1 Development of a novel educational intervention to promote case-finding in chronic viral hepatitis amongst South Asian migrants- an example of a higher- risk group Claire Kelly MBChB MRCP Department of Clinical and Experimental Medicine, University of Surrey Supervisors: Professor Aftab Ala Professor Simon de Lusignan Dr Martin Whyte

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Development of a novel educational
intervention to promote case-finding in
chronic viral hepatitis amongst South
Asian migrants- an example of a higher-
risk group
Claire Kelly MBChB MRCP
Department of Clinical and Experimental Medicine, University of Surrey
Supervisors:
Professor Aftab Ala
Professor Simon de Lusignan
Dr Martin Whyte
2
Abstract
Introduction
CVH is a leading contributor to the UK’s liver disease epidemic, but is often
undiagnosed. Guidance recommends case-finding in higher-risk groups in line with the
World Health Organisations call for elimination of CVH as a public health problem.
Migrants from high prevalence areas are one such higher-risk group. However, there
remains no consensus on the optimal case-finding strategy.
Methods
Focus groups (FG) were held with South Asian migrants to explore understanding of
CVH. Analysis of FG data identified key themes, which were used to develop a targeted
educational film.
A feasibility study assessing recruitment of South Asian migrants to view this film, to
promote case-finding for CVH, was completed in South-East England. Dried-blood-
spot testing for CVH was offered after the film. Statistical analysis was performed using
Stata IC V15.
Results
Eight FGs representative across age, gender and education levels were held. Five key
themes were identified: lack of awareness, access and attitude to healthcare, concerns
around testing and stigma. These were used to develop a culturally tailored educational
film shown in community settings to promote CVH testing.
Of the n=219 recruited to view the film, 84% (n=) tested for CVH. Fourteen had
exposure to CVH and all active cases were linked to care.
Discussion
This study showed it is feasible to recruit South Asian migrants to view an educational
film on CVH in community settings. The effectiveness of this intervention in

3
promoting testing for CVH (84% tested) has led to plans for a national randomised
controlled trial, demonstrating the importance of targeted case-finding in line with the
WHO plan for CVH elimination. Furthermore, its success means we can recommend
this approach as a model for targeted community-based interventions.
4
Table of Contents
ABSTRACT 2
ABBREVIATIONS 7
LIST OF FIGURES 9
LIST OF TABLES 10
SECTION A: INTRODUCTION 12
CHAPTER 1: CHRONIC VIRAL HEPATITIS AND LIVER DISEASE 13
LIVER DISEASE 14 I. UNITED KINGDOM 14
II. WORLDWIDE 16
CHRONIC VIRAL HEPATITIS 16
I. HEPATITIS B VIRUS (HBV) 19
II. HEPATITIS C VIRUS (HCV) 21
III. TREATMENT OF CVH 22
CHRONIC VIRAL HEPATITIS PREVALENCE 23
I. UK PREVALENCE 24
II. WORLDWIDE PREVALENCE 25
III. HIGH RISK GROUPS FOR CVH 28
LIVER DISEASE IN SURREY 29
CHAPTER 2: MIGRANT HEALTH 35
MIGRANT HEALTH 36 I. INTRODUCTION 36
II. UK MIGRATION PATTERNS 37
III. INTEGRATION OF MIGRANTS 39
IV. POLICY AND MIGRATION 43
V. MIGRANTS AND HEALTH 44
SURREY POPULATION 48
CHAPTER 3: HEALTHCARE POLICY AND CASE FINDING IN CVH 53
INTRODUCTION 54 I. SCREENING IN MEDICINE 54
II. SCREENING IN LIVER DISEASE 56
III. EXISTING LITERATURE ON CASE FINDING IN CVH HIGH RISK GROUPS 58
CHAPTER 4: AIMS, OBJECTIVES AND STUDY DESIGN 66
INTRODUCTION 67
STUDY 1 EXPLORING AWARENESS OF CVH IN THE SOUTH ASIAN MIGRANT 67
POPULATION IN ORDER TO DEVELOP A TAILORED EDUCATIONAL (FILM) INTERVENTION
STUDY 2 A NOVEL EDUCATIONAL INTERVENTION TO IMPROVE THE UPTAKE OF TESTING
FOR CHRONIC VIRAL HEPATITIS IN SOUTH ASIANS (SA): A FEASIBILITY STUDY I. STUDY AIM 69
II. PATIENT RECRUITMENT 69
III. TRIAL PROCESSES 69
IV. REGULATORY APPORVALS 70
CONTRIBUTIONS 71
5
SECTION B: STUDY 1 A NOVEL EDUCATIONAL INTERVENTION TO IMPROVE
THE AWARENESS OF VIRAL HEPATITIS IN THE SOUTH ASIAN COMMUNITY 72
CHAPTER 5: STUDY 1 METHODS 73
STUDY OVERVIEW 74
AIMS 75 STUDY INCLUSION AND EXCLUSION CRITERIA 75 STUDY STRUCTURE 76
I. COHORT 1: FOCUS GROUPS 76
II. UTILISATION OF FOCUS GROUPS AS A METHOD 78
III. COHORT 2: EDUCATIONAL INTERVENTION DEVELOPMENT 80
IV. QUESTIONNAIRE DEVELOPMENT 82
V. VALIDATION 83
DATA ANALYSIS 83
CHAPTER 6: STUDY 1 FOCUS GROUP RESULTS 87
FOCUS GROUP DEMOGRAPHICS 88
FOCUS GROUP DISCUSSION RESULTS 101
I. LACK OF AWARENESS 102
II. TESTING 106
III. ACCESS TO HEALTHCARE 114
IV. ATTITUDE TO HEALTH 117
V. STIGMA 122
ADVICE ON OUR STUDY 127
CHAPTER 7: STUDY 1 FOCUS GROUP DISCUSSION 131
STUDY 1 DISCUSSION 132
DEMOGRAPHIC SPREAD OF FOCUS GROUPS 132
PAST EXPERIENCE OF CVH 133
FG DISCUSSION OUTCOMES 134 THEME 1: LACK OF AWARENESS OF CVH 134
THEME 2: TESTING 135
THEME 3: ACCESS TO HEALTHCARE 137
THEME 4: ATTITUDE TO HEALTH AND HEALTHCARE PROFESSIONALS 138
THEME 5: STIGMA 140
COMMUNITY ADVICE ON OUR PROJECT 140
CHAPTER 8: FILM DEVELOPMENT FROM FG RESULTS 143
INTRODUCTION 144
DEVELOPMENT OF THE STORYLINE 144
KEY DOMAINS TO BE COVERED IN THE FILM 145
IDENTIFICATION OF PARTICIPANTS FOR THE FILM 146
SECTION C: STUDY 2 A NOVEL EDUCATIONAL INTERVENTION TO IMPROVE
THE UPTAKE OF TESTING FOR VIRAL HEPATITIS IN SOUTH ASIANS: A
FEASIBILITY STUDY 148
CHAPTER 9: PHASE 2 METHODS 149
INTRODUCTION 150
TRIAL DESIGN 150
STUDY OBJECTIVES 150 1. STUDY POPULATION 151
6
2. REGULATORY APPROVALS 151
3. RECRUITMENT TO FILM SCREENING 151
4. PRE AND POST FILM QUESTIONNAIRES 154
5. CVH TESTING 154
6. STATISTICAL ANALYSIS 156
CONTRIBUTIONS 156
CHAPTER 10: FEASIBILITY STUDY: RESULTS 157
RESULTS 158
GENERAL CHARACTERISTICS 158 TESTING FOR CVH 158 RESULTS OF QUESTIONNAIRES 159 RESULTS OF CVH TESTING 160
WORD OF MOUTH TESTING UPTAKE 164
CHAPTER 11: FEASIBILITY STUDY: DISCUSSION 166
FILM VIEWING AND TESTING UPTAKE 167
QUESTIONNAIRE DATA 169
RESULTS OF TESTING 171
SUMMARY OF FINDINGS 172
1. UNDERSTANDING OF CVH 172
2. WILLINGNESS TO ENGAGE IN COMMUNITY BASED ACTIVITIES 172
3. CONDUCTING A FEASIBILITY STUDY THAT COULD FORM THE BASIS OF AN RCT 175
COMPARISON WITH EXISTING LITERATURE 177
1. SCREENING UPTAKE 177
2. RECRUITMENT TO CLINICAL TRIALS TO IMPROVE SCREENING UPTAKE 177
3. TYPE OF INTERVENTION 178
4. COMMUNITY BASED TESTING 180
5. PRIMARY CARE RECRUITMENT 181
6. LINKAGE TO CARE 182
7. CONCLUSION 183
STRENGTHS AND LIMITATIONS OF THIS STUDY 183
CHAPTER 12: CONCLUSIONS AND FUTURE WORK 187
PUBLICATIONS FROM THIS THESIS 194
REFERENCES 195
APPENDIX 1: FOCUS GROUP ADVERTISEMENT 210
APPENDIX 2: FOCUS GROUP DEMOGRAPHIC INFORMATION 211
APPENDIX 3: DEMOGRAPHIC INFORMATION FOR STUDY 2 213
APPENDIX 4: QUESTIONNAIRE 215
APPENDIX 5: FULL RESULTS PF PRE AND POST QUESTIONNAIRE 218

7
ABBREVIATIONS
Anti-HBc Hepatitis B core antibody
Anti-HBs Hepatitis B surface antibody
ALT Alanine aminotransferase
AST Aspartate aminotransferase
BAME Black Asian and Minority Ethnic
BBV Blood borne virus
CBI Community based intervention
CCG Clinical Commissioning Group
CDC Centre for Disease Control
CVH Chronic viral hepatitis
DAA Direct acting anti-viral agents
DH Department of Health
EU European Union
GP General Practitioner
HAV Hepatitis A virus
HBIG Hepatitis B immune globulin
HBsAg Hepatitis B surface antigen
HBV Hepatitis B virus
HCC Hepatocellular carcinoma
HCV Hepatitis C virus
HIV Human immunodeficiency virus
IgM Immunoglobulin M
IMD Index of Multiple Deprivation
LHW Lay health worker
LSOA Lower-layer super output area
MDT Multi-disciplinary team
NAFLD Non-alcoholic fatty liver disease
NHS National Health Service
8
NICE National Institute for Health and Care
Excellence
ODN Operational Delivery Network
PWID People who inject drugs
STP Sustainability and Transformation
Partnerships
SVR Sustained virological response
UK United Kingdom
USA United States of America
WHO World Health Organisation

9
LIST OF FIGURES
FIGURE 1: STANDARDIZED UK MORTALITY [1] ...................................................................... 14
FIGURE 2: STANDARDISED LIVER DEATH RATES IN COUNTRIES IN THE EUROPEAN UNION
BEFORE 2004 [1] .............................................................................................................. 15
FIGURE 3: TIMELINE OF VIRAL HEPATITIS DISCOVERY HAV ................................................... 18
FIGURE 4: SUMMARY OF THE COMPLICATIONS OF LIVER DISEASE .......................................... 19
FIGURE 5: WORLDWIDE BURDEN OF CVH ............................................................................... 27
FIGURE 6: MAP OF SURREY ...................................................................................................... 30
FIGURE 7: EMPLOYMENT RATES IN SURREY COMPARED TO ENGLAND [68] .......................... 31
FIGURE 8: HEALTHY LIFE EXPECTANCY AT BIRTH FOR SURREY RESIDENTS COMPARED WITH
ENGLAND AS A WHOLE [68] ............................................................................................ 31
FIGURE 9: LIFE EXPECTANCY AT BIRTH FOR SURREY RESIDENTS COMPARED TO ENGLAND AS
A WHOLE [68] .................................................................................................................. 32 FIGURE 10: AGE OF SURREY RESIDENTS BY GENDER [68] ...................................................... 32
FIGURE 11: BARRIERS TO ELIMINATION OF CVH .................................................................... 34
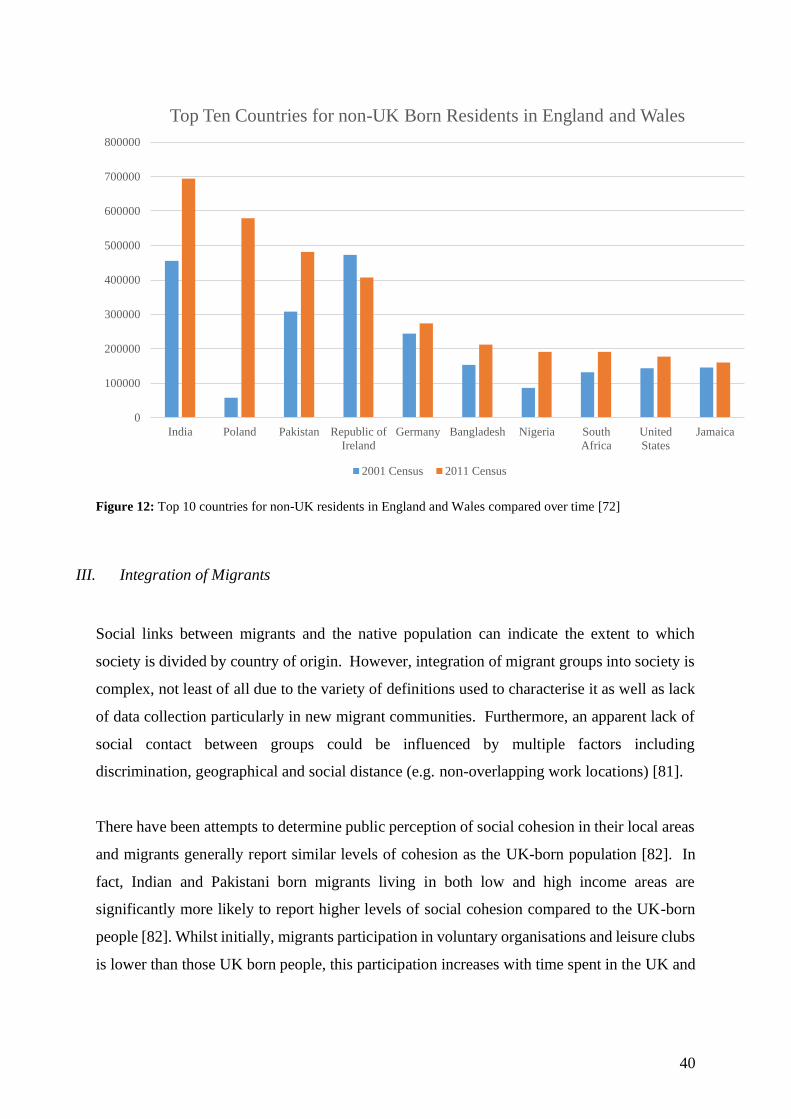
FIGURE 12: TOP 10 COUNTRIES FOR NON-UK RESIDENTS IN ENGLAND AND WALES
COMPARED OVER TIME [72] ............................................................................................. 39
FIGURE 13: THE DAHLGREN AND WHITEHEAD MODEL OF HEALTH DETERMINANTS [122]..... 48
FIGURE 14: NON-UK BORN POPULATION AS A PERCENTAGE OF ALL USUAL RESIDENTS
2011[72] .......................................................................................................................... 50
FIGURE 15: OVERVIEW OF THE STRUCTURE OF PHASE 1 ......................................................... 86
FIGURE 16: FOCUS GROUP PARTICIPANTS BY AGE AND GENDER ............................................. 90
FIGURE 17: NUMBER OF YEARS FOCUS GROUP PARTICIPANTS HAVE SPENT LIVING IN THE UK
......................................................................................................................................... 90
FIGURE 18: COUNTRY OF ORIGIN OF FOCUS GROUP PARTICIPANTS ........................................ 91
FIGURE 19: MAXIMAL EDUCATIONAL ATTAINMENT OF FOCUS GROUP PARTICIPANTS........... 91
FIGURE 20: RELIGIOUS BELIEF OF FOCUS GROUP PARTICIPANTS ............................................ 92
FIGURE 21: MAIN THEMES EMERGING FROM FG DISCUSSIONS.............................................. 101
FIGURE 22: SUMMARY OF THE OUTCOMES OF FG STUDIES ................................................... 130
FIGURE 23: COMMUNITY IDEAS ON REACHING OUR TARGET POPULATION ........................... 143
FIGURE 24: SUMMARY OF THE FILM MAKING PROCESS ......................................................... 144
FIGURE 25: RECRUITMENT BY TYPE OF SITE. THE TOTAL NUMBER RECRUITED TO VIEW THE
EDUCATIONAL FILM, WITH THOSE EXCLUDED AS NOT MEETING STUDY CRITERIA ARE
SHOWN BY TYPE OF VENUE ............................................................................................ 161
FIGURE 26: CHARACTERISTICS OF THOSE TESTING FOR CVH AFTER VIEWING OUR
EDUCATIONAL FILM. THIS DESCRIBES THE PERCENTAGE TESTED BY GENDER, AGE,
COUNTRY OF ORIGIN AND EDUCATIONAL ATTAINMENT. THE 95% CONFIDENCE
INTERVALS ARE SHOWN. ................................................................................................ 163
FIGURE 27: PROPORTION OF PARTICIPANTS TESTING FOR CVH AFTER VIEWING THE FILM BY
SITE, INCLUDING THE 2 SIDED 95% CONFIDENCE INTERVAL ......................................... 163
FIGURE 28: CASES OF EXPOSURE TO CVH (INCLUDING HBV AND HCV) IN THOSE TESTING
HAVING VIEWED THE FILM WITH PERCENTAGE OF THE OVERALL TESTED COHORT
SHOWN ........................................................................................................................... 164

10
LIST OF TABLES
TABLE 1: INTERPRETATION OF SEROLOGICAL MARKERS FOR HBV ........................................ 22
TABLE 2: NICE IDENTIFIED HIGHER-RISK GROUPS FOR HBV INFECTION [3] .......................... 28
TABLE 3: NICE IDENTIFIED HIGHER-RISK GROUPS FOR HCV INFECTION [3] .......................... 29
TABLE 4: ETHNIC GROUPS 2011, SURREY, ENGLAND AND SOUTH EAST [73] ......................... 51
TABLE 5: ETHNIC GROUPS BY AGE 2011 [73] ........................................................................... 52
TABLE 6: FEMALE FG 1 COMMUNITY CENTRE ........................................................................ 93
TABLE 7: FEMALE FG 2 MOSQUE............................................................................................. 93
TABLE 8: FEMALE FG 3 DOMESTIC RESIDENCE ...................................................................... 94
TABLE 9: FEMALE FG 4 COMMUNITY CENTRE ........................................................................ 95
TABLE 10: MALE FG 1 MOSQUE .............................................................................................. 96
TABLE 11: MALE FG 2 MOSQUE .............................................................................................. 97
TABLE 12: MIXED FG 3: LOCAL GP SURGERY ........................................................................ 98
TABLE 13: MALE FG3: LOCAL DOMESTIC RESIDENCE............................................................ 99 TABLE 14: SUMMARY OF DEMOGRAPHIC DETAILS OF FOCUS GROUP MEMBERS ................. 100
TABLE 15: SENSITIVITY AND SPECIFICITY OF THE DBS TEST KIT ......................................... 155
TABLE 16: CHARACTERISTICS OF PARTICIPANTS RECRUITED TO VIEW THE EDUCATIONAL
FILM, SHOWN BY TYPE OF SITE. ..................................................................................... 162
TABLE 17: CHARACTERISTICS OF THOSE ADDITIONAL PARTICIPANTS TESTING FOR CVH
WITHOUT VIEWING THE FILM ......................................................................................... 165
TABLE 18: FEASIBILITY STUDY: SPECIFIC AREAS OF CONCERN AND PROPOSED DETAILS FOR
FUTURE PROPOSED SCALE UP OF RCT ........................................................................... 176
TABLE 19: CHANGE IN PRE AND POST FILM RESPONSES (Q1) ................................................ 218
TABLE 20: CHANGE IN PRE AND POST FILM RESPONSES (Q2) ................................................ 219
TABLE 21: CHANGE IN PRE AND POST FILM RESPONSES (Q3) ................................................ 220
TABLE 22: CHANGE IN PRE AND POST FILM RESPONSES (Q4) ................................................ 221
TABLE 23: CHANGE IN PRE AND POST FILM RESPONSES (Q5) ................................................ 222
TABLE 24: CHANGE IN PRE AND POST FILM RESPONSES (Q6) ................................................ 223
TABLE 25: CHANGE IN PRE AND POST FILM RESPONSES (Q7) ................................................ 223
TABLE 26: CHANGE IN PRE AND POST FILM RESPONSES (Q8) ................................................ 224
TABLE 27: CHANGE IN PRE AND POST FILM RESPONSES (Q9) ................................................ 225
TABLE 28: CHANGE IN PRE AND POST FILM RESPONSES (Q10) .............................................. 226
TABLE 29: CHANGE IN PRE AND POST FILM RESPONSES (Q11) .............................................. 226
TABLE 30: CHANGE IN PRE AND POST FILM RESPONSES (Q12) .............................................. 227
TABLE 31: CHANGE IN PRE AND POST FILM RESPONSES (Q13) .............................................. 228
TABLE 32: CHANGE IN PRE AND POST FILM RESPONSES (Q14) .............................................. 229
TABLE 33: CHANGE IN PRE AND POST FILM RESPONSES (Q15) .............................................. 229
TABLE 34: CHANGE IN PRE AND POST FILM RESPONSES (Q16) .............................................. 230
TABLE 35: CHANGE IN PRE AND POST FILM RESPONSES (Q17A) ............................................ 231 TABLE 36: CHANGE IN PRE AND POST FILM RESPONSES (Q17B) ............................................ 232
TABLE 37: CHANGE IN PRE AND POST FILM RESPONSES (Q17C) ............................................ 232
TABLE 38: CHANGE IN PRE AND POST FILM RESPONSES (Q17D) ............................................ 233
TABLE 39: CHANGE IN PRE AND POST FILM RESPONSES (Q17E) ............................................ 234
TABLE 40: CHANGE IN PRE AND POST FILM RESPONSES (Q17F) ............................................ 234
TABLE 41: CHANGE IN PRE AND POST FILM RESPONSES (Q18) .............................................. 235
TABLE 42: CHANGE IN PRE AND POST FILM RESPONSES (Q19) .............................................. 235
TABLE 43: CHANGE IN PRE AND POST FILM RESPONSES (Q20) .............................................. 236
TABLE 44: CHANGE IN PRE AND POST FILM RESPONSES (Q21) .............................................. 237
TABLE 45: CHANGE IN PRE AND POST FILM RESPONSES (Q22) .............................................. 237
TABLE 46: OPINION ON THE USEFULNESS OF THE EDUCATIONAL FILM (Q23) ....................... 238
TABLE 47: EASE OF UNDERSTANDING OF THE INTERVENTION (Q24) .................................... 238
TABLE 48: RELEVANCE OF FILM (Q25) .................................................................................. 238
11
TABLE 49: CHANGE IN PRE AND POST FILM RESPONSES (Q26A) ............................................ 239
TABLE 50: CHANGE IN PRE AND POST FILM RESPONSES (Q26B) ............................................ 240
TABLE 51: CHANGE IN PRE AND POST FILM RESPONSES (Q26C) ............................................ 241
TABLE 52: CHANGE IN PRE AND POST FILM RESPONSES (Q26D) ............................................ 241
TABLE 53: CHANGE IN PRE AND POST FILM RESPONSES (Q27A) ............................................ 242
TABLE 54: CHANGE IN PRE AND POST FILM RESPONSES (Q27B) ............................................ 242
TABLE 55: CHANGE IN PRE AND POST FILM RESPONSES (Q27C) ............................................ 243
TABLE 56: CHANGE IN PRE AND POST FILM RESPONSES (Q27D) ............................................ 244
TABLE 57: CHANGE IN PRE AND POST FILM RESPONSES (Q27E) ............................................ 245
TABLE 58: CHANGE IN PRE AND POST FILM RESPONSES (Q28A) ............................................ 245
TABLE 59: CHANGE IN PRE AND POST FILM RESPONSES (Q28B) ............................................ 246
TABLE 60: CHANGE IN PRE AND POST FILM RESPONSES (Q28C) ............................................ 247
TABLE 61: CHANGE IN PRE AND POST FILM RESPONSES (Q28D) ............................................ 247
12
SECTION A: INTRODUCTION

13
CHAPTER 1: CHRONIC VIRAL HEPATITIS AND LIVER DISEASE
14
LIVER DISEASE
I. United Kingdom (UK)
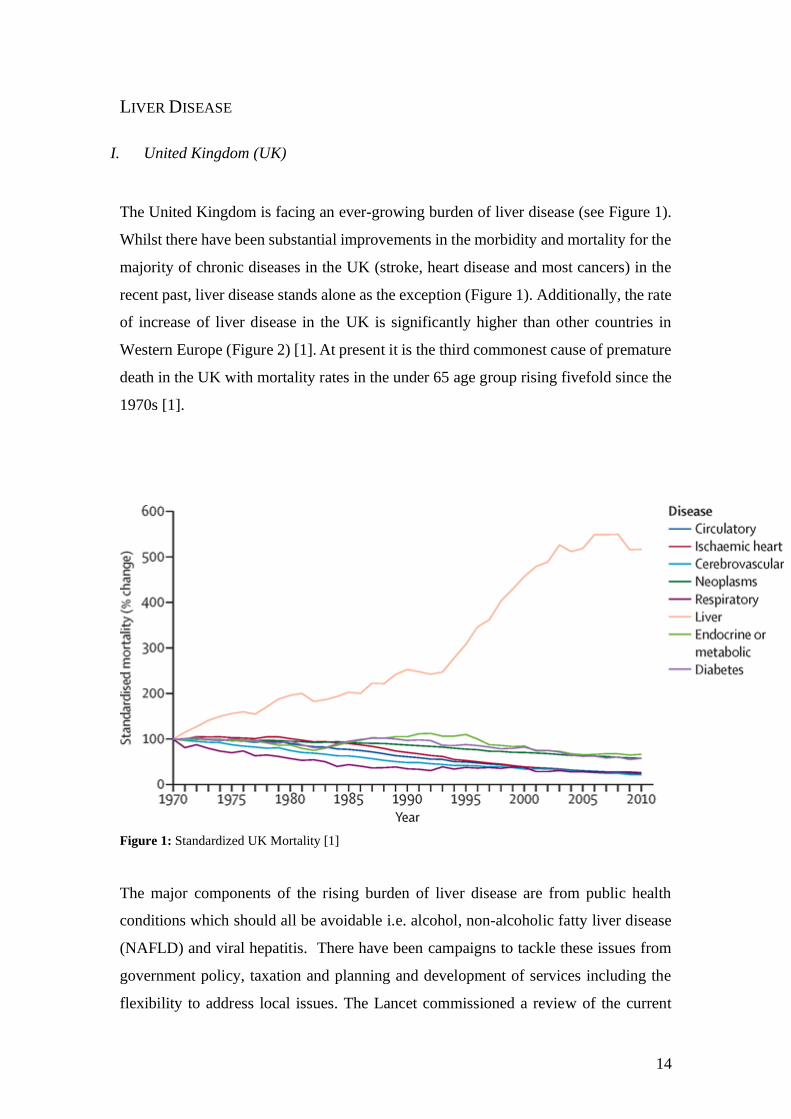
The United Kingdom is facing an ever-growing burden of liver disease (see Figure 1).
Whilst there have been substantial improvements in the morbidity and mortality for the
majority of chronic diseases in the UK (stroke, heart disease and most cancers) in the
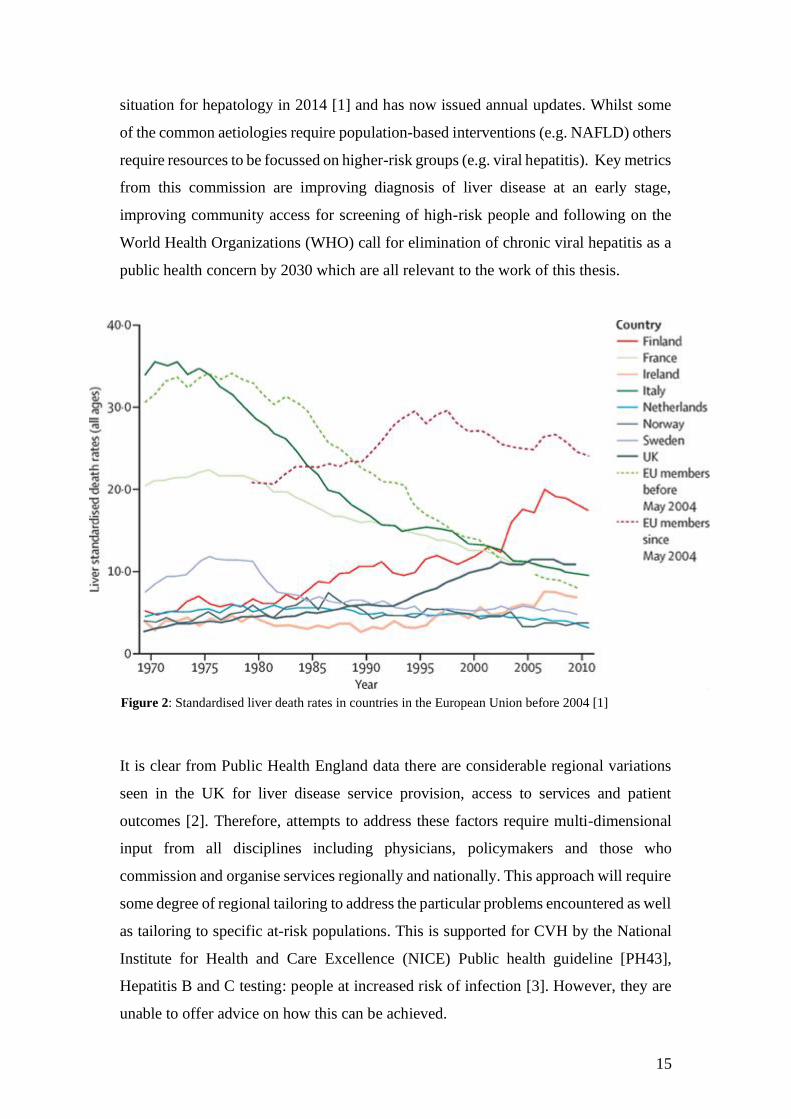
recent past, liver disease stands alone as the exception (Figure 1). Additionally, the rate
of increase of liver disease in the UK is significantly higher than other countries in
Western Europe (Figure 2) [1]. At present it is the third commonest cause of premature
death in the UK with mortality rates in the under 65 age group rising fivefold since the
1970s [1].
Figure 1: Standardized UK Mortality [1]
The major components of the rising burden of liver disease are from public health
conditions which should all be avoidable i.e. alcohol, non-alcoholic fatty liver disease
(NAFLD) and viral hepatitis. There have been campaigns to tackle these issues from
government policy, taxation and planning and development of services including the
flexibility to address local issues. The Lancet commissioned a review of the current
15
situation for hepatology in 2014 [1] and has now issued annual updates. Whilst some
of the common aetiologies require population-based interventions (e.g. NAFLD) others
require resources to be focussed on higher-risk groups (e.g. viral hepatitis). Key metrics
from this commission are improving diagnosis of liver disease at an early stage,
improving community access for screening of high-risk people and following on the
World Health Organizations (WHO) call for elimination of chronic viral hepatitis as a
public health concern by 2030 which are all relevant to the work of this thesis.
It is clear from Public Health England data there are considerable regional variations
seen in the UK for liver disease service provision, access to services and patient
outcomes [2]. Therefore, attempts to address these factors require multi-dimensional
input from all disciplines including physicians, policymakers and those who
commission and organise services regionally and nationally. This approach will require
some degree of regional tailoring to address the particular problems encountered as well
as tailoring to specific at-risk populations. This is supported for CVH by the National
Institute for Health and Care Excellence (NICE) Public health guideline [PH43],
Hepatitis B and C testing: people at increased risk of infection [3]. However, they are
unable to offer advice on how this can be achieved.
Figure 2: Standardised liver death rates in countries in the European Union before 2004 [1]
16
II. Worldwide
Liver disease is costly in terms of morbidity, mortality (particularly premature
mortality), hospital visits, and premature loss of productivity [4]. Globally, liver
cirrhosis was estimated to be responsible for over one million deaths in 2010, which
equates to approximately 2% of all deaths worldwide, with an estimated further one
million deaths due to liver cancer and acute hepatitis [5]. This is despite the clear issues
with documentation, identification and labelling of liver disease in some parts of the
world.
In 2013, 29 million people in Europe (European Union region) [6] and more than 30
million Americans had liver disease [7], with an estimated 170,000 deaths in Europe as
a result of liver cirrhosis [4].
Hepatocellular carcinoma (HCC) is a recognised complication of cirrhosis, and is
actively screened for, which is responsible for 70-90% of cases of primary liver cancer
[8]. Worldwide, liver cancer is the sixth most common cancer and the second most
common cause of cancer death, with only lung cancer a more common cause of cancer-
related mortality [9]. In 2012 there were 63,500 new cases of liver cancer diagnosed in
Europe and 745,000 worldwide deaths [10].
CHRONIC VIRAL HEPATITIS (CVH)
A large contributor to the burden of liver disease that we face is chronic viral hepatitis
(CVH) i.e. hepatitis B (HBV) and C (HCV) which are the leading causes of liver disease
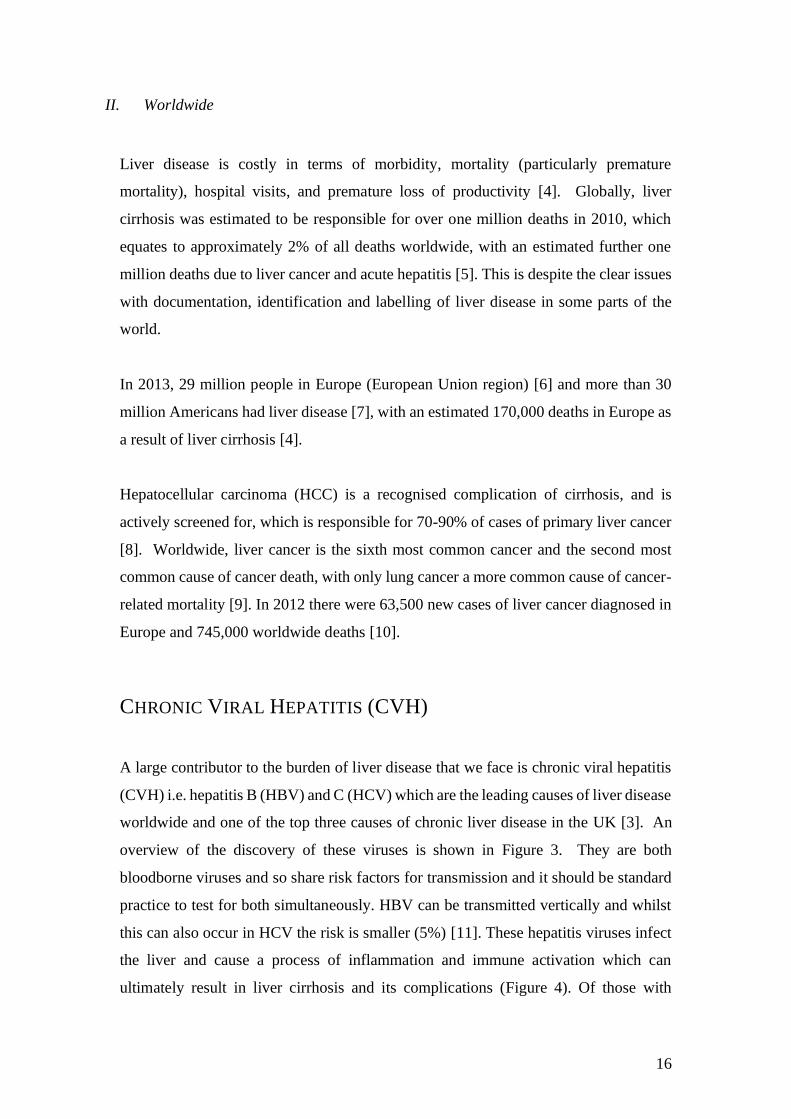
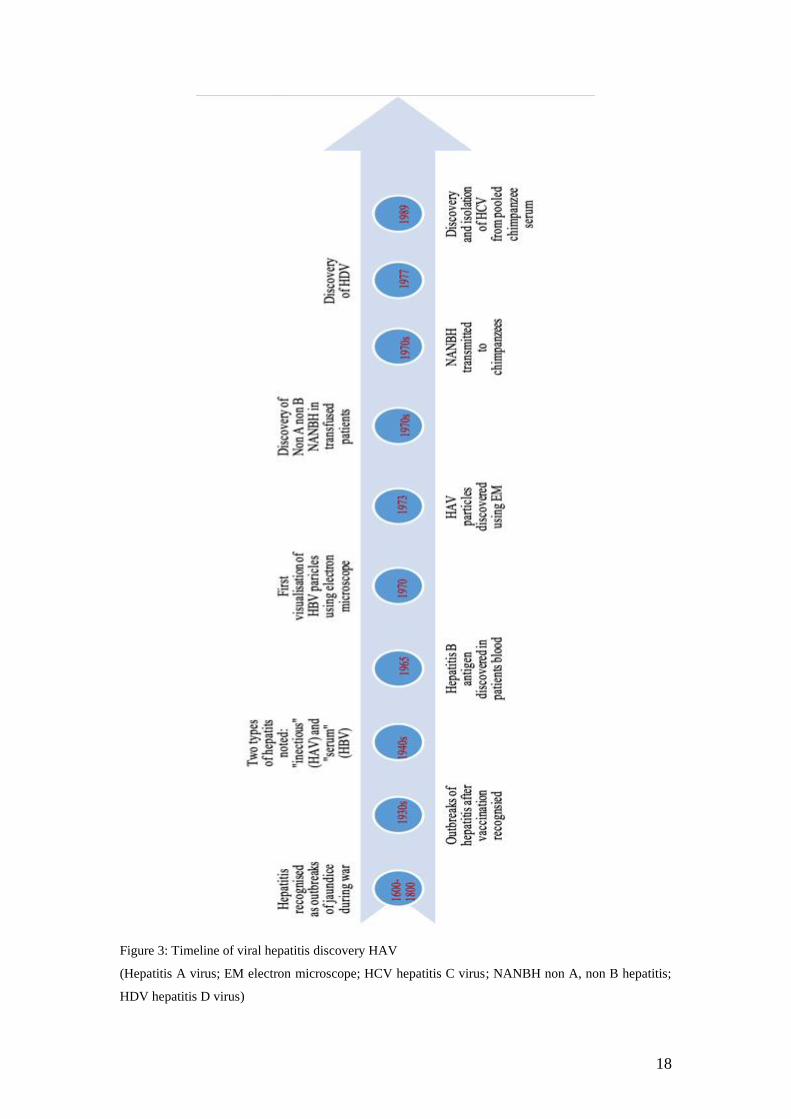
worldwide and one of the top three causes of chronic liver disease in the UK [3]. An
overview of the discovery of these viruses is shown in Figure 3. They are both
bloodborne viruses and so share risk factors for transmission and it should be standard
practice to test for both simultaneously. HBV can be transmitted vertically and whilst
this can also occur in HCV the risk is smaller (5%) [11]. These hepatitis viruses infect
the liver and cause a process of inflammation and immune activation which can
ultimately result in liver cirrhosis and its complications (Figure 4). Of those with

17
chronic viral hepatitis, 30% will have cirrhosis by the third decade after infection with
the resultant risks of hepatocellular carcinoma and recurrent admissions to hospital with
decompensation.
Not all patients infected with HBV and HCV will develop chronic infection, and there
is variation in this chronicity based on the age at acquisition [12]. Importantly though,
both acute and chronic infection may cause few symptoms, and infection therefore goes
unrecognised by patient and clinician alike until end-stage complications develop (70%
of adults and 90% of children may not develop symptoms of acute hepatitis B infection)
[13]. Testing is therefore the only way to identify infection, with effective and accurate
testing strategies available.
Initial infection and early, reversible stages of the disease are often asymptomatic or
non-specifically symptomatic and so go undiagnosed. It has been estimated that 75%
of chronic infections remain undiagnosed [1]. In the UK the higher-risk groups for CVH
infection are people who inject drugs (PWID) including performance enhancing drugs,
incarcerated individuals and migrants from countries with an intermediate or high
prevalence (>2%) of viral hepatitis. In the UK, 95% of new chronic HBV occurs in the
migrant population, having been acquired perinatally in the main [3]. There is evidence
to support the transmission of HCV by community barbers and contaminated blood
products in the developing world [14]. Those who acquire viral hepatitis as children are
more likely to develop chronic infection. This then means the potential for cirrhosis and
its complications in young adult life with resulting morbidity and mortality.
18
Figure 3: Timeline of viral hepatitis discovery HAV
(Hepatitis A virus; EM electron microscope; HCV hepatitis C virus; NANBH non A, non B hepatitis;
HDV hepatitis D virus)

19
Figure 4: Summary of the complications of liver disease
I. Hepatitis B Virus (HBV)
HBV is not directly cytopathic, with hepatic injury the consequence of immune system
activation and its attempt to clear the infection through a process of hepatic
inflammation (hepatitis), necrosis and fibrosis. This continual cycle of cell injury,
necrosis and attempted regeneration leads to cirrhosis (2-6% annually) [15, 16] and
potentially malignancy, with 0.5% developing HCC [17].
HBV is more infective than HIV, with vertical transmission rates that may be as high
as 90%, coupled with perinatal or childhood acquisition that are the main drivers of the
endemic nature of HBV seen globally. HBV may be also transmitted sexually, as well
as potential risks with the sharing of razors or toothbrushes in some circumstances [13].
Not all affected individuals become chronic carriers, with age a particularly important
risk-factor for HBV, with perinatal exposure leading to chronic infection in
approximately 80-90% of cases, and adult exposure that may lead to chronicity in
20
around 5% of cases [12]. Development of liver cirrhosis occurs more frequently in
patients who are older, who consume excess alcohol, those with pre-core mutation,
advanced disease at presentation and those with co-existing liver disease [15]. Around
6% of cirrhotic patients undergo decompensation each year [17]. Patients with chronic
HBV are many times more likely to develop HCC than people who resolve the acute
infection. HCC generally arises 25-30 years after the acute infection [18]. It has been
suggested that HCC develops when hepatocytes are damaged by the immune response
leading to regeneration attempts thus increasing the risk of carcinogenic mutations [18].
HBV is the second most frequent global carcinogen causing 50% of HCC worldwide
[15].
The annual rate of delayed clearance of Hepatitis B surface antigen (HBsAg) is
estimated as 0.5-2% in Western patients but lower (0.1-0.8%) in Asians [19, 20].
HBsAg loss with or without seroconversion may occur spontaneously in 1–3% of cases
per year [21], usually where serum HBsAg levels are low (<1,000 IU/ml) [22]. A
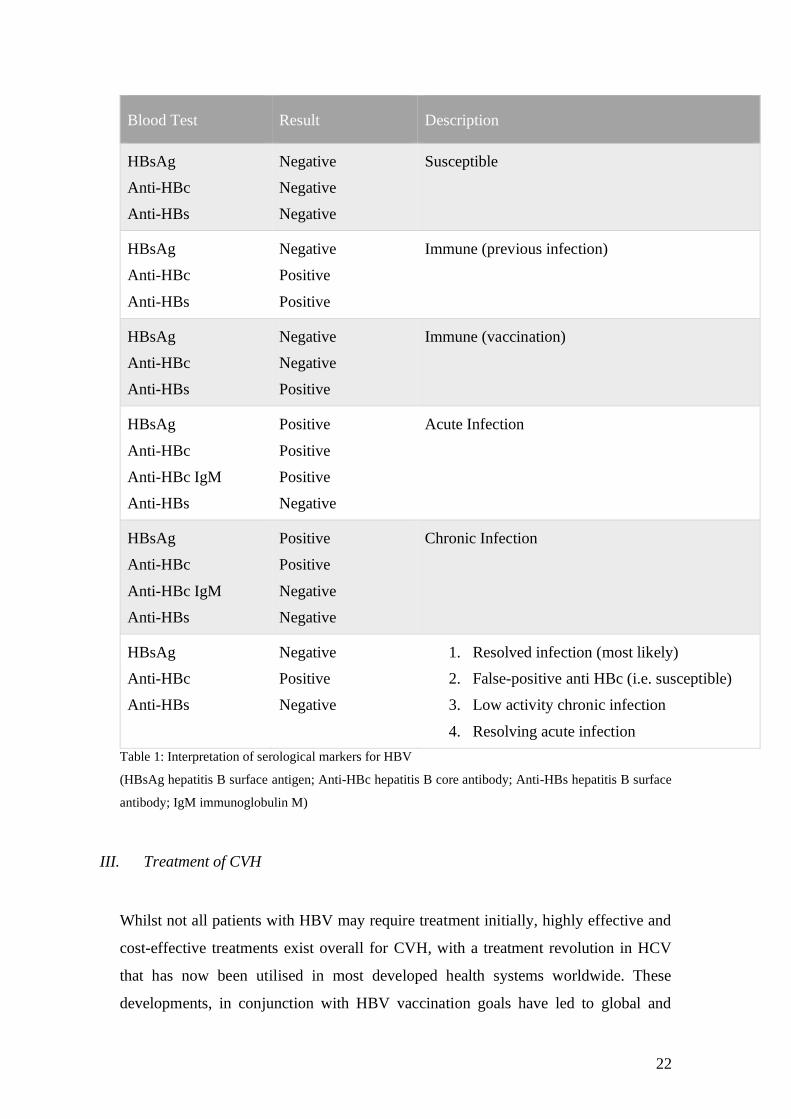
summary of the blood tests for HBV and their interpretation is shown in Table 1.
Hepatitis B vaccination has significantly reduced the risk of transmission worldwide.
The predominant mode of HBV transmission varies across geographical areas that
seems to be related to the background prevalence. In high-prevalence areas vertical
transmission is predominant [23], with horizontal transmission (especially in
childhood) in intermediate-prevalence areas, while unprotected sexual intercourse and
injection drug use predominant in low-prevalence areas.
Vertical transmission rates from HBsAg-positive mothers can be as high as 90% in
babies who do not receive hepatitis B immune globulin (HBIG) and vaccination at birth
[24]. However, prompt immunization with HBIG and vaccination has substantially
reduced the rate of transmission. This does not completely eliminate the risk, however.
There is a particularly high risk of transmission from mothers who are HBeAg positive
and who have a high viral load. By treating these mothers with anti-viral therapy, the
risk of transmission can be reduced.
Whilst risk of acquisition of HBV (and HCV) from blood product transfusion was a
major problem, transmission was significantly reduced after the introduction of

21
serologic screening of donors for HBsAg [25] and further reduced by addition of anti-
HBc screening. The World Health Organisation recommends screening with both.
II. Hepatitis C Virus (HCV)
It has been reported that 50-85% of patients infected with HCV become chronically
infected, depending on the population studied and the source of infection [26]. Of those
who are able to spontaneously clear HCV, this usually occurs within 12 weeks of
seroconversion, although longer periods have been described [26]. The mechanism
responsible for the high levels of chronic infection is unclear but both viral and host
factors are likely to contribute.
HCV is transmitted principally by exposure to contaminated blood or body fluids, with
injecting drug use thought to account for up to 90% of cases in the UK [27]. Vertical
transmission is less well defined, but likely to be an important factor globally, with
perinatal transmission risks that may be towards 6% [28], and with household
transmission that is difficult to quantify. The likelihood of chronicity varies with age
with younger people less likely than older people to develop chronic infection as is the
case with HBV. However, 75-80% of exposed individuals develop chronic HCV
infection. The risk of developing cirrhosis in chronic HCV infection is reported to be
around 20% at 20 years, rising to 36-45% at 30 years [29].
22
Blood Test Result Description
HBsAg
Anti-HBc
Anti-HBs
Negative
Negative
Negative
Susceptible
HBsAg
Anti-HBc
Anti-HBs
Negative
Positive
Positive
Immune (previous infection)
HBsAg
Anti-HBc
Anti-HBs
Negative
Negative
Positive
Immune (vaccination)
HBsAg
Anti-HBc
Anti-HBc IgM
Anti-HBs
Positive
Positive
Positive
Negative
Acute Infection
HBsAg
Anti-HBc
Anti-HBc IgM
Anti-HBs
Positive
Positive
Negative
Negative
Chronic Infection
HBsAg
Anti-HBc
Anti-HBs
Negative
Positive
Negative
1. Resolved infection (most likely)
2. False-positive anti HBc (i.e. susceptible)
3. Low activity chronic infection
4. Resolving acute infection
Table 1: Interpretation of serological markers for HBV
(HBsAg hepatitis B surface antigen; Anti-HBc hepatitis B core antibody; Anti-HBs hepatitis B surface
antibody; IgM immunoglobulin M)
III. Treatment of CVH
Whilst not all patients with HBV may require treatment initially, highly effective and
cost-effective treatments exist overall for CVH, with a treatment revolution in HCV
that has now been utilised in most developed health systems worldwide. These
developments, in conjunction with HBV vaccination goals have led to global and
23
national initiatives calling for CVH to be eradicated as a public health threat by 2030
(with a 90% reduction in new chronic infections, and 65% reduction in mortality) [1,
30]. Treatment is highly efficacious if delivered at the right time, to reduce or prevent
the development of cirrhosis or primary liver cancer with significant individual and
health system savings.
The introduction of direct acting anti-viral agents (DAAs) for hepatitis C (HCV) in
2011 represented a major step-forward in both the sustained virological response rates
(SVR) (>95%) and side-effects of therapy when compared to previous treatment
regimen of interferon and ribavirin. NHS England has commissioned HCV treatment
by networks called Operational Delivery Network (ODN) since July 2015. Treatment
can only be given through MDT working and in accordance with the confines of the
run-rate and the rate card which describes first-line therapy for each genotype and by
disease severity. These networks have increasingly adapted to have a case-finding role
as the list of patients awaiting treatment shortens.
CVH PREVALENCE
The prevalence of HBV and HCV is low in the background UK population but is
disproportionately higher in certain at-risk groups linked to geographic variation,
iatrogenic exposure and risk activity. The health impacts of HBV and HCV can be
severe, with significantly increased morbidity and mortality in those individuals who
progress to end stage liver disease without effective treatment.
There is marked geographic variation in HBV and HCV worldwide, particularly for
HBV, which is endemic in certain parts of the world. Prevalence data is lacking in many
countries, particularly in those with deprived health infrastructure systems, but overall
across Europe reported rates of HBV and HCV infection are between 2-6 times higher
in migrant groups than that seen in the existing population [31]. For both HBV and
HCV, there is uncertainty about the exact number of cases that have been diagnosed or
treated in the UK [32].
24
I. UK Prevalence
The most widely used estimates of chronic HBV infection in the UK arise from
historical Department of Health (DH) data in 2002, with prevalence rates of 0.3% and
an estimated 180,000 affected but there is variation in this estimate with some experts
placing the figure closer to 500,000 [33]. Importantly, up to 95% of new chronic HBV
cases in the UK occur in migrant individuals, with most individuals who would have
acquired Hepatitis B in early childhood in the country of birth [3]. Further information
from blood donor testing shows that of the 91 positively identified HBV cases, 60% of
patients were born in Africa or Asia [34].
Chronic HBV predominates in the positive cases identified, and given the
asymptomatic nature of HBV, there is likely to be a large pool of undiagnosed HBV
infections that would not be reached without a targeted testing approach [35]. Unlike
acute HBV, chronic HBV is not notifiable, so calculation of prevalence in the UK is
challenging.
Of the estimated 7,700 UK new chronic hepatitis B cases per year, 96% are infected
vertically or through medical treatment overseas who are UK immigrants (South Asia,
Eastern Europe and Africa). As the majority will be immunotolerant they will be
infectious but not symptomatic so will not necessarily present for health care for some
years.
Over nearly two decades there has been a steady increase in the number of laboratory
confirmed reports of HCV in England with more than five-fold increase between 1996
and 2013 [36]. Previous estimates suggest that around 214,000 individuals are
chronically infected with HCV in the UK, although it is challenging to determine
precise figures [36]. Hospital admissions rose from 608 in 1998 to 2390 in 2012 whilst
deaths rose from 98 in 1996 to 428 in 2012. Annual deaths from HCV in the UK
quadrupled since 1996 [1]. There is a disproportionate rise in morbidity and mortality
in ethnic minorities [37]. The rates of infection amongst recent immigrants is higher
than the background UK population and in Asians reaches 2%. Modelling shows that
provided the prevalence of chronic viral hepatitis in migrants from minority groups was
at least 2% then it was estimated that it would be cost effective to find, treat and test
25
within such communities [3]. Injecting drug use is the biggest risk factor for chronic
HCV in the UK, but HCV is disproportionally higher in migrant groups, particularly in
those from South Asian origin (Indian, Pakistani or Bangladeshi origin) and Eastern
Europe compared to the non-injecting white British population. Data from the sentinel
surveillance programme shows a HCV prevalence rate of 2.7% in Asian/Asian-British
individuals, and although there is no categorisation for those of Eastern European
origin, name recognition software has shown prevalence rates as high as 5.4% in this
groups of patients [27].
Importantly, it is estimated that between 50-75% of patients with HCV are unaware of
their infective status. The majority of chronic HCV therefore exists undetected in the
community, with projected morbidity and mortality that is expected to rise in this
undiagnosed population [1, 27].
II. Worldwide Prevalence
CVH has a global distribution with HBV endemic in some parts of the world [30, 38].
There is marked geographic variation in the prevalence of CVH, with a
disproportionate burden of disease that is seen in many parts of the world (see Figure
5) [31]. Globally, only around 9% of all HBV patients, and 22% of HCV patients are
estimated to have been diagnosed and aware of their disease state, and even by 2015,
only around 8% of these HBV patients and 7.4% of HCV patients had received or
commenced treatment [39].
Hepatitis C is found worldwide. The most affected regions are Central and East Asia
and North Africa [40]. Egypt has the highest prevalence of Hepatitis C in the world
and an estimated 40,000 people a year die as a consequence of the virus. At least one
in ten people aged 15-59 are infected [41]. Approximately 500,000 people die each year
from HCV related liver diseases [40]. In the WHO European Union (EU) region, it is
estimated that 15 million people have Hepatitis C, resulting in approximately 86,000
deaths every year [42], with four million Americans infected [7].
Most European countries report chronic HCV prevalence rates between 0.5 - 2%,
although Italy has rates as high as 3.9%. Egypt has the highest reported chronic HCV

26
rates with rates quoted between 20-30% [12]. One of the largest HCV populations is
thought to be in East Asia and the Indian subcontinent, with an estimated 100 million
HCV positive individuals in this region, and with prevalence rates of 4.9% reported in
Pakistan [43].
It is estimated that approximately two billion people worldwide have evidence of past
or present infection with HBV, with around 350 million people having chronic
Hepatitis B [44]. In the World Health Organization (WHO) EU region, it is estimated
that 13.3 million people have chronic Hepatitis B [42] with over one million Americans
infected [7]. Hepatitis B results in an estimated 36,000 deaths every year in Europe
[45] with roughly 600,000 deaths worldwide [46, 47]. The prevalence of chronic HBV
ranges from <2% in low-prevalence areas (e.g. United States, Canada, Western Europe)
to 2-7% in intermediate-prevalence areas (e.g. Mediterranean countries, Japan, Central
Asia, Middle East, and parts of South America) to ≥8% in high-prevalence areas (e.g.
Western Africa, South Sudan) most of these infections arise through vertical
transmission [15] with almost half (45%) of the global pandemic residing in these
countries [17, 46-48]. The wide range in the prevalence of patients with chronic HBV
in different parts of the world is largely related to differences in the age at infection,
which is inversely related to the risk of chronicity. The rate of progression from acute
to chronic HBV infection is approximately 90% for perinatally acquired infection [24],
20-50% for infections between the age of one and five years [49, 50], and less than 5%
for adult-acquired infection [49]. In areas of low prevalence, many of the patients who
have chronic HBV were born in areas where the prevalence is higher [51-56].
In 2013, chronic viral hepatitis was the seventh leading cause of death worldwide [57].
Most mortality was attributable to hepatocellular carcinoma and cirrhosis. Globally, the
total number of deaths due to HBV in 2013 was estimated to be 686,000 [58]. In the
United States, the rate of HBV-related mortality from 2009 to 2013 was
0.5 deaths/100,000 population [59]. In China, the age-standardized death rate for HBV-
related liver cancer and cirrhosis in 2013 was 10.95 and 4.91 per 100,000 people,
respectively [60].
The global death toll seen due to CVH is rising, and is higher than that reported with
HIV, and comparable to that seen for tuberculosis; with CVH the only one of these
conditions with a mortality rate that continues to rise [30, 38].

27
Figure 5: Worldwide burden of CVH
The World Health Organisation released a call for the elimination of chronic viral
hepatitis as a public health threat by 2030 in line with the Agenda for Sustainable
Development [61]. This reflects the fact that CVH is a neglected cause of worldwide
mortality that is increasing, and greater than global deaths from malaria and
tuberculosis [62]. Part of this call is to improve the current rate of diagnosis from a
baseline in 2015 of <5%, to 30% by 2020 and 90% by 2030 [63]. There are, however,

28
barriers to elimination as shown in Figure 11 and it is patient awareness and access to
testing that this thesis aims to address.
III. High Risk Groups for CVH
NICE guidelines recognised higher-risk groups for both HBV and HCV infection in the
UK Whilst most risk factors are the same for both viruses, there are some differences.
There are also differences in other Western countries such as those provided by the
centre for disease control (CDC) in America [64].
HBV Higher-Risk Groups
People born or brought up in a country with an intermediate or high prevalence (2%
or greater) of chronic HBV. This includes all countries in:
- Africa,
- Asia,
- the Caribbean,
- Central and South America,
- Eastern and Southern Europe,
- the Middle East and
- the Pacific islands.
Babies born to mothers infected with hepatitis B.
People who have ever injected drugs.
Men who have sex with men.
Anyone who has had unprotected sex, particularly:
- People who have had multiple sexual partners
- People reporting unprotected sexual contact in areas of intermediate and
high prevalence
- People presenting at sexual health and genitourinary medicine clinics
- People diagnosed with a sexually transmitted disease
- Commercial sex workers
Looked-after children and young people, including those living in care homes
Prisoners, including young offenders
Immigration detainees
Close contacts of someone known to be chronically infected with HBV
Table 2: NICE identified higher-risk groups for HBV infection [3]

29
HCV Higher-Risk Groups
People who have ever injected drugs.
People who received a blood transfusion before 1991 or blood products before 1986
when screening of donors for HCV infection, or heat treatment for inactivation of
viruses were introduced
People born or brought up in a country with an intermediate or high prevalence (2%
or greater) of chronic HCV. This includes all countries in:
- Africa,
- Asia,
- the Caribbean,
- Central and South America,
- Eastern and Southern Europe,
- the Middle East and
- the Pacific islands.
Babies born to mothers infected with HCV.
Prisoners, including young offenders
Looked-after children and young people, including those living in care homes
People living in hostels for the homeless or sleeping on the streets.
HIV positive men who have sex with men.
Close contacts of someone known to be chronically infected with HCV
Table 3: NICE identified higher-risk groups for HCV infection [3]
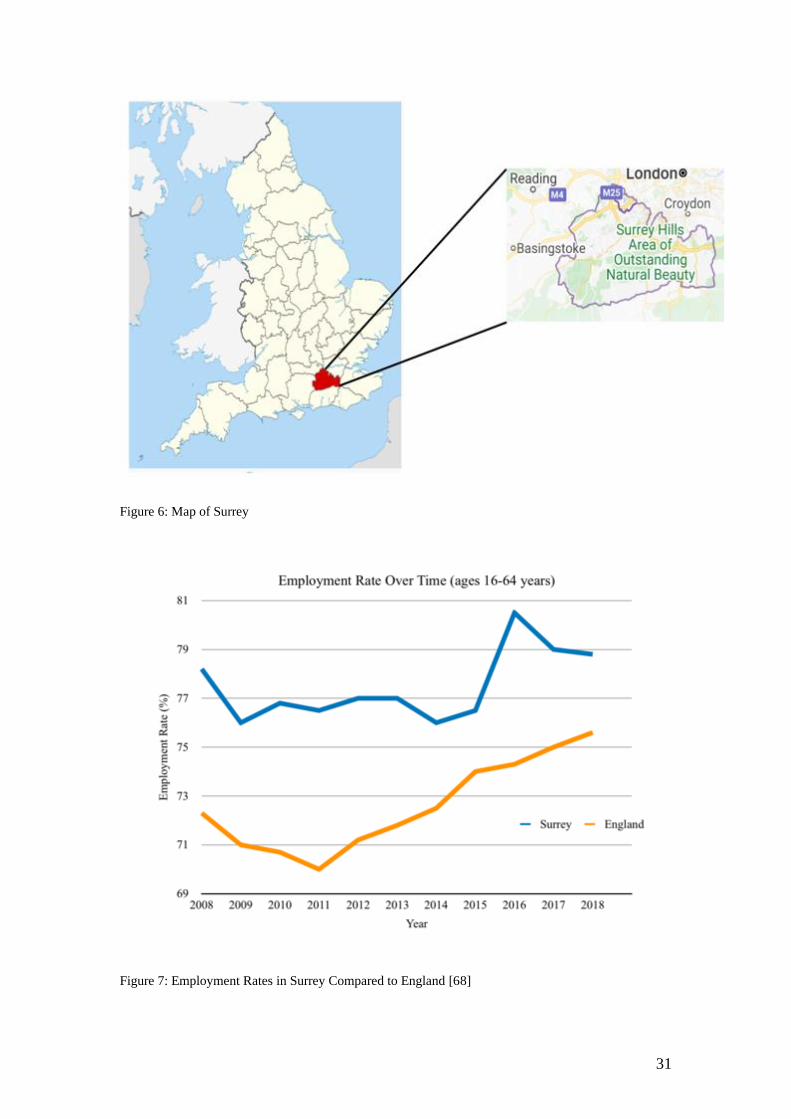
LIVER DISEASE IN SURREY
Surrey is a county in the South East of England, with a population of around 1.2 million
people (see Figure 6) [65]. It has a relatively older population (see Figure 10). It is an
affluent area, but with pockets of relative deprivation. In the UK the Department for
Communities and Local Government provide deprivation data by region [66]. The
overall index of multiple deprivation (IMD) is calculated based on multiple domains
(Income Deprivation, Employment Deprivation, Education, Skills and Training
Deprivation, Health Deprivation and Disability, Crime, Barriers to Housing and
Services and Living Environment Deprivation). Surrey is ranked 150 (1=most
deprived, 152=least deprived).
30
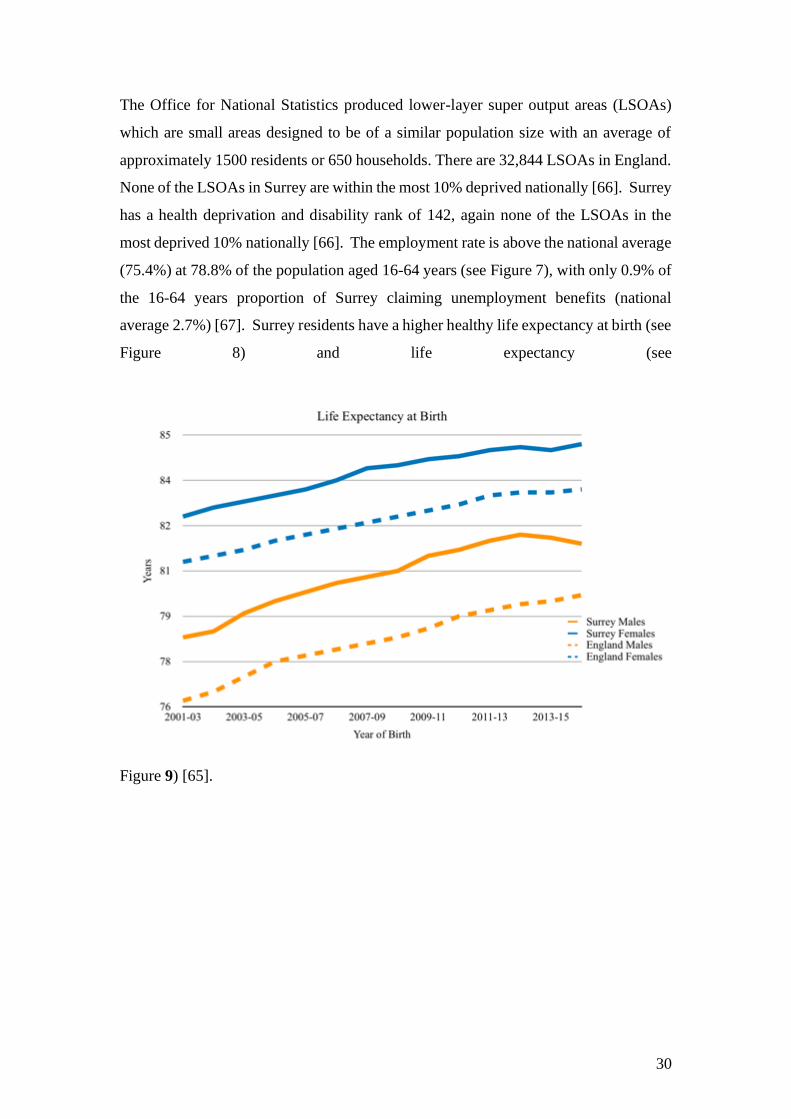
The Office for National Statistics produced lower-layer super output areas (LSOAs)
which are small areas designed to be of a similar population size with an average of
approximately 1500 residents or 650 households. There are 32,844 LSOAs in England.
None of the LSOAs in Surrey are within the most 10% deprived nationally [66]. Surrey
has a health deprivation and disability rank of 142, again none of the LSOAs in the
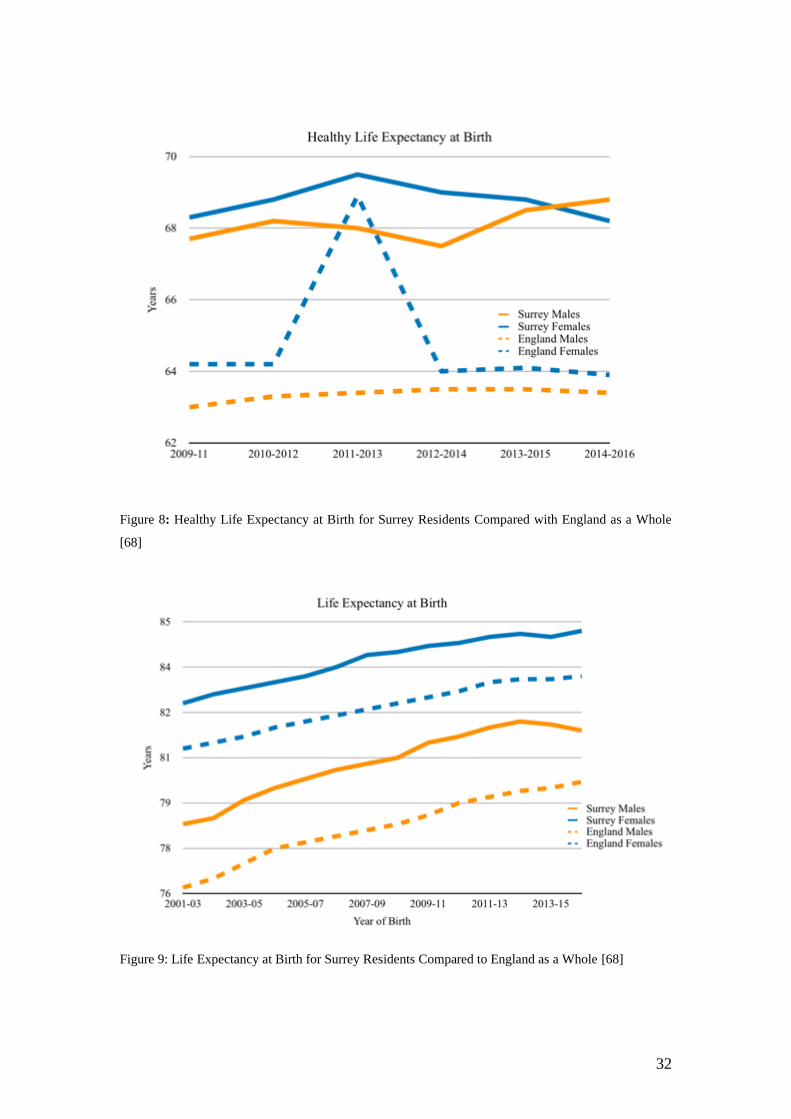
most deprived 10% nationally [66]. The employment rate is above the national average
(75.4%) at 78.8% of the population aged 16-64 years (see Figure 7), with only 0.9% of
the 16-64 years proportion of Surrey claiming unemployment benefits (national
average 2.7%) [67]. Surrey residents have a higher healthy life expectancy at birth (see
Figure 8) and life expectancy (see
Figure 9) [65].
31
Figure 6: Map of Surrey
Figure 7: Employment Rates in Surrey Compared to England [68]
32
Figure 8: Healthy Life Expectancy at Birth for Surrey Residents Compared with England as a Whole
[68]
Figure 9: Life Expectancy at Birth for Surrey Residents Compared to England as a Whole [68]

33
Figure 10: Age of Surrey Residents by Gender [68]
Public Health England have issued a document that describes the variation in risk
factors and healthcare across different levels from local authority, Clinical
Commissioning Groups (CCGs), and local Government offices [2]. This reveals that
the rate of years of life lost in people aged 1-64 years from chronic liver disease
including cirrhosis is not significantly different in Surrey than the rest of England [2].
In all Surrey CCG areas, there is significantly lower rates of admission to hospital (at
least once) for cirrhosis in people aged 18 years and over compared to England as a
whole.
Whilst not able to provide details for Surrey specifically, the South East area has
significantly lower laboratory confirmed HCV tests and new diagnoses of HBV in
pregnancy than England as a whole. Acute HBV rates were not significantly different
in the South East as compared to the whole of England [2].
The rate of hospital admissions for HCV related end stage liver disease or HCC is
significantly lower in Surrey Heartlands but significantly higher in East Surrey and
Sussex than the rate for England [2]. The mortality rate in all Surrey was not

34
significantly different from England rates [2]. The same metrics for HBV were also
described and neither hospital admissions nor mortality were significantly different
from England rates.
For markers of advanced chronic liver disease, regardless of aetiology, Surrey Downs
had a significantly higher percentage of oesophageal varices admissions as emergencies
(North West Surrey no significant difference, East Surrey no data) and North West
Surrey and Surrey Downs had significantly higher percentage of admissions for
paracentesis done as an emergency (Guildford and Waverley significantly lower, East
Surrey no significant difference) [2].

