..................................................................................................................................................................................... ..................................................................................................................................................................................... CLINICAL RESEARCH Heart failure/cardiomyopathy Determinants and prognostic value of pulmonary arterial pressure in patients with chronic heart failure Thibaud Damy 1,2,3,4 * , Kevin M. Goode 1 , Anna Kallvikbacka-Bennett 1 , Christian Lewinter 1 , James Hobkirk 1 , Nikolay P. Nikitin 1 , Jean-Luc Dubois-Rande ´ 2,3,4 , Luc Hittinger 2,3,4 , Andrew L. Clark 1 , and John G.F. Cleland 1 1 Department of Cardiology, University of Hull, Castle Hill Hospital, Kingston-upon-Hull, UK; 2 Fe ´de ´ration de cardiologie at the AP-HP, Groupe Henri-Mondor Albert-Chenevier, Cre ´teil F-94010, France; 3 INSERM, Unite ´ U955, Cre ´teil F-94010, France; and 4 Universite ´ Paris-Est 12, Faculte ´ de Me ´decine, UMR-S 9555, Creteil F-94010, France Received 19 November 2009; revised 3 June 2010; accepted 17 June 2010; online publish-ahead-of-print 5 August 2010 Aims The epidemiology of pulmonary arterial hypertension (PAH) in patients with heart failure (HF) is poorly described. Our aim was to investigate the determinants and prognostic significance of PAH in a large representative outpatient population with HF. Methods and results Routine measurement of right ventricular tricuspid pressure gradient (RVTG) was attempted among unselected, consecutive referrals to an HF clinic. The diagnosis of HF was based on symptoms, signs, echocardiography, and N-terminal pro-brain natriuretic peptide (NT-proBNP). Of 2100 patients referred, 1380 were diagnosed as HF, of whom 1026 had left ventricular systolic dysfunction (LVSD) and 354 did not. Right ventricular tricuspid pressure gra- dient could be measured in 270 (26%) patients with and 143 (40%) without LVSD. The highest RVTG quartile [RVTG . 35 mmHg equivalent to an estimated PA systolic pressure (PASP) . 45 mmHg] constituted 7% of all those with HF and was associated with higher LV filling pressures, LV end-diastolic volume, LVSD, and more severe mitral regurgitation (MR). During a median (inter-quartile range) follow-up of 66 (56–74) months, mortality was 40.3%. Mortality was similar in the lowest quartile of RVTG and in those in whom RVTG could not be measured and rose with increasing RVTG quartile (log-rank: 26.9; P , 0.0001). The highest RVTG quartile, age, blood pressure, and log NT-proBNP independently predicted mortality. Right ventricular tricuspid pressure gradient .35 mmHg had a 96% specificity to discriminate between those with and without HF in patients without LVSD. Conclusion Using a definition of PASP . 45 mmHg, 7% of the patients with HF have PAH, which is associated with worse LV function, MR, and prognosis. Whether PAH is a target for therapy in this population remains to be elucidated. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Pulmonary arterial hypertension † Heart failure † Echocardiography † Prognosis † Determinant Introduction Pulmonary arterial (PA) pressure may be increased in heart failure (HF) and is associated with more severe symptoms and worse out- comes. 1 Pulmonary arterial hypertension (PAH) can be defined as a mean PA pressure .25 mmHg at rest, 2 measured invasively by right heart catheterization, and can be detected non-invasively with Doppler echocardiography that allows PA systolic pressure (PASP) to be estimated from the peak velocity of tricuspid regurgitation (TRV). A PASP of .35 mmHg is used to define mild PAH. 2 However, PASP increases with age and body mass index (BMI) 3 and a higher threshold for diagnosing PAH may be more appropriate for older patients with HF. However, the threshold definition of PAH is important as it will determine the prevalence of PAH and may be used to guide prognosis and future treatment. Previous reports have focused on the determinants of PAH, its prevalence, and its effect on prognosis in selected groups of * Corresponding author. Tel: +33 1 482 461 917, Fax: +33 1 482 624 085, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2010. For permissions please email: [email protected]. European Heart Journal (2010) 31, 2280–2290 doi:10.1093/eurheartj/ehq245 by guest on October 14, 2011 eurheartj.oxfordjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCHHeart failure/cardiomyopathy
Determinants and prognostic value of pulmonaryarterial pressure in patients with chronic heartfailureThibaud Damy1,2,3,4*, Kevin M. Goode1, Anna Kallvikbacka-Bennett 1,Christian Lewinter1, James Hobkirk1, Nikolay P. Nikitin1, Jean-Luc Dubois-Rande 2,3,4,Luc Hittinger 2,3,4, Andrew L. Clark1, and John G.F. Cleland1
1Department of Cardiology, University of Hull, Castle Hill Hospital, Kingston-upon-Hull, UK; 2Federation de cardiologie at the AP-HP, Groupe Henri-Mondor Albert-Chenevier,Creteil F-94010, France; 3INSERM, Unite U955, Creteil F-94010, France; and 4Universite Paris-Est 12, Faculte de Medecine, UMR-S 9555, Creteil F-94010, France
Received 19 November 2009; revised 3 June 2010; accepted 17 June 2010; online publish-ahead-of-print 5 August 2010
Aims The epidemiology of pulmonary arterial hypertension (PAH) in patients with heart failure (HF) is poorly described.Our aim was to investigate the determinants and prognostic significance of PAH in a large representative outpatientpopulation with HF.
