Developmental & Behavioral Pediatrics: An Overview for the General Pediatrics Boards Andrew Adesman, MD Developmental & Behavioral Pediatrics Steven & Alexandra Cohen Children’s Medical Center of New York

Developmental & Behavioral Pediatrics: An Overview for the General Pediatrics Boards Andrew Adesman, MD Developmental & Behavioral Pediatrics Steven &
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Developmental & Behavioral Pediatrics:
An Overview for the General Pediatrics Boards
Andrew Adesman, MD
Developmental & Behavioral PediatricsSteven & Alexandra Cohen Children’s
Medical Center of New York

ABP Content Specs
Growth & Development (5%)
• Developmental Surveillance vs. Screening
• Milestones
ABP Content Specs
Disorders of Cognition, Language, Learning (3.5%)
• Intellectual Disability
• Autism Spectrum Disability
• Speech-Language Disorders
• Learning Disabilities

ABP Content Specs
Behavioral & Mental Health Issues (4%)
• Common Behavioral Issues (Birth – 12 years)
– Colic– Nail biting– Body rocking– Bruxism– Breath-holding– Enuresis– Night terrors vs. nightmares

ABP Content Specs
Behavioral & Mental Health Issues (4%)
• Externalizing Disorders– Aggressive behaviors, ODD, CD, – Anti-social behavior/delinquency
• Internalizing Disorders– Phobias, Anxiety Disorders, – OCD– PTSD– Mood and Affect Disorders – Psychosomatic disorders
ABP Content Specs
Behavioral & Mental Health Issues (4%)
• Suicidal behavior, psychotic behavior, thought disorders
• ADHD
Part 1:
Normal Development

ABP Content Specs
Growth & Development (5%)
• Developmental Surveillance vs. Screening
• Milestones

Surveillance
Comprehensive child development surveillance includes:
• Eliciting and attending to the parents’ concerns • Maintaining a developmental history • Making accurate and informed observations of the child • Identifying the presence of risk and protective factors • Periodically using screening tests • Documenting the process and findings

Screening
In monitoring development during infancy and early childhood, ongoing surveillance is supplemented and strengthened by standardized developmental screening tests:
- 9 months, 18 months, and 2 1/2 yrs
- at times when concerns are identified

Developmental MilestonesFull Term Infant
Category Description
Motor - Moro reflex
Cognitive/Behavioral - Becomes alert with the sound of
a bell or voice
Language
Social - Fixates on face/object and
briefly follows

Developmental Milestones2 Months
Category Description
Motor - Follows objects past mid-line
- Lifts head and shoulders off bed in prone position
Cognitive/Behavioral
Language
Social

Developmental Milestones4 Months
Category Description
Motor - Head lag disappears by 5 months- Moro disappears by 3-6 months - Bears weight on forearms while prone- Rolls from prone to supine- Bears weight while held standing
Cognitive/Behavioral
Language - Laughs out loud and squeals
Social - Imitates social interaction

Developmental Milestones6 Months
Category Description
Motor - Ability to transfer object from one hand to the other- Reaches for objects- Sits with support- Rolls over in both directions
Cognitive/Behavioral - Turns directly to sound and voice
Language - Babbles consonant sounds- Imitates speech
Social

Developmental Milestones9 Months
Category Description
Motor - Bangs two blocks together- Sits without support
Cognitive/Behavioral - Turns when name is called- Plays peek-a-boo
Language - Mama and Dada (non-specific)
Social - Stranger anxiety- Recognizes common objects and people

Developmental Milestones12 Months
Category Description
Motor - Takes a few steps- Pincer grasp- Drinks from a cup held by another person- Pulls to stand and cruises
Cognitive/Behavioral - Assists with dressing
Language - Speaks 1 additional word besides Mama and Dada- Mama and Dada specific
Social - Follows a single step command with gesture
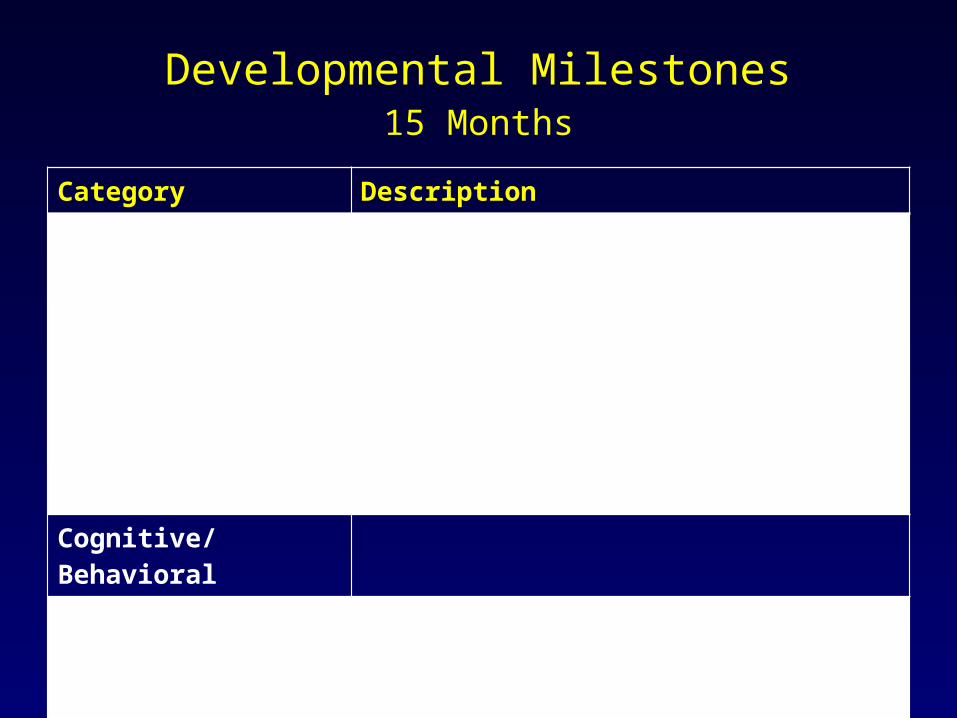
Developmental Milestones15 Months
Category Description
Motor - Gives and takes a ball- Drinks from a cup- Scribbles with a crayon- Puts cube into a cup- Walks independently- Stoops to floor and recovers to standing position
Cognitive/Behavioral
Language - Speaks 3-6 additional words besides Mama and Dada- Points to one body part- Follows single step command without gesture
Social

