GAURAV NAHAR DNB UROLOGY(STD.) MMHRC DETRUSOR SPHINCTER DYSSYNERGIA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
GAURAV NAHARDNB UROLOGY(STD.)
MMHRC
DETRUSOR SPHINCTER DYSSYNERGIA
INTRODUCTION
MICTURITION CYCLE:Micturition cycle involves two relatively
discrete processes:1. bladder filling and urine storage and2. bladder emptying or voiding

Bladder filling and urine storage :Accommodation of increasing volumes of
urine at a low intravesical pressure (normal compliance) and with appropriate sensation.
A bladder outlet that is closed at rest and remains so during increases in intra-abdominal pressure.
Absence of involuntary bladder contractions (detrusor overactivity).
Bladder emptying/voiding :A coordinated contraction of bladder
smooth musculature of adequate magnitude and duration.
A concomitant lowering of resistance at the level of the smooth and striated sphincter (no functional obstruction).
Absence of anatomic (as opposed to functional) obstruction.

NEURAL CONTROL OF THE LOWER URINARY TRACT
Peripheral Nervous System: The lower urinary tract is innervated by 3 sets of peripheral nerves involving parasympathetic, sympathetic, & somatic nervous systems.
1. Pelvic parasympathetic nerves arise at the sacral level of the spinal cord, excite the bladder, and relax the urethra.
2. Lumbar sympathetic nerves inhibit the bladder body and excite the bladder base and urethra.
3. Pudendal nerves excite the external urethral sphincter.

Mechanism of storage and voiding reflexesA) Storage reflexes. During urine storage, distention of bladder
produces low-level bladder afferent firing. This stimulates (a)sympathetic outflow to the
bladder outlet (base and urethra), and (b)pudendal outflow to the external urethral sphincter.
These responses occur by spinal reflex pathways & represent “guarding reflexes,” which promote continence.
Sympathetic firing also inhibits detrusor muscle and transmission in bladder ganglia.
B) Voiding reflexes.At the initiation of micturition, intense
vesical afferent activity activates brainstem micturition center(PMC), which inhibits spinal guarding reflexes (sympathetic and pudendal outflow to the urethra).
PMC also stimulates parasympathetic outflow to bladder & internal sphincter smooth muscle.
Smooth sphincter :Smooth musculature of the bladder neck
and proximal urethra.A physiologic (but not anatomic )sphincter.Not under voluntary control.

Striated sphincter:1. Striated musculature that is a part of the outer
wall of the proximal urethra in both male and female. a/k/s intrinsic or intramural striated sphincter or rhabdosphincter, &
2. bulky skeletal muscle group that closely surrounds the urethra at the level of the membranous portion in the male and primarily the middle segment in the female a/k/s extrinsic or extramural striated sphincter.
The extramural portion is the classically described external urethral sphincter and is under voluntary control.

ANATOMY OF BLADDER & ITS OUTLET

Bladder storage & emptying requires continual coordination of detrusor & external urinary sphincter (EUS), mediated by central & peripheral nervous systems.
Neurological conditions, lesions or trauma can cause disturbances in urinary storage and voiding, resulting in bladder dysfunction.
DEFINITION
Dyssynergia:Kinesiologic disassociation of two groups of muscles
that generally work in harmony.
Sphincter dyssynergia:An involuntary contraction or lack of relaxation of
either the striated sphincter (the striated muscle surrounding the proximal urethra and the striated muscle that forms a part of the urethra for a variable distance from the “urogenital diaphragm” to the bladder neck) or the smooth sphincter (the smooth muscle of the bladder neck and proximal urethra).
Detrusor sphincter dyssynergia (DSD):defined by the ICS as Impaired coordination between detrusor
and sphincter during voiding due to a neurologic abnormality (i.e. detrusor contraction synchronous with contraction of the urethral and/or periurethral striated muscles).
unless specified otherwise, refers to dyssynergia of the striated sphincter.
detrusor striated-sphincter dyssynergia and detrusor external-sphincter dyssynergia.
Smooth sphincter dyssynergia or Proximal sphincter dyssynergia occurs in an individual with autonomic hyperreflexia/dysreflexia (Spinal cord injury above T6 level).
True DESD: only in patients who have an abnormality in pathways between sacral spinal cord & brainstem PMC.
Detrusor sphincter dyssynergia (DSD) is the most common cause of neurogenic sphincteric obstruction.

