Psychotherapy Research 9(2) 127-153, 1999 DEVELOPMENT OF PSYCHOTHERAPISTS: CONCEPTS, QUESTIONS, AND METHODS OF A COUABORATIVE INTERNATIONAL STIJDY David Orlinsky M. Helge Rennestad Paul Gerin Ulrike Willutzki Alice Dazord Hansruedi Ambühl john Davis Marcia Davis jean-Francois Botennans Manfred Cierpka o ...• o N and Nicoletta Aapro Peter Buehheim Sue Bae Christine Davidson Eric Friis-]orgensen Eunsun joo Ekaterina Kalmykova Jan Meyerberg Terry Northeut Barbara Parks Elena Scherb Thomas Sehröder Gaby Shefler Dan Stiwne Seott Stuart Margarita Tarragona Antonio Braneo Vaseo Hadas Wiseman and the SPR Collaborative Research Network N N M N M ...• r-- o o N The aim of this international study is to examine the nature, correlates, and perceived determinants of development among professional psycho- therapists from different countries and cultures at all career levels, trained in different professions and theoretical orientations. Psychotherapeutic development was conceptualized and assessed from several perspectives, including concurrent and retrospective reports by therapists and cross- sectional and longitudinal analyses of therapists' practices and experiences. This paper presents the main questions guiding the study, defines its core concepts, introduces the survey instrument, describes data collection pro- cedures, and reports descriptive and scale development data from a multinational data base of nearly 3800 therapists. Analyses provide evi- dence for the reliability and validity of direct and indirect measures of retrospected career development and currently experienced development, and their applicability to diverse groups of psychotherapists. The work of the first author (David Orlinsky) was supported in part by N.I.M.H. Grant R-0142901-01. The Portuguese data collection was supported in part by grant PCSH/C/PSII345/92 to Antonio B. Vasco, from the Portuguese National Board for Scientific and Technological Research. Authors' affiliations follow: David Orlinsky, Universiry of Chicago, Hansruedi Ambühl, University of Bem, M. Helge Rennestad, University of Oslo, lohn Davis, University of Warwick, Paul Gerin, INSERM, Lyon, Marcia Davis, North Warwickshire Health Services, Ulrike Willutzki, Ruhr University-Bochum, 127

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psychotherapy Research 9(2) 127-153, 1999
DEVELOPMENT OF PSYCHOTHERAPISTS:CONCEPTS, QUESTIONS, AND METHODSOF A COUABORATIVE INTERNATIONAL STIJDY
David OrlinskyM. Helge RennestadPaul GerinUlrike WillutzkiAlice Dazord
Hansruedi Ambühljohn DavisMarcia Davisjean-Francois BotennansManfred Cierpka
o...•oN
andNicoletta Aapro Peter BuehheimSue Bae Christine DavidsonEric Friis-]orgensen Eunsun jooEkaterina Kalmykova Jan MeyerbergTerry Northeut Barbara ParksElena Scherb Thomas SehröderGaby Shefler Dan StiwneSeott Stuart Margarita TarragonaAntonio Braneo Vaseo Hadas Wiseman
and the SPR Collaborative Research Network
NN
MN
M...•
r--ooN
The aim of this international study is to examine the nature, correlates,and perceived determinants of development among professional psycho-therapists from different countries and cultures at all career levels, trainedin different professions and theoretical orientations. Psychotherapeuticdevelopment was conceptualized and assessed from several perspectives,including concurrent and retrospective reports by therapists and cross-sectional and longitudinal analyses of therapists' practices and experiences.This paper presents the main questions guiding the study, defines its coreconcepts, introduces the survey instrument, describes data collection pro-cedures, and reports descriptive and scale development data from amultinational da ta base of nearly 3800 therapists. Analyses provide evi-dence for the reliability and validity of direct and indirect measures ofretrospected career development and currently experienced development,and their applicability to diverse groups of psychotherapists.
The work of the first author (David Orlinsky) was supported in part by N.I.M.H. Grant R-0142901-01.The Portuguese data collection was supported in part by grant PCSH/C/PSII345/92 to Antonio B. Vasco,from the Portuguese National Board for Scientific and Technological Research.
Authors' affiliations follow: David Orlinsky, Universiry of Chicago, Hansruedi Ambühl, University ofBem, M. Helge Rennestad, University of Oslo, lohn Davis, University of Warwick, Paul Gerin, INSERM,Lyon, Marcia Davis, North Warwickshire Health Services, Ulrike Willutzki, Ruhr University-Bochum,
127
128 ORLINSKYET AL.
o.-<oN
The study of psychotherapists' characteristics, training, and performance is nearly asold as research on psychotherapy itself (e.g., Fiedler, 1950;Holt & Luborsky, 1958;Kelley & Fiske, 1951; Strupp, 1955a,b; also see Orlinsky & Russell, 1994). Relevantstudies have been reviewed in various works over nearly three decades (e.g., Gurman& Razin, 1977; Meltzoff & Kornreich, 1970), including successive editions of theHandbook 0/Psychotherapy and Bebauior Change (Beutler, Crago, &: Azrimendi, 1986;Beutler, Machado, & Neufeldt, 1994;Matarazzo, 1971, 1978;Matarazzo & Patterson,1986;Parloff,Waskow, & Wolfe, 1978;Truax & Mitchell, 1971).Yet despite this vener-able history, research on the processes and outcomes of various therapies has faroutweighed the study of psychotherapists, both in terms of the number of studiesthat have been done and the attention accorded to them. There is a strong presump-tion in psychotherapy research that treatment procedures are ultimately the maindeterminants of psychotherapeutic benefit, and that the nature and characteristics ofthe psychotherapists who provide those treatments should matter only with regardto their competence to perform the treatments in quest ion and their ability to engagepatients in cooperative relationships. The study of psychotherapists seems to slipfrom view again and again, as was tacitly recognized by a major journal which re-cently devoted a special section to "the therapist as a neglected variable in psycho-therapy research" (Special Series, 1997).
Partly to remedy this situation, members of the Society for Psychotherapy Re-search in 1989 responded to a ca!! for a program of research on the developmentof psychotherapists. Organized as an SPRCollaborative Research Network (CRN),this group designed a study of development over the entire course of the profes-sional career, and included therapists of all professtonal backgrounds, theoreticalorientations, and countries. Because little cornparative cross-national data on psy-
NN
co>N
co>.-<
r-,ooN
jean-Francois Botermans, Catholic University of Louvain, Alice Dazord, INSERM,Lyon, Manfred Cierpka,University of Heidelberg, Nicoleua Aapro, University of Geneva, Peter Buchheim, Technical Universiryof Munich, Sue Bae, University of Chicago, Christine Davidson, Illinois Dept. of Mental Health, EricFriis-jorgensen, University of Copenhagen, Eunsun joo, Duksung Women's University, EkaterinaKalmykova, Russian Academy of Seiences. Jan Meyerberg, Clinic Bad Herrenalb. Terry Northcut, Chi-cago Loyola University, Barbara Parks, Universiryof Chicago, Elena Scherb, A1GLE,Buenos Aires,ThemasSchröder, Derbyshire Health Service, Gaby Shefler, Hebrew University, Dan Stiwne, University ofLinköping, Scott Stuart, Universiry of Iowa, Margarita Tarragona, Universidad de las Americas, AntonioBranco Vasco, University of Lisbon, Hadas Wiseman, Haifa University.
Others in the SPR Collaborative Research Network who have contributed their thought, skills, anddata to this research program include (alphabetically): Jerzy Aleksandrowicz, Poland; Hector FernandezAlvarez, Argentina; Per Erik Arnesen, Norway, Jill Backfield, USA;Wouter Backx, Netherlands; TelmoMourinho Baprista, Portugal; George Bourkovski, Russia, Dietmar Czogalik, Gerrnany; Lorraine Donner,USA;RitvaErkolahti, Finland; Hector Fernandez-Alvarez, Argentina, Salvatore Freni, Italy: Ilse Frohburg,Germany; Alessandra Gabrielli, Italy, Inez Gitiziner, Germany; Steven Gryll, USA; Armin Hartmann,Germany; Thomas Herzog, Germany; Winfred Huber, Belgiurn: jean-Francois lahns, France, HorstKächele, Gerrnany, Sudhir Kakar, India; jean Kirsch, USA; Sirko Kupper, Gerrnany; Wolfgang Lutz,Germany; Gudrun Olsson, Sweden; Augusto Perez-Gornez, Colornbia, Connie Philipps, USA;MichaelRosander, Sweden; Seth Rubin, USA;Robert RusselI,USA;C. Shamasundar, lndia; Biing-jiun Shen, Taiwan,Barbara Stein, Germany; ]ean Thurin, France; Anna von der Lippe, Norway, Ritsuko Watanabe-Greene,Japan; Victor Wied, Russia, K. Yagnyk, Russia.
Correspondence concerning this article should be addressed to David Orlinsky, PhD, University ofChicago, Comrnittee on Human Development, 5730 South Woodlawn Ave., Chicago IL 60637. E-mail:[email protected].

