Diabetes Mellitus in Children Dr Nadeem Zubairi

Diabetes Mellitus in Children Dr Nadeem Zubairi. D.M. Diabetes mellitus is a group of metabolic diseases in which a person has high blood sugar, either.
Jan 11, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Diabetes Mellitus in Children
Dr Nadeem Zubairi
D.M.
Diabetes mellitus is a group of metabolic diseases in which a person has high blood sugar, either
because the body does not produce enough insulin, or because cells do not respond to the insulin that is
produced.
This high blood sugar produces the classical symptoms of polyuriapolyuria (frequent urination), polydipsiapolydipsia
(increased thirst) and polyphagiapolyphagia (increased hunger).

© 2004, John Walsh, P.A., C.D.E.
Before Insulin
Before insulin was discovered in 1921, everyone with type 1 diabetes died within weeks to years of its onset
JL on 12/15/22 and 2 mos later
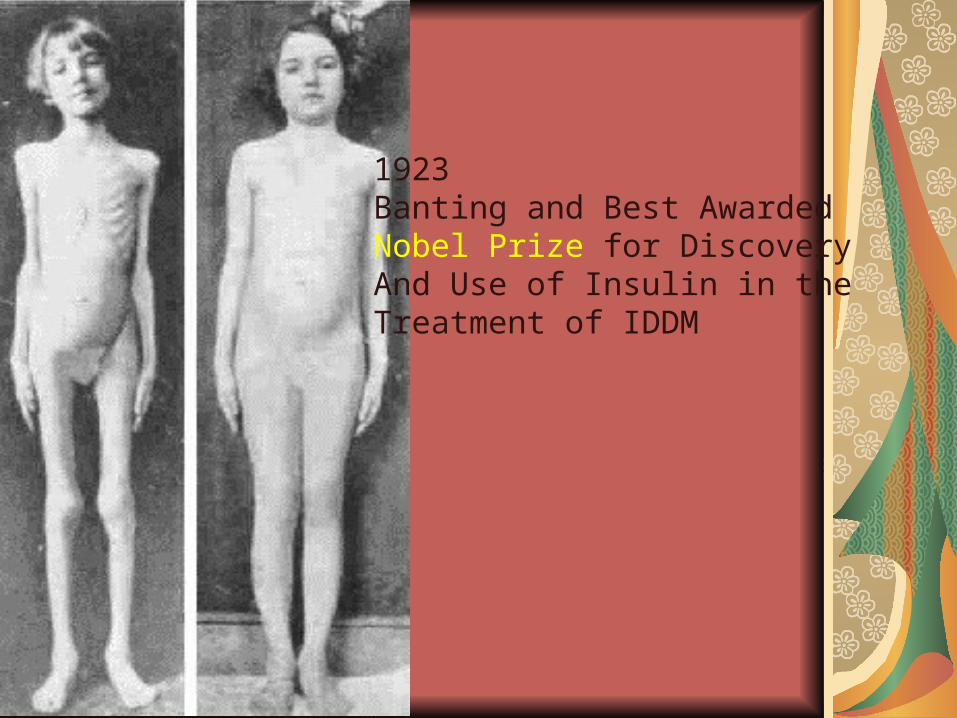
1923Banting and Best AwardedNobel Prize for Discovery And Use of Insulin in theTreatment of IDDM
OLD CLASSIFICATION (1985)
Type 1, Insulin-dependent (IDDM)Type 2, Non Insulin-dependent (NIDDM)
obesenon-obeseMODY
IGTGestational Diabetes
© 2004, John Walsh, P.A., C.D.E.
WHO CLASSIFICATION 2000
Is based on etiology not on type of treatment or age of the patient.Type 1 Diabetes
( autoimmune -cell destruction)
Type 2 Diabetes (defects in insulin secretion or action)
Other specific types
Types of Diabetes in Children
Type 1 diabetes mellitus accounts for >90% of cases.Type 2 diabetes is increasingly recognized in children with presentation like in adults.Permanent neonatal diabetesTransient neonatal diabetesSecondary diabetes e.g. in cystic fibrosis or Cushing syndrome.

EPIDEMIOLOGY Type 1 DM
– Most common metabolic disease in childhood– Annual incidence 15 new cases per 100,000
in children < 18 yrs– Frequency increases with increasing age.– 1: 1400 at age 5 yrs– 1: 400 at age 16 yrs– Males and females equally affected– No correlation with socioeconomic status
Etiology
Type 1 DM usually results from both an inherited risk and external triggers,
Infection,diet .
Type 1 diabetes is an autoimmuneautoimmune disorder in which the body attacks its pancreatic beta cells.

