Development of a ≤ 30 week EGA Golden Hour Guideline Stephen Kicklighter MD 1 , Susan Gutierrez RN, Tara Bastek MD, Jonathan Seigel, MD, Melissa Johnson PhD, James Helm, PhD, and the NICU VO Golden Hour Group WakeMed Health and Hospitals, Raleigh, North Carolina U.S.A. 1 3000 New Bern Avenue, Neonatology-3 rd Floor Main Hospital, Raleigh, NC 27610; 919-350-5585 (office); [email protected] Keywords: Golden Hour, VLBW, Delayed Cord Clamping, Chlorhexidine, Starter TPN, Starter Lipids Background: WakeMed Health & Hospitals in Raleigh, NC, is a tertiary center caring for all aspects of premature infants except for those with congenital heart disease or those requiring ECMO therapy. We 127 infants below 1500g birthweight and 89 infants ≤ 30 weeks of gestation in 2014. Through our participation in the Vermont Oxford Network (VON) we became aware that we did not have a ‘roadmap’ outlining the potentially better practices (PBP) for the ≤ 30 week infant to guide the admission process and care of the infant during the the steps of first hour of life. Through the development of this golden hour guideline, we could standardize our care by: 1) eliminating burns secondary to chlorhexidine use for central line placement 2) standardizing delayed cord clamping in the ≤ 34 week premature infant 3) placing central lines (as needed) and use of UVC in all infants <1500g birthweight 4) using Starter TPN and scavenged Starter IL to improve caloric and protein/fat delivery on DOL0 5) maintaining normothermia and euglycemia 6) updating the family in a timely manner. Aim: Smart Aim Our smart aim was to develop and implement/modify a consistent, evidence based guideline for the delivery, resuscitation, stabilization, and admission of the ≤ 30 week EGA infant (Golden Hour, GH) that supports the infant, family, and staff at WakeMed. Implementation and modification would coincide with the participation in the Micropreemie Homeroom in NICQNext and be completed by May of 2015. Sub-Aims 1. By March of 2014, we will reduce our incidence of skin burns from 6.4%, 3.2%, and 13% of VLBW infants in 2011, 2012, and 2013, respectively to 0% as a result of ChloraPrep (2% chlorhexidine gluconate in 70% ispropyl alcohol) using and changing to povidone-iodine as the antiseptic for umbilical central line placement. 2. By September 2014, we will develope a GH Guideline for use as a guide and data collection tool for the ≤ 30 week EGA Infant. Modification will continue through the timeframe of participation in NICQNext’s Micropreemie Homeroom. As part of this initiative, we plan to implement the following initial changes: a. Expand the use of the polyethylene body wrap to be used in all infants ≤ 30 week EGA at birth b. Standardize delayed cord clamping to 60 seconds for any infant ≤34 weeks of gestation c. For infants below 1500 grams birthweight: i. Initiate Lipids (IL) on DOL0 in infants at 0.5 g/kg/d ii. Place a double lumen UVC as initial line management with goal placement within 30 minutes of admission d. Update parents by the end of the first hour of life of their infant.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Development of a ≤ 30 week EGA Golden Hour Guideline
Stephen Kicklighter MD1, Susan Gutierrez RN, Tara Bastek MD, Jonathan Seigel, MD, Melissa Johnson PhD, James Helm, PhD, and the NICU VO Golden Hour Group
WakeMed Health and Hospitals, Raleigh, North Carolina U.S.A.
13000 New Bern Avenue, Neonatology-3rd Floor Main Hospital, Raleigh, NC 27610; 919-350-5585 (office); [email protected]
Keywords: Golden Hour, VLBW, Delayed Cord Clamping, Chlorhexidine, Starter TPN, Starter Lipids
Background:
WakeMed Health & Hospitals in Raleigh, NC, is a tertiary center caring for all aspects of premature infants except for those with congenital heart disease or those requiring ECMO therapy. We 127 infants below 1500g birthweight and 89 infants ≤ 30 weeks of gestation in 2014. Through our participation in the Vermont Oxford Network (VON) we became aware that we did not have a ‘roadmap’ outlining the potentially better practices (PBP) for the ≤ 30 week infant to guide the admission process and care of the infant during the the steps of first hour of life. Through the development of this golden hour guideline, we could standardize our care by: 1) eliminating burns secondary to chlorhexidine use for central line placement 2) standardizing delayed cord clamping in the ≤ 34 week premature infant 3) placing central lines (as needed) and use of UVC in all infants <1500g birthweight 4) using Starter TPN and scavenged Starter IL to improve caloric and protein/fat delivery on DOL0 5) maintaining normothermia and euglycemia 6) updating the family in a timely manner.
