CLIN. RESEARCH ®. AFFAIRS, 16(1&2), 1-1 1 (1999) Development of the First Clinical Classification of Medications Used during Lactation and the Evaluation of 1380 Drugs Gamal Hussein, Pharm.D. and Fathy Mohamed, M.D. Northeast Louisiana University and Medical Center of Louisiana,at New Orleans. Department of Pharmacy. 1532 Tulane Avenue, New Orleans, LA 701 12 ABSTRACT The infant may be recognized as the unintended recipient of drugs administered to the lactating mother. Our objective is to create a practical classification and to provide health care practitioners with the most updated data on drug use during lactation. Data on more than one thousand drugs have been collected from published medical literature. Data include drug excretion into breast milk, possible adverse effects on the infant, as well as the compatibility of the drug with breast-feeding. Each drug is represented by two letters and symbols to identify the aforementioned information. The first letter indicates compatibility with breast-feeding, which is denoted by C (Compatible), I (Incompatible), or U (Unknown). The second letter indicates Current Addresses: Gamal Hussein, Pharm.D. Associate Professor of Pharmacy, Coordinator of Post-Graduate Program in Clinical Pharmacy and Pharmacology, Northeast Louisiana University-School of Pharmacy and the Medical Center of Louisiana, New Orleans, Louisiana, USA Fathy Mohamed, M.D. Research Fellow, Northeast Louisiana University and the Medical Center of Louisiana, New Orleans, Louisiana, USA and OBGYN Specialist, AL-Galaa Maternity Teaching Hospital, Cairo, Egypt. 1 Copyright Q 1999 by Marcel Dekker, Inc. www .dekker.com Clinical Research and Regulatory Affairs Downloaded from informahealthcare.com by South College on 02/27/13 For personal use only.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLIN. RESEARCH ®. AFFAIRS, 16(1&2), 1-1 1 (1999)
Development of the First Clinical Classification of Medications Used during Lactation and the Evaluation of 1380 Drugs
Gamal Hussein, Pharm.D. and Fathy Mohamed, M.D. Northeast Louisiana University and Medical Center of Louisiana,at New Orleans. Department of
Pharmacy. 1532 Tulane Avenue, New Orleans, LA 701 12
ABSTRACT
The infant may be recognized as the unintended recipient of drugs administered to the
lactating mother. Our objective is to create a practical classification and to provide health care
practitioners with the most updated data on drug use during lactation. Data on more than one
thousand drugs have been collected from published medical literature. Data include drug
excretion into breast milk, possible adverse effects on the infant, as well as the compatibility of
the drug with breast-feeding. Each drug is represented by two letters and symbols to identify the
aforementioned information. The first letter indicates compatibility with breast-feeding, which is
denoted by C (Compatible), I (Incompatible), or U (Unknown). The second letter indicates
Current Addresses:
Gamal Hussein, Pharm.D. Associate Professor of Pharmacy, Coordinator of Post-Graduate Program in Clinical Pharmacy and Pharmacology, Northeast Louisiana University-School of Pharmacy and the Medical Center of Louisiana, New Orleans, Louisiana, USA
Fathy Mohamed, M.D. Research Fellow, Northeast Louisiana University and the Medical Center of Louisiana, New Orleans, Louisiana, USA and OBGYN Specialist, AL-Galaa Maternity Teaching Hospital, Cairo, Egypt.
1
Copyright Q 1999 by Marcel Dekker, Inc. www .dekker.com
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.

2 HUSSEIN AND MOHAMED
excretion into breast milk, which is denoted by e (excreted), n (not excreted), or u (unknown).
The symbols indicate expected adverse effects and their severity. Fifty-seven percent of the
drugs evaluated were compatible and twenty-three percent were incompatible with breast-
feeding; compatibility data on the remaining twenty percent were uncertain. While eighteen
percent of the drugs evaluated were excreted into breast milk, less than one percent were not
excreted, and data on the remaining eighty- one percent were not reported. The presented data,
simplified in a readily attainable pattern, offer a valuable source of knowledge for the healthcare
provider as well as the patient.
Introduction Breast-feeding is good for babies as well as for mothers; it is perfectly suited to nourish
and protect infants. Breast-fed infants have lower rates of hospital admissions, infections, allergies, and other medical problems than bottle-fed babies ( I -? . While the American Academy of Pediatrics recommends that babies be breast-fed for 6 to 12 months, less than 70% of American mothers breast-feed their babies in the hospital and less than 20% are still breast-feeding when their babies are 6 months old (*). While government and private health experts are working to raise those numbers, the compatibility of many medications with breast-feeding is not clear. The infant may be recognized as the unintended recipient of medications received by the lactating mother. Data on drug compatibility with breast-feeding are often not complete and appear confusing to clinicians. Currently, there is no standard format for conveying information related to drug compatibility with lactation, drug's excretion into breast milk or recommended actions if breast-feeding is continued. Information resources commonly utilized by healthcare providers include product package inserts, books, and statements by associations such as the American Academy of Pediatrics.