ETIOLOGY
Common causes:traumatic SCI,multiple sclerosis, Spinal dysraphism, andvarious forms of transverse myelitis.
PATHOPHYSIOLOGY
During normal filling, pelvic nerve afferents are modulated by sympathetic output to cause relaxation of the detrusor while maintaining the tone of the bladder neck sphincter.
There is tonic activity of EUS facilitated by input from PMC.

During voluntary micturition, inhibitory signals from frontal cortex to PMC are removed thus allowing activation of micturition reflex.
The PMC inhibits spinal guarding reflexes and transmits excitatory signals to bladder.
The EUS relaxes with synergistic contraction of the detrusor for a coordinated decrease in urethral pressure and rise in detrusor pressure to allow the outflow of urine.

DSD occurs in the setting of neurological abnormalities b/w PMC and sacral spinal cord.
This interruption of the spinobulbospinal pathways → failed inhibition of spinal guarding reflexes + erroneous excitation of Onuf’s nucleus causing EUS contraction to occur during detrusor contraction, generating elevated detrusor pressures.

CLASSIFICATIONBLAIVAS CLASSIFICATION:Type 1:concomitant increase in both detrusor
pressure & EMG activity;at the peak of detrusor contraction,
sphincter suddenly relaxes & unobstructed voiding occurs.
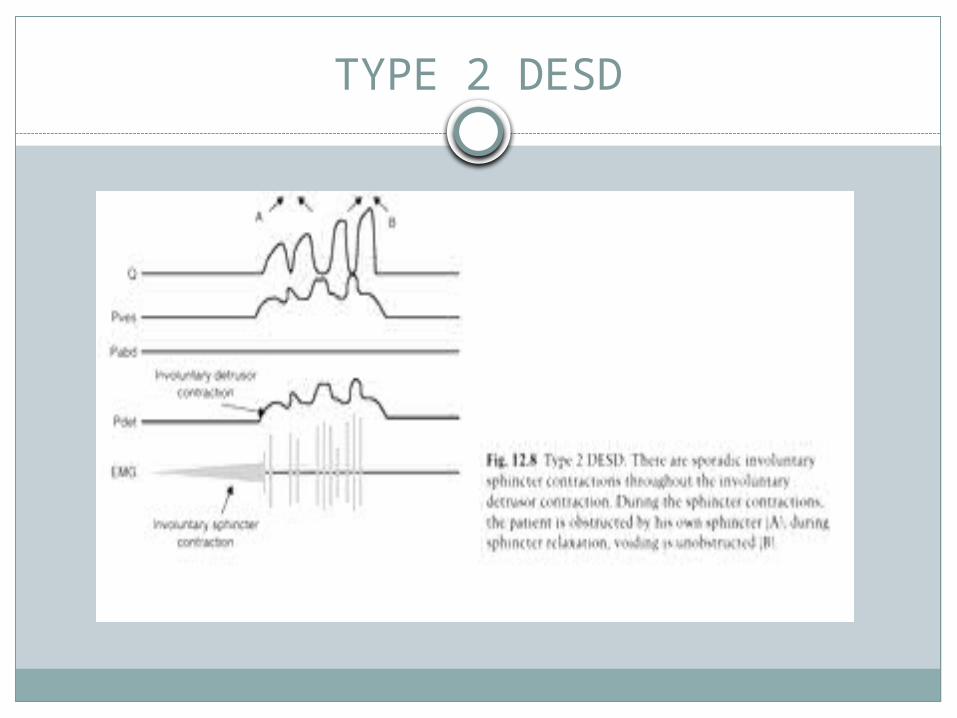
Type 2:Sporadic/clonic contractions of striated
sphincter intermittently during detrusor contraction.
Intermittent urinary stream.