Methodsand results
Routine measurement of right ventricular tricuspid pressure gradient (RVTG) was attempted among unselected,consecutive referrals to an HF clinic. The diagnosis of HF was based on symptoms, signs, echocardiography, andN-terminal pro-brain natriuretic peptide (NT-proBNP). Of 2100 patients referred, 1380 were diagnosed as HF, ofwhom 1026 had left ventricular systolic dysfunction (LVSD) and 354 did not. Right ventricular tricuspid pressure gra-dient could be measured in 270 (26%) patients with and 143 (40%) without LVSD. The highest RVTG quartile[RVTG . 35 mmHg equivalent to an estimated PA systolic pressure (PASP) . 45 mmHg] constituted 7% of allthose with HF and was associated with higher LV filling pressures, LV end-diastolic volume, LVSD, and moresevere mitral regurgitation (MR). During a median (inter-quartile range) follow-up of 66 (56–74) months, mortalitywas 40.3%. Mortality was similar in the lowest quartile of RVTG and in those in whom RVTG could not be measuredand rose with increasing RVTG quartile (log-rank: 26.9; P , 0.0001). The highest RVTG quartile, age, blood pressure,and log NT-proBNP independently predicted mortality. Right ventricular tricuspid pressure gradient .35 mmHg hada 96% specificity to discriminate between those with and without HF in patients without LVSD.
Conclusion Using a definition of PASP . 45 mmHg, 7% of the patients with HF have PAH, which is associated with worse LVfunction, MR, and prognosis. Whether PAH is a target for therapy in this population remains to be elucidated.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Pulmonary arterial hypertension † Heart failure † Echocardiography † Prognosis † Determinant
IntroductionPulmonary arterial (PA) pressure may be increased in heart failure(HF) and is associated with more severe symptoms and worse out-comes.1 Pulmonary arterial hypertension (PAH) can be defined asa mean PA pressure .25 mmHg at rest,2 measured invasively byright heart catheterization, and can be detected non-invasivelywith Doppler echocardiography that allows PA systolic pressure(PASP) to be estimated from the peak velocity of tricuspid
regurgitation (TRV). A PASP of .35 mmHg is used to definemild PAH.2 However, PASP increases with age and body massindex (BMI)3 and a higher threshold for diagnosing PAH may bemore appropriate for older patients with HF. However, thethreshold definition of PAH is important as it will determine theprevalence of PAH and may be used to guide prognosis andfuture treatment.
Previous reports have focused on the determinants of PAH, itsprevalence, and its effect on prognosis in selected groups of
* Corresponding author. Tel: +33 1 482 461 917, Fax: +33 1 482 624 085, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2010. For permissions please email: [email protected].
European Heart Journal (2010) 31, 2280–2290doi:10.1093/eurheartj/ehq245
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
patients with HF.1,4 –7 However, in these studies, patients withclinically obvious COPD were often excluded, lung function wasnot routinely assessed and the diagnosis of COPD lacked pre-cision.4 Chronic obstructive pulmonary disease and HF commonlyco-exist and their respective roles for the development of PAH inHF remain unclear.
We studied the prevalence, determinants, and prognosticimpact of PAH among consecutive patients referred for thediagnosis or exclusion of suspected HF. We also aimed to deter-mine a value of PASP that might be used to define a populationat high risk who might be candidates for treatments targeted atPAH.
Methods
Study population and proceduresThe patients enrolled were referred for the evaluation of suspectedHF, predominantly exertional breathlessness, between August 2001and May 2008 by local primary and secondary care physiciansserving a population of about 560 000 in Kingston-upon-Hull and theEast Riding of Yorkshire, UK.
All patients were clinically evaluated and had a 6 min walk test, elec-trocardiogram, blood tests, spirometry, and echocardiogram.
Heart failure was defined as the presence of an appropriate historyand symptoms and either left ventricular ejection fraction (LVEF) ≤45% [LV systolic dysfunction (LVSD)] or LVEF . 45% together withN-terminal pro-brain natriuretic peptide (NT-proBNP) ≥ 50 pmol/L(≥423 pg/mL) (preserved systolic HF or PS-HF). Ischaemic heartdisease (IHD) was defined as a previous myocardial infarction, coron-ary bypass surgery, or coronary disease on angiography. Patientsunderwent spirometry (Vitalograph, Vitalinkw, UK). Forced expiratoryvolume in 1 s (FEV1) and forced vital capacity (FVC) were measured.Chronic obstructive pulmonary disease was defined as ‘absent ormild’ if the FEV1/FVC ratio was .70% and ‘worse than (.) mild’ ifthe FEV1/FVC ratio was ,70% together with measured FEV1, 80%predicted.8 Patients with atrial fibrillation or atrial flutter weregrouped as ‘AF’.