Genetic issuesClear evidence suggests a genetic component in type 1 diabetes mellitus.
Monozygotic twins have a 60% lifetime concordance for developing type 1 diabetes mellitus, although only 30% do so within 10 years after the first twin is diagnosed. In contrast, dizygotic twins have only an 8% risk of concordance, which is similar to the risk among other siblings.
The frequency of diabetes developing in children with a diabetic mother is 2-3% and 5-6% if the father has type 1 diabetes mellitus. The risk to children rises to almost 30% if both parents are diabetic.
Type I – IDDM
Two shared HLA haplotypes
(DR3 + DR4)
12-20% risk
One shared HLA haplotype
(DR3 or DR4)
5-7% risk
No shared HLA haplotypes
1-2% risk
HLA DQ(beta) Asp57
virtual protection
HLA DQ(beta) non-Asp57
100 X increased risk
Environmental factors
Viral infections (most important) probably by initiating or modifying an autoimmune process.( Mumps, coxsackie virus, CMV, congenital rubella)
Dietary factors are also relevantBreastfed infants have a lower risk for Type 1 DM. Some cow's milk proteins (e.g., bovine serum albumin) have antigenic similarities to an islet cell antigen.
Diagnosis
Symptoms of diabetes + casual plasma glucose concentration 11.1 mmol/L ( 200mg/dl).¹≽ ≽
Casual is defined as at any time of the day without regard to time since the last meal.
Or
Fasting plasma glucose 7.0 mmol/L ( 126mg/dl).²≽ ≽
Fasting is defined as no caloric intake for at least 8h.
Or
2h post load glucose 11.mmol/L ( 200mg/dl) during≽ ≽ an OGTT.

Progression to Type 1 DM
Autoimmune destruction
“Diabetes threshold”
Honeymoon
100% Islet loss
Autoimmune markers (ICA, IAA, GAD
Honeymoon Period
In patients with new onset of DM1 who do not have DKA, the beta cell mass has not been completely destroyed.The remaining functional beta cells seem to recover with insulin treatment, and they are again able to produce insulin. When this occurs, insulin requirements decrease, and there is a period of stable blood glucose control, often with nearly normal glucose concentrations. This phase of the disease, known as the honeymoon period, usually starts in the first weeks of therapy and usually continues for a few months at most, but can last 2 years
CLINICAL PRESENTATIONS
Classical symptom triad: polyuria, polydipsia and
weight loss
DKAAccidental diagnosis

COMPLICATIONS OF DIABETES
Acute:DKAHypoglycemiaLate-onset:Retinopathy NeuropathyNephropathyIschemic heart disease &
stroke
© 2004, John Walsh, P.A., C.D.E.
DCCT And Other Studies
ResultsBetter health
Fewer complications
Improved sense of well-being
More flexible lifestyle
StudiesDCCT 1984-1992
EDIC 1996
UKPDS 1978-1998
Kumamoto 1992-2000
Research studies between 1970 and 2000 showed that complications could be prevented by lowering high glucose levels
TREATMENT ELEMENTS
EducationInsulin therapyDiet and meal planningExerciseMonitoringHbA1c every 2-monthsHome regular BG monitoring Home urine ketones tests when
indicated

EDUCATION
Educate child & care givers about: Diabetes Insulin Life-saving skills Recognition of Hypo & DKA Meal plan Sick-day management
ManagementPrinciples of insulin therapy
Varies between individuals and changes over time
The correct dose of insulin is the dose that achieves the best glycemic control without causing obvious hypoglycemia problems and achieving normal growth(height and weight)
Dosage depends on,Age, weight, stage of puberty, duration and phase of diabetes, state of injection sites, nutritional intake and distribution, exercise pattern, daily routine