DEVELOPMENTOF PSYCHOTHERAP1STS 129
chotherapists exists, the study also aimed to collect systematic descriptive infor-mation about the characteristlcs, practices, and experiences of clinicians in differ-ent countries.
This paper presents the questions, concepts, and design of the international studyof the development of psychotherapists, organized and opera ted by the SPR Col-laborative Research Network. It introduces the research instruments used in its SUf-
vey and provides a descriptive analysis of the large group of psychotherapists whocontributed to the first phases of the project. Subsequent reports from the ongoingCRNstudy will focus substantivelyon the nature and correlates of therapists' devel-opment, and on other characteristics of therapists that may influence the course andoutcome of their treatment of patients.
corloN
mE CONCEPT OF DEVELOPMENT
The idea of development has a lang and important history in biology, psychology,and the social sciences. LogicaIly, development implies an intelligible, directional(though not necessarily linear) change of stare in a system or set of conditions. De-velopment is a temporal process of transformations that, when viewed with respectto some ideal value or criterion, can be described in terms such as progress versusregress, evolution versus devolution, and/or improvement versus decline.'
PERSPECTIVESON DEVELOPMENT
Assessments of development in general can be made from several types of data.The type viewed as methodologically most sound from an objectivist perspectiveutilizes longitudinal data, i.e., data collected prospectively for a given set of indi-viduals at successive points in time. Development is also assessed objectively, thoughless surely, by cross-sectional comparisons of data collected from cohorts that are atdifferent points in a temporal trajectory (career). In both cases, the data being corn-pared can be based either on participant or nonparticipant observations, but in bothcases the comparisons are methodologically objective, in the sense that they are madeby the investigators instead of the subjects being studied. These objective compari-sons should be made with respect to essential phenomena in the domain of func-tioning being studied, which must be specified by the investigators.
The problem of defining the essential phenomena is solved, at least partially, bytwo other approaches, both of which rely on the tacit knowledge that subjects haveabout their own functioning. Data for one of these approaches can be collected byasking subjects directly whether, how much, and in what directions they currently
"Ihe modern concept of development is linked hisrorically ro ehe Enlightenmenr idea of progress, whichinspired scientiflc as weil as social and philosophical thought throughout ehe 19th and weil into ehe20eh century (e.g., Lerner, 1986; Whiee, 1983). Events of the 20eh century have shaken ehe generalconfidence that change means progress in most spheres of life, excepr perhaps in ehe realm of psycho-logical development, Judgmems of progress email the privileging of a specific state or stage as ideal, ofrnovement toward that stage as "improvernent" or "growth," and movernent away from that state orstage as "deterioration" or "decline." In this study, ehe concept of development is used as far as pos-sible in a value-neutral sense, as a pattern of change over time.
o.-<oN
NN
..""r--ooN
IDUCID.~..,
130 ORLINSKY ET AL.
feel themse!ves to be "developing"; i.e., experience themse!ves as "learning," "grow-ing," and/or "improving" (or the opposite). A fourth approach relies on asking sub-jects wh ether, how much, and in wh at directions they feel they have "developed"overall, from the start of their careers to the present time. Tapping the practice-basedtadt knowledge of subjects is an advantage when the essential phenomena in a specificdomain of functioning are not clearly known. Although these last two approachesare "subjective" (in the sense that comparisons are made implicitly or explicitly bythe subjects themselves rather than by the investigators), investigators can add depthto such da ta by examining the objective carrelates of subjects' judgments about theirdevelopment.
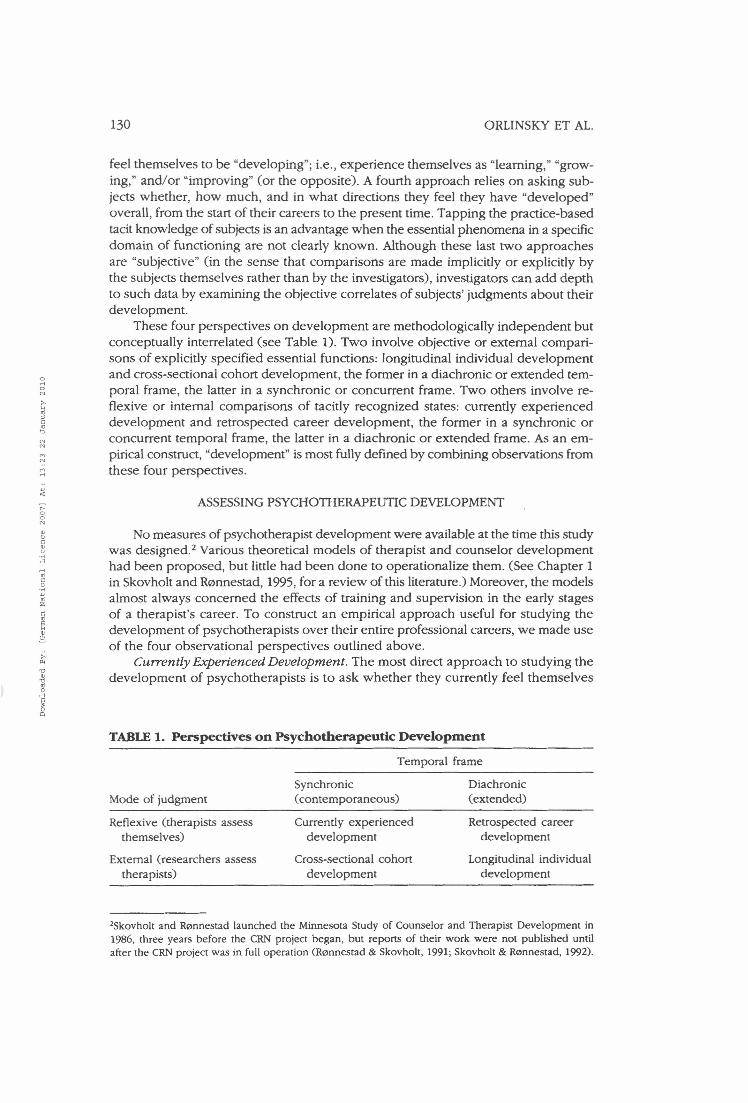
These four perspectives on deve!opment are methodologieally independent butconceptually interrelated (see Table 1). Two involve objective or external compari-sons of explicitly specified essential functions: longitudinal individual developmentand cross-sectional cohort development, the former in a diachronic or extended tem-poral frame, the latter in a synchronic or concurrent frame. Two others involve re-flexive or internal comparisons of tacitly recognized states: currently experienceddevelopment and retrospected career development, the former in a synchronic orconcurrent temporal frame, the latter in a diachronie or extended frame. As an em-pirical construct, "development'' is most fully defined by combining observations fromthese four perspectives .
ASSESSING PSYCHOTHERAPEUTIC DEVELOPMENT
No measures of psychotherapist development were available at the time this studywas designed.? Various thearetical models of therapist and counselor developmenthad been proposed, but little had been done to operationalize thern. (See Chapter 1in Skovholt and Rennestad, 1995, for a review of this literature.) Moreover, the modelsalmost always concerned the effects of training and supervision in the early stagesof a therapist's career. To construct an empirical approach useful for studying thedevelopment of psychotherapists over their entire professional careers, we made useof the four observational perspectives outlined above.
Currently Experienced Development. The most direct approach to studying thedevelopment of psychotherapists is to ask whether they currently feel themse!ves
TABLE1. Perspectives on Psychotherapeutic Development
Temporal frame
Mode of judgmentSynchronie(contemporaneous)
Diachronie(extended)
Reflexive (therapists assessthernselves)
External (researchers assesstherapists)
Currently experienceddevelopment
Cross-sectional cohortdevelopment
Retrospected careerdevelopment
Longitudinal individualdevelopment
2Skovholt and Rennestad launched the Minnesota Study of Counselor and Therapist Development in1986. three years before the CRN project began, but reports of their work were not published untilafter the CRNproject was in full operation (Ronnestad & Skovholt, 1991; Skovholt & Rennestad. 1992).

o~oN
NN
coN
r--ooN
"00
'0m'0~.sc3oCl
DEVELOPMENT OF PSYCHOTHERAP1STS 131
to be experiencing growth (and/or decline) in their ability and capacity to do thera-peutic work. Do they feel that they are acquiring new skills, learning new tech-niques, becoming more sensitive, responding more effectively, attaining new in-sights, overcoming past limitations, and deepening their understanding of patientsand of how to help them? Alternatively (or simultaneously but in different respects),do they fee! that they are growing stale, performing routinely, becoming "burnedout," or otherwise losing their capacity to be understanding and helpful? Present-oriented subjective observations like these have obvious methodological !imita-tions, but theyalso possess an inherent interest and obvious face validity. Researcherscan also independently probe these self reports by exploring the circumstances inwhich therapists experience themselves as currently deve!oping to a greater or lesserdegree.
Retrospected Career Deoelopment. Practitioners take a temporally extended viewof development when reflecting on how much they have changed in their abilities andin other ways sinee they started to do psychotherapy. Judgments such as these aremore complex than directly introspected assessments of current development, becausethey require implicit comparison of present abilities, limitations, and disabilities wirhestimates of past abilities, limitations, and disabilities, and they are liable to retrospec-tive distortions as an additional source of bias. Nevertheless, judgments like these aremade regularly by people in every calling. A sense of progress, stability, stagnation, ordecline over the course of one's career is probably inescapable for persons endowedwith memory and inclined to self evaluation, and is probably an important determi-nant of eurrent morale and motivation for therapeutic work. Additional informationcan be gained from these self reports by examining which therapists rate themselvesas having developed to a greater or lesser extent in their careers to date.
Cross-Sectional and Longitudinal Perspectives on Development. Cross-sectionaland longitudinal assessments of development both involve comparisons made byinvestigators, but those investigators in turn must specify the attributes on which changeis to be assessed. Our approach was based on a descriptive analysis of the psycho-therapist's role functioning, because clinical theories differ wide!y about the essen-tial features of therapeutic work, and our study aimed to include therapists of allorientations. First, a distinction was drawn between instrumental and interpersonalaspects of role functioning, following a common praetice of sociologists and socialpsychologists (e.g., Bales, 1970; Parsons, 1951). Therapists' instrumental or task-oriented functions were defined in terms of their typical goals when working withpatients, the skills they utilize in pursuing those goals, the difficulties they encounterin therapeutic work, and the ways in which they cope when experiencing difficul-ties. Sirnilarly,the interpersonal or relationship-focussed aspect of therapist functioningwas differentiated into the therapists' ideal manner in relating to patients, typicalmanner in relating to patients, case management with respect to relational normsand boundaries, and theoretical orientation (i.e., be!iefs and values) used to definethe soure es and solutions of patients' problems. Cross-sectional cohort developmentinvolves comparison of these role functions across groups of therapists at differentcareer stages. Longitudinal individual development involves comparison of these rolefunctions over different points in the therapist's career.
GENERALRESEARCHQUESTIONS
The definitions of development and approaches to its assessment described hereadd specificity to the primary goals of the study, wh ich center on three questions.

132 ORLINSKY ET AL.
r-.ooN
To wh at extent, and in what respects, do psychotherapists- develop over the courseof their professional careers? Wh ich factors facilitate or inhibit that development? Towhat extent are patterns of professional development, and the factors that appear toinfluence them, broadly similar for all therapists, and to wh at extent do they differamong therapists of different professions, theoretical persuasions, nationality, etc.?
Do Tberapists Deuelop? Specific descriptive questions to be answered include thefollowing: How much do therapists actually appear to develop when assessed fromeach of the four approaches? To wh at extent do assessments from these four per-spectives agree? Is psychotherapeutic development unidimensional or multidimen-sional within and across assessment modalities? Is psychotherapeutic development acontinuous or discontinuous process? To what extent does it fit a stage or level con-ception of development (Lerner, 1986)? Do psychotherapists at different points intheir careers develop in different ways or at different rates? Do individual therapistsdevelop along divergent paths, or does a common pattern of development apply tomost therapists?
Wbat Influences Psycbotberapeutic Deuelopment? Questions about the sourcesof psychotherapeutic development include the following: How much, and in whatways, do the traditional elements of professional education (didactic training, casesupervision, and personal therapy) contribute to psychotherapeutic development?How much does actual therapeutic work with patients, or therapists' work situationsand conditions, affect their development? Does providing training, supervision, orpersonal therapy to other professionals enhance the development of senior thera-pists? To wh at extent, and in what ways, do therapists' life situations and personali-ties influence their professional development? Does the impact of these various in-fluences change with the stage of the therapist's career?
One Profession or Seueral in Regard to Deuelopment? Practitioners of the modernpsychotherapies are subdivided variously by their professional training, theoreticalorientations, and national cultures. Those who practice psychotherapy, psychoanalysis,counseling, or provide some related form of help to psychologically and ernotion-ally distressed persons, may have had their basic professional training in medicine,psychology, social work, education, nursing, religion, or some other field. Practi-tioners from these professions may be adherents of (or eclectically combine) variousanalytic, behavioral, cognitive, humanistic, and systemic approaches to therapeuticpractice. Moreover, adherents of a particular orientation who work in different coun-tries may show differences among themselves based on national culture (Kurzweil,1989). Thus, it seems important to ask questions about the generality of therapeuticdevelopment across these various demarcations and divisions. To what extent dothe patterns, processes, and facilitators (or inhibitors) of professional developmentdiffer by profession, theoretical orientation, and nationality (or by interactions amongthose factors)? To what extent are personal and sociodemographic characteristics oftherapists (e.g., gender, marital status, minority status) differentially associated withtheir professional development? Is it true, as suggested by Henry, Sims, and Spray(971), that psychotherapists are essentially the same despite differences in profes-sional background, or does that view only reflect a "uniformity myth" (Kiesler, 1966)?
o.-<oN
3Here and elsewhere in this study, "psychotherapist" and "psychotherapy" are used as generic termsthat also cover c1early related variants which some may not call by that name, including psychoanaly-sis, behavior modification, counseling (for personal, marital, or family problerns), etc. The terms arealso meant to cover individual, couple, group, and other modes of organizing therapeutic interactions.