35
Figure 11: Barriers to elimination of CVH
Barriers to elimination
Poor test access & uptake
Inadequate funding for
public health campaigns
Stigma of diagnosis
Lack of awareness & knowledge in
healthcare professionals
Lack of patient
awareness
Lack of treatment
access
Long wait time for access to treatment
Harm reduction
availability
36
CHAPTER 2: MIGRANT HEALTH

37
MIGRANT HEALTH
I. Introduction
There is no definition in law as to what constitutes a migrant. The variety of definitions used
in healthcare policy and research include foreign nationals, people with foreign citizenship,
asylum seekers and those moving temporarily or permanently. Whilst the number of people
seeking asylum are a small proportion of the overall entrants to the UK, they attract a
disproportionate amount of public, media and policy attention. In the mass media and in some
areas of research the terms foreigner, migrant and immigrant are used interchangeably.
In the UK, the Office for National Statistics (ONS) uses the United Nations definition of a
long-term international migrant i.e. “A person who moves to a country other than that of his or
her usual residence for a period of at least a year so that the country of destination effectively
becomes his or her new country of usual residence”. However, this definition, like others, has
limitations in estimating net migration and has implications for policy as discussed below.
This variation in terminology as to what or who a migrant is can be important in public debate
where migrants are equated with minority groups, both ethnic and religious, as well as asylum
seekers and these terms can be used interchangeably particularly by the mass media [69]. It
also has an effect on migration data and analysis which in turn informs public debate and
policy. Those described as migrants in the UK can include people who are British citizens or
who have the right to work and access public services in this country and hence are not subject
to immigration control, for example EU citizens have not been limited by immigration law
(prior to Brexit).
Definitions also affect data, including measures of both the number of migrants in the country
at any given time and the flow of people moving into or out of the country. Current official
government estimates include several groups that would be excluded under other definitions.
In this thesis, I use the term ‘migrant’ to refer to those people born abroad regardless of whether
they have become UK citizens.

38
II. UK Migration Patterns
The UK has a history of migration from its former colonies, with many individuals who started
to arrive in the UK from the 1950’s to 1960’s from the Caribbean and South Asia. Immigration
to the UK has doubled since the 1990’s, and England and Wales have a higher proportion of
foreign-born residents in comparison to similar sized European countries [70]. In the UK, the
annual population survey showed the foreign-born population increased from approximately
5.3 million in 2004 to approximately 9.3 million in 2018 [71]. From 2008-2018 the number of
non-EU migrants outnumbered EU migrants while the number of EU migrants increased more
rapidly [71]. Despite this, EU migrants were less likely to become British citizens than non-
EU migrants, but this may be related to the fact that at the time, EU citizens have right to work
and access public services in other EU member states.
By 2010 the Office for National Statistics estimated that of the UK population, 4.76 million
people (7.7%) were born outside the EU and 2.24 million (3.6%) were born in another EU
member state [72]. Census data provided by the Office of National Statistics in 2011 for
England and Wales shows that there has been an increase in minority ethnic groups, alongside
a reduction in people who identify themselves as white British [73]. Whilst the immigration
rates overall are increasing, review of the country of origin of these migrants has shown people
from South Asia continue to be one of the predominant sources of immigration over time (see
Figure 12). More latterly, there has been a substantial increase in Polish born people migrating
to the UK with increases (but less total numbers) also from those born in Nigeria and South
Africa. Over the same timeframe, there has been a reduction in those coming from the Republic
of Ireland (see Figure 12) [72].
Once migrant communities are established, they can facilitate further migration by providing
a source of support and information for any new arrivals. It is believed that this establishment
of migrant communities throughout the UK has been a source of encouragement to others in
their native countries and accounts, at least in part, for the increasing levels of migration seen
from areas such as South Asia and Poland over time as these communities become established
[74].
Non-EU immigration has been more stable than EU immigration, particularly since 2004. It
may be this is largely due to the free movement rules of EU member states that means people
can respond to changes in the political and economic climate both in the UK and their country
39
of origin such as the economic crisis in the UK in 2008, the Eurozone crisis, and the EU
referendum. Following the referendum, EU immigration fell sharply whilst non-EU
immigration increased steadily [75].
However, changes in policy in immigration rules in 2010-2012 saw a fall in non-EU migration
but these changes had been reversed by 2018 where the main reasons for immigration to the
UK were employment, particularly in the health care sector, and study [76]. Following the
2016 referendum result, employment related immigration decreased due to a decline in EU
immigration. However, it is uncertain what the ongoing consequence of the UK leaving the EU
will be in respect to migration patterns and particularly what policy or legal changes will ensue
as well as the economic climate in the UK post EU withdrawal [77].
In 2019, people born outside the UK made up an estimated 14% of the UK’s population, or 9.5
million people. Compared to the UK born, migrants are more likely to be of working age (26-
64 years old) which reflects the two major reasons for immigration (employment and study).
London has the largest number of migrants comprising 35% of the UK’s total foreign-born
population.
As would be suggested from the discussion in nomenclature above, the reasons for migration
are many and varied, with the patterns fluctuating over time. Whilst there has been an
association between migration and the labour market, in reality the patterns of migration are
more complex than this. Migrant groups are diverse, and include migrant workers, students,
refugees, asylum-seekers, family re-union migrants, trafficked persons and undocumented
migrants [78]. In recent times the refugee crisis has been a significant factor due to the
displacement of people due to war and persecution with the United Nations High
Commissioner for refugees noting forcible displacement of 79.5 million people by the end of
2019, (including those internally displaced) [79]. Developing countries are hosting more of
these refugees than ever before, but the pressures of migration on the EU from these conflicts
as well as existing migrant communities are substantial, with no anticipated easing in the
complex migration trends in sight [80]. In 2016, an estimated 362,000 refugees crossed the
Mediterranean Sea attempting to reach Europe [79].
40
Figure 12: Top 10 countries for non-UK residents in England and Wales compared over time [72]
III. Integration of Migrants
Social links between migrants and the native population can indicate the extent to which
society is divided by country of origin. However, integration of migrant groups into society is
complex, not least of all due to the variety of definitions used to characterise it as well as lack
of data collection particularly in new migrant communities. Furthermore, an apparent lack of
social contact between groups could be influenced by multiple factors including
discrimination, geographical and social distance (e.g. non-overlapping work locations) [81].
There have been attempts to determine public perception of social cohesion in their local areas
and migrants generally report similar levels of cohesion as the UK-born population [82]. In
fact, Indian and Pakistani born migrants living in both low and high income areas are
significantly more likely to report higher levels of social cohesion compared to the UK-born
people [82]. Whilst initially, migrants participation in voluntary organisations and leisure clubs
is lower than those UK born people, this participation increases with time spent in the UK and
0
100000
200000
300000
400000
500000
600000
700000
800000
India Poland Pakistan Republic of
Ireland
Germany Bangladesh Nigeria South
Africa
United
States
Jamaica
Top Ten Countries for non-UK Born Residents in England and Wales
2001 Census 2011 Census
41
therefore may be related to familiarity with these organisations and confidence in factors such
as language [82].
Generally, people identify themselves in various domains such as national, ethnic and religious,
but migrant identification is more focused on ethnic and national identity [82]. Some people
argue that this national identity will hinder integration in the new country and thus are
proponents of identifying with the country now lived in, but studies have shown that people
can jointly identify with both in parallel [83, 84].
The term integration is not universally adopted as it can suggest migrants are separate and
different, projecting a sense of other and accordingly creating a division [85]. However, when
used it often describes a complex multifaceted process rather than a single event in time. It can
be described as participation social interaction, cultural practices, civic participation (e.g.
volunteering) and participation in the new countries institutions e.g. education. However, all
these factors are fluctuant over time depending on life circumstances and are inter-related, for
example, participation in social events can foster a sense of belonging but may require language
skills [84, 86]. There is some public and media perception that migrants are not willing to
integrate e.g. not mixing outside their own communities without necessarily identifying the
barriers that can be faced.
Central government policy to foster integration has really only occurred for refugees, however,
some government policies have included migrants e.g. discrimination legislation. Whereas
other EU member states targeted new arrivals as priority for policy that encourages and enables
integration. In 2017 the All Party Policy Group on Social Integration described our policy
approach as “remarkably non-interventionist” particularly when compared to other EU states.
Whilst there is no national UK policy framework on integration, there is a history of integration
policy beginning in the 1960s, directed at migrants from Commonwealth countries. This was
based on the significant hostility these migrants faced at the time and focused on
discrimination, incitement to racial hatred and on ways to develop better community relations.
A Refugee Integration Strategy (2000) was designed to enable refugees to maximise their
potential and become equal members of society by accessing jobs, accommodation and
healthcare [81]. The following year (2001) wide scale disturbance in Northern England
triggered the government to adopt a community cohesion framework to address tensions
42
between ethnic minorities, but not specifically migrants, and white people but this focussed on
assimilation rather than integration as delivered in a speech by the Prime Minister at the time,
Tony Blair [87].
The next major policy development came in 2012 where a strategy paper called ‘Creating the
Conditions for Integration’ described integration being achievable by people contributing at
neighbourhood level together. A green paper followed in 2018 and a multi-department action
plan for England in 2019. The emphasis here was to focus on the distinction between
assimilation and integration drawing attention to the fact that everyone has a role to play in
making communities where all people coexist together based on “shared rights, responsibilities
and opportunities”. A key issue raised in debate was whether this what central or local
government responsibility.
Whilst migrants are granted some basic rights on their arrival to the UK (as per the European
Convention on Human Rights) other day to day freedoms (e.g. right to work, family reunion
and entitlement to social security) are dependent on immigration status which in turn relates to
nationality and length of stay. This variability in entitlements can make it more challenging for
employers, statutory agencies and migrants themselves to know what their restrictions are. It
could be said that these immigration policies are therefore a challenge to integration themselves
by marking out differences between migrant groups and well as between migrants and the
native population. Generally, the focus has been on the migrants themselves to integrate rather
than identifying and ultimately countering the barriers migrants face. There is a lack of data on
interventions for migrants to integrate to aid government, either local or central, in developing
policy. In fact, definition of what the outcome measures for integration would be could
potentially lead to greater ownership of the problem at all levels (societal, government and
third sectors) [88].
Tensions in society with a particularly negative view of migration has been seen in the last few
years, although there are many cases where migration and ethnicity are conflated. This has
occurred at a time when political rhetoric has been more negative about migration rates. Whilst
there has been some emphasis on the contributions of migrants to society, the overall
impression is one of limiting migration. The consequences of this more negative perception of
migrants may well be seen in integration but also in the known health inequalities that migrants
experience, and the broader socio-economic, cultural and environmental conditions that effect
43
health and healthcare engagement in migrant communities (see Figure 13). These poorer
outcomes occur at a socio-economic level, with regard to unemployment and over-qualification
compared to native born individuals across Europe [89]. Lower income levels are also
documented for non-EU migrants, with the resultant increased risks of poverty, social isolation
and overcrowding. First generation migrants are more at risk from these outcomes, with the
lack of established support they tend to have and is potential even further risk to those new-
migrant populations who will lack existing communities to embed into [89]. Whilst migrants
are heterogeneous, with marked variation in existing socio-economic status as well as social
support, the population risk for these groups overall is higher for the variety of factors that
influence health and wellbeing that are shown in Figure 13.
As outlined above, there are multi-faceted reasons why migrants can experience
discrimination. Some of this discrimination is akin to that faced by UK born ethnic minorities
and so tied to race, whereas others are related to being foreign born e.g. accent [90]. In 2018,
non-EU born migrants were twice as likely to describe themselves as members of a group that
faces discrimination because of nationality, religion, language, race or ethnicity, compared to
EU-born migrants (19% v 8%) [91]. Although there was an increase in perceived
discrimination in EU-born migrants around the time of the EU referendum in 2016 when public
concerns over immigration were the top issue for voters [92, 93]. This increase in perceptions
of hostility and discrimination among EU migrants during and after the EU Referendum, led
to a worsening of their mental health [94]. Overall, rates of perceived discrimination in
migrants in the UK was similar to those rates seen in the EU [91]. Whilst most foreign born
people living in the UK found it welcoming for migrants, 13% had been insulted because of
their ethnicity, nationality, religion, language or accent [91]. Studies have shown that job
applicants from minority backgrounds, including migrants, face discrimination [95]. It should
be noted that migrants from less developed countries are often perceived more negatively than
those from developed nations, regardless of their personal characteristics [96]. However, not
all discrimination against migrants is related to race, with low-skilled migrants being viewed
less favourably than higher skilled migrants [97, 98].
Minorities from predominantly Muslim countries (e.g. Pakistan) also experience
discrimination due to their religion, with data showing hostility towards Muslims in Western
countries [99]. Previous research has found that hostility can also come from liberal supporters
of immigration, who perceive Islam as a threat to European liberal values [100].

44
Public perceptions of migration in the UK in 2019 remain a source of division, with around
39% opining the level of immigration should stay about the same, while 44% said they would
like immigration to be reduced [91]. However, since the EU referendum, there has been a
change in immigration no longer being mentioned as the most important issue in the UK [91].
There was an apparent hierarchy with highly skilled preferred to the unskilled, and those from
culturally similar countries (e.g. Australia) preferred over others perceived to be more
culturally distant (e.g. Nigeria). This preference for highly skilled migrants was again noted
where members of the British public were asked what criteria should be applied to incoming
migrants, skills were highly regarded, but less emphasis paid to skin colour and religion [101].
Overall though there is some suggestion that attitudes to migration are becoming less absolute
after the EU referendum from both leavers and remainers [91]. It is difficult to be sure about
what underpins this change in attitude.
It has been shown that experiencing discrimination affects achievement, sense of belonging
and mental health [102, 103]. Overall, a groups perception of unequal treatment is an important
factor in their health and wellbeing as well as being a measure of social cohesion and a sense
of not being welcome or accepted has implications for integration [104, 105].
IV. Policy and migration
Government policy is an important driver in migration, and indeed determines the rules around
movement of people (non-EU and non-UK citizens) but can also inform public opinion around
patterns of migration. However, overall influences around migration are multifactorial, with
economic and employment the predominant drivers of international migration [106]. In the
UK, work is the most common reason for travel by non-UK citizens, although in non-EU
individuals study predominates, but this may be more directly related to government policy on
visa restrictions for non-EU migrants rather than the desire of these groups. Indeed, in the
majority of cases UK citizenship is granted in relation to work, meaning economic issues and
employment key aspects in UK migration [106].
In order to estimate net migration, the ONS uses data from the international passenger survey
(IPS). The UN definition of long-term migrant used by the ONS is relevant to policy, as
reducing net migration is a key policy objective of the current government, and the ONS
45
estimate is the usual measure cited in policy discussions. However, measuring migration
according to this definition poses several challenges. Firstly, it is not known how long any
individual who arrives in the UK will stay as IPS data are based on respondents’ intentions
only. In calculating estimates of long-term international migration (LTIM), the ONS attempts
to adjust for those who stay longer or depart sooner than intended but this is only an estimate
and is also based on self-reports. Home Office data gathered from immigration control
processes can determine how long migrants are entitled to stay but cannot tell us whether they
will depart early or extend their stay. Moreover, since data on departures from the UK are not
available, it is not possible to determine actual length of stay retrospectively. Furthermore,
LTIM estimates include asylum seekers in counts of migrants entering the UK, while
attempting to adjust the total numbers to exclude those who stay for less than a year and thus
do not qualify as migrants defined by length of stay. Public opinion surveys on immigration
attitudes reflect and may add to this confusion. Some surveys do not define their terms, leaving
respondents to answer questions based on their own implicit definitions or use definitions that
are distinct from the ONS meaning e.g. those who come to the UK to settle but which fit
dictionary meaning of the term migrant. With such a variety of definitions there is implications
for public and media debate on migration, indeed public opinion surveys show that members
of the public who want to see immigration reduced are more likely to focus on certain types of
migrants, especially so-called illegal immigrants but also asylum seekers, extended family
members, and low-skilled workers. Other types of immigrants such as students and high-skilled
workers also are counted in immigration statistics but have been of less concern in public
opinion.
In light of our exit from the EU a new immigration bill (Immigration and Social Security Co-
ordination (EU Withdrawal) Bill is before Parliament, and if this becomes law freedom of
movement will end, making EU citizens subject to the same immigration rules as the rest of
the world. Transition arrangements over social security measures still need to be clarified.
V. Migrants and Health
Migrant groups can face a higher burden of disease, compounded by inequalities in healthcare
access. Migrant health is complex, and related to multiple determinants across socioeconomic,
cultural and environmental conditions as well as individual characteristics and considers the
relation of these to both the host nation and country of origin [107]. Health disparities are

46
widely reported in migrant communities, with ethnicity often used as the identifying
characteristic in disease prevalence and health inequality studies. New migrant groups are
underrepresented in these studies, as ethnicity definitions are usually tailored toward the
existing minority communities [108].
Avoidable inequalities in the health status of migrants, as well as the quality and accessibility
of services for migrant groups have been reported across the European WHO region. These
inequities have been related to the social determinants of health, and social exclusion in
particular, at individual and community levels excluded from access and engagement in health
services. This social exclusion itself is complex but perhaps related to imbalance of power
across economic, political, societal and cultural grounds, with individual or institutional
discrimination further detracting from the individuals and communities ability to manage their
health [107].
Socioeconomic status is an important consideration and likely co-factor in health inequalities
in migrant groups, and lower socioeconomic status in arriving migrants would account for risks
including overcrowding, nutrition and poor sanitation, but there is clearly more to health
inequities than socioeconomic status alone [109], with individual risks, cultural practices that
may be associated with disease or wellbeing, the background prevalence of disease in the
country of origin, as well as an additional socio-economic burden that many migrant groups
face on arrival to the host country that is independent of their background and educational
status [89, 107, 110]. This model, the social determinants of health, is used and advocated by
the WHO (see Figure 13) to understand the multi-faceted domains in which healthcare
inequalities can exist. The factors described above regarding migration add further complexity
and relationship between the listed factors and migration specific features such as status of the
migrant, factors relating to country of origin and host country.
Accessible health services are often lacking for migrant communities, with a lack of awareness
of existing facilities, and a mismatch in the provision of language and culturally appropriate
services. Perceptions towards healthcare are known to vary in migrant groups, and newer
communities may be unfamiliar with preventative strategies in healthcare or broader models
of Western healthcare provision. It may also be that the migration process itself influences
healthcare access and uptake. Multiple factors are likely to influence healthcare access and
uptake in migrant communities, with previous reports that identify six key factors to be
47
considered: the legal entitlement of migrants, knowledge and awareness of the healthcare
system in the new country, previous experiences of healthcare, language and cultural barriers,
health beliefs and attitudes, as well as the structure of the healthcare system in the host country
[111]. Migrant groups across Europe and the UK are heterogeneous in nature, but are generally
younger than the native population, and most migrant groups are healthy and active
contributors to society [71, 112]. Healthier migrants are also more likely to remain in the new
country creating a so-called Healthy Migrant Effect. Despite the initial health advantage of the
migrant population, their health tends to converge to that of the UK born as their time spent in
the UK increases [113].
There are health issues that are identified more frequently in some migrant groups. Migrant
health is determined by multiple factors such as exposure in the country of origin (e.g.
infectious disease), cultural practices, socioeconomic factors as well as environmental risk-
factors in the host country on arrival (e.g. smoking, diet, alcohol or drug-use). There are also
differences in health perception, and service utilisation in some migrant groups. Language
barriers are important in healthcare delivery, however culture can also be a significant
influence [114]. Whilst it is known that those with higher socio-economic status (e.g. income)
have better health outcomes, there are complex reasons for this beyond pure economics [115].
Some low-skilled jobs increase the risk of experiencing health problems [116] because of their
physical nature and also poor working conditions (e.g. cleaning or construction), or because
they are lower paying meaning people are less able to purchase goods and services to improve
their health [117]. In addition, people that are unable to move out of low-skilled and low-paid
jobs are more likely to experience chronic stress due to their socioeconomic situation [118],
which ultimately affects their overall health. The corollary may also be true with poor health
potentially affecting ability to work. Both migrants and the UK born employed in high-skilled
jobs are less likely to say they have a limiting health problem than those in low-skilled jobs.
Reviews looking at ethnic minority use of NHS services illustrate the presence of access
problems [119], and that these are not solely socioeconomic. Cultural differences (patients’
health and perception of disease as well as their health behaviours) are likely to last over
language issues in migrant groups. These factors, therefore, will require acknowledgement and
addressing ideally with the help of those members of the particular culture for the successful
development of an intervention.
Successful implementation of public health interventions to tackle health inequalities depends
on behaviour change. This requires understanding of the behaviours to be changed, the drivers

48
to maintain the current behaviour, barriers and facilitators to change and the expertise to
develop strategies to achieve change based on this understanding [120]. The evidence base for
interventions of this nature are largely centred around screening programmes. Most of the UK
data is therefore largely based around screening for malignancy. Whilst there is much data on
the factors that influence screening uptake the literature is less conclusive over the
effectiveness of interventions, particularly those in particular groups in the population rather
than in the population in general.
Migrant groups do however face inequalities in healthcare access in the host country, as well
as altered patterns of healthcare engagement that can leave this community vulnerable [107],
in addition to a higher burden of disease risk that may exist from their native environment.
First generation migrants, and new migrant communities may be at even greater need with
regard to disease burden compounded by uncertainty in how to reach these new communities
in healthcare engagement [121].
Migrant communities face health vulnerabilities, including the global risks of CVH that require
the delivery of effective testing strategies to understand and manage these risks, which will
otherwise remain undetected until complications develop. At the same time, migrant
communities are facing increasing anti-migrant sentiment, expressed at the political and social
level, coupled in the UK with uncertainty related to EU withdrawal.
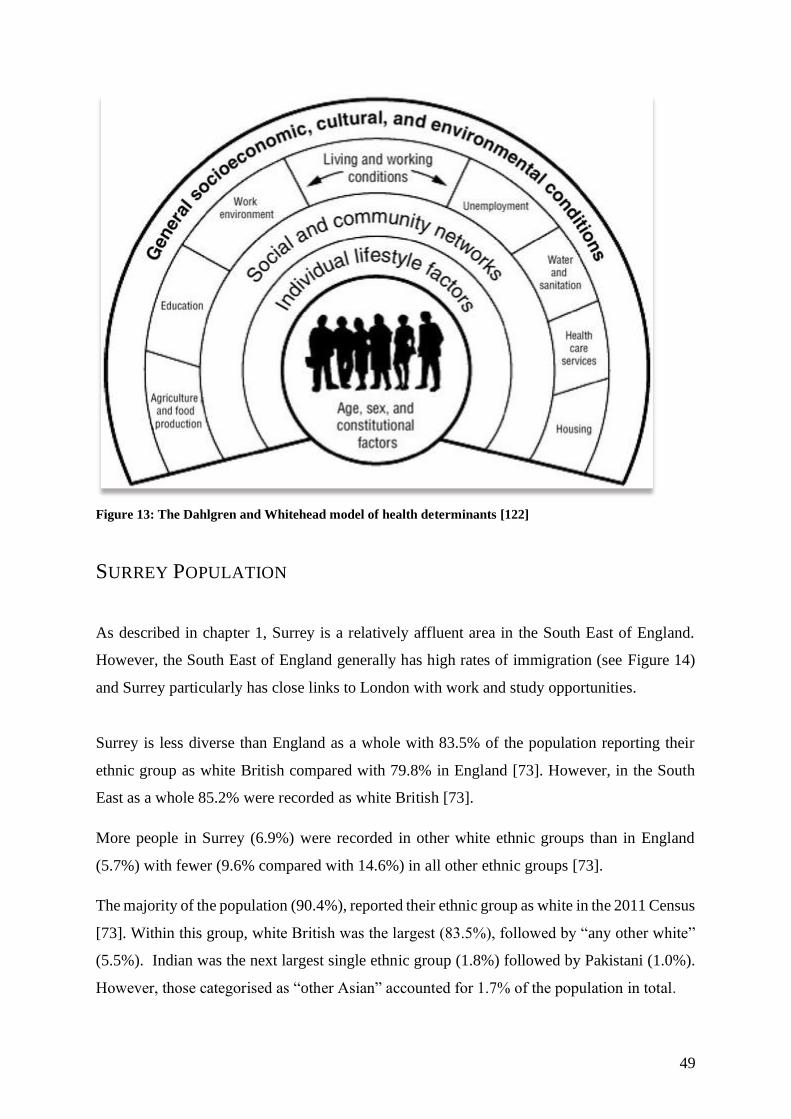
49
Figure 13: The Dahlgren and Whitehead model of health determinants [122]
SURREY POPULATION
As described in chapter 1, Surrey is a relatively affluent area in the South East of England.
However, the South East of England generally has high rates of immigration (see Figure 14)
and Surrey particularly has close links to London with work and study opportunities.
Surrey is less diverse than England as a whole with 83.5% of the population reporting their
ethnic group as white British compared with 79.8% in England [73]. However, in the South
East as a whole 85.2% were recorded as white British [73].
More people in Surrey (6.9%) were recorded in other white ethnic groups than in England
(5.7%) with fewer (9.6% compared with 14.6%) in all other ethnic groups [73].
The majority of the population (90.4%), reported their ethnic group as white in the 2011 Census
[73]. Within this group, white British was the largest (83.5%), followed by “any other white”
(5.5%). Indian was the next largest single ethnic group (1.8%) followed by Pakistani (1.0%).
However, those categorised as “other Asian” accounted for 1.7% of the population in total.

50
As compared to the previous census in 2001, Surrey appeared more ethnically diverse,
however, it is notable the wording of the question changed from cultural to ethnic background.
While white continued to be the majority ethnic group people identify with, it decreased over
the last decade. In 2001, the white ethnic group accounted for 95.0% of the population. This
decreased between the 2001 and 2011 Censuses to 90.4%. Within the white ethnic group, white
British had decreased from 89.3% in 2001 to 83.5% in 2011. There was an increase in all other
minority ethnic groups with a big increase in people reporting their ethnicity in “other Asian”
groups. Across the districts in Surrey, Woking was the most ethnically diverse area, and
Waverley the least.
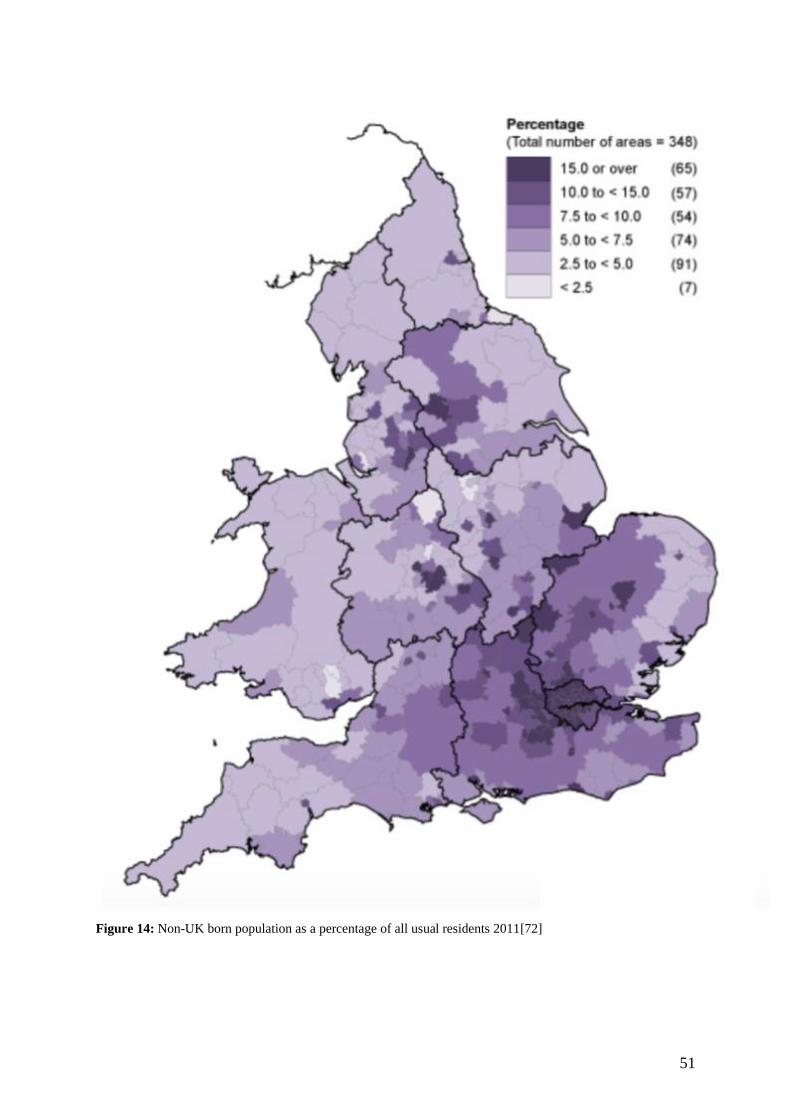
51
Figure 14: Non-UK born population as a percentage of all usual residents 2011[72]
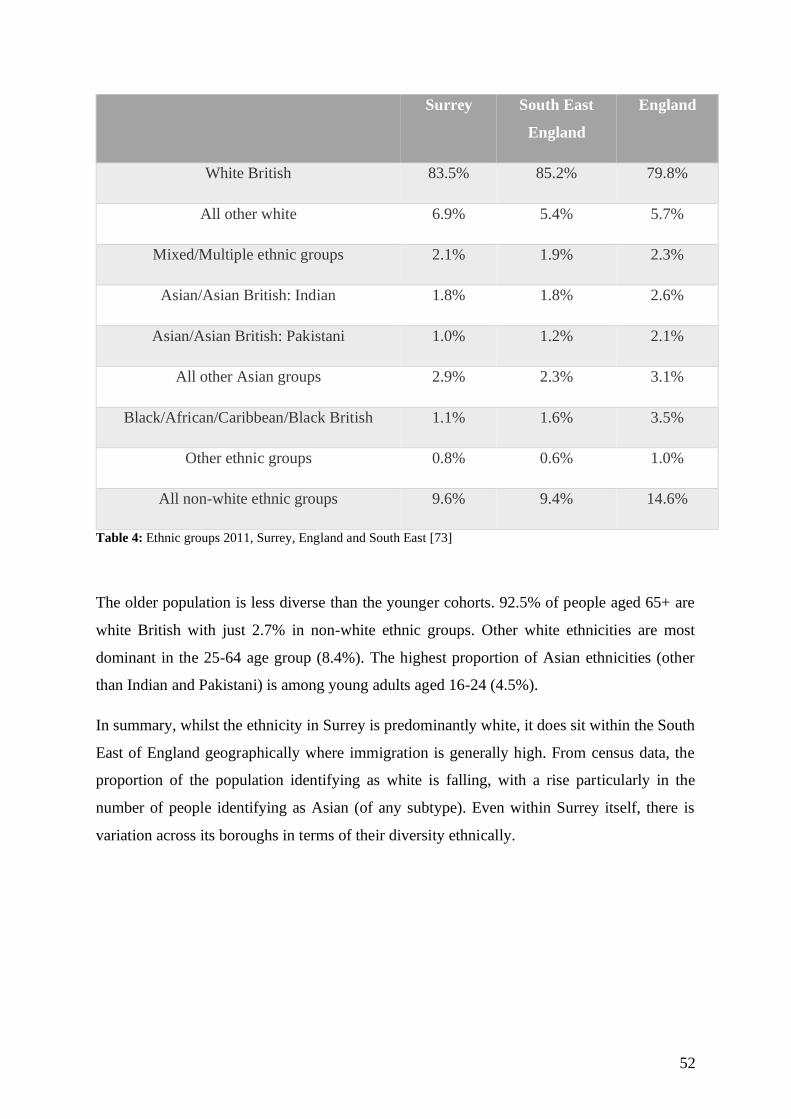
52
Surrey South East
England
England
White British 83.5% 85.2% 79.8%
All other white 6.9% 5.4% 5.7%
Mixed/Multiple ethnic groups 2.1% 1.9% 2.3%
Asian/Asian British: Indian 1.8% 1.8% 2.6%
Asian/Asian British: Pakistani 1.0% 1.2% 2.1%
All other Asian groups 2.9% 2.3% 3.1%
Black/African/Caribbean/Black British 1.1% 1.6% 3.5%
Other ethnic groups 0.8% 0.6% 1.0%
All non-white ethnic groups 9.6% 9.4% 14.6%
Table 4: Ethnic groups 2011, Surrey, England and South East [73]
The older population is less diverse than the younger cohorts. 92.5% of people aged 65+ are
white British with just 2.7% in non-white ethnic groups. Other white ethnicities are most
dominant in the 25-64 age group (8.4%). The highest proportion of Asian ethnicities (other
than Indian and Pakistani) is among young adults aged 16-24 (4.5%).
In summary, whilst the ethnicity in Surrey is predominantly white, it does sit within the South
East of England geographically where immigration is generally high. From census data, the
proportion of the population identifying as white is falling, with a rise particularly in the
number of people identifying as Asian (of any subtype). Even within Surrey itself, there is
variation across its boroughs in terms of their diversity ethnically.

53
Age
0-15
Age
16-24
Age
25-64
Age 65+ All
people
White British 81.4% 80.9% 81.9% 92.5% 83.5%
All other white 5.1% 6.1% 8.4% 4.8% 6.9%
Mixed/Multiple ethnic groups 5.2% 3.1% 1.3% 0.3% 2.1%
Asian/Asian British: Indian 1.9% 1.6% 2.1% 0.7% 1.8%
Asian/Asian British: Pakistani 1.5% 1.3% 0.9% 0.3% 1.0%
All other Asian groups 2.9% 4.5% 3.2% 0.8% 2.9%
Black/African/Caribbean/Black British 1.1% 1.5% 1.3% 0.2% 1.1%
Other ethnic groups 0.9% 1.0% 0.9% 0.3% 0.8%
All non-white ethnic groups 13.5% 13.0% 9.8% 2.7% 9.6%
Table 5: Ethnic groups by age 2011 [73]

54
CHAPTER 3: HEALTHCARE POLICY AND CASE-FINDING IN CVH

55
INTRODUCTION
Screening in healthcare is performed at a population level by testing people who are
asymptomatic e.g. bowel cancer screening with inclusion criteria of age. Case-finding is a more
targeted type of screening for groups in a population at higher risk, or perhaps could be viewed
as screening within a subgroup of the population. Data on case-finding somewhat lacking but
there is some data on screening, particularly methods to encourage the uptake of screening but
mainly the facilitators and blockers to screening uptake.
I. Screening in Medicine
Health screening and reduction in health inequalities are national and international priorities
[123, 124]. Screening identifies asymptomatic people, providing earlier diagnosis, better
health outcomes [125-130] and decreases mortality [126, 131]. Screening tests are introduced
based on analysis of the effectiveness, cost and acceptability of the program [132-134].
Significant proportions of the population must participate to observe improvements in outcome
with uptake being the most important factor in determining a program’s success [135-137].
Screening programs in adults are mainly cancer-related [45]. Many programs actively promote
screening, utilising resources to facilitate uptake and often offering free screening [134].
Despite this, uptake often remains suboptimal, mirroring health service uptake in general with
pockets of the population showing poor coverage [114]. At the same time, there is recognition
of the importance of cultural, social and economic factors on health and health behaviours.
Arguably, these requirements are more important in screening where there is a lack of driver
to seek health care as the population targeted is asymptomatic.
However, within the spectrum of screening is case-finding where rather than target whole
populations specific higher-risk subgroups are targeted. As such, the same accepted standards
for screening should apply to case-finding.
Minority groups generally have a lower uptake of screening. Across screening programs there
are identified logistical, psychological and cultural barriers [138]. Black, Asian and minority

56
ethnic groups (BAME) are more likely to have a poorer experience of care as well as lower
attendance at various screening programs in both the UK and USA [139-146] . Attempts to
improve uptake have been made by instituting various interventions, often based on single
screening modalities or single populations (i.e. akin to case-finding) [147-149].
Various systematic reviews looking at interventions to improve screening have been limited
by heterogeneity of methodology and the lack of rigorous assessment of the effect of
interventions used. There are, however, some important findings in the literature. In particular,
a systematic search of literature published between 2000-2008 was carried out, focusing on
interventions to improve uptake of screening in specific subgroups of populations with low
uptake, rather than increasing general screening rates [147]. A consistent problem across such
reviews is a substantial amount of data comes from North America where financial and
organizational factors are not in keeping with those in the UK There were findings that would
appear more generalizable with multiple reviews showing culturally relevant interventions
along with those that minimize logistical difficulties had the most effect [147].
A UK public health based systematic review conducted in the context of breast and cervical
cancer suggests a multifaceted approach is required to design interventions that are language
and culture specific for ethnic minorities [150]. These two systematic reviews of the evidence
on strategies for increasing screening participation concluded that almost all active recruitment
strategies examined were more effective than no intervention [147, 150]. It was, however,
unclear whether individualized messages helped or hindered, with contradictory literature.
Those interventions that provided logistical help with appointments were overall helpful,
although the use of peer educators and lay health advisors had mixed outcomes.
As part of this work, I have performed a systematic review of interventions to improve
screening uptake amongst ethnic minorities [151]. There was little UK based data as was found
in other reviews. The heterogeneity of groups and methodology of trials poses a challenge in
analysing the data available. However, I still found themes when reviewing the data by type of
intervention. Multifaceted interventions were broadly successful as were group-education
sessions and media interventions. Apparently less successful were lay-health worker (LHW)
interventions; despite being the most common intervention type.
Recommendations from these all these reviews include a call for more robust data and more
57
outcome measures to reduce inequality in screening in the UK In particular, they highlight a
need to focus on a small number of interventions with favourable outcomes in a UK context;
setting up a central facility for published and grey literature on interventions and systematic
introduction of new interventions locally with good practice highlighted with the ability to
assess the transferability to other geographical areas.
The problem faced by these studies is that many of the trialled interventions relate to
established national screening programmes with facilities in place to reach the target
population. This is something that is not yet in existence for our target population and
condition. Additionally, there are emotive and other issues around cancer screening that may
not be relevant to this project and as such the interventions and the data around them may not
be extrapolated well to this study.
II. Screening in Liver Disease
Screening for liver disease in general has been considered given the rising burden of both
morbidity and mortality this is causing in the UK (see Figure 1). Chronic liver disease has been
underestimated as a global public health problem. There would appear to be a need for
screening as it is a prevalent condition that is silent in the early stages of disease. There is a
need for effective global actions including education, prevention and early diagnosis for
management and treatment to prevent cirrhosis-related morbidity and mortality. The aetiology
of chronic liver disease will vary geographically and also over time as the expected fall in
chronic viral hepatitis makes way for other causes such as NAFLD. There does, however,
remain a need for public health population-based awareness and action. Health literacy in
liver disease remains low, even in those who are known to have chronic liver disease [152].
However, screening in liver disease can be problematic and it is unclear which test would have
adequate sensitivity, specificity and acceptability to the individual whilst still being affordable.
Liver function tests can be normal at all stages of liver disease. Invasive screening by liver
biopsy would represent an unacceptable clinical risk and resource utilisation. Whilst there is
an ever-increasing ability to screen non-invasively this is not always effective and is more
useful for determining risk of cirrhosis and prognosis in established liver disease. Furthermore,
serological markers can be difficult to interpret e.g. antimitochondrial antibody (AMA)
58
positivity with normal LFTs. However, there have been calls to screen the general population
for liver fibrosis, despite it being unclear what shape this will take [153, 154].
A population-based cross-sectional study in Barcelona aimed to determine the prevalence of
liver fibrosis in adults without known liver disease [154]. They randomly targeted adults aged
18-75 years from their primary health care registry, with a participation rate of 63.2%.
Participants underwent assessment of medical history including alcohol consumption,
anthropomorphic measurements, blood tests and assessment of liver fibrosis by measuring liver
stiffness with transient elastography (TE) with Fibroscan®. Increased liver stiffness was
judged as >6.8kPa. Those with liver stiffness measurement (LSM) >6.8kPa or ALT >x2 upper
limit of normal were referred to a hepatologist and this represented 10% (9% with raised liver
stiffness measurement) of their study population, with 66% ultimately taking up this consult.
Additional analysis using higher stiffness measurements were also reported with 5.8% of their
cohort having LSM >8.0kPa and 3.6% with LSM >9.0kPa. A correlation was demonstrated
with male gender, abdominal obesity, T2DM, serum glucose, HDL, TG and raised AST/ALT
and raised liver stiffness. Similar work with population based screening confirmed a link with
diabetes mellitus and steatosis, with liver stiffness >8.0kPa in 5.6% of a European population
[155] and 4.7% in a Taiwanese group who also found a significant association with AST and
diabetes mellitus [156].
A subgroup of the Barcelona study underwent liver biopsy with significant liver fibrosis (F2)
of 9.2kPa (sensitivity 93%, specificity 78%). The underlying aetiology was ultimately NAFLD
then alcohol. TE was more accurate than ALT, NAFLD fibrosis score and FIB-4. However,
these tests were designed for different purposes. This study found almost 75% of their cohort
with LSM >9.2kPa had normal ALT demonstrating that assessment of liver biochemistry on
its own is not a successful strategy. However, this was a white population, with only 5%
BAME. Importantly, there was no cost analysis. Additionally, this was aimed at detecting
those with risk of liver disease from primary care. However, in the UK funding of such a
program is likely to be difficult. Furthermore, there are still secondary care centres in the UK
who do not have direct access to Fibroscan® which would make such widespread roll-out
challenging.
A simpler approach has been advocated, utilising ALT for population-based screening, arguing
59
elevated ALT levels are correlated with the grade of necroinflammation which is known to be
important in progression of liver disease, even if not stage of fibrosis. Furthermore, ALT
measurement is simple and inexpensive which will allow further investigation to assess for
fibrosis. The sensitivity of ALT could be improved by better defining a normal range, and
repeat measurements could be achieved easily which would further improve sensitivity for
chronic liver disease detection [157].
Overall, there is currently no clear target for a single test that would meet accepted criteria for
a screening test for liver disease.
III. Existing Literature on Case-finding in CVH high risk groups
Given migrant communities are recognised as a higher-risk group for CVH, there have been
clinical trials to engage a range of migrant communities in CVH testing. These are a
heterogeneous group of studies in terms of the population studied and the methods used within
the trial.
Community based interventions (CBIs) are often multifactorial interventions combining
individual, group and policy features to promote health among population groups in a defined
local community. In most cases, entire communities (e.g. a whole city) are used as units of
intervention. From the ethical point of view, it seems reasonable to offer prevention to all
members of a community. Whilst they can offer the opportunity to trigger large scale change,
they can be expensive in resource and time and it can be challenging to measure outcomes as
the time scale needed to detect significant change (especially in less frequent events). CBI, an
example of a complex intervention, include the nature and extent of the relationship between
the clinical team and the target community. The ideal intervention having been described as an
equal partnership between experts and the communities they serve where the experts provide
scientific rigour in study design and implementation and the community involvement supports
the study in a sociocultural domain [158]. This relies on the community engaging and
supporting with the research team from study concept, design and implementation as well as
the intervention itself and the need for it.
60
The term community can be used to describe a population but can also describe a group of
people with a shared identify and sense of belonging which can be utilised to support change
and implement policy within the group. Community-based has a wide range of definitions,
however, in the public health setting it has been described in the following domains:
community as the setting; community as the target; community as the agent and community as
a resource [159].
Community as the setting principally defines a geographical location where an intervention is
carried out e.g. within a city or particular venues such as churches. The intervention can be
varied depending on the setting such as mass media strategies or educational classes targeted
at individuals, families, networks or policy areas. The interventions themselves may utilise
patient public involvement within the community to create investment within the target group
in the project as well as to facilitate appropriate targeting of the information and intervention
type to the defined population. Overall, the aim is to change the behaviour of individuals in
order to reduce the populations risk of illness as population change relies on the accumulation
of individual change.
The community as the target is a strategy that involves widespread change in public policy and
services in order to develop healthy community environments. The aim of this strategy is to
look further than change in individuals’ behaviour and target the interventions to foster
community changes, particularly related to public health, to change the health status
characteristics of the community such as the ban on smoking in public places or developing
intervention to improve air quality targets.
The community as a resource is an approach, often used in health promotion, that emphasises
community ownership of interventions affecting them to improve participation within the
target population to improve the long-term viability and success of interventions. This can be
for an outcome selected by the community itself, or a pre-existing focus from national or local
priorities but which relies on external agents and resources to achieve the desired outcomes.
This approach is often used in major public health campaigns.
The community as the agent is similar to the community as a resource but relies on utilising
and further developing the pre-existing support networks and adaptations within existing
communities such as families, social networks and clubs as well as local business, voluntary
sectors and local government.

61
However, these concepts are used in conjunction with each other, rather than in isolation as
community-based health promotion requires a multi-faceted approach to identify, engage and
develop relationships with the target community. Indeed, it has been suggested that modern
community based public health strategy has two core features namely strengthening the health
of communities and building community capacity to address health-related issues [159].
Most published studies focus on testing strategies in established migrant communities,
typically utilising lay community or religious leaders to facilitate testing, recruitment and
engagement. There is heterogeneity between studies, and the success of testing uptake is often
not apparent, with difficulties in knowing the number of people the intervention reached. Often
testing uptake is inferred by the study size, number of participants and recruiting events
required to achieve the number tested.
In all voluntary community-based approaches, self-selection bias a common factor, and it has
been suggested that rates of infection may indeed be higher in those individuals who do not
take up such offers, due to co-morbid disease, or risk-activity that makes them paradoxically
reluctant to attend [121]. Whilst primary care testing is an alternative that may reach out to
these individuals, recent studies in West London have shown poor attendance (10%) by
members of migrant communities in specially prepared new-patient testing sessions, despite
an estimated local migrant prevalence of over 40% [160].
A range of different techniques have been utilised to recruit to testing studies as well as for
testing itself. In the UK, various sites where there are large migrant groups were involved in a
study that tested almost five thousand people for viral hepatitis at fifty-two different sites with
oral fluid testing in community venues. Some were also approached in primary care waiting
rooms whilst attending for another reason. However, the primary aim of this study was to
determine prevalence and as such interventions were not utilised [121]. A pilot study in the
North of England invited members of the South Asian community to attend screening sessions
for CVH by finger prick testing in a mosque and community centre, testing 329 people in four
sessions finding 1.8% of HBsAg, 2.8% past HBV exposure and 1% HCV Ab positive [161].
Also, in the North of England, the South Asian population were targeted through mosques and
community centres to raise awareness of chronic HBV through advertisements and meetings.
All 156 people who attended these meetings were tested with dried blood spot with one active
62
and ten previous exposures found [162]. However, this may represent a selection bias as it
may be those already interested in health screening or hepatitis attended. It is not clear who did
not turn up to the sessions who the advertising reached.
Investigators in Dundee aimed to investigate the prevalence of HCV in an immigrant Pakistani
population and the effectiveness of an outreach testing intervention that was effective but had
problems with recruitment, small numbers and lack of female participation [11]. This study
involved a series of awareness meetings where risk factors for infection, prevalence, lack of
symptoms, the slow progressive nature of disease, complications and the existence of treatment
were discussed. The tested population was skewed towards males (85%) and attempts to
increase female participation by engaging community women’s group but these groups focused
on the older generation or those not working. There were issues with this study that are
acknowledged by the authors. Utilising mosques (and religious venues more generally)
excludes those members of the population who do not attend that venue. In line with the
majority of studies of this type, testing relied on study participants volunteering for it. Whilst
this is less problematic for pure case-finding it is a limitation in prevalence studies where
participants may only volunteer for testing if they feel they are at high risk [11]. Overall, the
authors conclude the Pakistani population has higher rates of infection that justify intervention,
particularly given the cultural and religious events that would provide effective arenas for a
targeted intervention [11]. This is supported by modelling from NICE showing that provided
the prevalence of chronic viral hepatitis in migrants from minority groups was at least 2% then
it was estimated that it would be cost effective to find, treat and test within such communities
[3].
In the UK, community-partnership approaches have been tested in the South Asian community,
utilising religious and community settings in Mosques, Temples and established community
venues. Such approaches and settings seem to be popular, with close to 4600 individuals tested
in (primarily) religious settings across the UK [121]. The support of religious leaders, and the
delivery of testing at the place of worship (through finger-prick blood tests, or mouth swabs)
do seem to be important, whether purely due to convenience or not, with the same group
showing no uptake in testing when 5000 invites were distributed to a Mosque without local
testing at that venue [121, 163].
Similar methods, utilising primarily religious settings have proved successful in studies in the

63
Egyptian Coptic community, and in the Korean Christian community in North America,
achieving a high number of HBV and HCV tests in these populations, with around 100
individuals tested per session in the US based Korean Church study [164, 165]. Similar studies
in the Chinese community in the UK have used established community venues, churches and
local wholesalers to advertise testing, with testing uptake in around 230 individuals (around 15
individuals per session) [166].
A study in the Netherlands mailed out invites to 1787 Dutch-Turkish people identified from
the regional migrant registration records. This letter (and a reminder invite where needed) led
to a 16% uptake of testing. When testing was further advertised in a local newspaper and
website the uptake of testing rose to 30% [167]. This method performed better than a previous
study of the same population using religious and community leaders only (10%) [168], but was
more intensive in requiring regional government input to identify and invite people.
An American based study utilising community based participatory research developed an
educational programme for Korean Americans based in churches to raise awareness and
promote testing for HBV [169]. Results of this pilot study showed at 6 months follow up 93%
of the intervention group were tested, with only 2.9% in the control arm tested [169].
A Belgian study in a South Asian population demonstrated linkage to care was better in a point
of care group than formal venepuncture as well as lower cost per person screened [170].
Behavioural modification has been attempted by researchers in the Netherlands, providing
behavioural and cultural prompts to link HBV and HCV tests to religious (Islam) and cultural
beliefs of healthcare, and wellness. Such methods have not shown a clear benefit in testing
uptake, but perceptions towards health and testing were higher in those individuals receiving
behavioural interventions with the potential for these strategies to have benefit over the longer
period in healthcare engagement in migrant communities [171]. As such community
partnership models with support from religious and community leaders seem an effective route
to approach migrant groups for testing, but with the limitation that these measures are largely
restricted to those established migrant groups with existing community venues, or religious
homogeneity.
The largest and community testing program based in New York City, the BfreeNYC project,
64
undertaken between 2004 and 2008 tested 8,888 migrants (mainly of Chinese and Korean
descent) for HBV. This was a large-scale program advertised extensively including in major
media outlets and championed by city councillors. Stigma was not reported from the wider
community during the advertising process, and indeed members of the Asian community
associated less stigma towards viral hepatitis as a result of the awareness-raising programme
[172, 173].
An electronic health record prompt to primary care physicians to test Asian American patients
for HBV versus a control with no prompt showed an increase in testing order in the intervention
group (40.9% v 1.1%) with uptake in testing in the intervention group of 30 of the 36 requested
patients [174].
Most community testing studies focus on testing in one community, with a Dutch study by one
of the few to describe testing in multiple geographically separate migrant communities in a
single event [168]. Individuals were identified and directly invited by mail from the local
municipality. Advertising was delivered in local media sources (newspapers, websites), with
no mention of any undue stigmatisation in the wider community, and with an uptake of HBV
and HCV testing in 30% (959 of 3226 individuals) who attended a community talk delivered
by hospital physicians. Individuals attended from Asia, Eastern Europe and the Middle East
with marked cultural diversity, but with reasonable levels of engagement from all groups. Rates
of infection differed between communities, but the high levels of uptake in first generation
migrants from different populations is positive [168].
A meta-analysis of interventions to promote HBV testing found nearly half (7/15) utilised lay
health workers (LHW). Six of the seven LHW-led interventions were one off activities that
delivered educational content tailored to a particular community’s cultural and social context
[169, 175-180]. All of these studies were conducted in the USA or Canada. Self-reported HBV
testing rates were higher among groups that received one of these single LHW educational
interventions to improve HBV knowledge and promote testing compared to groups that
received no or unrelated educational interventions (RR = 2.68, CI 95; 1.82–3.93). All studies
found LHW-led interventions had a positive effect on HBV screening; however, these results
were heterogeneous. This heterogeneity in effect size may be due to differing study design
(three were RCTs randomized by cluster, and three were RCTs randomized by individual) and
intervention setting (three were home visits, and three were delivered at a community-based
65
organisation). These findings are consistent with the growing body of evidence demonstrating
that lay health workers can effectively perform a range of interventions that would otherwise
be undertaken by trained medical personnel. The lay health workers in the six studies received
training in order to help tailor the educational intervention and this training component was
relatively simple and of low cost. Analysis found the interventions acceptable to the study
participants and to the LHWs. While the importance of cultural context in developing
interventions to improve HBV screening in high-risk populations and the usefulness of
community settings in the delivery of healthcare is important, the low-cost nature of this
intervention could facilitate its used in resource limited settings. However, many LHW studies
rely on self-report of testing and do not report on results of testing. The accuracy of this is not
established.
A UK based study utilising primary care databases in East London were screened for migrants
at risk of viral hepatitis. Identified patients were sent invitation letters with information sheets
in their native language and asked to attend for testing. However, the trial was stopped early as
only 2.3% took up this offer [181].
A more recent UK based study aimed to determine whether incentivising and supporting
primary-care physicians in areas with a high density of migrants increases the numbers of adult
migrants screened for viral hepatitis [182]. This was a multicentre, open, cluster-randomised
controlled trial in general practices in areas of the UK with a high density of migrants
(Bradford, Yorkshire, Northeast and Southeast London). General practices were randomly
assigned to an opportunistic screening (control) group or to one of four targeted screening
(interventional) groups. The interventions were either standard (i.e. hospital-based) care and a
standard or enhanced invitation letter or community care and a standard or community care
and an enhanced invitation letter. In control screening, general practitioners (GPs) were given
a teaching session on viral hepatitis and were asked to test all registered migrants. In the
intervention, GPs were paid a nominal sum for setting up searches of records, reimbursed for
signed consent forms, and supported by a dedicated clinician. The primary outcomes were the
proportion of patients eligible for screening, the proportion of those eligible who were sent an
invitation letter in the intervention groups, the uptake of viral hepatitis screening (in the
intention-to-treat population) within 31 days of being sent the letter, the proportion of patients
who tested positive for viral hepatitis, the proportion who complied with treatment, and the
cost-effectiveness of the intervention. To determine whether screening migrants in an area with
66
a low density of migrants was effective, they also did a parallel, non-randomised sub study
with identical procedures and outcome measures in Oxford. All patients who tested positive
for viral hepatitis in the screening trial were eligible for enrolment in the embedded trial to
compare standard hospital-based care to community care. Community care was delivered at
general practice surgeries that were not necessarily the surgery where the patient was normally
seen. Most of the primary care centres that were approached participated (63 of 70). In the
eight control general practices, screening was taken up by 1.7% of eligible participants, the 50
general practices that used the intervention, screening was taken up by19.5% of eligible
participants (p=0·014) and the intervention was cost-effective. Testing uptake was similar for
enhanced versus standard letters (p=0.26). The investigators conclude that screening migrants
for viral hepatitis in primary care is effective if doctors are incentivised and supported.
Community care is expensive and there is no evidence that this offers benefits in this setting or
that bespoke invitation letters add value.
Linkage to care for positive cases is poorly documented in most studies, with high rates of
individuals lost to follow-up. As noted above, the largest study of this nature, the BFreeNYC
study, around 57% of trial participants were kept in services until the end of the 4 year study
[158].
In summary, the SA population in the UK has a higher than average prevalence of chronic viral
hepatitis with morbidity and mortality also disproportionately higher. A key driver amongst
clinicians and health care policymakers is to identify the hidden burden of chronic infection
and thus minimise the burden of end stage liver disease and its complications. Identification of
this hidden burden of CVH is key to the aim to eliminate CVH as a public health problem by
2030. In order to facilitate the uptake of testing amongst this particular at-risk group
identification of the barriers to change and access to health care will be carried out within the
community setting with an aim to improve uptake of testing. A particular target will be females
who have been underrepresented in previous studies. There is no data at present on the effect
of an educational film and this project aims to explore the feasibility of performing such a trial
that if successful could be rolled out in other regions with a view to developing new policy and
services that are accessible.

