ANNE-MARIE DUPRE DPT, MS, NCS, AND SHELLEY GOODGOLD, S C D , PT Abstract: Many healthcare professions students are unaware of their own ethnocentrism, and movement along the continuum of cultural competence rnay not be possible until the students encounter individuals whose cultural beliefs, values, and needs differ significantly from their own. This project was an example of an international community service immersion experience in Nicaragua that led to increased cultural competency of five physical therapy students. Through immersion, the students progressed from cultural blindness to cultural precom- petence. To further foster student cultural competence, the conceptual framework needs to reflect the multiple facets of an individual's identity and influences on behavior change. Key Words: Cultural Competency, International Service, Physical Therapy, Physical Therapy Students DEVELOPMENT OF PHYSICAL THERAPY STUDENT CULTURAL COMPETENCY THROUGH INTERNATIONAL COMMUNITY SERVICE T he United States (U.S.) is steadily increasing in racial and ethnic diversity (U.S. Census Bureau, 2000). Consequently, providing quality health- care requires practitioners to have knowledge and respect for their patients' cultural point of reference, especially their patients' beliefs and attitudes toward health and illness. When life roles, value systems, and family expectations of patients in our care are incor- porated into practice, patient outcomes are enhanced [Black & Purnell, 2002). Since competency to treat individuals from other cultures is essential, it is the responsibility of academic and clinical educators to develop successful strategies for preparing students for this challenge. The purpose of this paper is to describe the de- Anne-Marie Dupre DPT, MS, NCS, is Clinical Assistant Professor of Physical Therapy, University of Rhode Island, Kingston, RL Shelley Goodgold, ScD, PT, is Professor of Physical Therapy, Simmons College, Boston, MA. Address correspondences to: Anne-Marie Dupre DPT, MS, NCS, 25 West In- dependence Way, Suite J, University of Rhode Island Kingston, RI 02881, or E-Mail: [email protected]. edu. velopment of student cultural competency through participation in an international community service course. Following a discussion of cultural competency in healthcare. Cross, Bazron, Dennis, and Isaacs' (1992) continuum of cultural competency was employed as a conceptual framework to elucid^ate the progress of five physical therapy students during an immersion community service experience in a small Nicaraguan village. The paper concludes with recommendations to improve future studies. DEFINITION OF CULTURE AND CULTURAL COMPETENCY Culture is a system of learned patterns of behavior that are shared by members of a given group (Lynch & Hanson, 1992). Children learn about their culture through a process of enculturation in which their par- ents and other older members of the group guide the younger generation in adopting the culture's ways of thinking and behaving. Each culture provides a flexible framework for members of the group to interact with each other and the environment, and an individual's culture also prescribes meaning for abstract concepts and symbolism (e.g., beauty or the colors for purity or death). Only when evaluated within the context of the individual's culture can behaviors be viewed as Journal of Cultural Diversity. • Vol. 14, No. 3 Fall 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANNE-MARIE DUPRE DPT, MS, NCS,AND SHELLEY GOODGOLD, S C D , PT
Abstract: Many healthcare professions students are unaware of their ownethnocentrism, and movement along the continuum of cultural competence rnaynot be possible until the students encounter individuals whose cultural beliefs,values, and needs differ significantly from their own. This project was an exampleof an international community service immersion experience in Nicaragua thatled to increased cultural competency of five physical therapy students. Throughimmersion, the students progressed from cultural blindness to cultural precom-petence. To further foster student cultural competence, the conceptual frameworkneeds to reflect the multiple facets of an individual's identity and influences onbehavior change.
Key Words: Cultural Competency, International Service, Physical Therapy,Physical Therapy Students
DEVELOPMENT OF PHYSICAL THERAPYSTUDENT CULTURAL COMPETENCY THROUGH
INTERNATIONAL COMMUNITY SERVICE
The United States (U.S.) is steadily increasing inracial and ethnic diversity (U.S. Census Bureau,2000). Consequently, providing quality health-
care requires practitioners to have knowledge andrespect for their patients' cultural point of reference,especially their patients' beliefs and attitudes towardhealth and illness. When life roles, value systems, andfamily expectations of patients in our care are incor-porated into practice, patient outcomes are enhanced[Black & Purnell, 2002). Since competency to treatindividuals from other cultures is essential, it is theresponsibility of academic and clinical educators todevelop successful strategies for preparing studentsfor this challenge.
The purpose of this paper is to describe the de-
Anne-Marie Dupre DPT, MS, NCS, is ClinicalAssistant Professor of Physical Therapy, Universityof Rhode Island, Kingston, RL Shelley Goodgold,ScD, PT, is Professor of Physical Therapy, SimmonsCollege, Boston, MA. Address correspondences to:Anne-Marie Dupre DPT, MS, NCS, 25 West In-dependence Way, Suite J, University of Rhode IslandKingston, RI 02881, or E-Mail: [email protected].
velopment of student cultural competency throughparticipation in an international community servicecourse. Following a discussion of cultural competencyin healthcare. Cross, Bazron, Dennis, and Isaacs' (1992)continuum of cultural competency was employed asa conceptual framework to elucid^ate the progress offive physical therapy students during an immersioncommunity service experience in a small Nicaraguanvillage. The paper concludes with recommendationsto improve future studies.