Hyperglycemia:Microangiopathiccomplications
Hypoglycemia:Neuronal lossPoor school performanceseizures
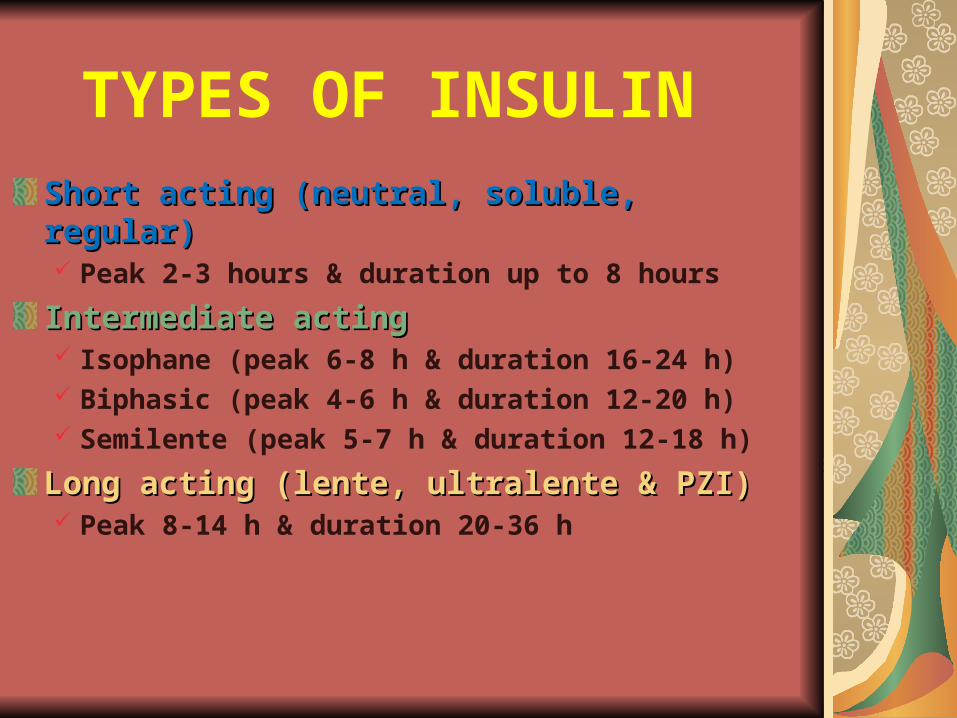
TYPES OF INSULIN
Short acting (neutral, soluble, regular)Short acting (neutral, soluble, regular) Peak 2-3 hours & duration up to 8 hours
Intermediate actingIntermediate acting Isophane (peak 6-8 h & duration 16-24 h) Biphasic (peak 4-6 h & duration 12-20 h) Semilente (peak 5-7 h & duration 12-18 h)
Long acting (lente, ultralente & PZI)Long acting (lente, ultralente & PZI) Peak 8-14 h & duration 20-36 h
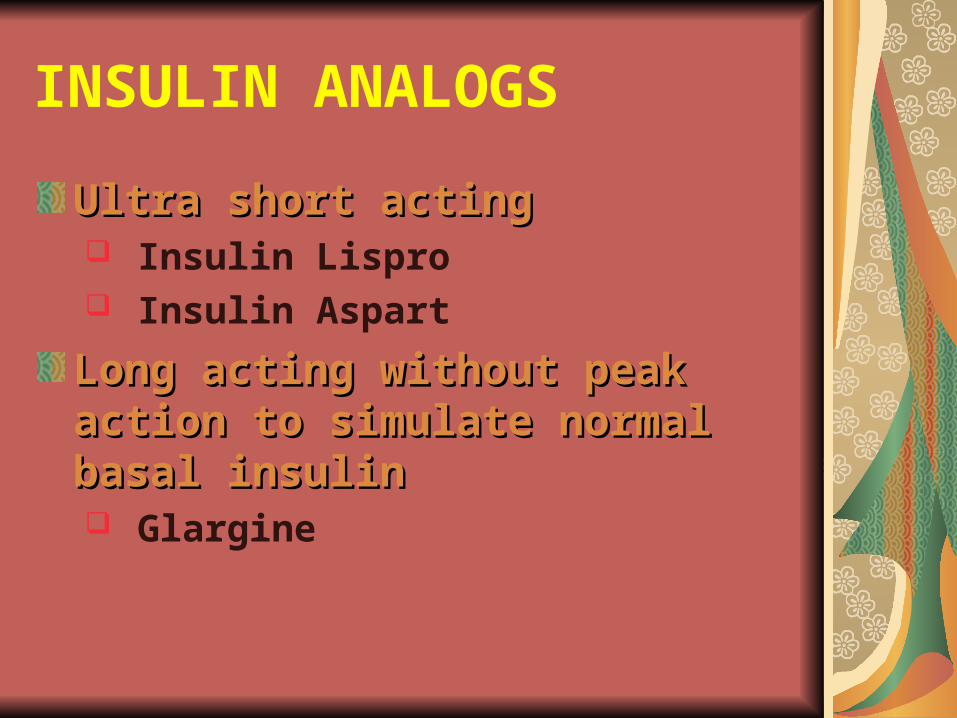
INSULIN ANALOGS
Ultra short actingUltra short acting Insulin Lispro Insulin Aspart
Long acting without peak Long acting without peak action to simulate normal action to simulate normal basal insulinbasal insulin Glargine
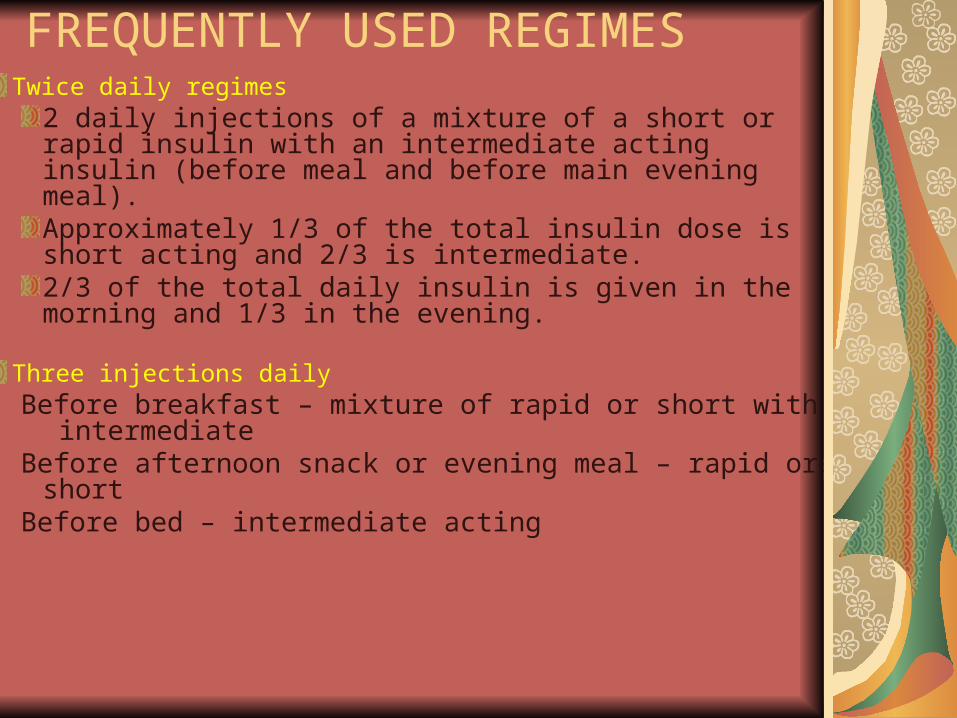
Twice daily regimes2 daily injections of a mixture of a short or rapid insulin with an intermediate acting insulin (before meal and before main evening meal).Approximately 1/3 of the total insulin dose is short acting and 2/3 is intermediate.2/3 of the total daily insulin is given in the morning and 1/3 in the evening.
Three injections daily Before breakfast – mixture of rapid or short with
intermediateBefore afternoon snack or evening meal – rapid or short Before bed – intermediate acting
FREQUENTLY USED REGIMES