Aim:
Smart Aim
Our smart aim was to develop and implement/modify a consistent, evidence based guideline for the delivery,
resuscitation, stabilization, and admission of the ≤ 30 week EGA infant (Golden Hour, GH) that supports the
infant, family, and staff at WakeMed. Implementation and modification would coincide with the participation in
the Micropreemie Homeroom in NICQNext and be completed by May of 2015.
Sub-Aims
1. By March of 2014, we will reduce our incidence of skin burns from 6.4%, 3.2%, and 13% of VLBW infants in
2011, 2012, and 2013, respectively to 0% as a result of ChloraPrep (2% chlorhexidine gluconate in 70%
ispropyl alcohol) using and changing to povidone-iodine as the antiseptic for umbilical central line
placement.
2. By September 2014, we will develope a GH Guideline for use as a guide and data collection tool for the ≤ 30
week EGA Infant. Modification will continue through the timeframe of participation in NICQNext’s
Micropreemie Homeroom. As part of this initiative, we plan to implement the following initial changes:
a. Expand the use of the polyethylene body wrap to be used in all infants ≤ 30 week EGA at birth b. Standardize delayed cord clamping to 60 seconds for any infant ≤34 weeks of gestation c. For infants below 1500 grams birthweight:
i. Initiate Lipids (IL) on DOL0 in infants at 0.5 g/kg/d ii. Place a double lumen UVC as initial line management with goal placement within 30
minutes of admission
d. Update parents by the end of the first hour of life of their infant.

Setting:
WakeMed’s Neonatal Intensive Care Unit (NICU) is a 48-bed unit with 24 single family rooms and 24 beds in a pinwheel
configuration. We are a level III-B unit as designated by VON. Our Hospital has roughly 5200 deliveries, 650 NICU
admissions. We admitted 127 VLBW infants and 50 ELBW infants in 2014. 87% of our VLBW infant admissions for 2014
were inborn. We have an active transport team and utilize mutual aid through two nearby institutions (University of
North Carolina-Chapel Hill and Duke University Medical Center). We have 3 Pediatric Surgeons on staff, who provide
surgical management of common neonatal surgerical conditions including: TEF, inguinal hernia, PDA ligation, NEC
surgery, bowel obstruction, gastroschisis and omphalocele repair, etc. Other subspecialist services available include:
Pediatric Neurology, Pediatric Endocrinology, Pediatric Cardiology and Pediatric Hematology-Oncology.
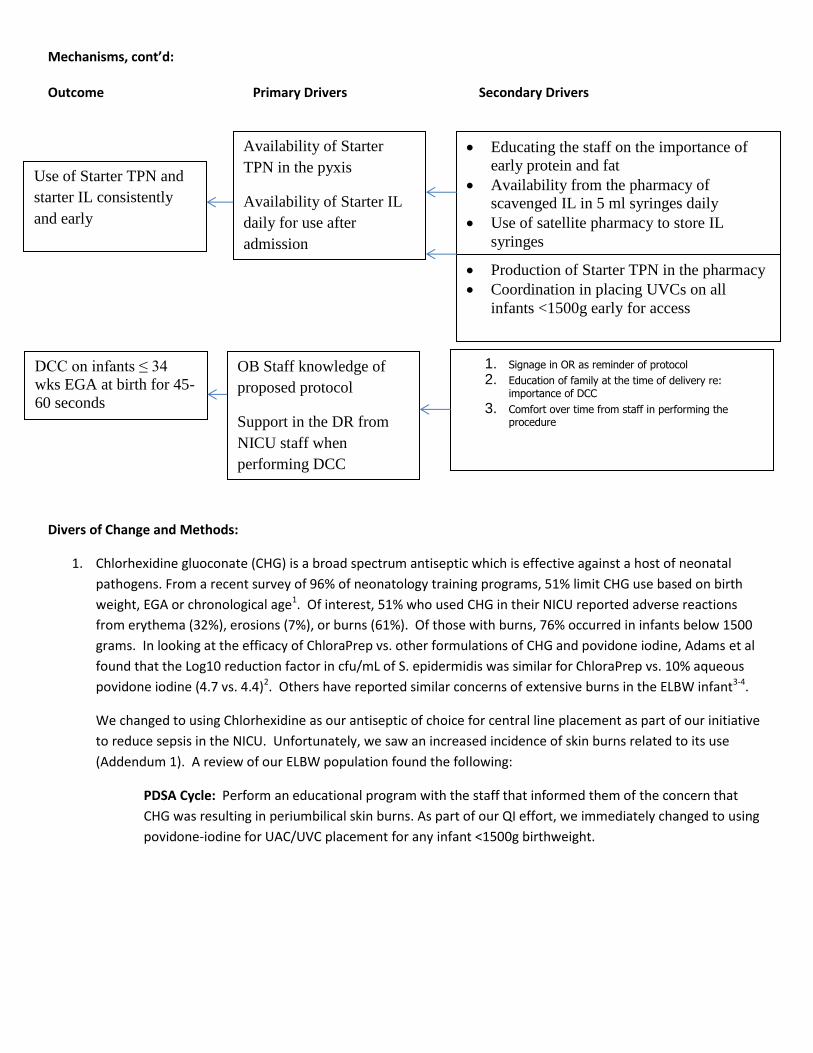
Mechanisms: Components of our Golden Hour Guideline A: Eliminating abdominal burns associated with the use of CHG Historically, we had used betadine as an antiseptic in the placement of umbilical central lines on DOL0 as well as for the placement of PICC lines at a later PCA. As part of our infection control bundle in 2010, we instituted the use of CHG as the primary antiseptic in both of these circumstances. Since that time, we noted significant burns to the abdomen on DOL0 in 9% of our ELBW infants (11 out of 122) between 1/2011 and 1/2014 that was felt to be directly related to the use of CHG. Some were very significant clinically as noted in Addendum 1. Exposure to CHG was identified as the primary driver. Secondary drivers included availability of Betadine in the bedside Central Line kits, staff education, and observation for burns after central line placement. B: Use of a Polyethylene drape in the DR Our unit has used the polyethylene drape in the DR for many years; however, in development of our GH bundle, we hoped to increase its use to encompass any infant ≤ 30 weeks EGA. Our data suggested that our incidence of having a ‘normothermic’ VLBW infant (admission temp of 36.5-37.5C) was 60% which was below the Q3 for VON of 66.7%. As part of our GH guideline, we wanted to expand its use to all infants who qualify for that data