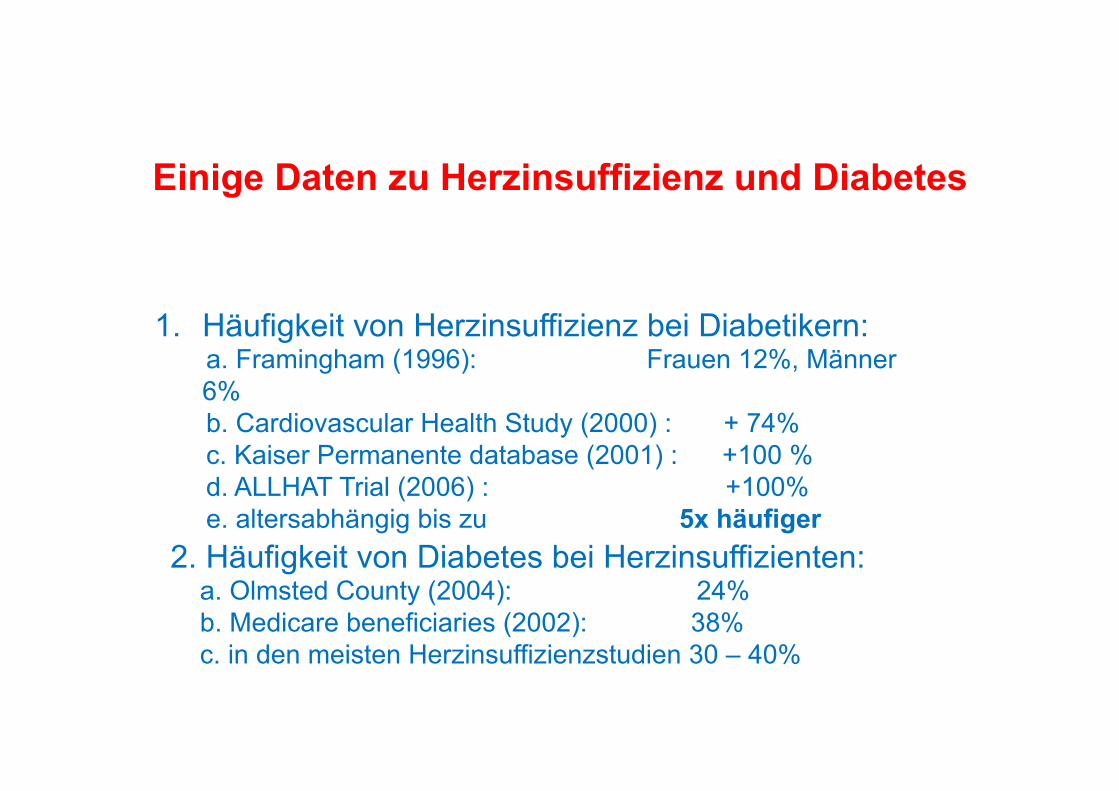
Einige Daten zu Herzinsuffizienz und Diabetes
1. Häufigkeit von Herzinsuffizienz bei Diabetikern: a. Framingham (1996): Frauen 12%, Männer
6% b. Cardiovascular Health Study (2000) : + 74% c. Kaiser Permanente database (2001) : +100 % d. ALLHAT Trial (2006) : +100% e. altersabhängig bis zu 5x häufiger 2. Häufigkeit von Diabetes bei Herzinsuffizienten:
a. Olmsted County (2004): 24% b. Medicare beneficiaries (2002): 38% c. in den meisten Herzinsuffizienzstudien 30 – 40%

1. Diabetiker haben häufiger Hypertonie, Lipidstoffwechselstörungen und Übergewicht dies führt zur koronaren Herzkrankheit 2. . Diabetes verursacht Anomalien der kardialen Struktur und Funktion mit Myozytenhypertrophie, interstitieller Fibrose und small vessel disease dies führt zu Herzinsuffizienz (mit erhaltener oder verminderter EF)
Der „typische“ Pa=ent mit Diabetes Typ 2
ist >65, hat BMI >30 und in der Regel bereits kardiovaskuläre „Probleme“
30 -‐ 40% haben eine Herzinsuffizienz 12%/Jahr werden herzinsuffizient
>60% haben eine KHK
Diabetes mellitus Herzinsuffizienz
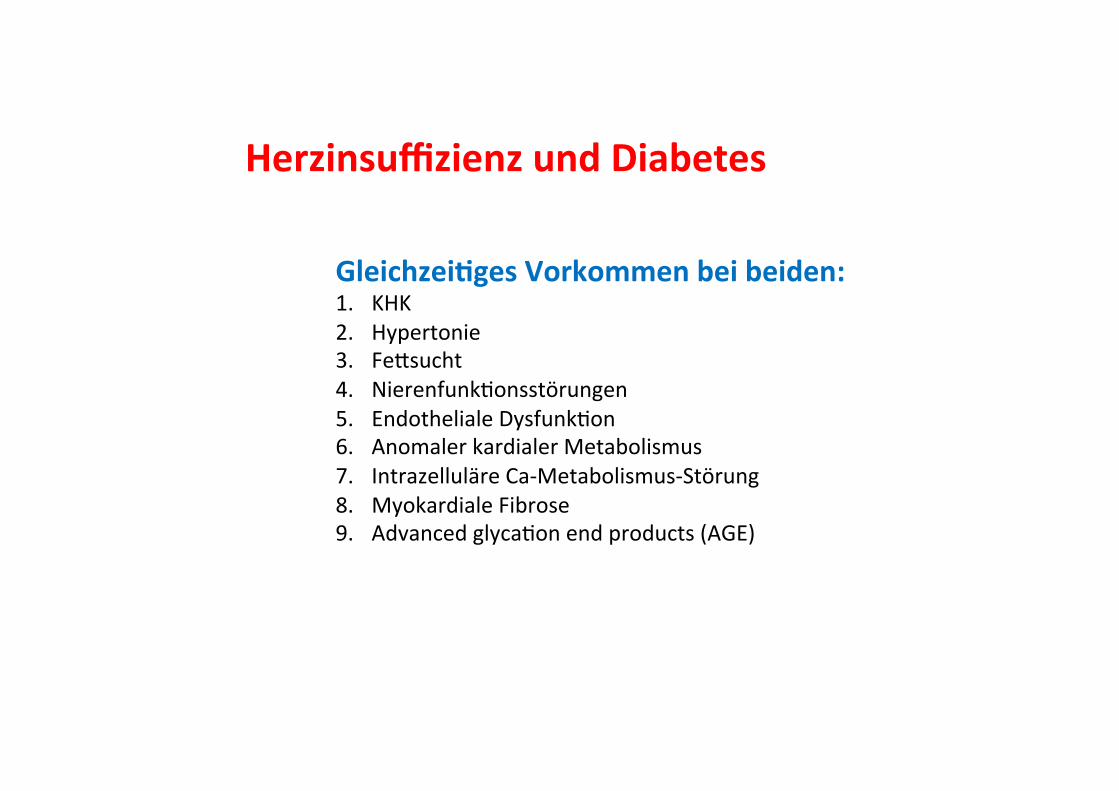
Herzinsuffizienz und Diabetes