Developmental Milestones18 Months
Category Description
Motor - Self-feeding with a spoon- Stacks 2 cube tower- Throws ball- Walks upstairs while holding hand
Cognitive/Behavioral - Imitates household chores like sweeping, vacuuming, etc.
Language - 10-20 word vocabulary
Social
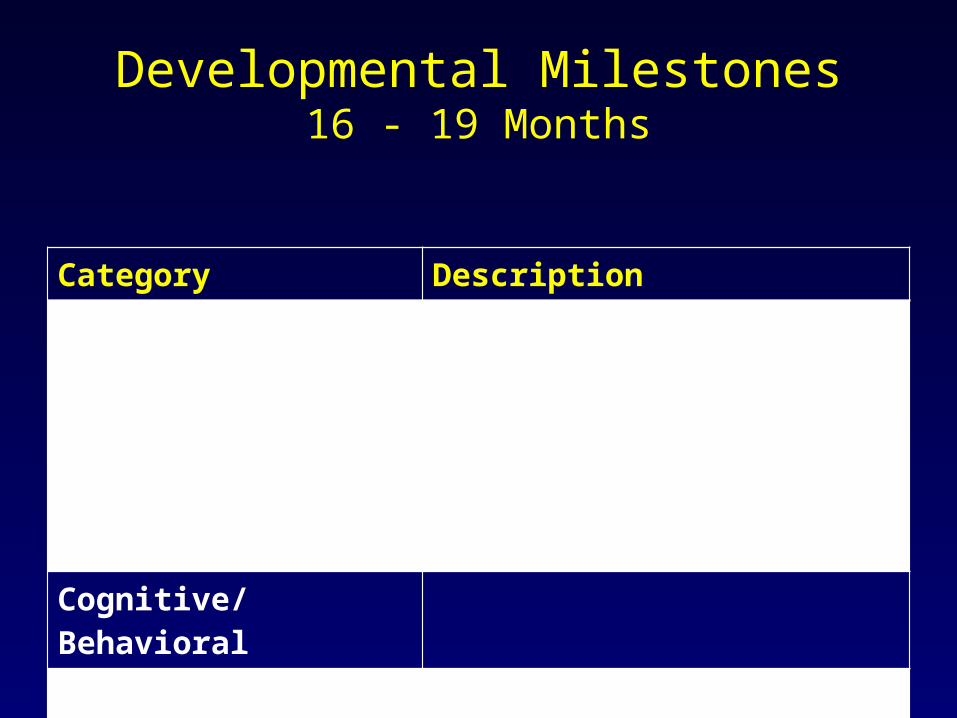
Developmental Milestones16 - 19 Months
Category Description
Motor - Builds a tower of 4 blocks- Releases a raisin into a bottle- Spontaneous scribbling (18 mo)
Cognitive/Behavioral
Language
Social

Developmental Milestones24 Months
Category DescriptionMotor - Builds a tower of 6 cubes
- Washes and dries hands- Removes clothing- Kicks a ball- Jumps with 2 feet
Cognitive/Behavioral
Language - Greater than 50 word vocabulary- Starts using pronouns -- such as I, me, and you- Speech is 50% intelligible to a stranger
Social
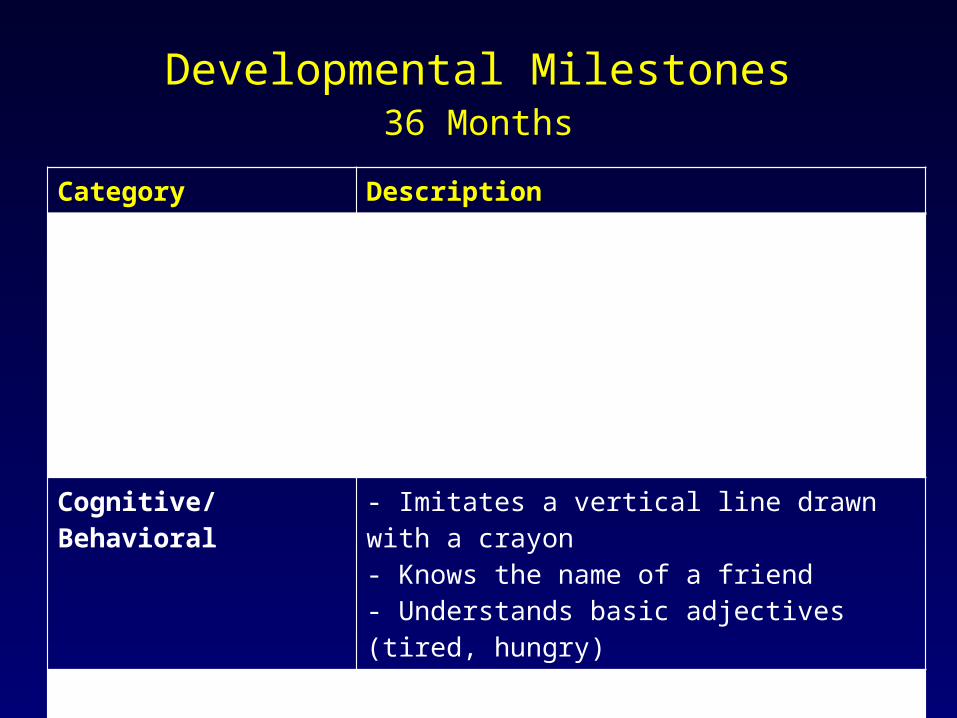
Developmental Milestones36 Months
Category Description
Motor - Copies a circle- Puts on a t-shirt/shorts- Stacks a tower of 8 cubes- Stands on one foot for 1-2 seconds- Pedals tricycle- Climbs stairs, alternating feet
Cognitive/Behavioral - Imitates a vertical line drawn with a crayon- Knows the name of a friend- Understands basic adjectives (tired, hungry)
Language - Speaks with 5-8 word sentences- 75% of what is said is intelligible- Starts using “what” and “who”
Social

Developmental Milestones4 Year Old
Category Description
Motor - Walks up and down stairs/steps- Draws a simple drawing of a person- Balances on 1 foot for 4 seconds
Cognitive/Behavioral - Dresses and brushes teeth without help- Names 4 colors
Language - Asks questions: -- Where? Why? How? What?- 100% intelligible to a stranger
Social - Pretend plays

Rule of 4’s
• Count to 4• Recite a 4-word sentence• Identify 4 primary colors• Draw a 4-part person• Build a gate out of blocks (picture a #4 as a
gate)• A stranger understands 4/4 (100%) of what
they’re saying