Echocardiographic measurementsTransthoracic echocardiography examinations were performed fol-lowing the recommendations of the British Society of Echocardiogra-phy9 using a Vivid Five (GE Healthcare, UK) system. Echocardiogramswere reviewed, blind of patients’ clinical information, by a single oper-ator (T.D.) using an EchoPAC station (GE Healthcare). The average ofthree measurements was used in patients in sinus rhythm and five inpatients in AF. Left ventricular ejection fraction was measured usingSimpson’s biplane method or, if measurements were technically notpossible [n ¼ 49, 12% of the patient with right ventricular tricuspidpressure gradient (RVTG)], LVSD was graded using a subjectivescale of normal/mild/mild to moderate/moderate/moderate tosevere and severe where ‘normal to mild’ was assumed to be equiv-alent to LVEF . 45%. The LV end-diastolic volume was indexed tothe body surface area (LVEDVind). Tricuspid regurgitation area wasmeasured during the review of echoes. Tricuspid regurgitation wasclassified as mild or less if TR area was ,5 cm2, severe if TR area.10 cm2, and moderate between these limits.9 To estimate TRprevalence, the scale was abbreviated to: none/≤mild and .mild(Figure 1). The maximum peak velocity of TR was measured usingcontinuous Doppler (Figure 1). The maximum peak velocity was not
clearly delineated in 44 patients who were thereafter considerednot to have had an RVTG measurement. Trans-tricuspid gradient(RVTG, mmHg) was estimated from the modified Bernoulliequation10 as RVTG ¼ 4 × (peak TR velocity).2 Right ventricular tri-cuspid pressure gradient can be considered equal to the PASP afteradding the estimated mean right atrial pressure of 10 mmHg11 inthe absence of RV outflow tract obstruction. We did not measureinferior vena cava size and its respiratory variation as it is poorlyrelated to mean right atrial pressure.12 Tricuspid annular planesystolic excursion and RV end-diastolic area were measured to eva-luate RV systolic function and dimension. Mitral regurgitation (MR)was quantified by measuring the area of the colour Doppler signaldivided by the left atrial (LA) area measured in the four-chamberview. Mitral regurgitation was considered ‘mild or less’ if MR area/LA area was ,10%, ‘severe’ if MR area/LA area was .40%, and mod-erate if between the two. Left atrial volume was measured in thefour-chamber view and indexed to the body surface area (LAind).Peak mitral early diastolic velocity (E, m/s), the E-wave decelerationtime (DCT, ms), and the velocity at atrial contraction (A, m/s) weremeasured using pulsed-wave Doppler. Left ventricular filling pressureclasses were defined in accordance with the ASE 2009 guidelines.13 InLVSD patients: raised LV filling pressure was defined as E/A ≥ 2 if insinus rhythm or DCT , 150 ms if in AF; normal LV filling pressurewas defined as E/A , 1 in patients in sinus rhythm or DCT ≥200 ms for those in AF; patients between these limits were classedas undetermined. In PS-HF patients, LV filling pressure was classifiedusing the LA volume indexed to body surface area as follows: raisedLV filling pressure if LAind . 34 mL/m2 and normal LV filling pressure ifLAind ≤ 34 mL/m2.13
EthicsThe investigation conforms to the principles outlined in theDeclaration of Helsinki. It was approved by the Hull and EastYorkshire Research Ethics Committee. All subjects gave their writteninformed consent.
Statistical analysisThe population was divided into quartiles by RVTG, and then intotwo groups after determining the best RVTG cut-off value topredict mortality. Data are presented as mean and standard deviationor median and inter-quartile range (IQR) if not normally distributedfor quantitative values and as numbers and percentages for categori-cal data. N-terminal pro-brain natriuretic peptide was normalizedby logistic transformation prior to testing. Differences betweencontinuous data were tested using the Kruskal–Wallis test and theMann–Whitney test as appropriate. The Pearson x2 test was usedto compare categorical data. Independent clinical and echocardio-gaphic determinants of RVTG were assessed using logistic regressionwith backward elimination of independent variables based onlikelihood-ratio tests. The probability of death at 12 months wasassessed as a continuous function of RVTG using a movingaverage estimator. The size of the averaging window was setto 10% of the available observations. The resultant curve wassmoothed using a best-fit polynomial equation. Multivariable Cox’sproportional hazard analysis was used to test the prognostic valueof variables. Independent prognostic factors were identified by abackward stepwise selection algorithm. Six models were tested.The Kaplan–Meier plots were used to present survival curves andthe log-rank test was used. Analyses were performed using SPSS16.0 (SPSS Inc., Chicago, IL, USA). P-values were considered signifi-cant if ,0.05.
Determinants and prognostic value of PAH in HF patients 2281
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
Results
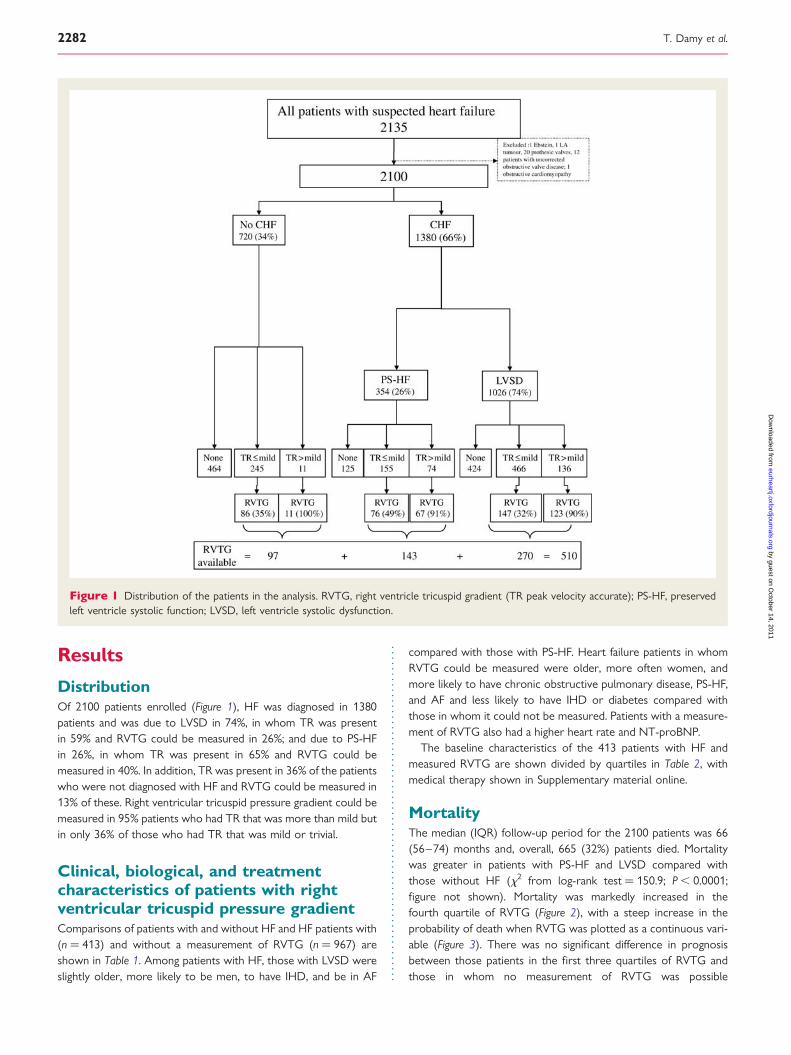
DistributionOf 2100 patients enrolled (Figure 1), HF was diagnosed in 1380patients and was due to LVSD in 74%, in whom TR was presentin 59% and RVTG could be measured in 26%; and due to PS-HFin 26%, in whom TR was present in 65% and RVTG could bemeasured in 40%. In addition, TR was present in 36% of the patientswho were not diagnosed with HF and RVTG could be measured in13% of these. Right ventricular tricuspid pressure gradient could bemeasured in 95% patients who had TR that was more than mild butin only 36% of those who had TR that was mild or trivial.
