Diabetes Mellitus Type 1 Gary Strokosch, MD Region V Medical Specialist Type 2 Drew Alexander, MD Region IV Medical Specialist November 4, 2013

Diabetes Mellitus Type 1 Gary Strokosch, MD Region V Medical Specialist Type 2 Drew Alexander, MD Region IV Medical Specialist November 4, 2013.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Diabetes MellitusType 1
Gary Strokosch, MD
Region V Medical Specialist
Type 2
Drew Alexander, MD
Region IV Medical Specialist
November 4, 2013
Two Main Types of Diabetes
• Type 1: formerly known as insulin-dependent diabetes mellitus (IDDM) or juvenile onset diabetes
• Type 2: formerly known as non-insulin-dependent diabetes mellitus (NIDDM) or adult onset diabetes
Type 1 Diabetes
• Type 1 accounts for only 10% of all cases of diabetes, but demands daily treatment with insulin.
• Type 1 alarms new patients with a variety of symptoms during a brief latency period.
Diagnosis• A diagnosis of diabetes is made if the fasting
glucose is >125 mg/dL, or if a 2-hour GTT results in a glucose >200 mg/dL.
• However, one abnormal glucose value is all that is needed in a patient with classical symptoms of diabetes, such as polyuria or polydipsia.
• A HgA1C ≥6.5% was added in 2010.• The diagnosis of diabetes should never be
made on the basis of glucose in the urine (glycosuria).
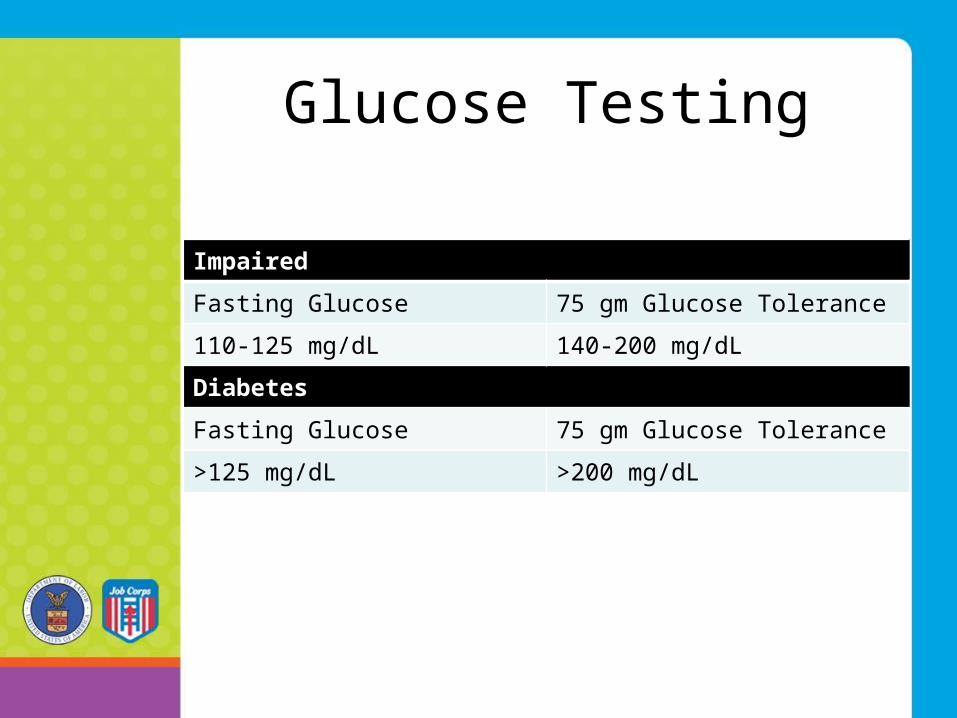
Glucose Testing
Impaired
Fasting Glucose 75 gm Glucose Tolerance
110-125 mg/dL 140-200 mg/dL
Diabetes
Fasting Glucose 75 gm Glucose Tolerance
>125 mg/dL >200 mg/dL
Glucohemoglobin
• HbA1C is a measure of integrated glucose control over the preceding 2-3 months and reflects the average life of a red blood cell.
• Glucose becomes attached to hemoglobin in a non-enzymatic fashion that is dependent on the average concentration of blood glucose.
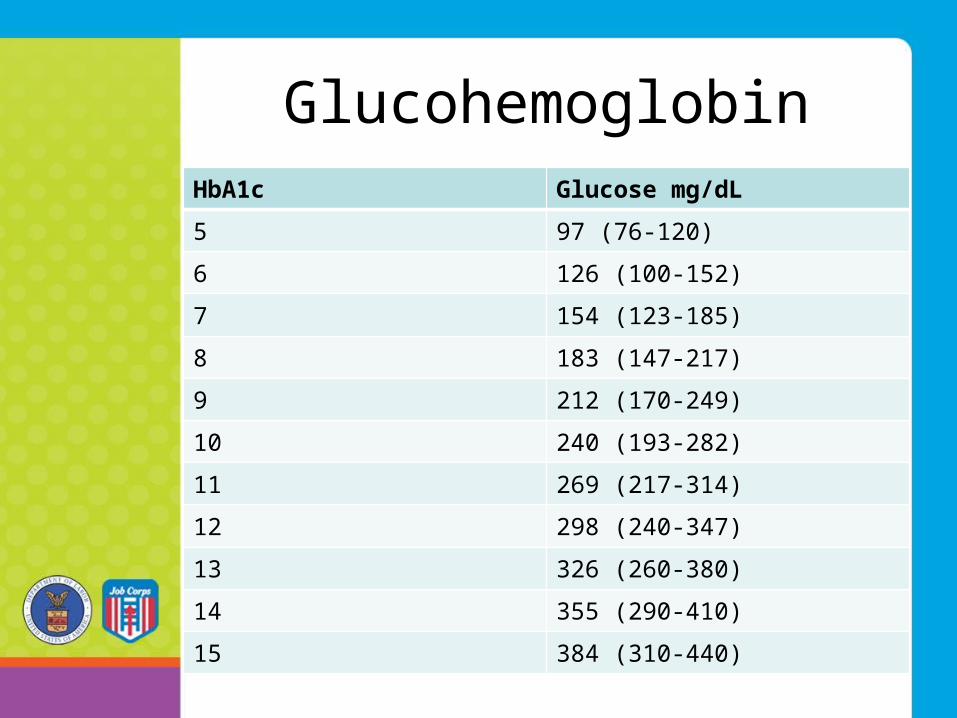
GlucohemoglobinHbA1c Glucose mg/dL
5 97 (76-120)
6 126 (100-152)
7 154 (123-185)
8 183 (147-217)
9 212 (170-249)
10 240 (193-282)
11 269 (217-314)
12 298 (240-347)
13 326 (260-380)
14 355 (290-410)
15 384 (310-440)
Historical NotesAbout Types of Diabetes
• 1550 BC: The oldest description of diabetes was noted to be a polyuric condition in ancient Egypt.
• In the 5th/6th century BC: The descriptions of diabetes recognized the distinction between two forms of diabetes, one in older, fatter people (type 2), and the other in thin people who rapidly succumbed to their illness (type 1).