Developmental Milestones5 Year Old
Category Description
Motor - Draws a person with 6 body parts- Prepares a bowl for food- Skips, alternating feet
Cognitive/Behavioral - Plays board games- Counts 5 blocks- Names all the primary colors
Language - Defines words
Social
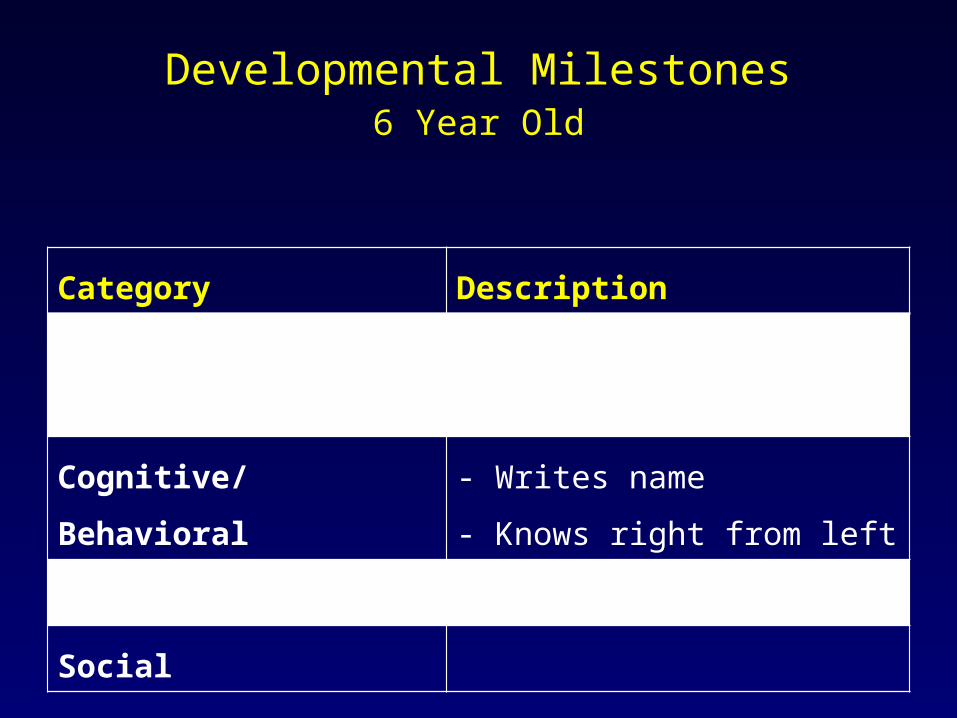
Developmental Milestones6 Year Old
Category Description
Motor - Ties shoelaces
- Rides a bicycle
Cognitive/Behavioral - Writes name
- Knows right from left
Language - Counts ten objects
Social

Block Stacking
Age Task
13-15 months 2 block tower
18 months 4 block tower
24 months 6 block tower
30 months 8 block tower
3 years 3 block bridge
4 years 5 block gate
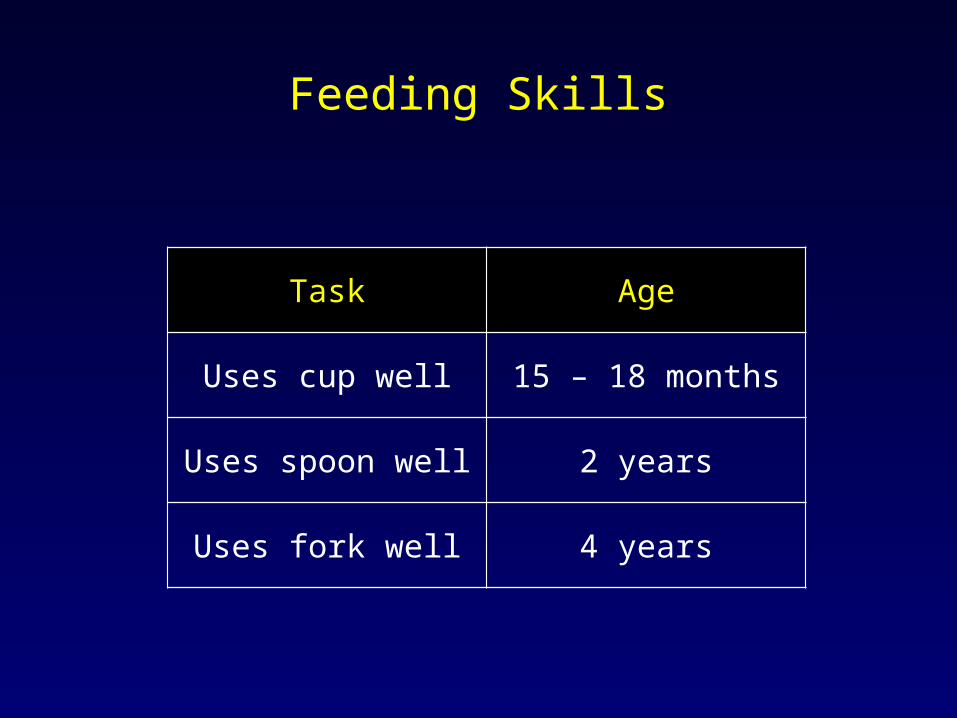
Feeding Skills
Task Age
Uses cup well 15 – 18 months
Uses spoon well 2 years
Uses fork well 4 years

Play Skills
Task Age
Symbolic Play(use one object to represent another object and engage in one or two simple actions of pretend play)
15 - 18 mo
Parallel play, empathy 24 mo
Fantasy Play(children engage in make-believe play involving several sequenced steps, assigned roles, and an overall plan and sometimes pretend by imagining an object without needing the concrete object present)
36 mo
Cooperative Play 3-4 yrs
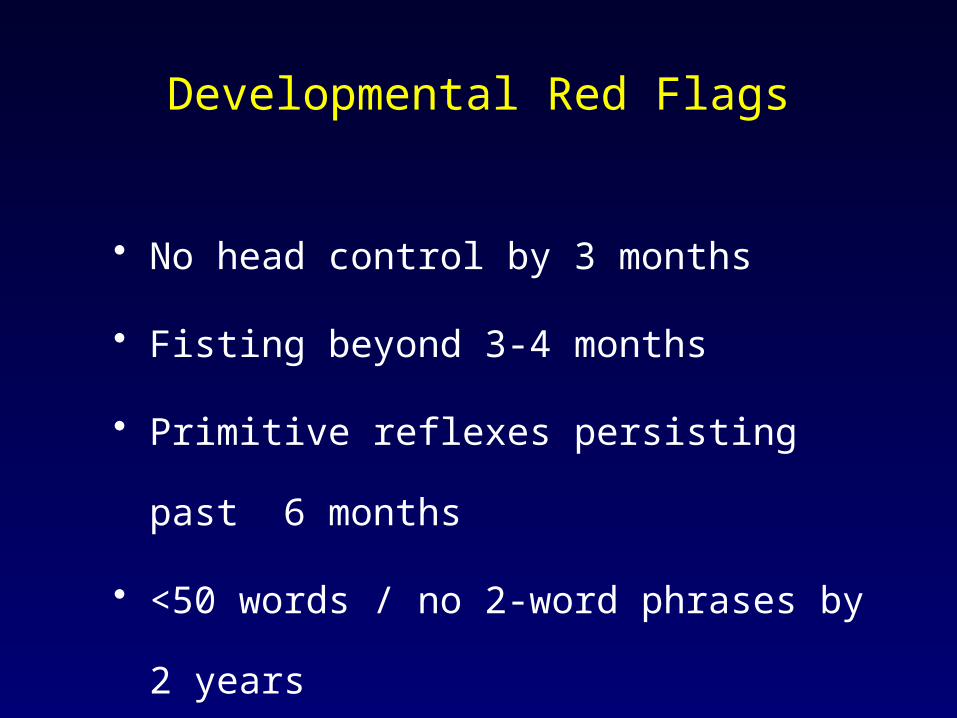
Developmental Red Flags
• No head control by 3 months
• Fisting beyond 3-4 months
• Primitive reflexes persisting past 6 months
• <50 words / no 2-word phrases by 2 years
• Echolalia beyond 30 months