DEFINITION OF CULTURE AND CULTURALCOMPETENCY
Culture is a system of learned patterns of behaviorthat are shared by members of a given group (Lynch& Hanson, 1992). Children learn about their culturethrough a process of enculturation in which their par-ents and other older members of the group guide theyounger generation in adopting the culture's ways ofthinking and behaving. Each culture provides a flexibleframework for members of the group to interact witheach other and the environment, and an individual'sculture also prescribes meaning for abstract conceptsand symbolism (e.g., beauty or the colors for purityor death). Only when evaluated within the context ofthe individual's culture can behaviors be viewed as
Journal of Cultural Diversity. • Vol. 14, No. 3 Fall 2007

adaptive or maladaptive. Not everyone, however, withina culture should be expected to think and behave thesame.
Culture is a multi-dimensional construct with influ-ences occurring at regional, community, family, andindividual levels (Black & Purnell, 2002; Purnell &Paulanka, 2003). Spoken language including dialectand common phases and idioms, materials produced,and diet are cultural influences occurring at the regionallevel. At the community level, examples of culturalinfluences are socioeconomic background and type ofhousing. For example, it is common in an ethnic, lowersocioeconomic neighborhood with multifamily homesfor residents to know each other well and shop at thesame local market. In contrast, in an upper middleclass neighborhood with single-family homes situatedon large plots of land, neighbors more often may notknow each other or may not move beyond acquaintance.In addition, purchases are more often made from awide variety of supermarkets and malls. At the familylevel, culture is reflected in the family power structure,religious or spiritual worship, and the ways that stressis manifested. For example, for families who followtraditional gender role models, the father typically hasfinal authority and is viewed as the "bread winner".In contrast, whether or not the mother works outsideof the home, she is responsible for child rearing andthe family's social activities. For families with nontra-ditional gender roles, both parents may be viewed assharing the financial and child rearing responsibilities.At the individual level, cultural influences include so-cialization, coping methods, and hobbies.
The delivery of culturally competent healthcarerequires more than knowledge of lists of cultural traitsfor each ethnic group. Rather, it is the ability of thepractitioner to think and behave in ways that supporteffective interactions with members of other cultures(Cross et al., 1992). To demonstrate cultural competency,the practitioner must understand his/her own culturalvalues and those of other cultures; accept cultural dif-ferences in communication, thought processes, and be-haviors; and grasp how an individual's culture impactson his/her health beliefs and actions (Campinha-Bacote,2003; Dillard et al., 1992). For optimal care, the culturallycompetent healthcare provider must adapt his/her careto the patient's cultural beliefs and behaviors. Failure todevelop cultural competence can result in practitioner-client miscommunication, which can lead to inaccuratepatient history or irvformed consent, decreased patientsatisfaction with care, and patient nonadherence withhome programs (Campbell & Wilmelm, 1991; Flores,2000; Leavitt, 2003). For example, to develop a success-ful health promotion program for an individual fromanother culture with Type II diabetes and obesity, theclinician, at minimum, must understand the diet andpreferred foods and image of beauty in the client's cul-ture as well as the roles and responsibilities expected ofthat client by her community and family.
Evaluation of Cultural CompetenceAccording to Cross et al. (1992), cultural competency
of an agency or company develops in stages along a con-
tinuum from cultural destructiveness, a stage where theagency's behaviors are detrimental to those of anotherculture, to cultural competence, where the agency adaptscare based on acceptance and respect of cultural differ-ences. The highest stage on the continuum is culturalproficiency. At this stage, the members of the agencypractice evidence-based^ healthcare. Interventions arebased on the best research evidence available and theclinician's experience and are individually tailoredto match the client's culture-specific background andpreferences.
Although Cross et al.'s (1992) stages were originallydeveloped to categorize an agency's stage of culturalcompetence, they have been extrapolated to identifythe cultural competence stage of individual healthcareprofessionals. To elucidate the potential impact ofprejudice and bias at the individual level. Table 1 pro-vides descriptions of behaviors and attitudes for eachof Cross et al.'s stages. Leavitt (2002, 2003) used Crosset al.'s stages within an American Physical Therapy As-sociation (APTA) home study course entifled DevelopingCultural Competence in a Multicultural World. This coursewas designed for physical therapists to learn and assesscultural competency. In a qualitative pilot study, Veldeand Wittman (2001) assessed the cultural competence ofthree occupational therapy faculty members and eightoccupational therapy students after immersion in acommunity program serving elderly African Americancitizens. Self-assessments, utilizing Cross et al.'s (1992)cultural competence continuum, were completed at theend of the program only. Through triangulation usingobservations, journals, and interviews, the authorsreported that Cross et al.'s Continuum for (lulturalCompetence was an effective self-assessment tool.
Challenges for Academic EducatorsAccreditation standards for most healthcare academ-
ic and clinical education programs require inclusion ofmaterial relevant to cultural diversity and competence;however, specific guidelines are often not prescribed(American Physical Therapy Association [APTA], 2004).Healthcare educators are, therefore, faced with the chal-lenge of developing curricula that enhance students'knowledge, beliefs, and attitudes toward acceptanceand respect of cultural differences. One teaching ap-proach commonly used by allied health programs isintegration of cultural concepts as threads throughoutthe curriculum (Black, 2001). Another common approachis to provide seminars or modules related to culture,and a third frequent approach is to provide a speciflccourse, either discipline specific or interdisciplinary, oncultural considerations in healthcare.
Black (2001) reviewed the literature on curricularinclusion of culture and diversity in physical therapy,social work, and nursing programs. Comparatively,this author found a paucity of published literaturefor physical therapy and interpreted this finding asevidence that physical therapy lagged behind the othertwo disciplines. Black noted^that physical therapy edu-cators generally recognized the importance of culturalcompetency but were only at the beginning stages ofthe continuum.