NN
t--ooN
<lIUC<lIU.~Cl
~~C.~.,~Z
C~EH<lI2,
DEVELOPMENT OF PSYCHOTHERAP1STS 133
Much preliminary work was required in order to answer these general questions,involving the construction of meaningful instruments and their evaluation with a broadrange of therapists. This paper concems these first essential steps.
METHOD
RESEARCH INSTRUMENTS
Although da ta relevant to the study of psychotherapists' development can beobtained from different observational perspectives, a survey of psychotherapistsseemed the best starting point, for several reasons. First, self reports of therapists areessential data with respect to assessments of currently experienced development andretrospected career development, and are also compatible with cross-sectional andlongitudinal approaches. Second, it was economically feasible to do as part of a projectthat was begun without extemal funding (Orlinsky, 1987). Also, by inviting thera-pists to share their experiences as colleagues asked to join in a collective self studyof therapeutic professions, we hoped to create a respectful research alliance, ratherthan one in which they would fee! like objects of extemal scrutiny and evaluation.Finally, therapists generally are trained and disposed to reflect constructively on theirmotives and behaviors (Skovholt & Rennestad. 1995), and may in fact be relativelyobjective in such self-evaluative tasks (e.g., Mabe & West, 1982; Wicklund, 1979).Eventual utilization of da ta from multiple observational perspectives does, however,remain a long-term goal of the CRN project.
Given persuasive reasons for starting in this way, a team consisting of clinician-researchers from different countries, professions, and theoretical orientations" workedto formulate a set of self-adrninistered research instruments that would describe par-ticipating therapists in adequate detail, incIude data for direct and indirect assessmentsof development and survey factors that seemed most likely to facilitate or hinder thatdevelopment. These instruments were composed originally in English (by a multilin-gual group of Arnerican, Belgian, Dutch, English, French, German, Italian, and Swissresearchers), taking care to use terms and phrases that would translate weil into otherlanguages. Subsequently, the questionnaire has been translated into Chinese, Danish,Finnish, French, German, Greek, Hebrew, Italian, ]apanese, Korean, Norwegian, Pol-ish, Portuguese, Russian, Spanish, and Swedish, in addition to separate English ver-sions following North Arnerican and British usage. To ensure the greatest cornparabil-ity in meaning between different vers ions of the questionnaire, each translation wassubmitted for evaluation to two independent bilingual colleagues before being usedin data collection. Each judge rated each question and set of instructions on 4-pointscales for exactness of translation and for correctness of expression Cl = excellent, 2 =
good, 3 = marginal; 4 = poor). Translations were accepted when both judges ratedeach item and instruction good or excellent in both respects. Items and instructionsthat were not approved were revised until these criteria were met. Translations of single
'ln alphabetical order, the team included Nicoletta Aapro, Hansruedi Ambühl, Wouter Backx, ]ean-Franccis Botermans, Christine Davidson,]ohn Davis, MarciaDavis,AliceDazord, Paul Gerin.jean-Francoislahns, David Orlinsky, and Ulrike Willutzki. The count ries represented by this group include Belgium,France, Germany, Netherlands, Switzerland, the United Kingdom, and the United States; the profes-sions represented included medicine, psychology and social work; the orientations included werebehavioral, cognitive, experiential, psychodynamic. and systemic.

onoN
NN
r-ooN
134 ORLINSKY ET AL.
term adjective scales (e.g., "accepting," "warm") were further checked by having themindependently translated back to English.
A Deuelopment of Psycbotberapists Common Co re Questionnaire CDPCCQ) instru-ment package was assembled from the various measures, which probed diverse as-pects of the therapist's background, functioning, and experiences. Table 2 summarizesthe content and organization of the composite instrument. Most of the 370 items gath-ered in it were designed as structured-response scales or checklists, for standardiza-tion and ease of response, but eight open-ended questions were also included. Theseveral sections of the DPCCQ package are separate multi-itern questionnaires on re-lated themes, assembled in a single package for ease of presentation.
The length of the DPCCQ was dictated partly by the complexity of the subjectmatter itself and partly by a need to collect extensive descriptive information abouttherapists in different countries. Because of its length, the DPCCQ generally requiresan hour or two of the therapist's time, and thus may deter some potential respon-dents. However, it also affords so me advantages that briefer, single issue question-naires do not, the chief among these being that those who do complete and returnthe DPCCQ can be viewed as seriously motivated respondents. Another major ad-vantage is that while each itern represents a bit information in its own right, it canalso be analyzed in conjunction with a great deal of other information about therespondent. Thus, the data can be viewed "in depth" (i.e., in a variety of relatedcontexts), and can be understood in terms of broader patterns in a manner analo-gous to clinical inference. It is possible to read through the responses of a single(anonymous) individual and gain a clear sense of the person who gave them, dem-onstrating the instrument's strength with regard to reconstructivity-defined as thecapa city to generate "a c1inically meaningful gestalt from distinct bits of coded infor-mation" (Pinsof, 1986, p. 220).
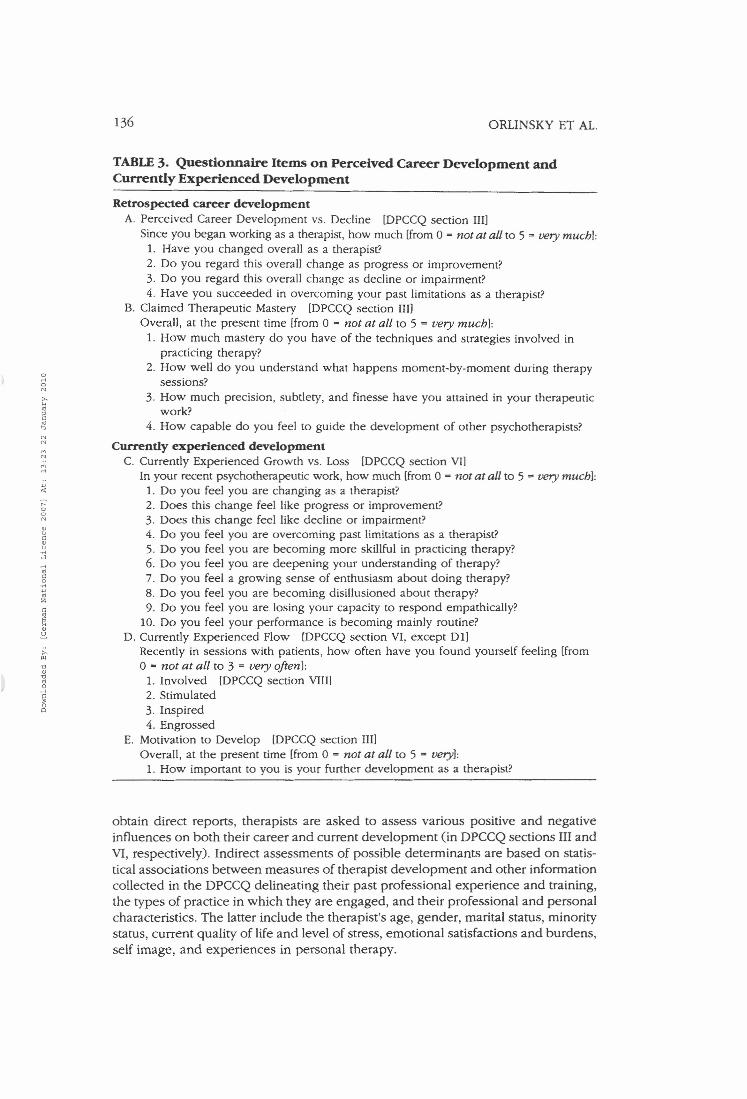
The content of the DPCCQ corresponds to the three main aims of this study, thefirst of which is to provide measures of development. Questions direetly assessingtherapist retrospective career development are shown in the upper part of Table 3(Perceived Career Development and Claimed Therapeutic Mastery), and the iternsused to construct an indirect measure (Skill "Change" Index) are presented in Table8. Similarly direct measures of therapist currently experienced development are madeby questions shown in the lower part ofTable 3 (Currently Experienced Growth andMotivation to Develop). An indirect measure of current development based onCsikszentmihalyi's (1975, 1990) concept of flow uses iterns shown in Table 3 CD).Flow refers to a subjective state of being fully absorbed in an activity, feit to be in-herently rewarding, which occurs when the individual is engaged in achallengingsituation that stimulates the growth of relevant skills.
Data for cross-sectional analyses of therapists at different stages of their careersare provided by re ports concerning specific current therapeuticskills CDPCCQ sec-tions III and VI), Initial and current theoretical orientations CDPCCQ sections III andV), ideal and typical styles of relating to patients CDPCCQ sections V and VIII), dif-fieulties currently encountered in therapeutie work CDPCCQ section VIII), and cop-ing strategies CDPCCQ seetion VIII). (Specific items from these sections will be pre-sented, as relevant, in later publications.) Longitudinal assessments of developmentwill use the same data when the DPCCQ is eompleted again at subsequent points inthe therapist's career.
The information collected can be used to study possible determinants of the extent,direction, and rate of therapeutic development, assessed directly and indirectly. To