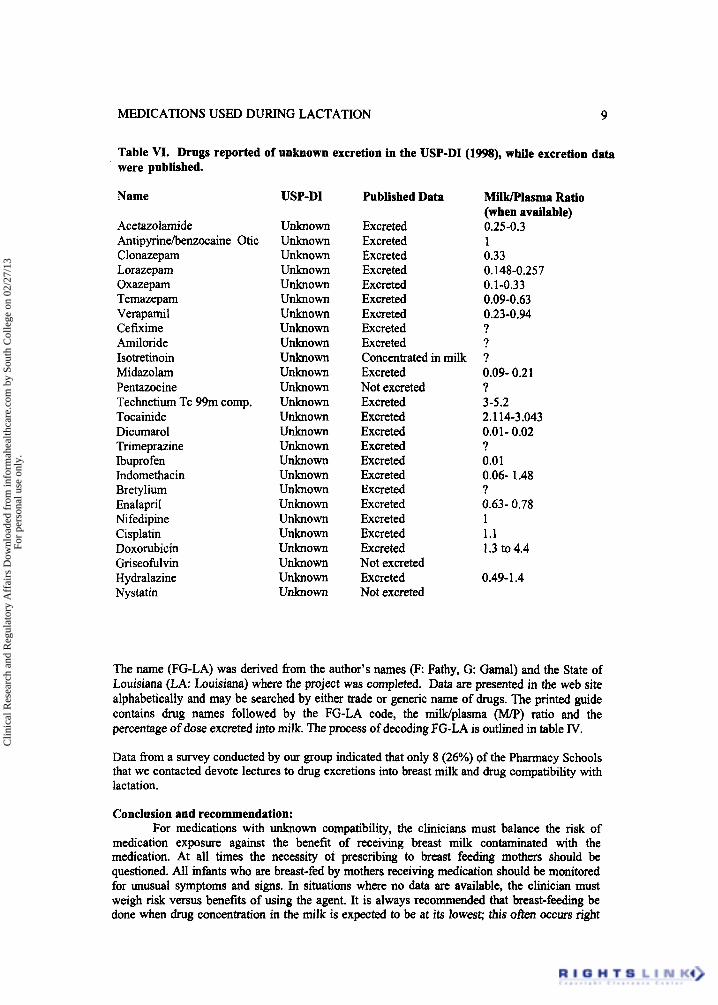
Not all information included in package inserts is updated; this information may reflect only the data available at the time the drug received marketing approval. The FDA does not demand the pharmaceutical manufacturer's updating of the package insert with regard to data on drug excretion into breast milk. As an illustration of this point, the package insert for hydralazine, a drug that was introduced to the market more than 20 years ago, still includes outdated information that indicates no knowledge of excretion into breast milk. However, available data indicates that hydralazine is excreted into breast milk at a milWplasma ratio of 0.49 to 1.4. Information included in the Physicians' Desk Reference (PDR) and in the United States Pharmacopoeia Drug Information for the Healthcare Provider (USP-DI) still indicates the unknown excretion of hydralazine (941) .
Breast-feeding information and drug compatibility data from books, as well as recommendations from associations, are often not updated (I2), Commonly used books do not provide data on all available drugs; they provide only a summary of some published data without critical assessment or classification. The American Academy of Pediatrics (AAF') Committee on Drugs meets periodically and issues statement on the safety of certain drugs during lactation ( I 3 ) . The most recent recommendation includes several lists of drugs and their anticipated effects. However, the number of drugs evaluated so far is less than 20% of available medications on the market (see table I).
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.

MEDICATIONS USED DURING LACTATION 3
Table I. Lists of tables of drugs evaluated by the Academy of Pediatrics-Committee on Drugs.
Pediatrics I994;93: I3 7-1 50
1. 2. 3. 4. 5.
6. 7.