collection which is any infant ≤ 30 weeks and inborn at WakeMed. The primary drivers are the availability of the polyethylene bag as well as consistent staff knowledge, education, timely review and consistent technique in the use of the polyethylene bag in this patient population. C: UVC placement in infants who are VLBW to obtain access w/in one hour of birth and initiation of Starter TPN/Starter IL Commonly, our infants have PIV’s placed as the primary mode of IV access unless they are either: extremely premature (<28 weeks) or we were unable to obtain IV access. Some concerns that our group had were: IVF initiation may be delayed through inability to acquire IV access and focusing on fully admitting the infant before a line is placed, inconsistency within our group as to who should have an IV placed vs a UVC, and a delay of IVF initiation through a central line pending CXR confirmation of accurate UVC line placement. In developing our GH guideline, we decided to initiate placement of a UVC on any infant ≤ 30 weeks as the primary venous line, and initiate fluids (Starter TPN) as soon as the line is placed as long as there is good blood return. Drivers for this implementation were availability of the UVC trays at the bedside on admission, teamwork between two NNP’s with their availability such that one could facilitate the admission while the other placed the line, staff education on the importance of secure IV access soon after admission, and change in mindset of initial nursing admission procedures to the mindset of IV line placement and initiation of dextrose and protein. Drivers for early initiation of Starter TPN/IL include availability of starter TPN in the pyxis within the NICU, availability of starter lipids to ‘scavenge’ after the daily TPNs are made, and staff education. D: Delayed cord clamping on infants ≤ 34 weeks EGA at birth Our unit had instituted DCC in 2010; however, there was no consistency regarding the gestation age below which it was performed and for how long. As part of our GH guideline, our team reviewed the literature and suggested that all infants ≤ 34 weeks EGA at birth should have DCC for 45 seconds to 1 minute unless the OB felt that there was a

contraindication (i.e. placental abruption, severe fetal distress). Drivers include OB staff education and knowledge of the process, development of signage for the ORs as a reminder, and NICU staff knowledge to request on any infant meeting the guideline. Outcome Primary Drivers Secondary Drivers
Eliminate burns
related to the placement
of UAC/UVCs on DOL0
Betadine use for aseptic
technique in Central
Line placement in the
VLBW infant on DOL0
Availability of Betadine in the bedside
Central Line kits
Staff education on the concern of using
CHG in the premature infant
Observation for burns after central line
placement
Use of Polyethylene drape
on any infant ≤ 30 week
gestation in the DR as a
mode to prevent heat loss
on admission
Staff education on the importance of use
of the polyethylene bag
Timely review process
Consistent technique in the DR on using
the polyethylene bag (i.e. placement under
the infant and wrapping over them)
Availability of the
polyethylene bag
Consistent staff
knowledge
UVC placement in infants
<1500g birthweight as IV
access within 1 hour of
birth
Availability of UVC
trays at the bedside on
admission
Teamwork/2 NNP
availability – one to
facilitate admission
orders and the other to
immediately place line
access
Staff education on the importance of
secure IV access early
Change in mindset of initial nursing
admission procedures to knowing the
importance of establishing early access to
aid in preventing hypoglycemia and
supporting initiation of Starter TPN
Materials for securing and comforting
infant during line placement
Educating the family about the
importance of early line placement