67
CHAPTER 4: AIMS, OBJECTIVES AND STUDY DESIGN
68
INTRODUCTION
This chapter provides an overview of the aims and objectives of this thesis. It was community-
based work looking specifically at detecting chronic viral hepatitis in South Asian migrants.
Migrants from moderate to high prevalence countries, such as South-Asia, are considered a
higher-risk group in line with NICE recommendations [3]. Case-finding for chronic viral
hepatitis is a national and international priority. Despite guidance recommending testing of
higher-risk people, it is unclear what specific intervention is effective in achieving this goal.
There are two studies which make up this thesis. The first explored existing knowledge of CVH
in our target community through focus group discussions. The knowledge gained from this was
used to develop a short educational film on CVH that was culturally and linguistically tailored
to our population. As part of the funding application the nature of the intervention (film) was
predetermined. The second study was a feasibility study using this film in community settings
to encourage testing for CVH. A questionnaire was developed to be used before and after the
film to help analyse its utility.
These two studies were funded by the National Institute of Health Research (NIHR) research
for patient benefit stream (PB-PG-1013-32094). This grant was awarded to Professor Aftab
Ala with the sponsor the Royal Surrey NHS Foundation Trust, Guildford and I was appointed
clinical research fellow thereafter.
STUDY 1: EXPLORING AWARENESS OF CVH IN THE SOUTH ASIAN MIGRANT
POPULATION IN ORDER TO DEVELOP A TAILORED EDUCATIONAL (FILM)
INTERVENTION
I. Aims
1. To report current ideas, knowledge and opinions on viral hepatitis amongst South Asian
migrants
2. To identify barriers to testing for CVH in the SA community, and more generally any
barriers and facilitators to accessing healthcare for this population
3. To identify key themes emerging from focus group data analysis to aid development of
an educational intervention (culturally and linguistically tailored film)
69
4. To develop a questionnaire to be complete pre- and post-educational intervention to aid
analysis of the intervention
To gather information, focus groups (FGs) were used. These have benefit over questionnaires
and individual interviews by allowing discussion and exchange of ideas. The role of facilitator
is key, and this was performed by a culturally and linguistically appropriate researcher.
The FGs were encouraged to discuss chronic viral hepatitis and to identify knowledge and
attitudes to risk, testing, diagnosis and treatment through the design of a FG guide. Data was
also gathered on opinions on healthcare, particularly access and stigma. Ideas were also
gathered from participants on how best to structure the film and also how to use existing
community groups to facilitate recruitment to study two. A particular aim was to gather and
incorporate the views of women as previously this group have been underrepresented.
Participants were recruited in a number of cohorts as shown below:
Cohort 1: Focus Group Participants:
Recruitment of first generation South Asian (SA) migrants to a series of focus groups
discussing CVH in community and religious settings. The FG data was analysed, using
thematic analysis, to create themes which were the basis of the structured message for
the educational film.
Cohort 2: Participants used in the filming of the educational intervention:
This was a mix of patients known to the clinicians on the study team, and clinicians
themselves. Combining expert testimony with real life stories was favoured by the
participants in the focus groups. A selection of questions were put to each participant
whilst being filmed leading to many hours of footage. These questions were designed
to address the key themes and common misunderstandings seen in the FG discussions.
The recordings were transcribed and subsequently refined to highlight the key messages
from the focus group data with the input of a professional film maker.
Cohort 3: Validation Cohort:
Validation of the educational intervention and questionnaire by new participants with
no prior involvement in the work.
70
STUDY 2: A NOVEL EDUCATIONAL INTERVENTION TO IMPROVE THE UPTAKE OF
TESTING FOR CHRONIC VIRAL HEPATITIS IN SOUTH ASIANS (SA): A
FEASIBILITY STUDY
I. Study Aim
To assess the feasibility of recruiting South Asian people in community settings to view an
educational film to promote testing for viral hepatitis in South East England.
II. Patient Recruitment
Awareness of the project was generated via an advertising campaign of leaflets and flyers
which were distributed in locations within the SA community and through word of mouth
spread of information. This built on the links already established from study 1, but those who
participated in the focus group study were not recruited to avoid bias. Recruitment and
advertising sites included:
➢ Local religious centres
➢ SA community social events
➢ Local community centres
➢ Primary care
III. Trial Process
After consenting to participate in the film screening, trial participants were asked to complete
the pre-film questionnaire. Thereafter, the film was shown and the post-questionnaire issued.
After showing the film, a simple announcement mentioning an offer of testing for CVH was
made, explaining this was a finger prick blood test. Fully informed consent for blood testing
for CVH was taken in addition to the consent for viewing the film. Following NICE guidelines
[3], I utilised Dried Blood Spot testing (DBS) previously successfully used in studying viral
hepatitis in British-Chinese and British-Asian populations. DBS testing entails a sample taken
using a commercial kit that involves placing a drop of blood on a prepared card. The sample
provided will be tested for:
71
1) HCV antibody and
2) Confirmation of positive results
3) HCV RNA
4) HBV surface antigen
5) HBV core Antibody
For the feasibility study the following criteria were set as measures of success:
o Monitor patient consent, recruitment and retention rates for participants who
attend the screening of the film and who are tested to inform future design and
methodological issues.
o 40% (n=80) of participants watching the educational intervention will go on to
be tested.
o 90% of participants to see the educational intervention will complete the pre-
film questionnaire
o 80% of participants will complete the post-film questionnaire
o Feasibility of methodological procedures, including collating data relating to
patient experience of completing the questionnaires, and assessing patient
feedback
o Generate data for primary outcome measure to enable exact sample size
calculation for the main trial
IV. Regulatory Approvals
Phase 1:
REC Reference: 16/EE/0138, (proportionate ethics approval) IRAS project ID: 195901. Ethics
committee: East of England: Cambridge Central Research Ethics Committee
Phase 2:
REC reference: 17/LO/0881, IRAS project ID: 224711
National Health Service Health Research Authority. Ethics Committee: Surrey

72
CONTRIBUTIONS
For both of these studies, I was principal investigator with Professor Aftab Ala chief
Investigator. The research assistant (Ayesha Ahmed) is a South Asian migrant with both
medical and public health degrees. Co-investigators for these studies were Jane Hendy (Brunel
University Business School) and Tushna Vandrevala (Kingston University – Psychology). I
wrote both study protocols and all study information (including participant information sheets
and consent forms) as well as writing and managing ethics approval applications and
amendments.
Study one Focus Group work:
Establishing PPI/stakeholder group: Claire Kelly, Aftab Ala
Identification of community sites: Claire Kelly, Ayesha Ahmed, Aftab Ala
Visits to community leaders and sites: Claire Kelly, Ayesha Ahmed
Focus Group moderation guide: Claire Kelly, Ayesha Ahmed, Jane Hendy, Tushna Vandrevala
FG moderator: Ayesha Ahmed (to provide cultural and linguistic congruency to help the flow
of discussion).
Translation and transcription of FG discussions was done by a professional translation and
transcription service to ensure accuracy. I transcribed a FG that was performed in English.
I performed a parallel separate analysis (thematics) for this thesis alongside contributing to the
analysis by the whole research team.
Study two Feasibility Study:
Identification of community sites: Claire Kelly, Ayesha Ahmed, Aftab Ala
Advertisement of the study: Claire Kelly, Ayesha Ahmed, Aftab Ala
Visits to community leaders and sites: Claire Kelly, Ayesha Ahmed, Aftab Ala
Recruitment sessions: Claire Kelly, Ayesha Ahmed, Aftab Ala
Consent of participants: Claire Kelly
Blood Testing: Claire Kelly
Data Analysis: Claire Kelly (supervision of a statistician - Professor Skene, University of
Surrey).

73
SECTION B: STUDY 1 DEVELOPING A NOVEL EDUCATIONAL
INTERVENTION TO IMPROVE THE AWARENESS OF VIRAL
HEPATITIS IN THE SOUTH ASIAN COMMUNITY

74
CHAPTER 5: STUDY 1 METHODS

75
STUDY OVERVIEW
This was a community based study using focus groups to explore knowledge, attitudes and
barriers to testing for viral hepatitis in the South Asian community. Data gained from these
focus groups was analysed to generate broad themes, which in turn led to key messages being
identified. These key messages centred around themes generated in FG data analysis and also
served to correct common misconceptions were found in FG discussions around CVH. These
themes and messages were then used to form questions to be put to interviewees that were then
edited to develop an educational intervention (a short film) to improve uptake of testing for
chronic viral hepatitis.
AIMS
1. To report current ideas, knowledge and opinions on viral hepatitis amongst South Asian
migrants
2. To identify barriers to testing for CVH in the SA community, and more generally any
barriers and facilitators to accessing healthcare for this population
3. To identify key themes emerging from focus group data analysis to aid development of
an educational intervention (culturally and linguistically tailored film)
4. To develop a questionnaire to be complete pre- and post-educational intervention to aid
analysis of the intervention
STUDY INCLUSION AND EXCLUSION CRITERIA
Participants were recruited to the study if they met the following inclusion criteria:
1. First or Second Generation South Asian migrant (participants were classified as
South Asian based on self-identifying as such)
2. Age 18 years of age or older
3. Ability to speak English or Urdu
4. Ability to consent to participation - consent will be taken as per ICH good clinical
practice (GCP) standards.
Exclusion criteria:
1. Involvement in an earlier cohort during this phase of work (excluding those identified
in FG as having relevant stories for our film)

76
South Asian migrants were recruited as an example of a higher-risk group based on prevalence
rates in this population. The World Health Organisation (WHO) have issued a call to eliminate
chronic viral hepatitis as a public health problem by 2030 and to achieve this there must be
efforts to diagnose the hidden burden of disease. However, there has been little evidence on
effective educational interventions to promote testing of those at increased risk. As part of the
funding application (National Institute of Health Research, research for patient benefit stream
(PB-PG-1013-32094) for this work, the nature of the intervention (film) was predetermined.
This first study was split into three sections. Firstly, focus groups were run with the South
Asian migrant population to address existing knowledge and opinions on CVH and to identify
issues with barriers to testing. Secondly, analysis of this focus group data allowed generation
of themes to structure key messages that would inform the development of an educational film
and aid identification of where we can show this in study 2. Thirdly, a questionnaire that could
be used pre and post film screening was developed, based on existing validated questions to
aid the interpretation of our results.
Participants were recruited in a number of cohorts, with the assistance of stakeholder and
patient public involvement (PPI) groups to identify potential recruitment sites and strategy.
Cohort 1: These participants were recruited to focus groups which were held in community
and religious settings. These focus group discussions allowed us to identify the knowledge,
ideas, concerns and expectations of the community and use this information to develop themes
for our intervention (film).
Cohort 2: These participants were recruited to be filmed as part of the intervention
development. The participants were filmed answering a variety of questions in their own
words. These questions were formed by analysis of FG data to generate themes for
discussion. This led to many hours of recording that were then transcribed and edited in
multiple rounds to select the most powerful statements and most appropriate participant for
each message e.g. knowledge coming from experts and experiences from patients.
Cohort 3: These participants were recruited for validation of the educational intervention and
questionnaire. They did not participate in earlier stages of this study to avoid bias. They were
shown the film in its final format and also completed the pre and post film questionnaire. This

77
was to ensure both the film and questionnaire were understandable in both English and Urdu
forms and to identify any difficulties in filling out the questionnaire or in viewing the film. A
final edit of the film and the questionnaires was then completed based on this feedback.
Regulatory Approvals
This was a proportionate ethics approval (REC Reference: 16/EE/0138, IRAS project ID:
195901)
STUDY STRUCTURE
I. Cohort 1 – Focus Groups Structure
Focus groups were utilised to determine existing knowledge and attitudes to CVH and
healthcare access in the SA community. These FGs had the benefit over questionnaires and
individual interviews of allowing discussion and exchange of ideas. The role of facilitator is
key and as such was performed by a culturally and linguistically appropriate researcher.
The stakeholder and PPI groups helped identify potential recruitment sites and develop links
with community leaders to facilitate recruitment. An advertising campaign detailing the study
was launched using leaflets. The advertising material (appendix 1) was distributed to local
community centres, social events and religious venues. This provided details on the FG venues
and timings and provided contact details for participants to obtain further information. The
patient information sheets and advertising were made available in both Urdu and English.
These languages were chosen as the most commonly spoken languages from the region, as we
could not provide interpretation for all languages and dialects.
I found that participants wished to attend a particular FG based on a combination of geography,
logistics and with family/friend groups wanting to attend together. This was at odds with our
original intention to recruit participants and then divide into FGs suitable for their
demographic, with groups split by age (older and younger adults) and gender.
The focus groups themselves were held in English or Urdu/Hindi as required by participants,
who were encouraged to discuss chronic viral hepatitis and to identify knowledge and attitudes
to risk, testing, diagnosis and treatment. In order to establish freedom to speak, there was no

78
list of predetermined questions to answer, but there was a guide for the moderator to ensure
our aims were met as far as possible. This had pre-determined information to obtain and
included questions if these did not automatically come up. The guide included a statement to
be read at the start of every focus group to emphasise there is no right or wrong answer and
that all contributions are valid. The focus groups were run by a native Urdu speaker (with both
public health and medical degrees) and as we were trying to obtain information on access to
healthcare, we felt this could be more difficult with UK born doctors present. The FG guide
highlighted the following key areas to be covered if they were not naturally addressed during
the discussion:
1. Knowledge and experience of CVH
2. Access to healthcare
3. Perceived stigma of CVH
4. Severity of disease
5. Transmission
6. Treatments of CVH
The focus group discussions were audio recorded to ensure accurate transcription and where
necessary translation. Those in Urdu were professionally transcribed and translated with back
translation to ensure accuracy and were read by those fluent in both languages to ensure
accuracy.
After consenting to participate in FGs, demographic data was gathered to ensure representation
across the SA population and to see whether any subgroup analysis would affect our results
and therefore impact the development of the educational film. Specifically, data on educational
attainment, language, time spent in UK and religion were gathered (appendix 2). A particular
aim was to determine the views of women as previously this group has been underrepresented
in studies of this type.
Whilst most of the FG were conducted along gender lines, one was not at the request of the
attendees who were more comfortable with a mixed group. Initially, we planned to recruit 32-
40 participants based on one FG (estimated attendance 8-10) for each gender and age group.
This was surpassed as initial analysis revealed that young, educated men were under-
represented in the cohort and so a further FG was arranged to address this gap. This was related
79
to the FG being less structured in age as we initially planned as per participants preference
described above.
Focus group data was analysed via thematic analysis using NVivo 10 software.
II. Utilisation of Focus Groups as a Method: Strengths and Weaknesses
There are a variety of methods of data collection in qualitative research. The most common
methods used, particularly in healthcare research, are interviews and focus groups [183]. FGs
were first employed in the early 1940s in an effort to move away from interviewer-dominated
research methods [184]. A focus group is a group discussion on a particular topic organised
for research purposes. This discussion is guided, monitored and recorded by a researcher
(facilitator or moderator). They are used for generating information on collective views, and
the meanings that lie behind those views. However, they will not function well where
participants are not comfortable with each other, are unable to speak as a group (language
factors) or where statistical analysis is required [185]. The make-up of a FG needs
consideration to ensure the data collected is optimal. The nature of the discussion and the
preferences of the target population will be important factors to consider before organising a
FG discussion. This was taken into account in this study where FGs were single gender as per
participant request, except for one group where a mixed-gender group was requested. The FG
method aims to obtain data from a purposely selected group of individuals rather than from a
statistically representative sample of a broader population.
Group size is important, the optimum size for a focus group has been described as six to eight
participants, but there have been successful FGs with anywhere between 3-14 participants. In
smaller groups, discussion may be limited but conversely larger groups may be more difficult
to manage and may mean not all participants get opportunity to speak.
The venue for a focus group is important and should be accessible, comfortable, private, quiet
and free from distractions [186]. This is why we held our FG in community venues that were
known to the participants.
The role of the moderator is to facilitate group discussion, not lead it. However, they should
also ensure all participants get the opportunity to contribute and that discussion is not shaped
by a dominant participant. The moderator should be able to allow different views to be
80
exchanged and discussed and encourage participation in those who are less vocal [186]. The
facilitator is central to the discussion not only by managing existing relationships but also by
creating a relaxed and comfortable environment for unfamiliar participants (this is why we
utilised a research assistant with a medical degree and spoke Urdu as a first-generation migrant
from SA).
With regards recording of FG data outputs, videotaping will require more than one camera to
capture the whole group, as well as additional operational personnel in the room. This can be
intrusive and affect the spontaneity of the group and does not usually yield additional
information. Therefore, our FG discussions were audio recorded only.
Whilst there are multiple ways to structure FGs, I utilised the single focus group. The key
feature of a single focus group is the interactive discussion of a topic by a collection of all
participants and a team of facilitators as one group in one place. This is the most common and
classical type of focus group discussion.
The purpose of the research interview is to explore the views, experiences, beliefs and/or
motivations of individuals on specific matters and provide a deeper understanding of topics
than would be obtained from purely quantitative methods, such as questionnaires. Interviews
are, therefore, most appropriate where little is already known about the study phenomenon or
where detailed insights are required from individual participants. I utilised FGs rather than
interviews to focus on the SA group collectively and to appeal to this community in its broadest
sense. Whilst we would hear individual views, these are by their very nature variable and
potentially conflicting and the value of FG was in hearing this discussion play out in the group
to see whether a consensus was achieved and to also note the frequency of any conflicting
viewpoints. Structured interviews are, essentially, verbally administered questionnaires, in
which a list of predetermined questions are asked, with little or no variation and with no scope
for follow-up questions to responses that warrant further elaboration. Consequently, they are
relatively quick and easy to administer and may be of particular use if clarification of certain
questions is required or if there are likely to be literacy or numeracy problems with the
respondents. However, by their very nature, they only allow for limited participant responses
and are, therefore, of little use if depth is required. I did not feel this was the best model for an
exploratory study of this nature. Unstructured interviews do not reflect any preconceived
theories or ideas and are performed with little or no organisation. Unstructured interviews are
81
usually very time-consuming (often lasting several hours) and can be difficult to manage and
to participate in, as the lack of predetermined interview questions provides little guidance on
what to discuss. However, given the number of participants to include and the comfort the
community took from meeting in groups it was felt this was not feasible.
Focus groups are particularly useful when there are power differences between the participants
and decision-makers or professionals, when the everyday use of language and culture of
particular groups is of interest, and to explore the degree of consensus on a topic [187].
Although focus group research has many advantages there are limitations. Some can be
overcome by moderating, but others are unavoidable and particular to the nature of this method
of data collection. The moderator must allow participants to interact and ask questions to keep
the conversation focussed on the topic without leading or controlling the discussion.
Additionally, participants are self-selected and study results are therefore harder to generalise
to the population as a whole [188]. Focus groups can be difficult to assemble, and this can
make getting a representative sample more difficult. There are certain groups who are less
likely to participate, such as those who are not confident, and those who have communication
or language problems. Finally, focus groups are not fully confidential or anonymous, because
the material is shared with the others in the group.
The principle of theoretical saturation, where focus group discussion sessions are run until a
clear pattern emerges and subsequent groups produce no new information has been applied in
most types of FG studies [189]. This is the technique used in this study.
III. Cohort 2 - Educational Intervention development
Focus group data was analysed to generate key themes. These themes formed the basis of the
questions to be put to each person being filmed. Prior to running the focus groups, it was
hypothesised that the film would feature the following categories:
1. Ease of testing
2. Patient story: Diagnosed positive and cured
3. Patient story: Diagnosed positive and on treatment
4. Physician explanation of CVH and the treatment process

82
However, this planned structure was modified after analysis of the results of our FG discussions
revealed there was significantly less knowledge on CVH than predicted (see chapter 8 for
further detail on the film production). Initially, it was expected that recruitment for the film
would come from FG participants. However, given there was less experience of CVH than
expected this was not possible. Additionally, feedback from the community suggested that it
was preferable to have cultural and linguistic congruity with the SA community and to be
identifiable as such. Therefore, an ethics amendment to recruit from our Hepatology clinic in
the Royal Surrey County Hospital was made. The aim of including those who tested negative
in our film was to give information and reassurance on the process of testing. Suitable patients
were approached and we recruited a patient who was treated for hepatitis C and cured, a liver
transplant recipient and a community leader who had previously been tested and was negative.
Two SA physicians (one male, one female) who are hepatology experts were also recruited.
These were recruited based on feedback from the FGs and also our stakeholder group.
In order to develop and produce the educational film, a professional filmmaker with healthcare
experience was hired. He was able to advise on technical aspects of the film production and
how to edit the story line.
Each film participant was recorded answering a series of questions. The two medical experts
(one SA male, one SA female) were asked the same questions. These were on knowledge,
access, the testing and treatment process. This focussed on correcting misconceptions seen in
the FG work The patient participants were asked to outline their experiences. Specific
questions were then asked of all participants to ensure all aspects of our messages were
covered. The question and answer format was advised by the film producer as it was felt this
would appear more natural and conversational than asking participants to read a set text. It was
also felt important that the participants own words came across particularly for the patients.
The film producer determined the ideal locations for the filming of both lay participants and
experts. Given the nature of the intervention, participants were filmed in a variety of
community settings to avoid the film appearing as a series of interviews.
The language of the film was the subject of discussion with the community, the researchers,
stakeholder and PPI groups, and we decided to incorporate this question into our focus group
discussions. It was felt both English and Urdu versions should be available.
83
Once each participant had been interviewed on film, there were seven hours of recording. The
content was then transcribed as this allowed all statements to be categorised into one of the
five key themes from the FG data. These were then further sub-categorised into individual
messages. We then decided which message gave the most powerful content (both from the
point of view of content and person delivering the message) and this was then highlighted as a
section of interest to the film producer. This led to a first draft of film containing key messages.
This was reviewed to ensure participants participated equally and all previously highlighted
messages were included. This first draft was long (over 30 minutes) and so was edited again
twice using the process above. The film producer then used his expertise in fillers and artistic
work to generate the final version to be validated.
The following represents a summary of the key steps in producing the educational film
intervention:
1. Story line development from analysed FG data and generation of questions for each
participant
2. Identification of filming sites for each participant
3. Recording and transcription of the interviews of film participants
4. Scene selection
5. Editing process- transcription and translation
6. Editing first round to summarise content and maximise impact of key messages
7. Editing second round
8. Fillers and artistic work on the advice of the film producer
9. Final version showed to participants as part of the consent process
IV. Questionnaire Development
A questionnaire was used to facilitate assessment of the utility of the film. This was self-
administered before and after viewing the film. The questionnaire was designed with a 5-point
Likert scale from strongly agree, agree, neither agree nor disagree, disagree and strongly
disagree. It was based on existing validated questionnaires where possible. Additional
questions around utility of the film, intention to test and knowledge on CVH specific factors
were designed by me. For ease of administration the same questionnaire was used pre and post
film. Individual questions were combined into broad categories reflecting attitudes of the
participants to health and health care; knowledge of chronic viral hepatitis; stigma;
84
transmission and infection with CVH; utility of the study intervention and processes;
experience of CVH; factors influencing testing and intention to test.
The knowledge domain was included after realising there was less awareness of CVH than
anticipated. Attitudes to health and healthcare helped us to understand how empowered the
community felt about their healthcare needs and intention would let us know if people were
already considering testing for CVH independently of the film. Stigma was included to be sure
the film addressed any concerns in this regard. Additionally, a free text box for comments was
included for any additional feedback.
V. Validation
A new group of people (n=5) who had not participated in this study before (to avoid bias) were
shown the film in its final format. This was to establish whether the film could be understood
and to gather feedback on its content prior to final edits. Each participant was recruited serially
and shown the film individually and feedback gained. By the time the fifth participant was
recruited there was no new opinions and all five participants agreed. Therefore, it was felt
feedback was saturated and no further recruitment was made. The film was further refined on
the basis of common themes in their feedback, namely that the film was too long, the Urdu
used was too formal and so less likely to be understood in all communities and sound issues
were corrected. Two versions of the film were ultimately produced one English, one Urdu.
As part of the validation, these participants also reviewed the pre and post film questionnaires.
This allowed me to refine the questions and ensure validity across languages (they were
reviewed in both English and Urdu forms). The Urdu questionnaire was back translated to
assess for accuracy and ease of understanding. The main issues encountered were formatting
based with some questions not suitable for the 5-point Likert scale and these questions were
therefore re-formatted. Again, the Urdu was noted to be too formal and so was edited to a more
colloquial form for all participants to understand.
DATA ANALYSIS
Focus groups were audio recorded. Each group recording was then transcribed and translated
where required. Where this was the case, back-translation was also performed to ensure
accuracy of meaning e.g. idioms were encapsulated.
85
This is a qualitative study; therefore, I conducted thematic analysis to generate salient themes
from the focus group discussions. Thematic analysis (TA) is a type of qualitative analysis
where patterns, or themes, are identified within data. It is flexible because it is not related to a
particular theoretical framework. Thematic analysis is particularly useful to examine people’s
experiences, views and perceptions as well as questions related to understanding and
representation. There are different ways TA can be approached, I used an inductive method
where coding and theme development are directed by the content of the data as this seemed
most appropriate to the nature of this work. However, the flexibility of TA can be considered
a weakness as it may be used as a way to summarise data rather than provide true analysis.
This has led to the generation of a six-step framework to provide a clear guidance through the
process of the key point of thematic analysis; to identify patterns in the data (themes) and to
use these to address the research question [190].
Step 1: Become familiar with the data
The first step in any qualitative analysis is reading and re-reading the transcripts to become
familiar with the entire data. This aids in later generation of codes.
Step 2: Generate Initial Codes
This phase involves the systematic organisation of the data. Coding is a key feature of this
stage and reduces the volume of data into smaller categories. Whilst coding can be done in
various ways, I used open coding that means I did not have pre-set codes but developed and
modified the codes as I worked through the coding process. I developed initial ideas about
codes when I finished Step 1.
Whilst a theme captures a common, recurring pattern across a dataset, codes tend to be more
specific, capturing a single idea that is of interest in relation to the research question. Related
codes are later combined together to create themes. Coding is flexible and continues to evolve
as analysis proceeds. There is no correct way to code and as such no reason to employ methods
relating to inter-rater reliability.
Step 3: Search for Themes
A theme is a recurring pattern or message that represents something significant from the
generated data and codes and/or the research question. By the end of this stage, the codes
86
should be captured into themes. It is, however, possible to generate miscellaneous themes for
codes that do not fit together or into the other themes. This can then be reviewed at the
following stages.
Step 4: Review themes
This stage involves the review, modification and development of the preliminary themes. The
data associated with each theme is reviewed to ensure the data does support the theme.
Thereafter, the themes themselves are reviewed as to ensure they represent distinct areas but
fit overall in the data. The frequency of themes may also be relevant in the analysis and so can
be noted.
Step 5: Define themes
This is the final refinement of the themes, and the aim is to determine the nature of each theme,
how themes relate to each other and what the core message of each theme is.
Step 6: Write Up
Whilst TA has many benefits, particularly in the context of this study, it is recognised that there
are potential weaknesses in its use. Use of the questions of the interview or focus group as
themes, having inappropriate themes in number (too many or too few) or in content (too much
overlap between themes or themes were content is not related) are recognised weaknesses.
Additionally, there can be a discrepancy between data and analysis, with either too many or
too few extracts to support analytic claims or failing to provide analysis and using a summary
from extracts. Each theme should be distinct and clear whilst all themes come together to
encapsulate the data obtained.
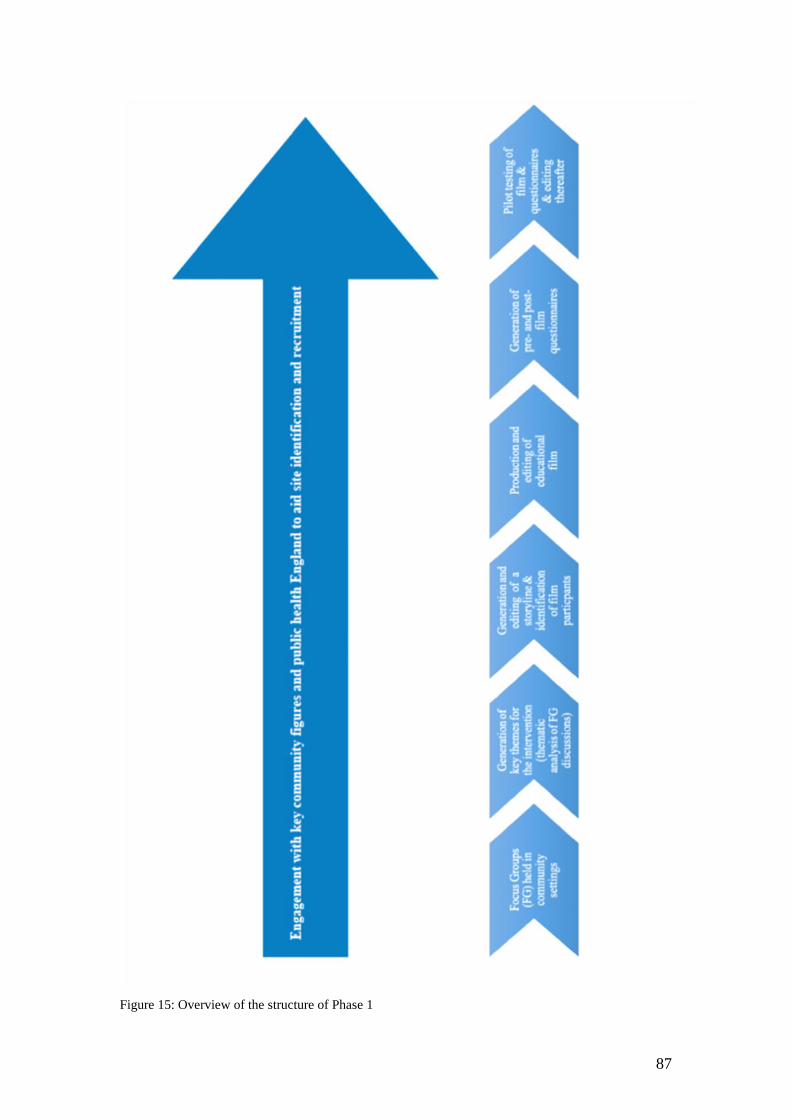
87
Figure 15: Overview of the structure of Phase 1
88
CHAPTER 6: FOCUS GROUP RESULTS
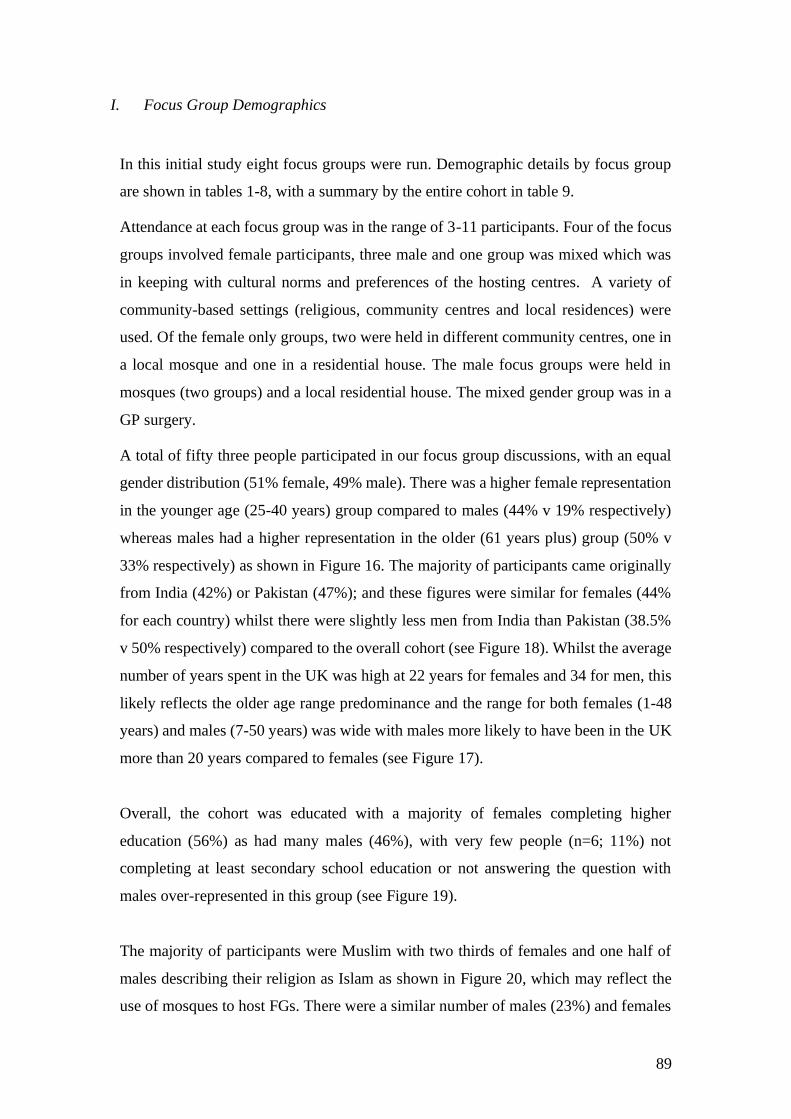
89
I. Focus Group Demographics
In this initial study eight focus groups were run. Demographic details by focus group
are shown in tables 1-8, with a summary by the entire cohort in table 9.
Attendance at each focus group was in the range of 3-11 participants. Four of the focus
groups involved female participants, three male and one group was mixed which was
in keeping with cultural norms and preferences of the hosting centres. A variety of
community-based settings (religious, community centres and local residences) were
used. Of the female only groups, two were held in different community centres, one in
a local mosque and one in a residential house. The male focus groups were held in
mosques (two groups) and a local residential house. The mixed gender group was in a
GP surgery.
A total of fifty three people participated in our focus group discussions, with an equal
gender distribution (51% female, 49% male). There was a higher female representation
in the younger age (25-40 years) group compared to males (44% v 19% respectively)
whereas males had a higher representation in the older (61 years plus) group (50% v
33% respectively) as shown in Figure 16. The majority of participants came originally
from India (42%) or Pakistan (47%); and these figures were similar for females (44%
for each country) whilst there were slightly less men from India than Pakistan (38.5%
v 50% respectively) compared to the overall cohort (see Figure 18). Whilst the average
number of years spent in the UK was high at 22 years for females and 34 for men, this
likely reflects the older age range predominance and the range for both females (1-48
years) and males (7-50 years) was wide with males more likely to have been in the UK
more than 20 years compared to females (see Figure 17).
Overall, the cohort was educated with a majority of females completing higher
education (56%) as had many males (46%), with very few people (n=6; 11%) not
completing at least secondary school education or not answering the question with
males over-represented in this group (see Figure 19).
The majority of participants were Muslim with two thirds of females and one half of
males describing their religion as Islam as shown in Figure 20, which may reflect the
use of mosques to host FGs. There were a similar number of males (23%) and females
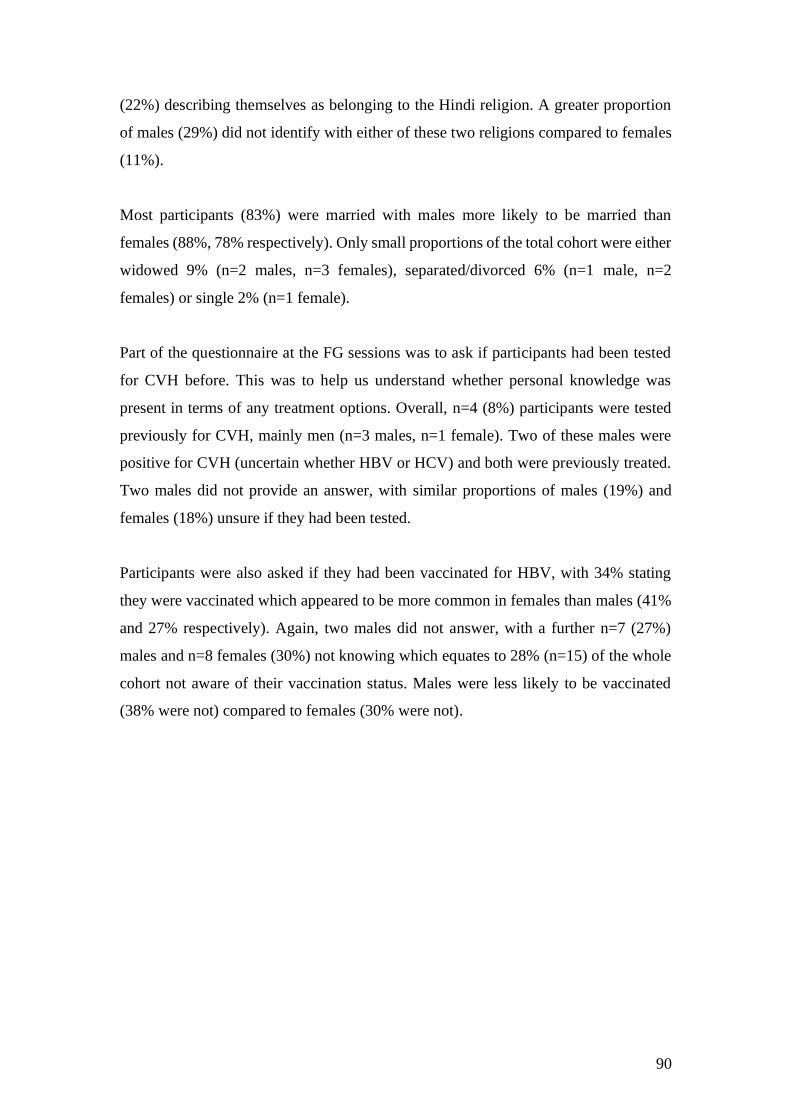
90
(22%) describing themselves as belonging to the Hindi religion. A greater proportion
of males (29%) did not identify with either of these two religions compared to females
(11%).
Most participants (83%) were married with males more likely to be married than
females (88%, 78% respectively). Only small proportions of the total cohort were either
widowed 9% (n=2 males, n=3 females), separated/divorced 6% (n=1 male, n=2
females) or single 2% (n=1 female).
Part of the questionnaire at the FG sessions was to ask if participants had been tested
for CVH before. This was to help us understand whether personal knowledge was
present in terms of any treatment options. Overall, n=4 (8%) participants were tested
previously for CVH, mainly men (n=3 males, n=1 female). Two of these males were
positive for CVH (uncertain whether HBV or HCV) and both were previously treated.
Two males did not provide an answer, with similar proportions of males (19%) and
females (18%) unsure if they had been tested.
Participants were also asked if they had been vaccinated for HBV, with 34% stating
they were vaccinated which appeared to be more common in females than males (41%
and 27% respectively). Again, two males did not answer, with a further n=7 (27%)
males and n=8 females (30%) not knowing which equates to 28% (n=15) of the whole
cohort not aware of their vaccination status. Males were less likely to be vaccinated
(38% were not) compared to females (30% were not).

91
Figure 16: Focus Group participants by age and gender
Figure 17: Number of years focus group participants have spent living in the UK
Other refers to missing data point
60 40 20 0 20 40 60
25-40
41-50
51-60
61+
% of attendees
Age
Ran
ge
Focus Group Participants by Age
Females Males
60 40 20 0 20 40 60 80
<5 years
5-10 years
11-20 years
>20 years
Other
% of attendees
Focus Group Participants Years in UK
Females Males
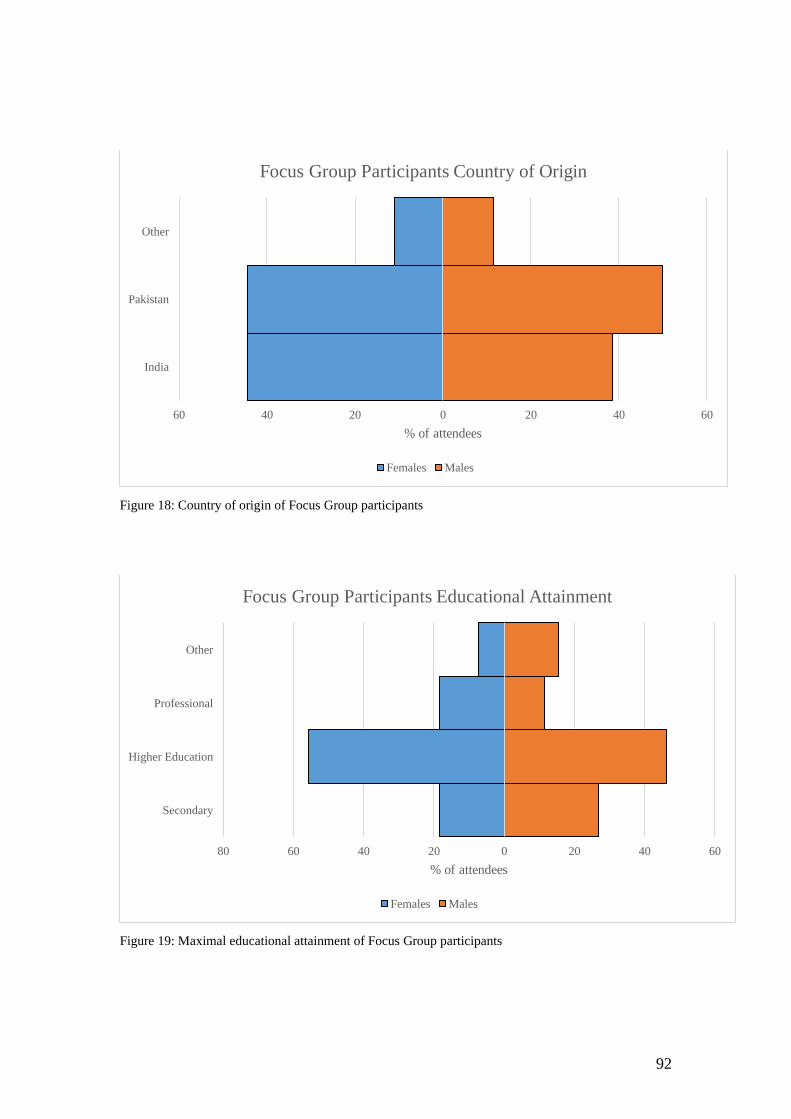
92
Figure 18: Country of origin of Focus Group participants
Figure 19: Maximal educational attainment of Focus Group participants
60 40 20 0 20 40 60
India
Pakistan
Other
% of attendees
Focus Group Participants Country of Origin
Females Males
80 60 40 20 0 20 40 60
Secondary
Higher Education
Professional
Other
% of attendees
Focus Group Participants Educational Attainment
Females Males
93
Figure 20: Religious belief of Focus Group participants
80 60 40 20 0 20 40 60
Islam
Hindu
Other
% of attendees
Focus Group Participants Religion
Females Males
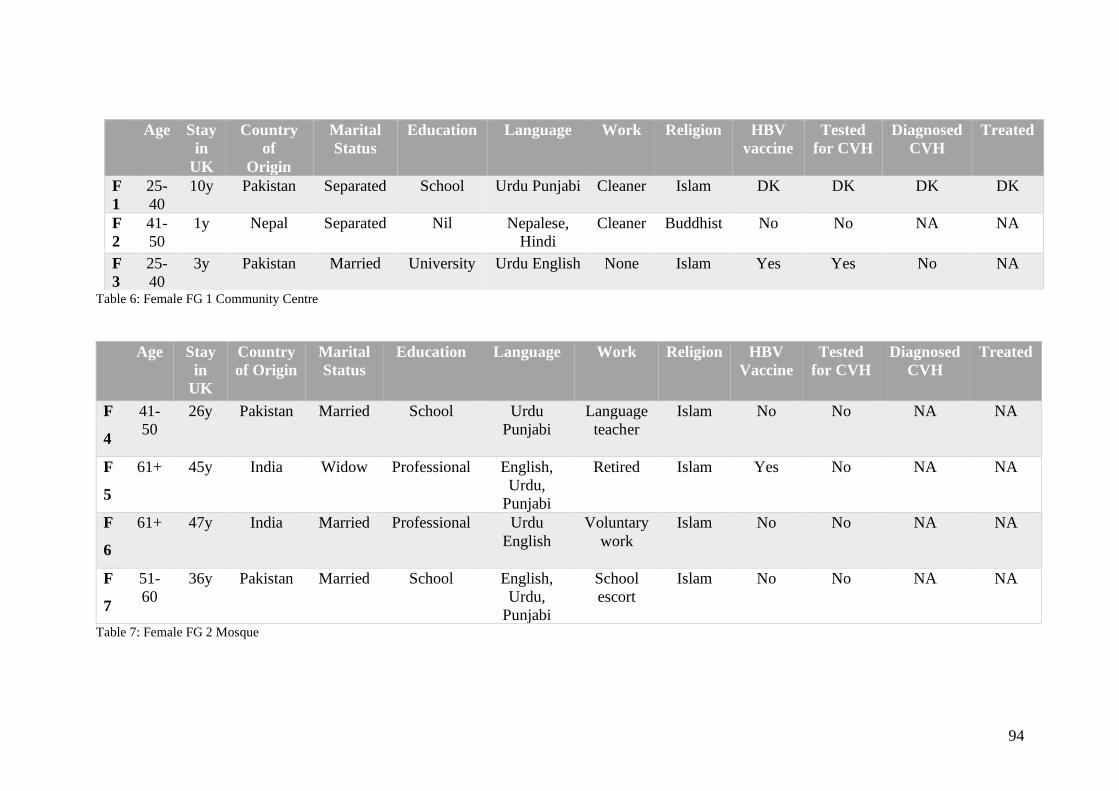
94
Table 6: Female FG 1 Community Centre
Age Stay
in
UK
Country
of Origin
Marital
Status
Education Language Work Religion HBV
Vaccine
Tested
for CVH
Diagnosed
CVH
Treated
F
4
41-
50
26y Pakistan Married School Urdu
Punjabi
Language
teacher
Islam No No NA NA
F
5
61+ 45y India Widow Professional English,
Urdu,
Punjabi
Retired Islam Yes No NA NA
F
6
61+ 47y India Married Professional Urdu
English
Voluntary
work
Islam No No NA NA
F
7
51-
60
36y Pakistan Married School English,
Urdu,
Punjabi
School
escort
Islam No No NA NA
Table 7: Female FG 2 Mosque
Age Stay
in
UK
Country
of
Origin
Marital
Status
Education Language Work Religion HBV
vaccine
Tested
for CVH
Diagnosed
CVH
Treated
F
1
25-
40
10y Pakistan Separated School Urdu Punjabi Cleaner Islam DK DK DK DK
F
2
41-
50
1y Nepal Separated Nil Nepalese,
Hindi
Cleaner Buddhist No No NA NA
F
3
25-
40
3y Pakistan Married University Urdu English None Islam Yes Yes No NA
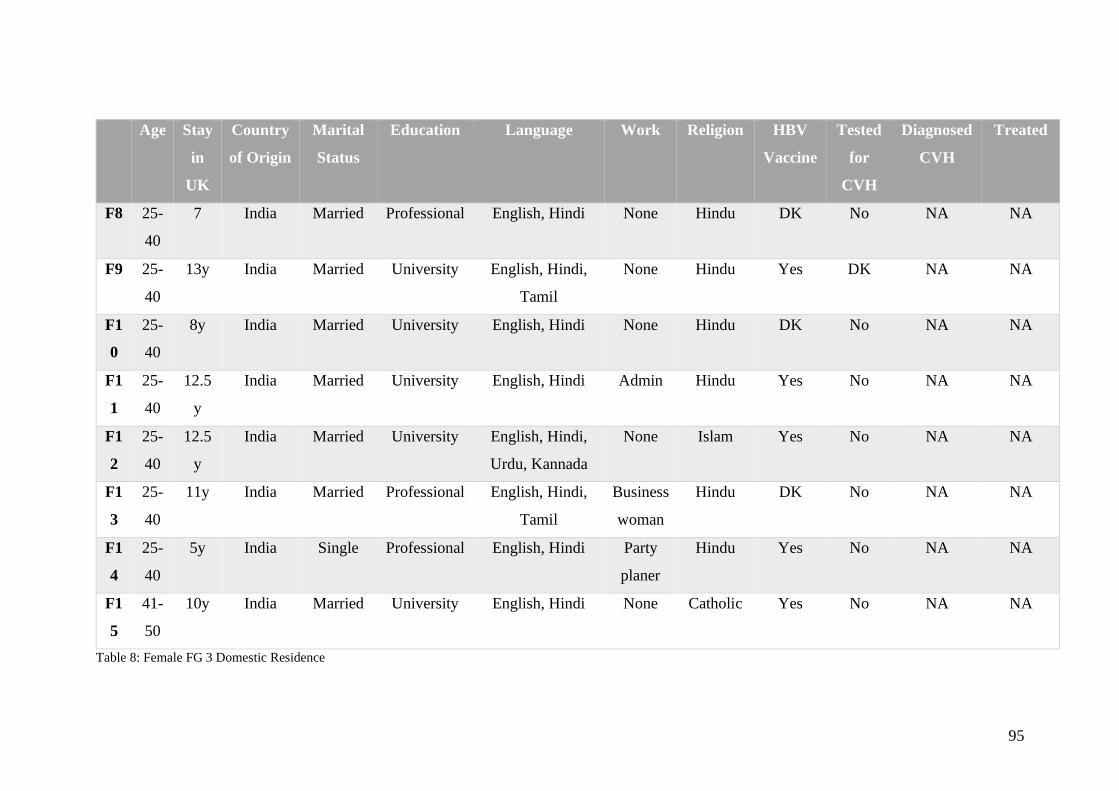
95
Age Stay
in
UK
Country
of Origin
Marital
Status
Education Language Work Religion HBV
Vaccine
Tested
for
CVH
Diagnosed
CVH
Treated
F8 25-
40
7 India Married Professional English, Hindi None Hindu DK No NA NA
F9 25-
40
13y India Married University English, Hindi,
Tamil
None Hindu Yes DK NA NA
F1
0
25-
40
8y India Married University English, Hindi None Hindu DK No NA NA
F1
1
25-
40
12.5
y
India Married University English, Hindi Admin Hindu Yes No NA NA
F1
2
25-
40
12.5
y
India Married University English, Hindi,
Urdu, Kannada
None Islam Yes No NA NA
F1
3
25-
40
11y India Married Professional English, Hindi,
Tamil
Business
woman
Hindu DK No NA NA
F1
4
25-
40
5y India Single Professional English, Hindi Party
planer
Hindu Yes No NA NA
F1
5
41-
50
10y India Married University English, Hindi None Catholic Yes No NA NA
Table 8: Female FG 3 Domestic Residence
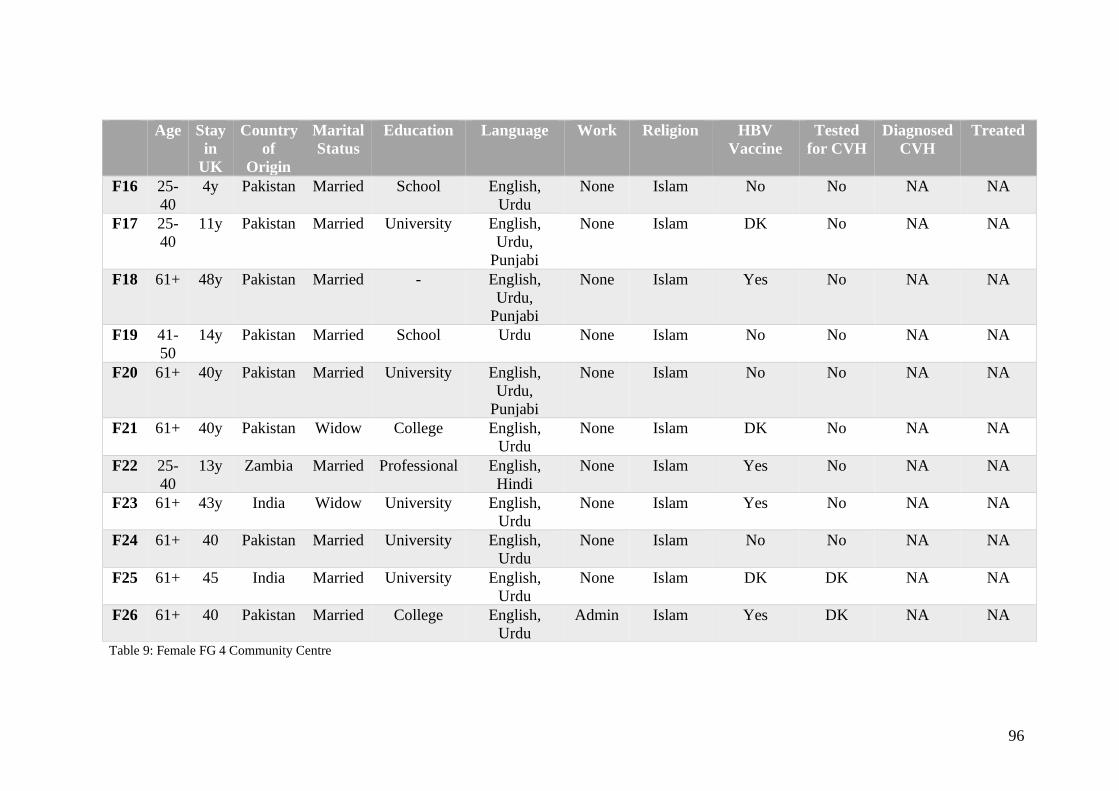
96
Table 9: Female FG 4 Community Centre
Age Stay
in
UK
Country
of
Origin
Marital
Status
Education Language Work Religion HBV
Vaccine
Tested
for CVH
Diagnosed
CVH
Treated
F16 25-
40
4y Pakistan Married School English,
Urdu
None Islam No No NA NA
F17 25-
40
11y Pakistan Married University English,
Urdu,
Punjabi
None Islam DK No NA NA
F18 61+ 48y Pakistan Married - English,
Urdu,
Punjabi
None Islam Yes No NA NA
F19 41-
50
14y Pakistan Married School Urdu None Islam No No NA NA
F20 61+ 40y Pakistan Married University English,
Urdu,
Punjabi
None Islam No No NA NA
F21 61+ 40y Pakistan Widow College English,
Urdu
None Islam DK No NA NA
F22 25-
40
13y Zambia Married Professional English,
Hindi
None Islam Yes No NA NA
F23 61+ 43y India Widow University English,
Urdu
None Islam Yes No NA NA
F24 61+ 40 Pakistan Married University English,
Urdu
None Islam No No NA NA
F25 61+ 45 India Married University English,
Urdu
None Islam DK DK NA NA
F26 61+ 40 Pakistan Married College English,
Urdu
Admin Islam Yes DK NA NA
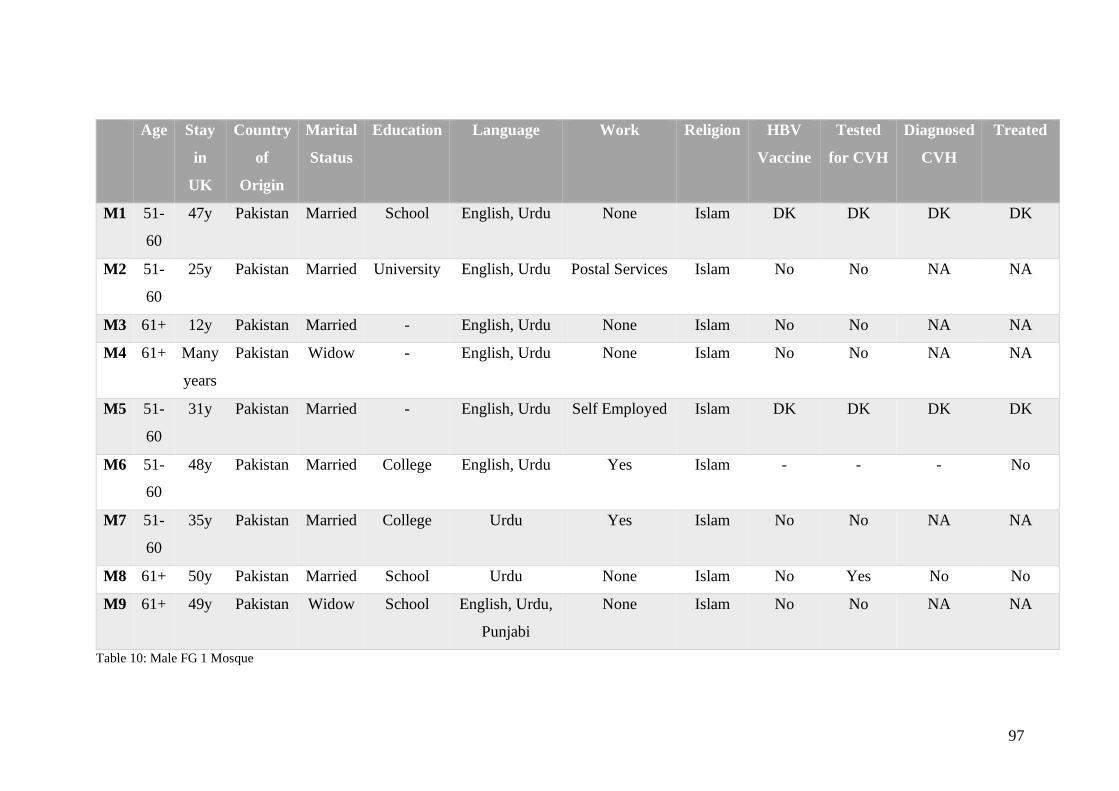
97
Age Stay
in
UK
Country
of
Origin
Marital
Status
Education Language Work Religion HBV
Vaccine
Tested
for CVH
Diagnosed
CVH
Treated
M1 51-
60
47y Pakistan Married School English, Urdu None Islam DK DK DK DK
M2 51-
60
25y Pakistan Married University English, Urdu Postal Services Islam No No NA NA
M3 61+ 12y Pakistan Married - English, Urdu None Islam No No NA NA
M4 61+ Many
years
Pakistan Widow - English, Urdu None Islam No No NA NA
M5 51-
60
31y Pakistan Married - English, Urdu Self Employed Islam DK DK DK DK
M6 51-
60
48y Pakistan Married College English, Urdu Yes Islam - - - No
M7 51-
60
35y Pakistan Married College Urdu Yes Islam No No NA NA
M8 61+ 50y Pakistan Married School Urdu None Islam No Yes No No
M9 61+ 49y Pakistan Widow School English, Urdu,
Punjabi
None Islam No No NA NA
Table 10: Male FG 1 Mosque
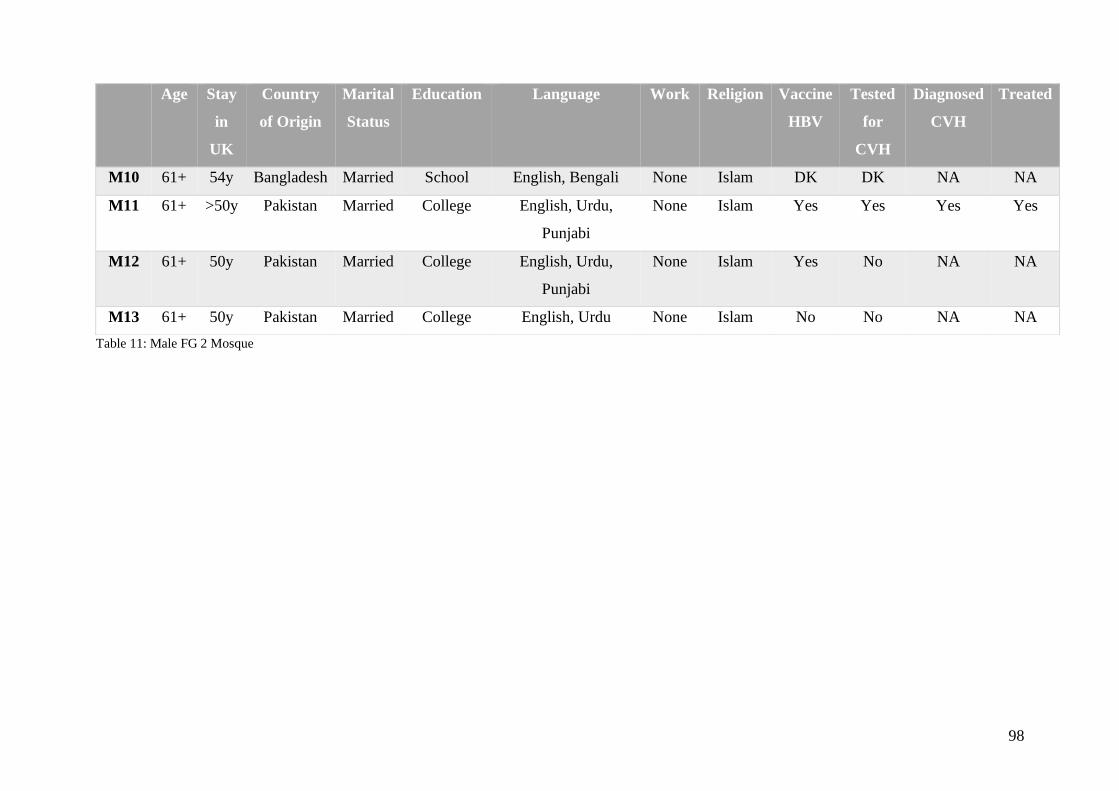
98
Table 11: Male FG 2 Mosque
Age Stay
in
UK
Country
of Origin
Marital
Status
Education Language Work Religion Vaccine
HBV
Tested
for
CVH
Diagnosed
CVH
Treated
M10 61+ 54y Bangladesh Married School English, Bengali None Islam DK DK NA NA
M11 61+ >50y Pakistan Married College English, Urdu,
Punjabi
None Islam Yes Yes Yes Yes
M12 61+ 50y Pakistan Married College English, Urdu,
Punjabi
None Islam Yes No NA NA
M13 61+ 50y Pakistan Married College English, Urdu None Islam No No NA NA
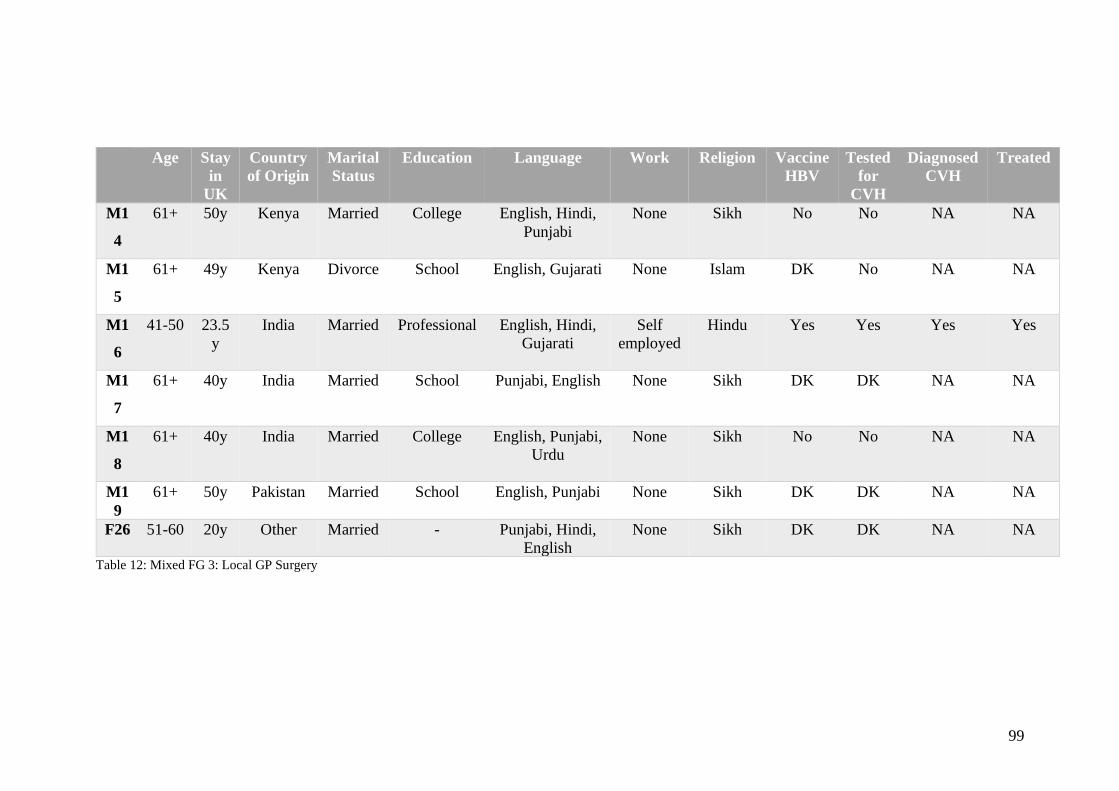
99
Age Stay
in
UK
Country
of Origin
Marital
Status
Education Language Work Religion Vaccine
HBV
Tested
for
CVH
Diagnosed
CVH
Treated
M1
4
61+ 50y Kenya Married College English, Hindi,
Punjabi
None Sikh No No NA NA
M1
5
61+ 49y Kenya Divorce School English, Gujarati None Islam DK No NA NA
M1
6
41-50 23.5
y
India Married Professional English, Hindi,
Gujarati
Self
employed
Hindu Yes Yes Yes Yes
M1
7
61+ 40y India Married School Punjabi, English None Sikh DK DK NA NA
M1
8
61+ 40y India Married College English, Punjabi,
Urdu
None Sikh No No NA NA
M1
9
61+ 50y Pakistan Married School English, Punjabi None Sikh DK DK NA NA
F26 51-60 20y Other Married - Punjabi, Hindi,
English
None Sikh DK DK NA NA
Table 12: Mixed FG 3: Local GP Surgery

100
Age Stay
in
UK
Country
of
Origin
Marita
l Status
Education Language Work Religion Vaccine
HBV
Tested
for
CVH
Diagnosed
CVH
Treated
M2
0
25-
40
1y India Married Professional English, Hindi Investment
Banker
Jainism Yes No NA NA
M2
1
41-
50
11y India Married University English, Hindi,
Gujarati
Software
developer
Hindu Yes No NA NA
M2
2
41-
50
13.5
y
India Married University English, Hindi,
Bengali
IT
Consultant
Hindu DK No NA NA
M2
3
25-
40
7-8m India Married University English, Hindi,
Bengali
IT Manager Hindu Yes No NA NA
M2
4
25-
40
12y India Married University English, Hindi,
Odia
Banker Hindu Yes No NA NA
M2
5
25-
40
11y India Married Professional English, Hindi, Business
Consultant
Hindu No No NA NA
M2
6
25-
40
- India Married - - - - - - - NA
Table 13: Male FG3: Local Domestic Residence
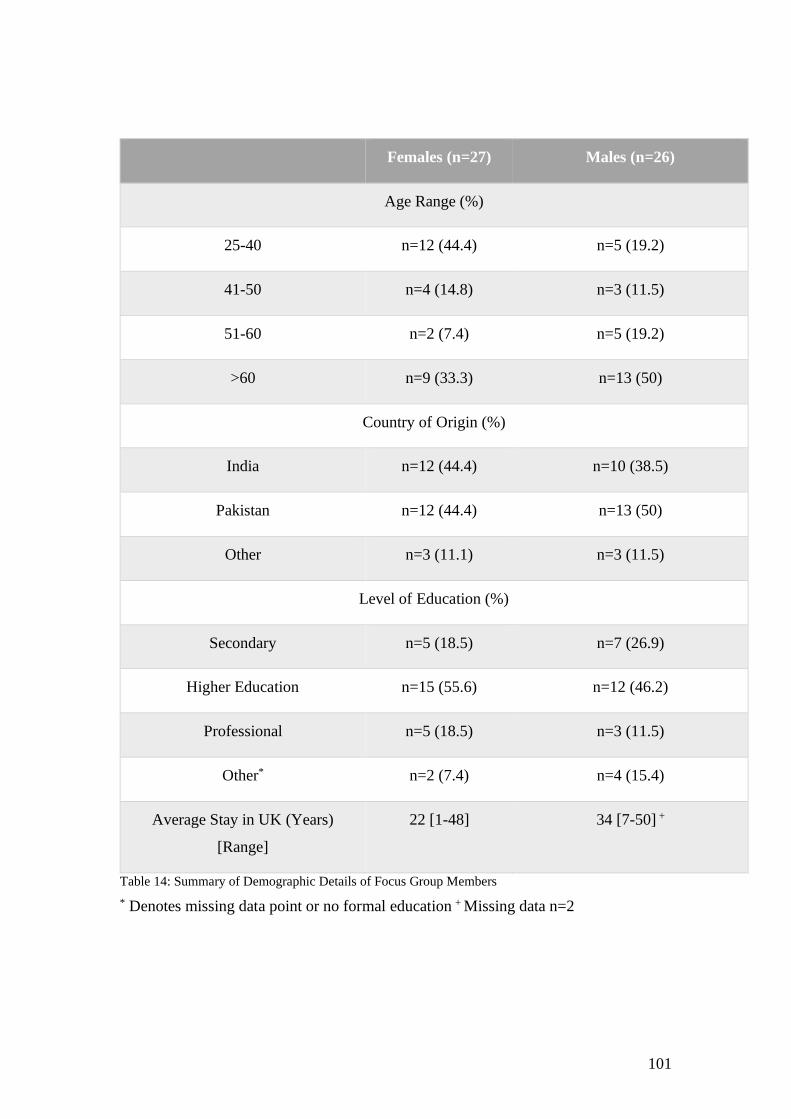
101
Females (n=27) Males (n=26)
Age Range (%)
25-40 n=12 (44.4) n=5 (19.2)
41-50 n=4 (14.8) n=3 (11.5)
51-60 n=2 (7.4) n=5 (19.2)
>60 n=9 (33.3) n=13 (50)
Country of Origin (%)
India n=12 (44.4) n=10 (38.5)
Pakistan n=12 (44.4) n=13 (50)
Other n=3 (11.1) n=3 (11.5)
Level of Education (%)
Secondary n=5 (18.5) n=7 (26.9)
Higher Education n=15 (55.6) n=12 (46.2)
Professional n=5 (18.5) n=3 (11.5)
Other* n=2 (7.4) n=4 (15.4)
Average Stay in UK (Years)
[Range]
22 [1-48] 34 [7-50] +
Table 14: Summary of Demographic Details of Focus Group Members
* Denotes missing data point or no formal education + Missing data n=2