Additional HistoryAbout Diabetes
• 2nd century AD: Because of the symptom of polyuria, Aretaeus of Cappadocia first used the term “diabetes”, which comes from Greek, meaning “siphon” or “pass through”.
• 10th century AD: Avicenna, living in Arabia, recognized the sugary nature of urine in diabetes.
Additional HistoryAbout Diabetes
• 17th century AD: Thomas Willis, physician to King Charles II, rediscovered the sweetness in the urine of subjects with diabetes.
• 1776: Matthew Dobson showed that urinary sweetness was caused by sugar and was associated with a rise in blood sugar.
Additional HistoryAbout Diabetes
• End of 18th century: John Rollo first used the term “diabetes mellitus” (honey) to distinguish the condition from “diabetes insipidus”, or tasteless urine.
• 1869: Paul Langerhans discovered the pancreatic islets that bear his name.
Additional HistoryAbout Diabetes
• 1889: Oskar Minkowski removed the pancreas from a dog and discovered that the animal developed diabetes.
• 1893: Edouard Laguesse showed that Langerhans’ islets were the endocrine tissue of the pancreas.
Additional HistoryAbout Diabetes
THE GAME CHANGER!• 1921: Frederick Banting, Charles
Best, James Collip & JJR Macleod discovered insulin.
• 1920s: The first patients with diabetes were treated with insulin.
Before and after pictures of one of the first people with diabetes to receive Insulin in
the 1920s

History In The Time OfTransplant Development
• 1955: The primary structure of insulin elucidated by Frederick Sanger.
• 1969: Dorothy Hodgkin described the three-dimensional structure of insulin using X-ray crystallography.
• 1980: Recombinant human insulin was introduced.
• 1996: Insulin analogues were introduced.
What Causes Type 1 Diabetes?
• Type 1 diabetes is cause by an absolute deficiency of insulin, a hormone which is produced in the beta cells of the Islets of Langerhans in the pancreas.
• Although poorly understood, it is likely that (1) some environmental factor triggers a (2) selective autoimmune destruction of the beta cells in (3) a genetically predisposed individual.