Tips for Clinical Cases
• If a child is ill or uncooperative, consider a “low score” invalid
• Chronic disease or recurrent hospitalizations can cause developmental delay
• For premature infants, continue age correction until 18-24 months of age
• For speech delay, always check hearing first

Suggestion: Use Bright Futures tables provided on course website

Drawing Capabilities
Age What They Can Draw
3
4
5
6
7

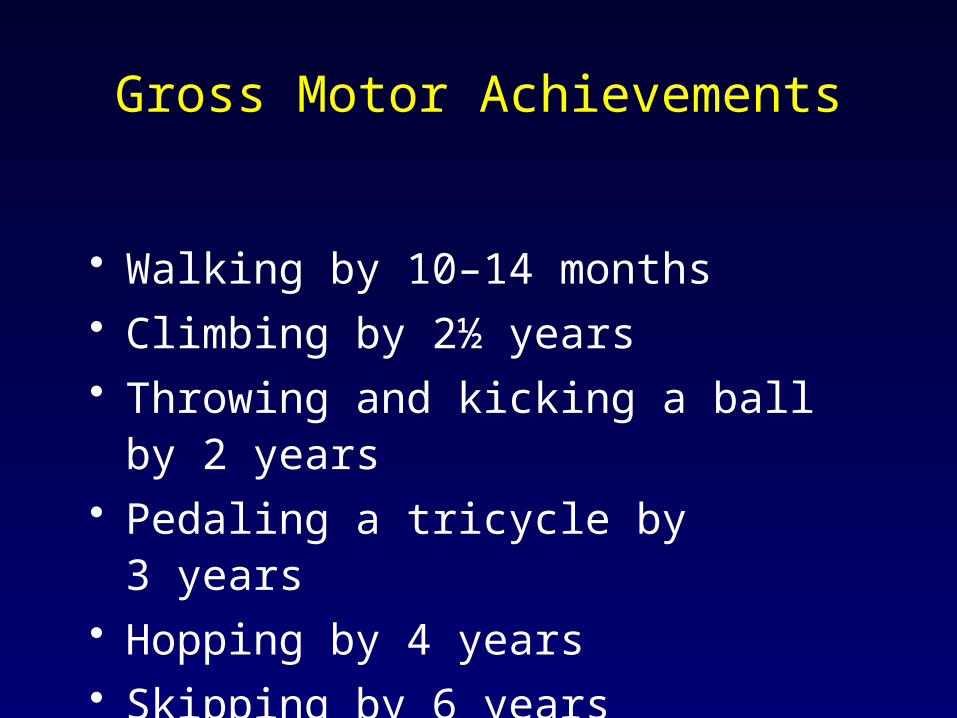
Gross Motor Achievements
• Walking by 10–14 months• Climbing by 2½ years• Throwing and kicking a ball by 2 years• Pedaling a tricycle by 3 years• Hopping by 4 years• Skipping by 6 years

Gross Motor Milestones
Fine Motor Achievements
• Stacking three or four blocks by 18 months• Completing simple form boards by 2 years• Threading beads by 3½ years• Cutting a piece of paper by 3 years• Copying geometric shapes by 4 years• Tying shoelaces by 5 years• Printing legibly by 6 years

Speech & Language Achievements
• Speaking single words by 12 months
• Making word combinations by 2 years
• Making clear, simple sentences and being
interested in books and stories by 3 years
• Making conversation clear to others by
3 or 4 years
• Reading by 5 to 6 years

Social Achievements
• Dressing by 2 years
• Self-feeding using cutlery by 3 years
• Being toilet-trained by 3½ years
• Playing cooperatively in groups by 3 years
• Playing team games by 7 years
Part 2:
Disorders of Cognition, Language, Learning
ABP Content Specs
Disorders of Cognition, Language, Learning (3.5%)
• Speech-Language Disorders
• Intellectual Disability
• Autism Spectrum Disability
• Learning Disabilities

Language Delay in a Toddler or Preschooler
CONSIDER:• Hearing Impairment• Communication Disorders• Global Developmental Delay: Intellectual
Disability• Pervasive Developmental Disorders• Environmental Factors• General Health

• 1-6/1000 newborns
• 50% genetic
– 30% syndromic (e.g. Waardenburg, Pendred, Usher)
– 70% non-syndromic, (e.g. connexin 26/GJB2)
• 77% AR, 22%AD, 1% X-linked or mitoch.
Hearing Impairment

• 50% Non-genetic:– TORCH infection
– Ear/craniofacial anomalies– Birth Weight < 1500 gm– Low Apgar Scores (0-3 at 5 min, 0-6 at 10 min)– Respiratory Distress/ Prolonged mechanical
ventilation, hyperbilirubinemia requiring exchg transfusion
– Bacterial meningitis/ Ototoxic meds
Hearing Impairment
Conductive Hearing Loss
• Failure of sound to progress to the cochlea
• Most common cause is an effusion, in the absence of inflammation, usually due to otitis media
• Clues of a mild conductive hearing loss would include ignoring commands and slight increasing of the TV volume
Sensorineural Hearing Loss Secondary to Meningitis
• Bacterial meningitis is the most common neonatal cause of hearing loss
• Tends to occur early in illness, usually in the first 24 hours
• It is not related to the severity of the illness, the age of the patient, or when antibiotics were started
HEARING LOSS: Post-newborn
• Recurrent or persistent OME – at least 3 mo
• Head trauma with fracture of temporal bone
• Congenital CMV
– often asymptomatic, HL may show up in later childhood (median age 44 months)
• Childhood infectious diseases – e.g. meningitis, mumps, measles
• Chemotherapy
• Structural anomalies: – e.g. Mondini malformation, enlarged
vestibular aqueduct
• Neurodegenerative disorders – e.g. Hunter syndrome, demyelinating
diseases (e.g, Friedreich ataxia, Charcot-Marie-Tooth)
HEARING LOSS: Post-newborn