Gleichzei=ges Vorkommen bei beiden: 1. KHK 2. Hypertonie 3. FeQsucht 4. NierenfunkUonsstörungen 5. Endotheliale DysfunkUon 6. Anomaler kardialer Metabolismus 7. Intrazelluläre Ca-‐Metabolismus-‐Störung 8. Myokardiale Fibrose 9. Advanced glycaUon end products (AGE)

Known diabetes 29.4 % 65.4 IGT or IFG 20.0 % 69.6 Newly diagnosed DM 15.9 % 72.6 No diabetes 34.7 % 58.3
(22 German Cardiac Centers, 750 patients undergoing cardiac catheterisation)
significant CAD (%)
Schöndorf, Lübben, Karagiannis, Erdmann, Forst, Pfützner Diabetes & Vascular Disease Research 7 (2010) 145–150

Faktoren, die das AuNreten einer Herzinsuffizienz bei Diabe=kern begüns=gen:
1. Höheres Alter (Steifigkeitszunahme) 2. Längere Diabetesdauer 3. Insulintherapie 4. Ischämische Herzkrankheit 5. pAVK 6. Erhöhtes Krea=nin 7. Mikroalbuminurie 8. Schlechte Blutzuckereinstellung
Defini=on der diabe=schen Kardiomyopathie (1):
1. Rubler beschrieb 1970 erstmals vier Pa=enten mit Diabetes und Herzinsuffizienz bei normalen Koronarien (!)
2. Heute definiert man sie als ventrikuläre Dysfunk=on (LVEDP >12) nach Ausschluß einer KHK aber mit diastolischer Funk=onsstörung
Rubler et al., New type of cardiomyopathy associated with diabeUc glomerulosclerosis. Am J Cardiol. 1972;30:595– 602.
