SOEPEL Diabetes mellitus type II Abdul Waris Khan Dept: Internal medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SOEPEL
Diabetes mellitus type II
Abdul Waris Khan
Dept: Internal medicine

SOEPEL
• Subjective: A 48 years old female presented to ER with blurring of vision and numbness in the feet and legs.
• H/O presenting illness: she is known to be diabetic for 15 years and the glycaemic control is poor.

• Objective: physical exam
• Evaluation: Complication of DM, MS
• Plan: CBC, FBG, HbA1c, OGTT
• Elaboration: management of DM & complications
• Learning goals: Complications of DM type-II
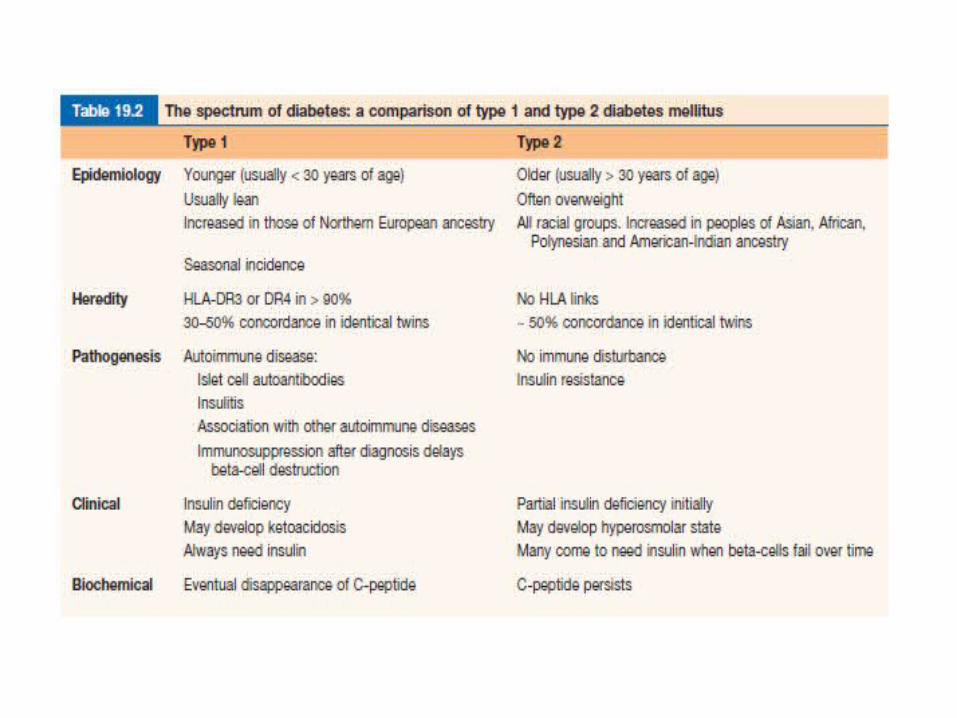
Definition
• Type 2 diabetes mellitus (NIDDM) consists of an array of dysfunctions characterized by hyperglycemia and resulting from the combination of resistance to insulin action and/or inadequate insulin secretion.

Epidemiology • Type 2 diabetes is relatively common in all populations enjoying an
affluent lifestyle.
• The four major determinants are:– increasing age, – obesity, – ethnicity – family history.
• In poor countries diabetes is a disease of the rich, but in rich countries it is a disease of the poor, obesity being the common factor.
• 25–50% of patients already have some evidence of vascular complications at the time of diagnosis.
• The onset may be accelerated by the stress of pregnancy, drug treatment or coexisting illness.
• The overall prevalence within the UK is 2–3%, and the lifetime risk is around 15%.
• Type 2 diabetes is 2–4 times as prevalent in people of South Asian, African and Caribbean ancestry who live in the UK.
• Obesity increases the risk of type 2 diabetes 80–100 fold.
• Type 2 diabetes is associated with central obesity, hypertension, hypertriglyceridemia, a decreased HDL cholesterol.
• Insulin resistance is strongly associated with many of these variables, as is increased cardiovascular risk

Aetiology • Exact cause is unknown, but following maybe responsible:-
• Genetics:– Identical twins of NIDDM have almost 100% chance of developing diabetes.
About 25% of patients have first degree relative with NIDDM
• Environmental factors: – lifestyle, overeating when specially combined with obesity acts as diabetogenic
factor (increasing resistance to action of insulin)
• Pancreatic pathology: – Reduction of insulin secretion cells– Resistance to insulin action– delayed insulin secretion in response to oral glucose

Clinical features
• Most patients are asymptomatic
• May present with lethargy, delayed wound healing, visual blurring, infections pruritus vulvae or balanitis.
• Complications may be the first presenting feature: – Infections– Deterioration of vision

Investigations
Complications
• The major cause of death in treated patients is due to cardiovascular problems (70%) followed by renal failure (10%) and infections (6%).
• The duration and degree of hyperglycaemia play a major role in the production of complications.
Complications of DM
Macrovascular
Macrovascular
• The central pathological mechanism in macrovascular disease is the process of atherosclerosis, which leads to narrowing of arterial walls throughout the body. – Stroke– Coronary artery disease– Peripheral vascular disease

Microvascular
• Small blood vessels throughout the body are affected but the disease process is of particular danger in three sites:
• Retina• Renal glomerulus• Nerve sheaths.