Drugs that are contraindicated during breast feeding (10 drugs) Drugs of abuse: contraindicated during breast feeding (6 drugs) Radioactive compounds that require temporary cessation of breast feeding (8 drugs) Drugs whose effect on the nursing infant is unknown but may be of concern (24 drugs) Drugs that have been associated with significant effect on some nursing infants and should be given to the nursing mother with caution (6 drugs) Maternal medication usually compatible with breast feeding (1 54 drugs) Food and environmental agents: Effects on breast-feeding (17 drugs)
The infant's reaction to its mother's intake of drugs is dependent on factors related to the drug itself, as well as factors related to the mother and the infant. Table 11 was prepared to familiarize readers with these factors (14-19). MilkPlasma (M/P) ratio is a factor that describes drug concentration in the mother's plasma in relation to the concentration in breast milk. M/P ratio depends on drug factors (such as degree of ionization, lipid solubility, molecular weight, and protein binding) and on mother factors, such as weight-dependent volume of distribution and clearance. It is important to note that M / P ratio is not a fixed value; it varies during the dosing interval. Plasma concentration is at its highest value after drug intake (at the beginning of the dosing interval), while milk concentration is at its lowest value before receiving the dose (at the end of the dosing interval). Reports of M / P ratio that do not include time of measuring concentrations should be evaluated with caution since these values may be misleading. M / P ratio can be helpful in estimating the infant's exposure to a drug. However, this parameter, on its own, does not predict the infant's response to the drug. Pharmacokinetic parameters (such as absorption distribution, metabolism and elimination) related to infant's handling of the drug and pharmacodynamic parameters (organ and receptor's sensitivity) related to the drug effect on the infant's body must be considered.
It0 and Koren introduced the exposure index for expressing an infant's exposure to drugs in breast milk (*O). The exposure index is based on milWplasma ratio, expected infant's clearance of the drug, and the expected amount of milk intake by the infant. The exposure index represents a good method to estimate infant exposure. However, its clinical application is complicated by many factors. Infant's clearance of many drugs is unknown. MilWplasma ratio reported in the literature may vary by many folds within the same study, since drug concentration in milk depends on the time it was measured in relation to the time of dose that was received by the mother. While the amount of milk intake by the infant may be predicted in some mothers, it may be different in mothers who supplement infants with additional sources of food. Additionally, because the composition of milk changes during the same feeding, the time spent on one breast might also influence the amount of drug ingested. It is important to note that the exposure index is a pharmacokinetic parameter that does not predict the infant's response (pharmacodynamics) to the estimated exposure. Adverse drug effects depend on the pharmacokinetics of the drugs and on individual susceptibility. The adverse drug effects that are dose-related reflect the extension of the pharmacological activities of each drug, are predictable and can be monitored. The effects that are not dose-related are said to be idiosyncratic and are not predictable.
Our objectives were 1) to create a practical classification that can be utilized for a standardized method to communicate findings related to drug effects on infants and mother as well as drug excretion into milk, and 2) to evaluate published data on more than 1300 drugs. The ultimate goal was to produce a handy reference for safe breast-feeding.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.

4 HUSSEIN AND MOHAMED
Table 11. Factors influencing infant's response to mother's drug intake
1. Maternal pharmacokinetics (drug handling by the body): A. Absorption B. Distribution C. Metabolism D. Elimination
2. Milk-to-Plasma drug concentration Ratio (M/P): A. Physiochemical Properties of Drugs
Proteinbound The degree of ionization
0 The liposolubility Molecular weight
B. Composition of milk and physiology of the breast Infant suckling pattern Time of feeding The number of feedings The amount of milk ingested The time spent on the breast
3. Infant pharmacokinetics (drug handling by the body) A. Absorption B. Distribution C. Metabolism D. Elimination
4. Infant pharmacodynamics (susceptibility to drug effects) and pharmacogenetics
Methods Data on 1380 drugs have been collected from published medical literature. Data included
drug excretion into breast milk, reported and possible adverse effects on the infant, as well as the compatibility of the drug with breast-feeding. Data from over 2000 articles and several reference books were reviewed and critically evaluated. Only data from human studies on excretion of specific agents, not classes of medications, were utilized. The long list of articles reviewed is available at our web sites at http://www.PhoneMed.comRGLA and at http:/Jwww.nlu.edu/pharmacylhussein.
Table I11 includes information entered in the Data Collection Sheet. The two investigators evaluated data for compatibility decision. A drug was considered compatible if it had been used by lactating mothers and no problems were reported or only mild to moderate side effects were reported. A drug was considered incompatible if serious problems were reported following its use by lactating mothers. Additionally, some drugs were considered incompatible if serious drug- related or disease-related problems were anticipated following its use. Drug-related problems were anticipated &om drugs of abuse, such as heroin. Disease-related problems were anticipated from anti-HIV drugs since infants may be exposed to the virus through breast-feeding. It is understood that cessation of breast-feeding while receiving incompatible drugs may occur a few days after discontinuing medications. Drug compatibility was considered unknown when no data on drug use were retrieved. It is understood that the benefits of using a drug must always be weighed against potential risks.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.