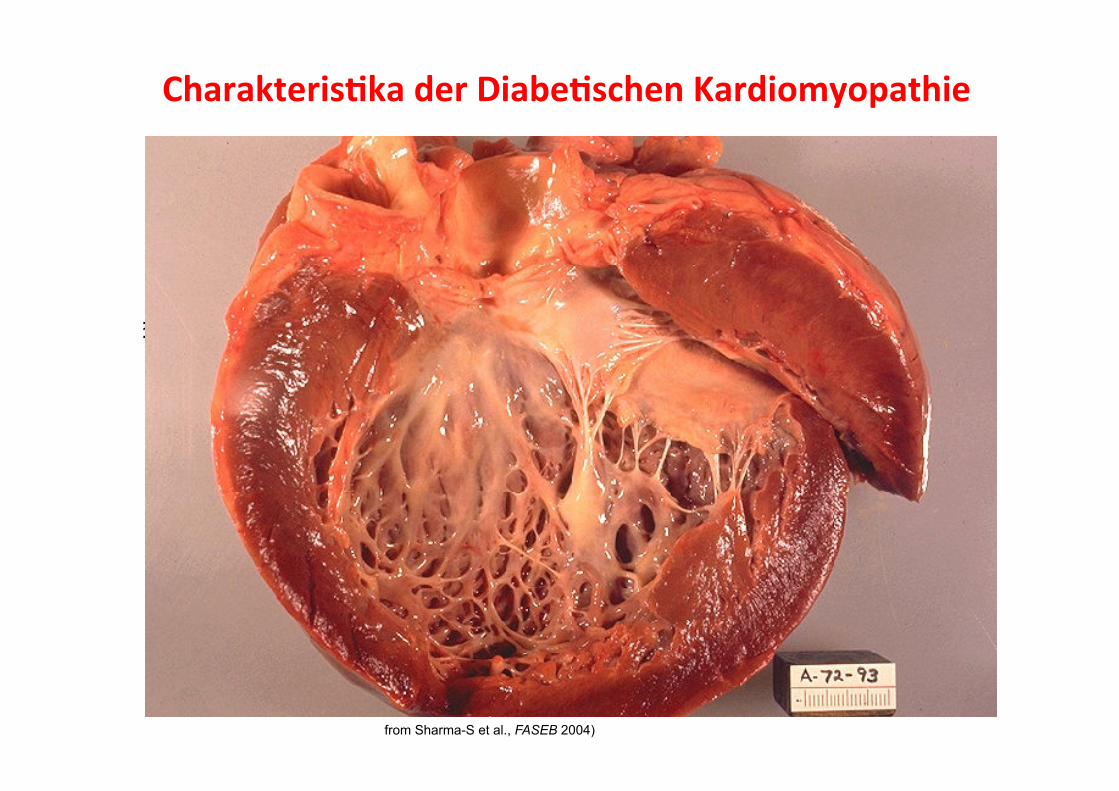
Charakteris=ka der Diabe=schen Kardiomyopathie
Myokardhypertophie
(Fujita-M et al., Int J Cardiol 2007)
Kardiale Fibrose
(Konduracka-E et al., Eur Heart J 2007)
+ Cardiac insulin resistance
Metabolische Veränderungen
from Sharma-S et al., FASEB 2004)

1. Impaired Calcium homeostasis 2. Upregula=on of the RAAS 3. Incresaed oxida=ve stress 4. Altered substrate metabolism 5. Mitochondrial dysfunc=on
Boudina et al., CirculaUon 2007;115:3213

Heart Failure and Mortality in the Elderly with Diabetes
0.00
0.50
0.75
Proportion Surviving
0 1 2 3 4 5
Diabetes without Heart Failure (n=69 083)
Diabetes with Incident Heart Failure (n=46 720) 0,25 0.20