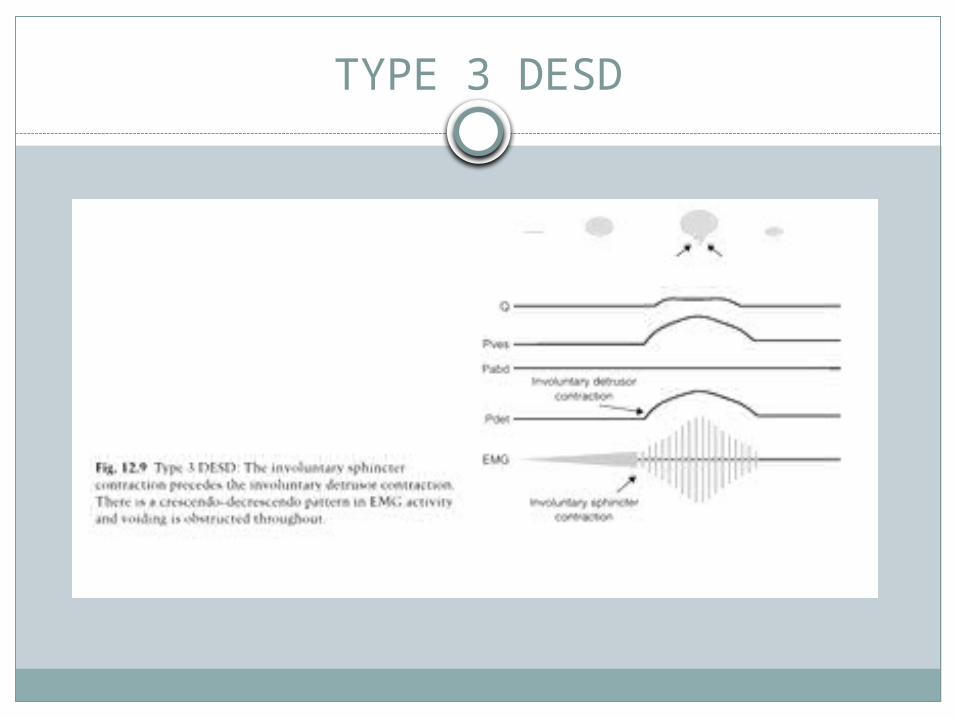
Type 3:Crescendo-decrescendo pattern of sphincter
contraction that results in outlet obstruction throughout entire detrusor contraction.
Urinary obstruction & Inability to urinate.

TYPE 1 DESD
TYPE 2 DESD
TYPE 3 DESD

CORRELATION b/w DSD type & degree of SCI lesions:
Incomplete sensory and motor lesion → type 1 DESD.
Complete sensory and motor lesions → type 2 and type 3.
WELD CLASSIFICATION:Continuous DESD.Intermittent DESD.
PSEUDO DYSSYNERGIA:Pseudodyssynergia is the presence of EUS
contraction occurring during micturition that may be misinterpreted for DSD.
Sphincter EMG activity increases simultaneously with intravesical or detrusor pressure.
Common causes of pseudodyssynergia include(1) abdominal straining to either initiate or
augment a bladder contraction or in response to discomfort and
(2) attempted inhibition of a bladder contraction either because of its involuntary nature or because of discomfort.

Pseudodyssynergia can reliably be differentiated from true DESD urodynamically by analyzing the patterns of detrusor and EMG activity.
EPIDEMIOLOGY
The precise incidence of DSD is unknown given the variability in neurological disease.
SCI contributes to a significant portion of cases of DSD.
≈ 75% of patients with suprasacral SCI have DSD.
Incidence of DSD in MS and spinal dysraphism is estimated at 25 – 50%.
CLINICAL PRESENTATION
Mixed storage and voiding symptoms,Urinary incontinence orComplications of DSD, i.e. UTIs and bladder
calculi.Neurological symptoms may predominate and
trigger initial neurourological investigation.
DIAGNOSTIC EVALUATION
HISTORY AND PHYSICAL EXAMINATION:Aim to diagnose the cause & nature of
bladder dysfunction, &To identify associated complications.assess for changes in urinary, bowel and
neurological symptoms,Disease duration, severity, prior
investigations and treatments.
Screening for occult neurological disease: inquiry regarding visual changes, back or neck pain, weakness, paraesthesia, urinary or bowel symptoms.
Abdominal examination: assess for palpable bladder, constipation, tenderness and previous incisions.
Genitalia: inspected for abnormality and skin irritation

DRE is necessary to assess anal sphincter tone at rest and during voluntary contraction.
Testing perineal sensation, bulbocavernosus reflex and cremasteric reflexes.
BASIC INVESTIGATIONS:Urine culture and sensitivity, if there is a
suspicion of UTI.Serum electrolytes, urea & creatinine.Voiding diaries helpful in characterising
voiding dysfunction.Ultrasonography helpful for assessment of
hydronephrosis, urinary calculi & post-void residual urine volumes.