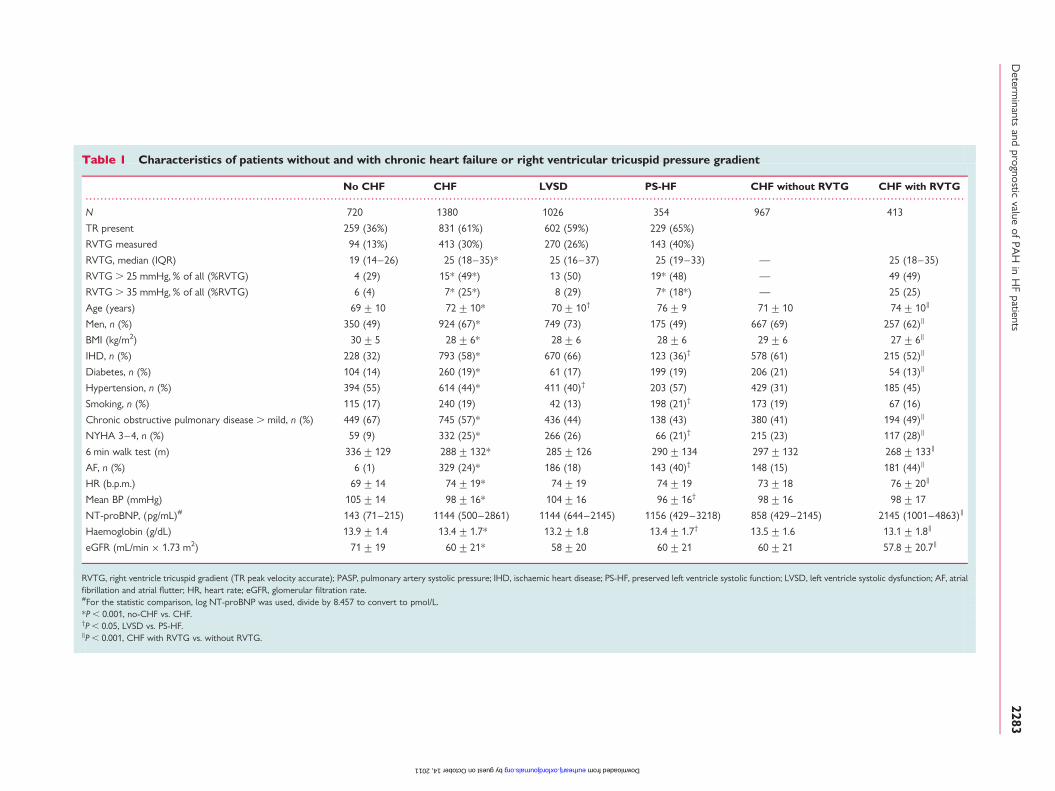
Clinical, biological, and treatmentcharacteristics of patients with rightventricular tricuspid pressure gradientComparisons of patients with and without HF and HF patients with(n ¼ 413) and without a measurement of RVTG (n ¼ 967) areshown in Table 1. Among patients with HF, those with LVSD wereslightly older, more likely to be men, to have IHD, and be in AF
compared with those with PS-HF. Heart failure patients in whomRVTG could be measured were older, more often women, andmore likely to have chronic obstructive pulmonary disease, PS-HF,and AF and less likely to have IHD or diabetes compared withthose in whom it could not be measured. Patients with a measure-ment of RVTG also had a higher heart rate and NT-proBNP.
The baseline characteristics of the 413 patients with HF andmeasured RVTG are shown divided by quartiles in Table 2, withmedical therapy shown in Supplementary material online.
MortalityThe median (IQR) follow-up period for the 2100 patients was 66(56–74) months and, overall, 665 (32%) patients died. Mortalitywas greater in patients with PS-HF and LVSD compared withthose without HF (x2 from log-rank test ¼ 150.9; P , 0.0001;figure not shown). Mortality was markedly increased in thefourth quartile of RVTG (Figure 2), with a steep increase in theprobability of death when RVTG was plotted as a continuous vari-able (Figure 3). There was no significant difference in prognosisbetween those patients in the first three quartiles of RVTG andthose in whom no measurement of RVTG was possible
Figure 1 Distribution of the patients in the analysis. RVTG, right ventricle tricuspid gradient (TR peak velocity accurate); PS-HF, preservedleft ventricle systolic function; LVSD, left ventricle systolic dysfunction.