(Bertoni et al., Diabetes Care 2004; 27:699)
1.00
Mortality was 80% after 3 years
years
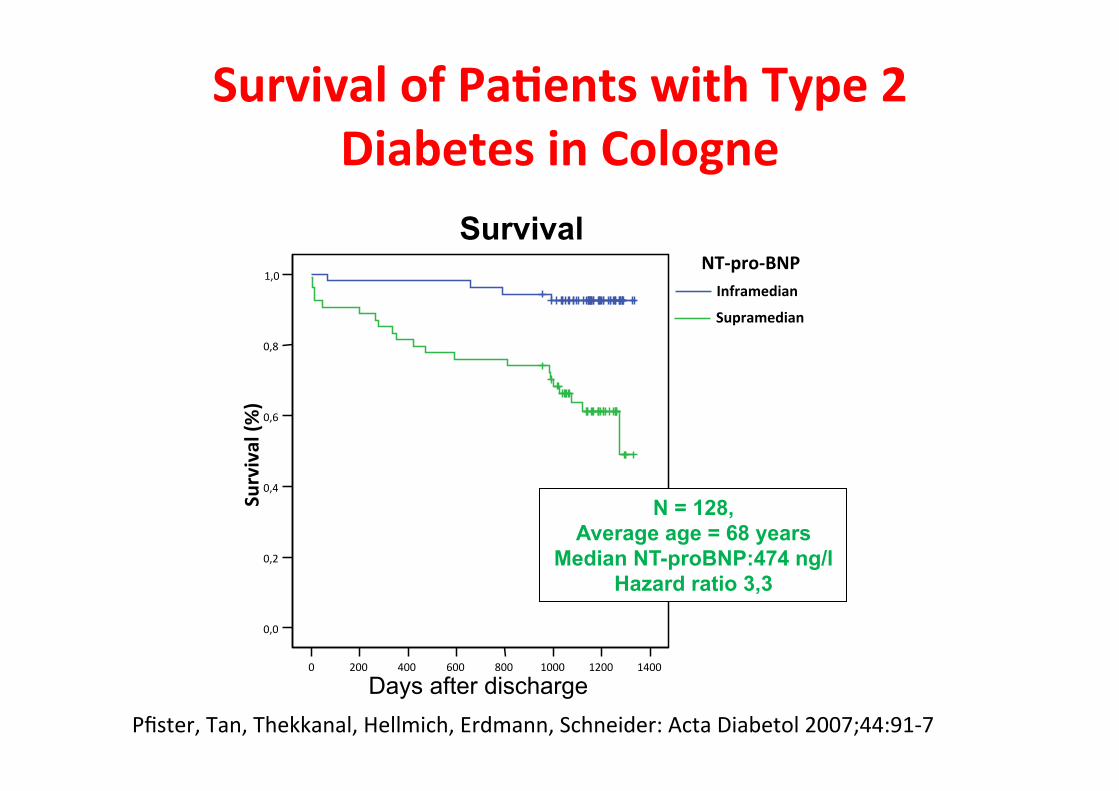
Survival of Pa=ents with Type 2 Diabetes in Cologne
P<0.001
Pfister , Schneider et al., Acta Diabetologia 2007; 44: 91-97
Days after discharge 0 200 400 600 800 1000 1200 1400
0,0
0,2
0,4
0,6
0,8
1,0 Survival (%
) NT-‐pro-‐BNP Inframedian Supramedian
Survival
N = 128, Average age = 68 years
Median NT-proBNP:474 ng/l Hazard ratio 3,3
Pfister, Tan, Thekkanal, Hellmich, Erdmann, Schneider: Acta Diabetol 2007;44:91-‐7

UKPDS: 16% increase of HF incidence per 1% HbA1c
worse glycemic control, as indicated by either fas=ng glucose or HbA1c levels, is associated with increased risk