Insulin Dosage
Prepubertal children usually require
0.7-1.0 IU/kg/day
During puberty, requirements may rise above 1 and even up to 2 IU/kg/day
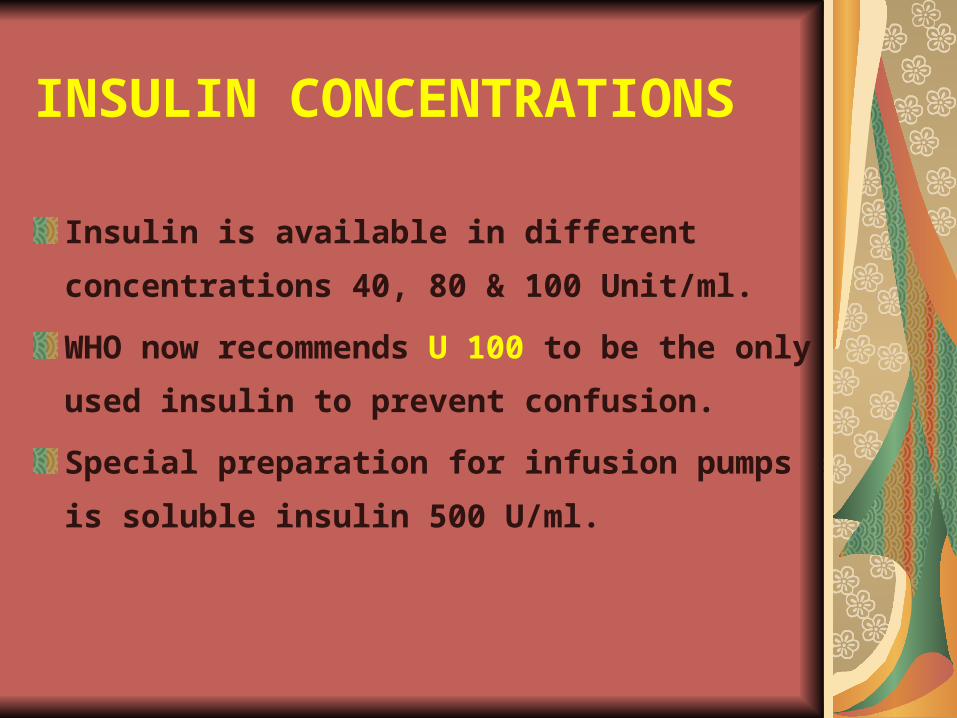
INSULIN CONCENTRATIONS
Insulin is available in different
concentrations 40, 80 & 100 Unit/ml.
WHO now recommends U 100 to be the
only used insulin to prevent confusion.
Special preparation for infusion pumps
is soluble insulin 500 U/ml.