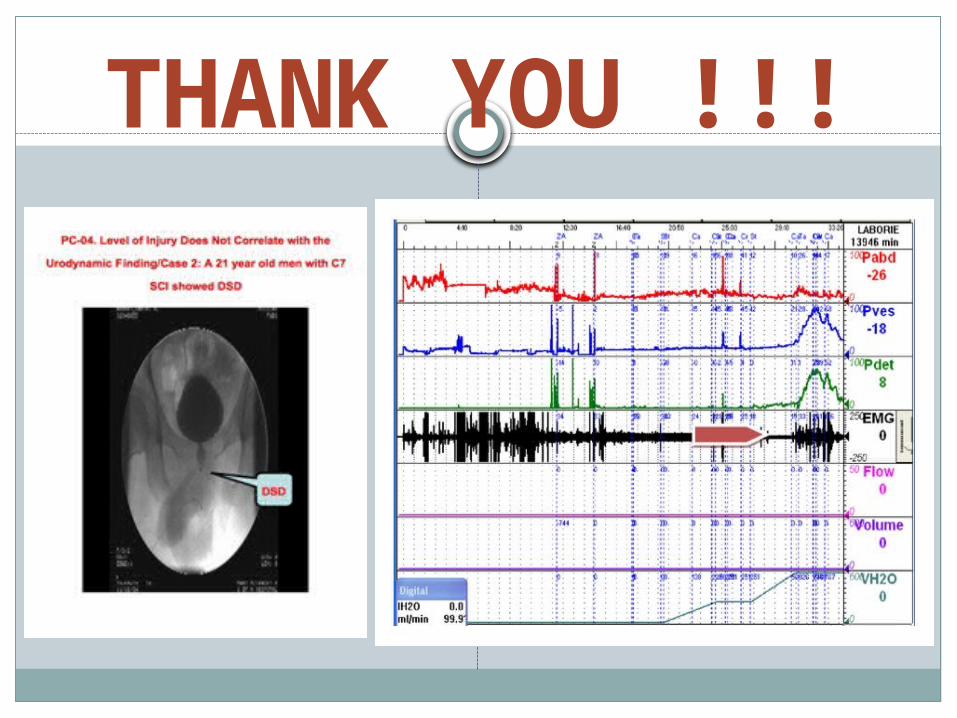
URODYNAMICS
Urodynamics: critical role in detection of DSD and monitoring for associated complications.
DSD can be diagnosed using electromyography (EMG), voiding cystourethrogram (VCUG) and/or urethral pressure profilometry.
Diagnosis of DSD by EMG requires elevated ‘EMG activity during detrusor contraction, in the absence of Valsalva and Crede manoeuvres .’
Typical VCUG findings: a closed bladder neck during filling and subsequent dilation of bladder neck & proximal urethra to the level of EUS during micturition.