MEDICATIONS USED DURING LACTATION 5
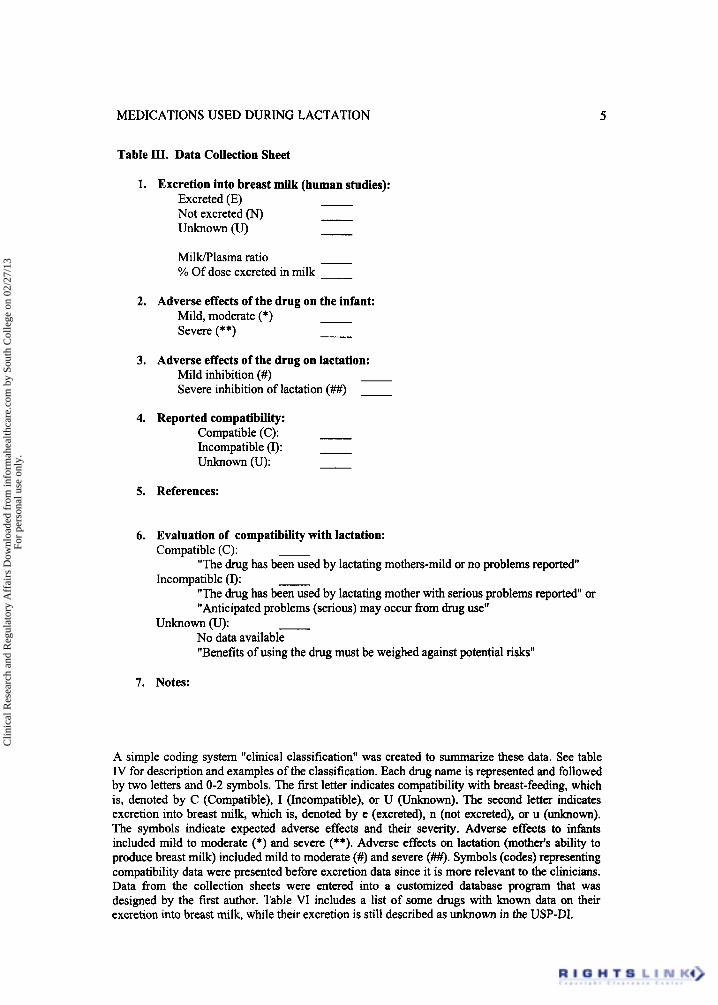
Table III. Data Collection Sheet
1. Excretion into breast milk (human studies): Excreted (E) - Not excreted (N) - Unknown (U) -
MilWlasma ratio - % Of dose excreted in milk -
2. Adverse effects of the drug on the infant: Mild, moderate (*) - Severe (**) -
3. Adverse effects of the drug on lactation: Mild inhibition (#) - Severe inhibition of lactation (##) -
4. Reported compatibility: Compatible (C): - Incompatible (I): Unknown (U): -
5. References:
6. Evaluation of compatibility with lactation: Compatible (C): -
Incompatible (I): - "The drug has been used by lactating mothers-mild or no problems reported"
"The drug has been used by lactating mother with serious problems reported" or "Anticipated problems (serious) may occur fi-om drug use"
No data available "Benefits of using the drug must be weighed against potential risks"
Unknown 0: -
7. Notes:
A simple coding system "clinical classification" was created to summarize these data. See table IV for description and examples of the classification. Each drug name is represented and followed by two letters and 0-2 symbols. The first letter indicates compatibility with breast-feeding, which is, denoted by C (Compatible), I (Incompatible), or U (Unknown). The second letter indicates excretion into breast milk, which is, denoted by e (excreted), n (not excreted), or u (unlrnown). The symbols indicate expected adverse effects and their severity. Adverse effects to infants included mild to moderate (*) and severe (**). Adverse effects on lactation (motherk ability to produce breast milk) included mild to moderate (#) and severe (##). Symbols (codes) representing compatibility data were presented before excretion data since it is more relevant to the clinicians. Data from the collection sheets were entered into a customized database program that was designed by the first author. Table VI includes a list of some drugs with known data on their excretion into breast milk, while their excretion is still described as unknown in the USP-DI.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.