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007

Table 1. Stages of Cultural Competency
Stage
1
2
3
4
5
6
Name
Cultural Destructiveness
Cultural Incapacity
Cultural Blindness
Cultural
Cultural Competence
Cultural Proficiency
Definition
• Purposefully destructs cultureDehumanizes or sub-humanizes minority clients
Holds paternal posture toward "lesser" races• Believes in the supremacy of the dominant culture
Holds philosophy of being unbiasedBelieves that helping approaches traditionally used by thedominant culture are universally applicableBehaviors reflect a well-intended liberal philosophyIgnores cultural strengths, encourages assimilation, andblames the victim for their problems
• Views differences from the cultural deprivation model whichasserts that problems are the result of inadequate culturalresources
PrecompetenceRealizes own weakness in serving minorities and attempts toimprove some aspect of serviceDesires to deliver quality services by asking "What can wedo?"Has begun the process of becoming culturally competent butlacks information on what is possible and how to proceedHas a false sense of accomplishment or of failure thatprevents the person from moving forward along thecontinuum
• Engages in continuous self-assessmentFocuses attention on the dynamics of difference, continuouslyincreases cultural knowledge, and implements a variety ofadaptations to service models
Holds culture in high esteemConducts research, develops new therapeutic approaches,publishes, and disseminates
Mote: Adapted from Cross et al. (1992).
While most healthcare students receive education onculture and developing cultural competency, applicationof this knowledge in practice may be lacking. Fitzgerald,Williamson, and Mullavey-O'Byrne (1998) investigatedcultural competency of two groups, students and thera-pists, from three allied health professions: occupationaltherapy, diversional therapy, and physical therapy. Thestudents were asked to define culture, and the thera-pists were not only asked to define culture but (also) toprovide examples from their clinical experiences. Theresearchers found that both groups expressed a limitedunderstanding of culture. The students and therapistsoften used words in association with ethnicity and raceto describe a materialistic or an outward manifestationof culture. Few words that reflected ideas, morals, orperceptions were used in their definitions, which indi-cated a limited understanding of how culture producesthese manifestations. In other words, students and thera-
pists treated culture as a concrete concept rather thanas an abstract one with concrete consequences. Whentherapists used terms that indicated values, attitudes,and beliefs in their definition, the investigators uponfurther questioning found that these were the therapists'ethnocentric interpretations and not a true reflection ofthe clients' attitudes and beliefs.
Cultural Encounters and ImmersionCultural encounters have been reported to enhance
the development of cultural competency (Black, 2002;Campbell & Wilhelm, 1991; Pope-Davis, Prieto, Whita-ker, & Pope-Davis, 1993; Utsey & Graham, 2001). Manyhealth professionals are unaware of their own ethnocen-trism (i.e., false assumptions about the ways of others orerroneous judgments based only on one's own culturalperspective). Professionals may not even recognizetheir prejudices until their awareness is raised through
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007

encounters with individuals whose values differ signifi-cantly from their own (Tabi & Mukherjee, 2003).
Thus, experience with individuals of different cul-tures is a key educational component to bring studentsto a level of cultural competency. Heuer and Bengiamin(2001) found improved^ cultural awareness of sevennursing students after spending 2 weeks in Moscow,Russia. Supporting these findings, Pope-Davis, Eliason,and Ottavi (1994) reported that nursing students withwork experience in a setting with diverse patient popu-lations scored higher on a scale of multicultural sensitiv-ity and knowledge than nursing students without suchwork experience. In another study with occupationaltherapists, Pope-Davis et al. (1993) reported that work-ing with patients from varied ethnic minorities was astronger contributor to developing cultural competencethan attending cultural sensitivity courses or work-shops. In addition, acceptance and respect of culturaldifferences was reported by Black (2002) when physicaltherapy students were immersed in a clinical experienceat a local homeless shelter. Using a qualitative design.Black employed triangulation and based conclusionson data collected through observation, journal entries,and interviews which were recorded during and afterthe clinical experience. This finding was further sup-ported by Utsey and Graham (2001) who, using a similarmethodology, reported that physical therapists whoparticipated in a community-based medical missiontrip moved to higher levels of cultural sensitivity.
Immersion, through living in a culture differentfrom ones' own, provides the potency of experiencingreal-life challenges on a first-nand basis (Leonard &Plotnikoff, 2000). The purpose of this project, therefore,was to promote the development of cultural competencefor physical therapy students who participated in aninternational community service course. As indicatedpreviously, many health professionals are unaware oftheir own ethnocentrism, and movement along thecontinuum of cultural competence is not possible untilthe individual is personally faced with providing health-care for individuals whose cultural beliefs, attitudes,values, and needs differ significantly from their own.With knowledge gained from this project, educationalexperiences to enhance student cultural competencycan be developed and empirically tested.
METHODSCourse
All entry-level professional doctorate in physicaltherapy (DPT) students at Simmons College are requiredto complete one-credit of community service. Com-munity service provides an opportunity for students tolearn through active participation in organized activitiesthat meet the needs of the community. The most crucialpart of this framework is immersion in the community.One community service opportunity at Simmons Col-lege includes international travel and immersion in theNicaraguan healthcare system. During winter break,physical therapy students, accompanied by a physicaltherapy faculty member and other members of the Sim-mons community, spend two weeks in San Juan del Sur,Nicaragua serving clients with physical therapy needs.