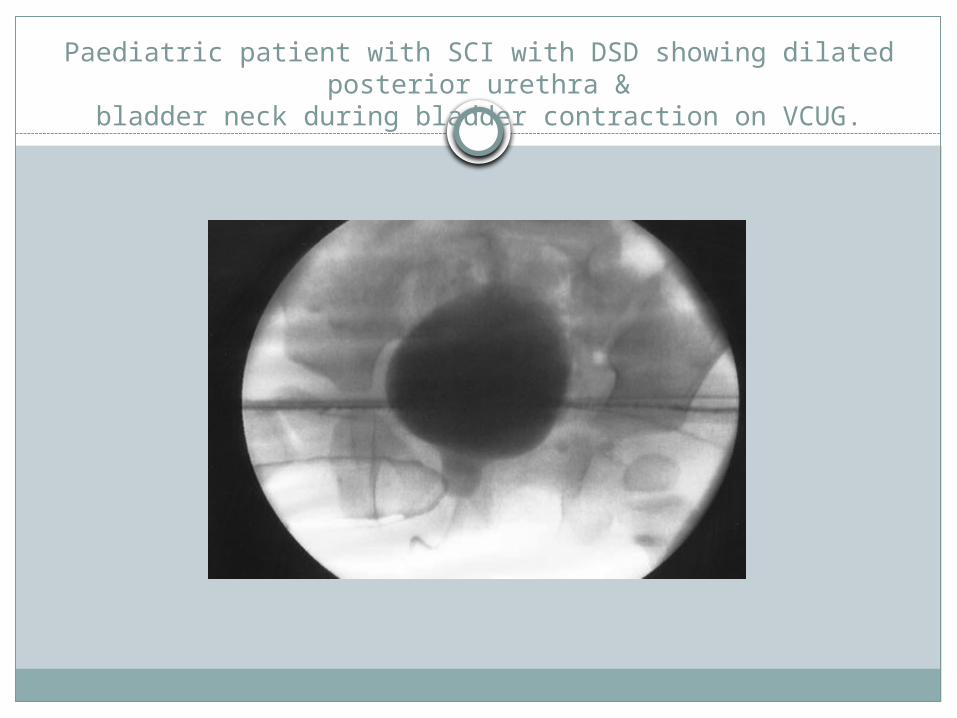
Paediatric patient with SCI with DSD showing dilated posterior urethra &
bladder neck during bladder contraction on VCUG.

EMG Vs VCUG
Diagnostic discrepancy between EMG & VCUG ranges from 40% to 46%.
Males more often diagnosed with EMG whereas females more often diagnosed by VCUG.
Diagnosis of DSD in males by VCUG may be impaired due to anatomical BOO by prostate and that in the female diagnosis by EMG may be impaired due to increased electrode artefact.

Role of urethral pressure profilometry in diagnosis of DSD is controversial.
Unfortunately, a perfect test for DSD does not exist.
Detection of DSD can be improved by using both EMG and VCUG.
Pathology such as BOO, Parkinson’s disease and dysfunctional voiding should be considered before diagnosis, as they may have similar symptomatology.

COMPLICATIONS
DESD results in a high bladder pressure with subsequent back pressure effects.
The rate of urological complications from DESD with no intervention is 50%.
Complications are much less common in females because of decreased detrusor pressures generated.

If left untreated, DESD can result in:• UTI/Urosepsis• VUR • Hydronephrosis • Upper tract deterioration• Renal insufficiency• Urolithiasis

TREATMENT
Goals of treatment:Adequate storage at low intravesical
pressure.Adequate emptying at low intravesical
pressure.Absence or control of infection.Upper urinary tract preservation or
improvement.Social acceptability and adaptability.

Type 1 DESD: observation alone unless there is persistent reflux, hydronephrosis, or autonomic hyperreflexia.
Types 2 and 3: treated.DLPP>40 cm water- significantly higher
incidence of upper tract damage and persistent DESD, hence warrants treatment.

Current approaches:1-Chronic indwelling catheterization.2-Intermittent self catheterization.3-Pharmacological therapy.4-Bladder reconstruction and urinary diversion.5-External sphincterotomy.6- Stent placement(Urolume)across the
sphincter.7-Sphincter ablation with Botulinum toxin inj.8-Intrathecal continuous baclofen infusion.9-Balloon dilatation.10-Laser sphincter ablation

C.I.S.C.
Intermittent catheterisation combined with anticholinergics to reduce detrusor pressures is the most common treatment for DSD.
Pharmacotherapy has a limited role in the management of DSD.

Surgical Sphincterotomy
Therapeutic destruction of the external urethral sphincter.
A surgical incision into the sphincter muscle to open it, then urine drains out and collected by condom drainage.
Female anatomy does not allow for condom drainage as an alternative.

The 12-o’clock sphincterotomy (Madersbacher and Scott), remains the procedure of choice for a number of reasons:
Main bulk of the sphincter is anteromedial. With the blood supply primarily lateral, a 12-
o’clock incision is least likely to cause hemorrhage.
The rate of postoperative erectile dysfunction with this incision is approximately 5%.