for the development of HF ! Frage: nimmt die Herzinsuffizienzmortalität ab, wenn der Diabetes sehr gut eingestellt wird?

Rela=onship of Hemoglobin A1C and Mortality in Heart Failure Pa=ents With Diabetes
Aguilar D et al. J Am Coll Cardiol 2009;54:422–8
n = 5.815 FU 2 Jahre
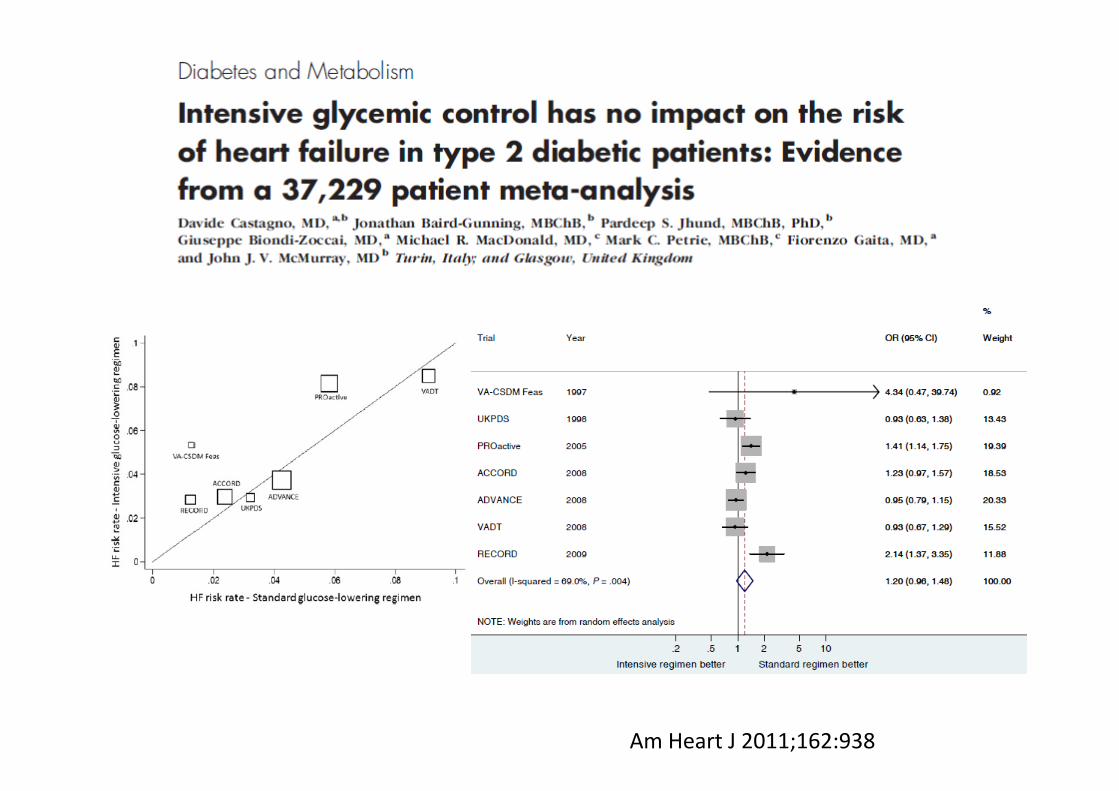
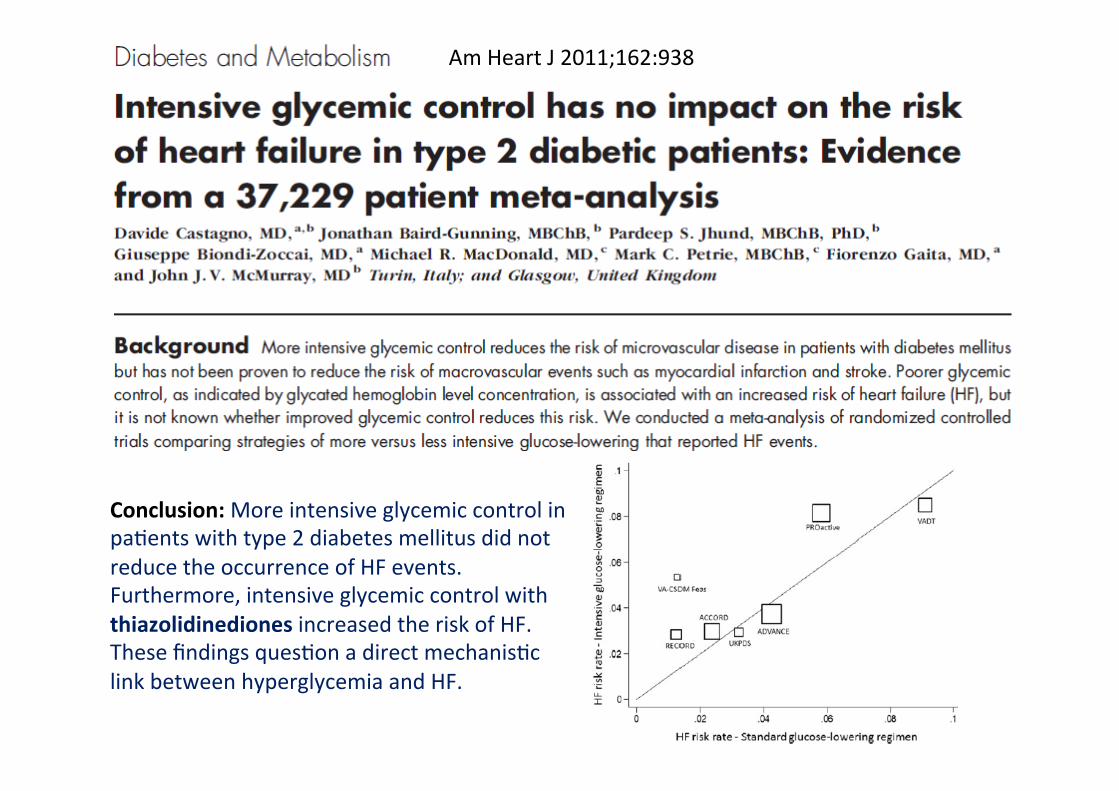
Am Heart J 2011;162:938
Am Heart J 2011;162:938
Conclusion: More intensive glycemic control in paUents with type 2 diabetes mellitus did not reduce the occurrence of HF events. Furthermore, intensive glycemic control with thiazolidinediones increased the risk of HF. These findings quesUon a direct mechanisUc link between hyperglycemia and HF.