This international immersion course provides the stu-dents with real-life situations that provoke self-aware-ness of the students' own beliefs, increase knowledgeof the culture through personal exposure, and provideopportunities for students to both observe modeling ofculturally competent care by their professor and practiceculturally competent healthcare.
Cultural competency objectives for this internationalcommunity service course are to (a) demonstrate anunderstanding of the differences among individualsand cultures; (b) display sensitivity by considering dif-ferences in race, creed, color, gender, age, national orethnic origin, sexual orientation, and disability or healthstatus in making clinical decisions; (c) recognize aspectsof behavior and care affected by individual needs andcultural differences; (d) discover, respect, and value in-dividual differences within and among cultures; and (e)individually tailor therapeutic programs and delivery ofhealthcare based on the client's impairments, functionallimitations, cultural background, roles and responsibili-ties, and preferences. At present, these objectives are notmeasured on a standardized scale. Rather, the topics areaddressed through required readings and class groupdiscussions prior to travel to Nicaragua as well as dailygroup discussions, observations by the physical therapyfaculty member, and student self-reflection throughjournaling during the stay in Nicaragua.
Description of SiteSan Juan del Sur is a Pacific Coast port in southern
Nicaragua, not far from the boarder of Costa Rica. About10,000 people live in town, and another 10,000 live in the250 square miles of countryside (referred to as campos)that comprise most of the municipal district. Fishing,farming, and tourism are the mainstays of the economy.There are two health clinics in town (i.e., one public,one private) and several smaller health clinics in thecountryside. In town clinics, there is only one physicaltherapist on staff, and space consists of two plints (e.g.,treatment tables), a hot plate with a pot for hot packs,and some posters on health and exercise. The smallerclinics are occupied by staff only one to two times permonth when the roads are passable in the dry season.These clinics lack diagnostic equipment, such as x-rayor ultrasound machines.
ParticipantsAll six of the Simmons College physical therapy stu-
dents who registered for the International CommunityService course between 2002 and 2004 volunteered toparticipate in the project, which was approved by theSimmons College Institutional Review Board. All ofthe students were in their second year of the physicaltherapy curriculum. At this point in their education,they have completed the foundational and clinical sci-ence courses for the cardiopulmonary system and themusculoskeletal system and a 14-week clinical rotationin either an outpatient or acute care setting. Ability tospeak Spanish is required for participation in the course,but only one of the six students was fluent. Data fromfive of the six students are presented in this paper, be-cause one student did not submit questionnaires.
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007
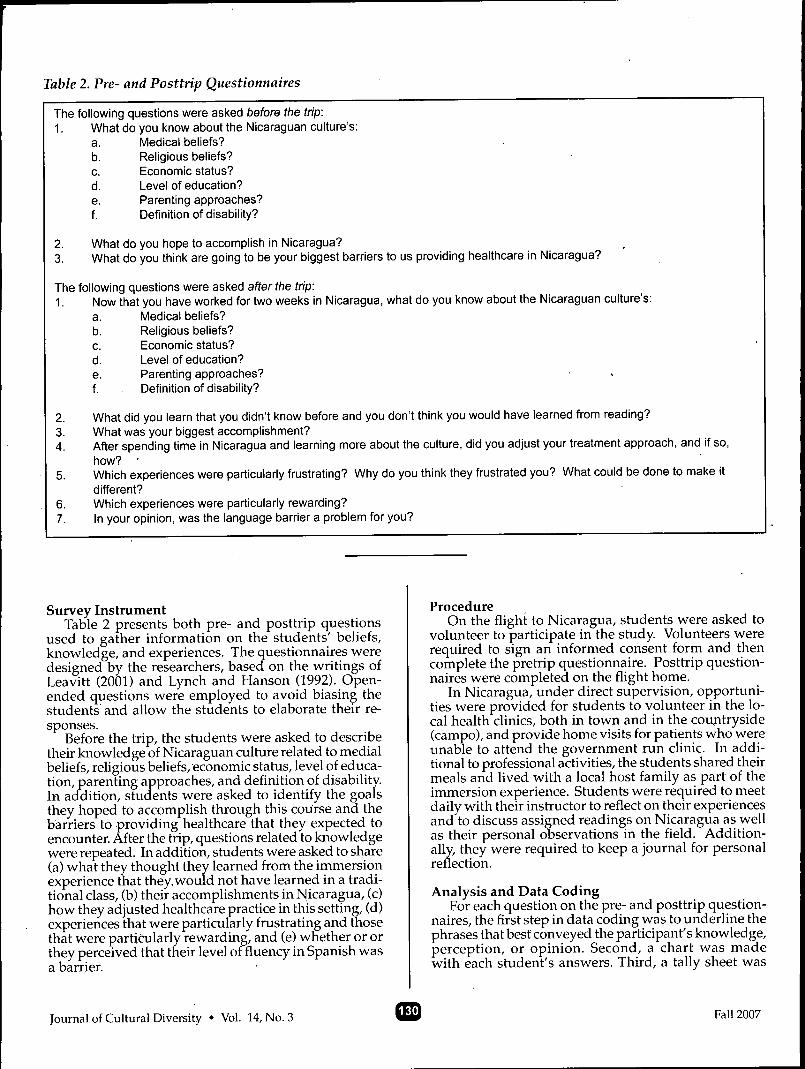
Table 2. Pre- and Posttrip Questionnaires
The following questions were asked before ttie trip:1. What do you l<now about the Nicaraguan culture's:
a. Medical beliefs?b. Religious beliefs?c. Economic status?d. Level of education?e. Parenting approaches?f. Definition of disability?