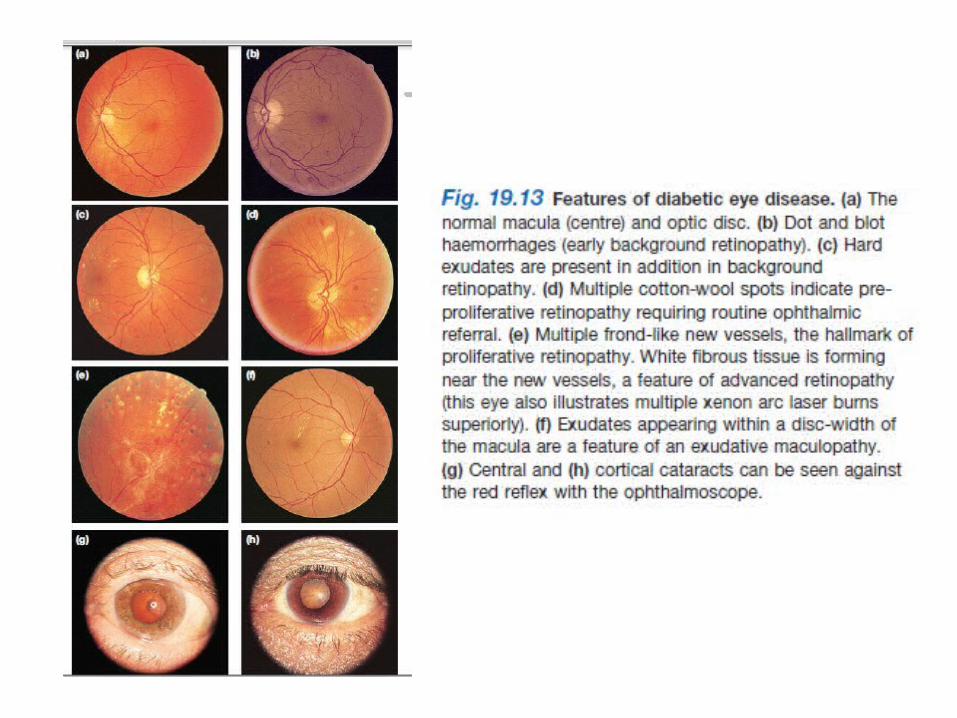
Retinopathy
• Diabetic retinopathy increases with the length of diabetes, 20% will have retinal changes after 10 years, rising to 80% after 20 years.
• In type 2 diabetes the progression is much slower and initially in the macular and paramacular region. These changes are associated with macular oedema and consequent loss of vision.