102
II. Focus Group Discussion Results
The focus group transcriptions were analysed using Thematic Analysis, aided by
NVivo10 software. Whilst the initial aim was to discover what was already known on
CVH, it was apparent there was no real knowledge. Instead, analysis led to the
emergence of five themes: lack of awareness of CVH; testing (testing processes -
logistics and identifying those most likely to benefit from testing); access to healthcare;
attitude to health and stigma. An overview of the findings is shown in Figure 21.
Figure 21: Main themes emerging from FG discussions

103
Each theme is explored in more detail below:
a. Lack of awareness:
Prior to commencing the focus groups, it was hypothesised there would be knowledge
within the community on viral hepatitis and we aimed to determine the level of existing
knowledge and identify the gaps in this knowledge. It was noted there was less
knowledge than expected.
Those who attended the FGs often described a complete lack of awareness of hepatitis
For me I don’t know anything of hepatitis.
Members of the community itself felt general knowledge of hepatitis was not high,
Maybe my perception is wrong, but I feel its low (hepatitis knowledge) in the
scale of 1 to 10 its two or three
and this was consistent across all focus groups of both genders and the spectrum of age
ranges. There was also a lack of awareness that hepatitis was a problem of the liver
Educated people may know the name hepatitis but they don’t know what it is,
like it’s going to impact my liver
And indeed, there was the perhaps common misconception that liver disease was
associated with alcohol
I think people don’t realise; they associate liver problems with alcohol
Whilst the term hepatitis is something people have heard of, they but did not have
understanding of what this is
I don’t know anything this is the first time I am hearing it…. I mean I have heard
but I don’t know what it is and what its symptoms are and how you get it
As well as the potential implications, relating to the possible severity of hepatitis
I think we still don’t know what hepatitis is and if its serious
There was a lack of understanding how hepatitis is transmitted amongst people
I think the problem in our countries is due to lack of awareness about this
condition. They don’t know as to how this disease can spread. I think the
community doesn’t have much awareness of it

104
There were some people with some knowledge of CVH, generally though personal
experience but again this was often confused with other forms of hepatitis or jaundice
There are two types of jaundice. One is hepatitis A which is also called yellow
jaundice and there is the other more dangerous one that leaves the patient with
no choice but to die.
There was particular confusion seen with reference to contaminated water
It is an infection of the liver, it is viral, it is contagious. I believe it has something
to do with water, through drinking water
As well as dietary restrictions
My friend’s son in law he had it, so he was strict in his diet… I mean eating a
lot of fish and whatever the doctor told him. But things like bread and rice you
cannot eat them.
This was further developed in that there was a widespread belief that poor sanitation
generally was responsible
It is more common in places with poor hygiene and in those countries where
there is a lack of clean drinking water
And as such CVH is not a problem of note in the UK
Never heard of it here (UK) unless somebody comes and brings it in with them
It was felt that lack of hepatitis awareness was not seen in other conditions felt more
common in SA
People know a thing or two about other diseases such as diabetes or blood
pressure but there is little awareness about this disease.
Many participants did not find the lack of awareness of CVH surprising, feeling that
generally, people are only informed of diseases when they have personal experience
People try to get information about a disease when they get it. They won’t go
around asking about it when they haven’t got it.
Some people took the general lack of awareness in their community
I think there is absolutely no awareness of this disease in our community
to mean that it was less likely to be prevalent in SA people, as they felt if it was

105
common, they would likely have heard of it
God forbid, this disease is not very common in our community and if it is I am
not sure I am aware of it.
There was a lack awareness that CVH was a public health burden for their community,
I think it’s more in our countries, but I think it is everywhere
particularly here in the U.K
I mean we have been living in this country fifty years right and I don’t think
anything is to do with hepatitis in this country
but this was unsurprising given the confusion between other forms of hepatitis and
jaundice and the association with uncleanliness
They can bring the disease into this country otherwise there are no chances to
pick up the disease in this country.
This confusion with other forms of hepatitis particularly with faeco-oral spread
hepatitis (Hepatitis A and Hepatitis E)
About hepatitis I don’t know much. Someone said that it happens after drinking
dirty water, eating bad food
was widespread and seen in all focus group discussions, even in those with personal
experience
I know hepatitis is through contaminated water or the food.
Also, confusion with jaundice more generally was noted but even then, the perceived
link to poor sanitation was evident
In India there is a lot of jaundice, but I didn’t know that is connected to hepatitis,
especially a lot with poor food and cleanliness
and it was not always clear the distinction between liver disease, hepatitis more
generally and jaundice was understood even when participants aimed to address this
directly
I think, in India, more than hepatitis, what I personally have come across might
be the word jaundice.
The misunderstanding relating to how hepatitis is spread was felt to be a source of
106
concern for some within the community
They don’t know that unless body fluids are mixed, they can’t contract this
disease. But what happens is that they want to avoid the patient because they
think they can catch it by interacting with them
and the association with poor hygiene reinforced an association with poverty and with
CVH being a problem in countries with perceived poorer sanitation and poorer areas
Uncleanliness causes hepatitis so poor countries with less cleanliness are likely
to have more chances of having more people with hepatitis. There are less
chances of it here.
However, there were some with some personal experience who did understand
transmission
It’s not through the air, it’s not contagious it’s like body contact and body fluid
that’s how we contract this hepatitis A, B or C
As well as some without personal experience but who had some understanding
I think that if you have a cut, you should be careful that their blood doesn’t
touch you.
It was felt the term hepatitis was not really recognised as a liver problem, but was a
broad term relating to poor sanitation
Hepatitis means using such things which could be harmful to your health. It
means not caring about your health, like, not keeping your dishes and utensils
and brushes clean and these things can cause hepatitis.
and associated as a marker of poverty
Its most common in poor communities. The reason being that clean drinking
water is not available which is very essential for life.
Furthermore, even where there is understanding there was also some misinformation
At times, not in this country, but in Pakistan we have seen people going to the
barber to get the haircut and to get a shave. The barber’s blade or razor can
cause this. And it can be spread through sharing the same injecting needles.
Maybe I am wrong but also sharing the toilet with a person suffering with
hepatitis

107
When discussing symptoms, there was some understanding of features of liver disease
Sometimes the symptoms are either the skin, you lose weight, plus your eyes,
they go yellow
as well as some recognition of the potentially silent nature of liver disease and hepatitis
specifically
I don’t know, I remember reading somewhere that it can be, you know, that you
have no symptoms, and you still have
There was a realisation that travel may increase risk of infection, but again this was felt
due to sanitation
South Asian communities are more at risk because if I talk of people of my age
and similar, they travel to their countries of origin and consume food and drinks
that could be contaminated
but also people did have an understanding of previous problems with healthcare
practices that were responsible for CVH transmission
You know in bygone days they would use the same syringe to give injections to
different people
Which was mentioned in more than one FG
Injections in Pakistan they use the same syringe, for different patients its
affected by that.
Also, there was recognition of the risks from other medical services such as dentistry
which many people describe having when they travel home due to cost restraints here
and felt able to enquire about the safety of equipment
When I went to the dentist I asked him did you sterilise that
but some misunderstanding about spread person to person
If you live with someone, in a joint family system you can get it.
However, some information did come from awareness of news stories and attempt at
raising awareness through the media
The body shop lady died of hepatitis C, she contracted it in those days, when
she needed a blood transfusion when she was delivering her kids.
108
There were some misconceptions about treatment of CVH, that tied up with the
misconceptions about types of hepatitis but notably it was understood this relied on
finding the illness
In the start if they find out then they can be saved-can cover and control. On the
first stage, on stage A but then if it reaches C then no.
But there was less awareness of vaccination for HBV
I have been vaccinated but I didn’t know exactly what it’s against
There were only a few people who describe personal experience of hepatitis. One of
these did give an account consistent with CVH. The other seems to conflate febrile
illness and jaundice with CVH. Some people did describe experience within the wider
family
I think she got it when she had an operation. Maybe it was due to a poorly
sterilised surgical instrument.
Generally, people did associate hepatitis as being a disease with significant
consequences
What I’ve heard, it’s a very bad disease
with others confirming this view
It is life threatening for sure.
Overall, there was less knowledge than anticipated. Consistent themes emerged
showing confusion between faeco-oral spread of illness and their link to poor sanitation.
Furthermore, jaundice was conflated with the term hepatitis. There was some
appreciation of the nature of spread of CVH with recognition of previous iatrogenic
spread as well as blood contact more generally. Despite these misunderstandings, there
was also recognition that the community overall is not very aware about CVH. There
was, however, a consistent opinion that hepatitis is a serious disease, indeed potentially
life threatening.
b. Testing:
The topic of testing for CVH was raised to determine any concerns about it. Generally,
in relation to the comments above that CVH is not a problem in this country, so it was
109
felt testing is not needed in the UK
No, not here (UK) and you feel safe here
There is a feeling that healthcare activities are safer here, so testing (for any condition)
should be safe where needed
Here I am satisfied. If I go somewhere else, I won’t be sure, which kind of
needles they are using… the compounders …. How clean are their hands? I
think here it is satisfactory.
Both these points were re-iterated across multiple focus groups, given apparent
improved sanitation here and as such testing in the UK may not be as important
It’s through blood or water or unhygienic conditions. So will testing here really
be relevant? Because here hygienic conditions are much better compared to
India
Given these opinions, the groups were specifically asked what they felt about access to
testing, should it be necessary. It was felt that if there is testing available it should be
widely available
Testing, yes if possible, testing should be there for everyone
And others thought testing should be done automatically for those with risk factors
Anyone having a higher risk should be automatically offered (testing)
A driver for testing was to ensure good health and overall for protection of the family.
It was generally felt that the SA population will do as instructed by their physician
I think more than 90% of people in our community do whatever the doctor tells
them to do
And that this extended to asymptomatic testing for medical conditions
I think if the doctor tells the patient to get screening, I think everyone will be up
for it.
It was felt that the onus was on doctors to inform patients
Unless the doctor speaks to us about the screening how on earth are we likely
to know about it?
It was, however, mentioned that the doctor should be clear that testing is required, not
110
optional
If the doctor tells them to do it then they will go for it even if they have to miss
out on their work. On the other hand, if the doctor tells then it’s up to them they
most probably won’t go for it. He would think if the doctor is giving the option
he doesn’t have the need to get screened after all
There was however some concern that the NHS did not always offer screening where
available due to financial concerns
Because at times the NHS doesn’t have the funding for testing and therefore,
they don’t invite people for testing
And participants were not clear on whether to ask the doctor for the test, feeling that
generally doctors did not like this approach
As you say there are no symptoms……. How would we know then? Do we ask
our doctors to get a test done for us, or…. Because they will not be happy,
definitely, and the test added to the test they’re doing
Others went further suggesting that the GP held the power to test or not and the patient
did not have much role to play
Depends on the GP if you get tested
There was some concern raised that the community may be reluctant to test due to fear
and this combined with busy life tasks made people less likely to be proactive
I think there is some kind of fear we have as a community we don’t go into these
things; we are just too busy with our own lives.
There was the impression that men were less likely to visit a doctor and also to get any
health care including testing for any conditions
Men absolutely don’t like going for testing
Although this was not specific to CVH.
It was emphasised that the more testing becomes widespread in the community it will
get normalised and testing will be easier
This is very important- if someone gets a routine testing then others are going
to follow. They will recommend it to you and tell you it’s fine just a small test.
111
This encourages others
There was acknowledgement that having medical tests can cause some anxiety
Will get a little scared
and that there were concerns over the nature of tests
It’s not a small amount of blood they draw, two bottles every time
which meant there should be prior explanation of what is involved and that this will
help allay concerns over the testing process
For testing a person should know everything about what is going to happen. If
you go all of a sudden and you don’t have any idea you will be fearful
Particularly for illness of perceived severity with people anxious over the consequences
of a positive result and as such it is important to give information on the condition prior
to testing
Hepatitis is a very scary disease. You live a normal life before getting screened
and all of sudden you are invited and if you find yourself tested positive for this,
your first reactions will be I’m gone
That will reassure people as to the nature of the illness as well as the testing method
It also depends in the person who explains the test to you or the literature you
get with regards to the screening. If they explain to the person to be tested that
the test was going to be minimally invasive through a small blood sample, they
would feel more reassured
And the particular concerns over the nature of testing were mentioned in multiple
discussions, particularly as it was felt blood tests were relatively minor
But if the person going for the test doesn’t know as to what would be done to
them, whether they are going to be hacked or cut into small pieces they would
obviously feel scared. I think the test must be explained in advance to the patient
that they would only prick
The motivation for testing was felt lacking where people felt well, and that they did not
necessarily associate this with a potential late diagnosis of CVH
A healthy person would normally think that he/she doesn’t need to get tested for
112
it because they are healthy. It is a different matter that some of them end up
being diagnosed with a disease towards the very last stage of the disease but as
long as they are healthy they can’t be bothered
And that the main impetus for seeking healthcare would be symptoms
Very few people like to take any form of action without going through or without
experiencing suffering
Whilst people did not think they were likely to consult a doctor without symptoms,
there was discussion that even apparently mild symptoms should prompt medical
review to seek more information from their doctors
If you know there is something happening to your body….and don’t know what
they are then you should go and get it investigated
Others did feel knowledge was important, and that individuals in the community could
spread awareness amongst each other
In my view, not knowing about it won’t be good for us. We must know about it
if we have it. This way we can spread awareness and encourage them to get
tested and get treatment on time. This way awareness can spread form one
person to another
This responsibility amongst the community towards their family and friends was
mentioned in all focus groups, and in particular word of mouth was important to the
community to spread information and knowledge.
The general consensus was that the main priority when it comes to testing should be
people at higher risk
The priority should be to test those who are more prone to contracting it
The importance of prioritising those at higher risk was re-iterated in other focus groups
where again it was stated the NHS cannot test all people
I think it depends on the risk factor…. if they are higher risk of getting it them
getting screened is more important. They have to assess the risk because they
can’t test every single person can they?
And if this risk was defined by country of origin this population should be offered
testing
113
People who belong to India, Pakistan, Bangladesh such countries where this
disease spreads more; if they wish they can be tested
If ethnicity was the risk factor, rather than country of origin, it was acceptable to target
testing in this way and testing should be offered routinely
I would say that if we are a high risk group, if South Asians are a high-risk
group, we should be at least offered once a year or something like that…. a test.
It was felt that testing campaigns would be more successful where people understood
the reasons for testing and had assurance regarding confidentiality if this was in non-
traditional settings
Firstly, awareness. You should give awareness to people as to what hepatitis is
and why testing is important. And then maybe if you keep it confidential…. you
know how one thing leads to another in this community
Whilst it was recognised there will be fear about testing, this was not specific to testing
for hepatitis and was felt to be the case for any health issue
Every illness has a fear regarding it. That up until the result comes out you will
be in tension and anxiety
Whilst others commented they were not sure on risk factors for CVH particularly, the
general opinion was regardless of the condition, it was felt if there was any risk to the
person, it would be important to seek testing
All I can say is get some blood test, get urgent medical care. That’s all I know
And whilst some felt this warranted family discussion, others felt not
Ill discuss with my husband and straight away go for the test…. (Reply) Me I’m
not discussing it even I’ll just go
And that it would be important to take up any offer for medical tests to keep yourself
as healthy as possible
Any kind of test request you get, I’m going
In order to find out if there are any problems requiring further investigation or treatment
I would like to know and then can do something about it
Particularly when the illness potentially is not self-limiting
114
Rather know than not know because it will not automatically go from the body
right?
And that people should be proactive in this regard, suggesting the onus is on the person
as well as medical professionals
One must take some precautions in advance to avoid it and the testing must be
done for the sake of your health
To allow more positive outcomes in the future
If testing is done, we can find out whether or not we are likely to become ill in
future, so if there is a problem then the treatment would be easier
However, others felt generally there was a fear of finding out about any serious
conditions, particularly in the SA community
I think majority of people in our community think it would be better if they did
not know about their diseases through testing. We don’t want to go for testing,
especially for the serious diseases, we don’t want to know God forbid I have it
or not.
But this was not agreed amongst all participants
I think everyone should be tested to find out what their actual position is like,
just to be on safeguard
And this was reiterated in discussions amongst participants in other FGs, both genders
I think some may be frightened to be tested (reply) it is not as if we are going to
war
It was noted, however, that there is a worry for people that testing will lead to a
diagnosis that can be fatal and so fear was not necessarily only over the mechanics of
testing
There is a fear that people don’t admit, the fear of death and because of this
people don’t want to go for testing
This was related to a fear that if unwell nothing can be done to treat them and so testing
was in essence futile
Before they (the doctors) find out there is hepatitis, you are too late, they are
115
gone
But others did recognise the importance of testing before symptoms start
Yes, test, why not, why wait until you are poorly
And that some people do already go for regular health checks anyway
Not just for this one (hepatitis) some people get their entire bodies checked on
regular basis, but others don’t
But others felt there was little knowledge about screening both for hepatitis
I want to say that people know very little about screening. If they don’t know
they aren’t likely to ask for it. I think the doctors should tell to get the screening
done.
and other conditions
I have heard about screening today (in general) I am shocked as I have lived in
this country for a very long time now but until today, I have not got any
information about the screening
And that people are likely to delay testing if they feel well, feeling other tasks are more
of a priority
They think they don’t need screening as everything is fine for now
We did ask opinion on where testing should be located to determine whether
community-based testing would be feasible. There was opinion that the location didn’t
matter as ensuring you are healthy is more of a priority
If you have to do it, it doesn’t matter where it is going to be. The point is we
need to go there to make sure everything is ok with us
Whereas others felt the GP was more convenient despite other concerns about primary
care noted above
GP, I think is much more comfortable, if we go to a GP
And others felt other mosque-based campaigns were a success and would lead to more
awareness of the condition as well as testing
Personally, I think if you test in the mosque then it will give more awareness for
116
others to be part of it
And that local testing was preferable to travelling to a hospital
Better whichever place is near you, rather than go to a far-off hospital
No-one felt that potential stigma around CVH would prevent them being tested for this
condition.
c. Access to healthcare
In the UK access to healthcare services is thought to be challenging
I strongly feel that, uh, accessing the healthcare facilities is not good here
And that only once unwell do you get offered tests, with no focus on preventative
medicine
The health services won’t offer the test; only on some cases if you are not well
or something otherwise, they don’t come and ask you
There was repeated concern that language can be a significant barrier to seeking
medical attention
I think lots of people feel shy because of the language
And even if one does present to doctors, language limits the utility of the consult
How can we go to the doctor and say our compliant? We cannot explain our
problem there is no language.
There was an appreciation, however, of the fact that there are SA people within the
health service who can speak the main languages of South Asia
Language can be a hindrance but not here because lots of the doctors are
Indians anyway
However, others did describe a lack of awareness of their own health due to language
difficulties, particularly where there is any social isolation
I cannot talk much with the doctor. I don’t have English. Otherwise, I have a
strong wish to be get myself checked for illness, but I don’t have the language.
That’s why I don’t go to the hospital. I have blood pressure and I don’t know
what else. I have a wish to get checked but I don’t go. I don’t have English and
117
I am alone here it is difficult for me
Language challenges, including during the consultation itself made it difficult for
people to seek medical attention, even when feeling unwell
It is very difficult to go to the doctor, there are so many things we cannot say
However, it was felt that even where testing and treatment exists, these were not always
available principally due to financial reasons and there were specific concerns whether
the NHS will fund such pre-emptive healthcare
NHS doesn’t have funds for all this does it. They are trying to cut down as well
(laughter)
It was consistently mentioned that the major driver for healthcare in the UK is financial
and the financial constraints the NHS faces determines what is offered to the public
I mean it boils down to what the government is doing yeah, it is not investing in
the NHS here
And if any intervention is expensive, this will determine whether it is well utilised
It’s a funding issue
It was felt that financial considerations are clearly a priority and that in GP surgeries
there is open mention of funding concerns which can put people off seeking medical
attention even when unwell
There are signs, every visit is costing the NHS this much
Some people did think that even if the money is there, this SA community is not
prioritised for any type of healthcare intervention regardless of whether they are at more
risk
30, 40, 50 years we have been living here. I think that the NHS has funds, but
they are not spent on our community
There was also the belief that GPs were time and resource constrained and this was
clear to patients in their consultation
I don’t think doctors like us even saying anything just go there see them for 5
minutes go.
whilst others felt the pressure on the NHS rather than individual clinicians would mean

118
this type of screening may not be possible
When our national health is already severely under pressure with other
illnesses, will it be able to bear the burden and costs for this as well?
Primary care services were not felt to proactively approach patients for preventative
medicine
The GP will never actually come and tell you to come for an annual health check
And it is often felt primary care is not responsive to individual patient needs
I haven’t had much personal encounters because I don’t go to the doctor, but
then they don’t care that much, the doctors, they just keep making you make
trips
And this contrasts with healthcare approaches in the country of origin
…they (UK physicians) don’t care. Even though it costs in Pakistan, but it is
proper. I mean if you go to the right doctor, you get the right treatment and you
get better
Whereas in the UK people felt there was generally a delay to make the correct diagnosis
with multiple trips to the doctor, illustrating this with personal anecdote
But the bottom line is she should have diagnosed it properly first time because
she had been a GP for donkeys’ years
Furthermore, there was a feeling that investigations are not carried out properly
I think the medical system also needs changing. If a patient approaches the
health service, they must make sure the conditions are properly investigated
d. Attitude to Health:
There was a perception that good healthcare relies on doctors leading patients to good
health
The patients only receive whatever treatment the doctors would give to them.
How do we know what treatment is available for this disease?
And that part of their role was to approach patients to encourage testing or investigation
where relevant, and for any individual at risk doctor should come to us regardless of
119
the condition
No see, the doctors that are here, so when people go to the doctor why they
don’t say you people should be tested for this also? No one has ever mentioned
that this is one more thing that you should get checked!!
Indeed, it was often felt so strongly in multiple focus groups that if this population was
truly at risk for CVH the doctors would approach them
But they did not test me for hepatitis. I think if we would have been at high risk
or coming from such a country, they would have done it but it didn’t happen
and as this did not happen, there was some scepticism that the population was actually
at an increased risk
If they feel that it’s such a big problem in the ethnicity or this sector, then
probably that is what they should be doing. But, again, you know, I think
because it’s not there, so it’s probably not that prevalent
Overall, people did not feel empowered to speak directly about what they wanted to the
GP
I did not even know there is an option to go to the GP and ask (for a test)
And even if they did, they felt they would not be listened to
The GP will ask what is wrong with me that I need this test. I mean they won’t
help me.
And that for some primary care services were overwhelmed which compromised the
care received by patients
the doctor in the NHS go there so many people say we are like a production line
you know one after another five minutes, two minutes just write a prescription
get them out he don’t go into detail
where others felt dismissed feeling, this was more related to the individual clinicians
They don’t really care, they don’t listen to you
Part of this lack of care, whether institutional or individual, was that the GP seen as
‘gatekeeper’
It’s hard to see a specialist here need to see the GP
120
And that there was reluctance to refer on
No see doctors will not recommend you to a specialist
It was felt that if healthcare services were visiting in the community this could be any
gender or ethnicity
I think any person with an NHS uniform/identification should be fine as people
would think that this person is professionally linked
And whilst the role for religious leaders were clear, it was still felt that the doctor had
an important role in health and wellbeing
It’s our community you are helping us the way I see imam is only doing the soul
but you’re our body
There was opinion that males were less proactive about their health than females
I think ladies are more concerned about their health. I do not know the reason
but I have observed that Asian men tend to avoid going to the doctor
And were less likely to seek medical attention
They seem to think that they (men) will automatically recover and they keep
avoiding going to the doctor until it is too late
There was also a belief that illness was out of their hands without recognising that the
individual can play in role in minimising the chances of some illnesses
We tend to believe what will be will be. So yes I understand that our people can
say that if something is going to come to them it will and what will not will not
and so they might be saying yes it better that we don’t find out. Of course, they
don’t realise that we also have to practice prevention from something in order
for it not to be contracted.
We discussed healthcare provision in non-standard settings such as the local
community. Using community venues for health care promotions has been noted before
in the local Surrey SA population
They (other campaigns) used mosques and the English language classes to
create awareness
Coupled with the idea that this population is pessimistic about ill health
121
But I think in our community people feel more remorse when they get it. They
think they are going to die and feel disheartened. But in other communities’
patients have more hope and they believe they can fight it. I think we have more
negativity in our community and people don’t believe that they can battle it out.
Therefore, the families can help each other and give moral support to each
other.
Even those who felt there should be individual responsibility to do what they can to
remain well, there was some feeling that there were so many illnesses that one cannot
be informed and proactive about all of them
There are so many diseases. We hear about meningitis, malaria, hepatitis so
it’s like if we start thinking about all of them, I think I will get into a panic state
Particularly when some members of the community still see ill health in any sense as a
stigma
Back home, sickness is a stigma
And this may have some impact on whether people seek medical attention
Going to the doctor is not their priority
But there was a feeling across most focus groups that attitudes in the community are
changing
I think, whether its hepatitis or anything else I think most important is this
generation we are kind of educated
And people are becoming more aware of their health
A lot of elders are not educated, not gone for schooling and they don’t have
awareness of all these diseases, and they are more superstitious and they stick
to it.
But this did not necessarily translate into preventative medicine
I don’t have much awareness about any disease or anything because when we
are healthy and we are running around, we don’t need to, we don’t go to see
the doctor even for routine check ups
And the role of God was felt important in terms of keeping well
122
People leave all that to Allah
Although there was a role for God, there was also some recognition of the potential
developments in society and how treatments become available
We could think of Allah’s will for a lot of things but now because there is a lot
of advanced things, one must try one should get treatment
But still some people felt ultimately Gods plan was pre-determined
There are medical ways but Allah has a plan that’s 100%
Whilst there was recognition of the role of individuals and healthcare professionals
there was some reticence to acknowledge the role of healthcare services for those that
are well
We don’t want to go to the doctor to find whether or not we have got any illness.
If I tell a friend that I want to go to the doctor to find out whether or not I am
carrying any illness he will tell me I am a fool because I look healthy and alright
Particularly given the expressed opinion that members of this community did not
always prioritise healthcare
I think most people in our community neglect their health
But did feel they should be informed about health risk factors
If it’s dangerous, if its epidemic like, if it’s contagious we should be told as soon
as possible
And if one does test, then there was recognition that earlier detection could be helpful
for recovery and long-term health
If you find out you have, you are tested, then you are healthy you have no
problem then if there is a problem at least it is treatable quicker rather than last
stage then you have problems
Particularly where it was recognised that later diagnosis can cause problems including
more advanced disease
I think I’ll rather be tested for disease than suffer later on
But there was some concern regarding ability of the NHS to manage screening, and this
would perhaps affect people’s willingness to ask for tests proactively
123
Currently we are trying to cover large shortages in the NHS so if something is
there I’ll be happy to go. But I’m not going to go to the GP and ask for screening
for every little thing
But that screening in general was not necessarily a priority for individuals, but
opportunistic testing when visiting the doctor for something else would be acceptable
I wouldn’t go if I am going only for hepatitis, if the screening will cover me for
things a mix, then I’ll go because I don’t really have time to think about
screening
But many did feel it would be better to know if you are facing health problems, whether
CVH or other illness
For me it’s better to know than live in a false reassurance
There was some concern expressed that screening should really only be prioritised if
there is a cure
I think if you know it’s a curable disease you will go and find out, but if you
know it’s not curable…. (Reply) because it will otherwise kill you earlier than
what you’re going to die
But others felt not knowing, regardless of treatment being offered was preferred
I think some people don’t want to know. They think that if they were screened,
they might get tested positive and that’s why they don’t want it. Some people
think this way, but it is wrong.
But that knowledge was key
Whatever the main germs are, or if you feel there is a disease that can ruin your
health and to safeguard from it you need to have a lot of information
And there was a sense of destiny that regardless of the precautions one can take, God
still has a final say
We try our best that all things are good, and we don’t get any illness, we try
from our side but even then from Allah….
e. Stigma:
Generally related to be ill not hepatitis specifically
124
There was a sense of stigma relating to ill health in general
They fear the concept of ‘achoot’. They are worried about being made into an
untouchable.
And that this would lead to isolation
People shun the person
And be seen as a risk to others
Because people fear that they may contract the illness from them. To try to avoid
them. Remain apart and away.
This was felt particularly important for men with their role still seen as providers for
the family
As a provider for his family, he feels concerned as to who will look after his
family if he dies
As such, they are less open about ill health
I think this (illness) is a very sensitive issue for men and they hide it from their
families and try to manage it on their own for as long as they can to manage to
do so
Particularly if it is perceived that the illness is related to lifestyle factors
I think people tend to be more suspicious towards men and you would be less
suspicious towards a female because you tend to think that women are less likely
to do a naughty thing
But this was balanced with a realisation that it was not the person but rather the illness
that could be problematic
I think we must try to avoid the illness not the person
And so isolating the person was not needed
Taking care does not mean that if a person is diagnosed with this condition they
should be made into an outcast, or we should completely isolate ourselves from
him. All we need to do is make sure the person gets the treatment and acts upon
the advice of the doctors
But patients should inform themselves as much as possible
125
The patient must try to gain more awareness about his condition and the
precautions they must take. They also need to ask on the doctor advice
There were some though, who felt they would find it difficult to act as usual towards
an ill person
I would not be able to be right near, next to the person
Which would be exacerbated by lack of knowledge
Without having the facts, they can kind of isolate that person
There were some people who did mention hepatitis specifically may raise questions
about the patients’ behaviour
So it’s like, you know, if someone husband or like you know someone’s wife is
diagnosed, then it, it is a possibility that people might think that, okay, what is
going on
And this could lead to people being more careful about disclosing health issues
If I am diagnosed, then I would be really careful about who to tell
To avoid the stigma that could be associated
You are vulnerable to those kind of judgements and people behaving differently
for no apparent reason
And this this not only protected themselves from judgement, but protected the whole
family
Yeah, it’s a culture of silence. I think the whole family gets affected if anything,
any kind of news comes out
But it was felt the immediate family would not isolate anyone
But I think in our culture families are already with you. They won’t leave you
left behind
And that for women particularly, they had to try to remain strong to hold the family
together
You have to be mentally strong for everything, and if you are sick, the whole
family goes down
And this included not informing others outside
126
Maybe we should just tell the close family members, not spread to everyone
To avoid this idea of being an untouchable
Oh, you are untouchable. Stay away.
Different issues were seen for men, however, and how illness changed the perception
of them
There is more stigma against men being sick. That means they are weak
Particularly if they were not working
The stigma for a man being unwell and at home would be more
Or looking to further their career prospects
He always thinks if he is unwell or diagnosed with anything that may affect his
job prospects
Which often meant women had to hold the family together
It’s all left to the women. You have to do it and I think it’s kind of embarrassing
for them to say it out yes I have a disease, you know pride or something like that
Particularly with hepatitis, which was seen as a potentially fatal condition, people were
scared and uncertain to approach the individual
The thing is that hepatitis, when people hear that name its quite serious, people
are very, sort of scared. Yeah, they are frightened. They say he’s got yarqaan
(jaundice) mate
As jaundice had stigma associated with it
(Yarqaan) is the word that they use for this disease in our language and people
are scared to hear this word
but that lack of knowledge was seen as responsible for many of these more negative
actions
People don’t know about this disease and we don’t want to admit it, we don’t
want to tell others about it. But this is common practice in our community
because of lack of awareness
But others did not think hepatitis was associated with negative views of the person

127
There is nothing like that, no discrimination
But much of the stigma was related to ill health more generally and the consequences
for the whole family
Yes, there is some discrimination for that yes, because if a lady is ill we don’t
know whether she is going to be fit for our boys and then she is already suffering
before she gets married and the boys life will be hell you know
Whilst others felt the isolation was really only for contagious illnesses
If someone thinks they can catch something from you, they will stay away, right?
That’s natural
But that sensible precautions should be taken
Take caution in everything, already there is a person in such a terrible state
another shouldn’t be getting it
And for hepatitis particularly there was a feeling that this involved complete separation
of household members
Separate everything clothing, utensils
Which is why it was felt more difficult for females who took on these household roles
It is more difficult for women to cope because a woman as always got to do one
or more chores at home so she can’t take a day off.
And there was not always gender equality in this community
They are not treated equally because there is a gender inequality in our
community, but our younger generation is different (older male comments)
But there was recognition of silence around health
I think most people would not tell others of they have a medical condition. They
would keep saying they are fine.
And it was only divulged when any illness is advanced, and it cannot be hidden any
longer
We speak about it when we think the stage has come when we are not left with
any other option but to talk about it and I think it applies to both male and
female genders
128
But this was felt to be something in all communities
I think in every community people hide these things. Those with no awareness
of how this disease spreads will be scared because it is a viral infection and
others will be scared, they might get it from me so they will try to avoid me,
because of this fear I will not tell others about it. Fear everyone will isolate me.
The research team also analysed independently the data and got similar results. These
factors were then used as the basis for the educational intervention.
III. Advice on our project:
The community feedback on our film was that we should not be too negative
You should give them hope. You should tell them what this is and why it is
caused and what can be the consequences of it
and reiterated the importance of imparting knowledge
The video should not only show the consequences, it should be informative and
it should explain what hepatitis is and how it can be spread. I mean, rather than
just telling them about its consequences, they should also raise the awareness
as to what it actually is. People in our community don’t know whether it is a
viral infection or any other disease. This way you can also give people hope,
for instance, you can tell them it is caused by a virus and you can treat them.
And GP surgeries, despite the negative sentiments expressed by some about primary
care, were felt to be important community places to show the film
At GP surgeries as well when people are waiting in the waiting area and you
can show the video on the TV monitor.
We sought advice about language and it was felt both English and Urdu (which is
understandable to most in this community) were important
I think in both languages. I know that some people may have lived in this country
for 30-40 years and even if they can’t read English, they can understand spoken
English. There might be some who may not be able to understand English at all,
you can translate the same video for them in Urdu.
And so we decided on voiceovers and subtitles as well as making the video in both
English and Urdu
…. if your item is in English, you can provide the translation
129
to appeal to the age range of people in this community
If there is the younger generation they are good in English. But the older
generation better in our own language.
As was true accounts from people who had experienced hepatitis
You can also include the view of those who have already gone through it.
It was also felt an explanation of why testing is being offered would be important
I don’t know what the method should be but really want this awareness to reach
people as to why this testing is being offered and that this testing is for our own
good. And I am sure they will pay attention.
As awareness was felt to be the key to encouraging testing
Without awareness we aren’t likely to get ourselves tested. If we don’t know
why we need to get tested, we won’t go for the testing
As well as providing notice especially for those with children
Like today you have kept this programme, run more. Wherever there are
gatherings for women, inform them beforehand last minute is very difficult and
they will come
Others re-iterated a simple approach of explaining hepatitis
Firstly, what is hepatitis point 1 point 2 how and where does it spread point 3
what are the effects
And not using too complex language and concepts to ensure all can follow the film
narrative
You have to go slow and steady. If you are a doctor, then you must have the skill
to be able to explain things to the common man. Praise be to God, doctors are
very learned, but many times they don’t reach to the limit up to which general
public has knowledge or ability to think, or to absorb. So it is not just enough
to say to them, they have to be able to absorb it and to be able to explain its
main points at home to family and children or friends.
The importance of having patients who have had hepatitis explain their positive
outcomes was mentioned
I think we should have someone who has already been through this, and the
positive response, outcomes
And using their stories to encourage people to get tested
Real life examples, resonates with people that they need to go and get tested
And how they experienced more complications from any delay to testing

130
The real-life story of someone who delayed the testing so what were the impacts
of that
And the nature of the diagnostic pathway
How easy is it to be diagnosed and what are treatment options?
The major ways it can be spread
And ideas on appealing directly to women, particularly emphasising the importance of
keeping well for the whole family
For us, family is very important so if we have awareness or if we tell those
women how important it is for the family and their wellbeing I don’t think any
woman will want to take that risk or take that chance in life that she is not there
for her kids or family
It was felt primary care as well as religious venues could be used as gathering points to
show the film
GP surgeries, gurdwara, temple religious places
It was felt that the only real constraint was to be aware of Ramadan
As long as it’s not the fasting month it won’t be a problem
But it was said that the religious venues in some areas where a focus for the community
In Woking we have a majority Muslim community so the focal point is the
mosque so if you really want to tackle any disease or anything get connected
with the mosque people
And that word of mouth was emphasised as being very important for the success of this
project
Say I get tested then I get back home and talk to the family about it and I will
voluntarily ask my wife to participate and my wife will in turn speak with a few
people and in this way the information will spread from 10 to 100 people
And the community did not feel the ethnicity of the healthcare staff was important
If it’s a doctor or nurse or public health doesn’t matter if they are Asian, a gora
(Caucasian) is fine
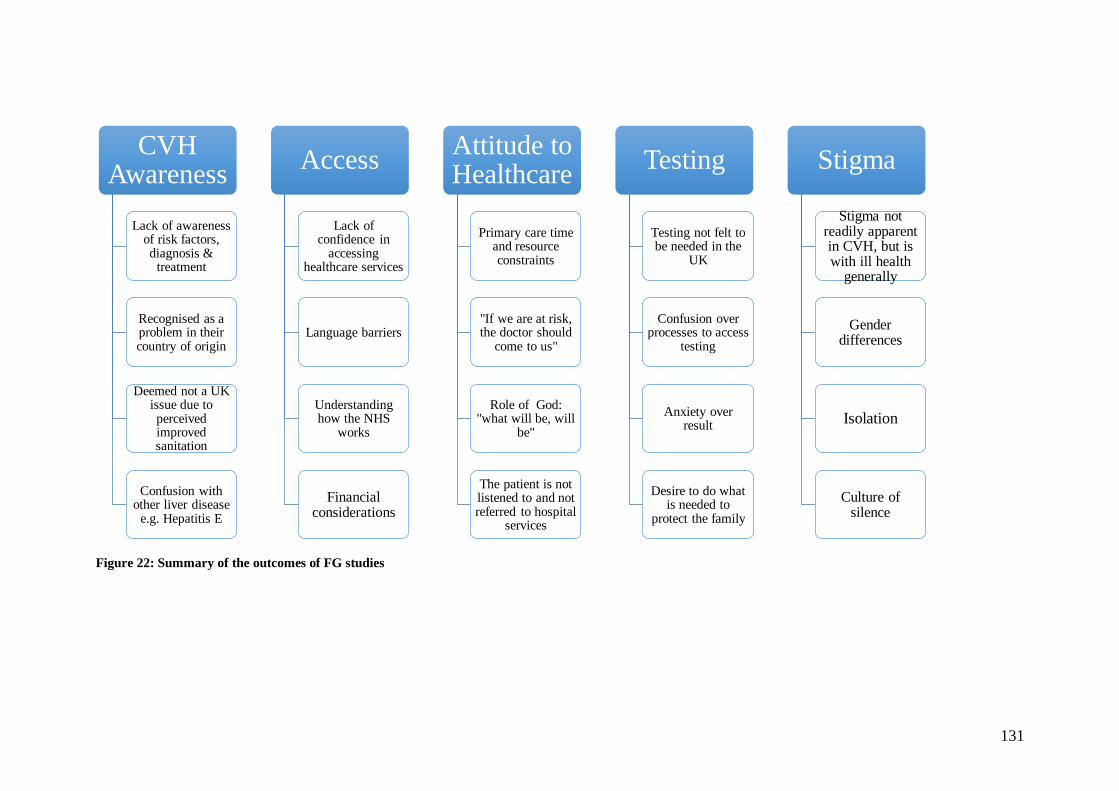
131
Figure 22: Summary of the outcomes of FG studies
CVH Awareness
Lack of awareness of risk factors, diagnosis &
treatment
Recognised as a problem in their country of origin
Deemed not a UK issue due to perceived improved sanitation
Confusion with other liver disease
e.g. Hepatitis E
Access
Lack of confidence in
accessing healthcare services
Language barriers
Understanding how the NHS
works
Financial considerations
Attitude to Healthcare
Primary care time and resource constraints
"If we are at risk, the doctor should
come to us"
Role of God: "what will be, will
be"
The patient is not listened to and not referred to hospital
services
Testing
Testing not felt to be needed in the
UK
Confusion over processes to access
testing
Anxiety over result
Desire to do what is needed to
protect the family
Stigma
Stigma not readily apparent in CVH, but is with ill health
generally
Gender differences
Isolation
Culture of silence
132
CHAPTER 7: FOCUS GROUP - DISCUSSION

133
STUDY 1 DISCUSSION
This study was successful in recruiting SA people based in Surrey to join our focus
group discussions. Initially, there was a smaller number of attendees than predicted
with only a few participants, however, as word in the community spread attendance
increased throughout the study. While some groups had only a small attendance the
findings did not differ significantly with the same broad points of discussion, with the
same themes emerging as summarised in Figure 21.
However, I recognise there could be limitations from the relatively small geographical
area of recruitment, particularly relatively to the Surrey population more generally.
Given this is a feasibility study I needed to pilot this program locally before it could be
rolled out more widely. It did mean that the area was saturated with this study 1 work
and meant there would need to be steps taken to widen the geographical area used in
study 2.
DEMOGRAPHIC SPREAD OF FGS
All FGs were run in the community namely local residences, community centres, GP
surgeries and religious venues (only mosques). Females were mainly recruited in
community centres (n=14; 52%) with smaller numbers in local residences (n=8; 30%),
mosque (n=4; 15%) and only one (3%) from a GP surgery. Males were mostly recruited
from mosques (n=13; 50%) with some from local residences (n=7; 27%) and local GP
surgery (n=6; 23%). The lack of males recruited in community centres likely relates to
patterns of behaviour in the community, with males more likely to be working during
the day and attending mosque rather than the community groups that were in place
specifically as support for females rather than any inherent difference in ability to
recruit each gender from these locations. One focus group was mixed gender at the
participants’ request (but only one female) in a GP surgery and the others were single
gender in keeping with cultural norms, particularly in mosques. A success of our
recruitment was the female representation (27 of 53 people). Female representation was
missing in other studies. There was an age discrepancy, with mainly younger women
and older men which may be due to men working and younger women in more caring
roles. Our initial aim was to split focus group attendees by age but we abandoned this
due to difficulties with logistics and family groups wanting to attend together.
134
The majority of our population was from either India or Pakistan (89%), with men
mostly Muslim which is probably because two of the male FGs were held in mosques.
The average number of years spent living in the UK was high for both males and
females (34 and 22 years respectively) which may be due to the fact that older men
were represented in our sample. Females were more likely to be newer migrants with
less time spent in the UK (range 1-48 years) than males (range 7-50 years). Education
levels were fairly high, but this may represent immigration and visa rules for SA
migrants being employment related with associated minimum caps on income (as
discussed in chapter 2) although clearly immigration rules have varied over time.
PAST EXPERIENCE OF CVH
A small number of FG participants described being previously tested for CVH, 3 males
and one female (8% overall). Two of these males tested positive and had treatment, the
others were negative. It is unknown if this was HBV or HCV or indeed another illness
altogether given some of the misunderstandings seen in the focus group discussions.
One in five (both males and females) did not know if they had been tested and this is a
common occurrence in clinical practice, where patients (from all communities) are not
always aware of the details of the tests they have had.
One third of the FG cohort described being vaccinated for HBV. Females were more
likely to be vaccinated than men (41% and 27% respectively). The reason is not clear
but may relate to females being younger and thus having exposure to more vaccines, as
well as more records of prior healthcare. It may also be related to pregnancy and local
practices in the country of origin. A similar number (28%) amongst both genders did
not know if they had been vaccinated, with males more likely to say they were not
vaccinated (38%) than females (30%). Again, this may represent males being generally
older and having less updated healthcare records from their childhood. It is also unclear
whether recall is accurate, either positive or negative, and so these figures may not be
entirely accurate. Certainly, in the UK it is only in recent years children have had
vaccination for HBV unless at particular risk.
135
FG DISCUSSION OUTCOMES
With thematic analysis, complete separation of results and discussion is not feasible.
The results section (Chapter 6) provides some discussion of themes (lack of awareness,
testing, access to healthcare, attitude to health and healthcare professionals and stigma)
and so in this section I focus on a summary of the findings within each of the main
identified themes (see Figure 21 and Figure 22).
THEME 1: LACK OF AWARENESS OF CVH
There was less knowledge than anticipated on all aspects of CVH. Many of the FG
participants had no awareness of the condition whereas other confused it with different
forms of hepatitis or jaundice particularly faeco-oral hepatitis (Hepatitis A and E) which
is more common in their country of origin. Whilst some participants claimed personal
experience of CVH, even they had some misunderstanding about the nature of CVH,
its transmission and treatment options. It is not known whether they had HBV or HCV
(or indeed if they had another illness) given the frequency of conflation of various terms
relating to hepatitis and jaundice. This lack of knowledge was seen in all groups,
including the younger and older participants as well as males and females. There was a
general conflation of hepatitis, liver disease, jaundice and on occasion alcohol. This,
however, is anecdotally a common misperception across all groups of patients that I
have seen in clinical training. The overriding theme was one of poor sanitation or
uncleanliness being a harbinger of CVH specifically, as well as other illness more
generally, and as such CVH was seen as less of a problem in the UK and was usually a
marker of poverty in individual cases as well as in countries.
There was, however, recognition of the previous iatrogenic spread of CVH in many of
the FGs particularly related to healthcare practices in their country of origin but also
noted was reference to contaminated blood products. Again, somewhat erroneously this
was principally not felt to be a problem in ‘developed’ countries other than by a small
number of FG participants. Those who did recognise it as a problem here had awareness
through previous campaigns (e.g. Anita Roddick, the owner of the Body Shop) to raise
awareness.
136
Whilst there was misunderstanding about transmission and potential treatment options,
I feel this was really related to the misunderstandings about the cause of CVH and led
to a general opinion that cleanliness will solve the problem.
Additionally, there was a perception of CVH as a serious illness. However, this was
more of a negative than positive as this opinion did not seem to make participants more
willing to inform themselves, but rather led to pessimism about outcomes if a person is
diagnosed with CVH and frequently, it was felt treatment was either not possible or
futile. This was something to be addressed in the making of the film, as it was felt that
it would impact willingness to test.
THEME 2: TESTING
The aim was to gather thoughts on the pros and cons of testing for CVH. In accordance
with the misunderstandings with knowledge of CVH and its transmission, people felt
testing when resident in the UK was unnecessary due to perceived higher levels of
sanitation and relative lack of poverty. Regarding medical tests in general, it was noted
people were confident this was safe in the UK (as discussed in the context of concern
over ‘compounders’ in participants’ countries of origin). On asking specifically for
views on NHS testing provision if needed, participants felt testing should be available,
while some felt it should be universally available others felt it should focus on those at
higher risk and that testing should be proactive, with the NHS/doctors actively seeking
out those that needed it. The SA community report generally being deferential to
physicians and as such the onus was on doctors to tell them what to do for optimal
health. There were, however, concerns over whether the NHS could afford widespread
testing and where it would lie in a priority list especially as it was felt unwell people
could not always access services and tests in a timely manner and so testing ‘well’
people was not ‘fair’ or a good use of precious resource. There was also discussion that
the SA population are less proactive about their health and accessing healthcare but this
could be countered by ‘normalising’ testing with the widespread introduction of testing
in the community allowing ‘word to get out’ which would naturally lead to more people
coming forward and agreeing to testing when offered.

137
Generally, medical appointments and tests were a source of concern and anxiety and
careful explanation of not just what is being tested for but what testing involves would
be helpful in encouraging people particularly as it was felt doctors often assume a
patient knows what testing is. This was felt to be particularly important for CVH where
the perception was one of a condition that is often fatal. This coincided with a feeling
there would be a lack of motivation to test for something so prognostically poor when
the person was feeling well, thinking news of a positive test would instantly bring their
mental state down to hopeless and as such their physical condition would deteriorate
more rapidly.
It was felt that if ethnicity or country of origin were risk factors for an illness then it
was acceptable to offer testing along those lines and this would not appear
discriminatory. Testing in community venue was felt to be acceptable but needed more
thorough education and care over confidentiality.
Some people felt they would take any test offered and felt it was important to try to
keep well for the sake of the wider family more than for themselves. However, other
did counter this with the impression people did not want tested for a serious condition
particularly when feeling well.
There was some recognition of the concept, an indeed examples of, preventative
medicine but whilst others were less aware, a few did not agree with the concept feeling
particularly the psychological effects of knowing about a serious illness were not good,
but this was in the context of general nihilism over CVH and the fact there was little or
no treatment for this condition that was generally fatal.
There was discussion over where would be best to test in the community, with local
testing preferred with discussion over whether GP, community centres or religious
venues were better but none were felt unacceptable. There was no stigma over testing
for this condition specifically.

138
THEME 3: ACCESS TO HEALTHCARE
It was felt that language was a barrier to accessing healthcare and could limit the utility
of consults. There was recognition that there were many South Asians working in the
NHS who could often speak the languages of the region and even when finding an
individual healthcare worker they could communicate with, there were still system wide
issues. This is in keeping with discussion in Chapter 2 section V about migrant health
and the factors that influence this. Language and also cultural congruency were felt to
be tied into health literacy especially where there was also social isolation where there
was no family or friends to help individuals navigate the system. UK based healthcare
was noticed to be different from that in the countries of origin and this led to confusion
and lack of confidence in navigating the system. This was felt to be particularly off
putting for screening or preventative medicine and indeed could stop people seeking
help even when they feel unwell as they did not have the language to describe what was
wrong.
The NHS was felt to have considerable burdens upon it, often tied to financial issues.
It was felt that financial considerations were a principal driver for the NHS and
determined what services are made available to patients. The financial pressures were
felt to be very open and indeed these pressures were transferred to patients with things
like signs up in GP surgeries detailing costs of missed appointments and what this cost
the NHS, making participants feel they were a drain on resources and so discouraging
them from visiting. Some participants felt that the South Asian community were less of
a priority for healthcare, even when funds were available to be allocated (marginalised).
The funding concerns meant that most people felt screening and preventative medicine
was not a priority and so even where tests and investigations do exist they would not
be carried out for well people and the focus would be on unwell people as there was a
feeling even unwell people do not always get access to the tests they need.
Healthcare provision in non-traditional settings was familiar to many participants, with
previous projects using mosques in this particular South Asian population (Surrey) for
health promotion and awareness campaigns. The community felt this was appropriate
as they viewed religious venues as a strong centre of the community and a natural
gathering point for people and somewhere they were familiar with and which felt
139
comfortable. There was concern raised that the same level of confidentiality should
apply as is seen in the more traditional healthcare venues.
THEME 4: ATTITUDE TO HEALTH AND HEALTHCARE PROFESSIONALS
It was felt that primary care services are time and resource constrained and this was
apparent in consultations. This led to a feeling the primary care institutionally is not
proactive about health and so any measures to detect asymptomatic disease would not
be a focus for GPs. This extended to a feeling amongst many participants that individual
GPs were not responsive to individual patient needs which contrasted with practices in
their countries of origin. It was felt there was delays with diagnosis, a lack of
investigation and delayed or lack of referral to secondary care. It was discussed the GPs
themselves and primary care as an institution aimed to limit access to tests and hospital
specialists, referring on only when they had no other choice and had delayed as far as
possible already. This resulted in a sense of futility in consulting GPs for some people.
Others did suggest this was not exactly the case but occurred as a result of primary care
being overwhelmed, but they agreed this compromised care but not directly at the level
of individual clinicians. Overall, participants felt they would be less likely to ask their
GP for investigations due to these financial and time constraints even when they
recognised earlier investigation could help recovery and long term outcomes.
Members of the South Asian community felt that paternalism was the best way to
achieve good healthcare, with the role of doctors being to encourage and indeed
proactively approach patients to have any care required. It was felt that the South Asian
community are deferential to doctors and they would do as the doctor told them to. All
participants in our focus groups felt that if they were at higher risk of CVH the doctor
would approach them to tell them with such conviction they doubted they were at risk.
However, perhaps the time challenges in primary care are not set up to drive this
opportunistic approach during other consultations and so there needs to be a ‘political’
will to drive this. Often, in primary care the quality and outcomes framework (QOF)
is used in this way. This is a system designed to improve the quality of care patients are
given by rewarding financially practices for the quality of care they provide based on a
number of indicators across a range of key areas of clinical care and public health.
Participation in this scheme is voluntary although uptake rates are high. The four main
140
domains are clinical, public health, additional services and quality improvement. Each
domain has a set of measures or indicators against which practices can score points
relating to their performance. It is notable that liver disease is not included in QOF.
There has, however, been a link between the Royal College of General Practitioners
and the British Liver Trust to form the liver clinical priority project, with the aims of
improving the detection and management of risk factors for liver disease and
diagnosing liver disease early to reduce progression to cirrhosis, liver cancer and end-
stage liver disease. Of course, GPs cannot know all details of all liver disease and
therefore these frameworks could be utilised to create awareness and incentivising
particularly in the public health domains may help raise awareness and ultimately
testing for CVH in primary care.
Our study participants felt GPs were gatekeepers for the NHS and they aimed not to
refer to secondary care until they were left with no option. They seemed less aware of
the role of primary care and how some conditions could be managed by GPs. This
contributed to the feeling the people did not feel empowered to ask the GP for what
they wanted and even if they did, felt they would not be listened to. It was felt that
doctors had a role, akin to that of religious leaders, in health and wellbeing and were in
a position of status in the community and as such it did not matter what gender or
ethnicity healthcare professionals were as their role transcends these considerations
even when there were language worries.
With regards to health, members of the South Asian community felt illness was out of
their hands and that the role of the individual in maintaining their health was not widely
recognised. Overall, people were pessimistic about ill health, and felt that even if they
made efforts in one area, there are so many illnesses that this would be impossible
overall. Generally, ill health was associated with stigma and this could limit access to
healthcare professionals, with individuals trying to hide their health problems. There
was agreement that people should be informed about any risk factors they had for ill
health. It was mentioned that screening, or preventative medicine, should only apply to
those illnesses that can be cured. However, many would prefer not to know about the
health challenges they were facing regardless of the potential for treatment. The role of
God was important in keeping well and there was recognition of modern medicine and
techniques but modern medicine and religion worked in tandem, with God the final

141
arbiter. It was felt that attitudes in the community were changing and people were
becoming more aware of their health but that perhaps this did not yet quite extend to
preventative medicine.
THEME 5: STIGMA
Stigma was mentioned frequently in all focus groups. It was associated with ill health
generally rather than CVH specifically and this led to a ‘culture of silence’ in the
community making people try to hide their illnesses at times even from close family
and resulted in reluctance to seek medical attention. This was felt particularly true of
men, who were still seen as the providers for the family and so made them reluctant to
seek medical attention. The stigma often led to social isolation where people could be
viewed as a risk to others. However, this was balanced with others stating the illness,
not the person, was to be avoided but that others would need to take care. Some
members of our FG did feel they would stay away from someone who was unwell. The
stigma of ill health was particularly pronounced where it was felt lifestyle factors
contributed or caused the illness. There was the concept of being untouchable where
social isolation would mean all but close family would stay away from the patient, and
there was concern the stigma around them could extend to the whole family. This was
particularly true where the illness was thought of as potentially fatal. Others did
disagree and said now attitudes are changing and that sensible precautions should be
taken but there was recognition the person is already suffering and should not be
isolated as this can lead to the person giving up and becoming more quickly unwell.
There was particular fear around the idea of jaundice due to this being seen as a terminal
condition with no hope for recovery. Stigma was felt to be related to lack of knowledge.
Overall, there was silence around ill health where information was divulged only when
it was serious and could not be hidden any longer, but perhaps this is true in many other
communities.
COMMUNITY ADVICE ON OUR PROJECT:
The key topic discussed was the importance of imparting knowledge. Many of the
negative issues we found related to lack of knowledge. This would also enable people

142
to feel more hopeful. It was felt important the film should be positive to further create
hope and address the concept of futility around ill health and CVH specifically. There
should also be mention of why SA particularly need testing and the consequences of
delayed diagnosis. The approach should be simple and not too medical particularly with
language problems, so that people could understand and then spread knowledge within
the community. It was felt that it is important to have personal stories of people affected
and there should be cultural congruency with this. The ethnicity of any healthcare
professionals was not deemed important. However, the diagnostic pathway should be
explained as should the nature of testing. It was felt that the film should appeal to
females as they were seen as key figures in drawing in whole families and in word of
mouth dissemination of information which was felt to be of prime importance in this
community. People felt both Urdu and English should feature to draw in most people
and prevent exclusion particularly in older people who were felt to be more comfortable
with Urdu.
Regarding where in the community would be ideal to show such a film, primary care
and religious venues were prominent as they were felt to be the hub of this community
with community centres mentioned specifically for females. Despite the views noted
above on primary care, it was still felt important to use these venues. A summary of
these outcomes is shown in Figure 23.
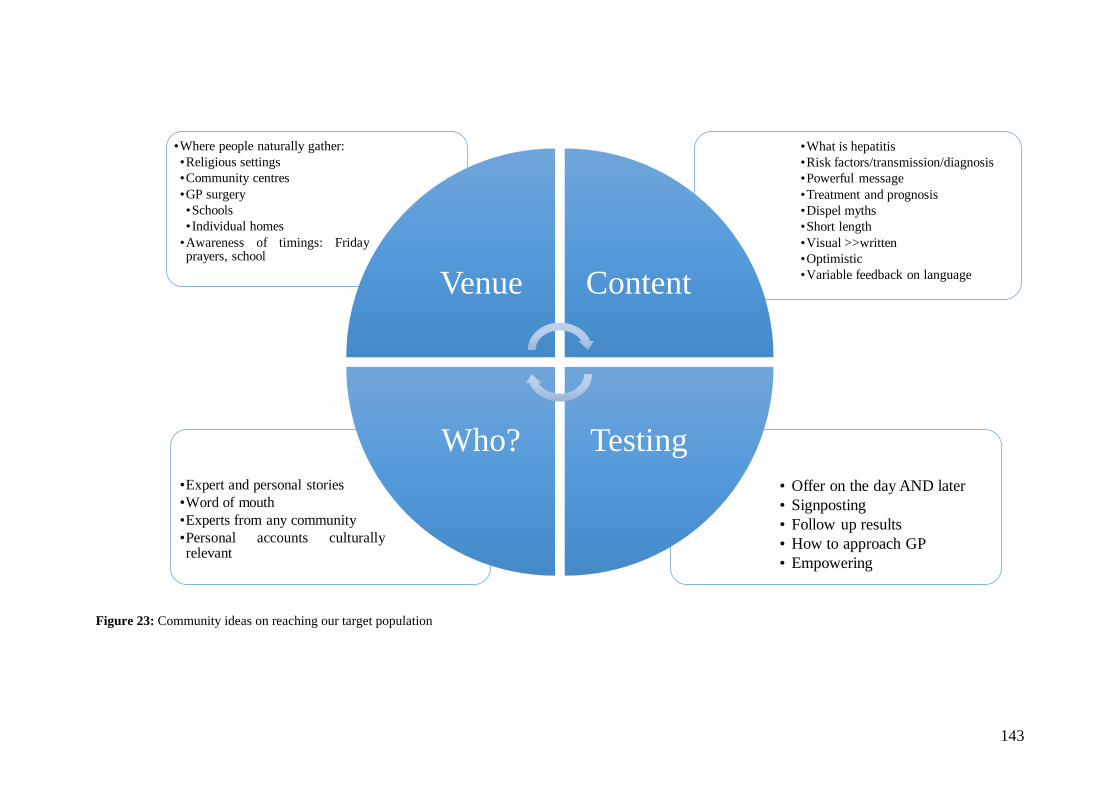
143
Figure 23: Community ideas on reaching our target population
• Offer on the day AND later
• Signposting
• Follow up results
• How to approach GP
• Empowering
•Expert and personal stories
•Word of mouth
•Experts from any community
•Personal accounts culturallyrelevant
•What is hepatitis
•Risk factors/transmission/diagnosis
•Powerful message
•Treatment and prognosis
•Dispel myths
•Short length
•Visual >>written
•Optimistic
•Variable feedback on language
•Where people naturally gather:
•Religious settings
•Community centres
•GP surgery
•Schools
• Individual homes
•Awareness of timings: Fridayprayers, school
Venue Content
TestingWho?
144
CHAPTER 8: FILM DEVELOPMENT FROM FOCUS GROUP
RESULTS
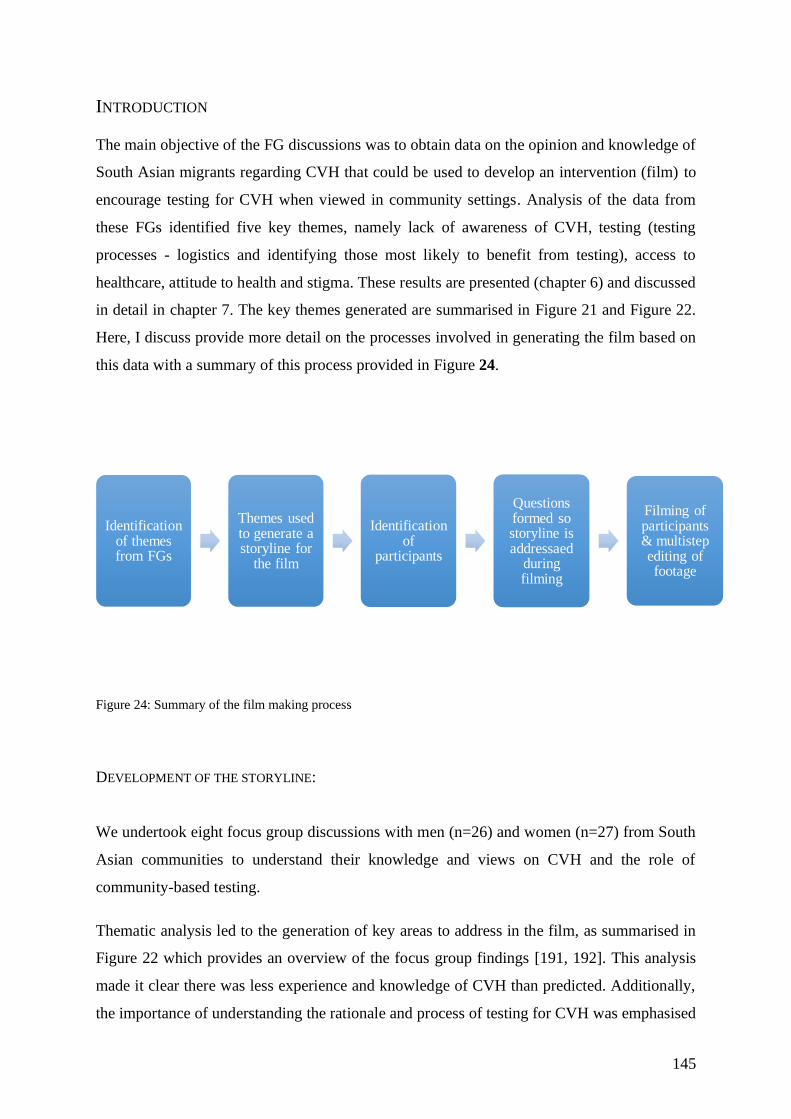
145
INTRODUCTION
The main objective of the FG discussions was to obtain data on the opinion and knowledge of
South Asian migrants regarding CVH that could be used to develop an intervention (film) to
encourage testing for CVH when viewed in community settings. Analysis of the data from
these FGs identified five key themes, namely lack of awareness of CVH, testing (testing
processes - logistics and identifying those most likely to benefit from testing), access to
healthcare, attitude to health and stigma. These results are presented (chapter 6) and discussed
in detail in chapter 7. The key themes generated are summarised in Figure 21 and Figure 22.
Here, I discuss provide more detail on the processes involved in generating the film based on
this data with a summary of this process provided in Figure 24.
Figure 24: Summary of the film making process
DEVELOPMENT OF THE STORYLINE:
We undertook eight focus group discussions with men (n=26) and women (n=27) from South
Asian communities to understand their knowledge and views on CVH and the role of
community-based testing.
Thematic analysis led to the generation of key areas to address in the film, as summarised in
Figure 22 which provides an overview of the focus group findings [191, 192]. This analysis
made it clear there was less experience and knowledge of CVH than predicted. Additionally,
the importance of understanding the rationale and process of testing for CVH was emphasised
Identification of themes from FGs
Themes used to generate a storyline for
the film
Identification of
participants
Questions formed so storyline is addressaed
during filming
Filming of participants & multistep editing of footage
146
by the community and so an explanation of CVH its transmission, diagnosis, testing and
treatment were required. This was broken down to key information domains (listed below) with
question formed for the film participants for each aspect.
It was also clear the community valued a story telling narrative with real life examples of people
with cultural congruency describing their experiences. As well as hearing from someone who
tested positive, they felt it was important to include the perspective of someone testing negative
and someone with a late diagnosis. Due to difficulties recruiting a patient currently on therapy,
a patient who had completed therapy was included. These stories were interspersed with expert
testimony (SA female and male Hepatology consultants). Due to the overlap in SA languages,
it was decided that the film would be in Urdu with English subtitles as well as an English
language version.
KEY DOMAINS TO BE COVERED IN THE FILM:
1. Knowledge domains aiming to correct widely held
misunderstandings on CVH:
a. What CVH is
b. Dispelling common myths that arose in FGs
c. Transmission and risk factors
d. Natural progression with emphasis on silent nature of this illness
e. Treatment availability
2. Testing:
a. Access to testing
b. What testing involves
3. Stigma
a. Focus on improving awareness will lessen stigma
4. Access
a. To develop confidence in understanding how to access services
b. Addressing language barriers
5. Personal stories:
a. Ease of testing
b. Silent nature of disease
c. Consequences of later diagnosis

147
d. Addressing potential impact on the family
IDENTIFICATION OF PARTICIPANTS FOR THE FILM:
Initially, it was thought there would be experience of CVH in focus group participants and they
would be invited to participate in the film. As this was not the case, an ethics amendment was
submitted to allow me to approach patients in our hepatology outpatient clinic.
Focus group data showed there was value placed on real-life stories as well as expert opinion,
and that people identifiable as South Asian would make the message more impactful. It was
decided the following people identified from liver clinic as well as experts would meet these
criteria:
1. One male and one female expert to appeal to the broadest audience.
2. Patients:
a. One tested for CVH who was negative,
b. One with previous CVH complicated by hepatocellular carcinoma (HCC) and
subsequent liver transplant,
c. One positive for HCV who has finished treatment and is now cured without any
sequelae.
Experts were previously identified as established hepatology consultants practicing in the NHS
and of South Asian origin. Both experts had involvement in this study and were aware of the
aims and results of the focus group discussions.
On the basis of this, the experts and participants were filmed, each of whom generated around
60-90 minutes of recordings. Filming was done individually and open questions relating to
each domain above were asked and recorded. The questions were deliberately open to make
verbal responses more natural on film and to avoid a question and answer type of setting. These
various film extracts were then transcribed allowing grouping of statements by theme and
according to our objectives with any duplicate information removed and any new issues
addressed. This cycle was completed multiple times. The most appropriate and impactful
statements for each domain were identified and highlighted for inclusion in the film. Some
features (such as explaining the nature of CVH were better delivered by certain participants, in

148
this case experts). A first draft of the film was then created and subsequently edited for content
and flow. This was then repeated until a final version was created which was shown to
stakeholders, our PPI group and a validation cohort (cohort 3) to ensure understanding and
suitability of language. It was also ensured that all participants were in the final version for a
similar amount of time, to ensure all voices were heard. Voice overs were used on the advice
of our film maker for consistency.
The finished film was a mixture of two hepatology experts explaining what CVH is, modes of
transmission and how to access testing. Additionally, the film included the testimonies of first-
generation South Asian migrants with experience of testing for CVH, including those who
tested negative and those who tested positive and who have been treated. The film addressed
the knowledge, concerns, cultural facilitators and barriers towards testing that were identified
in the focus group discussions [192]. The film was 12 minutes long and two versions were
produced, one in Urdu with English subtitles and the other in English and these can be viewed
online (English: https://youtu.be/K3AYyZ3uHro; Urdu with English subtitles:
https://youtu.be/dapPV4oul9s).