DEVELOPMENT OF PSYCHOTHERAP1STS 135
TABLE2. "Development ofPsychotherapists Common Core Questionnaire"Component Instruments
r-,ooco
O. Identifying data [5 items]Personal code: date of birth; sex; country of residence; date
1. Amount and types of profession training [23 itemslQuestionnaire on professional identifieation, academie background, professionalcertification, organizational affiliations, years of didactie training, years of supervi-sion, past and current training in special types of therapy, and current supervision.
Il. Professional experience to date [21 itemslQuestionnaire on years of therapeutie practice, years of practiee in specific settings,number of cases in different treatment modalities, number of patients in differentage groups, number of other therapists treated, and number of other therapistssupervised.
III. Overall development as a therapist [51 iternslQuestionnaire on overall change, improvement and dec1ine, transcendence ofpersonal limitations, commitment to further development, and sense of ability toguide development of other therapists, questionnaires on skill levels as a beginningtherapist and current therapeutie skill levels (to assess change), questionnaires oninitial (and later current) theoretical orientation (to assess change), questionnaire onpositive and negative influences on overall deveIopment
IV. Experience of personal therapy [7 itemslQuestionnaire on attitude toward personal therapy for therapists, on current andpast experiences of personal therapy, and on reasons for and beneflts of specificepisodes of personal therapy.
V. Ortentation of therapeutie work [52 ltemslQuestionnaires on current theoretical orientation; questionnaire on typieal goals oftherapeutie work; questionnaire on ideal seIf-concept as a therapist.
VI. Current development as a therapist [35 items]Questionnaire on current change, improvement and dec1ine, transcendence ofpersonal limitations, aspects of motivation and capacity for therapeutie work:questionnaire on feelings in recent sessions with patients: questionnaire on positiveand negative influences on current development.
VII. Settings, treatment modalities, and c1ientele in current therapeutic practice [43 items]Questionnaire on hours of therapy per week delivered in various settings, satisfac-tion with main setting of practiee, sense of support and control in main setting ofpractice, number of current cases in various therapy modalities, number of patientsof various age groups, most frequent diagnostic types of patients treated (currentlyand earlier in career), extent of reliance on diagnosis in eurrent practiee, and levelsof satisfaetion and dissatisfaction currently experienced in therapeutie work;questionnaire on level of disturbance of patients treated (currently and earlier incareer Ibased on the Global Assessment of Functioning Scale [American PsychiatrieAssociation, 1987]).
VIII. Experieneed quality of therapeutie work [96 iterns]Questionnaire on types of difficulty currently experienced in therapeutie practice,questionnaire on types of coping strategies used to deal with difficulties; question-naire on actual self concept as a therapist; questionnaire on style of managingtherapeutie relationships; questionnaire [open endedl on greatest strength as atherapist and most problematie limitation as a therapist.
IX. Personal life and self-experience of therapist [42 items]Questionnaire on nationality, minority status in country of residence, marital status,current life satisfaction and stress, and qualities of eurrent emotional experience;questionnaire on self-concept in dose personal relationships.
or<oco
coco
Mco
136 ORLINSKY ET AL.
TABLE3. Questionnaire Items on Perceived Career Development andCurrently Experienced Development
o...•oN
Retrospected career developmentA. Perceived Career Developrnent vs. Decline [DPCCQ section IIIl
Since you began working as a therapist, how much lfrom 0 = not at all to 5 = very muchl:1. Have you changed overall as a therapist?2. Do you regard this overall change as progress or improvernent?3. Do you regard this overall change as decline or impairment?4. Have you succeeded in overcoming your past !imitations as a therapist?
B. Claimed Therapeutic Mastery [DPCCQ section IIIlOverall, at the present time [from 0 = not at all to 5 = oery muchl:
1. How much mastery do you have of the techniques and strategies involved inpracticing therapy?
2. How weil do you understand what happens moment-by-rnoment during therapysessions?
3. How much precision, subtlety, and finesse have you attained in YOUf therapeuticwork?
4. How capable do you feel to guide the deve!opment of other psychotherapists?
Currently experienced developmentC. Currently Experienced Growth vs. Loss [DPCCQ section VIl
In your recent psychotherapeutic work, how much [from 0 = not at all to 5 = very muchl:1. Do you feel you are changing as a therapist?2. Does this change feel like progress or improvement?3. Does this change feel like decline or impairment?4. Do you feel you are overcoming past !imitations as a therapist?5. Do you feel you are becoming more skillful in practicing therapy?6. Do you feel you are deepening your understanding of therapy?7. Do you fee! a growing sense of enthusiasm about doing therapy?8. Do you feel you are becoming disillusioned about therapy?9. Do you feel you are losing your capa city to respond empathically?
10. Do you feel your performance is becoming mainly routine?D. Currently Experienced Flow [DPCCQ section VI, ex ce pt D1l
Recently in sessions with patients, how often have you found yourself feeling [from0- not at alt to 3 = uery oftenl:
1. Involved [DPCCQ section VIII]2. Stimulated3. Inspired4. Engrossed
E. Motivation to Develop [DPCCQ section IIIlOverall, at the present time [from 0 = not at alt to 5 = veryl:
1. How important to you is YOUf further development as a therapist?
NN
MN
r-,ooN
"uC".~..,...•"c.~""zc
~"2.
obtain direct reports, therapists are asked to assess various positive and negativeinfluences on both their career and current development (in DPCCQ sections III aridVI, respectively). Indirect assessments of possible determinants are based on statis-tical associations between measures of therapist development and other informationcollected in the DPCCQ delineating their past professional experience and training,the types of practice in which they are engaged, and their professional and personalcharacteristics. The latter include the therapist's age, gender, marital status, minoritystatus, current quality of life and level of stress, emotional satisfactions and burdens,self image, and experiences in personal therapy.

orloN
NN
MN
Mrl
..W
'"r--ooN
Q)U
"Q)
.~.:l
"cc'0Q)'0
"sc•oo
DEVELOPMENT OF PSYCHOTHERAP1STS 137
DATA COLLECTION
Systematic collection of data on therapists requires a satisfactory answer to thequestion: "Who is a psychotherapist?" Unfortunately, the total population of psycho-therapists is difficult to define preeisely, even within a single country. Although thereare many professional psychotherapists, there is no single profession of psychotherapywhose members belong to one organization (e.g., a national professional sociery).Instead, psychotherapy is typically practieed by some, but not all, members of sev-eral different professions, and the organizations which represent them are varied andoften confliet over matters of professional jurisdietion and economie advantage (Abbott,1988). Within these professions, members often divide into rival theoretical camps,making the situation even more complex. Besides, there are informal channels throughwhich persons of talent sometimes succeed in becoming established as psychothera-pists without conventional professional training. In an international study, one mustalso take account of local differences regarding which professions are allowed topractiee, which orientations are popular, and whieh types of therapy are supportedby national or private health insurance.
Representative sampling is problematic when the parent population cannot bedefined dearly or when it is not even dear whether one or several populationsmust be considered. In this situation, two alternative data collection strategies seemedpossible. One was to ask CRN colleagues in each country to collect da ta from abroad range of persons who are locally accepted as therapists, counselors, or simi-lar practitioners. The aim of this strategy is to gather a heterogeneous data basewhose size and internal diversity permitted disaggregation into meaningful sub-groups. In this case, the question of generalizibility to a parent population wouldremain moot, but the generality of findings across diverse professional and demo-graphie groups of therapists could be assessed. Collection of sufficient data to givea detailed description of the therapists studied would allow for a tentative gener-alization or "transferability" of findings to other therapists with similar professionaland demographie characteristies (Lincoln & Guba, 1985).
The second alternative was to seek representative sampies from organizationsof therapists who share a specific theoretical orientation, or from regional or nationalprofessional assoeiations in which many members are known to engage in therapy,counseling, or cognate practices. In this case, while the sampies might be readilygeneralizable to the limited populations from whieh they were drawn, the resultswould have unknown generality, in the sense they might not apply beyond the spe-eific groups that were studied. For example, findings from a representative sampieof psychologist psychotherapists could not be assumed to apply to psychiatrist psy-chotherapists, or to social workers or counselors, and findings from a representativesampie of psychodynamic therapists could not be assumed to apply to cognitive-behavioral, systernic, or humanistie psychotherapists.
Under the circumstances, the best long term solution is to attempt both approaches,but the first seemed acceptable as the initial approach in a discovery-oriented study,and was economically more feasible. Accordingly, a mixed model of data collectionwas pursued. One type involved solieitation of attendees at professional workshopsand conferences. A second involved cooperation with professional societies to sur-vey their members. A third approach involved collaboration with training programswhere the availability of faculty, supervisors, and graduates, as well as current train-ees, ensured the indusion of a wide range in therapist experience levels. A fourthprocedure depended on individual collegia 1networks, with CRN members asking

o.-<oN
NN
MN
M.-<
6oN
WUCW.~..,
138 ORLINSKY ET AL.
therapists they know to complete the questionnaire and to request their colleaguesto do the same. A fifth method was to contact individuals who listed themselves inclassified telephone directories as providers of counseling or thera py services tothe public. (The procedure by wh ich each local da ta collection was made is in-duded as da ta to be analyzed subsequently in assessing their possible impact onfindings.)
The responsiveness of psychotherapists to these varied approaches is indicatedby the large number who have completed and returned an obviously lengthy ques-tionnaire, without compensation for their time and sometimes even for the cost ofpostage. Local data collections have been made since 1991, and new ones con-tinue to be made as additional opportunities arise and as new colleagues becomeinterested in joining the project. The data collected by these means have been ag-gregated in successive stages, to make a single, continually expanding da ta basefor use by the CRN team, as a group, in pursuit of the study's main aims, and byindividual CRN members in return for their contributions to the project. In its firststage (circa 1992), the data base induded about 600 German and French thera-pists. The second stage (circa 1993) added approximately 800 therapists from othercountries, increasing the total to about 1400. A third stage (circa 1995) increasedboth the number of countries represented and the overall number of therapists toapproximately 2400. By mid 1997, the addition of new data from other countries broughtthe total number of therapists in the CRN data base dose to 3800. This was deemedsufficient in size, diversity, and interest to warrant a detailed descriptive report as afoundation for analyses of data with reference to the specific research questions ad-dressed by the project.
ANALYSES
As an introduction to and basic reference for the CRN research program, thispaper presents basic descriptive da ta on the 3800 therapists in the 1997 data base,and develops the direct and indirect measures for two central concepts, perceivedcareer development and currently experienced development. Descriptive statisticsare used to implement the first of these aims, and factor analysis (using PrincipalComponents extraction with Varimax rotation) the second.
RESULTS
PROFESSIONAL CHARACTERISTICS
Professional Identification. Identification with particular professions was establishedfrom therapist replies (multiple responses allowed) to the question: "What is your profes-sional identity? That is, how do you refer to yourself in professional contexts?" Table 4shows that the largest group of subjects (about 47%) identified themselves principallyas psychologists, and the second largest (about 36%) identified with medicine (eitheras psychiatrists or, among Gerrnans, as physicians specializing in psychosomatics andpsychotherapy), Social workers are not yet strongly represented in the data base, norare nurses, although their numbers perrnit a preliminary examination of potential dif-ferences. Particularly interesting are the 306 therapists (8%) who did not identify them-selves with the traditional mental health disciplines of medicine, psychology, socialwork, and nursing. Of these, two-fifths identified with another profession, while three-