ADVERSE EFFECTS OF INSULIN
HypoglycemiaLipoatrophyLipohypertrophyObesityInsulin allergyInsulin antibodiesInsulin induced edema
PRACTICAL PROBLEMS
injection sites & techniqueInsulin storage & transferMixing insulin preparationsInsulin & school hoursAdjusting insulin dose at homeSick-day managementRecognition & Rx of hypo at home
TREATMENT MADE EASYInsulin pens & new delivery productsHandy insulin pumpsfine micro needles Simple accurate glucometersFree educational materialcomputer programs for comprehensive management & monitoring
Diet On the standard twice daily regime, food intake is divided into 3 main meals with snacks between meals and before going to bed.
Diet should be high in fibre which will provide a sustained release of carbs.
Type of Food
The following are among the most recent consensus recommendations:Carbohydrates should provide 50-55% of daily energy intake. (No more than 10% of carbohydrates should be from sucrose or other refined carbohydrates.)Fat should provide 30-35% of daily energy intake.Protein should provide 10-15% of daily energy intake.

Activity
Type 1 diabetes mellitus requires no restrictions on activity; exercise has real benefits for a child with diabetes.
Most children can adjust their insulin dosage and diet to cope with all forms of exercise.
The current guidelines are increasingly sophisticated and allow children to compete at the highest levels in sport.
Dreams are the seedlings of realities
FUTURE PROMISESThe cure for IDDM is successful islet
cell transplantation, which will be
available in the near future.
Primary prevention by a vaccine or
drug will be offered to at risk subjects
identified by genetic studies.
Gene modulation therapy for
susceptible subjects is a promising
preventive measure.
DIABETES MELLITUS - TYPE 1MONITORING STRATEGIES
• Self Blood Glucose Monitoring – 2 to 4 / day
• Urine Testing – Ketones
• Glycosylated Hemoglobin - HbA1 C - quarterly
• Blood lipids - annually
• Thyroid function – annually
• Urine micro albumin – quarterly after 5 yr
• Dilated fundoscopy – age 10 yr + 3-5 yr

Diabetic ketoacidosis
Ketoacidosis is a state of uncontrolled catabolism associated with insulin deficiency
Diabetic ketoacidosis tends to occur in individuals younger than 19 years, but it may occur in patients with diabetes at any age.
Criteria
Hyperglycemia: blood glucose >11mmol/L(200mg/dL)
Venous pH<7.3 or bicarbonate <15 mmol/L
Ketonemia and ketonuria
Diabetic ketoacidosisIn the absence of insulin, hepatic glucose production accelerates, and peripheral uptake by tissues such as muscle is reduced.
Rising glucose levels lead to an osmotic diuresis, loss
of fluid and electrolytes, and dehydration.
Plasma osmolality rises and renal perfusion falls.
In parallel, rapid lipolysis occurs, leading to elevated circulating free fatty-acid levels.
The free fatty acids are broken down to fatty acyl-CoA within the liver cells, and this in turn is converted to
ketonebodies within the mitochondria
Diabetic ketoacidosis
Accumulation of ketone bodies produces a metabolic acidosis. Vomiting leads to further loss of fluid and electrolytes.
The excess ketones are excreted in the urine but also appear in the breath, producing a distinctive smell
similar to that of acetone.
Respiratory compensation for the acidosis leads to hyperventilation, graphically described as 'air hunger'.
Progressive dehydration impairs renal excretion of hydrogen ions and ketones, aggravating the acidosis
Diabetic ketoacidosisMostly the causes are
Previous undiagnosed diabetes
Interruption of insulin therapy
The stress of intercurrent illness
Goals of therapyCorrect dehydration
Correct acidosis and reverse ketosis
Restore blood glucose to near normal
Avoid complications of therapy
Identify and treat precipitating event
History Classic symptoms of hyperglycemia
Thirst Polyuria, polydipsia Nocturia
Other symptoms Generalized weakness Malaise/lethargy Nausea/vomiting Decreased perspiration Fatigue Anorexia or increased appetite Confusion
Symptoms of associated infections and conditions Fever Dysuria Chills Chest pain Abdominal pain Shortness of breath