Mild 25-39
Moderate 40-68
Severe 70-94
Hearing Loss - Audiogram
Age Appropriate Hearing Tests
• Conventional Pure Tone Audiometry Screen:– Appropriate for school age children who can
cooperate with commands– Tests each ear independently– Can differentiate between sensorineural and
conductive hearing loss• Newborn Hearing Screening (3 tests; for
newborns in the nursery):– Automated auditory brainstem response (AABR)– Transient evoked otoacoustic emissions (TEOAE)– Distortion product otoacoustic emissions (DPOAE)

Age Appropriate Hearing Tests
• Behavioral Observational Audiometry (BOA):– For infants <6 months of age– Only a screening test; infants who fail this must
undergo ABR testing
• Visual Reinforcement Audiometry (VRA):– For “pre-school” children– Tests for bilateral hearing loss so intervention to
prevent language development impairment can be started
Communication Disorders
• Expressive Language Disorders • Mixed Expressive / Receptive Disorders• Phonological Disorders
DSM 5 (May 2013):
- Language Disorder
(expressive and mixed receptive-expressive)
- Speech Sound Disorder
(new name for phonological disorder)
- Childhood-onset Fluency Disorder (stuttering)
- Social (pragmatic) Communication Disorder

• Expressive Disorders– Disorders of morphology (form), semantics (word
meaning), syntax (grammar), pragmatics (social use of language)
• Mixed Expressive/Receptive Disorders:– Above plus comprehension deficits
• Phonological Disorders– Disorders of articulation (motor movements),
dyspraxias (motor planning)– Disorders of fluency (flow,rhythm)– Disorders of voice/resonance
Communication Disorders

Childhood-Onset Fluency Disorder (“Stuttering”, Stammering”)
• Disturbance in fluency and time patterning of speech
• Begins age 2 ½ to 4, peak age 5• Normal up to age 3 or 4• Male:female ratio is 3-4: 1• 75% of preschoolers will stop• Often disappears once vocabulary rapidly
increases

Articulation IntelligibilityRule of Quarters
Age % of spoken language that is intelligible to strangers
2 2/4 = 50% intelligible
3 3/4 = 75% intelligible
4 4/4 = 100% intelligible
Stuttering
• Persistence beyond school age will require a workup
• Indications for evaluation:– Family history of stuttering– Persists 6 months or more– Presence of concomitant speech or language
disorders– Secondary emotional distress
Intellectual Disability(Mental Retardation)
Characterized by:
• Deficits in intellectual functions • Adaptive Skill Deficits• Onset before age 18
Level of severity determined by adaptive functioning, not IQ score (DSM V)

IQ Testing
• The predictive validity of IQ testing increases with age
Red Flags for ID2 to 9 Months
Age Deficiency Requiring Intervention
2 months Lack of visual attention/fixation
4 months Lack of visual trackingLack of steady head control
6 months Failure to turn to sound or voice
9 months Inability to sitLack of babbling

Red Flags for ID18 to >36 months
Age Deficiency Requiring Intervention
18 months Inability to walk independently
24 months Failure to use single words
36 months Failure to speak in 3-word sentences
>36 months Unintelligible speech

Lab Testing for Developmental Delay
• For speech delay, always check hearing first
• For a newborn/infant, always check previous metabolic screening done by state
• For older children, serum lead level, ?TSH
• Metabolic screening is not recommended for asymptomatic children with idiopathic ID
ID/MR- Etiology• Prenatal (50-70%)
– genetic, CNS malformations, fetal compromise, infection, teratogens
• Perinatal (<10%)– HIE, prematurity
• Postnatal– Trauma, asphyxia, infection, toxins, vascular
malformations, tumors, degenerative disease• Environmental (additive)
– Deprivation/malnutrition• More severe forms, more likely to find definitive
etiology
Fragile X Syndrome
• Most common form of inherited ID and the 2nd most common form of ID after Down’s Syndrome
• Caused by repeat of CGG trinucleotide on X chromosome
• Twice as likely to be seen in males vs. females
• Diagnosis: DNA testing is more sensitive than karyotyping for a child with ID

Williams Syndrome
• Facial features: elfin faces, wide spaced teeth, and an upturned nose
• Developmental delays and learning disabilities
• Hypercalcemia and supravalvular aortic stenosis
Pervasive Developmental DisordersDSM IV
• Autistic Disorder (total of 6, at least 2 from #1):1. Qualitative impairment in social interaction2. Qualitative impairment in communication3. Restrictive, repetitive, stereotyped patterns
of behaviors, interests and activities.• PDD NOS• Asperger’s Disorder• Rett’s Syndrome• Childhood Onset Disintegrative Disorder“Autism Spectrum Disorders”: DSM 5 (May, 2013)
1. Deficits in social communication and social interaction 2. Restricted repetitive behaviors, interests and activities

Autism Spectrum DisordersDSM-V
• Deficits in social communication and social interaction
• Restricted repetitive behaviors, interests and activities

Autistic Spectrum Disorders: Key Points
• Prevalence (CDC 2012): ~ 1/88• Male: Female 4:1 • Seen in association with:
– Seizure disorders, congenital infection, metabolic abnl (PKU)
– Neurocutaneous disorders (TS, NF)– Genetic Disorders (Fra X, Angelman’s, Smith-Lemli Opitz )– No proven ass’n with vaccines (MMR, thimerosal)
• Genetic Basis - Concordance rates:– MZ twins (60-80%) – DZ twins, sibs (3-7%)

Rett Syndrome
• Affects girls almost exclusively• Characterized by autistic-like behavior and hand
wringing• Normal development at first, but around age 4
months head growth decelerates• Stagnation of development from age 6-18 months• Loss of milestones (regression) from age 1-4 years• No further decline after regression period • Affected individuals usually survive into adulthood
– though never regain use of hands or attain meaningful ability to talk