T. Damy et al.2282
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Characteristics of patients without and with chronic heart failure or right ventricular tricuspid pressure gradient
No CHF CHF LVSD PS-HF CHF without RVTG CHF with RVTG
N 720 1380 1026 354 967 413
TR present 259 (36%) 831 (61%) 602 (59%) 229 (65%)
RVTG measured 94 (13%) 413 (30%) 270 (26%) 143 (40%)
RVTG, median (IQR) 19 (14–26) 25 (18–35)* 25 (16–37) 25 (19–33) — 25 (18–35)
RVTG . 25 mmHg, % of all (%RVTG) 4 (29) 15* (49*) 13 (50) 19* (48) — 49 (49)
RVTG . 35 mmHg, % of all (%RVTG) 6 (4) 7* (25*) 8 (29) 7* (18*) — 25 (25)
Age (years) 69+10 72+10* 70+10† 76+9 71+10 74+10‖
Men, n (%) 350 (49) 924 (67)* 749 (73) 175 (49) 667 (69) 257 (62)‖
BMI (kg/m2) 30+5 28+6* 28+6 28+6 29+6 27+6‖
IHD, n (%) 228 (32) 793 (58)* 670 (66) 123 (36)† 578 (61) 215 (52)‖
Diabetes, n (%) 104 (14) 260 (19)* 61 (17) 199 (19) 206 (21) 54 (13)‖
Hypertension, n (%) 394 (55) 614 (44)* 411 (40)† 203 (57) 429 (31) 185 (45)
Smoking, n (%) 115 (17) 240 (19) 42 (13) 198 (21)† 173 (19) 67 (16)
Chronic obstructive pulmonary disease . mild, n (%) 449 (67) 745 (57)* 436 (44) 138 (43) 380 (41) 194 (49)‖
NYHA 3–4, n (%) 59 (9) 332 (25)* 266 (26) 66 (21)† 215 (23) 117 (28)‖
6 min walk test (m) 336+129 288+132* 285+126 290+134 297+132 268+133‖
AF, n (%) 6 (1) 329 (24)* 186 (18) 143 (40)† 148 (15) 181 (44)‖
HR (b.p.m.) 69+14 74+19* 74+19 74+19 73+18 76+20‖
Mean BP (mmHg) 105+14 98+16* 104+16 96+16† 98+16 98+17
NT-proBNP, (pg/mL)# 143 (71–215) 1144 (500–2861) 1144 (644–2145) 1156 (429–3218) 858 (429–2145) 2145 (1001–4863)‖
Haemoglobin (g/dL) 13.9+1.4 13.4+1.7* 13.2+1.8 13.4+1.7† 13.5+1.6 13.1+1.8‖
eGFR (mL/min × 1.73 m2) 71+19 60+21* 58+20 60+21 60+21 57.8+20.7‖
RVTG, right ventricle tricuspid gradient (TR peak velocity accurate); PASP, pulmonary artery systolic pressure; IHD, ischaemic heart disease; PS-HF, preserved left ventricle systolic function; LVSD, left ventricle systolic dysfunction; AF, atrialfibrillation and atrial flutter; HR, heart rate; eGFR, glomerular filtration rate.#For the statistic comparison, log NT-proBNP was used, divide by 8.457 to convert to pmol/L.*P , 0.001, no-CHF vs. CHF.†P , 0.05, LVSD vs. PS-HF.‖P , 0.001, CHF with RVTG vs. without RVTG.
Determ
inantsand
prognosticvalue
ofPA
Hin
HF