DEVELOPMENT OF PSYCHOTHERAP1STS 139
TABLE4. Professional Characteristics ofPsychotherapists Surveyed:1991-1996 [N'" 37951
Professional identification t N [N] % [%]Medicine 1345 35.6
Psychiatrist 351 26.1Psychiatrist-in-training 332 24.7PsychiatristiPhysician 291 21.6Physician 337 25.1Physician-in-training 34 2.5
Psychology 1767 46.7Psychologist 1591 90.0Psychologist-in-training 176 10.0
Social work 294 7.8Social worker 156 53.1
0 Social worker-in-training 138 46.9r<0N Nursing 110 2.9>-'" Nurse 101 91.8'"~c Nurse-ln-training 9 8.2'"..,N Otber profession lnone of above) 126 3.3N
co 'Lay' practitioner l'function identification' only) 180 4.8N
co Psychotherapist 80 44.4r<
.. Psychotherapist-In-trainmg 19 10.6"'" Psychoanalyst 26 14.4r- Psychoanalyst-in-training 5 2.800N Counselor 45 25.0vu Counselor-in-training 29 16.1cv.~ Theoretical Orientationt N % M S.D...,r< Salient Ortentation lra ted 4+ on 0-5 scalel'"c8 Analytic/Psychodynamic 2194 59.2 3.4 1.6"'" Behavioral 483 13.1 1.5 1.5zc Cognitive 687 18.5 1.8 1.6'"E'" Humanistic 1136 30.7 2.2 1.8ill
S Systernic 702 18.9 1.7 1.7>- Other 497 13.4 0.7 1.6"''Cl Breadthv'Cl
'" Number of salient orientations [rated 4 or 5) 1.5 1.0.8c Uncommitted (0 salient orientations) 463 12.2•0Cl Focally Committed (1 salient orientation) 1746 46.0
]ointly Cornmitted (2 salient orientations) 1003 26.4Broadly Committed (3+ salient orientations) 583 15.4
Number of positive influences [rated 3-5) 2.3 1.3Uninfluenced (0 positive influences) 174 4.6Focally influenced (I positive influence) 1111 29.3]ointlyinfluenced (2 positive influences) 1013 26.7Broadly influenced (3+ positive influences) 1497 39.4
Professional experience M Med S.D. Range[Years in practice] 9.5 8 7.7 0-52
ISum of percentages for profession and theoretical orientation may exceed 100 because multiple rat-ings were allowed.

orloN
NN
~oN
wuCw.~Cl
rl~C.~
"~Z
C~~w2
""''0w'0~~c•o"
140 ORLINSKY ET AL.
fifths identified themselves only in terms of a professional function (i.e., simply as apsychotherapist, psychoanalyst, and/or counselor).
Tbeoreticai Orientation. Orientations were assessed from therapist replies (mul-tiple responses allowed) to the question: "How much is your current therapeuticpractice guided by each of the following theoretical frameworks?" Responses weremade to six items using a 0-5 scale (0 = not at all, 5 = very greatly). analytic/psy-chodynamic, behavioral, cognitive, humanistic, systemic, and other (conte nt speci-fied by respondents). Ratings of three or more were termed a "positive influence";ratings of four or five defined a "salient commitment" (Ambühl, Botermans, Meyerberg& Orlinsky, 1996). Table 4 shows the incidence with which each type of orienta-tion was rated as salient, as well as the number of different salient commitmentsand positive influences reported. The most prevalent salient orientation in this groupwas analytic/psychodynamic (60%), with humanistic a distant second (31%); butthere were also substantial numbers who rated systemic, cognitive, and behavioralas their salient orientations (the latter two either separately or jointly as cognitive-behavioral). Nearly as many therapists expressed a commitment to two or moresalient types of orientation as did to just one. The tendency toward eclecticismseems even clearer if each of the types is understood as a family of more specificorientations, and this impression is reinforced when noting that 66% of the thera-pists listed two or more types of orientation as positive influences. While there isa substantial group whose theoretical orientations are relatively pure, they are aminority in the present data base.
Practice Duration. Therapists were asked, "How long have you engaged in thepractice of psychotherapy?" They were instructed to include practice du ring trainingbut exclude periods during which they did not practice. Table 4 also shows the cur-rent data base includes therapists at all career stages-from some who had practicedhalf a century or more to others who had just started. A majority of the therapistswere experienced practitioners, the median for the total group being eight years inpractice (mean = 9.5).
PRACTICE CHARACTERISTICS
Treatment Settings. Table 5 shows that about half the therapists reported work-ing in just one type of treatment setting while the other half practiced therapy infrom twO to as many as four types of setting. The total amount of time devoted totherapeutic practice was about 20 hours per week on average, but with a large de-gree of variation. No single type of treatment setting was predominant, but a largeproportion of therapists did spend some time in independent practice (45%), andmany did at least some therapeutic work in public outpatient facilities (35%). Thosewho practice independently reported they averaged 12-15 hours oftherapeutic workper week, but the highest weekly average of treatment hours was reported by thera-pists in public inpatient settings.
Treatment Modalities. Table 5 also shows that individual therapy was by far themost common treatment modality reported, with 93% of the therapists having somecurrent individual treatment cases. For those, the median number of current caseswas nine (mean 12.4), but aga in with a large amount of variation. Other forms oftreatment trailed far behind, with the next most frequently practiced form being grouppsychotherapy (36%), followed by couples therapy (31%) and family therapy (25%).Only 10% reported practicing so me other therapy modality (content specified byrespondents). The average number of cases per treatment modality indicates that

DEVELOPMENT OF PSYCHOTHERAP1STS 141
TABLE5. Professional Practice ofPsychotherapists Surveyed: 1991-1996[N= 3795]
Practicing in category'
N % M Med sd Range
Treatment Setting [hours]Public inpatient 941 25.9 17.3 10 14.6 1-48
Public outpatient 1254 34.5 13.0 10 11.1 1-40Private inpatient 308 8.5 15.7 10 13.3 1-40
Private outpatient 475 13.1 12.5 9 10.8 1-35Group private practice 462 12.7 11.1 8 10.2 1-38Individual private practice 1635 44.9 15.1 12 12.0 1-45
Other 365 10.0 6.8 5 5.0 1-20
0Total treatment hours 22.8 20 14.8 1-63
.-<Number of treatment settings 1.5 1 .77 1-40
N
>-Treatment Modalities leasestH
"" Individual 3361 93.2 12.4 11.0 1-60c 9"r, Couples 30.6 2.6 2.2 1-10N 1107 2N
Family 896 24.8co 2.8 2 2.3 1-13N
36.3co Group 1313 2.3 1 2.3 1-15.-<
Other 336 9.4 52 4 4.4 1-20"" Total cases 15.6 11 16.0 1-71r-, Number of treatment modalities 2.0 2 1.0 1-400N
W Age groups' [patients]oc 12 years and younger 826 23.1 4.5 3 3.7 1-16w.~.., 13-19 years 1515 42.3 3.1 2 2.8 1-15r< 20-49 years 3284 91.9 12.9 10 10.7 1-60"c8 50-64 years 1911 53.5 3.6 2 3.1 1-18"or 65 years and older 646 18.0 2.5 2 2.2 1-10zc Total patients (by age groups) 17.4 14 14.3 1-87"EH
Number of age groups treated 2.2 2 1.2 1-5ws>- Symptom/impairment level-"' Minimal leveryday problemsl 724'0 21.5 3.2 2 3.0 1-17w'0 Transient lstress reactions] 1469 43.7 3.7 2 3.6 1-20"..cl
Mild but enduring symptoms 2356 70.3 4.9 3 4.4 1-25c•0 Moderate symptoms 2539 76.0 5.6 4 4.9 1-25" Serious symptoms 2493 7~.5 4.5 3 4.2 1-22Severe [borderline] 1625 48.4 3.2 2 3.0 1-16Very severe [psychotic] 995 29.5 2.6 2 2.2 1-10Extreme [danger to self/others] 766 22.7 2.5 2 2.2 1-10
Total patients (by impairment levels) 17.7 14 14.9 1-90Number of impalrrnent levels treated 4.0 4 1.7 1-8
tStatistics given per category for those currently practicing; Ns vary due to fluctuations in available data;range defined as 1 to the number marking the 99th percentile.'Current ehentele.

o.-<oN
r-OoN
•Uc:•.;:..,
142 ORLINSKY ET AL.
individual therapies are in fact the mainstay of practice for most therapists. Whilehalf the therapists reported using two or more treatment modalities, most had onlyone or two couples, families, or groups in treatment.
Patient Age Groups. Therapists were asked to indicate by age group the numberof patients they were currently treating. Table 5 shows that nearly all therapists (92%)treated 20-49 year old patients, and a majority (53%) also treated 50-64 year olds. Bycontrast, relatively few treated any children C23%)or seniors (18%), although a sub-stantial minority did treat adolescents C42%). The average number of patients perage group indicates that 20-49 year old adults comprise the bulk of most therapistpractices.
Patient Impairment Levels. Therapists were also asked to estimate the numberof patients they were currently treating at each of eight levels of impairment, basedon the Global Assessment of Functioning scale, constituting Axis V in the DSM diag-nostie system (lowest two levels were combined). Table 5 shows that most thera-pists (75%) reported treating patients with moderate or serious symptoms, and nearlyas rnany C70%)had patients with mild but enduring symptoms. Substantial numbersof therapists C44-4~Al) also treated severe1y disturbed (e.g., borderline) patients, orpatients considered to be just transiently impaired Ce.g., stress reactions), Smallerbut still substantial numbers of therapists treated patients with very severe (e.g.,psychotie) disturbances C30%) or extreme and potentially dangerous disturbancesC23%).These data strongly contradiet the occasionally stated opinion that therapistsmainly treat clients who have no significant mental health problems (ehe "worriedweil"). Patients rated as having no more than minimal problems accounted for thesmallest proportion of therapists' current practices.
Total CaseLoad. Therapists' reports of their patients' ages and impairment levelsprovided separate bases for calculating the total numbers of patients they were cur-rently treating. The median number estimated from patient age groups was 14 (rnean17.4), and from impairment levels it was also 14 (mean 17.7). Standard deviationsand ranges for these figures were also highly similar.
DEMOGRAPHIC CHARACTERISTICS
Nations. Table 6 shows that 12 countries are represented by a minimum of 100therapists each in the current data base, although their proportions vary from 28%(Germany) to about 3%. Smaller groups of therapists come from five other countries,but four of these are interesting because they have rarely been studied by therapyresearchers (Argentina, India, Italy, and Mexico). Most of the countries in which datahave been collected thus far lie in the "Northwest European/North American" cul-tural sphere, but with significant variations between regions (e.g., Scandinavian andLatin countries), and between these and historically rnore remote cultural spheresCe.g., East European and Asian countries). Ongoing da ta collection should broadenthe range of countries and cultures and balance the distribution of numbers in theCRN data base.
Minority and Immigrant Status. Questions concerning possible social and/or cul-tural marginality of psychotherapists were raised by a previous large-scale survey ofAmerican mental health professions (Henry, Sims, & Spray, 1971). However, only9% in the present survey said they would "be considered a member of a social, cul-tural, or ethnic minoriry" in the country where they live. Some evidence for themarginality hypothesis might be found in the 22% of therapists who reported ha v-ing been born in a country other than where they presently live. However, a very