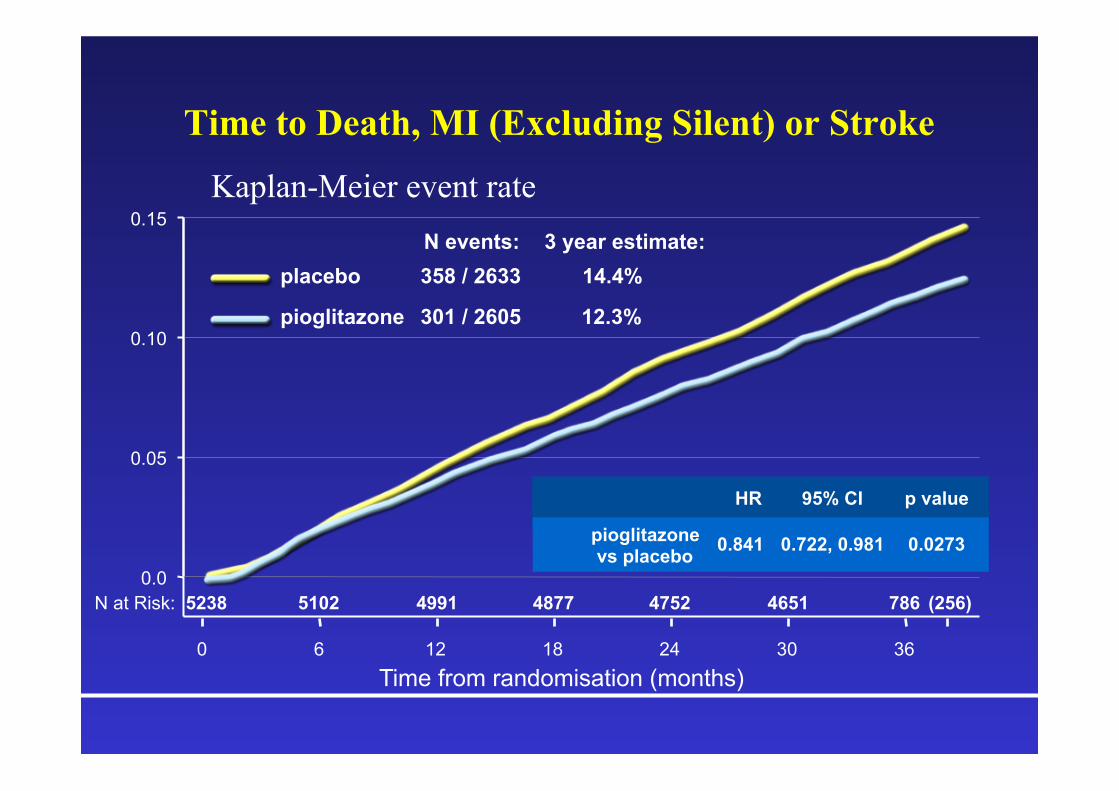
Time to Death, MI (Excluding Silent) or Stroke
Kaplan-Meier event rate
N at Risk: 5238 5102 4991 4877 4752 4651 786 (256)
Time from randomisation (months) 0 6 12 18 24 30 36
0.0
0.05
0.10
0.15
pioglitazone
placebo N events:
301 / 2605
358 / 2633 3 year estimate:
12.3%
14.4%
HR 95% CI p value
pioglitazone vs placebo 0.841 0.722, 0.981 0.0273

Lincoff et al., JAMA 2007;298:1180–1188.
Risk of serious HF with pioglitazone: data from the Lincoff meta-analysis
Weeks 0 20 40 60 80 100 120
0
4
8
10
Est
imat
ed e
vent
rate
(%)
140
2
6
HR 95% CI p value pioglitazone vs control 1.41 1.14, 1.76 0.002
0
4
8
10
2
6
Pioglitazone
Control
(n = 16.390)
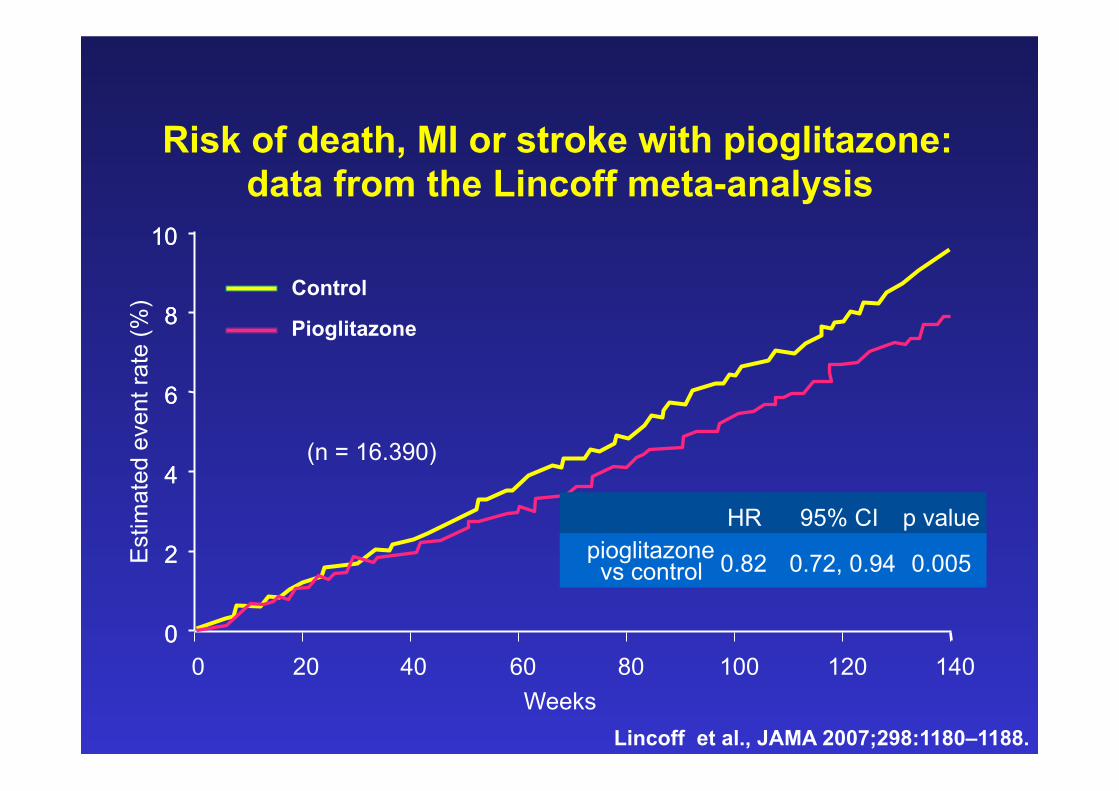
Lincoff et al., JAMA 2007;298:1180–1188. Weeks
0 20 40 60 80 100 120 0
4
8
10
Est
imat