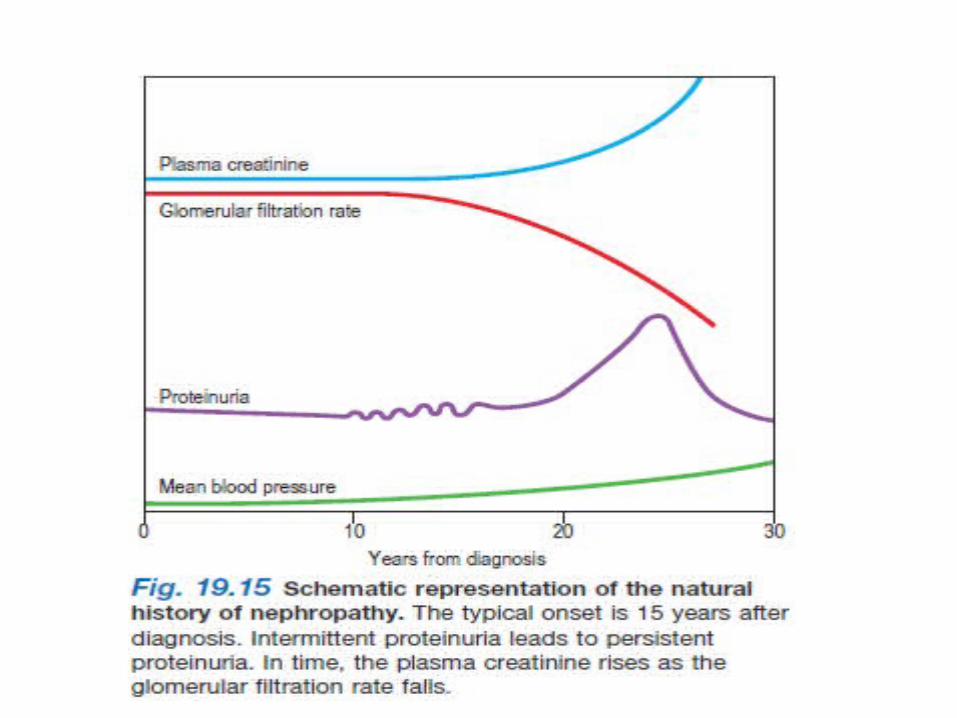
Nephropathy
• Clinical nephropathy secondary to glomerular disease usually manifests 15–25 years after diagnosis of diabetes and affects 25–35% of patients diagnosed under the age of 30 years. It is the leading cause of premature death in young diabetic patients.
The earliest functional abnormality in the diabetic kidney is renal hypertrophy associated with a raised GFR and is related to poor glycaemic control.
As the kidney becomes damaged by diabetes, the afferent arteriole (leading to the glomerulus) becomes vasodilated to a greater extent than the efferent glomerular arteriole. This increases the intraglomerular filtration pressure, further damaging the glomerular capillaries and leading to mesangial cell hypertrophy.
This process eventually leads to glomerular sclerosis. The initial structural lesion in the glomerulus is thickening of the basement membrane. Associated changes result in disruption of the protein cross-linkages which normally make the membrane an effective filter.
In consequence, there is a progressive leak of large molecules (particularly protein) into the urine.
Neuropathy • Diabetes can damage peripheral nervous tissue in a number of ways.
The vascular hypothesis postulates occlusion of the vasa nervorum as the prime cause. Since hyperglycaemia leads to increased formation of sorbitol and fructose in Schwann cells, accumulation of these sugars may disrupt function and structure.
• The earliest functional change in diabetic nerves is delayed nerve conduction velocity; the earliest histological change is segmental demyelination, caused by damage to Schwann cells.
• In the early stages axons are preserved, implying prospects of recovery, but at a later stage irreversible axonal degeneration develops.

• The following varieties of neuropathy occur:
• Symmetrical mainly sensory polyneuropathy (distal)
• Acute painful neuropathy
• Mononeuropathy and mononeuritis multiplex• (a) cranial nerve lesions• (b) isolated peripheral nerve lesions
• Diabetic amyotrophy (asymmetrical motor diabetic neuropathy).
• Autonomic neuropathy.
Symmetrical mainly sensory polyneuropathy
• This is often unrecognized by the patient in its early stages.
• Early clinical signs are loss of vibration sense, pain sensation and temperature sensation in the feet.
• • At later stages patients may complain of a feeling of
‘walking on cotton wool’ and can lose their balance when washing the face or walking in the dark owing to impaired proprioception.
Acute painful neuropathy• A diffuse, painful neuropathy is less common.
• The patient describes burning or crawling pains in the feet, shins and anterior thighs.
• These symptoms are typically worse at night, and pressure from bedclothes may be intolerable.
• It may present at diagnosis .
• It usually remits spontaneously after 3–12 months if good glycemic control is maintained.
Mononeuritis and mononeuritis multiplex(multiple mononeuropathy)
• Any nerve in the body can be involved in diabetic mononeuritis; the onset is typically abrupt and sometimes painful.
• Isolated palsies of nerves to the external eye muscles, especially the third and sixth nerves, are more common in diabetes.
• Full spontaneous recovery is the rule for most episodes of mononeuritis over 3–6 months
Diabetic amyotrophy
• This condition is usually seen in older men with diabetes. Presentation is with painful wasting, usually asymmetrical, of the quadriceps muscles or occasionally in the shoulders.
• The affected area is often extremely tender.
• Diabetic amyotrophy is usually associated with periods of poor glycaemic control and may be present at diagnosis.
• It often resolves in time with careful metabolic control of the diabetes.

Autonomic neuropathy
• Asymptomatic autonomic disturbances can be demonstrated on laboratory testing in many patients, but symptomatic autonomic neuropathy is rare. It affects both the sympathetic and parasympathetic nervous systems and can cause disabling postural hypotension.– Cardiovascular system– GIT system– Bladder involvement– Male Erectile dysfunction
References
• Kumar and Clarks clinical medicine 7th edition• Emedicine.medscape.com
Related Documents
![Clinical Effectiveness and Safety of Analog Glargine in Type 1 … · Type 1 Diabetes Mellitus[Text Word]) OR Sudden-Onset Diabetes Mellitus[Text Word]) OR Diabetes Mellitus, Type](https://static.cupdf.com/doc/110x72/60169f288f8b186d1345140c/clinical-effectiveness-and-safety-of-analog-glargine-in-type-1-type-1-diabetes-mellitustext.jpg)