6 HUSSEIN AND MOHAMED
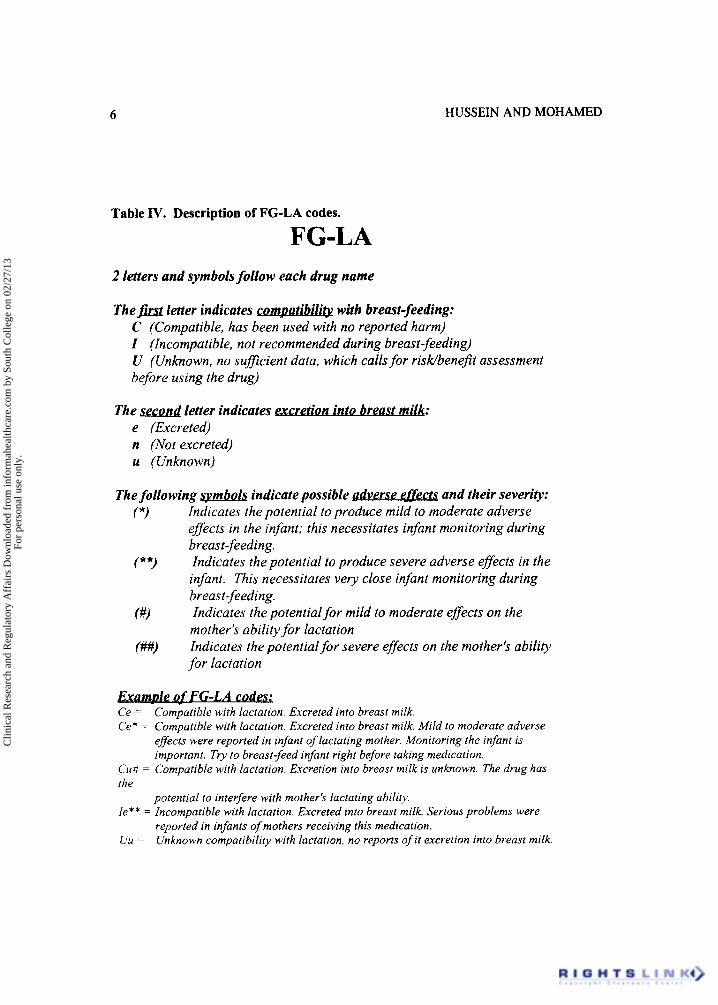
Table IV. Description of FG-LA codes.
FG-LA 2 letters and symbols follow each drug name
with breast-feeding: The first letter indicates cornpa&& . .. C (Compatible, has been used with no reported harm) I (Incompatible, not recommended during breast-feeding) U (Unknown, no sufficient data, which calls for risk/bene$t assessment before using the drug)
. . The second letter indicates acretion into b reast milk: e (Excreted) n (Not excreted) u (Unknown)
The following spbo l s indicate possible adverse effects and their severity: Indicates the potential to produce mild to moderate adverse effects in the infant; this necessitates infant monitoring during breast-feeding. Indicates the potential to produce severe adverse effects in the infant. This necessitates very close infant monitoring during breast-feeding. Indicates the potential for mild to moderate effects on the mother's ability for lactation Indicates the potential for severe effects on the mother's ability for lactation
(*)
(**)
(#I
(##)
FG-LA c o d a Ce = Ce* = Compatible with lactation. Excreted into breast milk. Mild to moderate adverse
Compatible with lactation. Excreted into breast milk.
effects were reported in infant of lactating mother. Monitoring the infant is important. Tiy to breast-feed infant right before taking medication.
Cu# = Compatible with lactation. Excretion into breast milk is unknown. The drug has the
Ie** = Incompatible with lactation. Excreted into breast milk. Serious problems were
Uir =
potential to intevfere with mother's lactating ability.
reported in infants of mothers receiving this medication. Unknown compatibility with lactation, no reports of it excretion into breast milk.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.