ed e
vent
rate
(%)
140
2
6
0
4
8
10
2
6
Pioglitazone
Control
(n = 16.390)
Risk of death, MI or stroke with pioglitazone: data from the Lincoff meta-analysis
HR 95% CI p value pioglitazone vs control 0.82 0.72, 0.94 0.005
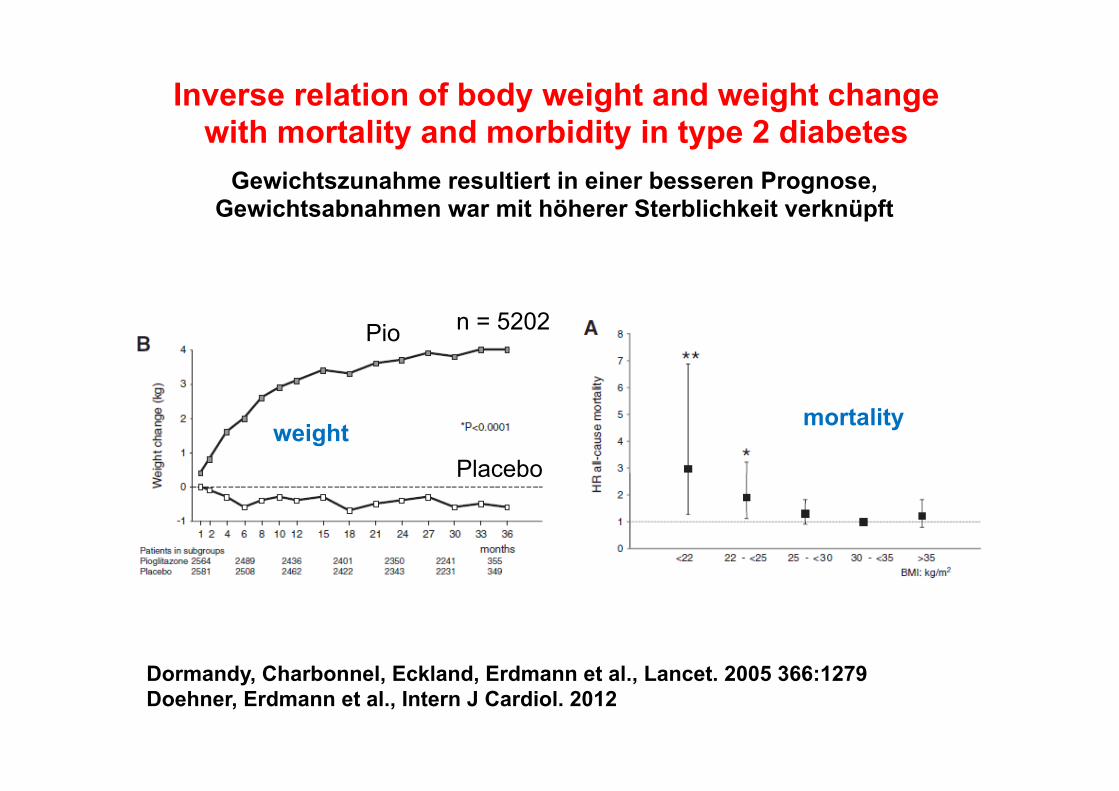
Inverse relation of body weight and weight change with mortality and morbidity in type 2 diabetes
Dormandy, Charbonnel, Eckland, Erdmann et al., Lancet. 2005 366:1279 Doehner, Erdmann et al., Intern J Cardiol. 2012
n = 5202
weight mortality
Gewichtszunahme resultiert in einer besseren Prognose, Gewichtsabnahmen war mit höherer Sterblichkeit verknüpft
Pio
Placebo

OAD insulin

„In trials to date of pa=ents with type 2 diabetes, =ght glycemic control with currently available diabe=c therapy does not appear to decrease the risk of incident HF.”