Age-standardized incidence of type 1 diabetesin children (per 100,000/year)
Worldwide Differences
Presenting Symptoms
• Polyuria / Nocturia• Thirst• Polydipsia• Polyphagia• Weight Loss• Ketoacidosis
Diabetic Ketoacidosis:A Rapid Onset Life-threatening
Complication
• Consists of hypergycemia, ketosis and acidosis• 10-25% of episodes of DKA result from new
patients presenting for the first time• 30-40% of episodes are from infections• Most of the rest are from stopping insulin• 1-2% mortality during each episode
Mortality / Morbidity
• Prior to 1921 the development of type 1 diabetes meant an almost certain death shortly after diagnosis.
• A significant proportion of deaths in young diabetics are attributable to DKA.
• Later deaths are more commonly associated with cardiovascular and renal disease.

Chronic Complications• Retinopathy: most common cause of blindness
in people of working age• Nephropathy: 20-44% of all new patients
needing renal replacement therapy have diabetes
• Erectile Dysfunction: may affect up to 50% of men with long-standing diabetes
• Macrovascular Disease: 2-3 fold increased risk of coronary heart disease and stroke
• Foot Problems: 15% of people with diabetes develop foot ulcers; 5-15% of people with diabetic foot ulcers need amputations

Applicant File Review
• Three things to remember1) Treatment of type 1 diabetes is not optional
and without treatment it will inevitably lead to death, as happened prior to 1921.
2) Some new patients have a “grace period” of weeks or months with minimal need for insulin after starting treatment. Management plans change frequently during the first few months of treatment and can require repeated adjustments of insulin timing and dose.
3) Highly effective self-management by an adolescent patient is unlikely and is not the criterion for entry into JC.
Treatment
• Insulin • Management of carbohydrate
intake• Exercise

Insulin Development
• 1921/22: In the US the original insulin was from bovine and later porcine sources
• 1982: Biosynthetic insulin was introduced
• 1996: Analogue insulins were introduced