Asperger’s Disorder
• Qualitative impairment in social interaction• No clinically significant general delay in language
– Impaired pragmatics– “Little professors”
• No clinically significant delay in cognitive development or in the development of age-appropriate self-help skills
– Motor coordination difficulties This disorder is not included in DSM V

Language DelaysRed Flags vs. Red Herrings
• A bilingual home and a second child (including a boy) with sibs and parents speaking for the child do not explain language delays
• A hearing evaluation is needed, especially with a history of TORCH infections, hyperbilirubinemia, or meningitis

School Failure
• “Slow Learner”: Borderline Intelligence
• Learning Disorders: Average Intelligence
• ADHD and Disruptive Behavior Disorders
(Oppositional Defiant Disorder, Conduct
Disorder)
• Mood and Anxiety Disorders
• Chronic Medical Illness
• Psychosocial stressors
• Receptive language, expressive language
• Basic reading skills, reading comprehension
• Written expression
• Mathematics calculation / reasoning
DSM 5 (May, 2013) : “Specific Learning Disorder”
Learning Disorders – Difficulties in:
Learning Disabilities (LD)
• A child can have a LD with normal or even superior intelligence; the two are not related
• Having a LD means there is a specific difficulty in one of the following areas:– Listening– Speaking– Reading– Writing– Reasoning– Math Skills

Learning Disabilities (LD)
• Social problems may be a manifestation of a LD, but they are not considered learning disorders in and of themselves
• A LD can often be compensated for in the early grades
• LD are then picked up in the later grades when things get tougher and more challenging
• A child who reverses the letters (e.g., b/d) or numbers (e.g., 6/9) may not have a LD. This can be a normal finding up to age 7

o
o
o
o
Part 3:
Behavioral & Mental Health Issues

ABP Content Specs
Behavioral & Mental Health Issues (4%)
• Common Behavioral Issues (Birth – 12 years)
– Colic– Nail biting– Body rocking– Bruxism– Breath-holding– Enuresis– Night terrors vs. nightmares

ABP Content Specs
Behavioral & Mental Health Issues (4%)
• Externalizing Disorders– Aggressive behaviors, ODD, CD, – Anti-social behavior/delinquency
• Internalizing Disorders– Phobias, Anxiety Disorders, – OCD– PTSD– Mood and Affect Disorders – Psychosomatic disorders
ABP Content Specs
Behavioral & Mental Health Issues (4%)
• Suicidal behavior, psychotic behavior, thought disorders
• ADHD

Colic
• Diagnosed based on history– Physical exam rarely shows anything
– No labs that confirm the diagnosis
• Stops after 3-4 months of age
• No “proven” methods to treat colic
• Typical presentation is crying episodes in an
otherwise healthy infant– Crying starts suddenly
Colic• Normal crying patterns of infants is up to 2
hrs/day and 3 hrs/day (for ages birth-6 wks, and 6 wks+, respectively)– When presented with a crying infant, add up the
total hours crying (if it is only 3 hours, this is normal and nothing more than parental reassurance is needed)
• Correct management is to reduce parental frustration by having another caretaker take over
• Often disturbing sleep patterns may just be part of the “temperament” of the infant with no intervention required

Television Viewing
• Known harmful effects of TV on children:– Trivializing violence and blurring lines between
reality and fantasy– Encouraging passivity at the expense of
activity– Increase of aggressive behavior and influence
of the toys played with and cereals eaten• TV watching takes up more time than school• Children watch 23 hrs/week• Only the time spent sleeping exceeds the
number of leisure hours watching TV

Nail Biting(onychophagia)
• Most common between ages 10 and 18 years
• Seen in 50% of children
• <10 years: equal in boys and girls
• >10 years: more common in boys
• Tx: positive reinforcement
– Praise when child is not biting his nails

Body Rocking
• Occurs at ~6 months in 5-20% of children
• Sitting or crawling position
• Most common around bedtime & lasts ~ ½ hours
• Usually stops by 2-3 years
• Rarely continues into adolescence
• May occur with standing in children with
developmental disabilities– ASD, visual impairment

Bruxism (clenching / grinding)
• Typically nocturnal during REM sleep• If prolonged, can cause T-M joint pain, tooth
damage, tension headaches, face pain, and neck stiffness in adolescents
• More common in boys• Familial• Children -- usually self-limited; tx not indicated• Teens -- splint or bite guards (dentist)
Breath-Holding Spells
• Typical presentation: anger, frustration, or infant in pain
• Occurs between ages 6-18 months• Simple breath holding-spell: child becomes
pale or cyanotic• Complex breath holding-spell: child continues
to cry until unconscious • Can progress to a hypoxic seizure with a
postictal period• Association between anemia and incidence of
BHS

Breath Holding Spells
• Usually associated when child is angry,
frustrated, in pain, or afraid
• Hold breath for up to 1 minute
• Most common in ages 1 – 3 years
• Reflexive, not purposeful
• Brief loss of consciousness

Breath Holding Spells
• May have a brief, benign seizure (not at risk for epilepsy)
• Cyanotic vs. Pallid• Dx is clinical; consider anemia• Family history is frequently positive
– autosomal dominant with reduced penetrance
• Tx: Reassurance– iron if anemic

EnuresisNocturnal Enuresis
• Initial workup for new onset consists of history, physical, and urinalysis
• Organic causes: SUDS (sickle cell trait, UTI, diabetes, seizure or sacral)
• Short term treatment is desmopressin acetate• Enuresis alarms for long term management• Seen up to 20% of children at age 5• 15% of cases per year will resolve with no
intervention
EnuresisDiurnal Enuresis
• Diurnal enuresis after a period of daytime continence is most likely due to an organic illness warranting workup
• UTI, DM, DI, or kidney disease• 97% of the time the cause is non-organic• Cannot be defined prior to age 3• Appropriate management is behavioral
intervention by designing a voiding routine
Night Terrors
• Occur during the first third of the night and happen rapidly
• Often family history present• Occurs more in boys than girls• Child exhibits distinctive physical findings
(deep breathing, dilated pupils, sweating, etc.)• Child can become mobile, which can result in
injury• If woken up, child will be “disoriented” with no
recall of episode
Nightmares
• Occur during the last third of the night
• Child can be woken easily
• Child will recall the nightmare, often vividly
• Not mobile

“Externalizing Disorders”
• ADHD• Oppositional-Defiant Disorder• Conduct Disorder
Attention-Deficit/Hyperactivity Disorder
• Symptoms of Inattention, Impulsivity, Hyperactivity
• Some symptoms present before age 7 years– DSM 5: Several inattentive or hyperactive-
impulsive symptoms present prior to age 12• Impairment from the symptoms is present in two
or more settings – DSM 5: Several symptoms in each setting
• Clear evidence of clinically significant impairment in social, academic, or occupational functioning.