patients2283
by guest on October 14, 2011 eurheartj.oxfordjournals.org Downloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
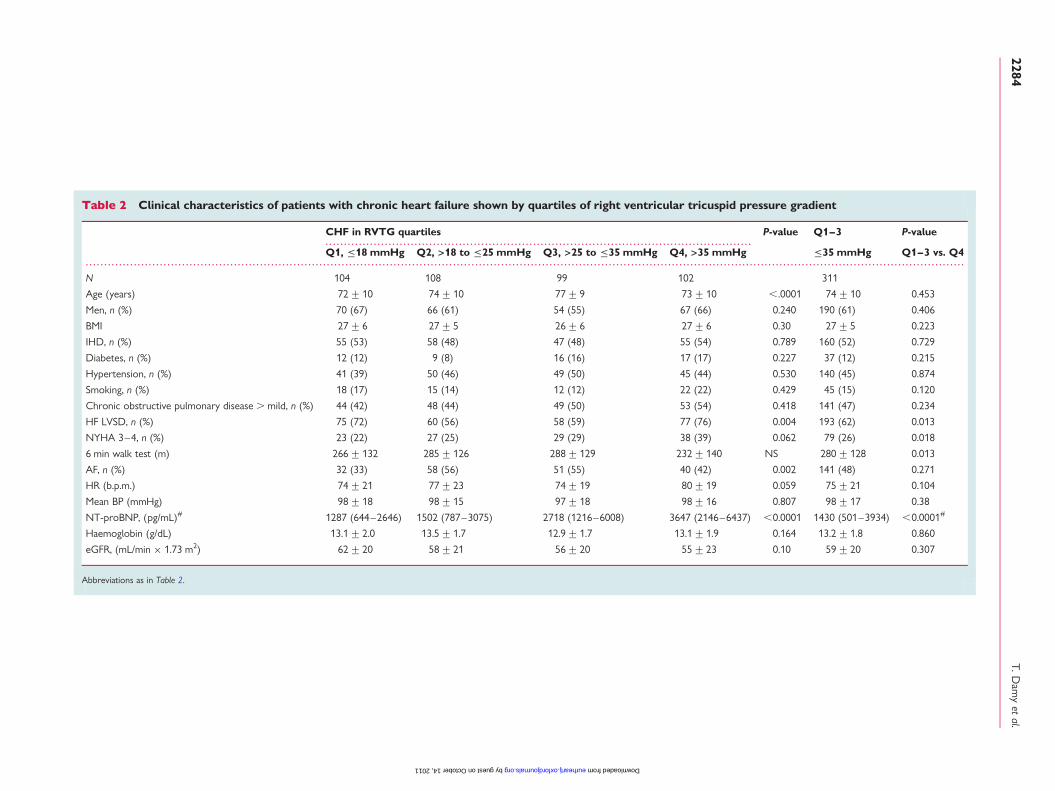
Table 2 Clinical characteristics of patients with chronic heart failure shown by quartiles of right ventricular tricuspid pressure gradient
CHF in RVTG quartiles P-value Q1–3 P-value
Q1, ≤18 mmHg Q2, >18 to ≤25 mmHg Q3, >25 to ≤35 mmHg Q4, >35 mmHg ≤35 mmHg Q1–3 vs. Q4
N 104 108 99 102 311
Age (years) 72+10 74+10 77+9 73+10 ,.0001 74+10 0.453
Men, n (%) 70 (67) 66 (61) 54 (55) 67 (66) 0.240 190 (61) 0.406
BMI 27+6 27+5 26+6 27+6 0.30 27+5 0.223
IHD, n (%) 55 (53) 58 (48) 47 (48) 55 (54) 0.789 160 (52) 0.729
Diabetes, n (%) 12 (12) 9 (8) 16 (16) 17 (17) 0.227 37 (12) 0.215
Hypertension, n (%) 41 (39) 50 (46) 49 (50) 45 (44) 0.530 140 (45) 0.874
Smoking, n (%) 18 (17) 15 (14) 12 (12) 22 (22) 0.429 45 (15) 0.120
Chronic obstructive pulmonary disease . mild, n (%) 44 (42) 48 (44) 49 (50) 53 (54) 0.418 141 (47) 0.234
HF LVSD, n (%) 75 (72) 60 (56) 58 (59) 77 (76) 0.004 193 (62) 0.013
NYHA 3–4, n (%) 23 (22) 27 (25) 29 (29) 38 (39) 0.062 79 (26) 0.018
6 min walk test (m) 266+132 285+126 288+129 232+140 NS 280+128 0.013
AF, n (%) 32 (33) 58 (56) 51 (55) 40 (42) 0.002 141 (48) 0.271
HR (b.p.m.) 74+21 77+23 74+19 80+19 0.059 75+21 0.104
Mean BP (mmHg) 98+18 98+15 97+18 98+16 0.807 98+17 0.38
NT-proBNP, (pg/mL)# 1287 (644–2646) 1502 (787–3075) 2718 (1216–6008) 3647 (2146–6437) ,0.0001 1430 (501–3934) ,0.0001#
Haemoglobin (g/dL) 13.1+2.0 13.5+1.7 12.9+1.7 13.1+1.9 0.164 13.2+1.8 0.860
eGFR, (mL/min × 1.73 m2) 62+20 58+21 56+20 55+23 0.10 59+20 0.307
Abbreviations as in Table 2.
T.Dam
yet
al.2284
by guest on October 14, 2011 eurheartj.oxfordjournals.org Downloaded from
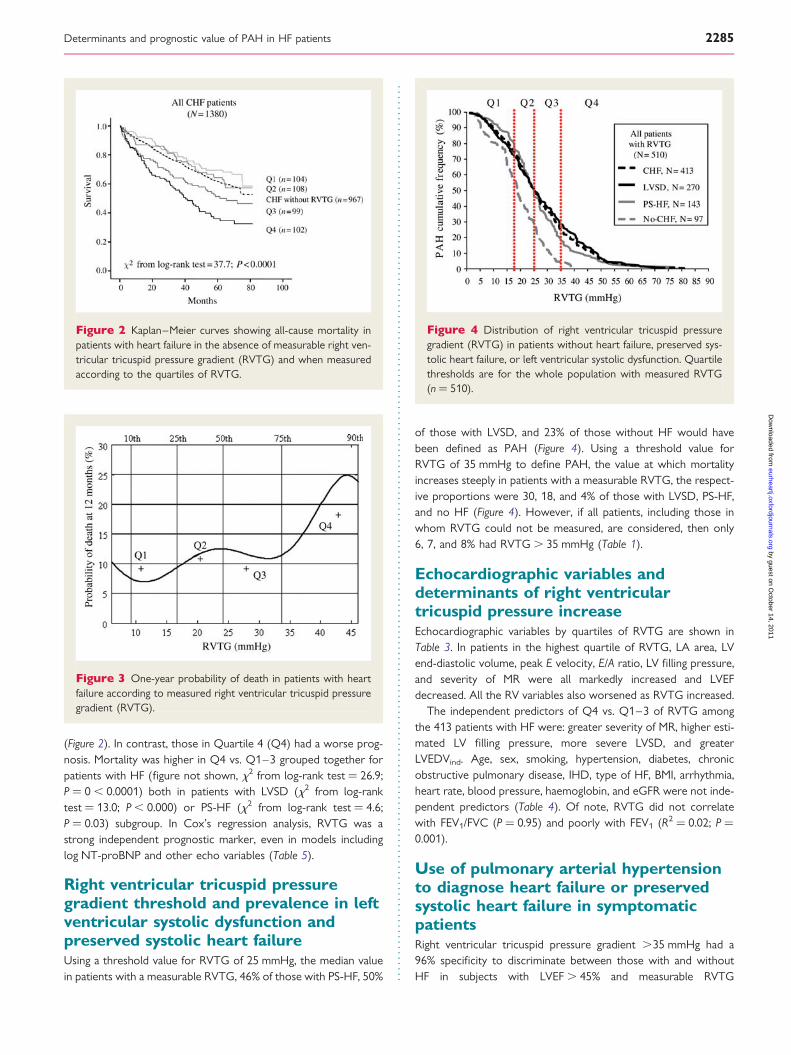
(Figure 2). In contrast, those in Quartile 4 (Q4) had a worse prog-nosis. Mortality was higher in Q4 vs. Q1–3 grouped together forpatients with HF (figure not shown, x2 from log-rank test ¼ 26.9;P ¼ 0 , 0.0001) both in patients with LVSD (x2 from log-ranktest ¼ 13.0; P , 0.000) or PS-HF (x2 from log-rank test ¼ 4.6;P ¼ 0.03) subgroup. In Cox’s regression analysis, RVTG was astrong independent prognostic marker, even in models includinglog NT-proBNP and other echo variables (Table 5).