MEDICATIONS USED DURING LACTATION 7
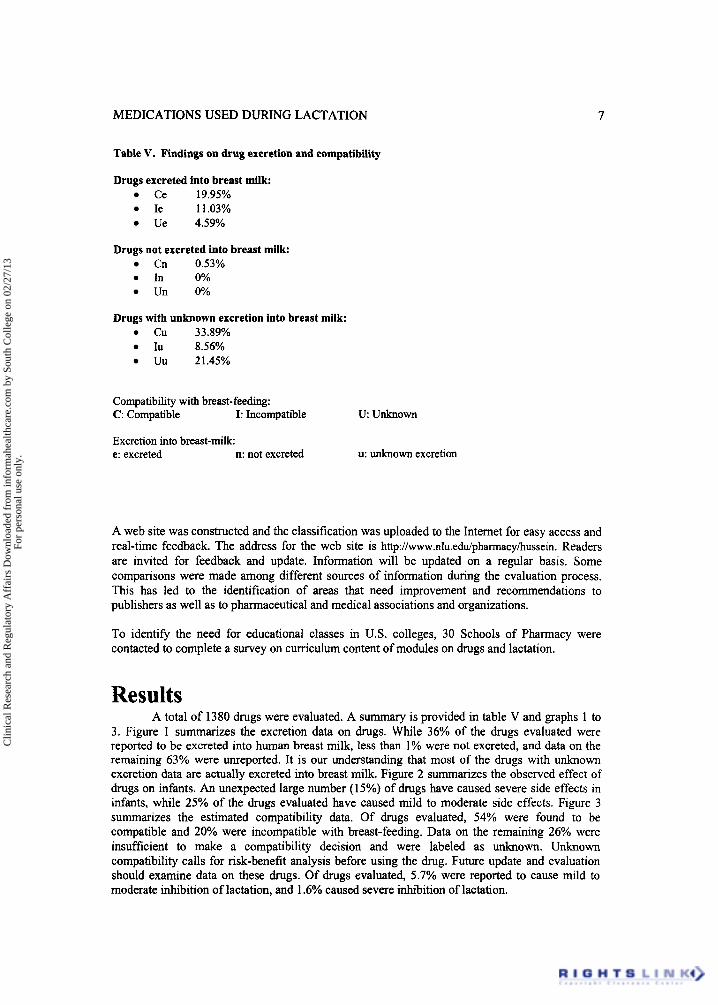
Table V. Findings on drug excretion and compatibility
Drugs excreted into breast milk Ce 19.95% Ie 1 1.03% Ue 4.59%
Drugs not excreted into breast milk Cn 0.53% In 0% Un 0%
Drugs with unknown excretion into breast milk: Cu 33.89% Iu 8.56% Uu 21.45%
Compatibility with breast-feeding: C: Compatible I: Incompatible
Excretion into breast-mik e: excreted n: not excreted
u unknown
u: unknown excretion
A web site was constructed and the classification was uploaded to the Internet for easy access and real-time feedback. The address for the web site is http://www.nlu.edu/pharmacy/hussein. Readers are invited for feedback and update. Information will be updated on a regular basis. Some comparisons were made among different sources of information during the evaluation process. This has led to the identification of areas that need improvement and recommendations to publishers as well as to pharmaceutical and medical associations and organizations.
To identify the need for educational classes in US. colleges, 30 Schools of Pharmacy were contacted to complete a survey on curriculum content of modules on drugs and lactation.
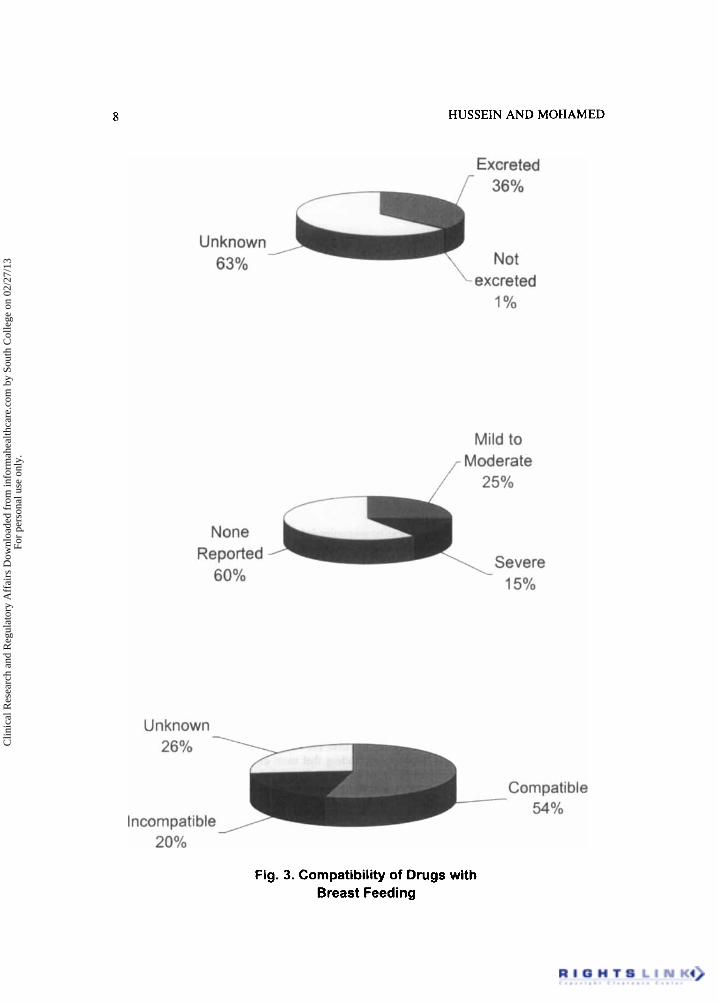
Results A total of 1380 drugs were evaluated. A summary is provided in table V and graphs 1 to
3. Figure 1 summarizes the excretion data on drugs. While 36% of the drugs evaluated were reported to be excreted into human breast milk, less than 1% were not excreted, and data on the remaining 63% were unreported. It is our understanding that most of the drugs with unknown excretion data are actually excreted into breast milk. Figure 2 summarizes the observed effect of drugs on infants. An unexpected large number (15%) of drugs have caused severe side effects in infants, while 25% of the drugs evaluated have caused mild to moderate side effects. Figure 3 summarizes the estimated compatibility data. Of drugs evaluated, 54% were found to be compatible and 20% were incompatible with breast-feeding. Data on the remaining 26% were insufficient to make a compatibility decision and were labeled as unknown. Unknown compatibility calls for risk-benefit analysis before using the drug. Future update and evaluation should examine data on these drugs. Of drugs evaluated, 5.7% were reported to cause mild to moderate inhibition of lactation, and 1.6% caused severe inhibition of lactation.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.
