DEVELOPMENT OF THE RESPIRATORY SYSTEM Name - A dhish Gautam Group - 216

Development of repiratory system By Adhish Gautam
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DEVELOPMENT OF THE
RESPIRATORY SYSTEMName- Adhish Gautam
Group-216

FORMATION OF THE LUNG BUDS
• Embryo is 4 weeks old
• respiratory diverticulum (lung bud) appears as an
outgrowth from the ventral wall of the foregut .
• Dependent upon: retinoic acid (RA) produced by
adjacent mesoderm.
• Epithelium of the internal lining of the larynx, trachea;
bronchi; lungs, is Endoderm
• The cartilaginous; muscular,; connective tissue
components of the trachea; lungs are splanchnic
mesoderm ( that surrounds the foregut)

A Embryo of approximately 25 days' gestation showing the relation
of the respiratory diverticulum to the heart, stomach, and liver.
B. Sagittal section through the cephalic end of a 5-week embryo
showing the openings of the pharyngeal pouches and the
laryngotracheal orifice.

FORMATION OF THE LUNG BUDS -2
• The diverticulum expands caudally, and two longitudinal
ridges, the tracheoesophageal ridges, separate it from the
foregut.
• These ridges fuse to form the tracheoesophageal septum
• The respiratory primordium communicates with the pharynx
through the laryngeal orifice
• Foregut Divides into:
1) Dorsal portion: Oesophagus.
2) Ventral portion: Trachea & Lung Buds.
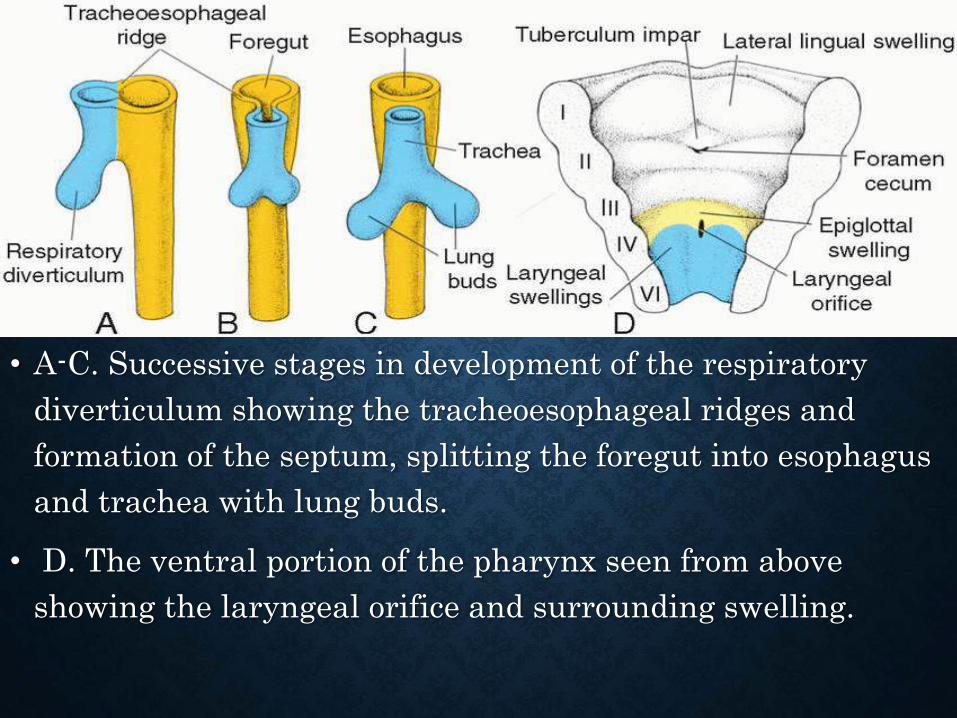
• A-C. Successive stages in development of the respiratory
diverticulum showing the tracheoesophageal ridges and
formation of the septum, splitting the foregut into esophagus
and trachea with lung buds.
• D. The ventral portion of the pharynx seen from above
showing the laryngeal orifice and surrounding swelling.
TRACHEOESOPHAGEAL FISTULAS (TEFS)
• Abnormalities in partitioning of the esophagus and
trachea by the tracheoesophageal septum ensuing
Esophageal Atresia with or w/o TEFs.
• Approx. 1/3,000 births
• Blind pouch and the lower segment forming a
fistula with the trachea (90% of cases)
• Isolated Oesophageal Atresia
• H-type TEF without oesophageal Atresia

• A. most frequent
abnormality (90% of
cases) occurs with the
upper oesophagus
ending in a blind
pouch and the lower
segment forming a
fistula with the
trachea.
• B. Isolated
oesophageal atresia
(4% of cases).
• C. H-type
tracheoesophageal
fistula (4% of cases).
• D,E. Other variations
(each 1% of cases).