Right ventricular tricuspid pressuregradient threshold and prevalence in leftventricular systolic dysfunction andpreserved systolic heart failureUsing a threshold value for RVTG of 25 mmHg, the median valuein patients with a measurable RVTG, 46% of those with PS-HF, 50%
of those with LVSD, and 23% of those without HF would havebeen defined as PAH (Figure 4). Using a threshold value forRVTG of 35 mmHg to define PAH, the value at which mortalityincreases steeply in patients with a measurable RVTG, the respect-ive proportions were 30, 18, and 4% of those with LVSD, PS-HF,and no HF (Figure 4). However, if all patients, including those inwhom RVTG could not be measured, are considered, then only6, 7, and 8% had RVTG . 35 mmHg (Table 1).
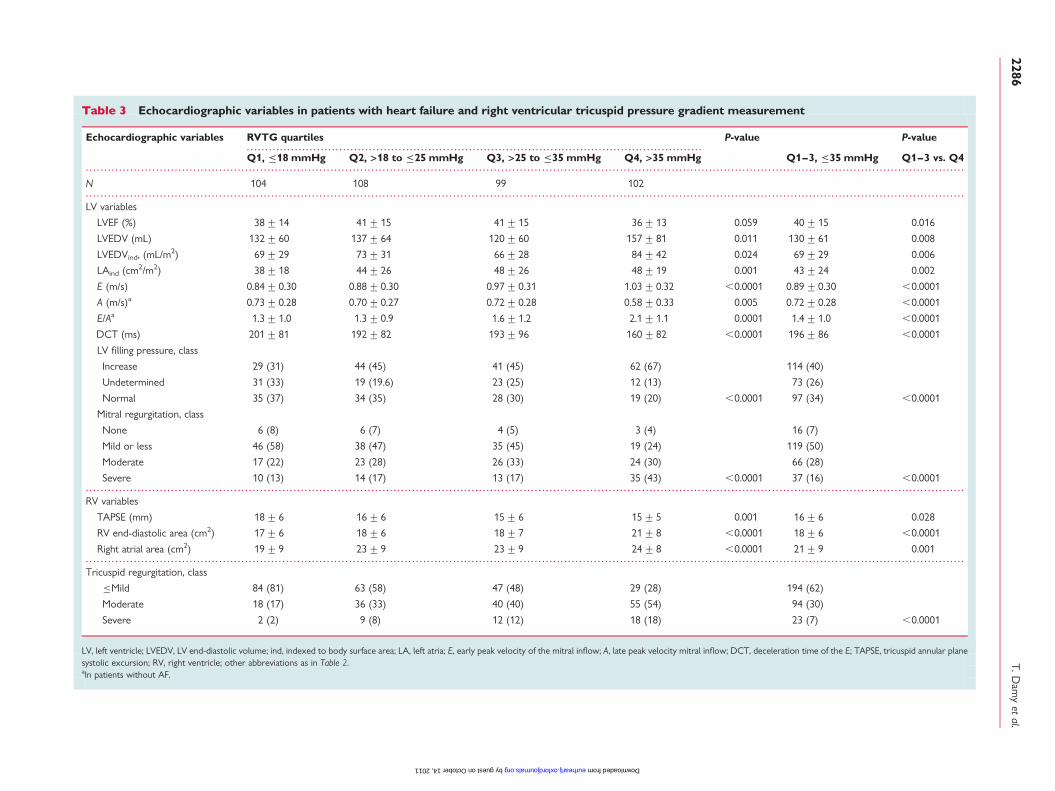
Echocardiographic variables anddeterminants of right ventriculartricuspid pressure increaseEchocardiographic variables by quartiles of RVTG are shown inTable 3. In patients in the highest quartile of RVTG, LA area, LVend-diastolic volume, peak E velocity, E/A ratio, LV filling pressure,and severity of MR were all markedly increased and LVEFdecreased. All the RV variables also worsened as RVTG increased.
The independent predictors of Q4 vs. Q1–3 of RVTG amongthe 413 patients with HF were: greater severity of MR, higher esti-mated LV filling pressure, more severe LVSD, and greaterLVEDVind. Age, sex, smoking, hypertension, diabetes, chronicobstructive pulmonary disease, IHD, type of HF, BMI, arrhythmia,heart rate, blood pressure, haemoglobin, and eGFR were not inde-pendent predictors (Table 4). Of note, RVTG did not correlatewith FEV1/FVC (P ¼ 0.95) and poorly with FEV1 (R2 ¼ 0.02; P ¼0.001).
Use of pulmonary arterial hypertensionto diagnose heart failure or preservedsystolic heart failure in symptomaticpatientsRight ventricular tricuspid pressure gradient .35 mmHg had a96% specificity to discriminate between those with and withoutHF in subjects with LVEF . 45% and measurable RVTG
Figure 2 Kaplan–Meier curves showing all-cause mortality inpatients with heart failure in the absence of measurable right ven-tricular tricuspid pressure gradient (RVTG) and when measuredaccording to the quartiles of RVTG.
Figure 3 One-year probability of death in patients with heartfailure according to measured right ventricular tricuspid pressuregradient (RVTG).
Figure 4 Distribution of right ventricular tricuspid pressuregradient (RVTG) in patients without heart failure, preserved sys-tolic heart failure, or left ventricular systolic dysfunction. Quartilethresholds are for the whole population with measured RVTG(n ¼ 510).