Physical General signs
Ill appearance Dry skin Labored respirations Dry mucous membranes Decreased skin turgor Decreased reflexes
Vital signs Tachycardia Hypotension Tachypnea Hypothermia Fever, if infection
Specific signs Ketotic breath (fruity, with acetone smell) Confusion Coma Abdominal tenderness

Management
1. Fluids- If in shock, initial resuscitation with normal saline. Dehydration
should then be corrected gradually over 48 to 72 hour
using 0.45% Saline - Monitor :
- Fluid input and output- Electrolytes, creatinine and acid-base status regularly- Neurological states
2. Insulin- insulin infusion is started, titrating the dose according to the
blood glucose. Monitor blood glucose regularly.
- aim for gradual reduction of blood glucose .
3. Potassium
Although the initial plasma concentration may be high, it will fall following treatment with insulin and rehydration
High doses (20 to 40 mEq/L) to be added to drips
4. Sodobicarb(used only in selected patients)
-severe acidemia(arterial pH<6.9)in whom decreased cardiac contractility and peripheral vasodilation can further impair tissue function
- life threatening hyperkalemia
- cautiously give 1-2 mmol/kg over 60 min
© 2004, John Walsh, P.A., C.D.E.
COMPLICATIONS OF THERAPY
Main complication is BRAIN EDEMA
TYPE 2 DM IN CHILDREN
Among 10 – 19 yr olds
T2 DM accounts for 33% of all new cases
African Americans – 42%
Caucasians – 10%

Obesity
Acanthosis Nigricans
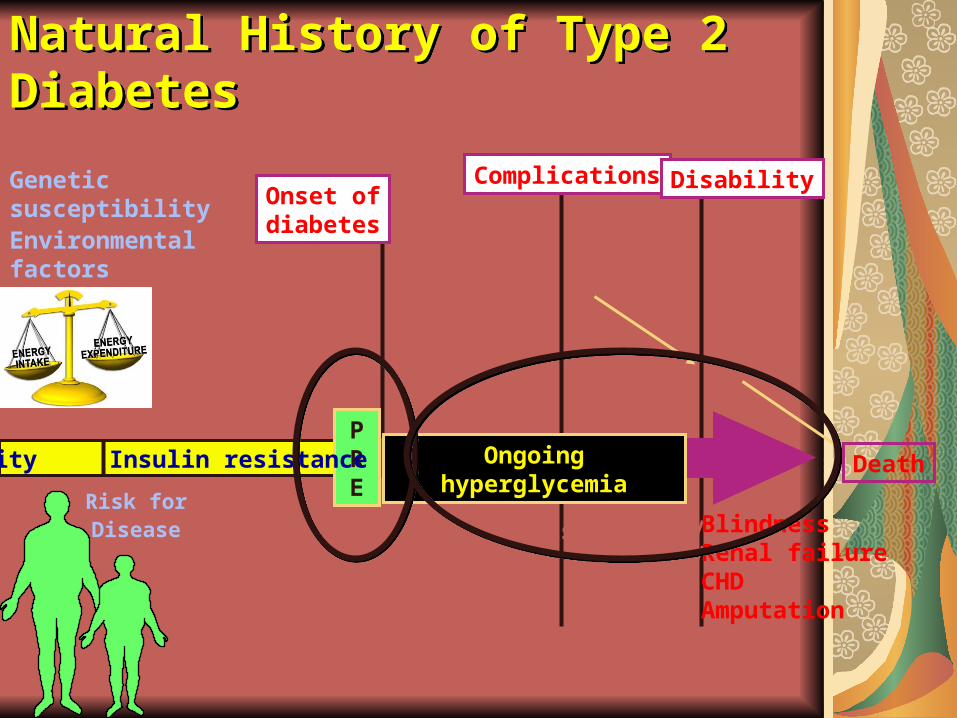
Natural History of Type 2 DiabetesNatural History of Type 2 Diabetes
Geneticsusceptibility Environmentalfactors
AtherosclerosisHyperglycemiaHypertension
RetinopathyNephropathyNeuropathy
BlindnessRenal failureCHDAmputation
Onset ofdiabetes
Complications Disability
DeathOngoing hyperglycemiaPRE
Obesity Insulin resistance
Risk forDisease
MetabolicSyndrome