DEVELOPMENT OF PSYCHOTHERAP1STS 143
TABLE6. Demographie Characteristics ofPsyehotherapists Surveyed:1991-1996 [N - 3795]
N %
Country of ResidenceBelgium 130 3.5Denmark 158 4.2France 117 3.1Germany 1059 28.3Israel 100 2.6Korea 538 14.4Norway 371 9.9Portugal 188 5.0Russia 110 2.9
0 Sweden 117 3.1'"0 6.8N Switzerland 255,.,~ USA 329 8.8~~c Other « 100 therapists) I 273 7.2~..,N Born elsewhere than country of residence 817 22.2N
M Minority status in country of residence 328 9.0N
M Sex'"'-' Female 2060 54.9'" Male 1695 45.1r- Marital starus-00N Single 715 20.2~c Married or partnered 2361 66.8c~.~ Separated or divorced 412 11.6.cl
~ Widowed 50 1.4~c.~ Age (years) 41.0 [M] 40 (Med) 9.8 (Sm 22-91 (Range)'-'~zc Age Group and Sex Female Male Total~E N % N % N %"~2. 22-29 284 64.1 159 35.9 443 12.0,., 30-39 675 52.7 606 47.3 1281 34.7Ol
-o 40-49 724 54.9 595 45.1 1319 35.7~" 50-69 323 52.7 290 47.3 613 16.6~.sc 70+ 14 389 22 61.1 36 1.0•0Cl
'Mexico ~ 67; Italy - 50; Argentina - 46; Uni ted Kingdom - 38; India ~ 32; others > 20.2Data unavailable for 257 cases.
large percentage of the therapists surveyed described themselves as native born, andbelieve they are seen as part of the social, cultural, and ethnic majorities in theirhomelands.
Age, Gender, and Marital Status. The gender balance among these therapistsfavors women over men (55% to 45%), Two-thirds reported they are currently mar-ried or living with a partner. Ages ranged from 22 to 91 years, but most therapistswere between 30 and 50 years old (mean 41, median 40).
MEASURESOF THERAPISTPERCEIVEDDEVELOPMENT
Deuelopment Scales. A factor analysis of the DPCCQ items related to therapists'perceived development is presented in Table 7. Five factors were retained, account-

144 ORLINSKY ET AL.
TADLE7. Dimensions ofRetrospected Career Development and CurrentlyExperienced Developmenr'
Factors
Measure M sd % high- 2 3 4 5
Perceived Career Development[Pcvd Car, scaled 0-5; alpha - .75J
A-I. Changed overall. 3.7 1.1 59.4 79A-2. Overall progress. 4.1 1.0 78.5 .33 .74
Claimed Therapeutic Mastery[Tx Mast, scaled 0-5; alpha = .801
B-I. Mastery of technique. 3.4 0.9 48.2 .82B-2. Understand rnoment-by-moment. 3.4 0.9 48.3 .78B-3. Precision, subtlety, finesse. 3.2 1.0 41.4 .80
0rl B-4. Capable to guide others. 3.0 1.3 39.5 .760
'"" [A-4. Overcame Iimitations.l 3.1 1.1 36.0 .51 .51H
'" Currently Experienced Growth"c'" (CE Growth, scaled 0-5; alpha = .87 /.78]..,'" C-2. Improving. 3.7 1.1 64.7 .78'"M C-5. Becoming more skillful. 3.5 1.0 58.2 .77 .30'"M C-I. Changing as a therapist. 3.3 1.1 44.1 .75rl
~ e-s. Deepening understanding. 3.7 1.0 65.3 .74.:r- C-4. Overcorning limitations. 3.1 1.1 39.7 .690
C-7. Growing enthusiasm. 3.2 1.3 46.1 .680
'"w [E-I. Motivated to develop.l 4.5 0.9 86.8 .40 .30ud• Currently Experienced Loss.~Cl [CE Loss, scaled 0-5; alpha - .70 /.67]rl
'" C-9. Losing empathy. 0.8 1.2 4.1 .69d
S C-8. Becoming disillusioned. 1.2 1.2 5.1 .69~'"z C-3. Declining ability. 0.4 0.9 1.5 .67c'" C-IO. Performance becoming routine. 1.1 1.2 4.4 .66~Hw (A-3. Overall decline in abiliry.l 0.4 0.8 0.9 .62"-"
Currently Experienced Flowco [CE Flow, scaled 0-3; alpha = .68]-0w D-3. Feeling inspired. 1.9 0.8 24.7 .75-0
'"~ D-2. Feeling stimulated. 1.9 0.8 23.6 .72d• D-1. Feeling involved. 2.2 0.8 37.7 .640Cl
D-4. Feeling engrossed. 2.0 0.8 30.3 .57% variance 28.0 10.9 8.6 6.5 4.7
'Median N for analyses ~ 3581, range 2912-3683.2"High" for A, B, and C items was 4 or 5 on a 0-5 scale: "very" for D items was 3 on a 0-3 scale.
ing for 58.7% of the common variance. Dimensional scales for different aspects ofdevelopment were constructed, based on these factors: Perceived Career Develop-ment (iterns A-1 and A-2); Claimed Therapeutic Mastery (iterns B-1 through B-4);Currently Experienced Growth (items C-l, C-2, and C-4, these being chosen be-cause available for the largest number of subjects); Currently Experienced Loss (itemsC-3, C-8, C-9, and C-lO); and Currently Experienced Flow (iterns D-l, D-2, and D-3indicate, item D-4 omitted because it slightly lowered the alpha value). The scalefor Motivation to Develop (itern EvI ) had minor loadings on two factors but no

DEVELOPMENTOF PSYCHOTHERAP1STS 145
o.-<oN
strong loading on any, and was retained for its conceptual interest as aseparatescale in subsequent analyses. Levels of Cronbach's alpha ranged from .67 to .80,and were judged satisfactory.
Descriptive statistics for the iterns assessing therapists' career and current devel-opment are also presented in Table 7. On Perceived Career Development, 600Alfeltthey had changed much or very much overall, and 79% feIt that the change repre-sented much or very much progress. By contrast, high levels on items comprisingClaimed Therapeutic Mastery were less frequent, ranging only from about 40% to48%. High levels on Currently Experienced Growth were reported by as many as65%for some items(C-2and C-6,improving and deepening understanding of therapy),and as few as 40% on others (C-4, overcoming limitations as a therapist). Levels onitems comprising Currently Experienced Loss were low on average, but 4% to 5%reported relatively high levels of disillusion with therapy, routine performance, andloss of empathic responsiveness CC-lO,C-8, and C-9). On a more positive note, 38%of therapists feltvery involved during recent sessions, and 24%to 30%feltvery stimu-lated, inspired, and engrossed-strongly suggesting that many therapists experiencedflow when working with patients (Parks & Orlinsky, 1998).
Table 8 shows the items used to construct an index to assess career develop-ment indirectly by computing difference scores on eleven therapeutic skills. Thera-pists rated each separately for how they were when they first started to do therapeu-tic work and for how they were at present. To facilitate interpretation, items arepresented in order of amount of "change" (i.e., difference) from most to least. Theaveraged mean difference for each subject was used as an overall Skill "Change"Index (alpha = .87).
M
N
r-.ooN
TABLE8. "Change" in Therapist Initial and Current Levels ofTherapeutic Sldlls
Itemst M sd
6 How much mastery do you have of the techniques and strategiesinvolved in practicing therapy? +1.22 1.1
7 How weil do you understand what happens moment-by-mornentdu ring therapy sessions? +1.18 1.0
11 How good are you at making constructive use of YOUf personalreactions to patients? +1.14 1.1
2 How 'natural' (authentically personal) do you fee! working with patients? +1.12 1.210 How weil are you able to detect and deal with your patients' emotional
reactions to you? +1.09 1.13 How good is your general theoretical understanding of therapy? +1.08 1.15 How good are you at grasping the essence of YOUf patients' problems? +0.93 1.09 How skillful are you ar getting your patients to play their part in therapy? +0.92 1.01 How effective are you at engaging patients in a working alliance? +0.85 1.08 How effective are you in communicating your understanding and
concern to your patients? +0.78 1.04 How empathic are you in relating to patients with whom you have
relatively little in common? +0.70 1.0
Total Skill "Change" Index [Cronbach's alpba - .871 1.03 0.7
tRated from 0 - Not at All to 5 - Very.

o...•oN
NN
r-OoN
146 ORLINSKYET AL.
GENERALITYOF DEVELOPMENTMEASURES
The analyses in Table 9 compare groups of therapists in the CRNdata base withrespect to the measures shown in Tables 7 and 8. Demographie subgroups wereconstructed in terms of gender and nationality (countries with substantial numbersof therapists in the data base). Professional subgroups were constructed in terms ofprofessional background (medical vs. psychological training) and salient theoreticalorientation. The mean number of years in therapeutic practice, including trainingbut omitting any periods without practice, is shown for convenience in column 1.Statistieal tests were not computed, because the airn in making these comparisonswas not to test hypotheses about national or other differences but rather to inspectthe reasonableness of analyzing the aggregate data base with respect to the devel-opment measures. The statistical equivalence of subgroups on each measure wasassessed by computing effect sizes for the differences of subgroup means from thetotal mean, using ES < .4 as a criterion for considering the difference small (Elliott,Stiles, & Shapiro, 1993; Rogers, Howard, & Vessey, 1993).
Scale scores for Perceived Career Development are shown in Table 9, column 2.These figures were virtually identical when calculated separately for male and femaletherapists. Means and standard deviations on this scale were also very similar for thelarger national groups, with the exception of Korea.There was also littlevariation acrossorientation groups, although therapists trained as psychiatrists averaged somewhat lessthan psychologists, due perhaps to the lower average practice duration among thepsychiatrists.The means for ClaimedTherapeutic Mastery(column 3) for the most partranged between 3.2 and 3.6. Two exceptions to this relativeconsistencywere the Koreanand American groups, both of which were noticeably lower than the others in practiceduration. The average difference in estirnates of Initial and current therapeutic skiIls(SkilI"Change" Index, column 4) cIustered consistently around +1 (overall range was-3.6 to +3.9), with the exception once more of the Korean subgroup. Mean scores forMotivation to Develop (column 5) ranged from 4.2 to 4.6, but was lower for the Ko-rean group. Similarly,except for the Korean group, means for Currently ExperiencedGrowth (column 6) cIustered mainly between 3.3 to 3.6. Scale means for CurrentlyExperienced Flow (column 7) ranged berween 1.8and 2.3, although the Korean groupaveraged only 1.0. Finally, Currently Experienced Loss (column 8) ranged between0.7 and 0.9, with the Korean as an outlier at 1.2.
Table 9 yields a general impression of relative consistency across therapist group-ings, with the major exception being the group of Korean therapists, who were con-sistently lower in both direct and indirect ratings of their career and current develop-ment. The consistent differences observed are congruent with the fact that the Koreangroup contained a large proportion of psychiatry residents, and more trainees thanall but the American group. The discrepancy also invites further exploration of cul-tural differences between the Korean and Western therapists in the data base (seee.g., Joo, 1993; Kim, 1979; Markus & Kitayama, 1991).
INTERRELATlONSOF DEVELOPMENTMEASURES
The DPCCQ asks therapists on the same occasion to reflect about their currentexperiences of development and their sense of overall career development, and theseseparate judgments thus might be expected to influence each other. To explore theextent of potential overlap, the various dimensions of current and career develop-ment were intercorrelated (see Table 10). Except for Currently Experienced Loss,