8 HUSSEIN AND MOHAMED
Excreted 36%
Unknown 63% Not
excreted 1 Yo
Mild to ,,- M;Fo;oate
/---
Severe
None Reported
60% 15%
Unknown
Compatible 54%
26%
Incompatible 20%
Fig. 3. Compatibility of Drugs with Breast Feeding
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.
MEDICATIONS USED DURING LACTATION 9
Table VI. Drugs reported of unknown excretion in the USP-DI (1998), while excretion data were published.
Name
Acetazolamide Antipyrinehenzocaine Otic Clonazepam Lorazepam Oxazepam Temazepam Verapamil Cefixime Amiloride Isotretinoin Midazolam Pentazocine Technetium Tc 9% comp. Tocainide Dicumarol Trimeprazine Ibuprofen Indomethacin Bretylium Enalapril Ni fedipine Cisplatin Doxorubicin Griseofulvin H ydralazine Nystatin
USP-DI
unknown unknown Unknown Unknown unknown Unknown unknown unknown unknown unknown Unknown unknown unknown unknown unknown unknown Unknown Unknown Unknown Unknown Unknown Unknown Unknown Unknown unknown Unknown
Published Data
Excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Concentrated in milk Excreted Not excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Excreted Not excreted Excreted Not excreted
MilWPlasma Ratio (when available) 0.25-0.3 1 0.33 0.148-0.257 0.1-0.33 0.09-0.63 0.23-0.94 ? ? ? 0.09- 0.21 ? 3-5.2 2.114-3.043 0.01- 0.02 ? 0.01 0.06- 1.48 ? 0.63- 0.78 1 1.1 1.3 to 4.4
0.49- 1.4
The name (FG-LA) was derived fiom the author’s names (F: Fathy, G: Gamal) and the State of Louisiana (LA: Louisiana) where the project was completed. Data are presented in the web site alphabetically and may be searched by either trade or generic name of drugs. The printed guide contains drug names followed by the FG-LA code, the milldplasma @UP) ratio and the percentage of dose excreted into milk. The process of decoding FG-LA is outlined in table IV.
Data from a survey conducted by our group indicated that only 8 (26%) of the Pharmacy Schools that we contacted devote lectures to drug excretions into breast milk and drug compatibility with lactation.
Conclusion and recommendation: For medications with unknown compatibility, the clinicians must balance the risk of
medication exposure against the benefit of receiving breast milk contaminated with the medication. At all times the necessity ot prescribing to breast feeding mothers should be questioned. All infants who are breast-fed by mothers receiving medication should be monitored for unusual symptoms and signs. In situations where. no data are available, the clinician must weigh risk versus benefits of using the agent. It is always recommended that breast-feeding be done when drug concentration in the milk is expected to be at its lowest; this often occurs right
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.

10 HUSSEIN AND MOHAMED
before getting the dose (at the end of the dosing interval). Where information is available, choose the drug which appears in the least concentration in breast milk and with short half-life and avoid breast-feeding when milk drug concentrations are at their peak (advise to breast- feed before the dose).
In conclusion, we have developed a simple clinical classification for drugs used during lactation and have evaluated over 1380 drugs. We are planning to continue updating the information collected. The status of drugs may be changed as more information becomes available. We hope that a similar classification is discussed for drugs used during pregnancy since the current classifications are very complicated, research-oriented and do not provide clinicians with practical recommendations. Education to both healthcare providers and consumers is essential for better understanding of safe breast-feeding. Implementing lecturers in the pharmacokinetics, pharmacodynamics and patient outcomes of breast-feeding in medical, pharmacy and nursing schools should be encouraged.