• Combined Type (80%*)
• Predominantly Inattentive Type (10-15%*)
• Predominantly Hyperactive-Impulsive Type (5%*)
*in school-age children
ADHD Subtypes

ADHD: Key Points
• Disorder of dopamine and norepinephrine systems in frontostriatal circuitry
• 3-7% of school age children• Male: female (6:1-3:1)• Genetic Predisposition: 5-6 fold increase in
first degree relatives• Environmental Factors: e.g. head trauma,
lead exposure, VLBW, prenatal teratogens• Symptoms Persist into Adulthood in 60-80%

ADHD - Key points (cont’d)
• Co-morbid Conditions:– Learning Disorders– Anxiety Disorders– Oppositional Defiant Disorder– Conduct Disorder– Tic Disorders– Mood Disorders– Substance abuse disorders (adolescents)

ADHD - Treatment
• Psychopharmacologic: stimulants = first line– Inhibit reuptake of dopamine and norepinephrine– Stimulant Side effects: appetite suppression,
headache, abdominal pain, growth suppression, irritability, onset/ exacerbation of tics
• Behavioral Interventions

• Mood Disorders: – e.g. Major Depressive Disorder, Dysthymic Disorder, Bipolar
Disorder – DSM 5: “Disruptive Mood Dysregulation Disorder”
• Anxiety Disorders: – e.g. Generalized Anxiety Disorder, Separation Anxiety Disorder,
Panic Disorder, Social Anxiety Disorder, School Phobia • Obsessive-Compulsive Disorder
– DSM 5: Included in “O-C and Related Disorders”, not “Anxiety Disorders”
• Post-traumatic Stress Disorder – DSM 5: Included in “Trauma- and Stressor-related Disorders”
“Internalizing Disorders”

Part 4:
Sample Questions

?? A baby is pulled to sit with no head lag, grasps a rattle, and follows an object visually 180 degrees. These milestones are typical for:
1. 2 months
2. 4 months
3. 6 months
4. 8 months
2 month
s
4 month
s
6 month
s
8 month
s
38%
13%
38%
13%

??Tanya is now walking well, and can stoop to the floor and get back up. She generally points to indicate what she wants, but can ask for her “bottle”, a “cookie” and her “blankie”. She drinks from a sippy cup and feeds herself cheerios. She places a toy bottle in her doll’s mouth. Tanya is most likely a typically developing:
1. 12 month old
2. 15 month old
3. 18 month old
4. 24 month old
12 month
old
15 month
old
18 month
old
24 month
old
0%
57%
0%
43%
?? Maria sits in your office with paper and crayons. She counts ten crayons and labels the colors. She can copy a square, print her first name and draw a picture of her mother with 6 body parts. Out in the hall she demonstrates hopping on each foot and skipping. Her age is closest to:
A. 42 months
B. 48 months
C. 60 months
D. 72 months
42 month
s
48 month
s
60 month
s
72 month
s
0%
33%33%33%

?? A 3 year old boy should have mastered each of the following except:
A. Naming a red truck
B. Towering 6 cubes
C. Stating his name and gender
D. Hopping on one foot
Naming a re
d truck
Towering 6
cubes
Stating his name and ge
...
Hopping on one foot
38%
25%25%
13%

??On a pre-kindergarten screening a school official is most concerned about
a 5 year old boy who cannot:
A. Draw a Person with 6 parts
B. Copy a Square
C. Name 4 colors
D. Tandem Walk
Draw a
Person w
ith 6
parts
Copy a Square
Name 4
colors
Tandem
Walk
10%
50%
20%20%
6

??On a pre-kindergarten screening a school official is most concerned about
a 5 year old boy who cannot:
A. Draw a Person with 6 parts (50%ile ~4 ½ yrs)
B. Copy a Square (50%ile ~ 5 yrs)
C. Name 4 colors (50%ile ~ 3 ¾ yrs)
D. Tandem Walk (50%ile ~ 4 ½ yrs)
6
??You would be most concerned about:
A. A one year old who doesn’t stand alone
B. A 15 month old who can’t stoop and recover
C. A four year old who cannot hop on each foot
D. A two year old who cannot jump
A one yea
r old w
ho doesn’t s
tand...
A 15 m
onth old w
ho can’t s
toop ...
A four y
ear o
ld who ca
nnot hop ..
A two ye
ar old w
ho cannot ju
mp
33%
27%27%
13%
6

??You would be most concerned about:
A. A one year old who doesn’t stand alone (50-90% of 1 year olds)
B. A 15 month old who can’t stoop and recover (>90% of 15 month olds)
C. A four year old who cannot hop on each foot (50-90% of 4 yr olds)
D. A two year old who cannot jump (50-90% of 2 yr olds)
6
??You would be less concerned about:
A. A 3 year old who cannot answer a “why”question
B. An 18 month old who uses 2 words
C. A one year old who doesn’t point
D. A 9 month old who doesn’t babble
A 3 yea
r old w
ho cannot a
nswer..
An 18 m
onth old w
ho uses 2
words
A one yea
r old w
ho doesn’t p
oint
A 9 month old w
ho doesn’t b
abble
27% 27%
0%
45%
6
??You would be less concerned about:
A. A 3 year old who cannot answer a “why”question (50% ile ~4-5 yrs)
B. An 18 month old who uses 2 words (over 90% of 15 mo olds)
C. A one year old who doesn’t point (over 90% of 1 yr olds)
D. A 9 month old who doesn’t babble (over 90% of 9 mo olds)
A 3 year old w
ho cannot..
.
An 18 month
old who use
s..
A one year old w
ho does...
A 9 month
old who doesn
..
0%
38%38%
25%

??Annie is a 16 month old brought by her parents who worry that she is not yet walking. Born at 25 weeks, she required oxygen, phototherapy and parenteral nutrition. She now eats with her hands, drinks from an open cup, pulls to stand and takes a step while holding on. Your exam is unremarkable. Your best recommendation is:
A. Send Annie to rehab for physical therapy
B. Request a neurological consultation
C. See Annie back in two months for follow up
D. Consider an MRI to r/o intraventricular hemorrhage Send Annie to
rehab fo
r...
Request a neuro
logical c
...
See Annie back in
two m
...
Consider a
n MRI to
r/o i..
.
43%
14%14%
29%

?? You are evaluating a 9 month old baby who is not yet sitting without support. She is a former 26 week premature infant. Brain MRI reveals periventricular leukomalacia. Of the following findings, which would you most likely expect to see:
A. Increased tone in all 4 extremities, especially the UE
B. Equally increased tone in all 4 extremities
C. Dyskinetic, choreoathetoid movements
D. Increased tone in all 4 extremities, especially the LE
E. Increased tone in the right upper extremities compared with the left
Increase
d tone in
all 4 ex..
.
Equally in
crease
d tone in
...
Dyskinetic,
chore
oatheto
..
Increase
d tone in
all 4 ex..
.
Increase
d tone in
the rig
..
30%
10%
20%
30%
10%

?? Parents of a 3 year old girl present with concerns about speech and language delays. Their daughter has a vocabulary of about 10 words, and she recently began pointing to body parts and following single un-gestured commands. She can imitate a vertical line, jump in place, and broad jump. She is able to wash and dry her hands, and put on a t-shirt. In your office, she points to your stethoscope, and when you hand it to her she smiles at you and places it on her father’s chest.