149
SECTION C: STUDY 2 A NOVEL EDUCATIONAL
INTERVENTION TO IMPROVE THE UPTAKE OF TESTING FOR
VIRAL HEPATITIS IN SOUTH ASIANS: A FEASIBILITY STUDY
150
CHAPTER 9: FEASIBILITY STUDY: METHODS
151
INTRODUCTION
This second study utilised the culturally and linguistically tailored educational film, produced
in study one on the basis of focus group data, as the basis of an intervention to encourage CVH
testing amongst UK-based South Asians. To the best of my knowledge there is no data on the
effect of an educational film in promoting case-finding in CVH.
TRIAL DESIGN
This is a feasibility study for a pragmatic RCT to assess the effectiveness of a novel educational
film in increasing testing for CVH in a high-risk population (South Asians) in a community
setting.
The objectives of this second study were to:
1. Determine the feasibility of recruiting South Asian migrants to view a short educational
film on CVH.
2. Determine the success of this educational intervention in promoting the uptake of
testing for CVH in various community settings familiar to our target population.
3. Identify methodological issues to inform acceptability and format of a definitive
randomised controlled trial which will assess the efficacy of our novel educational
intervention
For this feasibility study the following were criteria for success:
a. Monitor patient consent, recruitment and retention rates for participants who attend the
screening of the film and who consent to be tested to inform future design and
methodological issues.
b. 40% (n=80) of participants watching the educational intervention will go on to be
tested. Previous pilot work in the area has shown that uptake of testing without an
intervention in community setting is 15-20% [193].
c. 90% of participants to see the educational intervention will complete the pre-film
questionnaire
d. 80% of participants will complete the post-film questionnaire
e. Feasibility methodological procedures, including collating data relating to patient
152
experience of completing the questionnaires, and assessing patient feedback.
1. Study population
From February to June 2018, community centres, religious venues or primary care surgeries
were identified as potential recruitment sites. The target population was first generation South
Asian migrants aged over 18 years who could speak either English, Urdu or Hindi. The criteria
for South Asian was self-identifying as such. Those people aged less than 18 years, those
unable to consent and those failing to meet the inclusion criteria were excluded. These criteria
were deliberately broad to maximise the reach of our educational programme. Initially,
recruitment was based at sites in Surrey, South East England, UK. Due to concerns about
potential contamination of sites in this area, particularly from those who participated in the
design of this intervention, recruitment was widened to other centres i.e. Hounslow, London,
and the London Boroughs of Wandsworth and Merton.
The national Ethics approval process highlighted the fact that we were providing healthcare
education and so it was not felt appropriate to exclude anyone from viewing the film. Those
not matching study criteria were able to view the film but not recruited to provide research data
nor included in the analysis.
2. Regulatory Approvals
This study received ethical approval from the National Health Service Health Research
Authority (17/LO/0881) and was adopted on to the NIHR hepatology clinical trials network
portfolio (CPMS ID 34774). It was registered as a clinical trial, ISRCTN: 18001753.
3. Recruitment to film screening
Recruitment to this study was across three types of community domains namely religious
venues, community centres and primary care facilities. Guidance was sought from Public
Health England, who aided in the identification and approach to pivotal individuals and
organisations as well as key community-based sites to use as a recruitment base. Initial contact
from multi-lingual members of the research team was made with a key member of each target

153
site (e.g. religious leader) to explain the nature of the study and determine interest in
participation as a recruitment venue. When agreement to participate with individual sites was
reached, the research team visited each venue to outline the project aims and further develop
community links. Participant information sheets in English and Urdu were delivered and a
suitable area to show the film identified.
An advertising campaign within each recruitment site promoted the film screening event in
conjunction with community leaders at each site. The community leaders were faith leaders in
religious venues (e.g. Imam), primary care physicians or community link workers who
organised social gatherings in our selected venues.
Two weeks prior to the date of scheduled film screening, multilingual posters were displayed
in each venue advertising a health educational event and providing contact details for the
research team. Further advertising depended on the type of venue:
a. Religious venue: The religious leader announced the event at key attendance times,
including main prayers sessions e.g. Friday for those participants of Muslim
background.
b. Community venue: The community centre organiser announced to the regular attendees
of the group that there was a health education event and a date announced.
c. Primary care: Health care staff identified patients who attended their facility from our
target population and distributed the participant information sheet and a leaflet
containing research team contacts as well as the date of film screening.
On the date agreed with each key site, I organised a healthcare educational event. The research
team explained the nature of the work and collected initial epidemiological data e.g. country
of origin and age group to determine eligibility for this study. After consenting, participants
completed a baseline proforma (see appendix 3) which included knowledge of CVH, attitude
to CVH testing as well as any prior diagnosis or treatment for CVH and information on
potential risk factors for infection. I obtained consent at the start of the film viewing session
with the research assistant available to facilitate translation if required to ensure valid informed
consent. Consent was obtained as per Good Clinical Practice standards.
154
To facilitate the effective running of sessions, a minimum of 10 people were initially required
for each event. In order to manage potential requests for blood testing we planned to limit
attendance to 30 for each individual event. I planned events to run until the target recruitment
of 200 was reached. However, it was difficult to manage the planned numbers at each event
as participants generally turned up on the day without prior contact. This meant group sessions
had variable attendance (range n=1-80). I did not set a lower limit of attendance as it was felt
inappropriate to cancel events at late notice and would diminish the trust the research team
build up with the community.
After the film, I discussed with participants the possibility of testing for viral hepatitis. This
was a simple announcement mentioning an offer of testing by way of a finger prick blood test
then or at a later point. Thereafter, time was allocated for participants to ask any questions. It
was made clear that not testing is a choice and that this does not require any explanation from
the participant.
Following NICE guidelines [3], I utilised Dried Blood Spot testing (DBS) previously
successfully used in studying viral hepatitis in British-Chinese and British-Asian populations.
DBS testing entails a sample taken using a commercial kit that involves placing a drop of blood
on a prepared card. The sample provided will be tested for:
1) HCV antibody and
2) Confirmation of positive results
3) HCV RNA
4) HBV surface antigen
5) HBV core Antibody
I informed the participants that they can approach us in a separate area if they wish to discuss
the possibility further otherwise they were free to leave. Participants interested in testing were
given the opportunity to discuss individually with the research team and ask any questions.
There was reiteration of an option to test on the day and an option to come back at a later date
for testing for those who need more time to consider their decision. There was then an
explanation of how results will be given. I explained all Dried Blood Spot testing (DBS) testing
cards will be returned to the testing laboratory on the day of testing and not stored in the trust
or by the research team.
155
Separate testing rooms for women and men were offered and there were appropriately trained
voluntary health care advocates who speak Urdu and Hindi. Measures were taken to ensure
that participants giving informed consent do not feel coerced by the involvement of any
community or religious leaders.
4. Pre and post film questionnaires
To assess the effectiveness of the film, and to determine baseline opinion on CVH, pre- and
post-film questionnaires were distributed to those who viewed educational film to assess for
any change in knowledge and attitude to CVH testing.
Questionnaires were designed using a combination of externally validated existing questions,
as well as those designed for this study including knowledge of CVH, prior experience, utility
of the film and intention to test (see appendix 4). Answers were provided on a five point Likert
scale, from strongly disagree to strongly agree.
5. Chronic Viral Hepatitis (CVH) Testing
As this study was community based, finger prick testing using dried blood spot (DBS) testing
kits were utilised. These kits test for Hepatitis B surface antigen (HBsAg), Hepatitis B core
antibody (HBcAb), Hepatitis C (HCV) antibody and HCV RNA, and have high sensitivity and
specificity [194]. Each sample was tested in an accredited NHS laboratory, with results
available within 7-10 days.
DBS testing has been validated in health studies. It is recommended in national policy,
particularly where conventional phlebotomy may be challenging, with reported sensitivity and
specificity rates for HBsAg, HBcAb and HCV Ab close to 100% [36, 166, 195]. Genotyping
and HCV RNA testing can also be performed on DBS kits, with high levels of concordance to
conventional serology [196]. Internal validation data from the Central Manchester laboratories
who performed our tests is provided in Table 15.

156
Test Sensitivity % Specificity %
HCV Antibody 100 (96.5-100) 100 (97.6-100)
HCV RNA 100 (95.1-100) 100 (96.1-100)
HBsAg 100 (96.4-100) 100 (97.5-100)
Anti-HBc 87* (79.2-92.7) 100 (97.1-100)
Table 15: Sensitivity and Specificity of the DBS test kit
*100% in HBsAg +, 87% in HBsAg –
Testing was offered to participants immediately after the film was shown in a separate private
area of the venue. A return visit to the venue was scheduled for a week later, if the number
testing was not manageable on the day or if any participants wanted more time to consider
testing. Where there was oversubscription I tested as many as feasible on the day and arranged
to return the following week. This happened in two venues, one community venue and one
religious.
Testing was consented for separately by me (written informed consent) in private. Translators
were available (Urdu and Hindi from the research team with Bengali help from community
workers) if required. The consent process involved agreement on how the test results would be
given and specific consent for informing their usual primary care physician.
All patients completed a proforma that included preferred method of contact. I explained results
will be available 14 days after testing. We felt that if only those who test positive are informed
of the results in person this will be noticed by the community and make the process difficult
for those who test positive. When positive results needed to be given we ensure all participants
were given opportunity to ask questions and have an explanation of the findings. Consent will
be taken to inform their usual GP. There was also an explanation of the onward referral to
hospital-based services for further assessment with a view to treatment. The patient were
offered a referral to Royal Surrey County Hospital viral hepatitis service unless they express a
preference for another site. The Royal Surrey County Hospital is the lead site for HCV
Operational Delivery Network (ODN) and will coordinate their care.

157
6. Statistical analysis
The target sample size of 200 was derived to provide an estimate of the proportion seeking
testing following the intervention, with suitable precision, and provides for a half-width of a
95% confidence interval for this proportion in the region of 6-7% over a wide range (20-80%)
of possible values for this proportion.
As this is a feasibility study, the results are reported as mainly descriptive statistics. Participant
characteristics are presented by percentage for categorical variables. Two-sided 95%
confidence intervals, where applicable, were calculated using StataIC 15.1 (Statacorp LP,
College Station, TX).
CONTRIBUTIONS
I ran recruitment sessions, identifying sites, advertising sessions and facilitating attendance of
participants. At the recruitment events I consented the participants for the film screening as
well as blood testing and gathered demographic and questionnaire data. All data were analysed
by me with the supervision of a statistician (Professor Skene, University of Surrey).
158
CHAPTER 10: FEASIBILITY STUDY: RESULTS
159
RESULTS
A total of two hundred and twenty-one participants were recruited to view the educational film,
across fourteen different venues. Two participants were excluded as they did not meet the
inclusion criteria (not first generation migrants). Therefore, two hundred and nineteen were
included in the study (see Figure 25). The majority were recruited from religious (n=112; 51%)
or community settings (n=98; 45%), and a minority from primary care (n=9; 4%).
GENERAL CHARACTERISTICS
Demographic details, including age and highest educational attainment, were collected for
study participants and are illustrated in Table 16. There were similar numbers of females
(n=117) and males (n=102) who viewed the educational film. The majority were older adults
(61 years of age or older). Younger adults (18-24 years of age) were particularly under-
represented. The largest group of participants were originally from India (47%) and Pakistan
(39%). There was no information available on educational attainment for around one fifth of
the cohort, but otherwise the cohort had completed high school (29%), college (27%) or
university (14%). Smaller numbers received professional training (9%).
TESTING FOR CVH
One hundred and eighty-four of the two hundred and nineteen (84%) participants tested for
CVH after viewing our film (Figure 25). The overall proportion of participants testing for CVH
was similar across all types of site and is shown in Figure 27. Testing uptake was similar among
males and females (86% and 82% respectively). Testing uptake appeared to be lower in
younger age groups (less than 40 years) but interpretation of this is limited by the relatively
few numbers in these age groups and is reflected in the wide confidence intervals. Testing did
seem lower in Bangladeshi population than Indian and Pakistani (76%, 86% and 82%
respectively). This could again relate to the smaller cohort of Bangladeshi participants as
determined by the large confidence intervals. However, with retrospect, the film could appear
more focussed to India and Pakistan with the use of language and people in the film. There did
not appear to be any association with educational attainment and testing.

160
RESULTS OF PRE- AND POST-INTERVENTION QUESTIONNAIRES
Of the two hundred and nineteen who viewed the educational film, 78% (n=170) completed
the pre-intervention questionnaire with 70% (n=153) completing the post-intervention
questionnaire. A questionnaire was judged completed if any question was answered pre and
post film. However, many of the questionnaires had missing data points for individual
questions either not answered at all or answered only pre or post film therefore having no
comparator. Data were available for 65% (n=143) who filled in both questionnaires. This
overall sample is skewed to those who tested, with 82% (n=118) of questionnaire replies
coming from those who tested for CVH. However, this is in keeping with the fact that a similar
percentage of participants who viewed the film requested CVH testing. Of the 219 watching
the film, 39 (18%) did not complete either questionnaire (87% of whom tested for CVH and
13% who did not).
Given only a small group of participants did not go on to take up testing, combined with the
missing data points in those questionnaires that were completed, there is limited information
which can be gathered from this data. A detailed breakdown of the replies to each question in
tabular form is provided for reference in appendix 5 with an overview of findings of note
provided below.
Despite the limitations of the questionnaire data, some trends emerged. Very few (1%) of those
who replied disagreed that the film was useful with an 88% response rate to this question.
Regarding finding the film easy to understand, there was a 92% response rate with 90%
agreeing (90% tested; 88% non-tested). Most people agreed the film was relevant to them
(77%) which was similar for both cohorts.
Some questions did have a high response rate, including where participants were asked if they
should do what they can to remain healthy, even when busy with life tasks. All participants
agreed with this sentiment, with <5% not responding. Similar results were seen when asked
whether health checks are important even when well, with few invalid responses (<5% each
group). Of the valid responses, the vast majority agreed (100% tested and 96% non-tested).
High response rates were also seen when asked whether healthcare in the local community was
preferable to travelling to a hospital, with the majority of respondents in both groups (60%)
161
agreed they preferred local community based healthcare. Similar proportions (60% tested; 63%
non-tested) felt it was the doctors role to tell them what to do for their health. This is in keeping
with results in study 1, where the FG participants emphasised the role of their doctor above
themselves in health decisions.
Participants were also asked to rate their confidence in understanding what CVH is. One
hundred and twenty participants responded (85%), with a similar proportion responding
whether they tested for CVH or not. Overall, knowledge was unchanged pre- and post-film in
31% (n=37). Knowledge improved (from either neutral/not confident to confident) post-film
in 58% (n=70). Participants did recognise CVH can cause severe health problems, with 80%
recognising this, with few invalid response rates (8% tested and 8% non-tested). This was a
key message of the film.
Few patients had any personal experience of CVH (n=8; 7% in the tested group and n=1; 4%
in the non-testing group). This was in keeping with findings in our focus group work.
Results of CVH testing
Of the n=184 who tested for CVH having viewed the film, sixteen (all from religious venues)
required a repeat test as the original result was inconclusive (equivocal result, smaller sample
size affecting sensitivity of the test) but opted not to have this done. As there was no clear result
of testing, I have excluded these participants from this analysis.
Fourteen (8.3%) of the one hundred and sixty eight who viewed the film and tested with valid
results had exposure to CVH (see Figure 28). We found a HBV exposure rate of 6.0% (n=10
including n=1 active infection) and HCV exposure of 2.4% (n=4). Active infections for both
HCV and HBV were 0.6% (n=1 for each).
There were no infections detected in primary care patients and no cases of HCV exposure in
community venues. There were, however, three cases of previous HBV exposure (HBcAb) and
one active (HBsAg) HBV infection. The three patients with HCV exposure were discovered
in religious venues and included one active infection. In addition, six patients were found to
have HBV exposure. All patients who were HBsAg surface antigen positive or had active HCV

162
viraemia were counselled and successfully linked to care and referred directly to their local
secondary care provider for further management and subsequent treatment.
Figure 25: Recruitment by type of site. The total number recruited to view the educational film, with
those excluded as not meeting study criteria are shown by type of venue
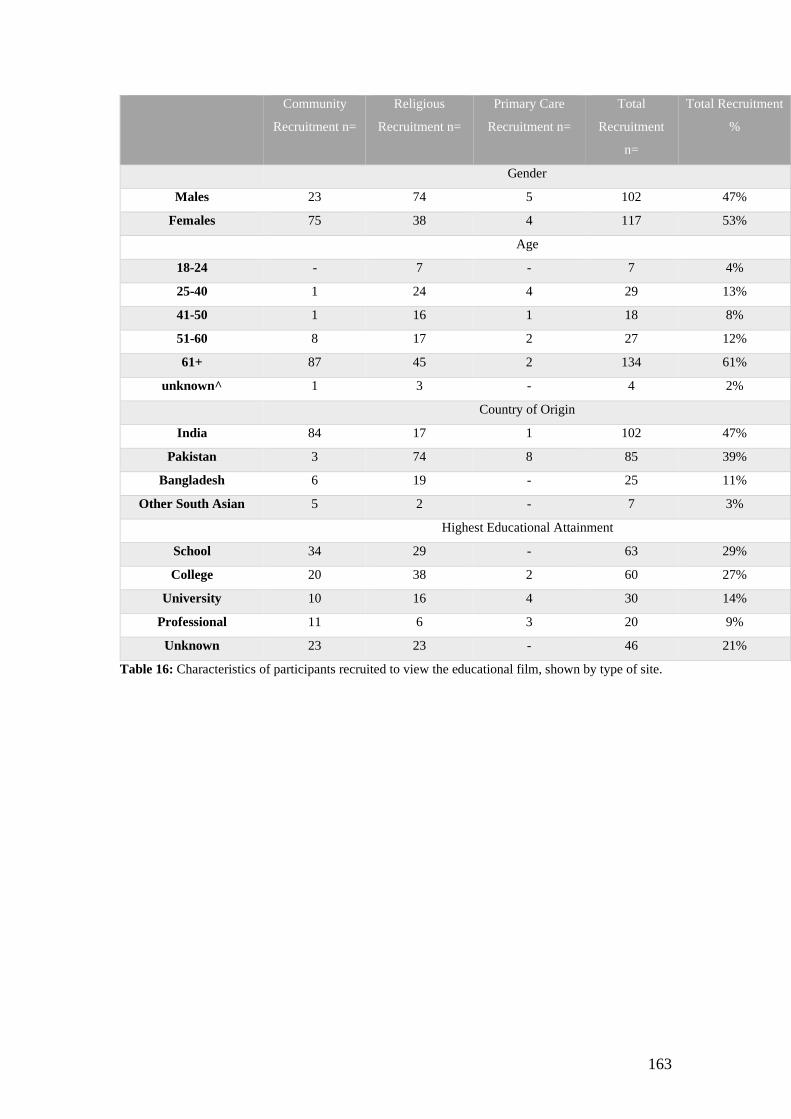
163
Community
Recruitment n=
Religious
Recruitment n=
Primary Care
Recruitment n=
Total
Recruitment
n=
Total Recruitment
%
Gender
Males 23 74 5 102 47%
Females 75 38 4 117 53%
Age
18-24 - 7 - 7 4%
25-40 1 24 4 29 13%
41-50 1 16 1 18 8%
51-60 8 17 2 27 12%
61+ 87 45 2 134 61%
unknown^ 1 3 - 4 2%
Country of Origin
India 84 17 1 102 47%
Pakistan 3 74 8 85 39%
Bangladesh 6 19 - 25 11%
Other South Asian 5 2 - 7 3%
Highest Educational Attainment
School 34 29 - 63 29%
College 20 38 2 60 27%
University 10 16 4 30 14%
Professional 11 6 3 20 9%
Unknown 23 23 - 46 21%
Table 16: Characteristics of participants recruited to view the educational film, shown by type of site.

164
Figure 26: Characteristics of those testing for CVH after viewing our educational film. This describes
the percentage tested by gender, age, country of origin and educational attainment. The 95% confidence
intervals are shown.
Figure 27: Proportion of participants testing for CVH after viewing the film by site, including the 2
sided 95% confidence interval
*97.5% one-sided confidence interval
0
10
20
30
40
50
60
70
80
90
100
% T
este
d
Characteristics of those testing for CVH after viewing educational
film (%)
0
10
20
30
40
50
60
70
80
90
100
Whole Cohort Community Religious Primary Care*
% T
este
d
Testing for CVH by venue type (%)
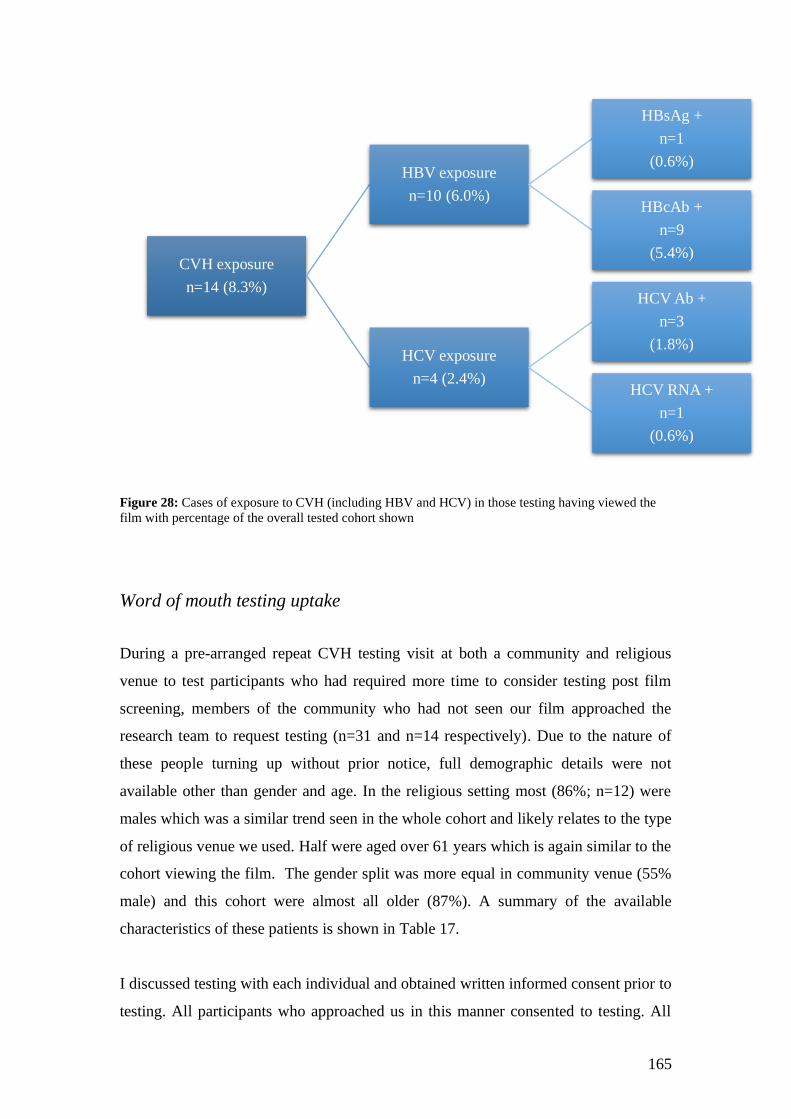
165
Figure 28: Cases of exposure to CVH (including HBV and HCV) in those testing having viewed the
film with percentage of the overall tested cohort shown
Word of mouth testing uptake
During a pre-arranged repeat CVH testing visit at both a community and religious
venue to test participants who had required more time to consider testing post film
screening, members of the community who had not seen our film approached the
research team to request testing (n=31 and n=14 respectively). Due to the nature of
these people turning up without prior notice, full demographic details were not
available other than gender and age. In the religious setting most (86%; n=12) were
males which was a similar trend seen in the whole cohort and likely relates to the type
of religious venue we used. Half were aged over 61 years which is again similar to the
cohort viewing the film. The gender split was more equal in community venue (55%
male) and this cohort were almost all older (87%). A summary of the available
characteristics of these patients is shown in Table 17.
I discussed testing with each individual and obtained written informed consent prior to
testing. All participants who approached us in this manner consented to testing. All
CVH exposure
n=14 (8.3%)
HBV exposure
n=10 (6.0%)
HBsAg +
n=1
(0.6%)
HBcAb +
n=9
(5.4%)
HCV exposure
n=4 (2.4%)
HCV Ab +
n=3
(1.8%)
HCV RNA +
n=1
(0.6%)
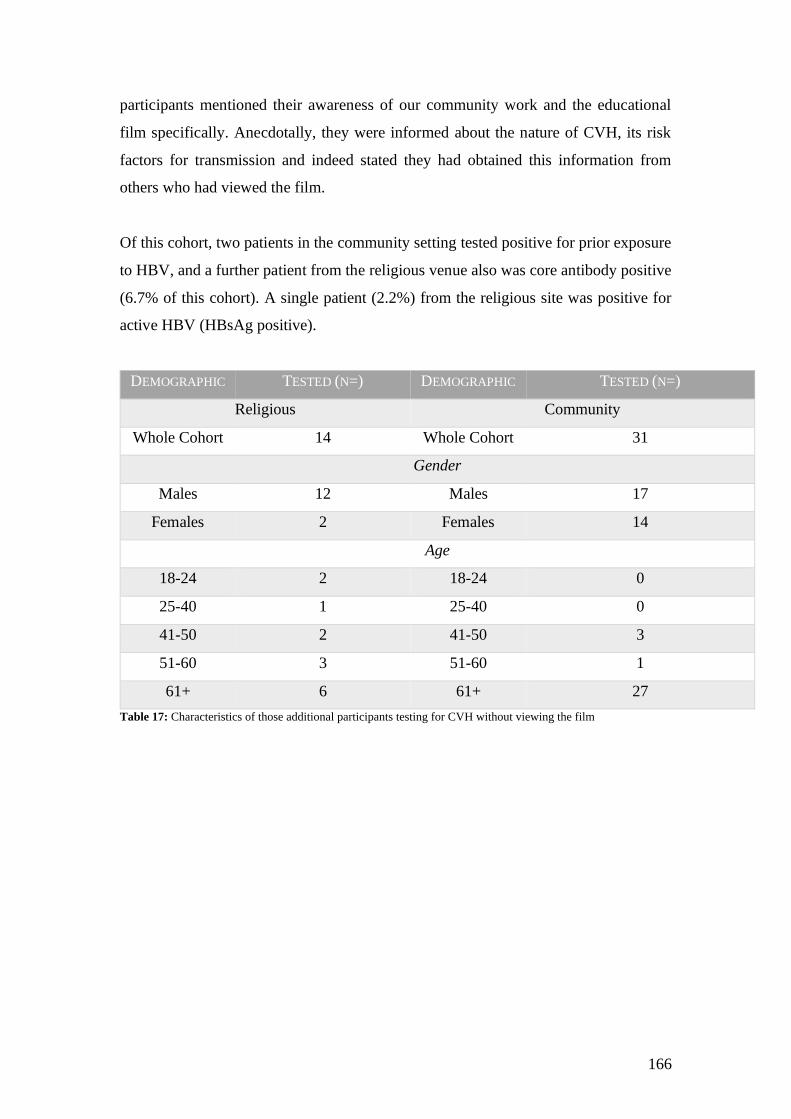
166
participants mentioned their awareness of our community work and the educational
film specifically. Anecdotally, they were informed about the nature of CVH, its risk
factors for transmission and indeed stated they had obtained this information from
others who had viewed the film.
Of this cohort, two patients in the community setting tested positive for prior exposure
to HBV, and a further patient from the religious venue also was core antibody positive
(6.7% of this cohort). A single patient (2.2%) from the religious site was positive for
active HBV (HBsAg positive).
DEMOGRAPHIC TESTED (N=) DEMOGRAPHIC TESTED (N=)
Religious Community
Whole Cohort 14 Whole Cohort 31
Gender
Males 12 Males 17
Females 2 Females 14
Age
18-24 2 18-24 0
25-40 1 25-40 0
41-50 2 41-50 3
51-60 3 51-60 1
61+ 6 61+ 27
Table 17: Characteristics of those additional participants testing for CVH without viewing the film

167
CHAPTER 11: FEASIBILITY STUDY: DISCUSSION
168
PRINCIPAL FINDINGS
1. FILM VIEWING AND TESTING UPTAKE
The South Asian migrant population in the UK represent a higher-risk group that are
often unaware of their risk for CVH. This study demonstrated the feasibility of reaching
the target audience and recruiting individuals from South Asian populations to view a
short educational film on CVH in community venues, with subsequent uptake of CVH
testing and treatment if required.
A marker of the success of this study was in recruiting over 200 people to view the
educational film. This number was pre-determined as part of the statistical analysis as
being able to provide an estimate of the proportion seeking testing following the
intervention with suitable precision. Additionally, the criteria for success whereby 40%
(80 people) who viewed the film would get tested for CVH was far exceeded.
The study targeted inner city areas (London) that were relatively deprived as well as
more affluent suburban areas of South-East England (Surrey) and did not find any
difference in ability to recruit to view the film nor uptake of testing for CVH. A
particular success of this work was in recruiting female participants to the film
screening as well as testing for CVH, as females have previously been under-
represented in other work [11, 122].
Whilst there was recruitment across a variety of religious venues, these were mainly
mosques and males were over-represented. On the other hand, the community venues
were mainly older Indian people. However, it was notable that recruitment in the
primary care arm was challenging compared to the other types of venue, with only 4%
of recruited patients in this arm. This may reflect a weakness in study design as
recruitment in this arm was different to the other two cohorts where recruitment was
led by the study team. In primary care, we relied on health care professionals
identifying potential participants (SA people) and distributing patient information
sheets without discussion of the nature of the study. This included a date and time for
film screenings. This meant no one from the study team could discuss at the time and
the onus was on participants to contact us without prior meeting. It was also not clear

169
how many people did receive the information and given appointment times in primary
care are short there may have been time constraints in distributing the study material.
Furthermore, patients attending primary care surgeries may have had other concerns
over their health at the time or the clinician may have felt raising the topic of a clinical
trial not appropriate (e.g. patients attending receiving a cancer diagnosis).
The majority (86%) of the people recruited to view the film were from either India
(47%) or Pakistan (36%). The other main group recruited were from Bangladesh (11%).
Both genders were well represented with 53% of those recruited to view the film
female. The recruitment of females was a particular target for this study as they have
been under-represented in other work [11]. Those recruited to watch the film were
mainly older people, with 61% aged 61 years or more. This is at odds with the census
data in Surrey and London which shows that those aged over 65 represent a smaller
proportion of the Asian population than younger age groups [74].
Whilst there did not appear to be any relationship between film venue, gender or level
of education and decision-to-test, age appeared linked. However, the study population
was skewed towards relatively older participants. This is likely due to some of the
recruitment sites being clubs for retired people and meetings often being held in the
week during day time when younger people may have childcare or work
responsibilities. There was an apparent lower uptake of testing in younger age groups
(57% for 18-24 year olds and 66% 25-40 year olds) compared with the cohort as a
whole (84%). However, the small numbers viewing the film in these age range (n=7;
n=29 respectively) precludes robust statistical inference.
Whilst a smaller proportion of those viewing the film were from Bangladesh (11%),
this cohort did seem to have less uptake of subsequent testing at 76%. Whilst this figure
is still high, it may be the focus of the film, particularly linguistically, is towards those
of Indian or Pakistani heritage and so there was less identification with it amongst those
from Bangladesh.
Notably, a number of participants (n=45) requested testing for CVH without having
seen the educational intervention. This may suggest other factors including community
170
endorsement may be relevant in deciding to test. Anecdotally, these participants had an
understanding of the risk factors for CVH and had knowledge of the wider work we
had been doing in the community. This was ascertained at the point of consent for
testing. Whilst possible the offer to test was taken up independently of the information
in the educational film, our experience in this study tells us that word-of-mouth spread
of information in this community appears critical and reasons given to test by these
participants included the film and its content.
2. QUESTIONNAIRE DATA
Of the two hundred and nineteen who viewed the educational film, 78% (n=170)
completed the pre-intervention questionnaire with 70% (n=153) completing the post-
intervention questionnaire, which was less than our pre-determined criteria for success
(90% and 80% respectively).
Whilst assistance was provided in either English or Urdu, the volume of paperwork
overall (consent forms, demographic information and questionnaires) was burdensome
to the participants and this will need to be addressed in the design of further studies.
The questionnaires were poorly filled out in terms of proportion of participants
completing pre and post to allow for comparison and also gaps with individual
questions not being answered and this limited data analysis and interpretation. This was
compounded by the small number of participants not testing after viewing the film.
With retrospect, the questionnaire was too long in an attempt to gather data on a variety
of parameters that were felt relevant to participants decision making as part of this study
such as attitude to health and healthcare, stigma and awareness of CVH. It was felt that
these domains may influence decision to test. Whilst the problems outlined here mean
that it was not possible to provide robust analysis of the questionnaire data, there were
some broad trends that were noted. There were some questions that were well filled out
and where the responses were consistent. An example is when asked about whether it
was important to do what they could to protect themselves from illness there was a high
171
response rate, over 95% of the whole cohort. This, and the strong preponderance to
agreeing with this sentiment, whether participants tested or not, suggests a degree of
proactivity and personal responsibility towards health. Alongside this, similar results in
terms of high response rates and high proportions of both tested and non-tested cohorts
agreeing with the importance of regular health checks even if feeling well were seen.
These findings, however, are at odds with our focus group data in study one about
regular health checks when asymptomatic. This could represent a selection bias, with
those attending a health education event self-selected as those who make effort to
safeguard their health.
Attitudes to healthcare provision and healthcare professionals were also explored as
they were raised as a key theme in study 1. Firstly, most people were in favour of
healthcare in the local community rather than hospitals. This was asked to ensure any
lack of uptake of testing for CVH after our film was not related to the community based
setting we used. Similarly most people agreed it was the role of the doctor agreed it was
to tell them what to do for their health.
Previous testing for CVH may well affect testing in this study and so this was asked
specifically. Unfortunately, the low levels of response, alongside the small numbers not
testing it is not possible to provide analysis of this.
Some topics had been structured to include multiple questions e.g. transmission, each
requiring a response. At each point there were many invalid responses and I wonder
whether this related to confusion on how to fill out the questionnaire with people
perhaps thinking they were to fill out only one section or the ‘most correct option’.
In order to check the validity of the questionnaire we included questions on the ease of
filling it in. Overall, most people did not report problems. Whilst some people changed
their mind after the film, I wonder if this is related to the knowledge aspects and feeling
more knowledgeable after, as most people who changed their mind changed to say they
did not have difficulties.
Regarding the film itself, all but one of the valid responses found the film useful. The
invalid responses were at the lower end of what we saw across all questions. Most also
172
found the film easy to understand and felt it relevant. It is possible this question was
not filled in honestly as the research team were present but given the very high uptake
of testing, this seems less likely.
3. RESULTS OF TESTING
Of the n=184 who tested for CVH having viewed the film, sixteen (all from religious
venues) required a repeat test as the original result was inconclusive (equivocal result,
smaller sample size affecting sensitivity of the test) but opted not to have this done. As
there was no clear result of testing, I have excluded these participants from the results
analysis. However, this is an important group in terms of emphasising the need for
adequate sample size being obtained in large volume events and to understand why
these participants did not have a repeat test. Those with a smaller sample size came
with a result of negative but with a description sensitivity may be affected by the small
sample size. There is no quantification of the effects of this and this concept can be
difficult for people to understand. Perhaps this effect is amplified by them feeling well
and attending a screening test and the presumed negative test was good enough for
reassurance. It is also possible that these people got retested elsewhere e.g. primary care
and we are unable to determine this.
Fourteen (8.3%) of the one hundred and sixty eight who viewed the film and tested with
valid results had exposure to CVH (see Figure 28). We found a HBV exposure rate of
6.0% (n=10 including n=1 active infection) and HCV exposure of 2.4% (n=4). Active
infections for both HCV and HBV were 0.6% (n=1 for each).
There were no infections with either HBV or HCV detected in primary care patients,
although as noted previously the sample size was very small. There were no cases of
HCV exposure in the community venues. There were, however, three cases of previous
HBV exposure (HBcAb) and one active (HBsAg) HBV infection.
The three patients with HCV exposure were discovered in religious venues and
included one active infection. In addition, six patients were found to have HBV
exposure. All patients who were HBsAg surface antigen positive or had active HCV
viraemia were counselled and successfully linked to care. However, this proved to be
173
time intensive and if there were higher numbers of positive patients this would have
proved challenging to manage.
Regards the participants who approached us for testing without viewing the film (word
of mouth cohort), three were hepatitis B core positive and one had active HBV
infection. Again, this patient was linked to care. This cohort demonstrates the value of
community based research, particularly with community members as key stakeholders.
Word of mouth spread of information is important in this community. It is possible the
involvement of community leaders added validation to our presence. Positive
experience of the film events spread quickly and did rapidly lead to more people testing.
SUMMARY OF FINDINGS
1. Understanding of CVH
Based on the results of the focus group work in study 1, it was apparent there was less
awareness of CVH in this community than we hypothesised. This was apparent across
multiple domains including knowledge on what CVH is, its distinction from jaundice
as well as the potential asymptomatic nature of infection. Unsurprisingly, this was
associated with a lack of awareness of the increased risk of CVH infection in South
Asian people. In particular there was misunderstanding about CVH being a condition
of poor sanitation and was spread through the faeco oral route. This, and the fact that
there are potential ongoing risk factors for CVH acquisition were the key messages of
the film. Whilst this was not a trial designed to assess the effectiveness of the film in
promoting testing for CVH, there was a higher than predicted uptake of testing. It is not
necessarily the case that this film provided knowledge to the extent it became the sole
factor for people testing, however, there were improvement in knowledge parameters
after the film. Furthermore, whilst recognising the issues with the questionnaire, there
was a positive response to the question asking whether the film was useful.
As the film provided education on the risk factors for infection acquisition, it may be it
has ongoing advantages out with testing per se for ongoing risk management for those
who viewed the film. Also, it cannot be ascertained whether some of those who did not
174
test with us spoke to other healthcare providers such as their own GP for advice on risk
or indeed testing.
A particular feature notable through this work in the SA community across all sites was
the role of word of mouth spread of information and the value this had for people. It
would therefore seem possible that knowledge gained will spread more widely in the
community beyond just those who viewed the film. I believe we saw evidence of this
in those who came forward for testing despite not having seen the film. When
consenting these people it was clear they had knowledge of our work as well as
knowledge of the particular messages given in the film.
While not strictly relating to understanding of CVH specifically, it was clear not all
people in this study had an understanding of healthcare access and provision in the UK
and this film provided some information on this which could have reach beyond the
scope of this project by improving health literacy in general. The health belief model
has been used to guide health promotion and disease prevention programs. This model
defines the key factors that influence health behaviours as an individual's perceived
susceptibility to illness, belief of consequence or severity of illness, the potential
benefits and barriers to action and self-efficacy i.e. confidence in their ability to
succeed.
2. Willingness to engage in community-based activities
Overall, the South Asian population were willing to engage with community based
healthcare. This was reflected in not only successful recruitment for both the film and
subsequent testing, but also in the links established with community and religious
groups in both phases of this work. In both the earlier focus group and subsequent
feasibility study trial participants valued care in their local community. Whilst many
stated a willingness to travel where required it was felt more favourable in logistics,
cost (financial and time) and engagement to provide care in familiar settings. Many
participants felt this was more important in migrant groups, where some people may
struggle to navigate traditional healthcare and travel and this was not purely a language
issue. It was repeatedly mentioned that when feeling well any strategy to promote
175
engagement would need to consider patient convenience particularly for people with
work and family commitments. Conceptually, therefore, community based healthcare
whether screening, case-finding or even engagement with healthcare professionals
should improve access. By tailoring the venues used to those culturally relevant to each
population and thus having familiarity can also have a role in improving the confidence,
comfort, engagement and ultimately improved experience of patients which has
potential to improve other health related metrics.
Recruitment was successful in both affluent and more deprived regions. However,
recruitment in primary care was poorer than non-traditional community healthcare
settings. This is somewhat at odds with the expressed views in both studies that a major
role of doctors is to tell people what to do for their health and in recommending testing
if needed. I believe the method of recruitment in primary care, being distinct from other
venue types, is a confounder for these results. Exploring alternative methods would be
important and I do not think there is enough data to preclude primary care venues from
being a recruitment venue in future work.
A particular success of this work was in recruiting female participants to both the focus
groups and the film screening as well as testing for CVH, as females have been under-
represented in other work [11, 122]. This was possible with the help of community
volunteers helping identify venues and groups set up specifically to help new female
migrants such as English language classes held during school hours. These volunteers
also promoted our studies within their social and family networks through word of
mouth.
The study cohort was skewed towards older participants. Whilst this may mean our
studies did not have the same reach to younger people, this is not certain. An alternative
explanation would be recruitment occurring during daytime where younger people are
working. On the occasions where recruitment was at weekends there were more
younger people present proportionately than daytime during the week.
Whilst engagement with both studies was good, there was an issue in study two with
paperwork. This was felt to be burdensome. The paperwork consisted of a consent form
for viewing the film, demographic information, pre and post film questionnaires and
176
consent form for testing where relevant. In retrospect, the pre and post film
questionnaires were too long and some questions were misinterpreted. Initially, the
questionaries were designed to encapsulate key domains – knowledge, efficacy,
attitudes to healthcare, experience of testing and intention to test. Whilst this would be
useful data, the time taken to complete was off putting especially to older people. This
resulted in failure to meet the pre-defined target for questionnaire completion. There
were also many invalid responses within each questionnaire i.e. part completed and
many answers incongruous with outcomes e.g. stating they will never be tested and
testing on the day. However, there were some questions with high response rates that
did yield meaningful results, simplifying these questionnaires would potentially create
more complete therefore meaningful data.
A key factor in both these studies was recognising the effect of word of mouth spread
of information in this community. Discussion within the community about our work
was crucial to recruitment. This was done through personal networks but also through
existing groups and clubs. This, in my opinion, is a contributing factor for the poor
recruitment in primary care where the study was advertised by a healthcare professional
handing an information sheet to potential participants. The spread of information
between community members was particularly apparent amongst those venues where
we returned to complete further testing where demand was high. On each occasion
where we revisited a site, we gave a date a week in the future and saw high levels of
attendees requesting testing. Many of these were people who had viewed the film the
week before but as discussed many had not attended to see the film but were aware of
its key messages. Thus, community involvement though PPI and stakeholder initiatives
will be mandatory for future studies in this community.
3. Conducting a feasibility study using a short educational film, that could form
the basis for an RCT.
This feasibility study generated useful results. Overall, recruitment to view the film
and subsequent testing were higher than predicted. There were, however, areas where
adaptation of study methods and pathways could be adapted in order to facilitate the
design of a randomised control trial of the effectiveness of this educational film in
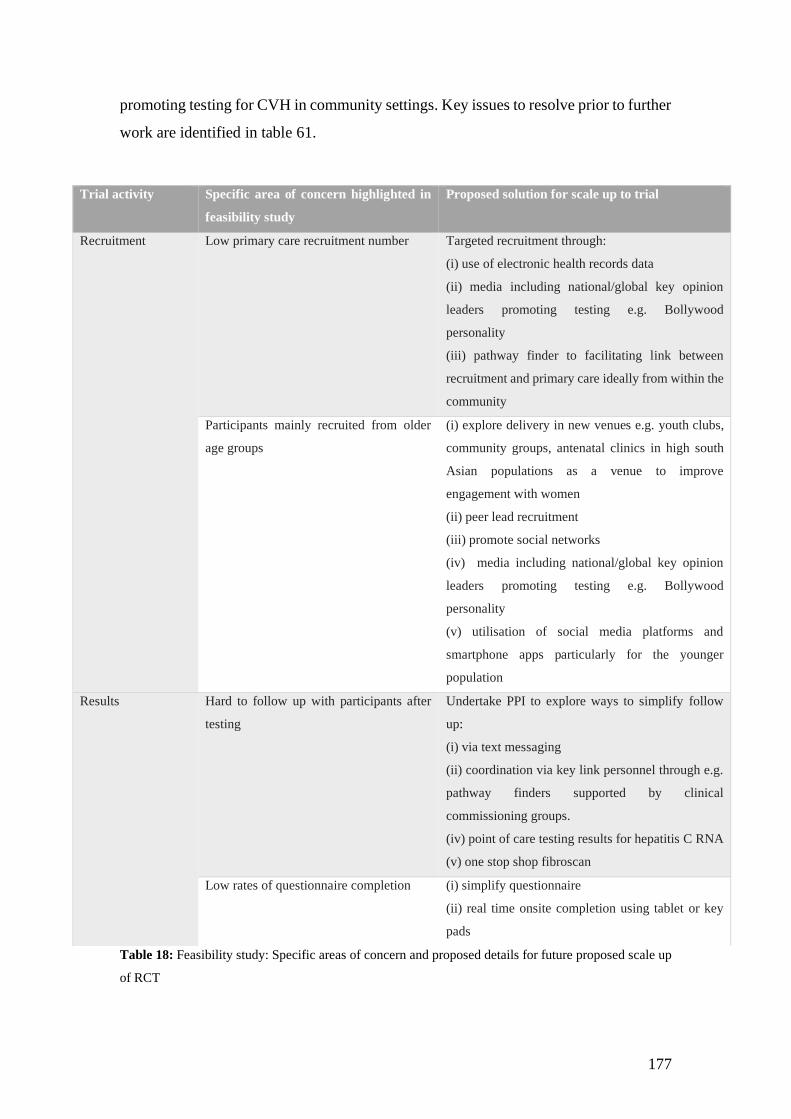
177
promoting testing for CVH in community settings. Key issues to resolve prior to further
work are identified in table 61.
Table 18: Feasibility study: Specific areas of concern and proposed details for future proposed scale up
of RCT
Trial activity Specific area of concern highlighted in
feasibility study
Proposed solution for scale up to trial
Recruitment Low primary care recruitment number Targeted recruitment through:
(i) use of electronic health records data
(ii) media including national/global key opinion
leaders promoting testing e.g. Bollywood
personality
(iii) pathway finder to facilitating link between
recruitment and primary care ideally from within the
community
Participants mainly recruited from older
age groups
(i) explore delivery in new venues e.g. youth clubs,
community groups, antenatal clinics in high south
Asian populations as a venue to improve
engagement with women
(ii) peer lead recruitment
(iii) promote social networks
(iv) media including national/global key opinion
leaders promoting testing e.g. Bollywood
personality
(v) utilisation of social media platforms and
smartphone apps particularly for the younger
population
Results Hard to follow up with participants after
testing
Undertake PPI to explore ways to simplify follow
up:
(i) via text messaging
(ii) coordination via key link personnel through e.g.
pathway finders supported by clinical
commissioning groups.
(iv) point of care testing results for hepatitis C RNA
(v) one stop shop fibroscan
Low rates of questionnaire completion (i) simplify questionnaire
(ii) real time onsite completion using tablet or key
pads
178
COMPARISON WITH EXISTING LITERATURE
Given the poor health related outcomes for patients with liver disease, there are efforts
to find cases that have previously been undiagnosed. Chronic viral hepatitis is one of
the most common aetiologies of liver disease and therefore case-finding is a national
and international priority. In the UK, NICE advocates community-based testing of
populations at higher risk for CVH but do not make recommendations on how this is
best achieved due to a lack of clear evidence.
1. Screening Uptake
The existing literature on interventions to improve participation in healthcare screening,
of which case-finding is a subgroup, principally relates to cancer diagnoses [45]. Many
programs actively promote screening by utilising resources to facilitate uptake and
offering financial incentives (e.g. free testing in healthcare systems with direct charges
to patients) [134]. Despite the removal of logistic and financial barriers, uptake of
screening tests often remains suboptimal. This does mirror health service uptake in
general with pockets of the population showing poorer coverage [114]. Across
screening programs there are identified logistical, psychological and cultural barriers
and their importance in health behaviour is recognised [138]. Arguably, these factors
are more important in screening where there is a lack of driver to seek health care as
the population targeted is asymptomatic. BAME groups are more likely to have lower
attendance at various screening programs as well as a poorer experience of care in both
the UK and USA [139-146] . Attempts to improve uptake have been made by instituting
various interventions, often based on single screening modalities or single populations
(i.e. akin to case-finding) [147-149].
2. Recruitment to Clinical Trials Aiming to Improve Uptake of Screening
The largest community testing program based in New York City, the BfreeNYC
project, undertaken between 2004 and 2008 tested almost 9000 migrants (mainly of
Chinese and Korean descent) for HBV. This was a large-scale program advertised
179
extensively including through major media outlets and championed by city councillors.
Stigma was not reported from the wider community during the advertising process, and
indeed members of the Asian community associated less stigma towards viral hepatitis
because of the awareness-raising programme [172, 173]. This suggests raising
awareness through education has wider ongoing benefits than pure case-finding.
Whilst our studies do not have a control (i.e. non-intervention arm), we found high
levels of participation in our work. The reasons for this cannot be elucidated from our
data but could include the familiarity people had with our earlier work in study 1 where
trust was built within the community [191] and resultant word of mouth spread within
the area, the convenience of using local facilities and in particular facilities know to
study participants (e.g. their own places of worship), the advertisement of events as
healthcare education (there was no initial mention of testing) and perhaps key the
involvement of SA people of ‘standing’ within the local community such as community
workers who provide English classes and advertising by religious leaders at prayers.
The help given by community workers was mainly in advertising the event to people in
the community through their networks and classes. They also attended most of the film
screenings but as participants rather than identifiably as members of the research team
and did not administer any aspects of the studies. We believe their role was key to
providing the research team access to the community and adding trust but feel their role
was distinct from the lay health workers often used in studies albeit with some overlap.
3. Types of Intervention
Existing data on improving healthcare screening has limitations in large part due to
heterogeneity of methods and a lack of rigorous assessment of the interventions used.
There are, however, some important findings in the literature particularly where the
focus is on interventions to improve uptake of screening in specific subgroups of
populations with lower uptake, rather than increasing general screening rates [147].
Furthermore, a substantial amount of the data available comes from North America
where financial and organisational factors are not in keeping with those in the UK. In
general though, it would appear culturally relevant interventions along with those that
minimise logistical difficulties have the most effect [147]. As part of this work, I have
performed a systematic review of interventions to improve screening uptake amongst

180
ethnic minorities [151]. There was little UK data as was also the case in other reviews.
The heterogeneity of groups and methodology of trials poses a challenge in analysing
the data available. However, I still found themes when reviewing the data by type of
intervention. As seen in previous studies, multifaceted interventions were broadly
successful as were group-education sessions and media interventions. Apparently less
successful were lay-health worker (LHW) interventions; despite being the most
common intervention type. This is in keeping with our findings that was culturally
tailored group education via a film, based in local community settings. Whilst we did
have community workers aid in recruitment, this role was distinct from LHWs in these
studies.
Given LHWs are often from the community being studied and are therefore aware of
cultural and local factors at play the idea seems appealing in studies of the type we
carried out. A meta-analysis of interventions to promote HBV testing where nearly half
(7/15) of studies analysed utilised LHWs. Six of the seven LHW-led interventions were
one off activities that delivered educational content tailored to a particular community’s
cultural and social context [169, 175-180]. All studies found LHW-led educational
interventions had a positive effect on self-reported rates HBV screening (RR = 2.68, CI
95; 1.82–3.93) compared to no HBV specific educational interventions; however, the
results were heterogeneous in study design and intervention setting (three were home
visits, and three were delivered at a community-based organisation). The LHWs in all
six studies received training to help tailor the educational intervention which was
relatively simple and low cost. Analysis found the interventions acceptable to the study
participants and to the LHWs. While the importance of cultural context in developing
interventions to improve HBV screening in high-risk populations and the usefulness of
community settings in the delivery of healthcare is important, the low-cost nature of
this intervention could facilitate its used in resource limited settings. However, these
LHW studies rely on self-report of testing and do not report on results of testing. The
accuracy of this is not established. Additionally, all the studies in this meta-analysis
were conducted in North America and it is not clear whether this data would be
transferable to the different healthcare system in the UK. However, in future work of
this type it may be valuable to further develop the role of the community workers we
used to assess their role as LHWs as the low-cost nature of this could be rolled out at
scale. I do feel there remains a role for physician input in studies of this type, and our

181
presence did add credence even in the focus group work that was not directly medical.
4. Community Based Testing
A community based UK study that used an outreach testing intervention that provided
education on HCV that also aimed to investigate the prevalence of HCV in a migrant
Pakistani population did report difficulties recruiting target numbers, particularly
struggling to recruit females with 85% of recruited patients male despite attempts to
target the female population [11]. Other UK based studies targeting SA people
recruited in mosque and community centres but similar to our work, it is unclear how
many people were reached by the advertising campaign and whilst the majority of those
attending did get tested, this may represent a selection bias as it may be those already
interested in health screening or hepatitis attended [161][162].
In the UK, community-partnership approaches have been tested in the South Asian
community, utilising religious settings such as Mosques or Temples to increase uptake
of testing for CVH [121]. The support of religious leaders in delivering testing in these
venues seems to be important as testing was offered to 5000 SA people identified
through attendance at Mosque directly by research teams and not religious leaders, with
no uptake of testing [121, 163].
This effect with religious leader involvement has been seen in other faiths including the
Egyptian Coptic community and the Korean Christian community in North America,
resulting in higher levels of CVH testing than seen out with religious venues [164, 165].
In the UK, similar studies in the Chinese community have used established community
venues, churches and local wholesalers to advertise testing, with testing uptake in
around 230 individuals (around 15 individuals per session) [166]. Again, this illustrates
the problem with identifying how many people an advertising campaign reaches.
However, an American study providing an HBV educational program utilised
community based participatory research in churches to raise awareness and promote
testing for HBV [169]. This showed a positive effect with 93% of the intervention group
were tested, with only 2.9% in the control arm tested at 6 months follow up [169].
182
5. Primary Care Recruitment
In all voluntary community-based approaches, self-selection bias is a common factor,
and it has been suggested that rates of infection may indeed be higher in those
individuals who do not take up such offers, due to co-morbid disease, or risk-activity
that makes them paradoxically reluctant to attend [121]. Additionally, for migrant
populations language and cultural factors may limit reach of whole population
advertisements. Whilst primary care testing in the UK is an alternative that may reach
out to these individuals, recent studies in West London have shown poor attendance
(10%) by members of migrant communities in specially prepared new-patient testing
sessions, despite an estimated local migrant prevalence of over 40% [160]. This low
uptake was also seen in East London where primary care databases were used to
identify migrants at risk of viral hepatitis. Identified patients were sent invitation letters
with information sheets in their native language and asked to attend for testing.
However, the trial was stopped early as only 2.3% took up this offer [181]. This mirrors
the recruitment challenges we saw in the primary care arm.
Given these difficulties, a range of different techniques have been utilised including
large scale recruitment drives of migrant groups in a study that tested almost five
thousand people for viral hepatitis at fifty-two different sites with oral fluid testing in
community venues. Some were approached in primary care waiting rooms whilst
attending for another reason as was the case in our study although they were directly
approached by the study team. However, the primary aim of this study was to determine
prevalence and as such interventions were not utilised [121]. Whilst this approach did
lead to some recruitment for their study, it was less successful than other community
venues used.
A more recent UK based study aimed to determine whether incentivising and
supporting primary-care physicians in areas with a high density of migrants increases
the numbers of adult migrants screened for viral hepatitis [182]. General practices were
randomly assigned to an opportunistic screening (control) group or to one of four
targeted screening (interventional) groups (standard or enhanced invitation letter based
either from standard (hospital) care or community-based care). In the control group,
general practitioners were given a teaching session on viral hepatitis and were asked to

183
test all registered migrants. In the intervention, GPs were paid a nominal sum for setting
up searches of records, reimbursed for signed consent forms, and supported by a
dedicated clinician. The primary outcomes relating to testing included the proportion
of those eligible who were sent an invitation letter in the intervention groups, the uptake
of viral hepatitis screening (in the intention-to-treat population) within 31 days of being
sent the letter and the proportion of patients who tested positive for viral hepatitis. Most
of the primary care centres that were approached participated (63 of 70). In the eight
control general practices, screening was taken up by 1.7% of eligible participants. In
the 50 general practices that used the intervention, screening was taken up by 19.5% of
eligible participants (p=0·014) and the intervention was cost-effective. Testing uptake
was similar for enhanced versus standard letters (p=0.26). The investigators conclude
that screening migrants for viral hepatitis in primary care is effective if doctors are
incentivised and supported. However, they found community care expensive without
evidence that it offered additional value and there was no additional value of bespoke
invitation letters over standard letters. It would seem, therefore, that primary care
recruitment can be successfully done but that the method used must be carefully
considered to recruit successfully and to be financially viable.
In the USA there has been success in using an electronic health record prompt to
primary care physicians to test Asian American patients for HBV versus a control with
no prompt showed an increase in testing order in the intervention group (40.9% v 1.1%)
with uptake in testing in the intervention group of 30 of the 36 requested patients [174].
It is not currently known whether this effect would be seen in a UK population within
the NHS. There are systems in our primary care databases that could make such
prompts possible.
6. Linkage to Care
Linkage to care for positive CVH cases is poorly documented in most studies, with high
rates lost to follow-up. As noted above, the largest study of this nature, the BFreeNYC
study, around 57% of trial participants were kept in services until the end of the 4 year
study [158]. Whilst we did link all positive cases to care, there were small numbers.
This was time and resource intensive and may pose challenges at scale and out with the
clinical trial setting. A robust mechanism will have to be in place to ensure all positive
184
cases have access to clinical care, advice and treatment.
7. Conclusion
In conclusion, chronic liver disease has been underestimated as a global public health
problem. There would appear to be a need for case-finding as it is a prevalent condition
that is silent in the early stages of disease. There is a need for effective global action
including education, prevention and early diagnosis for management and treatment to
prevent cirrhosis-related morbidity and mortality. Health literacy in liver disease
remains low, even in those who are known to have chronic liver disease [152]. This is
in line with our findings illustrating a lack of understanding on liver disease in general
as well as CVH specifically to include confusion amongst trial participants whether
they have had CVH or not.
At odds with much of the published literature, we found high levels of engagement in
a culturally and linguistically tailored educational program on CVH and subsequent
testing in a migrant population. To the best of my knowledge, this is the first time a
short, tailored film has been used to promote knowledge and testing of CVH in a BAME
population. Our study cohort addressed previous gaps where females were
underrepresented. However, in line with other studies primary care recruitment was
challenging and there remains a gap in the literature for how best to recruit in this
setting. We also confirm the low health literacy in liver disease in general and CVH
specifically. The role of LHW does have the potential to be further developed to
improve case finding in CVH in a cost-effective manner. The follow up rates in our
study were very high and whilst this is at odds with other literature it may be the small
numbers of cases allowed for an intensity of resource that may not be possible out with
the clinical trial setting or with a greater number of positive cases.
STRENGTHS AND LIMITATIONS OF THIS STUDY
Whilst recognising the feasibility nature of this study, I acknowledge a number of
limitations which provide useful lessons to consider for a future RCT to test the efficacy

185
of the intervention and in recruiting first generation migrants (see Table 18). Firstly,
Primary Care recruitment was unexpectedly poor, and identification of the specific
reasons for this would improve this dataset further and facilitate planning of further
studies. A possible factor was that patients were informed of the educational event when
attending an appointment with their health care provider and so may have had other
health concerns at that time unrelated to this study. A more systematic method of
identifying our target population via primary care records search, for example would
allow us to reach more participants and potentially improve recruitment. The method
of recruitment from primary care will be reviewed prior to this work being extended,
particularly considering other recent studies reporting higher levels of testing in this
area [183].
Secondly, many of our participants were from older age groups (aged 61+), reflecting
much of the recruitment came from community centres frequented by retired people.
Film screenings were also held in the evenings and at weekends to try to balance this
effect, and whilst we did recruit smaller numbers across other age ranges, our
population remains skewed towards older participants and so our results may not be as
applicable across other age groups. It is conceivable that younger migrants may be less
religious and less likely to frequent religious venues [19-20]. Additionally, religious
venues we utilised were mainly Mosques and there was a gender bias towards males
being recruited here. Future work should widen recruitment to include religious venues
of other faiths and more females.
Thirdly, we were unable to establish a baseline for recruitment to assess how many
participants opted to attend the film screening upon exposure to the advertising
campaign. The nature of this study was to advertise to existing groups of people
utilising the recruitment venues; thus it was not possible to specifically assess those
individuals who may have heard of this work but decided not to attend the screening
event. This limitation has been noted in other studies of this type as described in the
literature review. In part, we believe this was related to the feasibility nature of this
work and we have plans to address this in scale-up to a multi-site randomised trial.
Additionally, we used finger-prick DBS testing as this was logistically easier in the out
of hospital setting and appropriate for this study. However, results of these tests were