Downloaded By: [German National Licence 2007] At: 13:23 22 January 2010
TABU 9. Values of Career and Current Development for Total Data Base and Major Subgroups"
Prac Prcvd Tx Skill Dev CE CE CEGroup N dur dev mast change! motiv growth flow' loss
Total 3795 M 9.5 3.9 3.3 1.0 4.5 3.4 2.0 0.9sd 7.7 0.9 0.9 0.7 0.9 0.9 0.6 0.8
Women 2060 M 8.8 3.9 3.2 1.0 4.6 3.5 2.2 0.8Men 1695 M 10.3 3.8 3.3 1.0 4.3 3.3 1.9 0.9Germany 1059 M 8.8 3.9 3.2 1.1 4.6 3.4 2.1 0.9Korea 538 M 5.5 3.3 2.9 0.6 3.6 2.9 1.0 1.2Norway 371 M 13.6 3.9 3.4 1.1 4.6 3.4 2.3 0.9Portugal 188 M 10.1 4.0 3.5 0.9 4.4 3.4 2.1 0.7Switzerland 255 M 12.9 4.0 3.6 1.3 4.5 3.4 2.2 0.8USA 329 M 6.3 3.9 2.9 0.8 4.5 3.6 2.1 0.8Psychiatry 1345 M 8.3 3.7 3.1 1.0 4.2 3.2 1.8 0.9Psychology 1767 M 11.1 4.0 3.5 1.l 4.6 3.5 2.2 0.8Analytic dynamic 1236 M 10.3 3.9 3.3 1.1 4.5 3.4 2.0 0.8Dynamic eclectic 607 M 10.1 4.0 3.4 1.1 4.6 3.5 2.1 0.8Cognitive behavioral 327 M 8.8 4.0 3.5 0.9 4.6 3.6 2.1 0.8Noncognitive behavioral eclectic 362 M 10.7 4.1 3.6 1.1 4.6 3.7 2.2 0.9Humanistic 217 M 9.4 3.9 3.4 1.2 4.4 3.3 2.1 0.9Prac dur = Practice duration (years), Prcvd dev = Perceived Career Developrnent, Tx mast = Claimed Therapeutic Mastery; Skill Change = Skill "Change" Index, meandifference between ratings of initial and current skills, Dev motiv = rated importance of further development as a therapist; CE growth = Currently Experienced Growth;CE flow 4 Currently Experienced Flow; CE loss = Currently Experienced Loss, Unless noted, scale 0-5."Bold print subgroup means are deemed nonequivalent as ES of difference from totalsample mean ~ .4'Original scale 0-3.

orloN
NN
MN
Mrl
r-OoN
148 ORLINSKY ET AL.
TABLE10. Interrelation of Career Development and CurrentDevelopment Measures
Prcvd Tx Skill Dev CE CE CEVariable dev mast change motiv growth flow loss
Perceived Career DevelopmentClaimed Therapeutic Mastery .38SkiIl "Change" Index .43 .42Motivation to Develop .34 .26 .22Currently Experienced Growth .48 .26 .18 .40Currently Experienced Flow .29 .26 .19 .35 .36Currently Experienced Loss -.14 -.06 -.11 -.19 -.16 -.18Practice Duration .26 .50 .29 -.04 -.03 .14 .00Factor 1. Career Development .66 .79 .77 .30
[alpha = .681Factor Il. Current Development .41 .69 .68 .65 -.61
[alpha = .65 for positive loadingsl
Prac dur = Practice Duration (years), Prcvd dev = Perceived Career Development; Tx mast ~ ClaimedTherapeutic Mastery: SkiJIchange = Skill "Change" Index, mean difference between ratings of Initial andcurrent skills; Dev rnotiv = rated importance of further development as a therapist; CE growth = CurrentlyExperienced Growth; CE flow - Currently Experienced Flow; CE loss - Currently Experienced Loss. Un-less noted, scale 0-5. N ranges from approximately 2800 to 3500 cases due to fluctuations in available data.
which was slightly negatively related to the other dimensions, moderate to strongpositive correlations were found between all other development scales, raising thepossibility that they might be measuring a general evaluative factor. However, asecond-order factor analysis (bottom of Table 10) shows that therapists dearly dif-ferentiated between their current and their overall development, with only a moder-ate overlap of Perceived Career Development on Factor II (Current Development),and a marginal overlap of Currently Experieneed Growth on Factor I (Career Devel-opment). This factorial differentiation is supported by the significant correlations ofpractice duration with measures of Career Development (r = .50 with Claimed Thera-peutic Mastery), but not with measures of Current Development.
DISCUSSION
The substantive results show that scales of the DPCCQ offer internally consistent,adequately differentiated, and broadly applieable measures of therapists' currentlyexperienced development and retrospeeted Career Development. A degree of con-struct validity was also demonstrated by the fact that the length of time therapistshad been in practice correlated positively with the measures of Career Developmentbut was unrelated to measures of Current Development.
The descriptive data presented show multiple dimensions of variation in theeurrent data base. This heterogeneity, especially between countries,> requires cau-
'Apparent differences found between therapists from different countries may in fact have more to dowith "accidental" differences in other basic characteristics (e.g., profession, experience level, theoreti-cal orientation, and gender) than with factors usually associated with nationality (e.g., social institu-tions, language, and national culture), To prevent unwarranted generalizations, it is also essential todescribe findings precisely, for exarnple, "differences between these German and American therapists"rather than "differences between German and American therapists."

o.-<oN
NN
MN
M.-<
r-,ooN
QJUCQJ
.~..,
.-<
'".§"'"ZC
~QJ2,
DEVELOPMENT OF PSYCHOTHERAP1STS 149
tion in the analysis and interpretation of findings. To ensure substantively meaning-ful results, examination of the distributions of key variables across identifiable sub-groups should be a preliminary step in analyses using the aggregated data base. Whensubgroup differences reflect more than a small effect, caution would indicate sepa-rate data analyses of the divergent groups. Relative equivalence in scores acrossheterogeneous subgroups offers evidence supporting the generality of the findings,despite the problem of unknown sample-to-population generalizability. That is, find-ings would be shown to apply to therapists of different characteristics, even thoughthe groups in quest ion might not be representative of their respective populations orproportionally representative of therapists at large.
Several types of research question can be validly pursued with a large andvaried data base, even when sarnple-to-population generalizability is unknown.Strong hypotheses of the form "all or most therapists have characteristie X" or "fewif any therapists show quality Y" can be falsified by demonstrating that only mod-erate numbers of therapists have characteristic X or that a fairly large number showquality Y. Findings that a very high proportion of therapists share eertain charac-teristics, despite marked differences in other respects, can also be made. An ex-ample of the latter is the finding that 88% to 97% of 2,400 otherwise diverse thera-pists (in a previous version of the CRN data base) rated their typical manner towardpatients as accepting, committed, friendly, involved, and warm (Orlinsky et al.,1996).
The size and heterogeneity of the CRN data base also make it possible to con-duet certain types of data analyses with strong interna I validity (through eontrolledeomparisons using multiple eovariates with adequate statistical power, or throughreplication aeross internally defined subgroups) and with partial external validity(emphasizing generality as weil as generalizability). Questions of generalizability alsoean be addressed indirectly in several ways: by detailed description of therapist pro-fessional and demographie characteristies, so that findings may be tentatively gener-alized to other therapists with similar eharaeteristies; by eomparing the eharaeteris-ties of therapists in the CRN data base with published reports of therapist sampies inother studies, and by supplementing the eurrent data base with random sampies ofmembers from specific therapeutic organizations.
RESEARCH ORGANIZATION AND AGENDA
The SPR Collaborative Research Network was organized to eonduet a long-termprogram of studies by combining the resources of researehers who share astranginterest in the development and practiees of psychotherapists but whose resourcesfor research are too limited to permit doing so individually. Like eooperative soei-eties in other sectors of the economy, the CRN gives researchers who combinetheir resourees an opportunity to produce something that they eould not otherwiseafford, and pravides access to a major data base they could not otherwise hope tohave for the individuals who share in its creation. Oversight of CRN operations isvested in a steering committee composed of the most aetive members. Administra-tive responsibility is vested in North Ameriean and European coordinators.f Oper-
6p. Gerin, H. Ambühl, and M, H, Rennestad have served, successively, as European coordinators, D.Orlinsky has served as North American coordinator.