2. What do you hope to accomplish In Nicaragua?3. What do you think are going to be your biggest barriers to us providing healthcare in Nicaragua?
The following questions were asked after ttie trip:1. Now that you have worked for two weeks in Nicaragua, what do you know about the Nicaraguan culture's:
a. Medical beliefs?b. Religious beliefs?c. Economic status?d. Level of education?e. Parenting approaches?f. Definition of disability?
2. What did you learn that you didn't know before and you don't think you would have learned from reading?3. What was your biggest accomplishment?4. After spending time in Nicaragua and learning more about the culture, did you adjust your treatment approach, and if so,
how? •5. Which experiences were particularly frustrating? Why do you think they frustrated you? What could be done to make it
different?6. Which experiences were particularly rewarding?7. In your opinion, was the language barrier a problem for you?
Survey InstrumentTable 2 presents both pre- and posttrip questions
used to gather information on the students' beliefs,knowledge, and experiences. The questionnaires weredesigned by the researchers, based^ on the writings ofLeavitt (2001) and Lynch and Hanson (1992). Open-ended questions were employed to avoid biasing thestudents and allow the students to elaborate their re-sponses.
Before the trip, the students were asked to describetheir knowledge of Nicaraguan culture related to medialbeliefs, religious beliefs, economic status, level of educa-tion, parenting approaches, and definition of disability.In addition, students were asked to identify the goalsthey hoped to accomplish through this course and thebarriers to providing healthcare that they expected toencounter. After the trip, questions related to knowledgewere repeated. In addition, students were asked to share(a) what they thought they learned from the immersionexperience that they, would not have learned in a tradi-tional class, (b) their accomplishments in Nicaragua, (c)how they adjusted healthcare practice in this setting, (d)experiences that were particularly frustrating and thosethat were particularly rewarding, and (e) whether or orthey perceived that their level offluency in Spanish wasa barrier.
ProcedureOn the flight to Nicaragua, students were asked to
volunteer to participate in the study. Volunteers wererequired to sign an informed consent form and thencomplete the pretrip questionnaire. Posttrip question-naires were completed on the flight home.
In Nicaragua, under direct supervision, opportuni-ties were provided for students to volunteer in the lo-cal health clinics, both in town and in the countryside(campo), and provide home visits for patients who wereunable to attend the government run clinic. In addi-tional to professional activities, the students shared theirmeals and lived with a local host family as part of theimmersion experience. Students were required to meetdaily with their instructor to reflect on their experiencesand to discuss assigned readings on Nicaragua as wellas their personal observations in the field. Addition-ally, they were required to keep a journal for personalreflection.
Analysis and Data CodingFor each question on the pre- and posttrip question-
naires, the first step in data coding was to underline thephrases that best conveyed the participant's knowledge,perception, or opinion. Second, a chart was madewith each student's answers. Third, a tally sheet was
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007

developed by grouping similar answers into thematiccategories. For each theme, the number of students withsimilar answers was tallied. In this way, generalizedpatterns of responses were made evident.
To determine pre- and posttrip Continuum of Cul-tural Competence stages, each student's underlinedphrases and identified themes were compared and con-trasted to Cross et al.'s (1992) stage descriptions. Usingthis process, the stage or stages that reflected similarbehaviors, beliefs, and attitudes were identified, andeach student was categorized into a stage.
RESULTSPretrip Findings
Before the trip, students had limited knowledge ofa general nature. When asked about the Nicaraguanmedical or health beliefs, all five students responded "Idon't know". For the question on religious belief, all ofthe students identified that most Nicaraguans had strongCatholic beliefs. When asked to give information on theeconomic situation in Nicaragua, students respondedthat it was "poor", "poverty by the United States stan-dards", "third world with limited resources", and "thepoorest nation in the Western hemisphere". Educationallevel was defined as less than 6"' grade by three students;two students responded "I don't know".
Responses to questions on parenting and the defini-tion of^disability varied across the five students. Twostudents stated they did not know the typical Nicara-guan approach to parenting. One student was not sureand questioned if the Nicaraguan people had closefamily ties. Another student expressed that parent-ing was very family oriented, and in contrast, the fifthstudent expressed that Nicaraguan parenting was amaternal responsibility. For the definition of disability,two students responded "I don't know", one studentdescribed Nicaraguan definition of disability in termsof limitations in and individual's quality of life, and twostudents defined disability from the perspective of theindividual as a nonproductive member of society.
When asked to identify their goals, all of the studentsdocumented that they hoped to learn about a newculture. Other goals included to improve communica-tion skills, to improve physical therapy skills, and tohelp people. The students identified that the biggestanticipated barriers to providing healthcare serviceswere limited language fluency, limited resources fortreatment, not knowing or understanding the culture,and encountering unfamiliar conditions.
Pretrip questionnaire responses for all five studentsmatched four of the five descriptive criteria of Cross etal.'s (1992) Stage 3: Cultural Blindness. These includedbeliefs that traditional helping approaches are univer-sally applicable, a well intended^ liberal philosophy,ignorance of strengths in Nicaraguan culture, and viewof Nicaraguan culture from a deprivation model (i.e.,problems result from inadequate resources).