186
not available immediately and required further contact with the participants tested to
inform them of the results. A point-of-care test that could give immediate results could
lessen the time and logistical burden of this type of outreach work by removing the
need to re-contact all participants with the results, particularly given the nature of case-
finding work in CVH requires mass testing. This may also allow a one-stop treatment
clinic where fibroscan testing and on the day treatment could be possible. However,
careful consideration to maintaining confidentiality when given these results in the
community setting would be essential. A point of care result would also address the
issue where some people required a second confirmatory test and declined.
During the film screening events, it became clear the volume of paperwork was
burdensome. Additionally, there was some suspicion over the data we were gathering
and some reluctance to fill the questionnaires as they seemed lengthy and repetitive.
Some participants saw the knowledge domain as like an exam and were reluctant to fill
it out. Since this was a health education event for an underserved group, I did not
exclude anyone on the basis of reluctance to fill out paperwork. The only exception to
this was the consent for the DBS testing.
Despite these limitations, this study has significant findings that warrant further study
in a scaled-up randomised trial. Whilst there is some data on case-finding in higher-risk
minority groups these have mainly focussed on offering a single opportunistic testing
(such as those attending accident and emergency departments or utilising primary care
databases) of those already engaged with healthcare services [22]. This study utilised
the community itself to develop a novel educational intervention that provides
information to the community and the individuals within it on risk factors for CVH
acquisition as well as offering advice on how to obtain testing. This will help to address
the issue of reinfection and onwards transmission of CVH. A major issue in CVH
acquisition is vertical infection and so our success in recruiting female participants was
particularly important. Given the intervention we designed is culturally and
linguistically tailored to the South-Asian community we would hope that this film could
ultimately be widely available e.g. antenatal clinics in areas of high South-Asian
populations, if proven effective in a randomised trial to raise awareness of CVH and its
transmission. To the best of our knowledge there are no other studies examining the use
of a film to provide education as well as offering testing. This method, once fully

187
evaluated with a randomised trial, should be particularly useful in the real-world with
the ready availability of technology such as social media and file sharing sites.
A particular success of our work was in recruiting female participants, and those from
a lower socio-economic status to both the focus groups and the film screening as well
as testing for CVH, as females have been under-represented in other work [11, 122].
Additionally, we were able to provide testing and so did not rely on self-reporting which
is a particular issue with other studies. There is no data on the accuracy of self-reporting
and furthermore, we saw confusion amongst participants as to whether they had been
tested for CVH and so self-report represents a potential source of bias.
188
CHAPTER 12: CONCLUSIONS AND FUTURE WORK

189
These two linked studies successfully met their objectives and allowed us to gather
current ideas, knowledge and opinions on chronic viral hepatitis amongst South Asian
migrants through recruitment to a series of focus groups. These focus group discussions
also allowed identification of potential barriers to testing for CVH in the South Asian
community, and more generally any barriers and facilitators to accessing healthcare for
this population. Through analysis of the data gathered, five key themes emerged; lack
of knowledge on CVH, access to healthcare, testing for CVH, attitudes to health and
healthcare professionals and stigma (relating to ill health generally but not CVH
particularly). These themes were used to develop a structured message to produce a
culturally and linguistically tailored educational film on chronic viral hepatitis to be
shown in various community settings to promote testing for CVH. Additionally, a
questionnaire used both pre- and post-film was developed to aid the analysis of the
impact of the film. The SA community were willing to engage in community-based
activities and were receptive to our presence within the variety of community and
religious settings we visited. These studies did successfully address the NICE, NHS
England and WHO aim of offering testing, and indeed treatment, in areas familiar to
the migrant community.
The key metric of these studies was uptake of CVH testing after viewing a tailored
educational film. The uptake of testing (84%) far exceeded the criteria set as a marker
of success for this feasibility study at 40%. This is also far higher than is seen in other
studies aiming to test people for CVH, regardless of intervention type or nature of the
study. Despite this clear success, we noted some aspects that did not work as effectively
as intended. As such, there are lessons we have learned about elements of these studies
that could be refined in future work. Firstly, our recruitment revealed challenges with
the primary care arm and also in recruiting younger people. Primary care recruitment
was significantly more challenging than in the other venues. Plausible explanations for
this include the reliance on clinical staff opportunistically handing out the trial
information during consultations (the only recruitment not reliant on the research team).
It was not possible to track how many patients were approached. Additionally, it may
well be patients attending their surgery have other health concerns at the time that are
more pressing. Primary care could still be helpful in recruiting to studies, particularly
as the role of doctors being crucial in healthcare and access to service was highlighted
by the SA community throughout this work. It should be feasible to highlight studies
190
opportunistically in primary care such as posters in waiting rooms and short adverts on
the TV that are usually in waiting rooms. This advertising would create awareness of
the relevant health condition but may create bias in the trial setting and may be better
used for real world roll out of interventions once their effectiveness has been shown in
trial settings. Relying on the clinician to take time out of a short consult to give
information did not work well. However, research team presence in the waiting room
to advertise the study and potentially recruit does not tackle the issue of patients having
other health concerns as a reason for attending which would take priority. Therefore,
consideration should be made to targeting recruitment using electronic health record
data to identify eligible participants. Additionally, a pathway finder to facilitate a link
between recruitment and primary care ideally from within the target community could
be effective and we noted the success of a similar approach in recruiting to our focus
groups.
A further issue was the recruitment of younger people. This could well be because
younger people were either working or busy with family commitments during the day
when we were recruiting. Additionally, the venues we targeted were more commonly
used by retired people e.g. social clubs. We recommend a considered approach to
community venues used in these type of study to include new types of place such as
youth clubs or venues such as parent and baby groups. Peer led recruitment may be
helpful here, as the members of the community we worked with were older. However,
we hypothesis the most successful strategy would be through utilisation of social media
platforms and smartphone apps and promotion of the trial in social networks. This
would be particularly useful in this community where we have seen the effect of word
of mouth spread of information. It would also allow advertising in the native language
of target communities where this is not English.
Another issue for consideration is the follow up of new diagnosed cases. In our study,
all patients were linked to care either in our own centre or locally to them. The small
numbers of patients involved made this possible. However, each case was time
intensive and if there is a large volume of positive cases a robust system should be
developed. We did, however, contact all patients with their results although this was
quicker with negative cases. We recommend PPI involvement at an early stage to
determine how this will be done. This can be more complicated where there is language
differences. Possible solutions to this would be the use of point of care testing with
191
results available on the day. In the case of CVH, this could also incorporate other tests
such as Fibroscan. This would require strict confidentiality arrangements. If not
possible, exploration of digital media such as text messaging for patient apps for
negative tests (e.g. patient knows best) or utilisation of link personnel e.g. pathway
coordinators which may be more effective for elderly or non-English speakers.
A major issue identified was in completion of the questionnaire. This was intended to
provide data on key aspects of the film, particularly where uptake of testing was poor
to aid analysis of why this was the case. It was developed to assess for lack of self-
efficacy as a potential reason for not testing as well as assessing changes in knowledge
to ensure our key messages were delivered. Furthermore, determining who would be
important in delivering a message to get tested would be helpful if the film was not
effective in promoting testing. However, it is important to understand that there were
flaws with the questionnaire out with the low numbers not testing making the sample
too small to analyse. The questionnaires were too long, and some questions too complex
(multi-step questions). Additionally, it would have been simpler to take out some
questions for the post-film questionnaire from the pre-film version that were not
designed to change with the film but to assess characteristics of the individuals attitude
to their health. Overall, the concept was valid and simplification of the questionnaire
(both length and structure) as well as using digital methods such as key pads or tablets
to complete could be helpful, particularly where an intervention is less successful in
promoting testing.
The features of this work that contributed to its success were the engagement and
involvement of the SA population in all aspects, particularly notable the recruitment,
strategy (locations to recruit from and ideas on how to target the intervention to
maximum effect) and in developing the intervention itself. Providing education,
including more broadly on healthcare access as well as liver disease and CVH
specifically, with health literacy on CVH and liver disease itself lower than predicted.
However, identification of helped in generating key messages to be delivered by our
educational intervention. Given a particular issue was lack of awareness on
transmission, including this information in the film means that people can be made
aware of ongoing risks and take precautions were necessary and as such the film should
have benefits beyond pure case-finding. To address misconceptions on CVH we also
managed to impart more general information on liver disease. The film contained

192
information on accessing healthcare services and GP provision of free healthcare, it
was felt to be useful for those people new to the UK. Throughout both studies I saw the
importance of word of mouth spread of information for this community and so I feel
educational interventions will have potential benefits beyond that which can be
measured in a clinical trial setting. Female recruitment was a key target for this study,
and we were successful in this thus addressing a gap in the literature. This is particularly
important for some illness, like CVH, with vertical transmission. Additionally, by not
relying on existing healthcare databases e.g. primary care we could include those people
not already engaged with healthcare services.
Considerations for a scale up and future RCT in the UK will be driven by a robust
stakeholder committee to support roll-out. This strategy would include engagement
with key Public Health agencies, for example, Public Health England, the National
Screening Committee, Primary Care Networks and liver networks who would use this
film in their locality. Most importantly, the population itself will play an essential role
and engagement with them is necessary. This will require local hepatitis treatment
networks and secondary care sites being supported by community organisations and
faith leaders to set up screening and recruitment processes. Local Council Public Health
Teams, regional Public Health England teams and voluntary sector organisations will
need to be involved in discussions of how to deliver this sustainably.
Despite the limitations in our studies, the very high level of testing uptake leads us to
believe our work can provide a framework for researchers interested in case-finding
and indeed for targeted interventions generally. The main features are engaging with
the target community and developing the intervention in partnership with them by
determining existing knowledge of the relevant condition as well as determining the
barriers and facilitators to testing. This allows the intervention to be specific to the
condition and population being studied. We found further benefits in this partnership
with the community that built trust and engagement with our presence and undoubtedly
aided recruitment. This was noted with the word of mouth spread of information on our
study and the fact that people came forward to us as a result. This model would be of
particular benefit marginalised groups, where healthcare engagement can address some
of the barriers to healthcare more generally some communities face.
193
In the time between these studies finishing and the production of this thesis, we have
faced a global pandemic of covid-19 caused by infection with the Sars-Cov-2 virus. To
try to halt this pandemic, there has been recognition of risk factors for severe disease
and a recognition that BAME people are at a higher risk. The widespread reporting of
this in the mass media has really elevated public awareness of individual risk in
infective disease and in particular the link between ethnicity and risk. I believe some of
the lessons gained here would help in the development of interventions for BAME
communities relating to covid-19 and will further aid this work in promoting
recognition of BAME communities of the potential risk they may have in certain
illnesses.
In summary, we tested higher-risk first generation migrants (South Asian) for CVH,
detected positive cases and subsequently linking patients successfully to care. This
linkage to care is a fundamental factor in any intervention to improve testing rates for
CVH and we recommend robust plans are made for this in the design of any study of
this type. Equally, we believe it is important to test comprehensively for viral hepatitis
including previous Hepatitis B exposure, particularly as modern healthcare is
increasingly utilising therapeutic agents that carry a risk of HBV reactivation [23] and
we counselled our patients on this risk and informed their primary care physician.
We believe that the benefits of this study are three-fold. Firstly, in offering CVH testing
and thus potential diagnosis and treatment to a higher-risk group; secondly, providing
education to be shared more widely within the community and finally engagement of a
higher-risk group with community-based healthcare. Overall, we found a higher than
anticipated uptake of testing for CVH after viewing the educational film, however, the
feasibility nature of this study limits its ability to prove causation between the
intervention and subsequent testing.
The effectiveness of this study in promoting CVH testing has led to plans for an RCT
to further evaluate this intervention. If successful, this could be the basis of a model to
be utilised nationally and internationally in keeping with the emphasis on targeted case-
finding, in line with the WHO plan for global CVH elimination. More generally, we

194
have produced a model of how to generate a healthcare educational intervention that is
adaptable for other researchers to use for any health condition and population.
195
Publications Relating to the Thesis
1. Kelly, Pericleous, Ahmed, Vandrevala, Hendy, Shafi, Skene, Verma, Edge,
Nicholls, Gore, de Lusignan, Ala; Improving uptake of hepatitis B and hepatitis
C testing in South Asian migrants in community and faith settings using
educational interventions - a prospective descriptive study: International
Journal of Infectious Diseases doi: https://doi.org/10.1016/j.ijid.2020.08.059
2. Kelly, Pericleous, Hendy, de Lusignan, Ahmed, Vandrevala, Ala; Interventions
to Improve the Uptake of Screening Across a Range of Conditions in Ethnic
Minority Groups: A Systematic Review: Int J Clin Pract. 2018 Jun 19: e13202.
doi: 10.1111/ijcp.13202
3. Hendy, Vandrevala, Ahmed, Kelly, Gray, Ala; Feeling misidentified:
Understanding migrant's readiness to engage in health care screening. Social
Science & Medicine. 112481. 10.1016/j.socscimed.2019.112481.
4. Ahmed, Vandrevala, Hendy, Kelly, Ala; An examination of how to engage
migrants in the research process: building trust through an ‘insider’
perspective, Ethnicity & Health, 2019 DOI: 10.1080/13557858.2019.1685651
Conference Presentations:
1. Kelly, Pericleous, Ahmed, Hendy, Vandrevala, Mathew de Lusignan, Ala; A
Novel Educational Intervention for Chronic Viral Hepatitis (CVH) Case-
Finding in UK South-Asians, a High-Risk Population: Preliminary Results from
a National Institute for Health Research (NIHR) Feasibility Study AASLD The
Liver Meeting 2018
2. Kelly C, Pericleous M, Ahmed A, Hendy J, Vandrevala T, Mathew S, De
Lusignan S, Ala A; A novel educational intervention for chronic viral hepatitis
(CVH) case-finding in UK South Asians, a high-risk population: preliminary
results from a National Institute for Health Research (NIHR) feasibility study
BASL Annual scientific meeting 2018
3. Kelly C, Ahmed A, Pericleous M, Hendy J, Vandrevala T, Ala A; Factors
Preventing Testing for Chronic Viral Hepatitis (CVH) in UK South-Asians: A
Novel National Institute for Health Research (NIHR) Study in a High Risk
Group; AASLD Annual Meeting-The Liver Meeting 2017
4. Kelly C, Ahmed A, Pericleous M, Hendy J, Vandrevala T, de Lusignan S, Ala
A; Factors Preventing Testing for Chronic Viral Hepatitis (CVH) In UK South-
Asians - A Novel National Institute for Health Research (NIHR) Study to
Improve Recognition of CVH in a High Risk Population; BASL Annual
Meeting 2017
196
REFERENCES
1. Williams R, Aspinall R, Bellis M, Camps-Walsh G, Cramp M, Dhawan A, Ferguson J,
Forton D, Foster G, Gilmore I, Hickman M, Hudson M, Kelly D, Langford A, Lombard
M, Longworth L, Martin N, Moriarty K, Newsome P, O'Grady J, Pryke R, Rutter H,
Ryder S, Sheron N, Smith T. Addressing liver disease in the UK: a blueprint for
attaining excellence in health care and reducing premature mortality from lifestyle
issues of excess consumption of alcohol, obesity, and viral hepatitis. Lancet. 2014 Nov
29;384(9958):1953-97. doi: 10.1016/S0140-6736(14)61838-9. Erratum in: Lancet.
2014 Dec 20;384(9961):2212. PMID: 25433429.
2. Public Health England. The 2nd Atlas of variation in risk factors and healthcare for
liver disease in England: Reducing unwarranted variation to improve health outcomes
and value. September 2017. Available:https://fingertips.phe.org.uk/profile/atlas-of-
variation.
3. National Institute for Health and Care Excellence. Hepatitis B and C Testing: People
at Risk of Infection. 2012. Available: https://www.nice.org.uk/guidance/ph43
4. Zatoński WA, Sulkowska U, Mańczuk M, Rehm J, Boffetta P, Lowenfels AB, La
Vecchia C. Liver cirrhosis mortality in Europe, with special attention to Central and
Eastern Europe. Eur Addict Res. 2010;16(4):193-201. doi: 10.1159/000317248. Epub
2010 Jul 2. PMID: 20606444.
5. Mokdad AA, Lopez AD, Shahraz S, Lozano R, Mokdad AH, Stanaway J, Murray CJ,
Naghavi M. Liver cirrhosis mortality in 187 countries between 1980 and 2010: a
systematic analysis. BMC Med. 2014 Sep 18;12:145. doi: 10.1186/s12916-014-0145-
y. PMID: 25242656; PMCID: PMC4169640.
6. European Association for the Study of the Liver. HEPAMAP. A roadmap for
hepatology research in Europe: An overview for policy makers. Available from:
https://easl.eu/wp-content/uploads/2018/09/Hepamap.pdf
7. American Liver Foundation. The Liver Lowdown – Liver Disease: the big picture.
Available from:
http://www.liverfoundation.org/education/liverlowdown/ll1013/bigpicture. Last
accessed: March 2017.
8. Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, Roudot-Thoraval F. The
burden of liver disease in Europe: a review of available epidemiological data. J Hepatol.
2013 Mar;58(3):593-608. doi: 10.1016/j.jhep.2012.12.005. PMID: 23419824.
9. Cancer Research UK. Risks and causes of liver cancer. Available from:
http://www.cancerresearchuk.org/about-cancer/type/liver-cancer/about/risks-and-
causes-of-liver-cancer. Accessed May 2017.
10. Arase Y, Ikeda K, Chayama K, Murashima N, Tsubota A, Suzuki Y, Saitoh S,
Kobayashi M, Kobayashi M, Suzuki F, Kumada H. Fluctuation patterns of HCV-RNA
serum level in patients with chronic hepatitis C. J Gastroenterol. 2000;35(3):221-5. doi:
10.1007/s005350050334. PMID: 10755692.
11. Jafferbhoy H, Miller MH, McIntyre P, Dillon JF. The effectiveness of outreach testing
for hepatitis C in an immigrant Pakistani population. Epidemiol Infect. 2012
Jun;140(6):1048-53. doi: 10.1017/S095026881100152X. Epub 2011 Aug 19. PMID:
21854668.
12. Hyams KC. Risks of chronicity following acute hepatitis B virus infection: a review.
Clin Infect Dis. 1995 Apr;20(4):992-1000. doi: 10.1093/clinids/20.4.992. PMID:
7795104.
13. Foundation for Liver Research. Hepatitis B: Out of the Shadows; A Report into the
Impact of Hepatitis B onto the Nations Health. 2004. Available from:
197
https://www.liver-research.org.uk/liver-research-files/Hepatitis-B---Out-of-the-
Shadows.pdf Accessed May 2017
14. Waheed Y, Shafi T, Safi SZ, Qadri I. Hepatitis C virus in Pakistan: a systematic review
of prevalence, genotypes and risk factors. World J Gastroenterol. 2009;15(45):5647-
5653. doi:10.3748/wjg.15.5647
15. de Franchis R, Hadengue A, Lau G, Lavanchy D, Lok A, McIntyre N, Mele A,
Paumgartner G, Pietrangelo A, Rodés J, Rosenberg W, Valla D; EASL Jury. EASL
International Consensus Conference on Hepatitis B. 13-14 September, 2002 Geneva,
Switzerland. Consensus statement (long version). J Hepatol. 2003;39 Suppl 1:S3-25.
PMID: 14708673.
16. Fattovich G, Brollo L, Giustina G, Noventa F, Pontisso P, Alberti A, Realdi G, Ruol A.
Natural history and prognostic factors for chronic hepatitis type B. Gut. 1991
Mar;32(3):294-8. doi: 10.1136/gut.32.3.294. PMID: 2013423; PMCID: PMC1378837.
17. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current
and emerging prevention and control measures. J Viral Hepat. 2004 Mar;11(2):97-107.
doi: 10.1046/j.1365-2893.2003.00487.x. PMID: 14996343.
18. Lin KW, Kirchner JT. Hepatitis B. Am Fam Physician. 2004 Jan 1;69(1):75-82.
Erratum in: Am Fam Physician. 2004 Apr 15;69(8):1863. PMID: 14727820.
19. Alward WL, McMahon BJ, Hall DB, Heyward WL, Francis DP, Bender TR. The long-
term serological course of asymptomatic hepatitis B virus carriers and the development
of primary hepatocellular carcinoma. J Infect Dis. 1985 Apr;151(4):604-9. doi:
10.1093/infdis/151.4.604. PMID: 2982971.
20. Liaw YF, Sheen IS, Chen TJ, Chu CM, Pao CC. Incidence, determinants and
significance of delayed clearance of serum HBsAg in chronic hepatitis B virus
infection: a prospective study. Hepatology. 1991 Apr;13(4):627-31. PMID: 2010157.
21. European Association For The Study Of The Liver. EASL clinical practice guidelines:
Management of chronic hepatitis B virus infection. J Hepatol. 2012 Jul;57(1):167-85.
doi: 10.1016/j.jhep.2012.02.010. Epub 2012 Mar 20. Erratum in: J Hepatol. 2013
Jan;58(1):201. Janssen, Harry [corrected to Janssen, Harry L A]. PMID: 22436845.
22. Cornberg M, Wong VW, Locarnini S, Brunetto M, Janssen HLA, Chan HL. The role
of quantitative hepatitis B surface antigen revisited. J Hepatol. 2017 Feb;66(2):398-
411. doi: 10.1016/j.jhep.2016.08.009. Epub 2016 Aug 27. PMID: 27575311.
23. Alter MJ, Hadler SC, Margolis HS, Alexander WJ, Hu PY, Judson FN, Mares A, Miller
JK, Moyer LA. The changing epidemiology of hepatitis B in the United States. Need
for alternative vaccination strategies. JAMA. 1990 Mar 2;263(9):1218-22. PMID:
2304237.
24. Stevens CE, Beasley RP, Tsui J, Lee WC. Vertical transmission of hepatitis B antigen
in Taiwan. N Engl J Med. 1975 Apr 10;292(15):771-4. doi:
10.1056/NEJM197504102921503. PMID: 1113797.
25. Goh KT. Prevention and control of hepatitis B virus infection in Singapore. Ann Acad
Med Singap. 1997 Sep;26(5):671-81. PMID: 9494677.
26. Grebely J, Page K, Sacks-Davis R, van der Loeff MS, Rice TM, Bruneau J, Morris MD,
Hajarizadeh B, Amin J, Cox AL, Kim AY, McGovern BH, Schinkel J, George J,
Shoukry NH, Lauer GM, Maher L, Lloyd AR, Hellard M, Dore GJ, Prins M; InC3
Study Group. The effects of female sex, viral genotype, and IL28B genotype on
spontaneous clearance of acute hepatitis C virus infection. Hepatology. 2014
Jan;59(1):109-20. doi: 10.1002/hep.26639. Epub 2013 Nov 22. PMID: 23908124;
PMCID: PMC3972017.
27. Public Health England. Hepatitis C in the UK. 2013. Available:
http://www.hcvaction.org.uk/sites/default/files/resources/Hepatitis%20in%20the%20
198
UK%20-%202013%20Report%20%28Public%20Health%20England%29.pdf
Accessed July 2017
28. Benova L, Mohamoud YA, Calvert C, Abu-Raddad LJ. Vertical transmission of
hepatitis C virus: systematic review and meta-analysis. Clin Infect Dis. 2014 Sep
15;59(6):765-73. doi: 10.1093/cid/ciu447. Epub 2014 Jun 13. PMID: 24928290;
PMCID: PMC4144266.
29. Thein HH, Yi Q, Dore GJ, Krahn MD. Estimation of stage-specific fibrosis progression
rates in chronic hepatitis C virus infection: a meta-analysis and meta-regression.
Hepatology. 2008 Aug;48(2):418-31. doi: 10.1002/hep.22375. PMID: 18563841.
30. World Helath Organization. Combating Hepatitis B and C to Reach Elimination by
2030. 2016; Available from:
http://apps.who.int/iris/bitstream/10665/206453/1/who_HIV_2016.04_Eng.pdf?Ua=1.
31. Hahné SJ, Veldhuijzen IK, Wiessing L, Lim TA, Salminen M, Laar Mv. Infection with
hepatitis B and C virus in Europe: a systematic review of prevalence and cost-
effectiveness of screening. BMC Infect Dis. 2013 Apr 18;13:181. doi: 10.1186/1471-
2334-13-181. PMID: 23597411; PMCID: PMC3716892.
32. Ramsay M, Gay N, Balogun K, Collins M. Control of hepatitis B in the United
Kingdom. Vaccine. 1998 Nov;16 Suppl:S52-5. doi: 10.1016/s0264-410x(98)00295-3.
PMID: 9915036.
33. Department of Health UK. Getting ahead of the curve. Action to strengthen the
microbiology function in the prevention and control of infectious diseases
2002. Available
https://webarchive.nationalarchives.gov.uk/ukgwa/20120504020310/http://www.dh.g
ov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_
4073288
34. Health Protection Agency Migrant Health: Infectious diseases in non-UK born
populations in the UK; an update to the baseline report. 2011. Available:
https://webarchive.nationalarchives.gov.uk/ukgwa/20140714084455/http://www.hpa.
org.uk/MigrantHealthGuide/ Accessed June 2017
35. Health Protection Agency Targeting testing in England: Health protection services
sentinel surveillance of blood bourne virus testing in England. 2011. Available
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachme
nt_data/file/363846/Sentinel_Surveillance_Annual_Review_2011.pdf
36. Public Health England Hepatitis C in the UK:2014 Report. Available:
http://www.hcvaction.org.uk/sites/default/files/resources/HCV%20in%20the%20UK
%202014%20-%20July.pdf Accessed July 2017
37. Mann AG, Trotter CL, Balogun MA, Ramsay ME. Hepatitis C in ethnic minority
populations in England. J Viral Hepat. 2008 Jun;15(6):421-6. doi: 10.1111/j.1365-
2893.2007.00958.x. Epub 2008 Jan 15. PMID: 18208498.
38. World Health Organization Hepatitis B Factsheet. 2017. Available
https://www.who.int/news-room/fact-sheets/detail/hepatitis-b Accessed January 2018
39. World Health Organization Global Hepatitis Report 2017. Available:
https://www.who.int/publications/i/item/global-hepatitis-report-2017 Accessed
December 2017
40. World Helath Organization Hepatitis C. Available from:
http://www.who.int/mediacentre/factsheets/fs164/en/.
41. World Health Organization (WHO). Global Hepatitis Report 2017. Available
from: https://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/
Accessed January 2018
199
42. World Health Organization Hepatitis: Data and Statistics. Available from:
http://www.euro.who.int/en/healthtopics/communicable-diseases/hepatitis/data-and-
statistics. Accessed January 2018
43. Sharma S, Carballo M, Feld JJ, Janssen HL. Immigration and viral hepatitis. J Hepatol.
2015 Aug;63(2):515-22. doi: 10.1016/j.jhep.2015.04.026. Epub 2015 May 8. PMID:
25962882.
44. World Health Organization, W.H. Emergencies preparedness, response: Hepatitis B.
Available from:
http://www.who.int/csr/disease/hepatitis/whocdscsrlyo20022/en/index1.html.
Accessed January 2018
45. UK National Screening Committee Available from:
https://www.gov.uk/topic/population-screening-programmes. Accessed June 2017
46. Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus
infection: new estimates of age-specific HBsAg seroprevalence and endemicity.
Vaccine. 2012 Mar 9;30(12):2212-9. doi: 10.1016/j.vaccine.2011.12.116. Epub 2012
Jan 24. PMID: 22273662.
47. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide
prevalence of chronic hepatitis B virus infection: a systematic review of data published
between 1965 and 2013. Lancet. 2015 Oct 17;386(10003):1546-55. doi:
10.1016/S0140-6736(15)61412-X. Epub 2015 Jul 28. PMID: 26231459.
48. Zhang Q, Qi W, Wang X, Zhang Y, Xu Y, Qin S, Zhao P, Guo H, Jiao J, Zhou C, Ji S,
Wang J. Epidemiology of Hepatitis B and Hepatitis C Infections and Benefits of
Programs for Hepatitis Prevention in Northeastern China: A Cross-Sectional Study.
Clin Infect Dis. 2016 Feb 1;62(3):305-12. doi: 10.1093/cid/civ859. Epub 2015 Oct 3.
PMID: 26433720.
49. Tassopoulos NC, Papaevangelou GJ, Sjogren MH, Roumeliotou-Karayannis A, Gerin
JL, Purcell RH. Natural history of acute hepatitis B surface antigen-positive hepatitis
in Greek adults. Gastroenterology. 1987 Jun;92(6):1844-50. doi: 10.1016/0016-
5085(87)90614-7. PMID: 3569758.
50. Wasley A, Grytdal S, Gallagher K; Centers for Disease Control and Prevention (CDC).
Surveillance for acute viral hepatitis--United States, 2006. MMWR Surveill Summ.
2008 Mar 21;57(2):1-24. PMID: 18354374.
51. Ghany MG, Perrillo R, Li R, Belle SH, Janssen HL, Terrault NA, Shuhart MC, Lau
DT, Kim WR, Fried MW, Sterling RK, Di Bisceglie AM, Han SH, Ganova-Raeva LM,
Chang KM, Lok AS; Hepatitis B Research Network; Hepatitis B Research Network.
Characteristics of adults in the hepatitis B research network in North America reflect
their country of origin and hepatitis B virus genotype. Clin Gastroenterol Hepatol. 2015
Jan;13(1):183-92. doi: 10.1016/j.cgh.2014.06.028. Epub 2014 Jul 8. PMID: 25010003;
PMCID: PMC4268271.
52. Kowdley KV, Wang CC, Welch S, Roberts H, Brosgart CL. Prevalence of chronic
hepatitis B among foreign-born persons living in the United States by country of origin.
Hepatology. 2012 Aug;56(2):422-33. doi: 10.1002/hep.24804. Epub 2012 Feb 16.
PMID: 22105832.
53. Mossong J, Putz L, Patiny S, Schneider F. Seroepidemiology of hepatitis A and
hepatitis B virus in Luxembourg. Epidemiol Infect. 2006 Aug;134(4):808-13. doi:
10.1017/S0950268805005789. Epub 2006 Jan 25. PMID: 16436219; PMCID:
PMC2870464.
54. MacLachlan JH, Allard N, Towell V, Cowie BC. The burden of chronic hepatitis B
virus infection in Australia, 2011. Aust N Z J Public Health. 2013 Oct;37(5):416-22.
doi: 10.1111/1753-6405.12049. Epub 2013 Mar 20. PMID: 24090323.

200
55. Roberts H, Kruszon-Moran D, Ly KN, Hughes E, Iqbal K, Jiles RB, Holmberg SD.
Prevalence of chronic hepatitis B virus (HBV) infection in U.S. households: National
Health and Nutrition Examination Survey (NHANES), 1988-2012. Hepatology. 2016
Feb;63(2):388-97. doi: 10.1002/hep.28109. Epub 2015 Oct 27. PMID: 26251317.
56. Jung M, Kuniholm MH, Ho GY, Cotler S, Strickler HD, Thyagarajan B, Youngblood
M, Kaplan RC, Del Amo J. The distribution of hepatitis B virus exposure and infection
in a population-based sample of U.S. Hispanic adults. Hepatology. 2016
Feb;63(2):445-52. doi: 10.1002/hep.28328. Epub 2015 Dec 9. PMID: 26523403;
PMCID: PMC4718892.
57. Stanaway JD, Flaxman AD, Naghavi M, Fitzmaurice C, Vos T, Abubakar I, Abu-
Raddad LJ, Assadi R, Bhala N, Cowie B, Forouzanfour MH, Groeger J, Hanafiah KM,
Jacobsen KH, James SL, MacLachlan J, Malekzadeh R, Martin NK, Mokdad AA,
Mokdad AH, Murray CJL, Plass D, Rana S, Rein DB, Richardus JH, Sanabria J, Saylan
M, Shahraz S, So S, Vlassov VV, Weiderpass E, Wiersma ST, Younis M, Yu C, El
Sayed Zaki M, Cooke GS. The global burden of viral hepatitis from 1990 to 2013:
findings from the Global Burden of Disease Study 2013. Lancet. 2016 Sep
10;388(10049):1081-1088. doi: 10.1016/S0140-6736(16)30579-7. Epub 2016 Jul 7.
PMID: 27394647; PMCID: PMC5100695.
58. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national
age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-
2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015
Jan 10;385(9963):117-71. doi: 10.1016/S0140-6736(14)61682-2. Epub 2014 Dec 18.
PMID: 25530442; PMCID: PMC4340604.
59. Centers for Disease Control and Prevention (CDC) Surveillance for Viral Hepatitis –
United States, 2013. Available from
http://www.cdc.gov/hepatitis/statistics/2013surveillance/commentary.htm - hepatitisB.
2013. Accessed January 2018
60. Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu S, Li Y, Wang L, Liu Y, Yin P, Liu J,
Yu S, Tan F, Barber RM, Coates MM, Dicker D, Fraser M, González-Medina D,
Hamavid H, Hao Y, Hu G, Jiang G, Kan H, Lopez AD, Phillips MR, She J, Vos T, Wan
X, Xu G, Yan LL, Yu C, Zhao Y, Zheng Y, Zou X, Naghavi M, Wang Y, Murray CJ,
Yang G, Liang X. Cause-specific mortality for 240 causes in China during 1990-2013:
a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet.
2016 Jan 16;387(10015):251-72. doi: 10.1016/S0140-6736(15)00551-6. Epub 2015
Oct 26. PMID: 26510778.
61. United Nations Department of Economic and Social Affairs: Transforming our world:
the 2030 Agenda for Sustainable Development. 2016. Available
https://sdgs.un.org/2030agenda Accessed March 2018
62. Institute for Helath Metric and Evaluation Global Burden of Disease estimates.
Available from: http://ihmeuw.org/3pms Accessed June 2019
63. World Health Organization. Global health sector strategy on viral hepatitis 2016-2021.
Towards ending viral hepatitis (2016) Available
https://apps.who.int/iris/handle/10665/246177 Accessed June 2017
64. Centers for Disease Control and Prevention. Recommendations for Identification and
Public Health Management of Persons with Chronic Hepatitis B Virus Infection.
MMWR 2008; 57 (No. RR-8). Available www.cdc.gov/hepatitis Accessed June 2017
65. Surrey County Council 2020; Available from: https://www.surreyi.gov.uk/. Accessed
January 2020

201
66. UK Government, Ministry of Housing, communities and local government English
Indicies of Deprivation 2015. Available from English Indicies of Deprivation 2015.
2015. Accessed June 2017
67. Surrey County Council Employment Rates in Surrey. Accessed August 2020; Available
from: https://www.surreyi.gov.uk/dataset/exzxm/annual-population-survey-economic-
activity-and-occupation. Accessed August 2018
68. Surrey County Council Available from: https://www.surreyi.gov.uk/. Accessed August
2018
69. Baker, P., et al., A useful methodological synergy? Combining critical discourse
analysis and corpus linguistics to examine discourses of refugees and asylum seekers
in the UK press. Discourse & Society, 2008. 19(3): p. 273-306.
70. Münz, Rainer; Straubhaar, Thomas; Vadean, Florin P.; Vadean, Nadia (2006) : The
costs and benefits of European immigration, HWWI Policy Report, No. 3,
Hamburgisches WeltWirtschaftsInstitut (HWWI), Hamburg Available from:
http://hdl.handle.net/10419/46220 Accessed June 2017
71. Vargas-Silva C, Rienzo C, The Migrant Observatroy Migrants in the UK: An overview.
2020 25/11/2020]. Available from: https://migrationobservatory.ox.ac.uk/wp-
content/uploads/2017/02/Briefing-Migrants-in-the-UK-An-Overview.pdf Accessed
December 2020
72. Office for National Statistics International Migrants in England and Wales. 2012.
Available from:
https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/inte
rnationalmigration/articles/internationalmigrantsinenglandandwales/2012-12-11
Accessed June 2019
73. Office for National Statistics Ethnicity and national identity in England and Wales
2011. Available from:
https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/arti
cles/ethnicityandnationalidentityinenglandandwales/2012-12-11 Accessed June 2019
74. Czaika M, de Haas H. The Migration Observatory Determinants of migration to the
U.K. 2013; Available from:
https://migrationobservatory.ox.ac.uk/resources/briefings/determinants-of-migration-
to-the-uk/. Accessed October 2020
75. Kierans, D The Migration Observatory Who migrates to the UK and why? 2020:
https://migrationobservatory.ox.ac.uk/resources/briefings/who-migrates-to-the-uk-
and-why/. Accessed October 2020
76. Office for National Statistics, Population of the UK by country of birth and nationality.
2019. Available from:
https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/inte
rnationalmigration/bulletins/ukpopulationbycountryofbirthandnationality/2019
Accessed June 2020
77. Bijak, D., Wisniowski, How to forecast international migration. ESRC Centre for
Population change, University of Southampton, 2015. Available from:
https://eprints.soton.ac.uk/382862/
202
78. Aspinall PJ. Inclusive Practice: Vulnerable Migrants, Gypsies/Irish Travellers, People
Who Are Homeless, and Sex Workers: A Review and Synthesis of
Interventions/Service Models that Improve Access to Primary Care & Reduce Risk of
Avoidable Admission to Hospital. London: Department of Health, 2014. Available
from: https://www.gov.uk/government/publications/access-to-primary-care-among-
vulnerable-groups-review-of-evidence
79. The UN Refugee Agency Fogures at a glance. 2020. Available from:
https://www.unhcr.org/uk/figures-at-a-glance.html Accessed March 2020
80. The UN Refugee Agency, The Global Report 2019; Available from:
https://www.unhcr.org/uk/the-global-report.html. Accessed March 2020
81. Ager S, Strang A: Understanding integration: A conceptual framework. Journal of
Refugee studies, 2008. 21(2): p. 166-191.
82. Lessard-Phillips L, Fajth V: The Migration Observatory, Migrants’ social
relationships, identity and civic participation in the UK. 2020. Available from:
https://migrationobservatory.ox.ac.uk/resources/briefings/migrants-social-
relationships-identity-and-civic-participation-in-the-uk/ Accessed April 2020
83. Bilgili. Simultaneity in Transnational Migration Research. Links between migrants
host and home country orientation. Maastricht: Boekenplan 2014. Available from:
https://www.semanticscholar.org/paper/Simultaneity-in-transnational-migration-
research%3A-Bilgili/65ea18e93fea0a10591942a3a0ee4b3af1ac94b2
84. Spencer S, Charsley K: Conceptualising integration: a framework for empirical
research, taking marriage migration as a case study. Comparative Migration Studies,
2016. 4(1): p. 18.
85. Rytter, M: Writing Against Integration: Danish Imaginaries of Culture, Race and
Belonging. Ethnos, 2019. 84(4): p. 678-697.
86. Rutter J, Cooley L, Jones N, Pillai R: Moving up together: promoting equality and
integration among the UKs diverse communities, The Institute for Public Policy
Research 2008. Available from: Rutter., Moving up together: promoting equality and
integration among the UKs diverse communities, I.f.p.p. research, Editor. 2008.
Accessed July 2017
87. Blair T. The Duty to integrate: shared British values. Runnymede Quality (348) 1-5
2006
88. Broadhead J, Spencer S: Policy primer: Integration The Migration Observatory 2020.
Available from: https://migrationobservatory.ox.ac.uk/resources/primers/policy-
primer-integration/ Accessed June 2020
89. Eurostat, Migrants in Europe: A statistical portrait of the first and second generation
2011. Available from: https://ec.europa.eu/eurostat/documents/3217494/5727749/KS-
31-10-539-EN.PDF.pdf/bcf27a60-7016-4fec-98c5-e8488491ebbd?t=1414775922000
Accessed June 2017
90. Fernandez-Reino M, Migrants and discrimination in the UK, The Migration
Observatory, 2020. Available from
https://migrationobservatory.ox.ac.uk/resources/briefings/migrants-and-
discrimination-in-the-uk/ Accessed May 2020
91. Blinder S, Richards L, UK Public Opinion toward Immigration: Overall Attitudes and
Level of Concern, The Migration Observatiory, 2020. Available from:
https://migrationobservatory.ox.ac.uk/resources/briefings/uk-public-opinion-toward-
immigration-overall-attitudes-and-level-of-concern/ Accessed May 2020
92. Rzepnikowska, A., Racism and xenophobia experienced by Polish migrants in the UK
before and after Brexit vote. Journal of Ethnic and Migration Studies, 2019. 45(1): p.
61-77.

203
93. IPSOS-Mori, Immigration is now the top issue for voters in the EU referendum. 2016:
Available from: https://www.ipsos.com/ipsos-mori/en-uk/immigration-now-top-issue-
voters-eu-referendum. Accessed May 2019
94. Guma T, Dafydd Jones R, “Where are we going to go now?” European Union
migrants' experiences of hostility, anxiety, and (non-)belonging during Brexit.
Population, Space and Place, 2019. 25(1): p. e2198.
95. Zschirnt, Ruedin: Ethnic discrimination in hiring decisions: a meta-analysis of
correspondence tests 1990–2015. Journal of Ethnic and Migration Studies, 2016. 42(7):
p. 1115-1134.
96. Kustov, ‘Bloom where you’re planted.’ Explaining public opposition to (e)migration.
Journal of Ethnic and Migration Studies, 2020.
97. Ceobanu A.M. Escandell M, Comparative Analyses of Public Attitudes Toward
Immigrants and Immigration Using Multinational Survey Data: A Review of Theories
and Research. Annual Review of Sociology, 2010. 36(1): p. 309-328.
98. Hainmueller J, Hiscox M, Margalit Y: Do concerns about labor market competition
shape attitudes toward immigration? New evidence. Journal of International
Economics, 2015. 97(1): p. 193-207.
99. Helbling M, Traunmüller R: What is Islamophobia? Disentangling Citizens’ Feelings
Toward Ethnicity, Religion and Religiosity Using a Survey Experiment. British Journal
of Political Science, 2018. 50: p. 1-18.
100. Van der Noll J, Saroglou V, Latour D, Dolezal N: Western Anti-Muslim Prejudice:
Value Conflict or Discrimination of Persons Too? Political Psychology, 2018. 39(2):
p. 281-301.
101. European Social Study: Attitudes towards Immigration and their antecedents. 2016:
ESS Topline results from Round 7 of the European Social Study Available from:
https://www.europeansocialsurvey.org/docs/findings/ESS7_toplines_issue_7_immigr
ation.pdf Accessed March 2018
102. Safi, Immigrants’ life satisfaction in Europe: Between assimilation and discrimination.
European Sociological Review, 2009. 26(2): p. 159-176.
103. Schmitt MT, Branscombe NR, Postmes T, Garcia A. The consequences of perceived
discrimination for psychological well-being: a meta-analytic review. Psychol Bull.
2014 Jul;140(4):921-48. doi: 10.1037/a0035754. Epub 2014 Feb 17. PMID: 24547896.
104. Auer D, Ruedin D, Who Feels Disadvantaged? Reporting Discrimination in Surveys,
in Migrants and Expats: The Swiss Migration and Mobility Nexus, I. Steiner and P.
Wanner, Editors. 2019, Springer International Publishing: Cham. p. 221-242.
105. de Vroome, T., M. Verkuyten, and B. Martinovic, Host National Identification of
Immigrants in the Netherlands. International Migration Review, 2014. 48(1): p. 1-27.
106. The Migration Observatory: Why do international migrants come to the U.K. 2015.
Available from: https://migrationobservatory.ox.ac.uk/resources/briefings/election-
2015-briefing-why-do-international-migrants-come-to-the-uk/ Accessed January 2020
107. World Health Organization, How health systems can address health inequities linked
to migration and ethnicity. Copenhagen, WHO Regional Office for Europe, 2010.
Available from: https://www.who.int/docs/default-
source/documents/publications/how-health-systems-can-address-
ethnicity.pdf?sfvrsn=2c7cba14_1 Accessed January 2019
108. Jayaweera H, Quigley MA, Health status, health behaviour and healthcare use among
migrants in the UK: evidence from mothers in the Millennium Cohort Study. Soc Sci
Med, 2010. 71(5): p. 1002-10.
109. Marmot, M: Social justice, epidemiology and health inequalities. Eur J Epidemiol,
2017. 32(7): p. 537-546.

204
110. Ingleby D: Ethnicity, migration and the Social determinants of health agenda.
Psychosocial Intervention, 2012. 21(3): p. 331-341.
111. O'Donnell CA, Burns N, Mair FS, Dowrick C, Clissmann C, van den Muijsenbergh M,
van Weel-Baumgarten E, Lionis C, Papadakaki M, Saridaki A, de Brun T, MacFarlane
A; RESTORE Team. Reducing the health care burden for marginalised migrants: The
potential role for primary care in Europe. Health Policy. 2016 May;120(5):495-508.
doi: 10.1016/j.healthpol.2016.03.012. Epub 2016 Apr 6. PMID: 27080344.
112. Antecol H, Bedard K, Unhealthy assimilation: Why do immigrants converge to
American health status levels? Demography, 2006. 43(2): p. 337-360.
113. Fernandez- Reino M, The health of migrants in the UK, The Migration Observatory,
2020. Available from: https://migrationobservatory.ox.ac.uk/resources/briefings/the-
health-of-migrants-in-the-uk/ Accessed August 2020
114. Szczepura A Access to health care for ethnic minority populations. Postgrad Med J,
2005. 81(953): p. 141-7.
115. Elo IT: Social Class Differentials in Health and Mortality: Patterns and Explanations
in Comparative Perspective. Annual Review of Sociology, 2009. 35(1): p. 553-572.
116. Pampel, FC, Krueger PM, Denney JT, Socioeconomic Disparities in Health Behaviors.
Annual Review of Sociology, 2010. 36(1): p. 349-370.
117. Benzeval, Campbell, Egan, Lorenc, Petticrew, Popham,, How does money influence
health, Joseph Rowntree Foundation, 2014. Available from:
https://www.jrf.org.uk/sites/default/files/jrf/migrated/files/income-health-poverty-
full.pdf Accessed January 2019
118. Layte R, Whelan CT, Who Feels Inferior? A Test of the Status Anxiety Hypothesis of
Social Inequalities in Health. European Sociological Review, 2014. 30(4): p. 525-535.
119. Anderson LM, Scrimshaw SC, Fullilove MT, Fielding JE, Normand J; Task Force on
Community Preventive Services. Culturally competent healthcare systems. A
systematic review. Am J Prev Med. 2003 Apr;24(3 Suppl):68-79. doi: 10.1016/s0749-
3797(02)00657-8. PMID: 12668199.
120. Medical Research Council: Developing and Evaluating Complex Interventions
Available from https://mrc.ukri.org/documents/pdf/complex-interventions-guidance/
Accessed August 2017
121. Uddin G, Shoeb D, Solaiman S, Marley R, Gore C, Ramsay M, Harris R, Ushiro-Lumb
I, Moreea S, Alam S, Thomas HC, Khan S, Watt B, Pugh RN, Ramaiah S, Jervis R,
Hughes A, Singhal S, Cameron S, Carman WF, Foster GR. Prevalence of chronic viral
hepatitis in people of south Asian ethnicity living in England: the prevalence cannot
necessarily be predicted from the prevalence in the country of origin. J Viral Hepat.
2010 May;17(5):327-35. doi: 10.1111/j.1365-2893.2009.01240.x. Epub 2009 Dec 9.
PMID: 20002307.
122. Dahlgren G, Whitehead M: Policies and strategies to promote social equity in health.
Background document to WHO - Strategy paper for Europe, Arbetsrapport 2007:14,
Institute for Futures Studies. https://ideas.repec.org/p/hhs/ifswps/2007_014.html
123. Public Health England UK National Screening Committee Screening in the UK:
Making Effective Recommendations 2015-2016 Available from:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachme
nt_data/file/733227/Screening_in_the_UK___making_effective_recommendations_2
015_to_2016.pdf Accessed January 2018
124. World Health Organization. Regional Office for Europe, European Observatory on
Health Systems and Policies, Holland, Walter W, Stewart, Susie & Masseria,
Cristina. (2006). Screening in Europe. World Health Organization. Regional Office for
Europe. https://apps.who.int/iris/handle/10665/107742 Accessed January 2019
205
125. World Health Organisation The Global Burden of Disease:2004 update. 2008
Available from:
https://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.
pdf Accessed January 2018
126. Unal B. Critchley JA, Capewell S, Explaining the decline in coronary heart disease
mortality in England and Wales between 1981 and 2000. Circulation, 2004. 109(9): p.
1101-7.
127. Laara E, Day NE, Hakama M, Trends in mortality from cervical cancer in the Nordic
countries: association with organised screening programmes. Lancet, 1987. 1(8544):
p. 1247-9.
128. Tabár L, Gad A, Holmberg L, Ljungquist U. Significant reduction in advanced breast
cancer. Results of the first seven years of mammography screening in Kopparberg,
Sweden. Diagn Imaging Clin Med. 1985;54(3-4):158-64. PMID: 3896614.
129. Kerlikowske K, Grady D, Ernster V, Benefit of mammography screening in women
ages 40-49 years: current evidence from randomized controlled trials. Cancer, 1995.
76(9): p. 1679-81.
130. Kerlikowske K, Grady D, Rubin SM, Sandrock C, Ernster VL. Efficacy of screening
mammography. A meta-analysis. JAMA. 1995 Jan 11;273(2):149-54. PMID: 7799496.
131. Tunstall-Pedoe, Hugh, Kuulasmaa, Kari, Tolonen, Hanna, Davidson, Moira, Mendis,
Shanthi. et al. (2003). MONICA monograph and multimedia sourcebook: world's
largest study of heart disease, stroke, risk factors, and population trends 1979-2002 /
edited by Hugh Tunstall-Pedoe ; prepared by Hugh Tunstall-Pedoe ... [et al.] with 64
other contributors for the WHO MONICA Project. World Health
Organization. https://apps.who.int/iris/handle/10665/42597
132. Australian Government National Health and Medical Research Council Screening to
prevent cervical cancer: guidelines for the management of asymptomatic women with
screen-detected abnormalities Available from:
https://webarchive.nla.gov.au/awa/20170816100344/https://www.nhmrc.gov.au/guide
lines-publications/wh39 Accessed August 2017
133. Reed, MW: Scottish Intercollegiate Guidelines Network (SIGN) 84 -- National Clinical
Guideline for the Management of Breast Cancer in Women. Clin Oncol (R Coll Radiol),
2007. 19(8): p. 588-90.
134. World Health Organization. (2002). National cancer control programmes : policies and
managerial guidelines, 2nd ed. World Health
Organization. https://apps.who.int/iris/handle/10665/42494 Accessed Aug 2020
135. Barratt, Mannes, Irwig, Trevena, Craig, Rychetnik Cancer screening. J Epidemiol
Community Health, 2002. 56(12): p. 899-902.
136. Parkin DM, Tappenden P, Olsen AH, Patnick J, Sasieni P. Predicting the impact of the
screening programme for colorectal cancer in the UK. J Med Screen. 2008;15(4):163-
74. doi: 10.1258/jms.2008.008024. PMID: 19106256.
137. National Center for Health Statistics, Centers for disease control and prevention
Services: Healthy People 2010 Final Review, Available from:
https://www.cdc.gov/nchs/data/hpdata2010/hp2010_final_review.pdf Accessed June
2018
138. Patnick, J. Accessing Screening Services: A Review of the Literature and Local
Practice in the context of the Equality Delivery System. NHS Screening Programmes,
Available from:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachme
nt_data/file/398818/EDS_Screening_Literature_Review.pdf accessed June 2018
206
139. Commission for Health Improvement (2004) Unpacking the Patients’ Perspective:
Variations in NHS Patient Experience in England. CHI. Available
from: http://www.healthcarecommission.org.uk/_db/_documents/04003496.pdf
Accessed June 2018
140. Yu, J A systematic review of issues around antenatal screening and prenatal diagnostic
testing for genetic disorders: women of Asian origin in western countries. Health Soc
Care Community, 2012. 20(4): p. 329-46.
141. Moser, K, Patnick J, Beral V, Inequalities in reported use of breast and cervical
screening in Great Britain: analysis of cross sectional survey data. BMJ, 2009. 338: p.
b2025.
142. Applebee, Analyses of Inequality in National Screening Programmes Using Existing
Data Systems: A Supplementary Report for the UK National Screening Committee.
2012.
143. Botha JL, Manku-Scott TK, Moledina F, Williams A. Indirect discrimination and breast
screening. Ethn Dis. 1993 Spring;3(2):189-95. PMID: 8324497.
144. Swan J, Breen N, Coates RJ, Rimer BK, Lee NC. Progress in cancer screening practices
in the United States: results from the 2000 National Health Interview Survey. Cancer.
2003 Mar 15;97(6):1528-40. doi: 10.1002/cncr.11208. PMID: 12627518.
145. Reuben DB, Bassett LW, Hirsch SH, Jackson CA, Bastani R. A randomized clinical
trial to assess the benefit of offering on-site mobile mammography in addition to health
education for older women. AJR Am J Roentgenol. 2002 Dec;179(6):1509-14. doi:
10.2214/ajr.179.6.1791509. PMID: 12438046.
146. Katz, SJ, Zemencuk JK, Hofer TP, Breast cancer screening in the United States and
Canada, 1994: socioeconomic gradients persist. Am J Public Health, 2000. 90(5): p.
799-803.
147. Porter, Interventions to reduce inequality and inequality in accessing national
screening programmes: A report for the UK National Screening Committee. Public
Health Resource Unit, 2008.
148. Brouwers MC, De Vito C, Bahirathan L, Carol A, Carroll JC, Cotterchio M, Dobbins
M, Lent B, Levitt C, Lewis N, McGregor SE, Paszat L, Rand C, Wathen N. What
implementation interventions increase cancer screening rates? a systematic review.
Implement Sci. 2011 Sep 29;6:111. doi: 10.1186/1748-5908-6-111. PMID: 21958556;
PMCID: PMC3197548.
149. Everett T, Bryant A, Griffin MF, Martin-Hirsch PPL, Forbes CA, Jepson RG,
Interventions targeted at women to encourage the uptake of cervical screening.
Cochrane Database of Systematic Reviews, 2011(5).
150. Threlfall, Approaches to increase attendance at Breast and Cervical Cancer Screening
in Greater Manchester. 2009.
151. Kelly, Pericleous, Hendy, de Lusignan, Ahmed, Vandrevala, Ala, Interventions to
Improve the Uptake of Screening Across a Range of Conditions in Ethnic Minority
Groups: A Systematic Review. Int J Clin Pract, 2017.
152. Gulati R., Nawaz M, Pyrsopoulos NT, Health literacy and liver disease. Clin Liver Dis
(Hoboken), 2018. 11(2): p. 48-51.
153. Ginès P, Graupera I, Lammert F, Angeli P, Caballeria L, Krag A, Guha IN, Murad SD,
Castera L. Screening for liver fibrosis in the general population: a call for action. Lancet
Gastroenterol Hepatol. 2016 Nov;1(3):256-260. doi: 10.1016/S2468-1253(16)30081-
4. Epub 2016 Oct 12. PMID: 28404098.
154. Caballería L, Pera G, Arteaga I, Rodríguez L, Alumà A, Morillas RM, de la Ossa N,
Díaz A, Expósito C, Miranda D, Sánchez C, Prats RM, Urquizu M, Salgado A,
Alemany M, Martinez A, Majeed I, Fabrellas N, Graupera I, Planas R, Ojanguren I,
207
Serra M, Torán P, Caballería J, Ginès P. High Prevalence of Liver Fibrosis Among
European Adults With Unknown Liver Disease: A Population-Based Study. Clin
Gastroenterol Hepatol. 2018 Jul;16(7):1138-1145.e5. doi: 10.1016/j.cgh.2017.12.048.
Epub 2018 Feb 13. PMID: 29452268.
155. Koehler EM, Plompen EP, Schouten JN, Hansen BE, Darwish Murad S, Taimr P,
Leebeek FW, Hofman A, Stricker BH, Castera L, Janssen HL. Presence of diabetes
mellitus and steatosis is associated with liver stiffness in a general population: The
Rotterdam study. Hepatology. 2016 Jan;63(1):138-47. doi: 10.1002/hep.27981. Epub
2015 Oct 1. PMID: 26171685.
156. Cheng PN, Chiu YC, Chiu HC, Chien SC. The Application of Liver Stiffness
Measurement in Residents Without Overt Liver Diseases Through a Community-Based
Screening Program. Medicine (Baltimore). 2016 Mar;95(12):e3193. doi:
10.1097/MD.0000000000003193. Erratum in: Medicine (Baltimore). 2016 Jun
17;95(24):e4044. PMID: 27015215; PMCID: PMC4998410.
157. Marcellin P, Kutala BK, Liver diseases: A major, neglected global public health
problem requiring urgent actions and large-scale screening. Liver Int, 2018. 38 Suppl
1: p. 2-6.
158. Robotin MC, George J, Community-based hepatitis B screening: what works? Hepatol
Int, 2014. 8(4): p. 478-92.
159. McLeroy KR, Norton BL, Kegler MC, Burdine JN, Sumaya CV. Community-based
interventions. Am J Public Health. 2003 Apr;93(4):529-33. doi: 10.2105/ajph.93.4.529.
PMID: 12660190; PMCID: PMC1447783.
160. Hargreaves, S., Seedat, F., Car, J. et al. Screening for latent TB, HIV, and hepatitis B/C
in new migrants in a high prevalence area of London, UK: a cross-sectional study. BMC
Infect Dis 14, 657 (2014). https://doi.org/10.1186/s12879-014-0657-2
161. Mcpherson S, Valappil M, Moses SE, Eltringham G, Miller C, Baxter K, Chan A,
Shafiq K, Saeed A, Quereshi R, Hudson M Bassendine MF A pilot of targeted case
finding for hepatitis B virus (HBV) and hepatitis C (HCV) in the British South Asian
community. Gut, 2012. 61.
162. Landon, M., Hepatitis B: raising awareness in the South Asian community in Preston.
British Journal of Community Nursing, 2013. 18(1).
163. Lewis, H., Burke, K., Begum, S., Ushiro-Limb, I., & Foster, G. (2011). P56 What is
the best method of case finding for chronic viral hepatitis in migrant communities? Gut,
60, A26 - A26.
164. Zuure FR, Bouman J, Martens M, Vanhommerig JW, Urbanus AT, Davidovich U, van
Houdt R, Speksnijder AG, Weegink CJ, van den Hoek A, Prins M. Screening for
hepatitis B and C in first-generation Egyptian migrants living in the Netherlands. Liver
Int. 2013 May;33(5):727-38. doi: 10.1111/liv.12131. Epub 2013 Mar 1. PMID:
23448397.
165. Navarro N, Lim N, Kim J, Joo E, Che K, Runyon B, Mendler M: Lower than expected
hepatitis B virus infection prevalence among first generation Koreans in the U.S.:
results of HBV screening in the Southern California Inland Empire. BMC Infect
Dis 14, 269 (2014). https://doi.org/10.1186/1471-2334-14-269
166. Vedio AB, Ellam H, Rayner F, Stone B, Kudesia G, McKendrick MW, Green ST.
Hepatitis B: report of prevalence and access to healthcare among Chinese residents in
Sheffield UK. J Infect Public Health. 2013 Dec;6(6):448-55. doi:
10.1016/j.jiph.2013.05.004. Epub 2013 Jun 28. PMID: 23999342.
167. Veldhuijzen IK, van Driel HF, Vos D, de Zwart O, van Doornum GJ, de Man RA,
Richardus JH. Viral hepatitis in a multi-ethnic neighborhood in the Netherlands: results
of a community-based study in a low prevalence country. Int J Infect Dis. 2009
208
Jan;13(1):e9-e13. doi: 10.1016/j.ijid.2008.05.1224. Epub 2008 Aug 3. PMID:
18678518.
168. Richter C, Ter Beest G, Gisolf EH, VAN Bentum P, Waegemaekers C, Swanink C,
Roovers E. Screening for chronic hepatitis B and C in migrants from Afghanistan, Iran,
Iraq, the former Soviet Republics, and Vietnam in the Arnhem region, The Netherlands.
Epidemiol Infect. 2014 Oct;142(10):2140-6. doi: 10.1017/S0950268813003415. Epub
2014 Jan 7. PMID: 24398373.
169. Ma GX, Gao W, Tan Y, Chae WG, Rhee J. A community-based participatory approach
to a hepatitis B intervention for Korean Americans. Prog Community Health Partnersh.
2012 Spring;6(1):7-16. doi: 10.1353/cpr.2012.0002. PMID: 22643783; PMCID:
PMC5573181.
170. Ho E, Michielsen P, Van Damme P, Ieven M, Veldhuijzen I, Vanwolleghem T. Point-
of-Care Tests for Hepatitis B Are Associated with A Higher Linkage to Care and Lower
Cost Compared to Venepuncture Sampling During Outreach Screenings in an Asian
Migrant Population. Ann Glob Health. 2020 Jul 16;86(1):81. doi: 10.5334/aogh.2848.
PMID: 32742939; PMCID: PMC7366862.
171. van der Veen YJ, Voeten HA, de Zwart O, Richardus JH. Awareness, knowledge and
self-reported test rates regarding Hepatitis B in Turkish-Dutch: a survey. BMC Public
Health. 2010 Aug 24;10:512. doi: 10.1186/1471-2458-10-512. PMID: 20735831;
PMCID: PMC2940913.
172. Pollack H, Wang S, Wyatt L, Peng CH, Wan K, Trinh-Shevrin C, Chun K, Tsang T,
Kwon S. A comprehensive screening and treatment model for reducing disparities in
hepatitis B. Health Aff (Millwood). 2011 Oct;30(10):1974-83. doi:
10.1377/hlthaff.2011.0700. PMID: 21976342; PMCID: PMC3333793.
173. Yoo GJ, Fang T, Zola J, Dariotis WM. Destigmatizing hepatitis B in the Asian
American community: lessons learned from the San Francisco Hep B Free Campaign.
J Cancer Educ. 2012 Mar;27(1):138-44. doi: 10.1007/s13187-011-0252-9. PMID:
21748476; PMCID: PMC4537654.
174. Hsu L, Bowlus CL, Stewart SL, Nguyen TT, Dang J, Chan B, Chen MS Jr. Electronic
messages increase hepatitis B screening in at-risk Asian American patients: a
randomized, controlled trial. Dig Dis Sci. 2013 Mar;58(3):807-14. doi:
10.1007/s10620-012-2396-9. Epub 2012 Oct 17. PMID: 23073671; PMCID:
PMC3578075.
175. Chen MS Jr, Fang DM, Stewart SL, Ly MY, Lee S, Dang JH, Nguyen TT, Maxwell
AE, Bowlus CL, Bastani R, Nguyen TT. Increasing hepatitis B screening for hmong
adults: results from a randomized controlled community-based study. Cancer
Epidemiol Biomarkers Prev. 2013 May;22(5):782-91. doi: 10.1158/1055-9965.EPI-12-
1399. Epub 2013 Apr 23. PMID: 23613027; PMCID: PMC3650126.
176. Juon HS, Lee S, Strong C, Rimal R, Kirk GD, Bowie J. Effect of a liver cancer
education program on hepatitis B screening among Asian Americans in the Baltimore-
Washington metropolitan area, 2009-2010. Prev Chronic Dis. 2014 Feb 6;11:130258.
doi: 10.5888/pcd11.130258. PMID: 24503341; PMCID: PMC3921910.
177. Taylor VM, Bastani R, Burke N, Talbot J, Sos C, Liu Q, Do H, Jackson JC, Yasui Y.
Evaluation of a hepatitis B lay health worker intervention for Cambodian Americans. J
Community Health. 2013 Jun;38(3):546-53. doi: 10.1007/s10900-012-9649-6. PMID:
23299978; PMCID: PMC3633619.
178. Taylor VM, Gregory Hislop T, Bajdik C, Teh C, Lam W, Acorda E, Li L, Yasui Y.
Hepatitis B ESL education for Asian immigrants. J Community Health. 2011
Feb;36(1):35-41. doi: 10.1007/s10900-010-9279-9. PMID: 20559696; PMCID:
PMC2952282.