Mechanisms, cont’d: Outcome Primary Drivers Secondary Drivers
Divers of Change and Methods:
1. Chlorhexidine gluoconate (CHG) is a broad spectrum antiseptic which is effective against a host of neonatal
pathogens. From a recent survey of 96% of neonatology training programs, 51% limit CHG use based on birth
weight, EGA or chronological age1. Of interest, 51% who used CHG in their NICU reported adverse reactions
from erythema (32%), erosions (7%), or burns (61%). Of those with burns, 76% occurred in infants below 1500
grams. In looking at the efficacy of ChloraPrep vs. other formulations of CHG and povidone iodine, Adams et al
found that the Log10 reduction factor in cfu/mL of S. epidermidis was similar for ChloraPrep vs. 10% aqueous
povidone iodine (4.7 vs. 4.4)2. Others have reported similar concerns of extensive burns in the ELBW infant3-4.
We changed to using Chlorhexidine as our antiseptic of choice for central line placement as part of our initiative
to reduce sepsis in the NICU. Unfortunately, we saw an increased incidence of skin burns related to its use
(Addendum 1). A review of our ELBW population found the following:
PDSA Cycle: Perform an educational program with the staff that informed them of the concern that
CHG was resulting in periumbilical skin burns. As part of our QI effort, we immediately changed to using
povidone-iodine for UAC/UVC placement for any infant <1500g birthweight.
Use of Starter TPN and
starter IL consistently
and early
Availability of Starter
TPN in the pyxis
Availability of Starter IL
daily for use after
admission
Educating the staff on the importance of
early protein and fat
Availability from the pharmacy of
scavenged IL in 5 ml syringes daily
Use of satellite pharmacy to store IL
syringes
Production of Starter TPN in the pharmacy
Coordination in placing UVCs on all
infants <1500g early for access
DCC on infants ≤ 34
wks EGA at birth for 45-
60 seconds
OB Staff knowledge of
proposed protocol
Support in the DR from
NICU staff when
performing DCC
1. Signage in OR as reminder of protocol
2. Education of family at the time of delivery re: importance of DCC
3. Comfort over time from staff in performing the procedure
2. The use of a polyethylene body wrap in infants below 27 weeks EGA was initially published by Vohra,
et al in 1995 and repeated in a multicenter trial with VON6. We, at WakeMed, have been using the
polyethylene bag for those infants below 27 weeks gestation since 2001. As part of our VLBW
initiative, and to make its use more consistent, we extended the use of polyethylene bag covering to any
infant ≤ 30 weeks.
PDSA Cycle: As part of this GH guideline (Addendum 3), we expanded the use of our polyurethane drape to encompass its use in any infant ≤ 30 weeks of gestation. The staff was educated as part of the development of the VLBW guideline prior to implementation the drape’s use in this expanded group of infants.
3. The need for secure access is very important for premature infants. It allows for the delivery of a
higher amount of nutrition than is possible using a peripheral IV. Up to this point, our unit was inconsistent as to which infants had a UVCUVC placed. As part of our guideline, we standardized the placement of s double lumen UVCs in any infant below 30 weeks of gestation at birth. As part of our delivery and admission process, most of the nursing admission data is collected prior to the practitioner placing the central line for access/fluid administration. Our goal was to shift the focus to early placement of a central line and delay the full nursing assessment. Another goal with early UVC placement was to decrease the incidence of hypoglycemia immediately after birth in these fragile infants. Obtaining quick central access allows for the administration of IV dextrose to prevent early hypoglycemia.