Posttrip FindingsAt the completion of the immersion experience, stu-
dents' responses regarding Nicaraguan culture weremore developed and refined. Descriptions of Nicara-
guan medical beliefs included "limited understanding/education on pathology or causes of most illnesses";"blend of scientific, spiritual, naturalistic, and folklorebeliefs"; "belief that God will help"; and "very trustingof medical personnel with the expectation for a quickfix".
All of the students responded that Roman Catholi-cism was the most prevalent religion and that Nicara-guans are very religious. One student, however, alsoacknowledged that there were "more Protestants andEvangelists than expected". One student indicated thatNicaraguan people had a strong faith in God and heldthe belief that God will always help. Another studentnoted stated that the Nicaraguans demonstrated theirreligious devotion by displaying many statues andsymbols.
With respect to economic status, in addition to stilldescribing most Nicaraguan citizens as poor, the stu-dents noted that there was an economic class system inNicaragua. The students also identified that many Ni-caraguan men had to leave their hometowns or villagesto find work in the city; however, due to the corruptionwithin the government, Nicaraguans with the greatestwealth were generally politicians. Despite the povertythat was observed on a first-hand basis, one studentreported that most Nicaraguan citizens were "o.k." withtheir economic status and adapted to the status quo.
On the question related to educational status, al-though all of the students again reported that mostcitizens of Nicaragua had little formal education (i.e.,equal or less than 6"" grade) and limited reading abilities,they also noted that there were emerging educationalopportunities for children. The students knew thatsecondary education was now available to Nicaraguanyouth in larger, more populated towns like San Juandel Sur than in rural areas, and one student made theconnection between economic status and educationby identifying the opportunity for students to obtain acollege education in the capital of Managua if familiescould afford to pay.
Through living with their host families, the studentsobserved the influences of an extended family of grand-parents, aunts, and uncles living in the same home andsharing the responsibilities of raising the children. Acollectivist perspective, in which the family is viewedas a whole, was developed by all five students. Themembers of the family were not viewed as individualsas much as working as a whole and representing fam-ily in society. The students, however, observed anddescribed the relative inequality between the sexes.They reported that Nicaraguan men worked outside thehome, whereas women typically stayed in the home tocare for the children and the elderly family members.
A collectivist perspective was also reflected in four ofthe five students' responses to the question on the defini-tion of disability. Except for one student who stated thatshe did not know how the Nicaraguan people defineddisability, other students relayed that in the small vil-lages they encountered families that considered a childor an adult with a disability as nonproductive. Thestudents observed that these families perceived having
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007

a family member with a disability as being "shameful"and hid the individual from the community.
When asked what they learned from the immersionexperience that they did not think they would havelearned from reading, one student indicated that "beingthere helped me understand the culture more than anybook could". Four students reported that they learnedthat communication, both verbal and nonverbal, wasthe key to understanding the Nicaraguan way of life.One student also reported the value of learning to be"comfortable with the unknown". Another studenthighlighted a better understanding of the "strong politi-calbeliefs and opinions" of the Nicaraguan people. Allstudents identified that their biggest accomplishmentwas adapting physical therapy so that the goals wereimportant and̂ meaningful in the Nicaraguan cultureand that the interventions were practical in this villagesetting. Students commented on the challenge of "pick-ing PT treatment outcomes that are important to them[Nicaraguans]" which were, at times, different fromoptimal outcomes that were learned in school.
When asked about the experiences that were par-ticularly frustrating, all five students reported beingfrustrated by the lack of medical care for the Nicara-guans, especially for Nicaraguans who could not affordservices. They were also frustrated that they were notable to provide more or better care given the limitedresources. One student reported that, "when I couldn'thelp, it felt like the energy was being drained out of meemotionally". Many students also reported that limitedfluency in Spanish was a significant barrier to under-standing the Nicaraguan people and their culture.
Analysis and coding of posttrip responses indicatedthat all five students met descriptive criteria of Crosset al.'s (1992) Stage 4: Cultural Precompetence. Thesecharacteristics included self-awareness of weakness inthe ability to serve individuals of another culture butintention to improve, the desire to delivery quality care,a lack of information on what is possible and how toproceed, and a false (i.e., inaccurate, incomplete) senseof accomplishment or failure.
DISCUSSIONRace, ethnicity, and culture are powerful influences
that affect an individual's personal identity and howthat individual thinks, feels, and behaves. This includeshow individuals perceive health, illness, and participatein their own healthcare. Cultural competency in the de-livery of healthcare services is an important key to suc-cessful patient outcomes, and immersion in a differentculture nas been shown to enhance cultural sensitivity.This project is an example of an intemationai communityservice immersion experience in Nicaragua that led toincreased cultural competency of professional doctoratein physical therapy (DPT) students.
Prior to the immersion experience, all of the studentswere categorized as being in Cross et al.'s (1992) Stage 3:Cultural Blindness. They had little to no factual under-standing of the Nicaraguan culture, and ethnocentrismwas reflected in their description of the Nicaraguanculture through a comparison to their own. For example,they described the Nicaraguan economy by comparing it
to U.S. standards. The student's decision to participatein this international community service course, however,revealed their desire to learn about another culture anda different way of life.
Cultural shock describes the anxiety produced whenan individual is immersed in a completely differentenvironment from his or her own (Leavitt, 1999). Forthree of the five students, this immersion trip was theirfirst time outside of the United States. Being in a foreigncountry and living with a Nicaraguan family was acultural shock for them.