It is clear that more research and documentation are needed and should be encouraged. It is of interest that while the American Academy of Pediatrics Committee on Drugs reported no cases of antidepressant-related side effects to infants, we have found 26 cases of moderate to serious side effects ( I 3 ) . Indeed, the package insert of fluoxetine lists two such cases. The American Academy of Pediatrics Committee on Drugs has issued 3 recommendations since 1983 (1983, 1989, and 1994). The committee may need to issue recommendations more frequently. It will be beneficial if all pharmaceutical manufacturers update the package inserts with information on drug use during lactation. The Food and Drug Administration (FDA) may play an important role promoting such a recommendation. It is also important to encourage healthcare providers and consumers to report infant response to mother's intake of medications. Complications of drug use during lactation should be reported as adverse drug reactions to the FDA MedWatch Program. Experiences that are reported to our web site would be very beneficial for future assessment and safe breast-feeding. We would like to take this opportunity to call for the establishment of a registry for drug use during lactation. We are pleased to present this work and encourage constructive feedback.
Acknowledgement: The authors would like to thank Barbara Esquerre for her excellent technical support and editing input.
References:
1.
2.
3.
4.
5 .
6 .
?.
A Wright, S Rice, S Wells. Changing hospital practices to increase the duration of breast-feeding. Pediatrics 1996; 97: 669-675 Wright AL, Baure M, Naylor A, Sutcliffe, Clark L. Increasing breast-feeding rates to reduce infant illness at the community level. Pediatrics 1998;lOl: 837-844. Duffy LC, Faden H, Wasielewski R, Wolf J, Krystofik, Williamsville T. Exclusive breast-feeding protects against bacterial colonization and day care exposure to otitis media. Pediatrics 1997;100:e7 Hylander MA, Strobino DM, Dhanireddy R. Human milk feedings and infection among very low birth weight infants. Pediatrics 1998;102: e38 Clemens JD, Rao MR, Chakraborty J, Yunus M, Ali M, Kay B, Frederick Van Loon PL, Naficy A, Sack DA. Breast-feeding and the risk of life-threatening Enterotoxigenic Escherichia Coli diarrhea in Bangladeshi infants and children. Pediatrics 1997; 100: e2 Dewey KG, Peerson JM, Brown KH, Krebs NF, Michaelsen KF, Persson LA, Salmenpera L, Whitehead RG, Yeung DL. Growth of breast-fed infants deviates from current reference data: a pooled analysis of US, Canadian, and European data sets. World Health Organization Working Group on Infant Growth. Pediatrics 96:495-503. Scariati PD, Grummer-Straw LM, Fein SB. A Longitudinal Analysis of Infant Morbidity and the Extent of %Teast-feeding in the United States. Pediatrics 99: e5.
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.

MEDICATIONS USED DURING LACTATION 11
8. Ryan AS. The Resurgence of Breast-feeding in the United States. Pediatrics 1997; 99:p. el2 9. Hydralazine Package Insert 10. Physicians' Desk Reference, 1998 1 1. United states Pharmacopoeia - Drug Information for the Healthcare Providers, 1998 12. Hussein G, Mohamed F. FG-LA: the first classification of drugs used during lactation. Abstract
Presented at the 126" Annual Meeting of American Public Health Association, November 1998, Washington, D.C. AJPH 1998;314
13. The Committee on drugs, Academy of Pediatrics (AAP): The transfer of drugs and other chemicals into human breast milk, Pediatrics 1994;93:137-150
14. Wilson JT, Brown RD, Cherek DR, et al: Drug excretion in human breast: principles, pharmacokinetics and projected consequences. Clin Pharmacokinet 1980;5: 1
15. Taddio A, It0 S. Drug use and Lactation. In Koren G (ed): Maternal-Fetal Toxicology, Ed 2. New York, Dekker, 1994
16. Morris FH, Brewer ED, Spedale SB, et al: Relationship of human milk pH during course of lactation to concentrations of citrates and fatty acids. Pediatrics 1986;78:458
17. Prentice A, Prentice AM, Whitehead RG. Breast- milk fat concentrations of rural African women. I. Short term variations within individuals. Br J Nutr 1981;45: 483
18. Besunder JB, Reed MD, and BLUMER JL: Principles of drug biodisposition in the neonate. A critical evaluation of the pharmacokinetics-pharmacodynamics interface (partl). Clin pharmacokinet 1988; 14: 189
19. Atkinson HC, Begg EJ. Prediction of drug distribution into human milk from physicochemical characteristics. Clin Pharmacokinet 1990;18(2): 15 1-167
20. Ito S, Koren G. A novel index for expressing exposure of the infant to drugs in breast milk. Br J Clin Pharmacol 1993;38:99-102
Clin
ical
Res
earc
h an
d R
egul
ator
y A
ffai
rs D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y So
uth
Col
lege
on
02/2
7/13
For
pers
onal
use
onl
y.
Related Documents