PDSA Cycle: Our guideline outlines obtaining the admission weight, HC, length while the infant is in the DR which then allows for the early placement of the central lines as soon as the infant is admitted to the NICU. We planned to also initiate fluids as soon as the line is placed rather than waiting x-ray confirmation as long as the UVC was placed easily and blood return was noted. Education was given at our bi-annual nursing education blitz that is attended by all nursing staff.
4. Delaying the clamping of the umbilical cord (DCC) may transfer an added volume of 25-40 ml/kg to the
premature infant. Most of the transfusion comes within the first 60-90 seconds after birth7,8. In a Cochrane review on the benefits of DCC in premature infants, they found decreased incidence of any IVH in 7/10 trials (16.4% vs 28.7 %) (RR 1.90 for early clamping (95% CI 1.27-2.84). There was no increase in need for exchange transfusion for polycythemia or hyperbilirubinemia9. We have had a DCC policy, however the implementation was inconsistent.
PDSA Cycle: Our goal was to implement a standardized guideline related to DCC in infants ≤ 34 weeks. A joint OB – Neonatology conference was given on the evidence based importance of DCC in the premature infant. Further, a ‘reminder’ sign was developed (Addendum 2) which was then posted in the scrub area of each of the obstetric ORs. DCC was planned for 60 seconds for any infant ≤ 34 weeks of gestation. Education was given at our bi-annual nursing education blitz that is attended by all nursing staff.
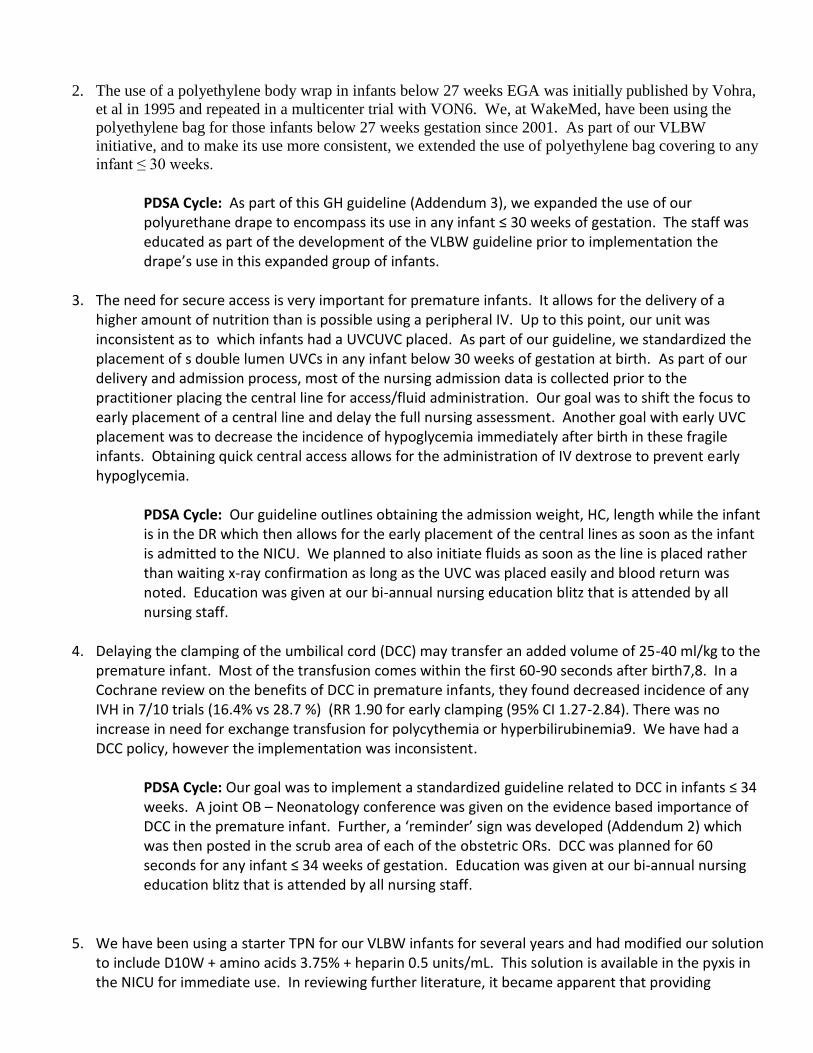
5. We have been using a starter TPN for our VLBW infants for several years and had modified our solution
to include D10W + amino acids 3.75% + heparin 0.5 units/mL. This solution is available in the pyxis in the NICU for immediate use. In reviewing further literature, it became apparent that providing
increased calories in the first day(s) of life is very important to help improve the long term outcome of the very premature infant.