o.-<oN
NN
MN
M.-<
r-,ooN
150 ORLINSKYET AL.
ating on an international scale (via email, fax, and attendance at SPR meetings)without paid staff, the CRNcan itself be viewed as testing an alternative model ofresearch organization that might prove useful in times of reduced funding (Orlinsky,1987).
Since it is not limited to the term of a research grant, the CRNprogram cancontinue, and continue to develop, as long as interest is sustained by those in-volved and by new colleagues who volunteer to participate. In order to promotecontinuity of effort among a slowly changing roster of participants, the CRNsteer-ing committee has adopted a long-term agenda consisting of aseries of steps to betaken in successive phases (see Table 11). Phase I extended from late 1989through1994, Phase II from 1994 through 1998, and steps are now under way to imple-ment Phase III.
The next step in our agenda involves presentation of analyses that explore themeanings of currently experienced development and perceived career developmentto the large and varied group of psychotherapists we have described (Orlinsky,Rennestad. Ambühl, et al., in press).
TABLE11. Phases and Steps in the CRNResearch Program
Phase I1. Recruitrnent and organlzation of colleagues into an international research team.2. Design of Initial research instrument to examine therapists' perspectives on
development.3. Creation and evaluation of parallel translations in several languages.4. Initial data collections.5. Data coding, and construction of an integrated, expandable data base.6. Preliminary data analyses and presentation of research reports at conferences.
Phase 117. On-going data collection to enlarge marginal groups in the initial data base.8. Integration of new colleagues and data collection in new geographie and cultural
areas.9. Publieation of initial analyses of developrnent and related areas of therapist
functioning.10. Collection of initial data on longitudinal individual development.
Phase III11. Expansion and refinement of research instrurnents:
Ca) expansion of instrumentation and data collection to collateral observationalperspectives;
(b) refinement of initial research instrument on basis of initial results and evalua-tion with newly collected data.
12. Expansion and refinernent of data base:Ca) comparison of accumulated data base to other studies reporting therapist
characteristics:(b) implementation of supplementary data collection initiatives ro balance areas of
evident under-representation and to compare the general data base wichtargeted random sampies.
13. Further analysis of interrelations and determinants of aspects of development.14. Assessment of therapist developrnent and related variables in relation to treatment
processes and outcomes.
o.-<oN
NN
MN
M.-<
<-ooN
DEVELOPMENT OF PSYCHOTHERAP1STS
REFERENCES
Abbott, A. (988). Tbe system of professions. Anessay on tbe diuision of expert labor. Chicago:University of Chicago Press.
Arnbühl, H., Botermans, j.-F., Meyerberg,).. &Orlinsky, D. 09%). Continuous or categoricalmeasures of tberapeutic orientation. Paper pre-senred at the 27th annual meeting of the Societyfor Psychotherapy Research, Amelia Island, FL.
American Psychiatrie Association. (1987). Diag-nostic and statistical manual of mental disor-ders, 3rd ed. revised. Washington, OC: Author,
Bales, R. F. (970). Personality and interpersonalbebaoior. New York: Holt, Rinehart, and Winston.
Beutler, L. E., Crago, M., & Azrimendi, T. G. (986).Therapist variables in psychotherapy process andoutcome. In S. L. Garfield & A. E. Bergin (Eds.)Handbooe cfpsycbotberapy and bebaoior cbange,3rd ed. New York: lohn Wiley.
Beutler, L. E., Machado, P. P. P., & Neufeldt, S. A.(994). Therapist variables. In A. E. Bergin &S. L. Garfield (Eds.) Handbook of 'psycbotberapyand bebaoior cbange, 4th ed. New York: lohnWiley.
Csikszentmihalyi, M. (975). Beyond boredom andanxiety. San Francisco: ]ossey-Bass.
Csikszentrnihalyi, M. (990). Flow: The psycbologyof optimal experience. New York: Harper & Row.
Elliott, R, Stiles, W. B., & Shapiro, D. A. (993).Are some psychotherapies more equivalentthan others? In T. R. Giles (Ed.) Handbook ofeffectiue psycbotberapy (pp, 455-479). NewYork: Plenum Press.
Fiedler, F. (950). The concept of an ideal thera-peutic relationship. fournal of Consulting Psy-cbology, 14, 239-245.
Gurman, A. S., & Razin, A. M. (977). Effectiuepsycbotberapy. A handbook of researcb. Oxford:Pergamon Press.
Henry, W. E., Sims, ]. H., & Spray, S. L. (971).Tbe fiftb profession: Becoming a psycbotbera-
pist. San Francisco: ]ossey-Bass.Holt, R R, & Luborsky, L. (958). Personality pat-
terns of psycbiatrists. New York: Basic Books.]00, E. (1993). Psycbotberapists in Korea: A cross-
cultural study of tbe 'Deuelopment of psycbo-tberapists common core questionnaire' andKorean psycbotberapists' current practice. Un-published master's thesis, University of Chicago,Committee on Human Development.
Kelley, F. L., & Fiske, D. W. (1951). Tbe predic-tion of 'performance in clinical psychology. AnnArbor: University of Michigan Press.
Kiesler, D. ]. (1966). So me myths of psycho-therapy research and the search for a paradigm.Psycbological Bulletin, 65, 110-136.
Kim, T. W. (1979). The Korean national characteras seen from the sociological perspective. Na-
151
tional Etbics, 8. Seoul: The Academy of KoreanStudies.
Kurzweil, E. (989). Tbe Freudians: A compara-live perspectioe. New Haven: Yale UniversityPress.
Lerner, R. M. (986). Concepts and tbeories ofhuman deuelopment, 2nd ed. Reading, MA:Addison-Wesley.
Lincoln, Y. S., & Guba, E. G. (985). Naturalisticinquiry. Newbury Park, N]: Sage.
Mabe, P. A., & West, S. G. (1982). Validity of self-evaluation of ability: A review and metaanalysis.
journal of Applied Psycbology, 67, 280-2%.Markus, H. R., & Kitayama, S. (991). Culture and
the self: Implications for cognition, emotion, andmotivation. Psycbological Review, 98, 224-253.
Matarazzo, R G. (1971). Research on the teach-ing and learning of psychotherapeutic skills. InA. E. Bergin & S. L. Garfield (Eds.) Handbookof psycbotherapy and bebauior cbange. NewYork: lohn Wiley.
Matarazzo, R. G. (978). Research on the teach-ing and learning of psychotherapeutic skills. InS. L. Garfield & A. E. Bergin (Eds.) Handbookof psycbotberapy and bebauior cbange, 2nd ed.New York: lohn Wiley.
Matarazzo, R. G., & Patterson, D. (986). Re-search on the teaching and learning of thera-peutic skills. In S. L. Garfield & A. E. Bergin(Eds.) Handbook of 'psycbotberapy and bebau-ior cbange, 3rd ed. New York: lohn Wiley.
Meltzoff, ]., & Kornreich, M. (970). Research inpsycbotberapy. New York: Atherton Press.
Orlinsky, D. E. (987). Houi to do researcb on psy-cbotberapy untbout a grant. Ulm: PSZ-VerlagUlm.
Orlinsky, D. E., Rennestad. M. H., Ambühl, H., Davis,J. D., Davis, M., WiUutzki, U., Boterrnans, ]-F., &Cierpka, M. (998). Psychotherapists' assessmentsof their development at different career levels.Psycbotberapy, in .press.
Orlinsky, D. E., & RusselI, R. L. (994). Traditionand change in psychotherapy research. InR. L. Russell (Ed.) Reassessing psycbotberapyresearcb. New York: Guilford.
Orlinsky, D. E., Willutzki, U., Meyerberg, ].,Cierpka, M., Buchheim, P., & Arnbühl, H. (19%).Die Qualität der therapeutischen Beziehung:Entsprechen gemeinsame Faktoren in der Psy-chotherapie gemeinsamen Characteristika vonPsychotherapeutInnen? [Qualities of the psy-chotherapeutic relationship: Do common fac-tors in psychotherapy reflect common charac-teristics of psychotherapists?] Psycbotberapie,Psychosomatik, medizinische Psychologie, 19%46, 102-110.
Parks, B. K., & Orlinsky, D. E. (998). Intrinsic

152
NN
MN
motiuations for psycbotberapeutic work. Unpub-lished manuscript, Unlversity of Chicago.
Parloff, M. B., Waskow,l. E., & Wolfe, B. E. (978).Research on therapist variables in relation to pro-cess and outcome. In S. L. Garfield & A.E. Bergin(Eds.) Handhook 0/psycbotberapy and bebau-ior cbange, 2nd ed. New York: lohn Wiley.
Parsons, T. (951). Tbe social system. Glencoe, IL:The Free Press.
Pinsof, W. M. (986). The process of family therapy:The development of the family therapist cod-ing systern. In L. S. Greenberg & W. M. Pinsof(Eds.) The psycbotberapeutic process: A researcbbandbook. New York: Guilford.
Rogers.]. L., Howard, K. 1.,& Vessey,J. T. (993).Using significance tests to evaluate equivalencebetween two experimental groups. Psycbologi-cal Bulletin, 113, 553-Q56.
Rennestad. M. H., & Skovholt, T. M. (991). Enmodell for profesjonell utvikling og stagnasjonhos terapeuter og radgivere. (A model ofthe professional development and stagnationof therapists and counselors.) Tidsserift forNorsk psyeologforening (Journal of the Norwe-gian Psychological Association), 28, 555-567.
Skovholt, T. M. & Rennestad. M. H. (992).Themes in therapist and counselor develop-
M...•
r-ooN
ORLINSKY ET AL.
ment. Journal 0/ Counseling & Deoelopment, 70,505-515.
Skovholt, T. M., 8i. Rennestad. M. H. (995). Theeooluing professional se/f: Stages and tbemes intberapists and counselor deoelopment (2nd ed.),Chichester, U.K.: lohn Wiley.
Special Series. (997). The therapist as a neglectedvariable in psychotherapy research. ClinicalPsycbology Science and Practice, 4, 41-89.
Strupp, H. H. 0955a). Psychotherapeutic technique,professional affiliation and experience level.Jour-nal of Consulung Psycbology, 19,97-102.
Strupp, H. H. 0955b). The effect of the therapist'spersonal analysis upon his techniques. Journal0/ Consulting Psycbology, 19, 197-204.
Truax, C. B., & MitchelI, K. M. (971). Researchon certain therapist interpersonal skills in rela-tion to process and outcome. In A. E. Bergin &S. L. Garfield (Eds.) Handbook 0/'psycbotberapyand bebauior cbange. New York: john Wiley.
White, S. H. (983). The idea of development indeveloprnental psychology. In R. M. Lerner (Ed.)Deoelopmental psycbology. Historical and pbilo-sopbical perspectioes. Hillsdale, N]: LawrenceErlbaum Associates.
Wicklund, R. A. (979). The influence of self-awareness on human behavior. Americari Sei-en/ist, 67, 187-193.
ZusammenfassungDiese internationale Studie hat zum Ziel, die Inhalte, Korrelate und wahrgenommenen Determinantender Entwicklung von professionellen Psychotherapeut(inn)en in unterschiedlichem Berufsstadium zuanalysieren. Die Psychotherapeutünnren kommen aus verschiedenen Ländern und Kulturen, gehörenunterschiedlichen Berufen an und sind unterschiedlichen theoretischen Orientierungen verpflichtet.Psychotherapeutische Entwicklung wird aus unterschiedlichen Perspektiven konzeptualisiert und erfaßt:durch aktuelle und retrospektive Berichte der Therapeuten, Querschnitts- und Längschnittanalysen dertherapeutischen Praxis und therapeutische Erfahrungen. In diesem Beitrag werden die wesentlichenFragen der Studie präsentiert, Kemkonzepte definiert und das Erhebungsinstrument vorgestellt. Außerdemwerden die Datenerhebung beschrieben und deskriptive bzw. auf die Skalenentwicklung bezogeneErgebnisse vorgestellt, die sich auf eine multinationale Datenbasis von ungefähr 3800 Therapeut(inn)enbezieht. Die Analysen deuten auf die Reliabilität und Validität direkter und indirekter Messungen derrückblickend berichteten und aktuellen Kariereentwicklung hin und zeigen deren Eignung für unter-schiedliche Gruppen von Psychotherapeut(inn)en.
ResumeCette etude internationale veut examiner la nature, les correspondances, et les determinants percus dudeveloppernent des psychotherapeutes professionnels ä tous les niveaux de carriere, provenant de payset de cultures variees, er form es dans des orientations theoriques et professionnelles differentes. Ledeveloppernent psychotherapeutique est conceptualise et evalue 1'1 partir de plusieurs perspectives, ycompris des rapports paralleles et retrospectifs par les therapeutes, et des analyses transversales etlongitudinales des pratiques er experiences des therapeutes. Cet article presente !es questions essentiellessous-jacentes ä l'etude, iI definit ses concepts de base, introduit l'Instrurnent de l'enquete, decrit le procedede recolte des donnees, et rapporte les donnees descriptives et concernant le developpernent de l'ecnellepour une base de donnees multinationale de presque 3800 therapeutes, Les analyses confirment la fideliteet la validite des mesures directes er indirectes du developpernent de la carriere du point de vue retrospectifer actuel, ainsi que leur validite d'application pour des groupes de psychotherapeutes divers.

DEVELOPMENT OF PSYCHOTHERAP1STS 153
ResurnenEste estudio intenta examinar la percepci6n que de la naturaleza, los correlatos y los determinantes desu formaci6n tuvo un grupo de psicoterapeutas profesionales de todos los niveles de formaci6n, dediferentes paises y culturas, y entrenados en diferentes profesiones y orientaciones te6ricas. EI desarrollodeI psicoterapeuta se conceptualiza y evalüa desde varias perspectivas, las que incluyen informes actualesy retrospectivos elaborados por los mismos terapeutas, asi tarnbien corno anälisis cruzados y longitu-dinales de sus experiencias y präcticas, Este trabajo presenta los principales interrogantes que guiaronel estudio, define su nücleo conceptual, introduce el instrumento utilizado para el relevarniento: de-scribe los procedimientos de recolecci6n de informaciön: e informa sobre los datos descriptivos y loscorrespondientes al desarrollo de escala de una base multinacional de datos de casi 3800 terapeutas.Los anälisis dan evidencia de la confiabilidad y la validez de las medidas directas e indirectas tanto deidesarrollo retrospectivo de sus carreras corno de 10 experienciado actualmente por ellos, asi tambiencorno de su aplicabilidad a diversos grupos de pslcoterapeuras.
o...•oN
Received June 14, 1996Revision Received June 13, 1998
Accepted July 17, 1998
NN
'"N'"...•
6oN
WUcW.~..,
Related Documents