Insulin Names
Generic
• aspart• glulisine• lispro• regular• NPH• determir• glargine
Brand
• Novolog• Apidra• Humalog• Humulin R / Novolin R• Humulin N / Novolin N• Levemir• Lantus
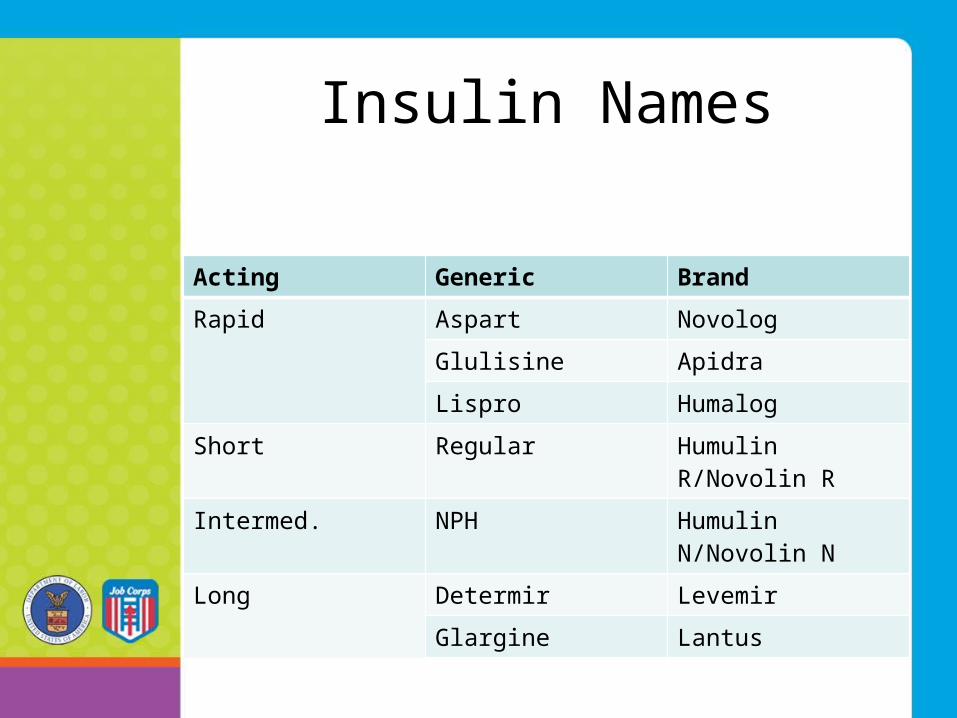
Insulin Names
Acting Generic Brand
Rapid Aspart Novolog
Glulisine Apidra
Lispro Humalog
Short Regular Humulin R/Novolin R
Intermed. NPH Humulin N/Novolin N
Long Determir Levemir
Glargine Lantus
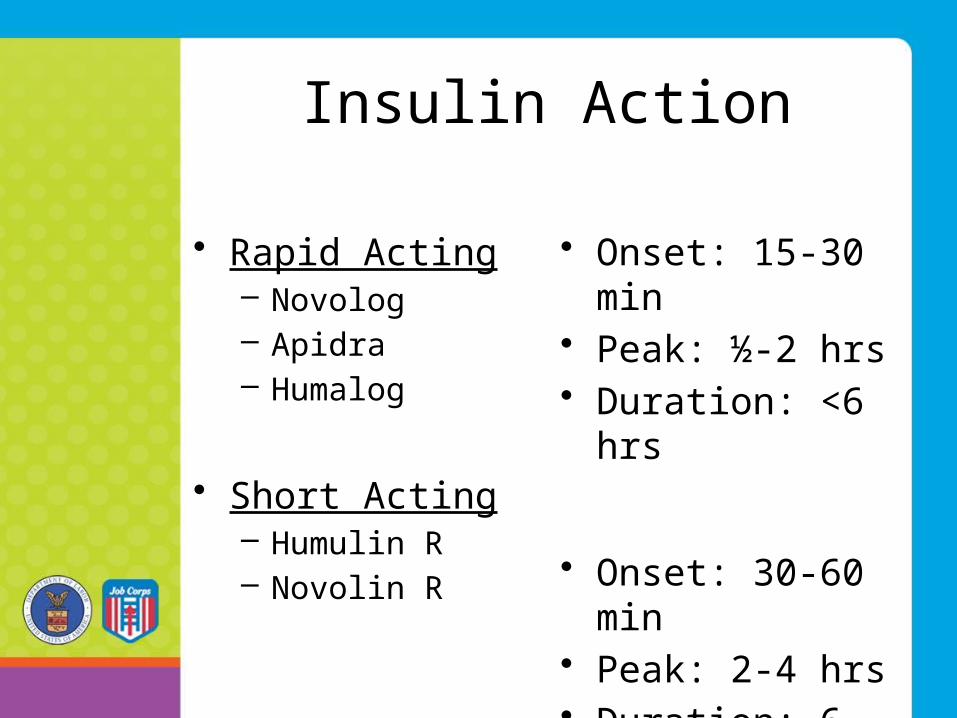
Insulin Action
• Rapid Acting– Novolog– Apidra– Humalog
• Short Acting– Humulin R– Novolin R
• Onset: 15-30 min• Peak: ½-2 hrs• Duration: <6 hrs
• Onset: 30-60 min• Peak: 2-4 hrs• Duration: 6-12 hrs
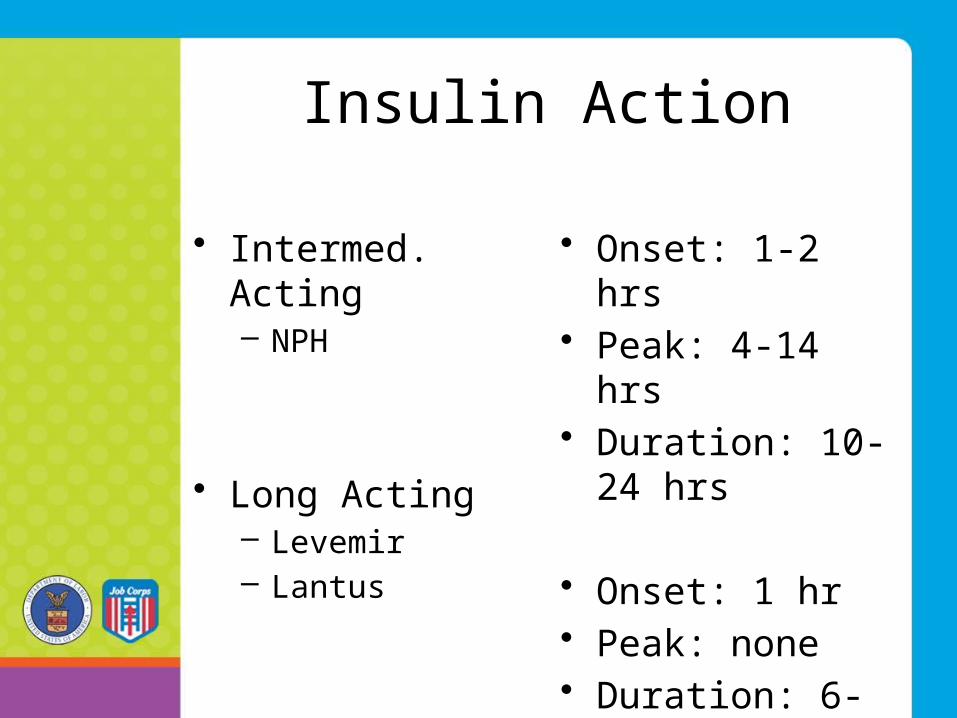
Insulin Action
• Intermed. Acting– NPH
• Long Acting– Levemir– Lantus
• Onset: 1-2 hrs• Peak: 4-14 hrs• Duration: 10-24
hrs
• Onset: 1 hr• Peak: none• Duration: 6-24 hrs
Pre-mixed Insulins(biphasic)
• Novolog mix: aspart protamine / aspart– 70/30 mix (vials and pens)
• Humalog mix: lispro protamine / lispro– 50/50 mix (vials and pens)– 75/25 mix (vials and pens)
• Novolin mix: NPH / regular– 70/30 mix (vials)
• Humulin mix: NPH / regular– 70/30 mix (vials and pens)– 50/50 mix (discontinued in US)