PDSA Cycle: Have pharmacy prepare 5 ml syringes of IL daily using the excess IL from TPN
prepared from our NICU patients. These syringes will then be delivered to the Satellite
pharmacy (which is close to the NICU) for dispensing when needed for a new VLBW admission.
Measures: (as collected from data tool in Addendum 3)
For the incidence of burns related to skin prep on DOL0, we will perform an audit on any infant whose
birthweight is below 1500g to assure that povidone-iodine is used as the skin antiseptic and to verify the
presence/absence of skin burns as a result of its application. Data will be reflected as a % of total.
Use of the polyethylene body wrap will be measured as part of the process of stabilization/admission of the
VLBW infant. Data will be reflected as a % of total.
Central line placement and time of fluid initiation (both Starter TPN and Starter IL) will be measured. Data will
be reflected by demonstrating the time after birth when TPN and Starter IL are initiated. Glucose level will be
measured to ascertain the % of admissions with a glucose <50 mg/dL.
DCC adherence will be measured. Data on whether or not it is performed and the length of DCC will be
collected accordingly.
Data/Results:
Figure One: Skin Burns on DOL0
Year (Pre Data) N, % incidence of skin burns
related to CHG
Birth Weight
Range (N)
2011 3/47 (6.4%) 500-750g (3)