Therapy of T2 DM in Children
Reduce calories – weight lossNOT T1 DM diet with high complex CHO
No Between meal snacksNOT T1 DM where hypoglycemia is frequent
Reduce CHO intake
Reduce fat intake
Exercise – increase healthy
life style
Drug treatment early x
TZD = thiazolidinedioneSilverstein JH, Rosenbloom AL.J Pediatr Endcrinol Metab. 2000;13 Suppl 6:1406-1409.
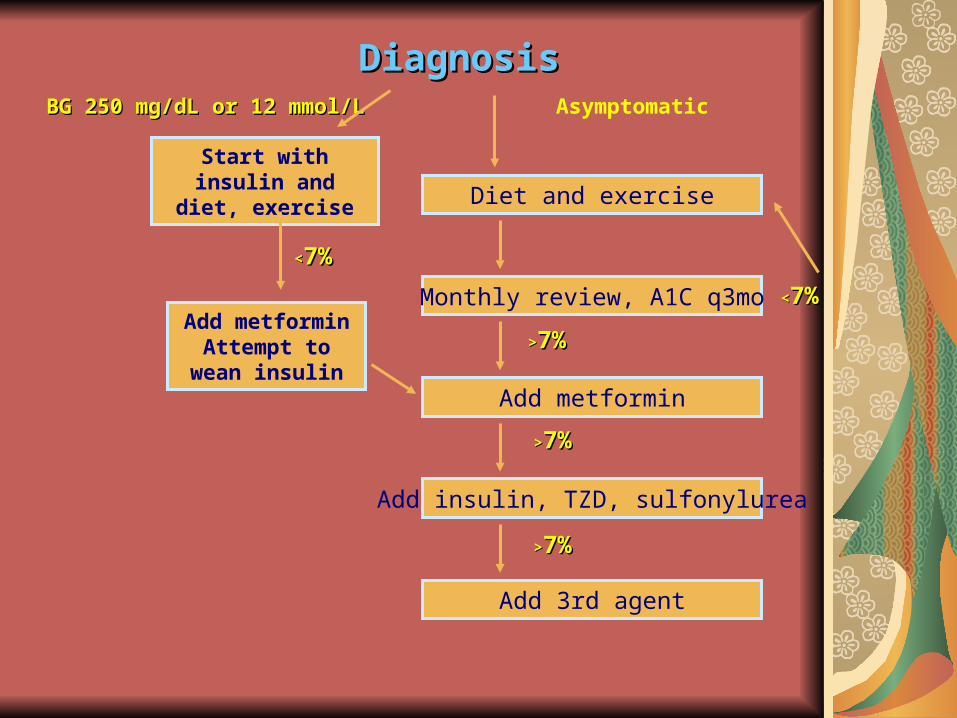
DiagnosisDiagnosisAsymptomatic
Start with insulin and diet, exercise
Diet and exercise
Monthly review, A1C q3mo
>>7%7%
Add metformin
Add metforminAttempt to
wean insulin
Add insulin, TZD, sulfonylurea
BG 250 mg/dL or 12 mmol/LBG 250 mg/dL or 12 mmol/L
Add 3rd agent
<<7%7%
>>7%7%
>>7%7%
<<7%7%
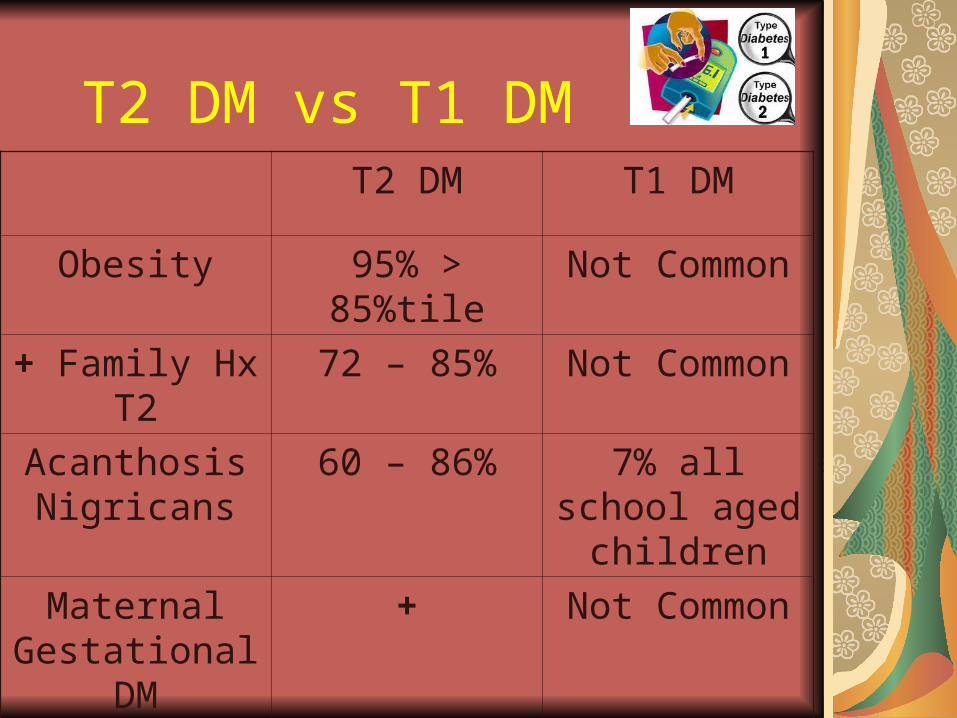
T2 DM vs T1 DMT2 DM T1 DM
Obesity 95% > 85%tile Not Common