BUT THESE ABNORMALITIES ARE ASSOCIATED WITH OTHER BIRTH DEFECTS
• Including cardiac abnormalities (33% of cases)
• TEFs are a component of the VACTERL Group:
• Vertebral anomalies
• Anal Atresia
• Cardiac Defects
• Tracheoesophageal Fistula
• Esophageal Atresia,
• Renal Anomalies
• Limb Defects

• A, Tracheoesophageal fistula (TEF) in a 17-week male fetus. The upper esophageal segment
ends blindly (pointer).
• B, Contrast radiograph of a newborn infant with TEF. Note the communication (arrow)
between the esophagus (E) and trachea (T).

LARYNX
• Internal lining: originates from endoderm.
• Cartilages; muscles originate from mesenchyme of
the 4th & 6th pharyngeal arches.
• Laryngeal orifice changes from a sagittal slit to a T-
shaped opening.
• Caracteristic adult shape of the laryngeal orifice
can be recognized when mesenchyme of the two
arches transforms into the thyroid; cricoid;
arytenoid cartilages.

• Laryngeal orifice and surrounding swellings
at successive stages of development:
• A. 6 weeks.
• B. 12 weeks

TRACHEA & BRONCHI & LUNGS
• The bronchial buds forms
• 5th week, each of these buds enlarges
to form right and left main bronchi.
• The right forms three secondary
bronchi.
• The left forms two.

• Stages in development of the trachea and lungs:
• A. 5 weeks.
• B. 6 weeks.
• C. 8 weeks
FURTHER DEVELOPMENT
• Subsequent growth in caudal and lateral directions, the
lung buds expand into the body cavity .
• The spaces for the lungs, which are the
pericardioperitoneal canals, are narrow.
• The mesoderm[covers outside of the lung] develops into
the visceral pleura.
• The somatic mesoderm layer[covering the body wall
from the inside] becomes the parietal pleura
• The space between the parietal and visceral pleura is
the pleural cavity .
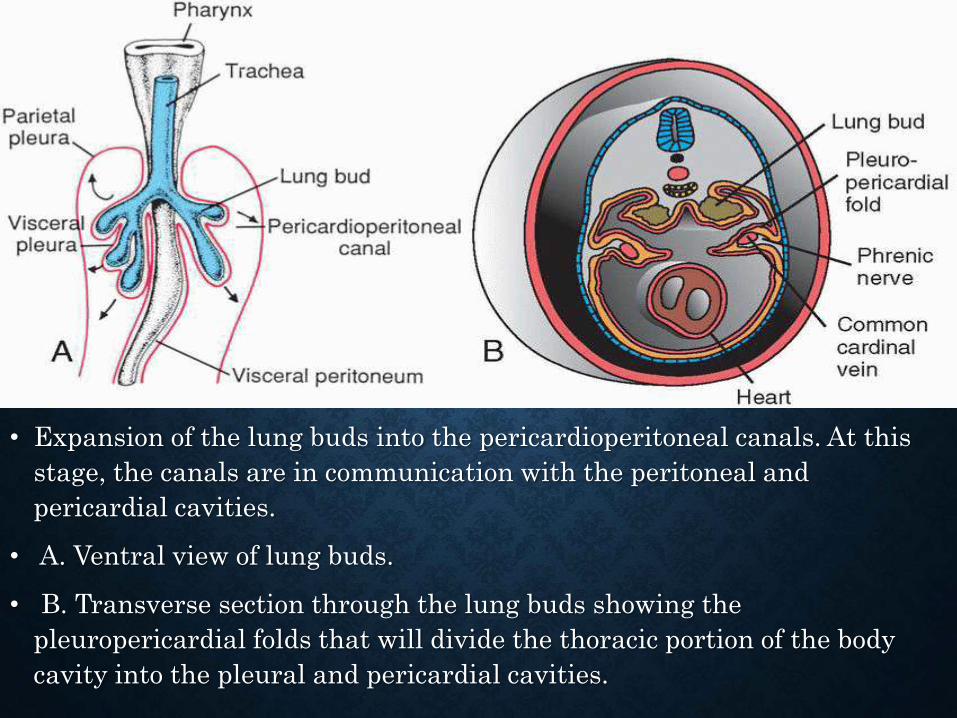
• Expansion of the lung buds into the pericardioperitoneal canals. At this
stage, the canals are in communication with the peritoneal and
pericardial cavities.
• A. Ventral view of lung buds.
• B. Transverse section through the lung buds showing the
pleuropericardial folds that will divide the thoracic portion of the body
cavity into the pleural and pericardial cavities.

• pericardioperitoneal
canals separate from
the pericardial and
peritoneal cavities,
• the lungs expand in
the pleural cavities.
• Note the visceral
and parietal pleura
and definitive
pleural cavity. The
visceral pleura
extends between the
lobes of the lungs.

SURFACTANT
• Important for survival of the premature infant.
• When insufficient, the air-water (blood) surface
membrane tension becomes high, bringing great
risk that alveoli will collapse during expiration.
• Resulting in respiratory distress syndrome (RDS)
• Common cause of death in the premature infant.

THE END
Related Documents