Early failure due toan inadequate surgical procedure (either not
deep enough or not extensive enough),inadequate detrusor function, and bladder neck or prostatic obstruction.Late failure may occur because of fibrosis somewhere along the extent of the
sphincterotomy,a change in detrusor function,development of prostatic obstruction, or a change in neurologic status such that smooth
sphincter dyssynergia develops.

Failure defined as 1. presence of large PVRU associated with UTI 2. autonomic hyperreflexia symptomatology
associated with bladder overdistention or high voiding pressures, and/or
3. progressive upper tract deterioration from persistent reflux or poor bladder emptying.

Lower urinary tract complications may occur:Recurrent infection, calculi, urethral
diverticula, stricture, bladder neck stenosis, and recurrent epididymitis.

Urethral Stenting
Use of a urethral stent to bypass the striated sphincter.
A significant decrease in 1. detrusor leak point pressure2. residual urine volume3. Mean voiding pressure4. symptoms of autonomic dysreflexia.One obvious advantage: sphincteric stent is
potentially reversible.
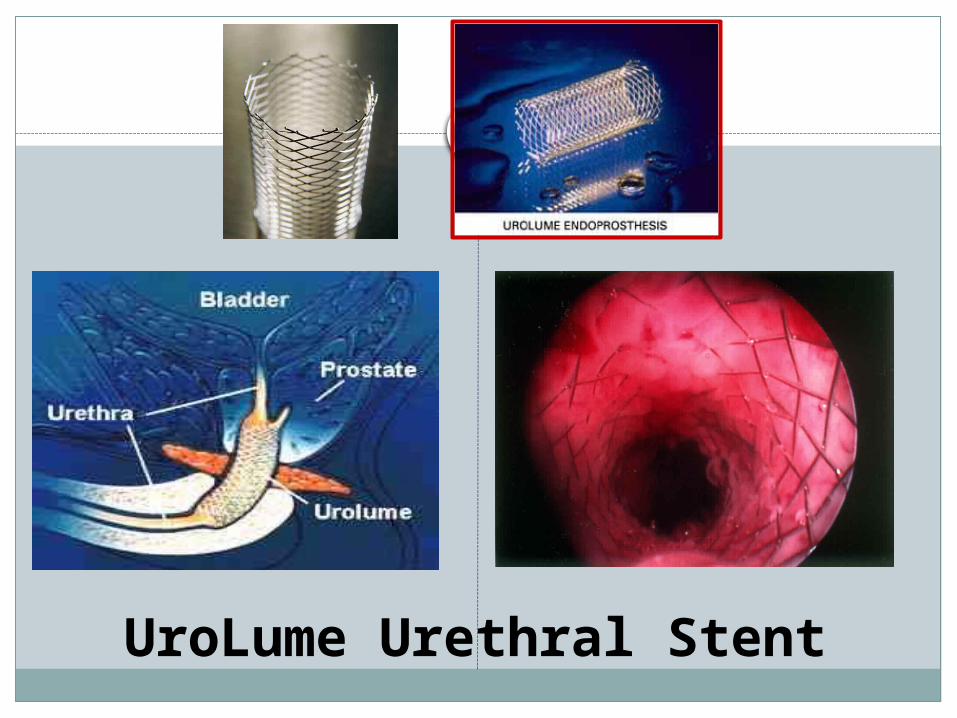
UroLume Urethral Stent

The Urolume (cont.)

Complications includeobstruction by urothelial ingrowth,stent encrustation,stricture,stent migration,&UTI.
Pharmacologic Sphincterotomy
Periurethral injections of botulinum A toxin.
Acts by inhibiting acetylcholine release from presynantic cholinergic nerve terminals, thereby inhibiting striated & smooth muscle contractions.
Use remains uncommon & unclear.
Urethral Overdilatation
Urethral overdilatation through the use of urethral sounds or balloon procedures may improve compliance and decrease outlet resistance.
Urethral overdilatation to 40 to 50 Fr in females & 22 to 28 Fr in 11 myelodysplastic children with high intravesical pressures refractory to traditional forms of treatment.
An ineffective long-term treatment for striated sphincter dyssynergia.

Neuromodulation
Pudendal nerve interruption is seldom performed today due to potential complications, including impotence and significant fecal and stress urinary incontinence.
Dorsal root rhizotomy with sacral anterior nerve root stimulation.
THANK YOU !!!
Related Documents