2012 1/31 (3.2%) 750-1000g (1)
2013 5/39 (13%) 500-750g (1) 750-1000g (3)
January 2014 2/5 (40%) 500-750g (1) 750-1000g (1)

Figure Two: Delayed Cord Clamping
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
2011 2012 2013 Jan-14 Feb-Apr14
May-Jul14
Aug-Oct14
Nov-Jan14
Feb-Jul 15
% <1000g with skin burns on DOL0
Initiation of use of Povidone-Iodine for antisepsis on DOL0
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Q4 2014 Q1 2015 Q2 2015
% Infants ≤ 34 wks with DCC
OB Grand Rounds regarding re-focus on ≤ 34 week infants
Education reminder postings in OR and NICU
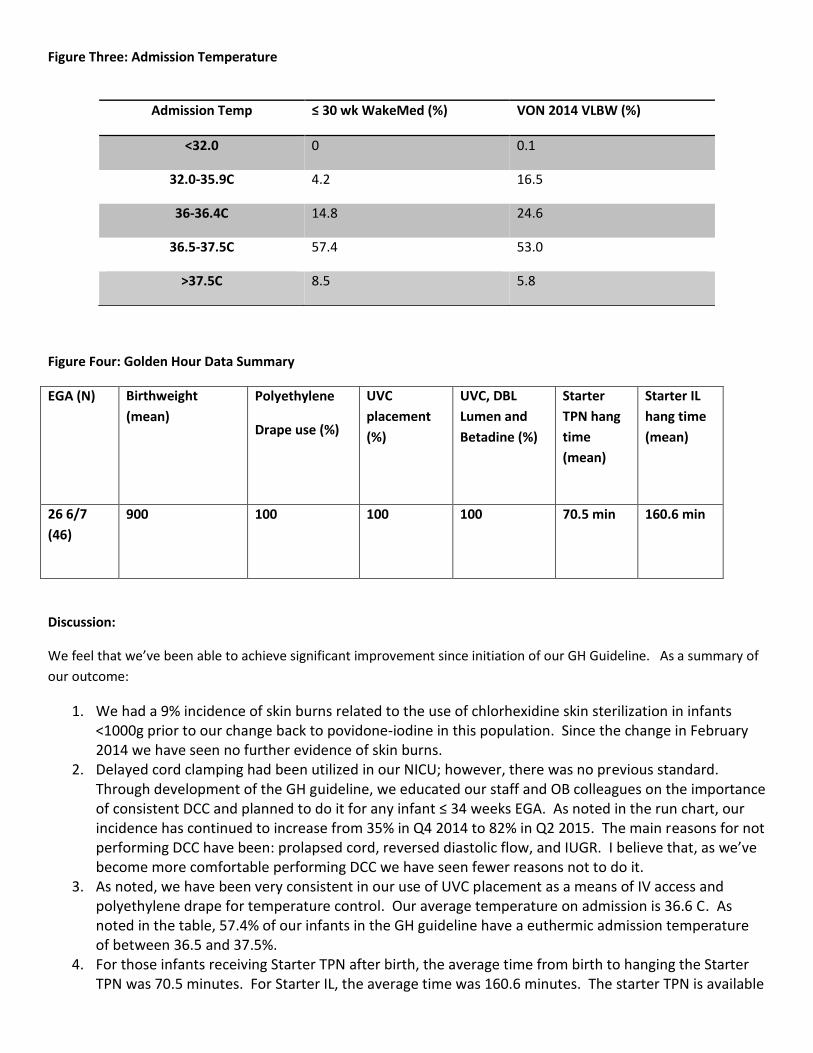
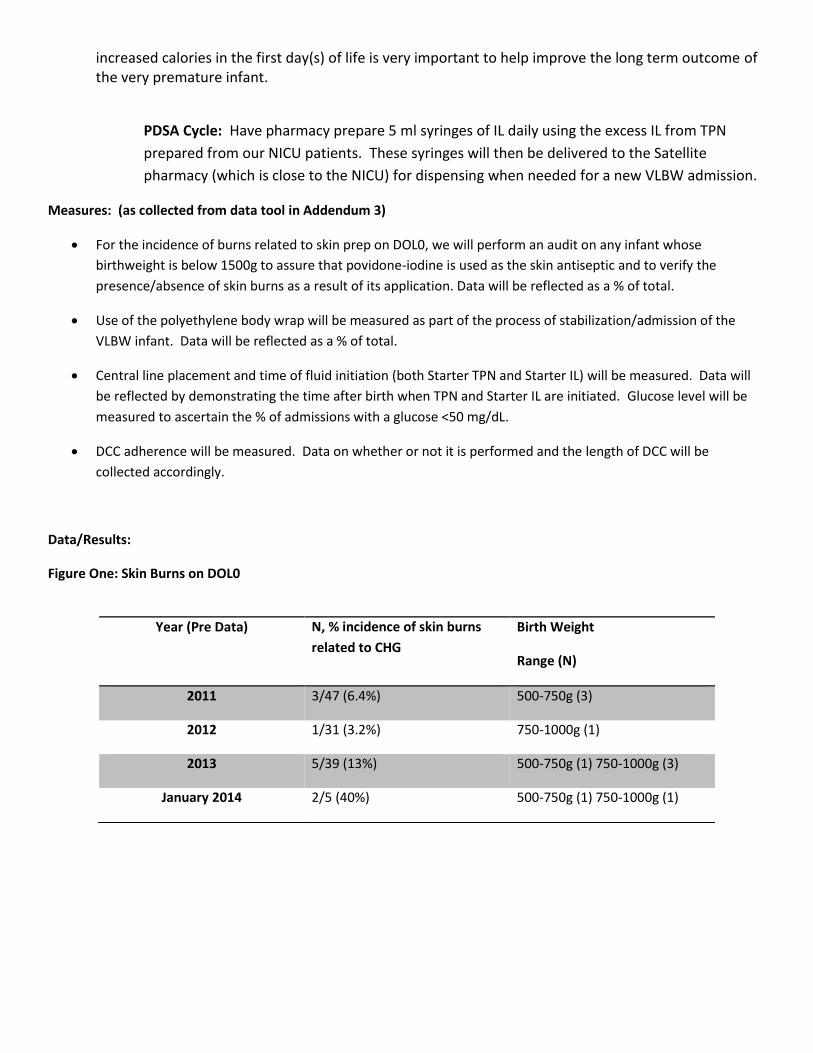
Figure Three: Admission Temperature
Figure Four: Golden Hour Data Summary
EGA (N) Birthweight
(mean)
Polyethylene
Drape use (%)
UVC
placement
(%)
UVC, DBL
Lumen and
Betadine (%)
Starter
TPN hang
time
(mean)
Starter IL
hang time
(mean)
26 6/7
(46)
900 100 100 100 70.5 min 160.6 min
Discussion:
We feel that we’ve been able to achieve significant improvement since initiation of our GH Guideline. As a summary of
our outcome:
1. We had a 9% incidence of skin burns related to the use of chlorhexidine skin sterilization in infants <1000g prior to our change back to povidone-iodine in this population. Since the change in February 2014 we have seen no further evidence of skin burns.