209
179. Taylor VM, Hislop TG, Tu SP, Teh C, Acorda E, Yip MP, Woodall E, Yasui Y.
Evaluation of a hepatitis B lay health worker intervention for Chinese Americans and
Canadians. J Community Health. 2009 Jun;34(3):165-72. doi: 10.1007/s10900-008-
9138-0. PMID: 19127416; PMCID: PMC2735565.
180. Bastani R, Glenn BA, Maxwell AE, Jo AM, Herrmann AK, Crespi CM, Wong WK,
Chang LC, Stewart SL, Nguyen TT, Chen MS Jr, Taylor VM. Cluster-Randomized
Trial to Increase Hepatitis B Testing among Koreans in Los Angeles. Cancer Epidemiol
Biomarkers Prev. 2015 Sep;24(9):1341-9. doi: 10.1158/1055-9965.EPI-14-1396. Epub
2015 Jun 23. PMID: 26104909; PMCID: PMC4560609.
181. Kunkel, S., Falla, Veldhuijzen, Foster, Screening for viral hepatitis among migrants in
the EU: What lessons can we learn from poor response to a pilot trial using GP
registers? Journal of Hepatology, 2015. 62: p. P1277.
182. Flanagan S, Kunkel J, Appleby V, Eldridge SE, Ismail S, Moreea S, Griffiths C, Walton
R, Pitt M, Salmon A, Madurasinghe V, Barnes E, Simms E, Agarwal K, Foster GR.
Case finding and therapy for chronic viral hepatitis in primary care (HepFREE): a
cluster-randomised controlled trial. Lancet Gastroenterol Hepatol. 2019 Jan;4(1):32-
44. doi: 10.1016/S2468-1253(18)30318-2. Epub 2018 Nov 24. PMID: 30477810.
183. Legard, R., Keegan, J. and Ward, K. (2003) In-depth Interviews. In: Richie, J. and
Lewis, J., Eds., Qualitative Research Practice, Sage, London, 139-168.
184. Leung, F.H. Savithiri R, Spotlight on focus groups. Can Fam Physician, 2009. 55(2): p.
218-9.
185. Morgan DL, The focus group guide book. 1998: Sage Publications.
186. Bloor M, F.J., Thomas M, Robson K, Focus groups in social research. 2001: Sage
Publications.
187. Morgan DL, Krueger R. A, Chapter 1 When to use focus groups and why, in Successful
Focus Groups: Advancing the state of the art. 1993.
188. Mansell I, Bennett G, Northway R, Mead D, Moseley L. The learning curve: the
advantages and disadvantages in the use of focus groups as a method of data collection.
Nurse Res. 2004;11(4):79-88. doi: 10.7748/nr2004.07.11.4.79.c6217. PMID:
15227901.
189. Krueger RA, Focus groups: A practical guide for applied research. 1994: Sage
Publications.
190. Braun, V Clarke V, Using thematic analysis in psychology. Qualitative Research in
Psychology, 2006. 3(2): p. 77-101.
191. Hendy J, Vandrevala T, Ahmed A, Kelly C, Gray L, Ala A. Feeling misidentified:
Understanding migrant's readiness to engage in health care screening. Soc Sci Med.
2019 Sep;237:112481. doi: 10.1016/j.socscimed.2019.112481. Epub 2019 Aug 8.
PMID: 31421461.
192. Kelly C, Ahmed A, Pericleous M, Hendy J, Vandrevala T, Ala A, Factors Preventing
Testing for Chronic Viral Hepatitis (CVH) in UK South-Asians: A Novel National
Institute for Health Research (NIHR) Study in a High Risk Group. Hepatology, 2017.
66(S1): p. 319A.
193. Readhead S, Ahmed A, Jenkins H, Nicholls M, Berry P, Foster G, Ala A, The use of
dry blood spot tests(DBS) for viral hepatitis in mosques-A pilot study of 3 Surrey
centres. Gut, 2012. 61: p. A131.
194. Mössner BK, Staugaard B, Jensen J, Lillevang ST, Christensen PB, Holm DK. Dried
blood spots, valid screening for viral hepatitis and human immunodeficiency virus in
real-life. World J Gastroenterol. 2016 Sep 7;22(33):7604-12. doi:
10.3748/wjg.v22.i33.7604. PMID: 27672281; PMCID: PMC5011674.
210
195. Mohamed S, Raimondo A, Pénaranda G, Camus C, Ouzan D, Ravet S, Bourlière M,
Khiri H, Dukan P, Olive D, Halfon P. Dried blood spot sampling for hepatitis B virus
serology and molecular testing. PLoS One. 2013 Apr 16;8(4):e61077. doi:
10.1371/journal.pone.0061077. PMID: 23613788; PMCID: PMC3628702.
196. Greenman J, Roberts T, Cohn J, Messac L. Dried blood spot in the genotyping,
quantification and storage of HCV RNA: a systematic literature review. J Viral Hepat.
2015 Apr;22(4):353-61. doi: 10.1111/jvh.12345. Epub 2014 Nov 4. PMID: 25367722;
PMCID: PMC4409077.
211
APPENDIX 1
FOCUS GROUP ADVERTISEMENT
212
APPENDIX 2: FOCUS GROUP DEMOGRAPHIC INFORMATION
213

214
APPENDIX 3: DEMOGRAPHIC INFORMATION FOR STUDY 2
Title of study: Intervention to Promote Testing for Viral Hepatitis in
People of South Asian Heritage
Thank you for your participation. Please answer the following questions. The information
you provide will only be used to help us better understand the views shared in this
questionnaire. It will be stored anonymously and will remain confidential.
1. Name:
_____________________________________________________________________
2. Your contact details:
Address
_____________________________________________________________________
_____________________________________________________________________
____________
Phone Email
____________________________________________________________________
3. Age in years
18-24 ☐ 25-40 ☐ 41-50 ☐
51-60 ☐ 61 and over ☐
4. Gender: ☐ Male ☐ Female
5. Length of Stay in UK (years/months):
____________________________________________
6. Where were you born? ☐Bangladesh ☐India ☐Pakistan
☐Sri Lanka
☐Other: __________________
215
7. Marital Status: ☐ Single ☐Married ☐Widowed ☐Divorced ☐ Co-
habiting
8. Education: ☐School level ☐College level ☐University Level
☐Professional
9. Which language (s) can you speak?
______________________________________________
10. Do you work? ☐ YES ☐
NO
If yes, what do you do?
_____________________________________________________________________
11. Religion:
____________________________________________________________________
12. Have you ever received vaccination for Hepatitis? ☐ YES ☐ NO ☐ DON’T
KNOW
13. Have you ever been tested for Viral Hepatitis B or C? ☐YES ☐NO ☐ DON’T
KNOW
14. If yes, have you ever been diagnosed
with Hepatitis B or C? ☐ YES ☐ NO ☐ DON’T
KNOW
15. If yes, have you received treatment for it? ☐ YES ☐ NO ☐ DON’T
KNOW
16. Have you had a blood transfusion before 1990? ☐ YES ☐ NO ☐ DON’T
KNOW
17. Have you shared injection needles for
medications or drugs before? ☐ YES ☐ NO ☐ DON’T KNOW
18. Have you been to Hajj? ☐ YES ☐ NO
19. If yes, did you have your head shaved? ☐ YES ☐ NO
Thank you
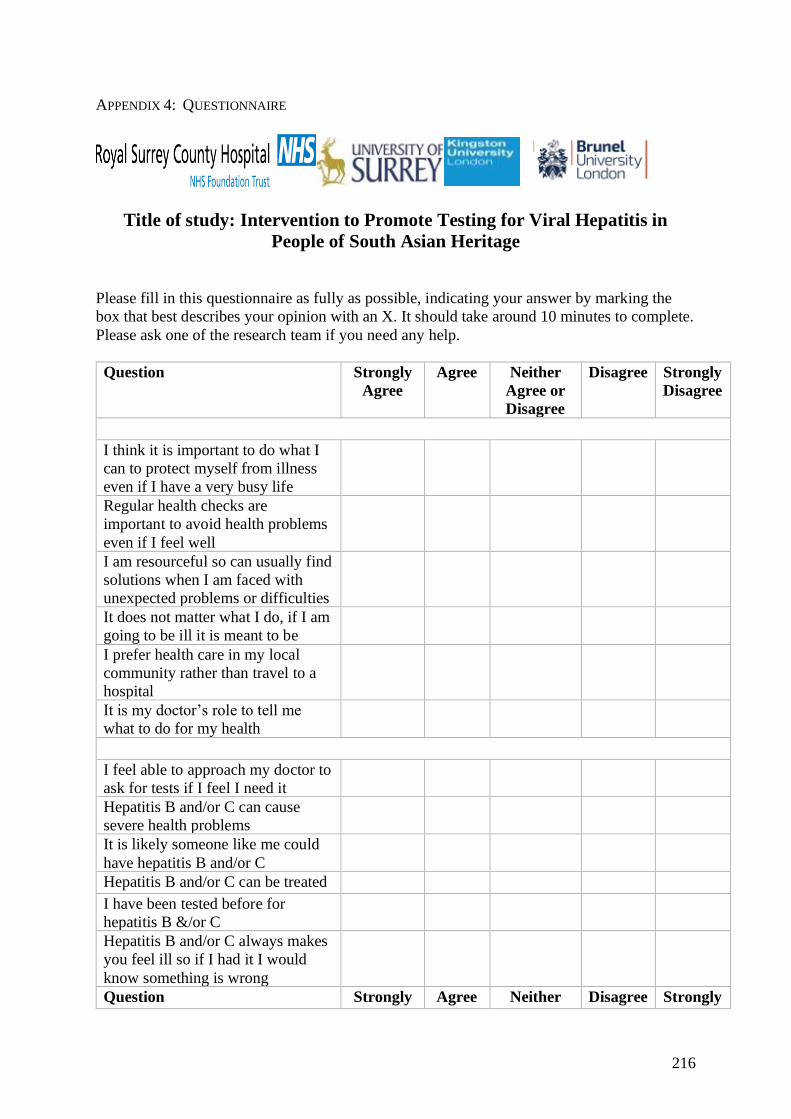
216
APPENDIX 4: QUESTIONNAIRE
Title of study: Intervention to Promote Testing for Viral Hepatitis in
People of South Asian Heritage
Please fill in this questionnaire as fully as possible, indicating your answer by marking the
box that best describes your opinion with an X. It should take around 10 minutes to complete.
Please ask one of the research team if you need any help.
Question Strongly
Agree
Agree Neither
Agree or
Disagree
Disagree Strongly
Disagree
I think it is important to do what I
can to protect myself from illness
even if I have a very busy life
Regular health checks are
important to avoid health problems
even if I feel well
I am resourceful so can usually find
solutions when I am faced with
unexpected problems or difficulties
It does not matter what I do, if I am
going to be ill it is meant to be
I prefer health care in my local
community rather than travel to a
hospital
It is my doctor’s role to tell me
what to do for my health
I feel able to approach my doctor to
ask for tests if I feel I need it
Hepatitis B and/or C can cause
severe health problems
It is likely someone like me could
have hepatitis B and/or C
Hepatitis B and/or C can be treated
I have been tested before for
hepatitis B &/or C
Hepatitis B and/or C always makes
you feel ill so if I had it I would
know something is wrong
Question Strongly Agree Neither Disagree Strongly
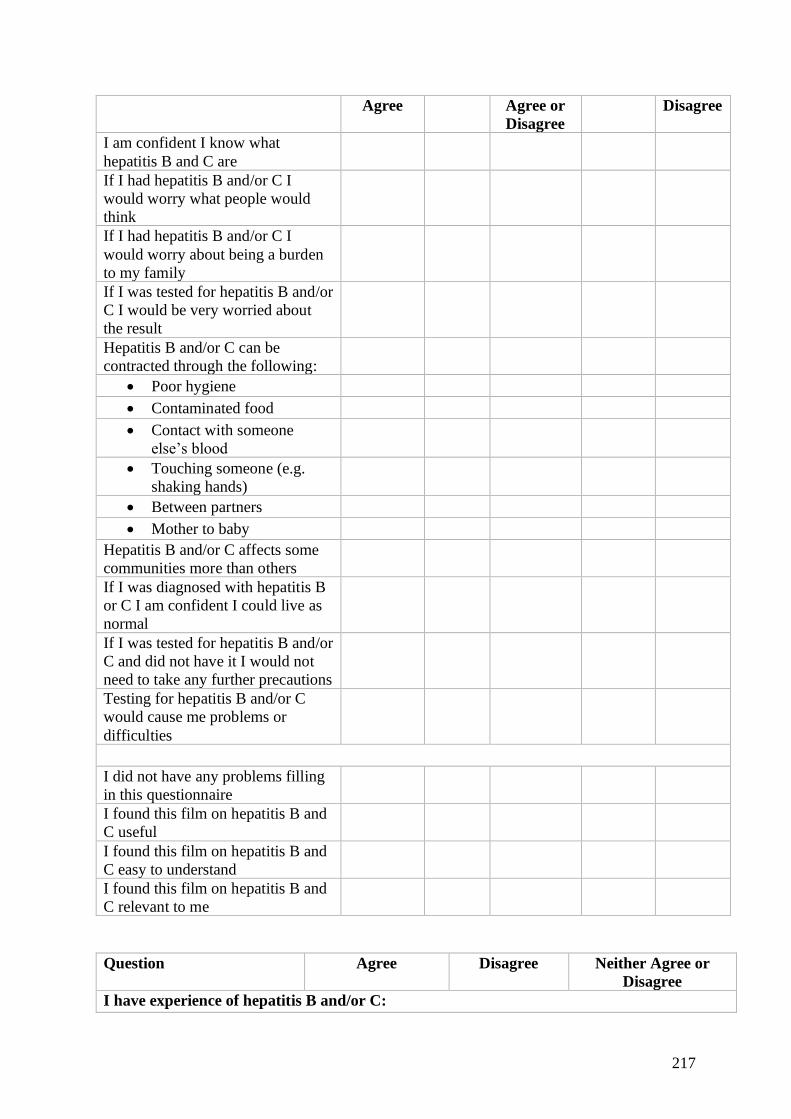
217
Agree Agree or
Disagree
Disagree
I am confident I know what
hepatitis B and C are
If I had hepatitis B and/or C I
would worry what people would
think
If I had hepatitis B and/or C I
would worry about being a burden
to my family
If I was tested for hepatitis B and/or
C I would be very worried about
the result
Hepatitis B and/or C can be
contracted through the following:
• Poor hygiene
• Contaminated food
• Contact with someone
else’s blood
• Touching someone (e.g.
shaking hands)
• Between partners
• Mother to baby
Hepatitis B and/or C affects some
communities more than others
If I was diagnosed with hepatitis B
or C I am confident I could live as
normal
If I was tested for hepatitis B and/or
C and did not have it I would not
need to take any further precautions
Testing for hepatitis B and/or C
would cause me problems or
difficulties
I did not have any problems filling
in this questionnaire
I found this film on hepatitis B and
C useful
I found this film on hepatitis B and
C easy to understand
I found this film on hepatitis B and
C relevant to me
Question Agree Disagree Neither Agree or
Disagree
I have experience of hepatitis B and/or C:
218
• Myself
• Someone important to
me (family or friends)
• I have heard of people
with it
• I do not have
experience of hepatitis
I would consider getting myself tested for hepatitis B and/or C if it was recommended by:
• My doctor
• My friends or family
• I heard about it
somewhere else (e.g.
TV, social media)
• Someone else
important to me
recommended it (e.g.
community leader)
• I would not consider
testing
I am planning to get tested for hepatitis B and/or C:
• Never
• Soon
• Within the next year
• At some point
Thank you for your time and participation in this study. Please leave any further comments
on this study, the film or the questionnaire in the box below:

219
APPENDIX 5: FULL RESULTS OF PRE AND POST FILM QUESTIONNAIRE
A breakdown of the replies to each question is detailed below (see Table 19 to Table 61). In
order to follow patterns of response more clearly, I have combined agree and strongly agree as
one reply in most questions, and the same for disagree and strongly disagree. Individual
questions can be combined into broad categories, or themes, reflecting attitudes of the
participants to health and health care; knowledge of chronic viral hepatitis; stigma;
transmission and infection with CVH; utility of the study intervention and processes;
experience of CVH; factors influencing testing and intention to test.
I. Attitudes to health and healthcare
The questions in this section were designed to help understand the general beliefs of
participants rather than having an expectation their answers to these questions would
necessarily change in response to the film.
Q1: I think it is important to do what I can to protect myself from illness even if I have a very
busy life
Of those who responded all people either agreed or strongly agreed that they should do what
they can to remain healthy, even when busy with life tasks. This was the same for those who
tested and those who did not. Relatively few did not respond to this question (<5% for both
groups) which could suggest a degree of certainty with the answer to this question.
Tested, n= (%) Non Tested, n= (%)
Invalid 3 (2.5) 1 (4)
Unchanged Pre- Post-Film Responses
Agree/Strongly Agree 115 (97.5) 24 (96)
Table 19: Change in pre and post film responses (Q1)
Q2: Regular health checks are important to avoid health problems even if I feel well
Again, there were few invalid responses (<5% each group). Of the valid responses, the vast
majority did not change their mind (98%: tested 97%; non-tested 100%) with most people in
both groups either agreeing or strongly agreeing (100% tested and 96% non-tested). Only small
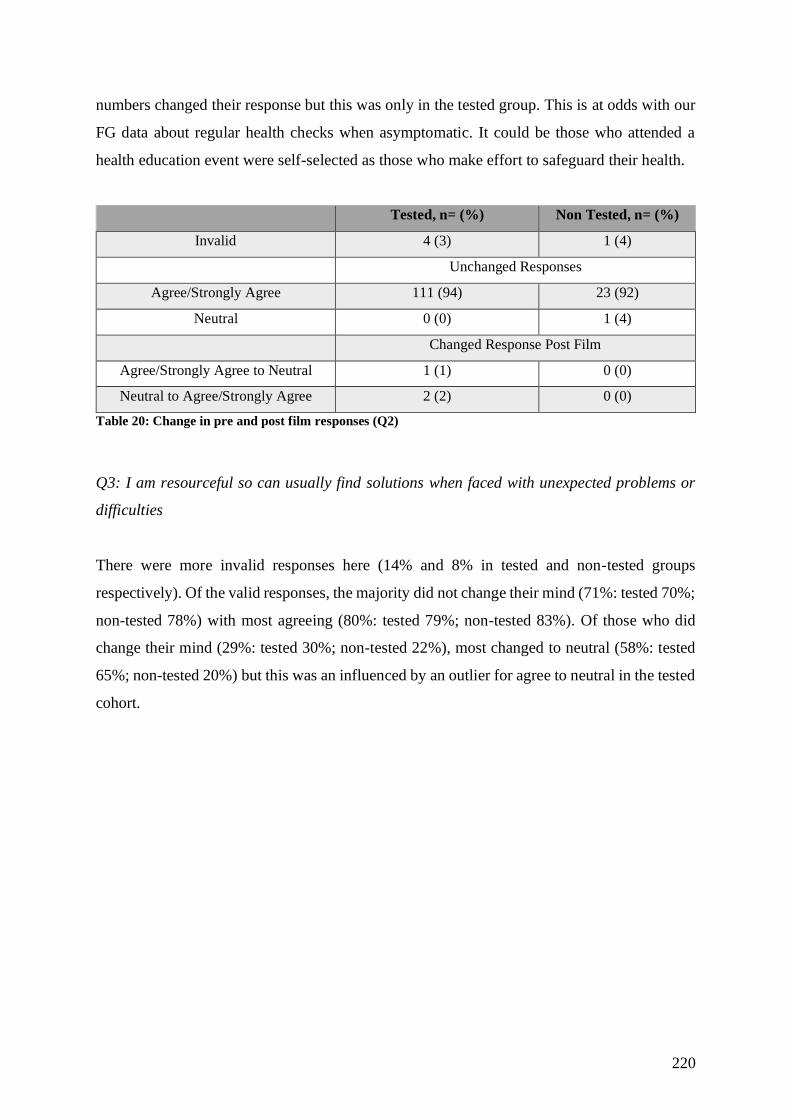
220
numbers changed their response but this was only in the tested group. This is at odds with our
FG data about regular health checks when asymptomatic. It could be those who attended a
health education event were self-selected as those who make effort to safeguard their health.
Tested, n= (%) Non Tested, n= (%)
Invalid 4 (3) 1 (4)
Unchanged Responses
Agree/Strongly Agree 111 (94) 23 (92)
Neutral 0 (0) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 0 (0)
Neutral to Agree/Strongly Agree 2 (2) 0 (0)
Table 20: Change in pre and post film responses (Q2)
Q3: I am resourceful so can usually find solutions when faced with unexpected problems or
difficulties
There were more invalid responses here (14% and 8% in tested and non-tested groups
respectively). Of the valid responses, the majority did not change their mind (71%: tested 70%;
non-tested 78%) with most agreeing (80%: tested 79%; non-tested 83%). Of those who did
change their mind (29%: tested 30%; non-tested 22%), most changed to neutral (58%: tested
65%; non-tested 20%) but this was an influenced by an outlier for agree to neutral in the tested
cohort.
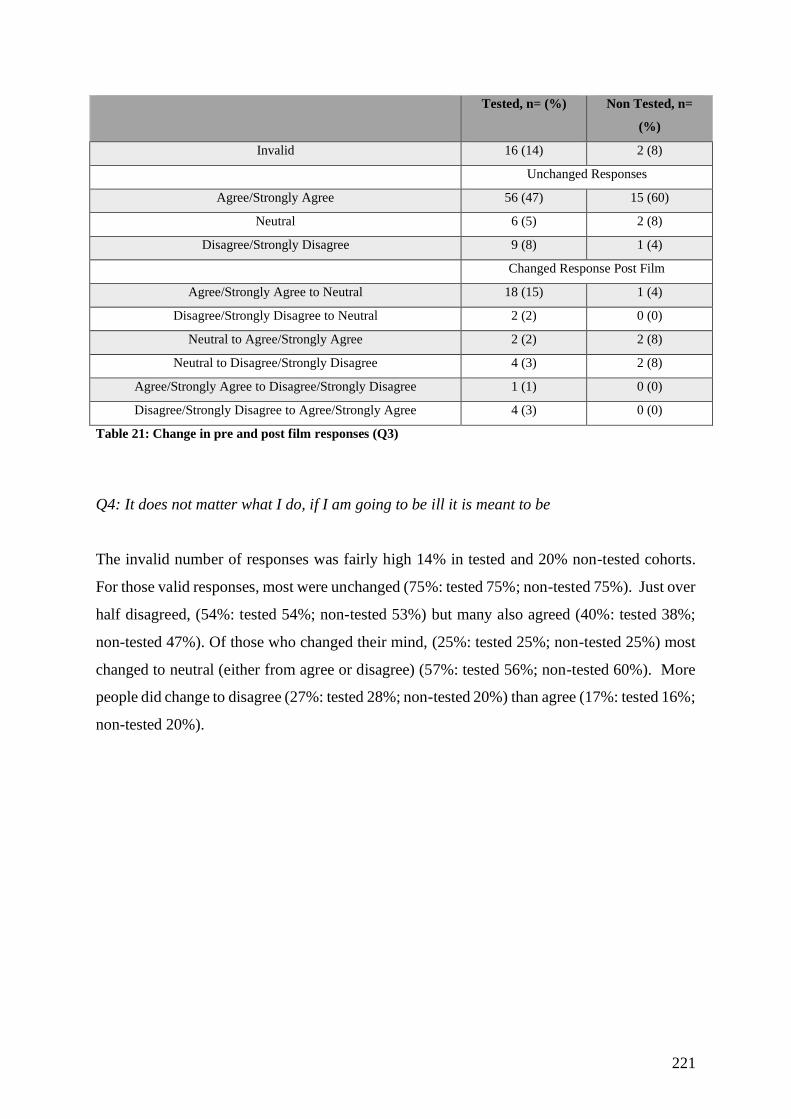
221
Tested, n= (%) Non Tested, n=
(%)
Invalid 16 (14) 2 (8)
Unchanged Responses
Agree/Strongly Agree 56 (47) 15 (60)
Neutral 6 (5) 2 (8)
Disagree/Strongly Disagree 9 (8) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 18 (15) 1 (4)
Disagree/Strongly Disagree to Neutral 2 (2) 0 (0)
Neutral to Agree/Strongly Agree 2 (2) 2 (8)
Neutral to Disagree/Strongly Disagree 4 (3) 2 (8)
Agree/Strongly Agree to Disagree/Strongly Disagree 1 (1) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 0 (0)
Table 21: Change in pre and post film responses (Q3)
Q4: It does not matter what I do, if I am going to be ill it is meant to be
The invalid number of responses was fairly high 14% in tested and 20% non-tested cohorts.
For those valid responses, most were unchanged (75%: tested 75%; non-tested 75%). Just over
half disagreed, (54%: tested 54%; non-tested 53%) but many also agreed (40%: tested 38%;
non-tested 47%). Of those who changed their mind, (25%: tested 25%; non-tested 25%) most
changed to neutral (either from agree or disagree) (57%: tested 56%; non-tested 60%). More
people did change to disagree (27%: tested 28%; non-tested 20%) than agree (17%: tested 16%;
non-tested 20%).
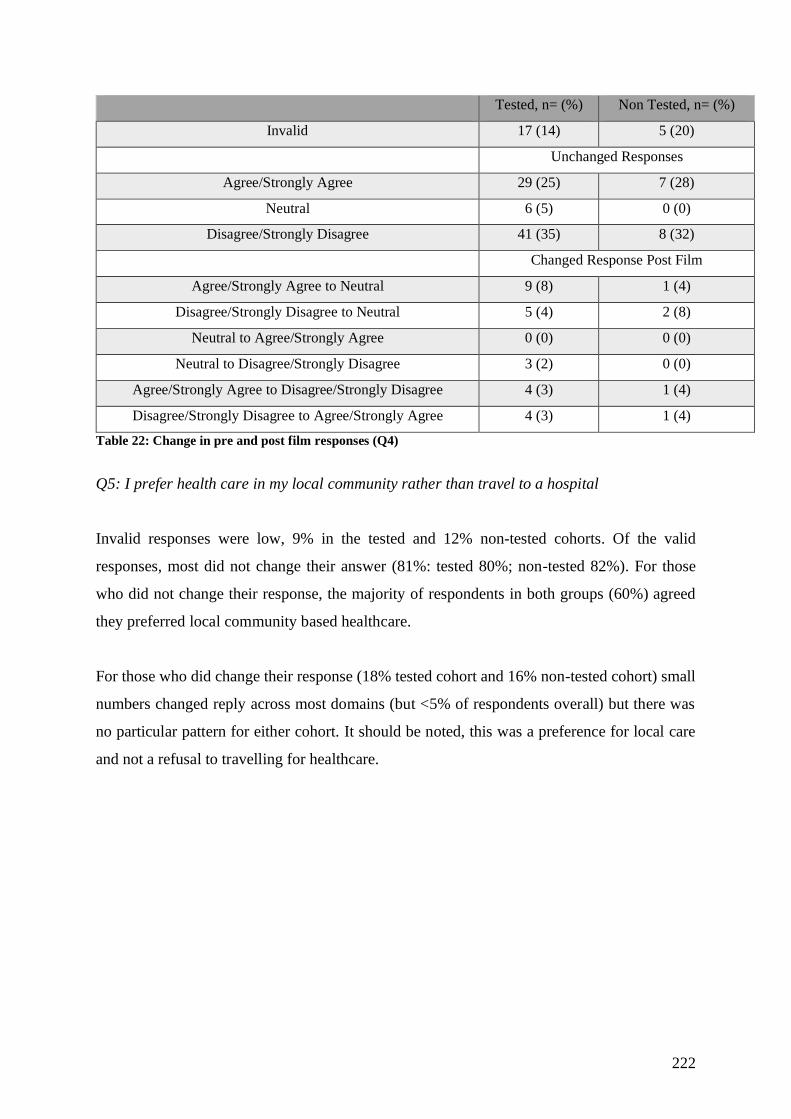
222
Tested, n= (%) Non Tested, n= (%)
Invalid 17 (14) 5 (20)
Unchanged Responses
Agree/Strongly Agree 29 (25) 7 (28)
Neutral 6 (5) 0 (0)
Disagree/Strongly Disagree 41 (35) 8 (32)
Changed Response Post Film
Agree/Strongly Agree to Neutral 9 (8) 1 (4)
Disagree/Strongly Disagree to Neutral 5 (4) 2 (8)
Neutral to Agree/Strongly Agree 0 (0) 0 (0)
Neutral to Disagree/Strongly Disagree 3 (2) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 4 (3) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 1 (4)
Table 22: Change in pre and post film responses (Q4)
Q5: I prefer health care in my local community rather than travel to a hospital
Invalid responses were low, 9% in the tested and 12% non-tested cohorts. Of the valid
responses, most did not change their answer (81%: tested 80%; non-tested 82%). For those
who did not change their response, the majority of respondents in both groups (60%) agreed
they preferred local community based healthcare.
For those who did change their response (18% tested cohort and 16% non-tested cohort) small
numbers changed reply across most domains (but <5% of respondents overall) but there was
no particular pattern for either cohort. It should be noted, this was a preference for local care
and not a refusal to travelling for healthcare.
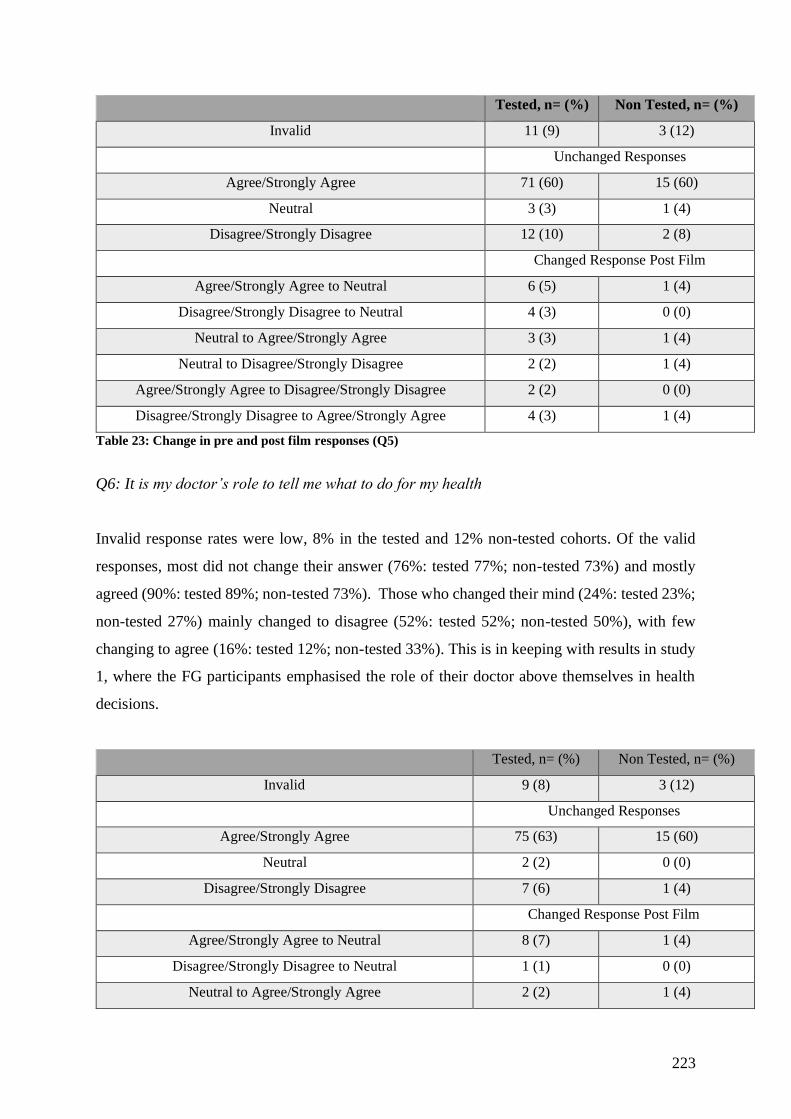
223
Tested, n= (%) Non Tested, n= (%)
Invalid 11 (9) 3 (12)
Unchanged Responses
Agree/Strongly Agree 71 (60) 15 (60)
Neutral 3 (3) 1 (4)
Disagree/Strongly Disagree 12 (10) 2 (8)
Changed Response Post Film
Agree/Strongly Agree to Neutral 6 (5) 1 (4)
Disagree/Strongly Disagree to Neutral 4 (3) 0 (0)
Neutral to Agree/Strongly Agree 3 (3) 1 (4)
Neutral to Disagree/Strongly Disagree 2 (2) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 2 (2) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 1 (4)
Table 23: Change in pre and post film responses (Q5)
Q6: It is my doctor’s role to tell me what to do for my health
Invalid response rates were low, 8% in the tested and 12% non-tested cohorts. Of the valid
responses, most did not change their answer (76%: tested 77%; non-tested 73%) and mostly
agreed (90%: tested 89%; non-tested 73%). Those who changed their mind (24%: tested 23%;
non-tested 27%) mainly changed to disagree (52%: tested 52%; non-tested 50%), with few
changing to agree (16%: tested 12%; non-tested 33%). This is in keeping with results in study
1, where the FG participants emphasised the role of their doctor above themselves in health
decisions.
Tested, n= (%) Non Tested, n= (%)
Invalid 9 (8) 3 (12)
Unchanged Responses
Agree/Strongly Agree 75 (63) 15 (60)
Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree 7 (6) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 8 (7) 1 (4)
Disagree/Strongly Disagree to Neutral 1 (1) 0 (0)
Neutral to Agree/Strongly Agree 2 (2) 1 (4)
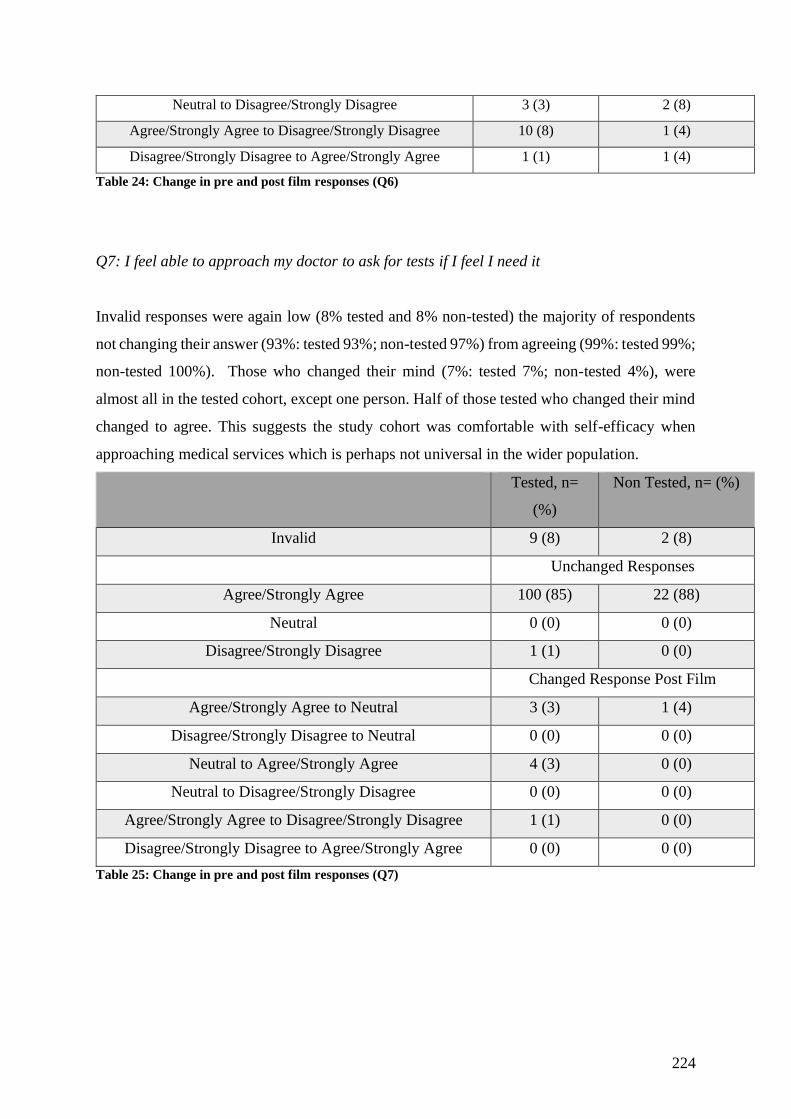
224
Neutral to Disagree/Strongly Disagree 3 (3) 2 (8)
Agree/Strongly Agree to Disagree/Strongly Disagree 10 (8) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 1 (1) 1 (4)
Table 24: Change in pre and post film responses (Q6)
Q7: I feel able to approach my doctor to ask for tests if I feel I need it
Invalid responses were again low (8% tested and 8% non-tested) the majority of respondents
not changing their answer (93%: tested 93%; non-tested 97%) from agreeing (99%: tested 99%;
non-tested 100%). Those who changed their mind (7%: tested 7%; non-tested 4%), were
almost all in the tested cohort, except one person. Half of those tested who changed their mind
changed to agree. This suggests the study cohort was comfortable with self-efficacy when
approaching medical services which is perhaps not universal in the wider population.
Tested, n=
(%)
Non Tested, n= (%)
Invalid 9 (8) 2 (8)
Unchanged Responses
Agree/Strongly Agree 100 (85) 22 (88)
Neutral 0 (0) 0 (0)
Disagree/Strongly Disagree 1 (1) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (3) 1 (4)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 4 (3) 0 (0)
Neutral to Disagree/Strongly Disagree 0 (0) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 1 (1) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 0 (0) 0 (0)
Table 25: Change in pre and post film responses (Q7)
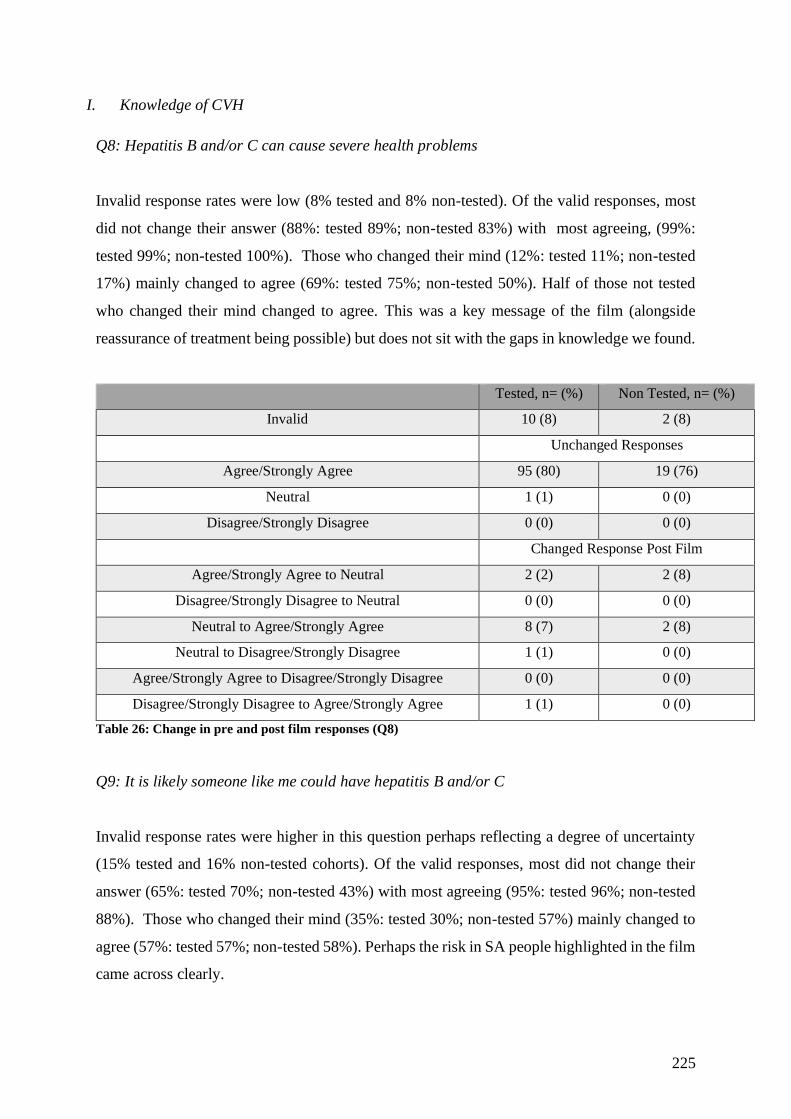
225
I. Knowledge of CVH
Q8: Hepatitis B and/or C can cause severe health problems
Invalid response rates were low (8% tested and 8% non-tested). Of the valid responses, most
did not change their answer (88%: tested 89%; non-tested 83%) with most agreeing, (99%:
tested 99%; non-tested 100%). Those who changed their mind (12%: tested 11%; non-tested
17%) mainly changed to agree (69%: tested 75%; non-tested 50%). Half of those not tested
who changed their mind changed to agree. This was a key message of the film (alongside
reassurance of treatment being possible) but does not sit with the gaps in knowledge we found.
Tested, n= (%) Non Tested, n= (%)
Invalid 10 (8) 2 (8)
Unchanged Responses
Agree/Strongly Agree 95 (80) 19 (76)
Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree 0 (0) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 2 (2) 2 (8)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 8 (7) 2 (8)
Neutral to Disagree/Strongly Disagree 1 (1) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 0 (0) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 1 (1) 0 (0)
Table 26: Change in pre and post film responses (Q8)
Q9: It is likely someone like me could have hepatitis B and/or C
Invalid response rates were higher in this question perhaps reflecting a degree of uncertainty
(15% tested and 16% non-tested cohorts). Of the valid responses, most did not change their
answer (65%: tested 70%; non-tested 43%) with most agreeing (95%: tested 96%; non-tested
88%). Those who changed their mind (35%: tested 30%; non-tested 57%) mainly changed to
agree (57%: tested 57%; non-tested 58%). Perhaps the risk in SA people highlighted in the film
came across clearly.
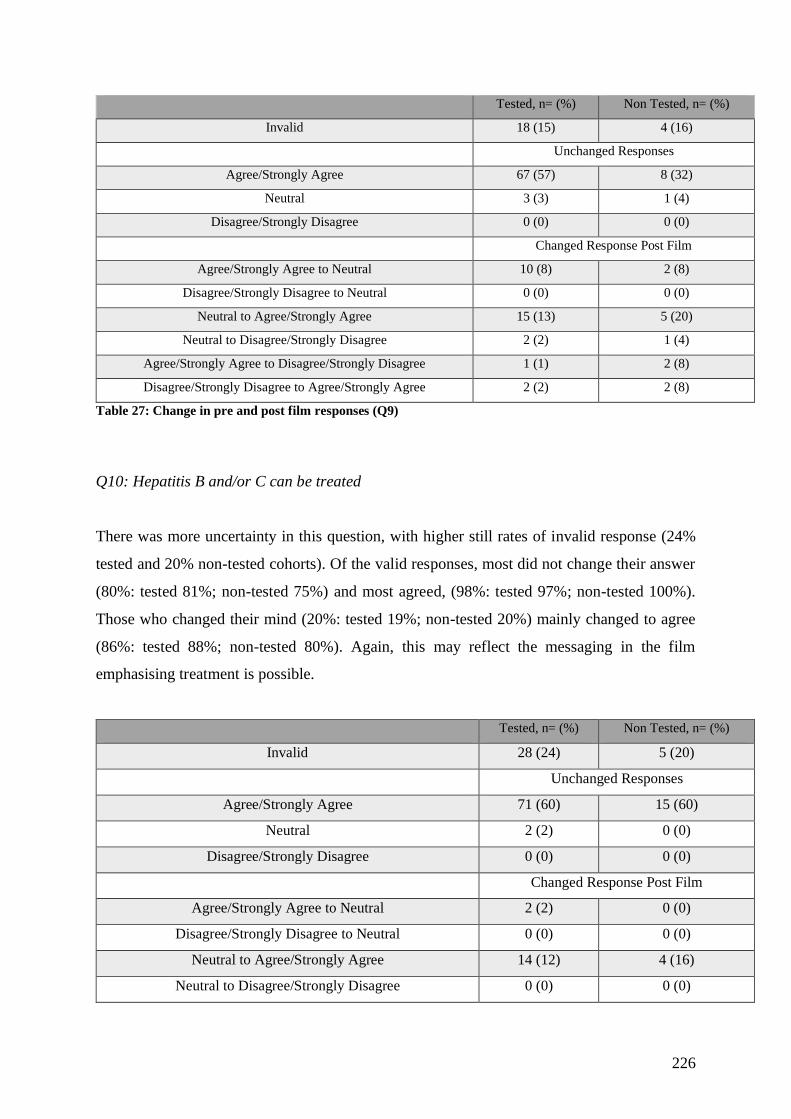
226
Tested, n= (%) Non Tested, n= (%)
Invalid 18 (15) 4 (16)
Unchanged Responses
Agree/Strongly Agree 67 (57) 8 (32)
Neutral 3 (3) 1 (4)
Disagree/Strongly Disagree 0 (0) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 10 (8) 2 (8)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 15 (13) 5 (20)
Neutral to Disagree/Strongly Disagree 2 (2) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 1 (1) 2 (8)
Disagree/Strongly Disagree to Agree/Strongly Agree 2 (2) 2 (8)
Table 27: Change in pre and post film responses (Q9)
Q10: Hepatitis B and/or C can be treated
There was more uncertainty in this question, with higher still rates of invalid response (24%
tested and 20% non-tested cohorts). Of the valid responses, most did not change their answer
(80%: tested 81%; non-tested 75%) and most agreed, (98%: tested 97%; non-tested 100%).
Those who changed their mind (20%: tested 19%; non-tested 20%) mainly changed to agree
(86%: tested 88%; non-tested 80%). Again, this may reflect the messaging in the film
emphasising treatment is possible.
Tested, n= (%) Non Tested, n= (%)
Invalid 28 (24) 5 (20)
Unchanged Responses
Agree/Strongly Agree 71 (60) 15 (60)
Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree 0 (0) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 14 (12) 4 (16)
Neutral to Disagree/Strongly Disagree 0 (0) 0 (0)

227
Agree/Strongly Agree to Disagree/Strongly Disagree 0 (0) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 1 (1) 0 (0)
Table 28: Change in pre and post film responses (Q10)
Q11: I have been tested before for hepatitis B &/or C
Invalid responses were again high (21% tested and 28% non-tested). This could reflect
concerns about confidentiality as well as uncertainty with knowledge. Of the valid responses,
most did not change their answer (64%: tested 60%; non-tested 83%) and whilst almost half
disagreed (49%: tested 48%; non-tested 53%) many also agreed (25%: tested 25%; non-tested
27%) with similar proportions neutral (25%: tested 27%; non-tested 20%). Those who changed
their mind (36%: tested 40%; non-tested 17%) mainly changed to disagree (50%: tested 51%;
non-tested 33%). In those who tested and who changed their mind, a change to disagree they
have been tested before was seen in 51%. Perhaps post film they better understood what CVH
was. However, this cannot be compared with the non-tested cohort as very small numbers
changed their mind, limiting interpretation.
Tested, n= (%) Non Tested, n= (%)
Invalid 25 (21) 7 (28)
Unchanged Responses
Agree/Strongly Agree 14 (12) 4 (16)
Neutral 15 (13) 3 (12)
Disagree/Strongly Disagree 27 (23) 8 (32)
Changed Response Post Film
Agree/Strongly Agree to Neutral 7 (6) 0 (0)
Disagree/Strongly Disagree to Neutral 8 (7) 0 (0)
Neutral to Agree/Strongly Agree 2 (2) 0 (0)
Neutral to Disagree/Strongly Disagree 12 (10) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 7 (6) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 1 (1) 2 (8)
Table 29: Change in pre and post film responses (Q11)
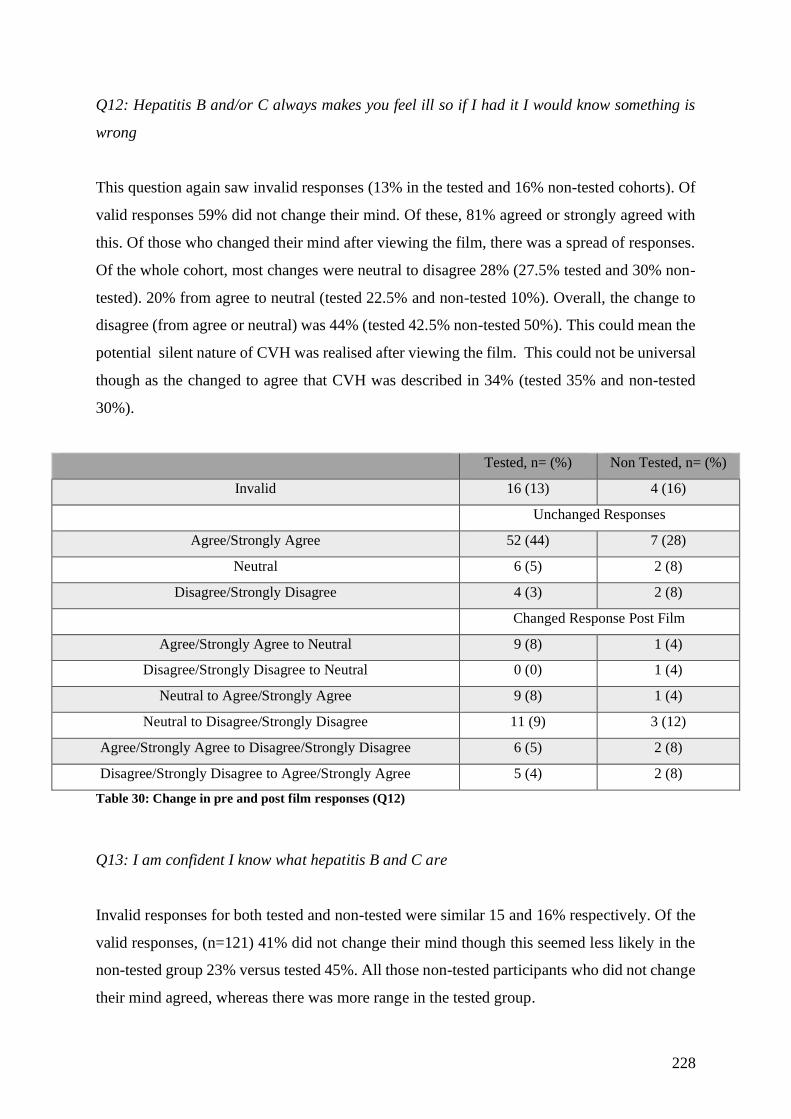
228
Q12: Hepatitis B and/or C always makes you feel ill so if I had it I would know something is
wrong
This question again saw invalid responses (13% in the tested and 16% non-tested cohorts). Of
valid responses 59% did not change their mind. Of these, 81% agreed or strongly agreed with
this. Of those who changed their mind after viewing the film, there was a spread of responses.
Of the whole cohort, most changes were neutral to disagree 28% (27.5% tested and 30% non-
tested). 20% from agree to neutral (tested 22.5% and non-tested 10%). Overall, the change to
disagree (from agree or neutral) was 44% (tested 42.5% non-tested 50%). This could mean the
potential silent nature of CVH was realised after viewing the film. This could not be universal
though as the changed to agree that CVH was described in 34% (tested 35% and non-tested
30%).
Tested, n= (%) Non Tested, n= (%)
Invalid 16 (13) 4 (16)
Unchanged Responses
Agree/Strongly Agree 52 (44) 7 (28)
Neutral 6 (5) 2 (8)
Disagree/Strongly Disagree 4 (3) 2 (8)
Changed Response Post Film
Agree/Strongly Agree to Neutral 9 (8) 1 (4)
Disagree/Strongly Disagree to Neutral 0 (0) 1 (4)
Neutral to Agree/Strongly Agree 9 (8) 1 (4)
Neutral to Disagree/Strongly Disagree 11 (9) 3 (12)
Agree/Strongly Agree to Disagree/Strongly Disagree 6 (5) 2 (8)
Disagree/Strongly Disagree to Agree/Strongly Agree 5 (4) 2 (8)
Table 30: Change in pre and post film responses (Q12)
Q13: I am confident I know what hepatitis B and C are
Invalid responses for both tested and non-tested were similar 15 and 16% respectively. Of the
valid responses, (n=121) 41% did not change their mind though this seemed less likely in the
non-tested group 23% versus tested 45%. All those non-tested participants who did not change
their mind agreed, whereas there was more range in the tested group.

229
Most people who changed their mind did so to agree after the film, of the whole cohort who
changed their mind this was 77% (tested 76% and non-tested 81%).
Tested, n= (%) Non Tested, n= (%)
Invalid 18 (15) 4 (16)
Unchanged Responses
Agree/Strongly Agree 28 (24) 5 (20)
Neutral 10 (8) 0 (0)
Disagree/Strongly Disagree 7 (6) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 2 (2) 1 (4)
Disagree/Strongly Disagree to Neutral 5 (4) 2 (8)
Neutral to Agree/Strongly Agree 18 (15) 6 (24)
Neutral to Disagree/Strongly Disagree 4 (3) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 2 (2) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 24 (20) 7 (28)
Table 31: Change in pre and post film responses (Q13)
II. Stigma
Q14: If I had hepatitis B and/or C I would worry what people would think
Of the valid responses, n=115, 62% did not change their mind however there was a spread of
answers. Of those valid responses 42% agreed (tested 44% non-tested 36%) they would be
worried what people would think of them if they had CVH whilst 45% disagreed (tested 44%,
non-tested 43%). Most people who changed their mind changed from agree to neutral (39%)
which was 41% tested and 29% non-tested. This may mean we successfully targeted concerns
of stigma.
Tested, n= (%) Non Tested, n= (%)
Invalid 24 (20) 4 (16)
Unchanged Responses
Agree/Strongly Agree 25 (21) 5 (20)
Neutral 7 (6) 3 (12)
Disagree/Strongly Disagree 25 (21) 6 (24)
Changed Response Post Film
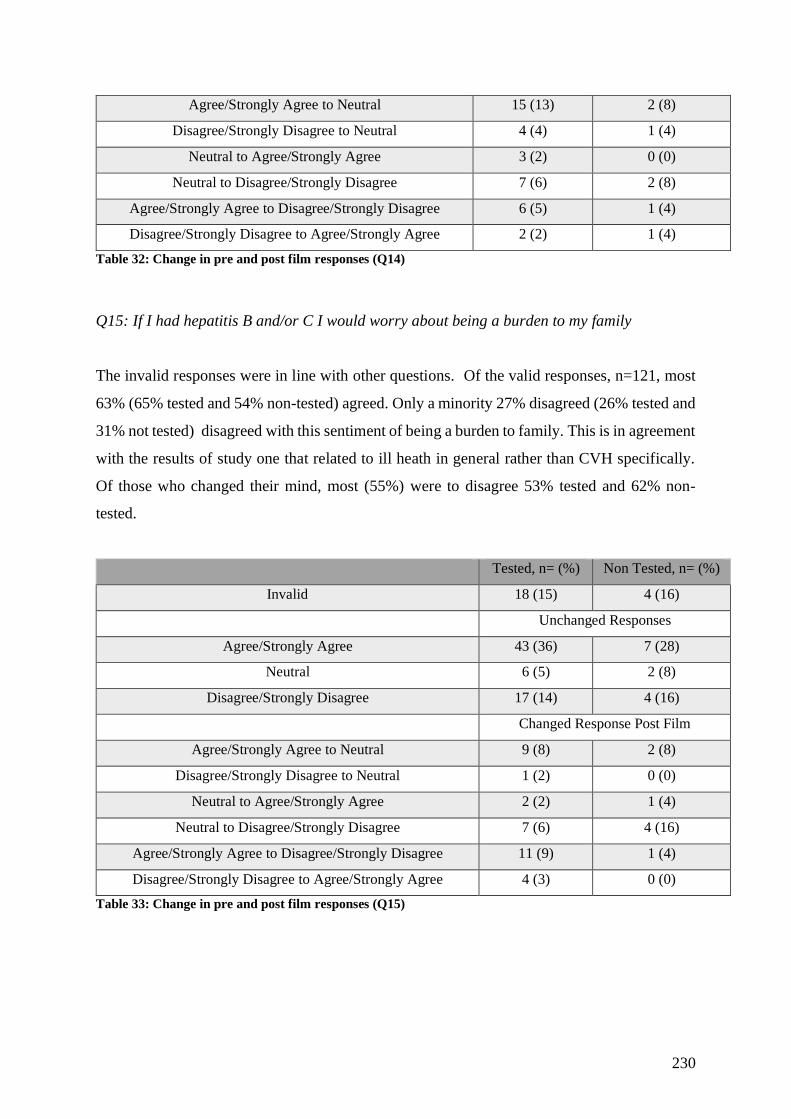
230
Agree/Strongly Agree to Neutral 15 (13) 2 (8)
Disagree/Strongly Disagree to Neutral 4 (4) 1 (4)
Neutral to Agree/Strongly Agree 3 (2) 0 (0)
Neutral to Disagree/Strongly Disagree 7 (6) 2 (8)
Agree/Strongly Agree to Disagree/Strongly Disagree 6 (5) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 2 (2) 1 (4)
Table 32: Change in pre and post film responses (Q14)
Q15: If I had hepatitis B and/or C I would worry about being a burden to my family
The invalid responses were in line with other questions. Of the valid responses, n=121, most
63% (65% tested and 54% non-tested) agreed. Only a minority 27% disagreed (26% tested and
31% not tested) disagreed with this sentiment of being a burden to family. This is in agreement
with the results of study one that related to ill heath in general rather than CVH specifically.
Of those who changed their mind, most (55%) were to disagree 53% tested and 62% non-
tested.
Tested, n= (%) Non Tested, n= (%)
Invalid 18 (15) 4 (16)
Unchanged Responses
Agree/Strongly Agree 43 (36) 7 (28)
Neutral 6 (5) 2 (8)
Disagree/Strongly Disagree 17 (14) 4 (16)
Changed Response Post Film
Agree/Strongly Agree to Neutral 9 (8) 2 (8)
Disagree/Strongly Disagree to Neutral 1 (2) 0 (0)
Neutral to Agree/Strongly Agree 2 (2) 1 (4)
Neutral to Disagree/Strongly Disagree 7 (6) 4 (16)
Agree/Strongly Agree to Disagree/Strongly Disagree 11 (9) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 0 (0)
Table 33: Change in pre and post film responses (Q15)
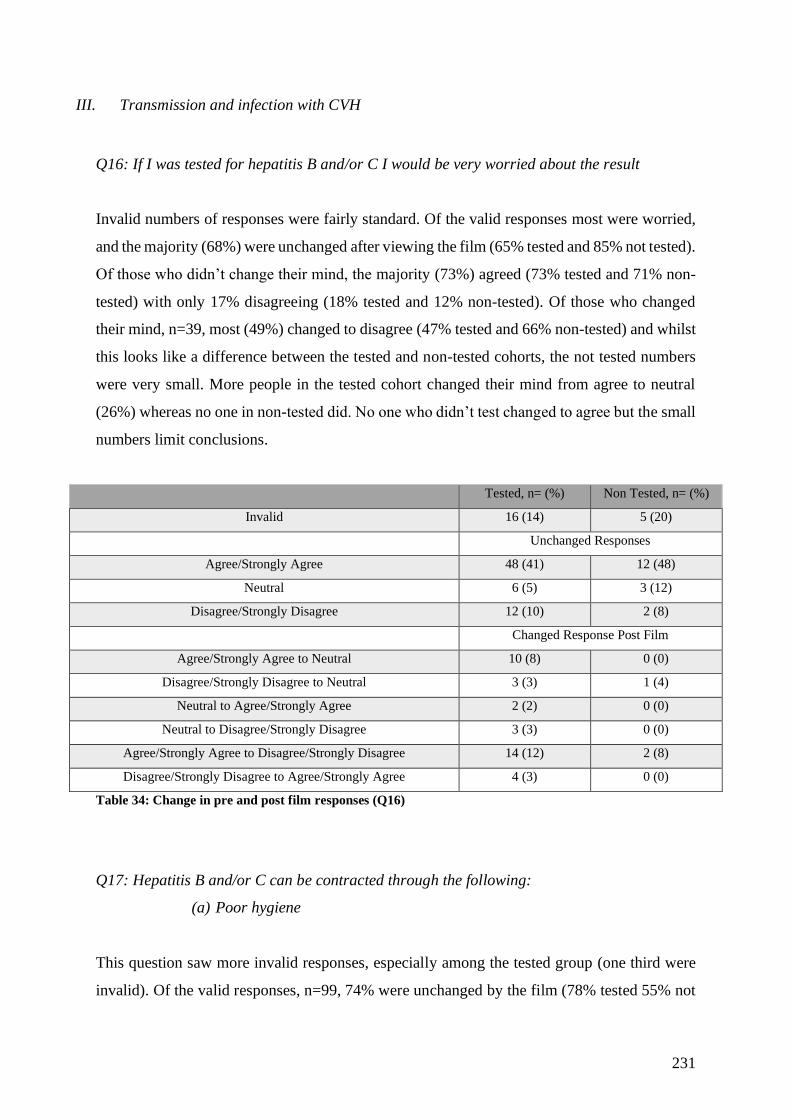
231
III. Transmission and infection with CVH
Q16: If I was tested for hepatitis B and/or C I would be very worried about the result
Invalid numbers of responses were fairly standard. Of the valid responses most were worried,
and the majority (68%) were unchanged after viewing the film (65% tested and 85% not tested).
Of those who didn’t change their mind, the majority (73%) agreed (73% tested and 71% non-
tested) with only 17% disagreeing (18% tested and 12% non-tested). Of those who changed
their mind, n=39, most (49%) changed to disagree (47% tested and 66% non-tested) and whilst
this looks like a difference between the tested and non-tested cohorts, the not tested numbers
were very small. More people in the tested cohort changed their mind from agree to neutral
(26%) whereas no one in non-tested did. No one who didn’t test changed to agree but the small
numbers limit conclusions.
Tested, n= (%) Non Tested, n= (%)
Invalid 16 (14) 5 (20)
Unchanged Responses
Agree/Strongly Agree 48 (41) 12 (48)
Neutral 6 (5) 3 (12)
Disagree/Strongly Disagree 12 (10) 2 (8)
Changed Response Post Film
Agree/Strongly Agree to Neutral 10 (8) 0 (0)
Disagree/Strongly Disagree to Neutral 3 (3) 1 (4)
Neutral to Agree/Strongly Agree 2 (2) 0 (0)
Neutral to Disagree/Strongly Disagree 3 (3) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 14 (12) 2 (8)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 0 (0)
Table 34: Change in pre and post film responses (Q16)
Q17: Hepatitis B and/or C can be contracted through the following:
(a) Poor hygiene
This question saw more invalid responses, especially among the tested group (one third were
invalid). Of the valid responses, n=99, 74% were unchanged by the film (78% tested 55% not
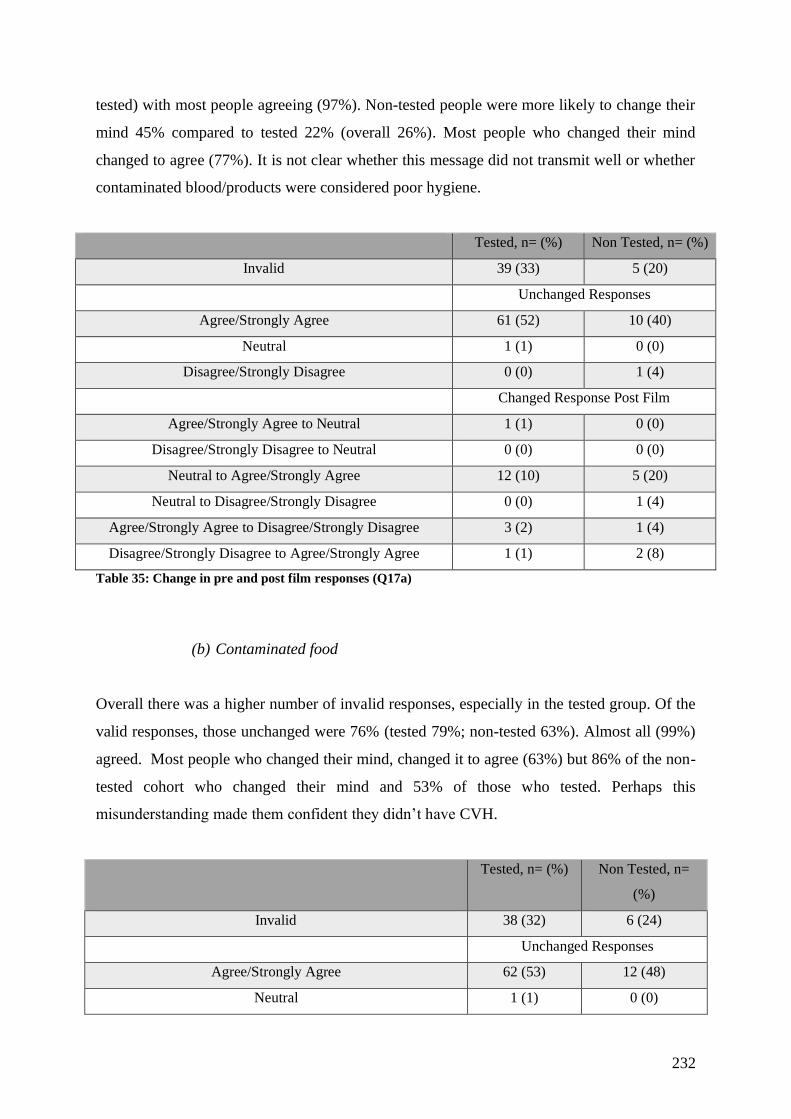
232
tested) with most people agreeing (97%). Non-tested people were more likely to change their
mind 45% compared to tested 22% (overall 26%). Most people who changed their mind
changed to agree (77%). It is not clear whether this message did not transmit well or whether
contaminated blood/products were considered poor hygiene.
Tested, n= (%) Non Tested, n= (%)
Invalid 39 (33) 5 (20)
Unchanged Responses
Agree/Strongly Agree 61 (52) 10 (40)
Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree 0 (0) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 12 (10) 5 (20)
Neutral to Disagree/Strongly Disagree 0 (0) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 3 (2) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 1 (1) 2 (8)
Table 35: Change in pre and post film responses (Q17a)
(b) Contaminated food
Overall there was a higher number of invalid responses, especially in the tested group. Of the
valid responses, those unchanged were 76% (tested 79%; non-tested 63%). Almost all (99%)
agreed. Most people who changed their mind, changed it to agree (63%) but 86% of the non-
tested cohort who changed their mind and 53% of those who tested. Perhaps this
misunderstanding made them confident they didn’t have CVH.
Tested, n= (%) Non Tested, n=
(%)
Invalid 38 (32) 6 (24)
Unchanged Responses
Agree/Strongly Agree 62 (53) 12 (48)
Neutral 1 (1) 0 (0)