+ Family Hx T2 72 – 85% Not Common
Acanthosis Nigricans
60 – 86% 7% all school aged children
Maternal Gestational DM
+ Not Common
IUGR + Not common
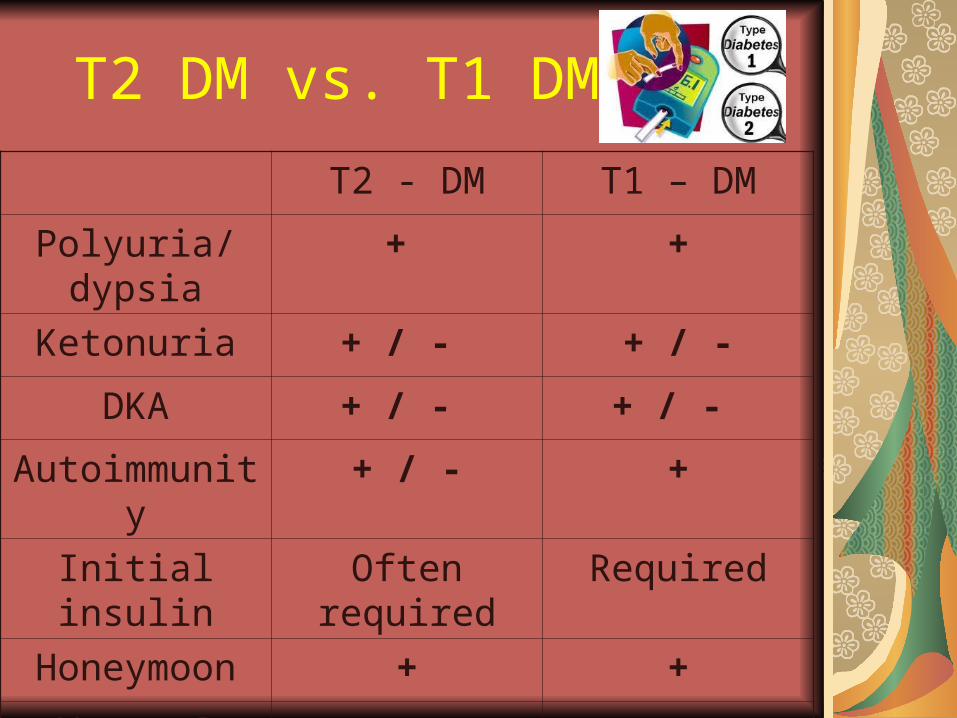
T2 DM vs. T1 DM
T2 - DM T1 – DM
Polyuria/dypsia + +
Ketonuria + / - + / -
DKA + / - + / -
Autoimmunity + / - +
Initial insulin Often required Required
Honeymoon + +
Worse @ illness + +

Uncontrolled diabetes can lead to…
Kidney failure
AmputationsLoss of Sensations
Heart disease and strokes
Blindness
Death
© 2004, John Walsh, P.A., C.D.E.
By learning you will teach;
By teaching you will learn.
Latin Proverb
Thanks AmigosThanks Amigos
Research tells us 14 out of any 10 Research tells us 14 out of any 10 individuals likes Candy individuals likes Candy
Related Documents