Treatment Regimens
• Pre-mixed insulin twice daily (2 shots daily)
• Basal-bolus regimen with rapid acting insulin at the three meals and long acting insulin at bed time (4 shots daily)
• Continuous subcutaneous insulin infusion (CSII) or insulin pumps (1 needle insertion every 3 days)

FRONT BACK
Injection Sites

Injection Site Side Effects• Lipohypertrophy: when insulin is
repeatedly injected into the same site there can be a local tropic effect and lead to lumps at the site and compromise absorption of insulin
• Lipoatrophy: immunoglobulin G immune complexes against insulin can form and produce atrophy as well as compromise the action of insulin
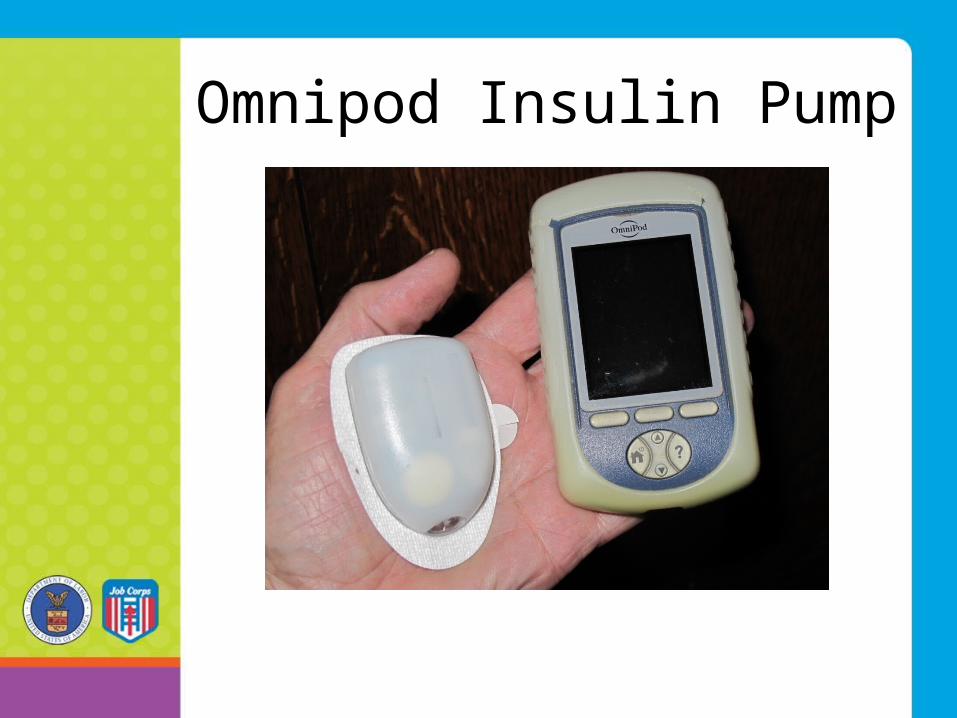
Omnipod Insulin Pump