At the beginning, ethnocentrism was demonstratedas the students observed their surroundings; they didnot accept and respect the differences. Instead, theysaw only what they perceived to be lacking in the Ni-caraguan culture. They talked about how "messed up"the Nicaraguan healthcare system was with its pooraccessibility and limited resources (e.g., medications,diagnostic equipment). They discussed the profoundpoverty they encountered in the campos. They saw thatmany standard procedures (e.g., surgery for a hip frac-ture) could not he provided, and they viewed povertyas limiting all aspects of the Nicaraguan people's lives.The students also viewed the low educational level oftheir Nicaraguan clients as a limiting factor to providinghealthcare.
Early on, the students focused on the outwardmanifestations of the Nicaraguan culture rather thanexamine how these outward manifestations reflected theunderlying beUefs and values of the people. In addition,their perceptions were unidimensional. For example,they expressed their knowledge of Nicaraguan religiousbeliefs as "Catholicism", economic status as "poverty",and level of education as "less than 6"" grade". Theseresponses are similar to previously reported findings.Fitzgerald et al. (1998) found that physical therapy stu-dents treated culture as a concrete concept rather thanan abstract one with concrete consequences.
Although the students in our project anticipated thattheir limited knowledge about trie Nicaraguan culturewould be a barrier, they thought that Western helpingapproaches would be applicable in Nicaragua. Whenthe students first started providing physical therapyservices, they prescribed exercises based on protocolswith which they were familiar. Frequently, the studentsblamed the patients for their problems, stating "They(the Nicaraguans) don't want to learn about physicaltherapy and exercise. They just want a quick fix."
After a week of immersion in Nicaragua, the studentsbecame aware of the need to modify and adapt theirinterventions and programs to better match the limitedresources and limited time in their clients' days to exer-cise. The students became more realistic and providedmore ecologically valid programs and functional solu-tions to each patient's individual needs.
Often, however, the students lacked therapeuticknowledge of what was possible and how to proceedin the Nicaraguan culture. With instructor modeling,mentoring, and guided questions, the students learnedto use tape to adapt a pencil for a child with cerebralpalsy; constructed a ladder from an old pipe and ropepurchased at the local market to serve as an over head
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007

trapeze for a elderly man who was bedridden after astroke and hip fracture, and collaborated with a localcarpenter to construct a standing frame for a child witha movement disorder.
By the end of the two weeks, all students had pro-gressed to the next stage in Cross et al.'s (1992) con-tinuum. Stage 4: Cultural Precompetence. While thestudents recognized the weaknesses of the Nicaraguanhealthcare system, they also better understood their ownculture and the Nicaraguan culture. During discussionswith their instructor, the students identified two factorsthat greatly influenced their overall development ofcultural competency. The first was the ability to speakthe client's language. Speaking Spanish allowed thestudents to explore the Nicaraguan customs and healthpractices. While all of the students improved in theircommunication skills and fluency, the language barriercontinued to be the biggest challenge in the provisionof physical therapy services.
The second factor was the students' raised awarenessthat they could learn from "the locals". Before they leftthe U.S., all of the students believed that they were goingto be the expert, helping professionals (e.g., "I am goingto teach them everything I know."). Instead, they foundthat learning couW and should be a two-way street. Oneexample was when the students met a Nicaraguan manwho had had a left-sided stroke and a right shoulderirijury resulting in partial paralysis affecting both sideso/his body The students and instructor were awed withthis man's independence with dressing and functionalmobility despite significant motor and sensory impair-ments. He exercised every day pushing a homemadewooden wheelbarrow up and down the unpaved streetsdespite his significant impairments. The students sawhow a wheelbarrow could substitute for a walker; itwas, in fact, more functional than a rolling walker giventhe cobblestone and dirt roads and the capacity of thewheelbarrow to transport large items.
Although not identified by the students, two ad-ditional influences fostered cultural competency: (a)multiple role relationships the students developed byliving with host families, and (b) the clients' perceptionsthat the students possessed a high level of expertise. Thestudents gained the affection and trust of the familiesthrough living in their homes and sharing daily life. Inaddition, the students were viewed as credible basedon their U.S. nationality and training, and the Nicara-guans who received healthcare services made no overtdifferentiation between the students and the instructor.These factors have been shown to enhance help seekingand therapeutic effectiveness, respectively (Sue, 2001).
CONCLUSION AND DIRECTIONS FOR FUTURERESEARCH
This project is an example of an international com-munity service immersion experience in Nicaragua thatled to increased cultural competency of the participants.Cross et al.'s (1992) continuum of cultural competencywas employed to assess the physical therapy students'progress, which advanced from cultural blindness tocultural precompetence. Cross et al.'s model providedour conceptual framework for evaluating cultural
competency; however, the criteria for the stages wereextrapolated from descriptions of institutional culturalcompetency. Also, the stages do not explicitly identifythe three domains of cultural competency (i.e., beliefs,knowledge, and skill) adopted by the counseling profes-sions (Sue, 2001). In addition, measures adapted fromthe model need further testing of validity and reliability.Another limitation of this project was that the question-naires focused on knowledge about Nicaraguan cultureand did not address the influences of other group refer-ences, such as age, gender, marital status, or geographiclocation. Furthermore, this study did not explore noweach student's cultural background or identity or otherdemographic variables interact with the developmentof cultural competency.