2. Delayed cord clamping had been utilized in our NICU; however, there was no previous standard. Through development of the GH guideline, we educated our staff and OB colleagues on the importance of consistent DCC and planned to do it for any infant ≤ 34 weeks EGA. As noted in the run chart, our incidence has continued to increase from 35% in Q4 2014 to 82% in Q2 2015. The main reasons for not performing DCC have been: prolapsed cord, reversed diastolic flow, and IUGR. I believe that, as we’ve become more comfortable performing DCC we have seen fewer reasons not to do it.
3. As noted, we have been very consistent in our use of UVC placement as a means of IV access and polyethylene drape for temperature control. Our average temperature on admission is 36.6 C. As noted in the table, 57.4% of our infants in the GH guideline have a euthermic admission temperature of between 36.5 and 37.5%.
4. For those infants receiving Starter TPN after birth, the average time from birth to hanging the Starter TPN was 70.5 minutes. For Starter IL, the average time was 160.6 minutes. The starter TPN is available
Admission Temp ≤ 30 wk WakeMed (%) VON 2014 VLBW (%)
<32.0 0 0.1
32.0-35.9C 4.2 16.5
36-36.4C 14.8 24.6
36.5-37.5C 57.4 53.0
>37.5C 8.5 5.8

directly in the NICU in the pyxis; however, the Starter IL is in the Satellite pharmacy and requires our initiating the order and obtaining it from the pharmacy prior to being able to hang it.
Team Acknowledgement:
We would like to acknowledge the work of the following: Stephen Kicklighter, MD (lead QI head for the project);
Jonathan Siegel, MD and Tara Bastek, MD who both were very instrumental in the development of the guideline and
helped to perform education to the staff; Susan Gutierrez RN is our charge nurse and was very helpful in reviewing the
guideline and providing feedback; Maria Friday RN, Mary Parker RN, and Jodi DeJoseph RN (our nursery managers) were
also very instrumental in its initiation; Donna Hirschi RN, Erin Brouch RN, Jennie Stephens RN, Josie Chow RN are 4
nurses who were involved as well as Marie Reilley PT and Jim Helm PhD (developmentalist) were also very helpful in
initiation. Rebecca Mastin was a parent who had a previous premature infant in our nursery as well as a second infant
who had spinal muscular atrophy. She participated in the development of the protocol and was able to come with us to
Peoria, Ill for our Onsite meeting.
Addendum 1: Two ELBW infants with significant skin burns related to antisepsis with chlorhexidine for UAC/UVC line placement.

Addendum 2: Delayed Cord Clamping reminder
Addendum 3: Golden Hour Guideline

Bibliography:
1. Tamma PD, Aucott SW and Milstone AM. Chlorhexidine use in the Neonatal Intensive Care Unit: Results from a National Survey. Infect Control Hosp Epidemiol. 2010 August; 31(8):846-849.
2. Adams D, Quayum M, Worthington T, et al. Evaluation of a 2% chlorhexidine gluconate in 70% isopropyl alcohol skin disinfectant. J Hosp Infection. 2005;61:287-290.
3. Mannan K, Chow P, Lissauer T, et al. Mistaken identity of skin cleansing solution leading to extensive chemical burns in an extremely preterm infant. Acta paediatrica. 2007;96:1536-1545.
4. Kutsch J, Ottinger D. Neonatal Skin and Chlorhexidine: A Burning Experience. Neonatal Network. 2014;33(1):19-23.
5. Vohra S, Frent G, Campbell V, et al. Effect of polyethylene occlusive skin wrapping on heat loss in very low birth weight infants at delivery: A randomized trial. J Pediatr. 1999;134:547-51.
6. Vohra S, Reilly M, Rac VE, Bhaloo Z, Zayack D, Wimmer J, Vincer M, Ferrelli K, Kiss A, Soll R, Dunn M. Study protocol for multicentre randomized controlled trial of HeLP (Heat Loss Prevention) in the delivery room. Contemporary Clinical Trials. 2013;36(1): 54-60.
7. Farrar D, Airey R, Law GR, et al. Measuring placental transfusion for term births; weighing babies with cord intact. BJOG 2010;118:70-75.
8. Raju, TN. Timing of umbilical cord clamping after birth for optimizing placental transfusion. Curr Opin Pediatr. 2013;25(2):180-187.

9. Rabe H, Diaz-Rosello JL, Duley L, et al. Early cord clamping versus delayed cord clamping or cord milking for preterm infants. Cochrane Summaries; August 2012.
Related Documents