Medtronics Insulin Pump

Medtronics Connections

Hypoglycemia• When blood glucose falls below 63 mg/dL• The most common side effect of insulin therapy• A barrier to obtaining optimal glycemic control• Most type 1 patients will experience several
mild episodes per week and 1-2 severe episodes per year needing outside help
• Occurs more frequently in young patients and those under tight glycemic control
Hypoglycemia Signs/Symptoms
• Autonomic– Sweating– Pins & needles– Feeling hot– Shakiness– Anxiety– Palpitations– Pallor
• Neuroglycopenic – Difficulty speaking– Loss of concentration– Drowsiness– Dizziness– Hemiplegia– Fits– Coma
• Non-specific – Nausea– Hunger– Weakness

Type II Diabetes Mellitus (DM II)
• It is the most common glucose disorder• Use of meds: 1994 1:63 and 2007 1:14
youth• Insulin resistance is its dominant feature• Resistance most often results from
unhealthy lifestyle behaviors• Medication often helps as adjunctive
therapy
Glucose Disorder: DM II
• Genetic, cytogenic precursors (to be defined)
• Defect in the transport or storage of insulin and/or glucose
• Defect in fat, liver and muscle cells response
• Slow onset of hyperglycemia and symptoms
Contributing Factors to DM Type II
• Family and parental influence• Cultural/Environmental/Community
Influence• Personal lifestyle behavior
influence

Variants Inclusive of DM Type I and II
• Maturity Onset of Youth (MODY)
• Combined Variant Diabetes

“Ounce of Prevention=Pound of Cure”
• Health and wellness• Student life• Academic and trade• HEALS “Healthy Eating and Active
Lifestyles”• TEAP / TUPP
Onset / Monitoring• Any age where precipitating factors exist• Gradual, slow in onset delaying early dx• Initial symptoms may wax and wane• More often diagnosis is made on center• Biochemical testing, monitoring and
risks are the same as DM I with the exception of glucose swings and mortality

Symptoms often Associated with DM II
• Loss of energy / stamina and fatigue• Gradual decline in activity and
performance• Unusual increase in appetite• Unusual increase in thirst• Increased frequency of urination• Increased frequency awakening to
urinate• Often but not always overweight
Treatment Goals
• Medical evaluation and management plans
• Address lifestyle behaviors (HEALs on center)
• Certified Diabetic Education• Adopt a lifestyle reducing insulin
resistance• Lifetime monitoring DM II (CCMP
on center)

Diabetic Education / Management
• Wellness team assessing / promoting health
• Medical team diagnosing and treating
• Measurable change in student’s life behavior
• Life time monitoring: CPP, CDP and CTP
Lifestyle Behavior• Monitor: Weight, BMI, BP, UA, Fam Hx, labs• Monitor Diet: Balance carbs, fats and protein• Monitor Daily Activity: Scheduled and not• Monitor Sleep Patterns: Quality lasting @8hrs• Monitor Stress Reduction: MH/ counselor/ RA• Reduce risk behavior• Reduce susceptibility to infectious disease
Common Pharmacologic Adjuncts
• Alpha-glucosidase Inhibtors (ie Acarbose)
• Biguanides (i.e., Metformin)• Meglitinides (i.e., Repaglinide /
Nateglinide)• Sulfonylureas (i.e., Tolazimide
Glimepiride)• Thiazolidinediones (i.e., Rosiglitazone)• Injectibles (i.e., Exenatide / Sitagliptin)
Management of DM on a JC Center
• When the IDT sees an applicant with DM I or II is this grounds for rejection?
• When DM is diagnosed on center, should the wellness team do the work up and begin Rx?
• To best manage DM, especially type II, who on center needs to know the students status?
PRH 6.12, R11: MSWR
• Students are medically separated:– when they are determined to have a
health condition that significantly interferes with or precludes further training in JC,
– when the health problem is too complicated to manage, or
– when the necessary treatment will be unusually costly.
Thank you for your attention.
Questions?
Related Documents