Immersion is a potent force that perturbs the statusquo and facilitates self-awareness and culturally com-petent behaviors. To further foster development ofstudent cultural competence, our conceptual frameworkneeds to be expanded to reflect the multiple facets ofan individual's identity and the influences on behaviorchange. Then, the framework needs to be empiricallytested with larger samples in varied settings. In ad-dition, as healthcare providers, we function withinorganizational and societal contexts. Therefore, whenhealthcare professions students return to their nativecountry, the ability to maintain and transfer beliefs,knowledge, and skills learned through immersion ex-periences needs to be examined.
REFERENCESAmerican Physical Therapy Association. (2004). A nor-
mative model of physical therapist professional education:Version 2004. Alexandria VA: Autlior.
Black, R. M. (2001). Comparison of multicultural Htera-ture in three health professions: Physical therapy,nursing and social work. Journal of Cultural Diversity,8(1), 3-13.
Black, J. D. (2002). "Hands of hope": A qualitative in-vestigation of a student physical therapy clinic in ahomeless shelter. Journal of Physical Therapy Education,16(2), 32-34.
Black, J. D, & Purnell, L. D. (2002). Cultural competencefor the physical therapy professional. Journal of Physi-cal Therapy Education, 16(1), 3-10.
Campbell, S. K., & Wilhelm, I. J. (1991). Meaning ofculture in pediatric rehabilitation and healthcare.Physical and Occupational Therapy in Pediatrics, 21(4),1-42.
Campinha-Bocote, J. (2003). The process of cultural com-petence in the delivery of healthcare services: A cultur-ally competent model of care (4"' ed.). Cincinnati,OH: Transcultual Care Associates.
Cross, T. L, Bazron, B. J., Dennis, K. W, & Isaacs, M. R.(1992). Towards a culturally competent system of care(Vol. 1). Washington, DC: Georgetown UniversityChild Development Program, Child and Adoles-cent Service System Program Technical Assistance
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007 •!

Center.Dillard, M., Andonian, L., Flores, D., Lai, L;, MacRae,
A., & Shakir, M. (1992). Culturally competent oc-cupational therapy in a diversely populated mentalhealth setting. The American Journal of OccupationalTherapy, 46(8), 721-726.
Fitzgerald, M. H., Williamson, P., & Mullavey-O'Byrne,C. (1998). Analysis of therapistdefinitions of culture.Physical and Occupational Therapy in Geriatrics, 15(4),41-65.
Flores, G. (2000). Culture and the patient-physician re-lationship: Achieving cultural competency in health-care. Journal of Pediatrics, 136(1), 14-23.
Heuer, L. J., & Bengiamin, M. I. (2001); American nurs-ing students experience shock during a short-terminternational program. Journal of Cultural Diversity,8(4), 128-134.
Leavitt, R. L. (Ed.) (1999). Cross-cultural rehabilitation: Aninternational perspective.Fhiladelphia: Saunders.
Leavitt, R. L. (2002). Developing cultural competence ina multiciiltural world. Part I. PT—Magazine of PhysicalTherapy, 10(12), 36-48.
Leavitt, R. L. (2003). Developing cultural competence in amulticultural world. Part II. PT^Magazine of PhysicalTherapy, 11{1), 56-70.
Leonard, B. J., & Plotnikoff, G. (2000). Awareness: Theheart of cultural competence.AACN Clinical Issues:Advanced Practice in Acute & Critical Care. Complemen-tary and Alternative Therapies, 11(1), 51-59.
Lynch, E. W., & Hanson, M. J. (1992). Developing cross-cultural competence: A guide for working with childrenand their families. Baltimore, MD: Brookes.
Pope-Davis, D. B., Eliason, M. J., & Ottavi, T. M. (1994).Are nursing students multiculturally competent? Anexploratory investigation. Journal of Nursing Educa-tion, 33(1), 3\-33.
Pope-Davis, D. B., Prieto, L. R., Whitaker, C. M., & Pope-Davis, S. A. (1993). Exploring multicultural com-petencies of occupational therapists. The AmericanJournal of Occupational Therapy, 47(9), 838-844.
Purnell, L. D., & Paulanka, B. J. (2003). The PurnellModel for Cultural Competence. In In L. D. Purnell& B. J. Paulanka (Eds.), Transcultural health care: Aculturally competent approach {2"'^ ed.) (pp. 8-39). Phila-delphia: Davis.
Sue, D.W. (2001). Multidimensional facets of culturalcompetence. The Counseling Psychologist, 29(6), 790-821.
Tabi, M. M., & Mukherjee, S. (2003). Nursing in a globalcommunity: A study abroad program. Journal oJTrans-cultural Nursing, 14(2), 134-138.
Utsey, C., & Graham, C. (2001). Investigation of inter-disciplinary learning by physical therapist studentsduring a community-based medical mission trip.Journal of Physical Therapy Education, 15(1), 53-59.
Velde, B. P, & Wittman, P. P (2001). Helping occupationaltherapy students and faculty develop cultural conr\-petence. Occupational Therapy in Health Care, 13(3/4),
23-32.U.S. Census Bureau. (2000). Census 2000 Summary
File 1 (SF 1), 100-Percent Data, Detailed Tables (P3).Retrieved September 5, 2007, from http:/ /fact-finder.census.gov/ servlet/DTTable?_bm=y&-geo_id-01000US&-ds_name=DEC_2000_SFl_U&-_lang=:en&-redoLog=false&-mt_name=DEC_2000_SFl IJ P003&-format-&-CONTEXT=dt
Journal of Cultural Diversity • Vol. 14, No. 3 Fall 2007

Related Documents