233
Disagree/Strongly Disagree 0 (0) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 7 (6) 3 (12)
Neutral to Disagree/Strongly Disagree 2 (1) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 4 (3) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 2 (2) 3 (12)
Table 36: Change in pre and post film responses (Q17b)
(c) Contact with someone else’s blood
This question saw fewer invalid responses compared with other questions in this category.
Of the valid responses, 74% were unchanged all of whom agreed. Of those who changed
their mind, most (60%) changed to agree 60% (55% who tested and 75% who did not).
This could mean those who did not test felt less at risk as they did not feel they have had
this contact.
Tested, n= (%) Non Tested, n=
(%)
Invalid 22 (19) 4 (16)
Unchanged Responses
Agree/Strongly Agree 74 (63) 13 (52)
Neutral 0 (0) 0 (0)
Disagree/Strongly Disagree 0 (0) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 9 (8) 5 (20)
Neutral to Disagree/Strongly Disagree 2 (2) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 5 (4) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 3 (2) 1 (4)
Table 37: Change in pre and post film responses (Q17c)
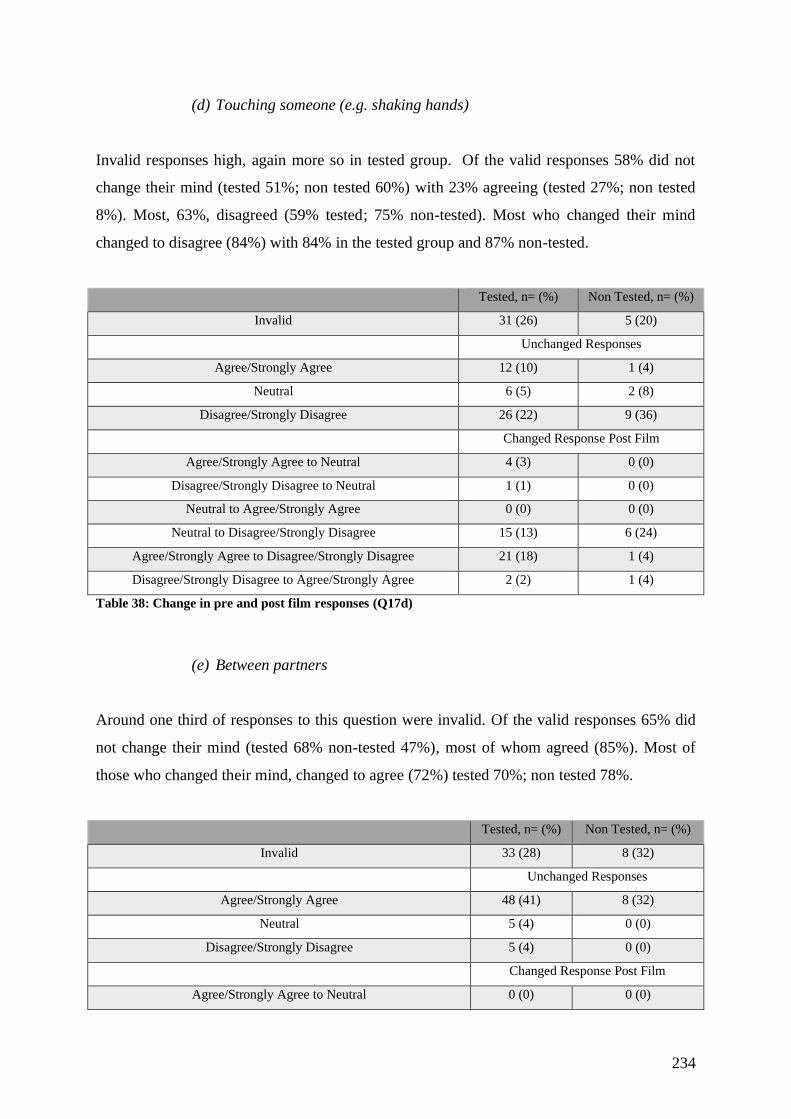
234
(d) Touching someone (e.g. shaking hands)
Invalid responses high, again more so in tested group. Of the valid responses 58% did not
change their mind (tested 51%; non tested 60%) with 23% agreeing (tested 27%; non tested
8%). Most, 63%, disagreed (59% tested; 75% non-tested). Most who changed their mind
changed to disagree (84%) with 84% in the tested group and 87% non-tested.
Tested, n= (%) Non Tested, n= (%)
Invalid 31 (26) 5 (20)
Unchanged Responses
Agree/Strongly Agree 12 (10) 1 (4)
Neutral 6 (5) 2 (8)
Disagree/Strongly Disagree 26 (22) 9 (36)
Changed Response Post Film
Agree/Strongly Agree to Neutral 4 (3) 0 (0)
Disagree/Strongly Disagree to Neutral 1 (1) 0 (0)
Neutral to Agree/Strongly Agree 0 (0) 0 (0)
Neutral to Disagree/Strongly Disagree 15 (13) 6 (24)
Agree/Strongly Agree to Disagree/Strongly Disagree 21 (18) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 2 (2) 1 (4)
Table 38: Change in pre and post film responses (Q17d)
(e) Between partners
Around one third of responses to this question were invalid. Of the valid responses 65% did
not change their mind (tested 68% non-tested 47%), most of whom agreed (85%). Most of
those who changed their mind, changed to agree (72%) tested 70%; non tested 78%.
Tested, n= (%) Non Tested, n= (%)
Invalid 33 (28) 8 (32)
Unchanged Responses
Agree/Strongly Agree 48 (41) 8 (32)
Neutral 5 (4) 0 (0)
Disagree/Strongly Disagree 5 (4) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 0 (0) 0 (0)
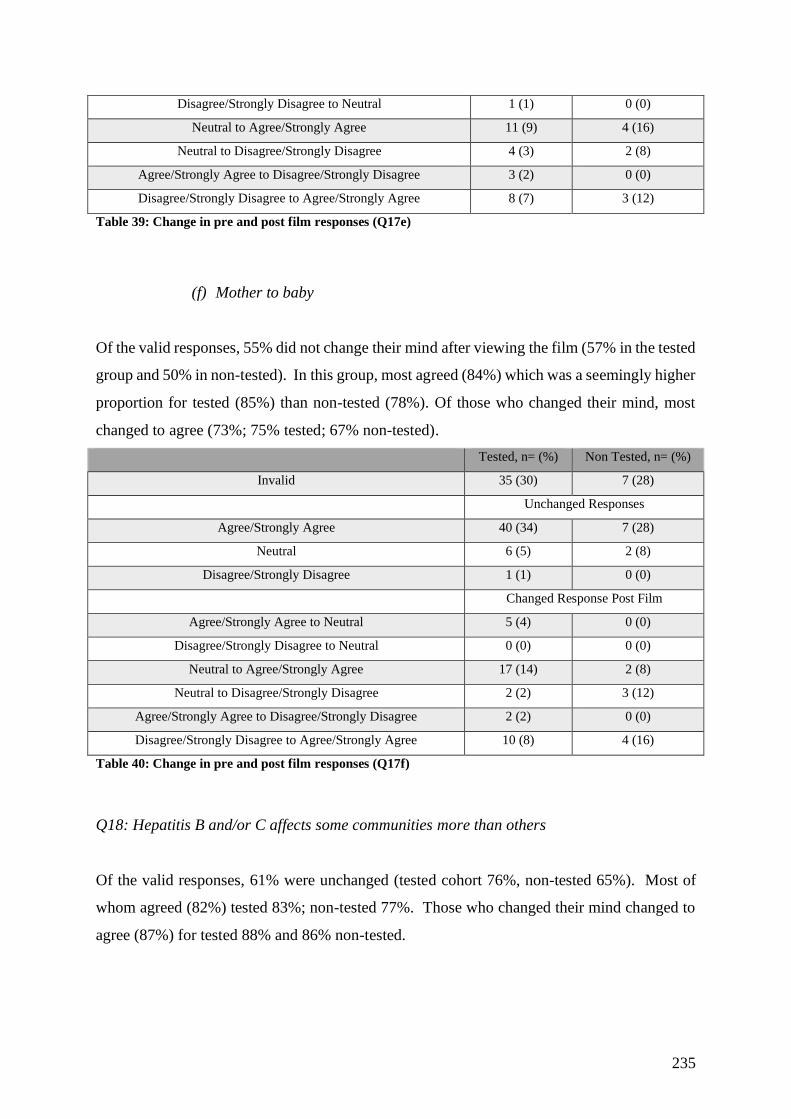
235
Disagree/Strongly Disagree to Neutral 1 (1) 0 (0)
Neutral to Agree/Strongly Agree 11 (9) 4 (16)
Neutral to Disagree/Strongly Disagree 4 (3) 2 (8)
Agree/Strongly Agree to Disagree/Strongly Disagree 3 (2) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 8 (7) 3 (12)
Table 39: Change in pre and post film responses (Q17e)
(f) Mother to baby
Of the valid responses, 55% did not change their mind after viewing the film (57% in the tested
group and 50% in non-tested). In this group, most agreed (84%) which was a seemingly higher
proportion for tested (85%) than non-tested (78%). Of those who changed their mind, most
changed to agree (73%; 75% tested; 67% non-tested).
Tested, n= (%) Non Tested, n= (%)
Invalid 35 (30) 7 (28)
Unchanged Responses
Agree/Strongly Agree 40 (34) 7 (28)
Neutral 6 (5) 2 (8)
Disagree/Strongly Disagree 1 (1) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 5 (4) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 17 (14) 2 (8)
Neutral to Disagree/Strongly Disagree 2 (2) 3 (12)
Agree/Strongly Agree to Disagree/Strongly Disagree 2 (2) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 10 (8) 4 (16)
Table 40: Change in pre and post film responses (Q17f)
Q18: Hepatitis B and/or C affects some communities more than others
Of the valid responses, 61% were unchanged (tested cohort 76%, non-tested 65%). Most of
whom agreed (82%) tested 83%; non-tested 77%. Those who changed their mind changed to
agree (87%) for tested 88% and 86% non-tested.
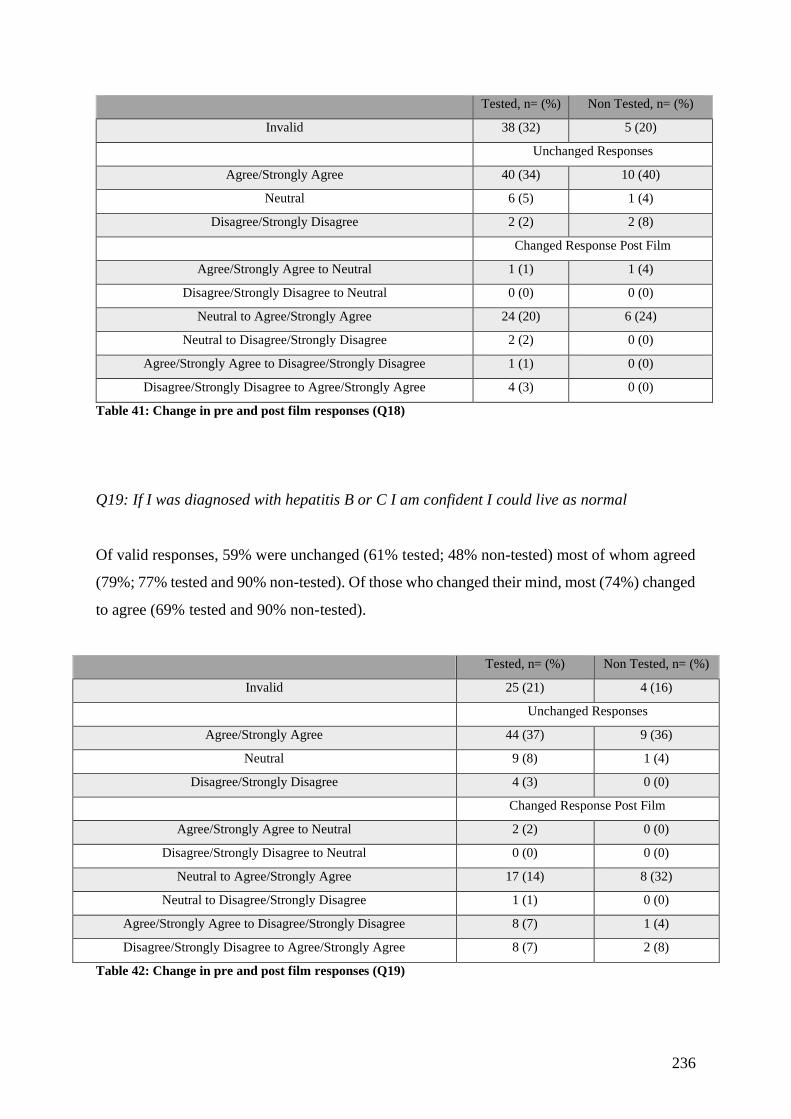
236
Tested, n= (%) Non Tested, n= (%)
Invalid 38 (32) 5 (20)
Unchanged Responses
Agree/Strongly Agree 40 (34) 10 (40)
Neutral 6 (5) 1 (4)
Disagree/Strongly Disagree 2 (2) 2 (8)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 1 (4)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 24 (20) 6 (24)
Neutral to Disagree/Strongly Disagree 2 (2) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 1 (1) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 0 (0)
Table 41: Change in pre and post film responses (Q18)
Q19: If I was diagnosed with hepatitis B or C I am confident I could live as normal
Of valid responses, 59% were unchanged (61% tested; 48% non-tested) most of whom agreed
(79%; 77% tested and 90% non-tested). Of those who changed their mind, most (74%) changed
to agree (69% tested and 90% non-tested).
Tested, n= (%) Non Tested, n= (%)
Invalid 25 (21) 4 (16)
Unchanged Responses
Agree/Strongly Agree 44 (37) 9 (36)
Neutral 9 (8) 1 (4)
Disagree/Strongly Disagree 4 (3) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 17 (14) 8 (32)
Neutral to Disagree/Strongly Disagree 1 (1) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 8 (7) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 8 (7) 2 (8)
Table 42: Change in pre and post film responses (Q19)
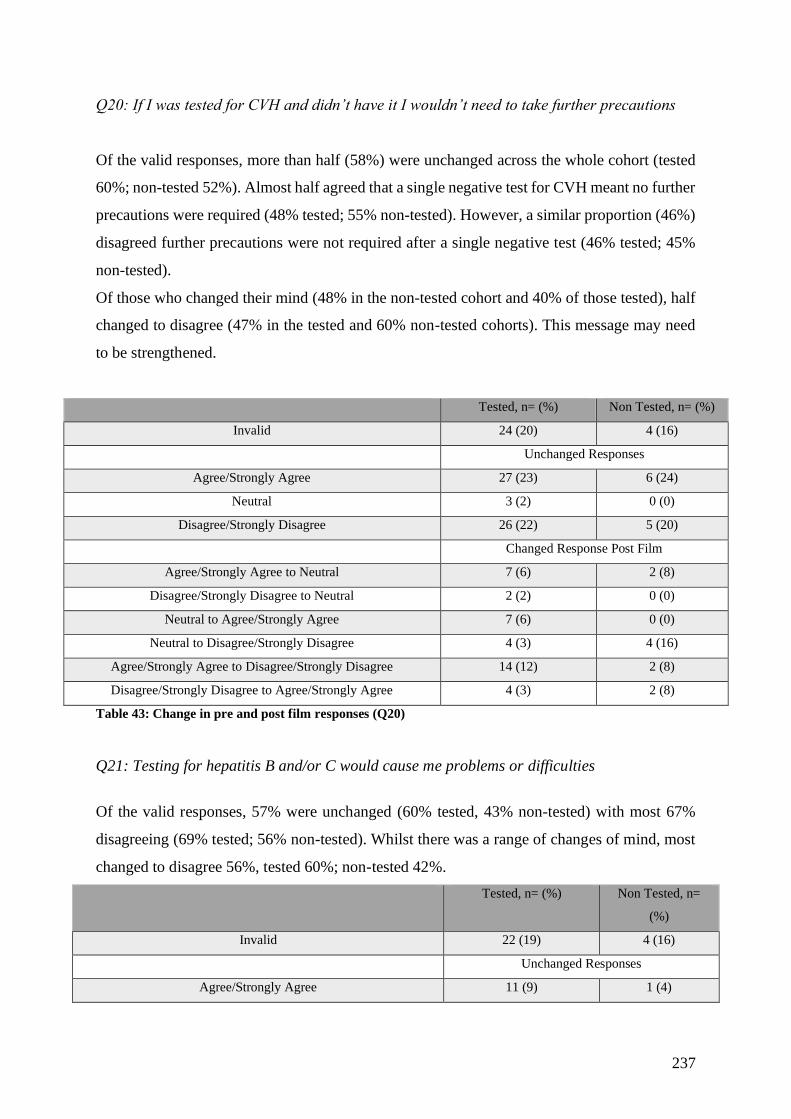
237
Q20: If I was tested for CVH and didn’t have it I wouldn’t need to take further precautions
Of the valid responses, more than half (58%) were unchanged across the whole cohort (tested
60%; non-tested 52%). Almost half agreed that a single negative test for CVH meant no further
precautions were required (48% tested; 55% non-tested). However, a similar proportion (46%)
disagreed further precautions were not required after a single negative test (46% tested; 45%
non-tested).
Of those who changed their mind (48% in the non-tested cohort and 40% of those tested), half
changed to disagree (47% in the tested and 60% non-tested cohorts). This message may need
to be strengthened.
Tested, n= (%) Non Tested, n= (%)
Invalid 24 (20) 4 (16)
Unchanged Responses
Agree/Strongly Agree 27 (23) 6 (24)
Neutral 3 (2) 0 (0)
Disagree/Strongly Disagree 26 (22) 5 (20)
Changed Response Post Film
Agree/Strongly Agree to Neutral 7 (6) 2 (8)
Disagree/Strongly Disagree to Neutral 2 (2) 0 (0)
Neutral to Agree/Strongly Agree 7 (6) 0 (0)
Neutral to Disagree/Strongly Disagree 4 (3) 4 (16)
Agree/Strongly Agree to Disagree/Strongly Disagree 14 (12) 2 (8)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 2 (8)
Table 43: Change in pre and post film responses (Q20)
Q21: Testing for hepatitis B and/or C would cause me problems or difficulties
Of the valid responses, 57% were unchanged (60% tested, 43% non-tested) with most 67%
disagreeing (69% tested; 56% non-tested). Whilst there was a range of changes of mind, most
changed to disagree 56%, tested 60%; non-tested 42%.
Tested, n= (%) Non Tested, n=
(%)
Invalid 22 (19) 4 (16)
Unchanged Responses
Agree/Strongly Agree 11 (9) 1 (4)
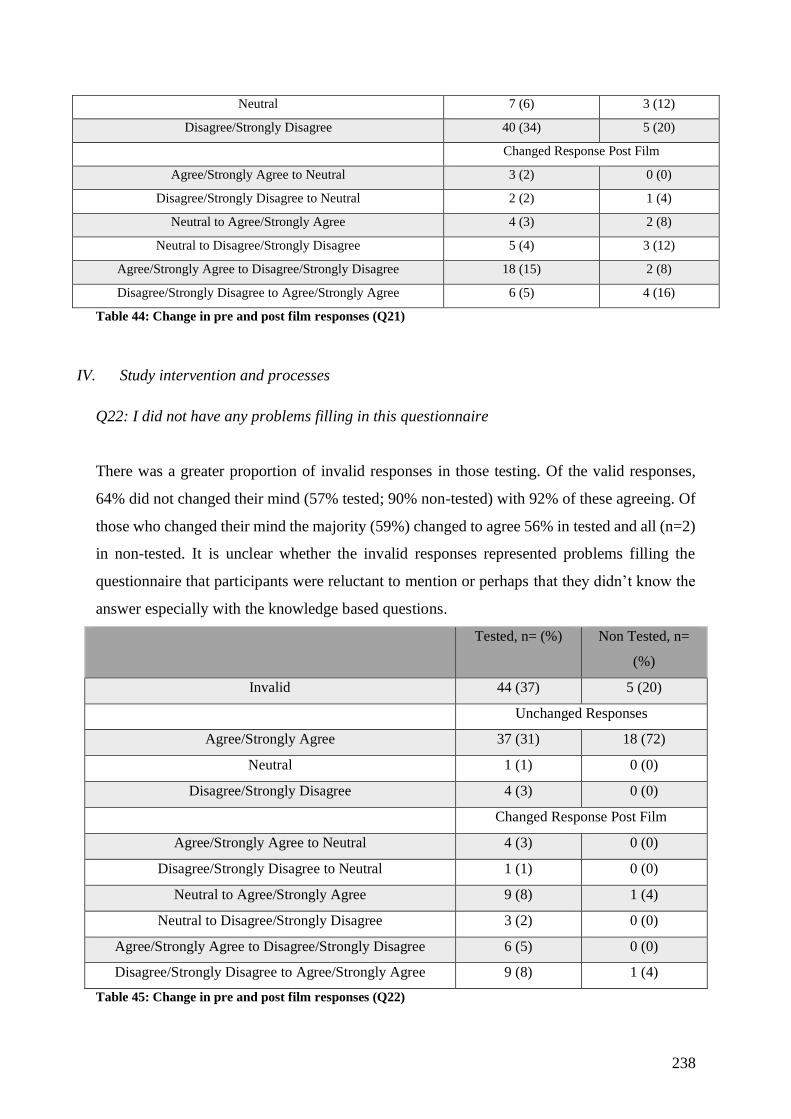
238
Neutral 7 (6) 3 (12)
Disagree/Strongly Disagree 40 (34) 5 (20)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 2 (2) 1 (4)
Neutral to Agree/Strongly Agree 4 (3) 2 (8)
Neutral to Disagree/Strongly Disagree 5 (4) 3 (12)
Agree/Strongly Agree to Disagree/Strongly Disagree 18 (15) 2 (8)
Disagree/Strongly Disagree to Agree/Strongly Agree 6 (5) 4 (16)
Table 44: Change in pre and post film responses (Q21)
IV. Study intervention and processes
Q22: I did not have any problems filling in this questionnaire
There was a greater proportion of invalid responses in those testing. Of the valid responses,
64% did not changed their mind (57% tested; 90% non-tested) with 92% of these agreeing. Of
those who changed their mind the majority (59%) changed to agree 56% in tested and all (n=2)
in non-tested. It is unclear whether the invalid responses represented problems filling the
questionnaire that participants were reluctant to mention or perhaps that they didn’t know the
answer especially with the knowledge based questions.
Tested, n= (%) Non Tested, n=
(%)
Invalid 44 (37) 5 (20)
Unchanged Responses
Agree/Strongly Agree 37 (31) 18 (72)
Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree 4 (3) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 4 (3) 0 (0)
Disagree/Strongly Disagree to Neutral 1 (1) 0 (0)
Neutral to Agree/Strongly Agree 9 (8) 1 (4)
Neutral to Disagree/Strongly Disagree 3 (2) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 6 (5) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 9 (8) 1 (4)
Table 45: Change in pre and post film responses (Q22)
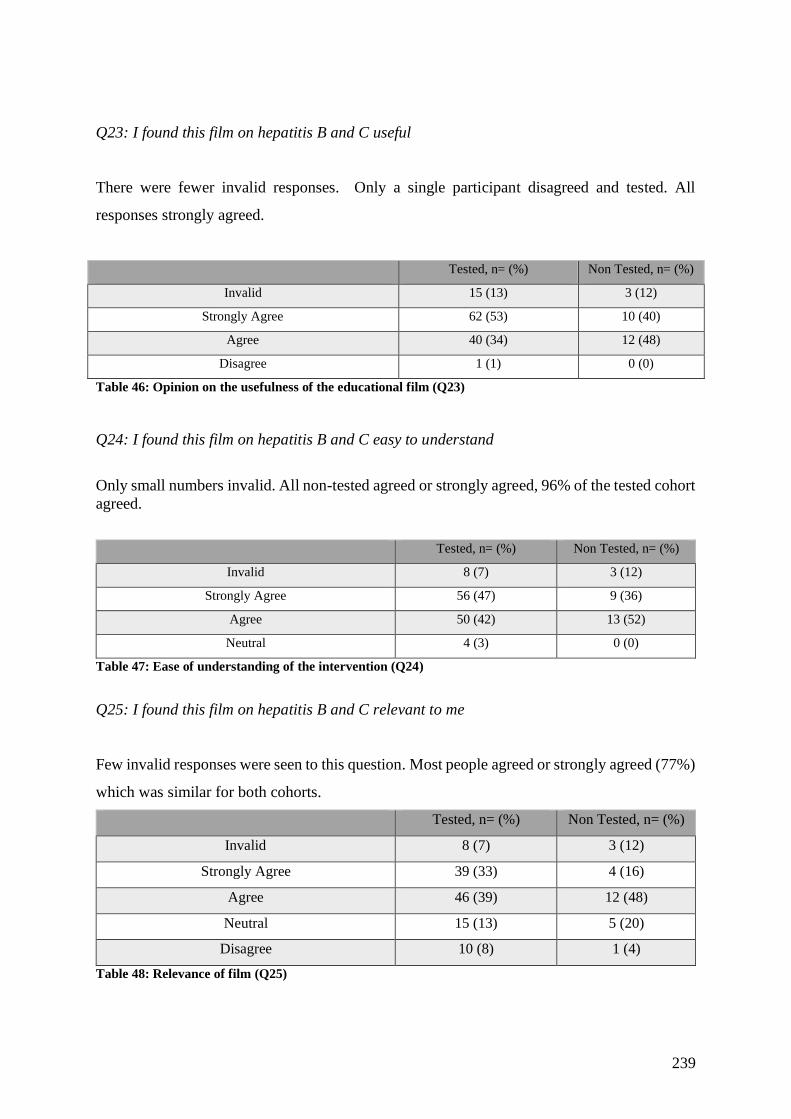
239
Q23: I found this film on hepatitis B and C useful
There were fewer invalid responses. Only a single participant disagreed and tested. All
responses strongly agreed.
Tested, n= (%) Non Tested, n= (%)
Invalid 15 (13) 3 (12)
Strongly Agree 62 (53) 10 (40)
Agree 40 (34) 12 (48)
Disagree 1 (1) 0 (0)
Table 46: Opinion on the usefulness of the educational film (Q23)
Q24: I found this film on hepatitis B and C easy to understand
Only small numbers invalid. All non-tested agreed or strongly agreed, 96% of the tested cohort
agreed.
Tested, n= (%) Non Tested, n= (%)
Invalid 8 (7) 3 (12)
Strongly Agree 56 (47) 9 (36)
Agree 50 (42) 13 (52)
Neutral 4 (3) 0 (0)
Table 47: Ease of understanding of the intervention (Q24)
Q25: I found this film on hepatitis B and C relevant to me
Few invalid responses were seen to this question. Most people agreed or strongly agreed (77%)
which was similar for both cohorts.
Tested, n= (%) Non Tested, n= (%)
Invalid 8 (7) 3 (12)
Strongly Agree 39 (33) 4 (16)
Agree 46 (39) 12 (48)
Neutral 15 (13) 5 (20)
Disagree 10 (8) 1 (4)
Table 48: Relevance of film (Q25)
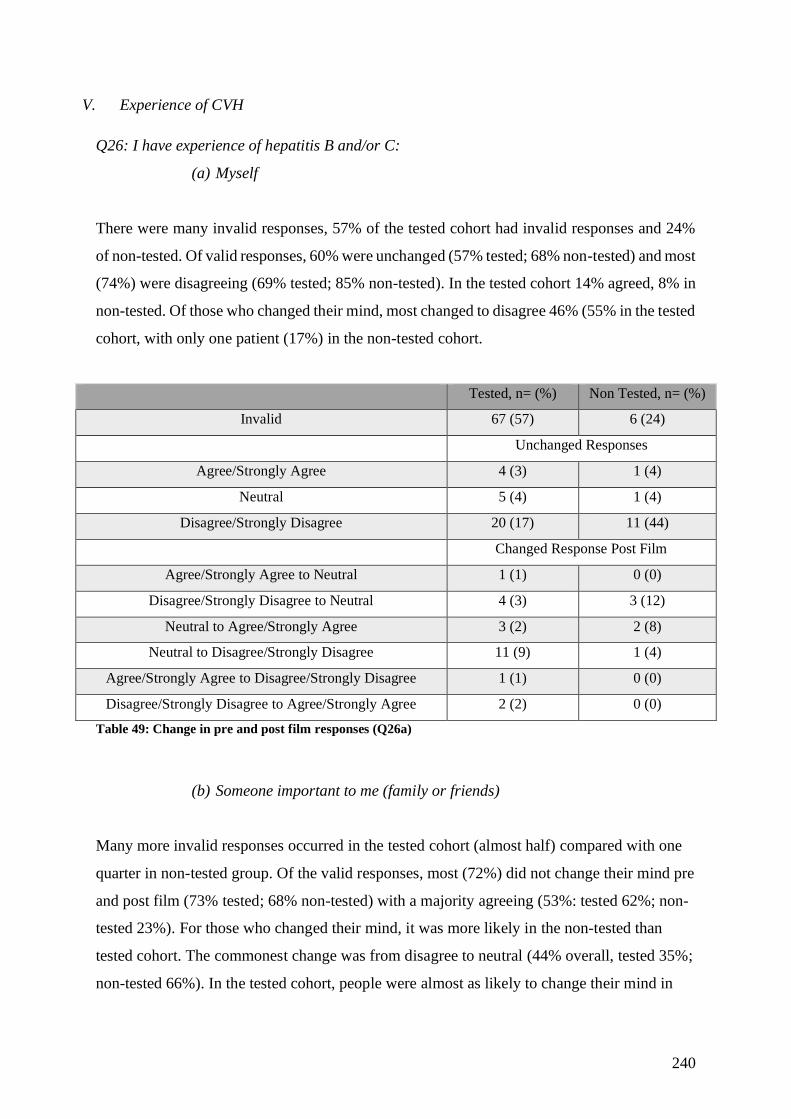
240
V. Experience of CVH
Q26: I have experience of hepatitis B and/or C:
(a) Myself
There were many invalid responses, 57% of the tested cohort had invalid responses and 24%
of non-tested. Of valid responses, 60% were unchanged (57% tested; 68% non-tested) and most
(74%) were disagreeing (69% tested; 85% non-tested). In the tested cohort 14% agreed, 8% in
non-tested. Of those who changed their mind, most changed to disagree 46% (55% in the tested
cohort, with only one patient (17%) in the non-tested cohort.
Tested, n= (%) Non Tested, n= (%)
Invalid 67 (57) 6 (24)
Unchanged Responses
Agree/Strongly Agree 4 (3) 1 (4)
Neutral 5 (4) 1 (4)
Disagree/Strongly Disagree 20 (17) 11 (44)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree to Neutral 4 (3) 3 (12)
Neutral to Agree/Strongly Agree 3 (2) 2 (8)
Neutral to Disagree/Strongly Disagree 11 (9) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 1 (1) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 2 (2) 0 (0)
Table 49: Change in pre and post film responses (Q26a)
(b) Someone important to me (family or friends)
Many more invalid responses occurred in the tested cohort (almost half) compared with one
quarter in non-tested group. Of the valid responses, most (72%) did not change their mind pre
and post film (73% tested; 68% non-tested) with a majority agreeing (53%: tested 62%; non-
tested 23%). For those who changed their mind, it was more likely in the non-tested than
tested cohort. The commonest change was from disagree to neutral (44% overall, tested 35%;
non-tested 66%). In the tested cohort, people were almost as likely to change their mind in
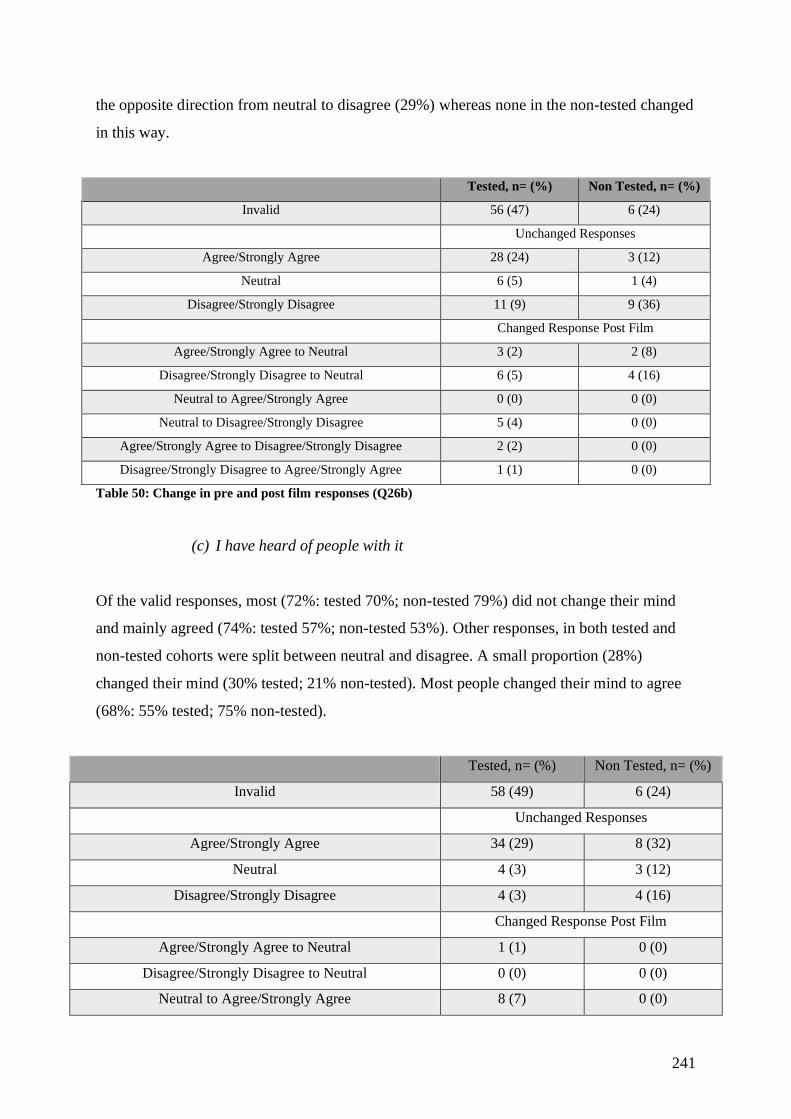
241
the opposite direction from neutral to disagree (29%) whereas none in the non-tested changed
in this way.
Tested, n= (%) Non Tested, n= (%)
Invalid 56 (47) 6 (24)
Unchanged Responses
Agree/Strongly Agree 28 (24) 3 (12)
Neutral 6 (5) 1 (4)
Disagree/Strongly Disagree 11 (9) 9 (36)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (2) 2 (8)
Disagree/Strongly Disagree to Neutral 6 (5) 4 (16)
Neutral to Agree/Strongly Agree 0 (0) 0 (0)
Neutral to Disagree/Strongly Disagree 5 (4) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 2 (2) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 1 (1) 0 (0)
Table 50: Change in pre and post film responses (Q26b)
(c) I have heard of people with it
Of the valid responses, most (72%: tested 70%; non-tested 79%) did not change their mind
and mainly agreed (74%: tested 57%; non-tested 53%). Other responses, in both tested and
non-tested cohorts were split between neutral and disagree. A small proportion (28%)
changed their mind (30% tested; 21% non-tested). Most people changed their mind to agree
(68%: 55% tested; 75% non-tested).
Tested, n= (%) Non Tested, n= (%)
Invalid 58 (49) 6 (24)
Unchanged Responses
Agree/Strongly Agree 34 (29) 8 (32)
Neutral 4 (3) 3 (12)
Disagree/Strongly Disagree 4 (3) 4 (16)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 0 (0)
Neutral to Agree/Strongly Agree 8 (7) 0 (0)
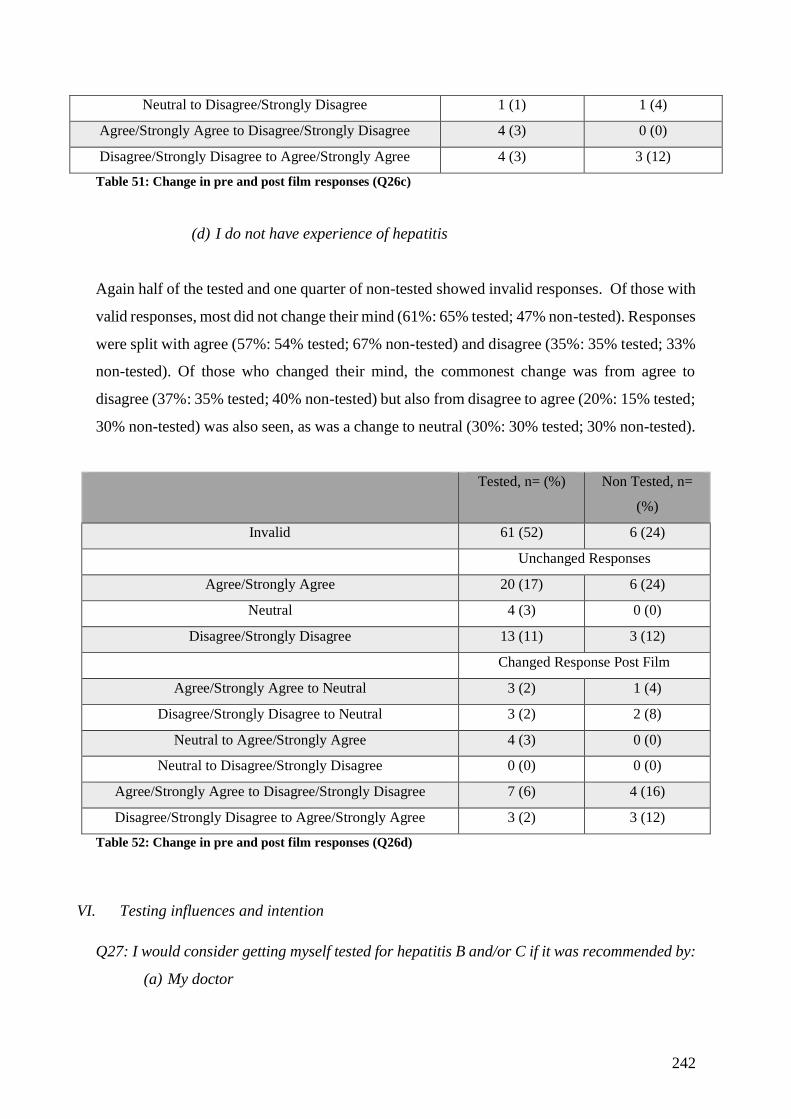
242
Neutral to Disagree/Strongly Disagree 1 (1) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 4 (3) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 3 (12)
Table 51: Change in pre and post film responses (Q26c)
(d) I do not have experience of hepatitis
Again half of the tested and one quarter of non-tested showed invalid responses. Of those with
valid responses, most did not change their mind (61%: 65% tested; 47% non-tested). Responses
were split with agree (57%: 54% tested; 67% non-tested) and disagree (35%: 35% tested; 33%
non-tested). Of those who changed their mind, the commonest change was from agree to
disagree (37%: 35% tested; 40% non-tested) but also from disagree to agree (20%: 15% tested;
30% non-tested) was also seen, as was a change to neutral (30%: 30% tested; 30% non-tested).
Tested, n= (%) Non Tested, n=
(%)
Invalid 61 (52) 6 (24)
Unchanged Responses
Agree/Strongly Agree 20 (17) 6 (24)
Neutral 4 (3) 0 (0)
Disagree/Strongly Disagree 13 (11) 3 (12)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (2) 1 (4)
Disagree/Strongly Disagree to Neutral 3 (2) 2 (8)
Neutral to Agree/Strongly Agree 4 (3) 0 (0)
Neutral to Disagree/Strongly Disagree 0 (0) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 7 (6) 4 (16)
Disagree/Strongly Disagree to Agree/Strongly Agree 3 (2) 3 (12)
Table 52: Change in pre and post film responses (Q26d)
VI. Testing influences and intention
Q27: I would consider getting myself tested for hepatitis B and/or C if it was recommended by:
(a) My doctor
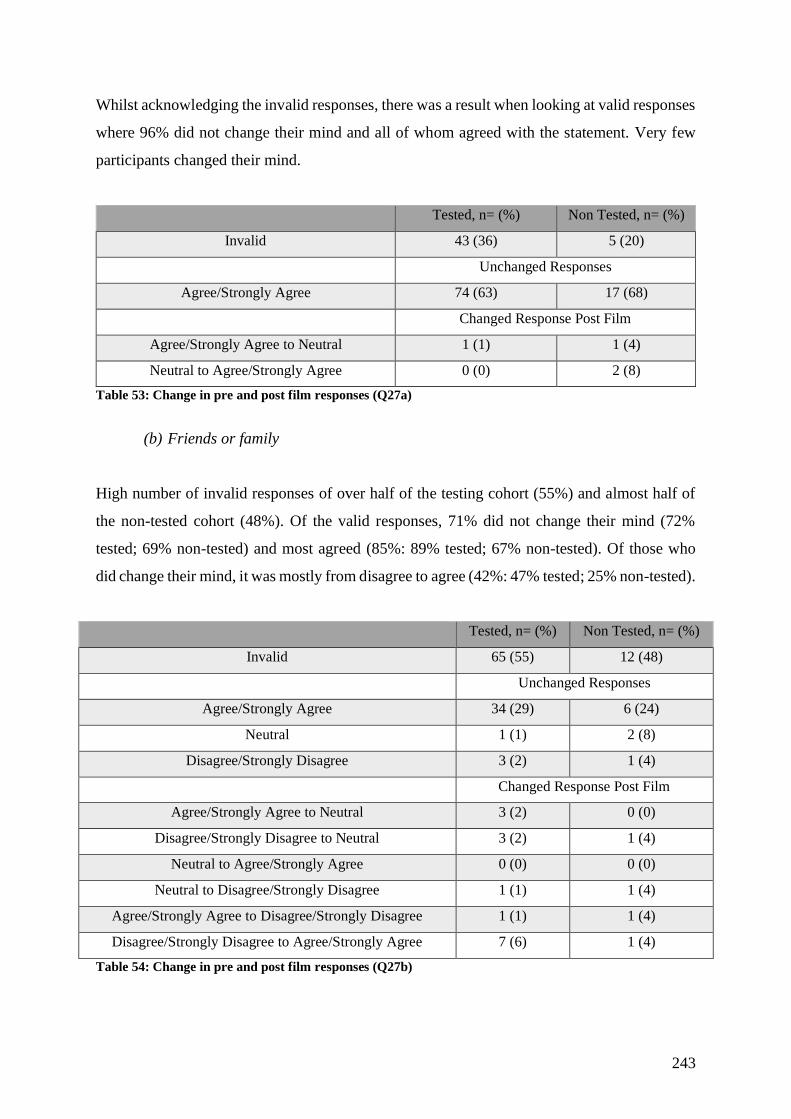
243
Whilst acknowledging the invalid responses, there was a result when looking at valid responses
where 96% did not change their mind and all of whom agreed with the statement. Very few
participants changed their mind.
Tested, n= (%) Non Tested, n= (%)
Invalid 43 (36) 5 (20)
Unchanged Responses
Agree/Strongly Agree 74 (63) 17 (68)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 1 (4)
Neutral to Agree/Strongly Agree 0 (0) 2 (8)
Table 53: Change in pre and post film responses (Q27a)
(b) Friends or family
High number of invalid responses of over half of the testing cohort (55%) and almost half of
the non-tested cohort (48%). Of the valid responses, 71% did not change their mind (72%
tested; 69% non-tested) and most agreed (85%: 89% tested; 67% non-tested). Of those who
did change their mind, it was mostly from disagree to agree (42%: 47% tested; 25% non-tested).
Tested, n= (%) Non Tested, n= (%)
Invalid 65 (55) 12 (48)
Unchanged Responses
Agree/Strongly Agree 34 (29) 6 (24)
Neutral 1 (1) 2 (8)
Disagree/Strongly Disagree 3 (2) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 3 (2) 1 (4)
Neutral to Agree/Strongly Agree 0 (0) 0 (0)
Neutral to Disagree/Strongly Disagree 1 (1) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 1 (1) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 7 (6) 1 (4)
Table 54: Change in pre and post film responses (Q27b)
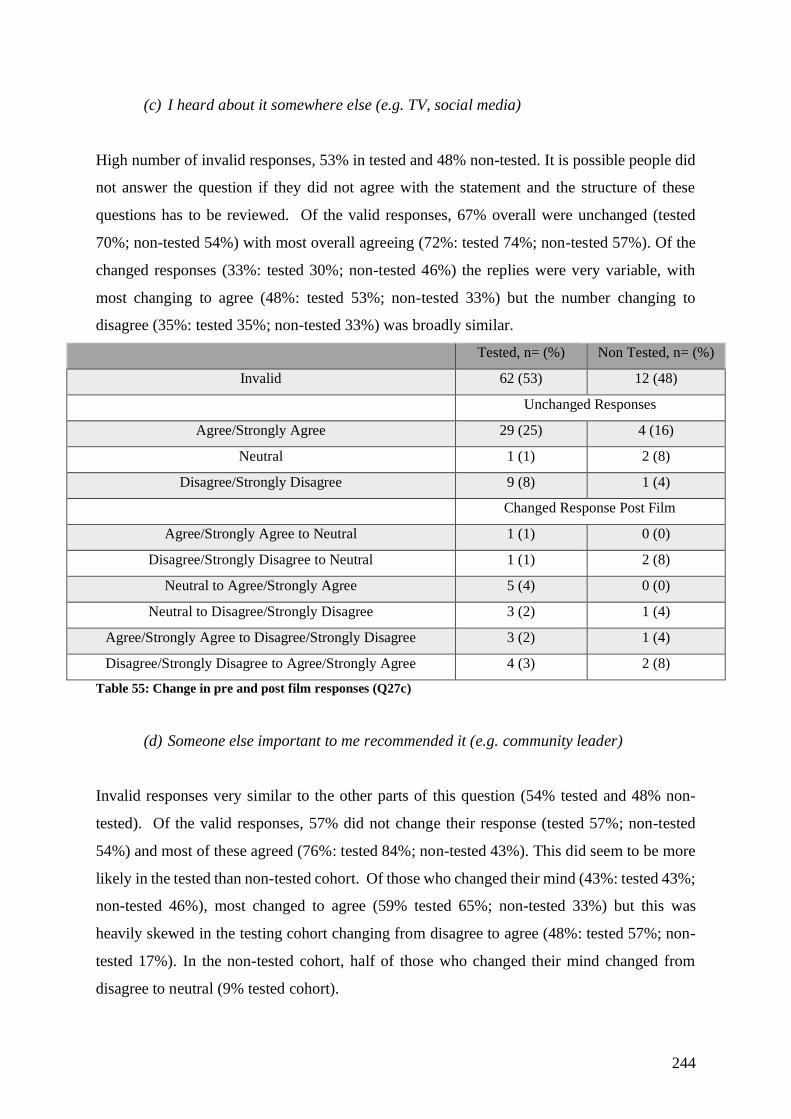
244
(c) I heard about it somewhere else (e.g. TV, social media)
High number of invalid responses, 53% in tested and 48% non-tested. It is possible people did
not answer the question if they did not agree with the statement and the structure of these
questions has to be reviewed. Of the valid responses, 67% overall were unchanged (tested
70%; non-tested 54%) with most overall agreeing (72%: tested 74%; non-tested 57%). Of the
changed responses (33%: tested 30%; non-tested 46%) the replies were very variable, with
most changing to agree (48%: tested 53%; non-tested 33%) but the number changing to
disagree (35%: tested 35%; non-tested 33%) was broadly similar.
Tested, n= (%) Non Tested, n= (%)
Invalid 62 (53) 12 (48)
Unchanged Responses
Agree/Strongly Agree 29 (25) 4 (16)
Neutral 1 (1) 2 (8)
Disagree/Strongly Disagree 9 (8) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 1 (1) 0 (0)
Disagree/Strongly Disagree to Neutral 1 (1) 2 (8)
Neutral to Agree/Strongly Agree 5 (4) 0 (0)
Neutral to Disagree/Strongly Disagree 3 (2) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 3 (2) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 2 (8)
Table 55: Change in pre and post film responses (Q27c)
(d) Someone else important to me recommended it (e.g. community leader)
Invalid responses very similar to the other parts of this question (54% tested and 48% non-
tested). Of the valid responses, 57% did not change their response (tested 57%; non-tested
54%) and most of these agreed (76%: tested 84%; non-tested 43%). This did seem to be more
likely in the tested than non-tested cohort. Of those who changed their mind (43%: tested 43%;
non-tested 46%), most changed to agree (59% tested 65%; non-tested 33%) but this was
heavily skewed in the testing cohort changing from disagree to agree (48%: tested 57%; non-
tested 17%). In the non-tested cohort, half of those who changed their mind changed from
disagree to neutral (9% tested cohort).
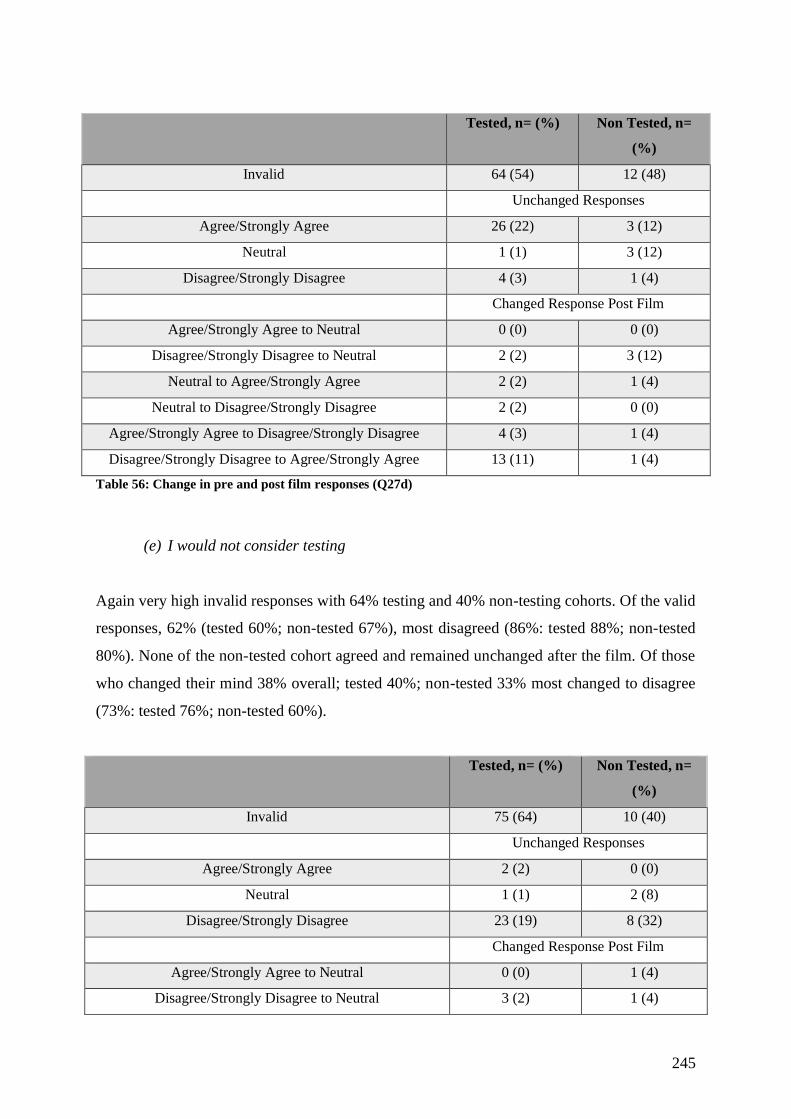
245
Tested, n= (%) Non Tested, n=
(%)
Invalid 64 (54) 12 (48)
Unchanged Responses
Agree/Strongly Agree 26 (22) 3 (12)
Neutral 1 (1) 3 (12)
Disagree/Strongly Disagree 4 (3) 1 (4)
Changed Response Post Film
Agree/Strongly Agree to Neutral 0 (0) 0 (0)
Disagree/Strongly Disagree to Neutral 2 (2) 3 (12)
Neutral to Agree/Strongly Agree 2 (2) 1 (4)
Neutral to Disagree/Strongly Disagree 2 (2) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 4 (3) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 13 (11) 1 (4)
Table 56: Change in pre and post film responses (Q27d)
(e) I would not consider testing
Again very high invalid responses with 64% testing and 40% non-testing cohorts. Of the valid
responses, 62% (tested 60%; non-tested 67%), most disagreed (86%: tested 88%; non-tested
80%). None of the non-tested cohort agreed and remained unchanged after the film. Of those
who changed their mind 38% overall; tested 40%; non-tested 33% most changed to disagree
(73%: tested 76%; non-tested 60%).
Tested, n= (%) Non Tested, n=
(%)
Invalid 75 (64) 10 (40)
Unchanged Responses
Agree/Strongly Agree 2 (2) 0 (0)
Neutral 1 (1) 2 (8)
Disagree/Strongly Disagree 23 (19) 8 (32)
Changed Response Post Film
Agree/Strongly Agree to Neutral 0 (0) 1 (4)
Disagree/Strongly Disagree to Neutral 3 (2) 1 (4)
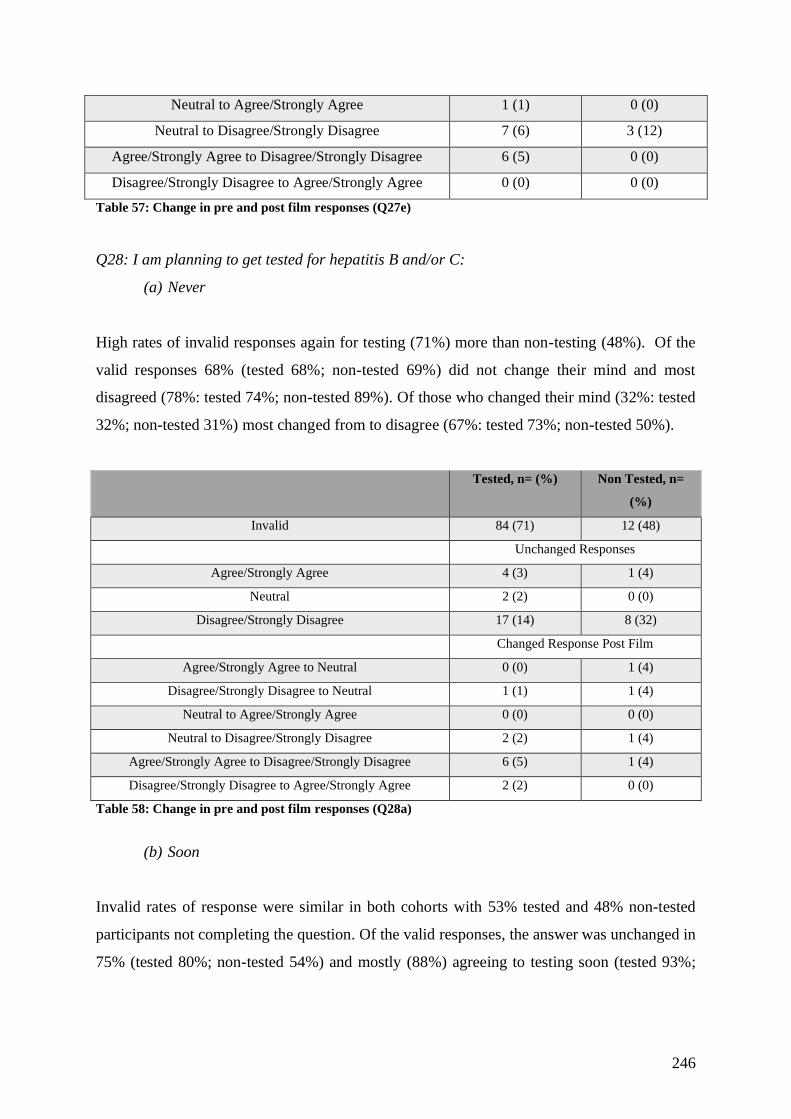
246
Neutral to Agree/Strongly Agree 1 (1) 0 (0)
Neutral to Disagree/Strongly Disagree 7 (6) 3 (12)
Agree/Strongly Agree to Disagree/Strongly Disagree 6 (5) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 0 (0) 0 (0)
Table 57: Change in pre and post film responses (Q27e)
Q28: I am planning to get tested for hepatitis B and/or C:
(a) Never
High rates of invalid responses again for testing (71%) more than non-testing (48%). Of the
valid responses 68% (tested 68%; non-tested 69%) did not change their mind and most
disagreed (78%: tested 74%; non-tested 89%). Of those who changed their mind (32%: tested
32%; non-tested 31%) most changed from to disagree (67%: tested 73%; non-tested 50%).
Tested, n= (%) Non Tested, n=
(%)
Invalid 84 (71) 12 (48)
Unchanged Responses
Agree/Strongly Agree 4 (3) 1 (4)
Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree 17 (14) 8 (32)
Changed Response Post Film
Agree/Strongly Agree to Neutral 0 (0) 1 (4)
Disagree/Strongly Disagree to Neutral 1 (1) 1 (4)
Neutral to Agree/Strongly Agree 0 (0) 0 (0)
Neutral to Disagree/Strongly Disagree 2 (2) 1 (4)
Agree/Strongly Agree to Disagree/Strongly Disagree 6 (5) 1 (4)
Disagree/Strongly Disagree to Agree/Strongly Agree 2 (2) 0 (0)
Table 58: Change in pre and post film responses (Q28a)
(b) Soon
Invalid rates of response were similar in both cohorts with 53% tested and 48% non-tested
participants not completing the question. Of the valid responses, the answer was unchanged in
75% (tested 80%; non-tested 54%) and mostly (88%) agreeing to testing soon (tested 93%;

247
non-tested 57%). Of those who changed their mind, most changed to agree (59%: tested 55%;
non-tested 67%).
Tested, n= (%) Non Tested, n=
(%)
Invalid 63 (53) 12 (48)
Unchanged Responses
Agree/Strongly Agree 41 (35) 4 (16)
Neutral 1 (1) 1 (4)
Disagree/Strongly Disagree 2 (2) 2 (8)
Changed Response Post Film
Agree/Strongly Agree to Neutral 0 (0) 0 (0)
Disagree/Strongly Disagree to Neutral 1 (1) 2 (8)
Neutral to Agree/Strongly Agree 3 (2) 0 (0)
Neutral to Disagree/Strongly Disagree 1 (1) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 3 (2) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 3 (2) 4 (16)
Table 59: Change in pre and post film responses (Q28b)
(c) Within the next year
There were many more invalid responses in the tested cohort (70%) than tested non-tested
(52%). Of the valid tests, those whose replies were unchanged (45%: tested 49%; non-tested
33%) there was a spread of answers with the most common overall disagree (48%: tested 47%;
non-tested 50%) with neutral (24%: tested 17%; non-tested 50%) and agree (29%: tested 35%;
non-tested 0%) similar but no non-tested agreed. Of those who changed their mind, most
changed to agree (46%: tested 39%; non-tested 62%). I believe there were issues understanding
this question and this making interpretation of the results challenging.
Tested, n= (%) Non Tested, n=
(%)
Invalid 83 (70) 13 (52)
Unchanged Responses
Agree/Strongly Agree 6 (5) 0 (0)
Neutral 3 (2) 2 (8)
Disagree/Strongly Disagree 8 (7) 2 (8)
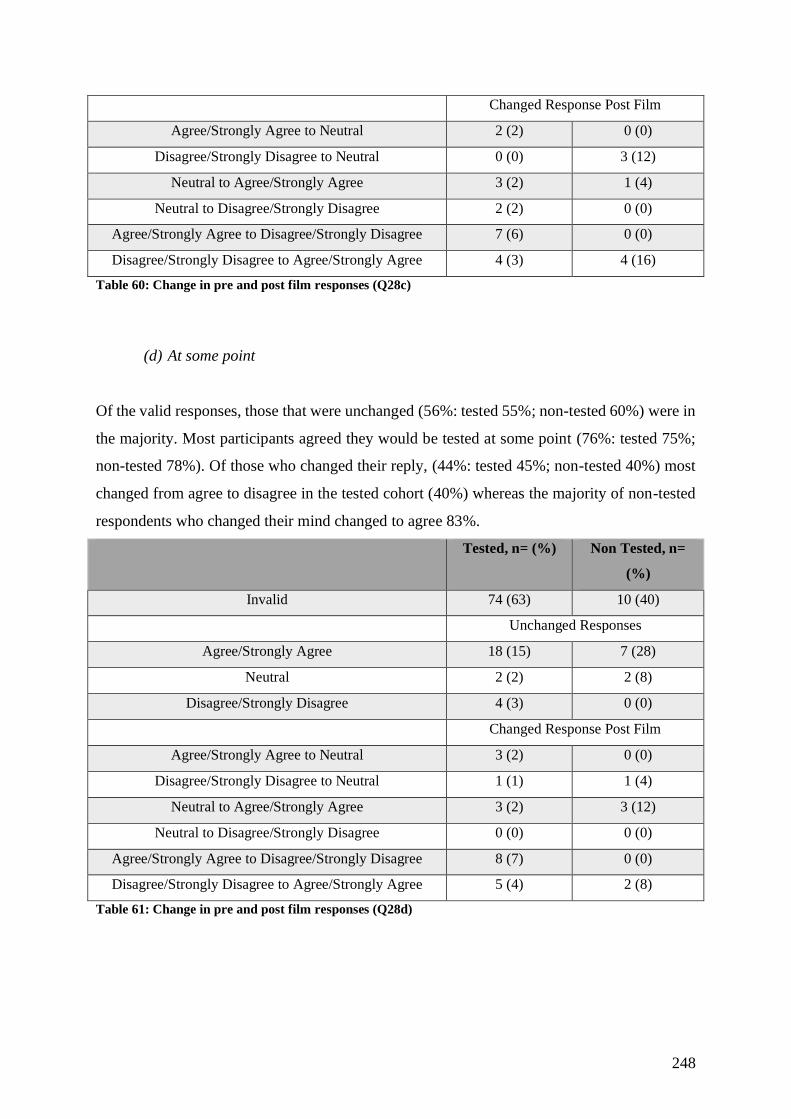
248
Changed Response Post Film
Agree/Strongly Agree to Neutral 2 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 0 (0) 3 (12)
Neutral to Agree/Strongly Agree 3 (2) 1 (4)
Neutral to Disagree/Strongly Disagree 2 (2) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 7 (6) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 4 (3) 4 (16)
Table 60: Change in pre and post film responses (Q28c)
(d) At some point
Of the valid responses, those that were unchanged (56%: tested 55%; non-tested 60%) were in
the majority. Most participants agreed they would be tested at some point (76%: tested 75%;
non-tested 78%). Of those who changed their reply, (44%: tested 45%; non-tested 40%) most
changed from agree to disagree in the tested cohort (40%) whereas the majority of non-tested
respondents who changed their mind changed to agree 83%.
Tested, n= (%) Non Tested, n=
(%)
Invalid 74 (63) 10 (40)
Unchanged Responses
Agree/Strongly Agree 18 (15) 7 (28)
Neutral 2 (2) 2 (8)
Disagree/Strongly Disagree 4 (3) 0 (0)
Changed Response Post Film
Agree/Strongly Agree to Neutral 3 (2) 0 (0)
Disagree/Strongly Disagree to Neutral 1 (1) 1 (4)
Neutral to Agree/Strongly Agree 3 (2) 3 (12)
Neutral to Disagree/Strongly Disagree 0 (0) 0 (0)
Agree/Strongly Agree to Disagree/Strongly Disagree 8 (7) 0 (0)
Disagree/Strongly Disagree to Agree/Strongly Agree 5 (4) 2 (8)
Table 61: Change in pre and post film responses (Q28d)
Related Documents