You most strongly suspect:
A. Mental Retardation
B. Autistic Spectrum Disorder
C. Mixed receptive/expressive language disorder
D. Hearing Impairment
E. Environmental under-stimulation
Mental R
etardation
Autistic S
pectrum Diso
rder
Mixe
d rece
ptive/exp
ressi..
Hearing Im
pairment
Environmenta
l under-s
ti...
7%
21%
0%
50%
21%

??Your first referral is to:
A. Social service
B. Audiology
C. Psychology
D. Speech and Language Pathology
Social s
ervice
Audiology
Psychology
Speech and La
nguage Pa...
29%
57%
14%
0%
??A 5 year old boy presents for health maintenance. Developmental surveillance reveals that he can copy a circle, knows the adjectives “tired” and “hungry” and can broad jump, but cannot hop in place, draw a person in 3 parts or name 4 colors. You suspect:
A. Learning Disability
B. Mild Intellectual Disability (Mental Retardation)
C. Cerebral palsy
D. Autistic Spectrum Disorder
E. Severe Intellectual Disability
Learn
ing Disa
bility
Mild
Inte
llectu
al Disa
bili..
Cerebral pals
y
Autistic S
pectrum Diso
rder
Severe
Inte
llectu
al Disa
bility
14% 14%
43%
29%
0%
?? Devin has a vocabulary of about 300 words, speaks in 2-3 word combinations and understands and asks simple “what” questions. He can follow simple prepositional commands using “on” and “in”. His age is most likely:
A. 18m
B. 24m
C. 30m
D. 36m
E. 42m
18m 24m 30m 36m 42m
0% 0%
100%
0%0%

??A stranger should be able to understand half of a child’s speech at age:
Remember the rule of fours!
A. 12 months
B. 18 months
C. 24 months
D. 36 months
12 month
s
18 month
s
24 month
s
36 month
s
20%
30%30%
20%
??Three year old Jason is brought by frustrated parents due to constant tantrums. He is hyperactive, impulsive and often does not respond when called. He interacts mostly with adults in his daycare. You note that he grabs mother’s hand to reach a toy from a nearby shelf. Mother reports that he constantly watches “Thomas the Train” videos at home, and carries his toy Thomas figure everywhere. Based on this information, the first assessment tool you would consider would be:
A. Conners III Comprehensive Behavior Rating Scale
B. Wechsler Preschool and Primary Scales of Intelligence III
C. Childhood Autism Rating Scale II Edition
D. Preschool Language Scale V Edition
E. Child Behavior Checklist (CBCL)
Conners III
Comprehensiv
e Behav...
Wec
hsler P
resch
ool and Pr
imary
...
Childhood Autism
Rating S
cale II
E...
Presch
ool Langu
age S
cale V Edition
Child Beh
avior C
hecklist
(CBCL)
33%
17%
33%
0%
17%

??All of the following observations are considered risk factors for an Autism Spectrum Disorder except:
A. Lack of pointing at 12 months
B. Lack of babbling at one year
C. Lack of gaze monitoring at 10 months
D. Echoing phrases at 18 months
Lack
of pointing a
t 12 m
...
Lack
of bab
bling at o
ne year
Lack
of gaz
e monito
ring a...
Echoing phrase
s at 1
8 m...
33%
0%0%
67%

?? An 8 year old second grade boy was referred for evaluation due to academic difficulties. His psychological and psychoeducational evaluations revealed:WISC 4: Full scale IQ = 99,Verbal Comprehension = 85, Perceptual Reasoning = 105, Working Memory = 110, Processing Speed = 108
WIAT 2: Word reading = 92, Reading comprehension = 81 Numerical operations: 98, Math reasoning = 79
The child’s likely diagnosis is:
A. Borderline Intellectual Functioning
B. Learning Disability
C. Attention-deficit/Hyperactivity Disorder
D. Auditory Processing Disorder Bord
erline In
tellectu
al F...
Learn
ing Disa
bility
Attention-deficit
/Hyp
era...
Auditory
Proce
ssing D
iso...
40%
20%20%20%

?? A 9 year old third grade boy is brought to your office by his mother who is distraught about his report card. He is below average in reading and spelling and his teaching states that he does not complete assignments and is distractible in class. He is not a management problem at home other than when it’s time to do his homework. He has friends and excels on the baseball field. An appropriate next step would be:
A. Request completion of parent and teacher Vanderbilt Questionnaires
B. Initiate a trial of methylphenidate
C. Order psychological and psychoeducational testing
D. Refer to Child PsychiatryRequest
completion of p
...
Initiate a tr
ial of m
ethyl...
Order p
sych
ological a
nd ...
Refer to Child
Psych
iatry
20% 20%20%
40%

?? A distraught mother phones you asking for advice. She met with her 9 year old son’s teacher who states that your patient Johnny does not listen, talks back, and recently has been physically lashing out at other children. He is in jeopardy of repeating the 4th grade. Mother wonders whether a trial of “that medication my nephew takes that starts with r” would be helpful. You conclude:
A. Johnny’s behavior is most consistent with the lack of impulse control associated with ADHD.
B. Johnny’s behavior is likely to meet criteria for a disorder often co-morbid with ADHD, but not consistent with ADHD alone.
C. Johnny is also likely to be cruel to animals, to steal and to run away from home.
D. Johnny’s behavior is consistent with the general class of “internalizing” behaviors.
Johnny’s behav
ior is m
ost co
nsis...
Johnny’s behav
ior is lik
ely to
mee
...
Johnny is als
o likely
to be cr
uel to...
Johnny’s behav
ior is co
nsisten
t wi..
43%
14%14%
29%
Related Documents