Aguilar D., Amer Heart J. 2011;162:795

Rela=onship of Walking to Mortality Among 2896 Adults with Diabetes
those, who walked at least 2 hrs/week had a 39% lower mortality
Gregg et al., Arch Intern Med 2003; 163:1440
HS

20.8%
26.1%
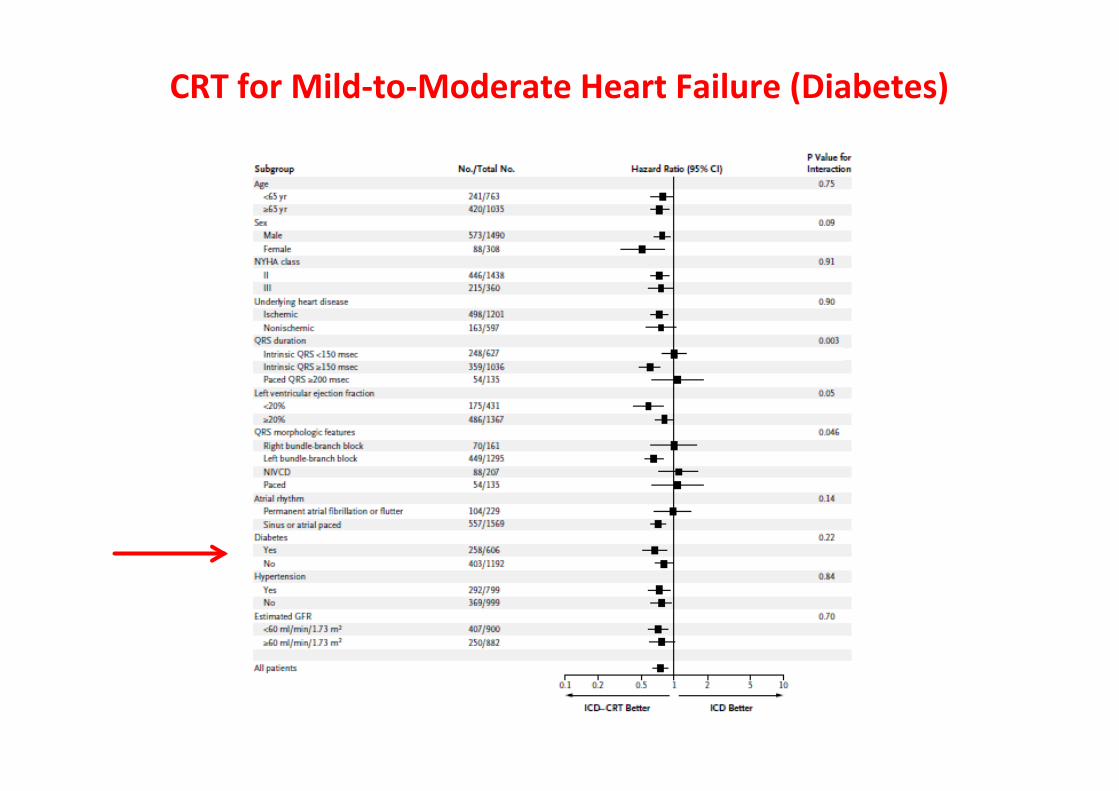
CRT for Mild-‐to-‐Moderate Heart Failure (Diabetes)
Beta-‐blockers are not contraindicated in diabetes and are as effec=ve in improving outcome in diabe=c pa=ents as in non-‐diabe=c individuals. Thiazolidinediones (glitazones) cause sodium and water reten=on and increased risk of worsening HF and hospitaliza=on, and should be avoided. Meoormin is not recommended in pa=ents with severe renal or hepa=c impairment because of the risk of lac=c acidosis, but is widely (and apparently safely) used in other pa=ents with HF. The safety of newer an=diabe=c drugs in HF is unknown.
European Heart Journal (2012) 33, 1787–1847
Diabetes

1. Herzinsuffizienz + Diabetes sind häufig 2. Die Prognose ist sehr schlecht 3. Keine spezifische Therapie 4. Herzinsuffizienz: nach Guidelines 5. Diabetes: A1c um 7 – 8 % 6. CRT (auch bei milder Herzinsuffizienz)
Diabetes und Herzinsuffizienz aus der Sicht des Kardiologen
Zusammenfassung

Danke für die Aufmerksamkeit!
Related Documents