Determinants and prognostic value of PAH in HF patients 2285
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Echocardiographic variables in patients with heart failure and right ventricular tricuspid pressure gradient measurement
Echocardiographic variables RVTG quartiles P-value P-value
Q1, ≤18 mmHg Q2, >18 to ≤25 mmHg Q3, >25 to ≤35 mmHg Q4, >35 mmHg Q1–3, ≤35 mmHg Q1–3 vs. Q4
N 104 108 99 102
LV variables
LVEF (%) 38+14 41+15 41+15 36+13 0.059 40+15 0.016
LVEDV (mL) 132+60 137+64 120+60 157+81 0.011 130+61 0.008
LVEDVind, (mL/m2) 69+29 73+31 66+28 84+42 0.024 69+29 0.006
LAind (cm2/m2) 38+18 44+26 48+26 48+19 0.001 43+24 0.002
E (m/s) 0.84+0.30 0.88+0.30 0.97+0.31 1.03+0.32 ,0.0001 0.89+0.30 ,0.0001
A (m/s)a 0.73+0.28 0.70+0.27 0.72+0.28 0.58+0.33 0.005 0.72+0.28 ,0.0001
E/Aa 1.3+1.0 1.3+0.9 1.6+1.2 2.1+1.1 0.0001 1.4+1.0 ,0.0001
DCT (ms) 201+81 192+82 193+96 160+82 ,0.0001 196+86 ,0.0001
LV filling pressure, class
Increase 29 (31) 44 (45) 41 (45) 62 (67) 114 (40)
Undetermined 31 (33) 19 (19.6) 23 (25) 12 (13) 73 (26)
Normal 35 (37) 34 (35) 28 (30) 19 (20) ,0.0001 97 (34) ,0.0001
Mitral regurgitation, class
None 6 (8) 6 (7) 4 (5) 3 (4) 16 (7)
Mild or less 46 (58) 38 (47) 35 (45) 19 (24) 119 (50)
Moderate 17 (22) 23 (28) 26 (33) 24 (30) 66 (28)
Severe 10 (13) 14 (17) 13 (17) 35 (43) ,0.0001 37 (16) ,0.0001
RV variables
TAPSE (mm) 18+6 16+6 15+6 15+5 0.001 16+6 0.028
RV end-diastolic area (cm2) 17+6 18+6 18+7 21+8 ,0.0001 18+6 ,0.0001
Right atrial area (cm2) 19+9 23+9 23+9 24+8 ,0.0001 21+9 0.001
Tricuspid regurgitation, class
≤Mild 84 (81) 63 (58) 47 (48) 29 (28) 194 (62)
Moderate 18 (17) 36 (33) 40 (40) 55 (54) 94 (30)
Severe 2 (2) 9 (8) 12 (12) 18 (18) 23 (7) ,0.0001
LV, left ventricle; LVEDV, LV end-diastolic volume; ind, indexed to body surface area; LA, left atria; E, early peak velocity of the mitral inflow; A, late peak velocity mitral inflow; DCT, deceleration time of the E; TAPSE, tricuspid annular planesystolic excursion; RV, right ventricle; other abbreviations as in Table 2.aIn patients without AF.
T.Dam
yet
al.2286
by guest on October 14, 2011 eurheartj.oxfordjournals.org Downloaded from

(Figure 4). However, this value identified only 7% of all patientswith PS-HF when patients in whom RVTG could not be measuredwere included (Table 1).
DiscussionIn this analysis, TR could be detected in about 60% of the patientswith and about 36% of those without HF and TRV could bemeasured in 30 and 13%, respectively. This is similar to the rateof RVTG measurement in other studies.4 Tricuspid regurgitationvolume suggesting a PASP of .45 mmHg was rare in patientswithout HF but moderately common in patients with HF. Pulmon-ary hypertension was associated with factors likely to cause raisedpulmonary venous pressure, including the severity of MR, raised LVfilling pressures, LV systolic dysfunction, and LV dilation. AnRVTG . 35 mmHg (�PASP ¼ 45 mmHg) was an independentpredictor of mortality in patients with HF even when adjustedfor age, LV function, and NT-proBNP. Heart failure patientswithout measurable PASP had a prognosis similar to those withlower PA pressures suggesting, as might be expected, thatundetectable TR is rare in patients with PAH and HF.
Determinants of and associations withpulmonary arterial pressurePulmonary arterial pressure is determined by pulmonary vascularresistance (PVR), pulmonary blood flow, and pulmonary venouspressure. Our study suggests that in patients with HF, factorsassociated with increased pulmonary venous pressure are thekey determinants of PAH. Heart failure, MR and LV filling pressurehave previously been shown to be determinants of RVTG in aselected LVSD population.6 We have extended this finding to abroader spectrum of patients with HF. Although, NT-proBNPwas not an independent predictor of PAH in a multivariablemodel, there was a strong association between NT-proBNP andquartile of TRV. Removing either LV filling pressure, MR class, orHF class each allowed NT-proBNP to enter the model, consistentwith the view that these variables are associated with an increase inLA filling pressure and that this is a key determinant of PAH.
Although raised pulmonary venous pressure was the main determi-nant of PAH, this may lead to changes in pulmonary arteriolartone14 and structure.15 In health, there is very little pre-capillarysmooth muscle in the PA circulation but it hypertrophies inpatients with HF. These secondary changes might be importantin protecting the pulmonary capillary circulation from high PApressures and reducing the risk of pulmonary oedema. However,these changes probably cause pulmonary hypertension tobecome relatively fixed, so that the correction of pulmonaryvenous hypertension does not lead to the resolution of PAHand may ultimately lead to a ‘vicious cycle’ whereby PAH gets pro-gressively worse independent of pulmonary venous pressures. Onthe other hand, we did not find airways function, measured byspirometry, to be a determinant of PAH.16 Patients with HF andchronic obstructive pulmonary disease do have a worse prognosis,but this may be mediated through other mechanisms than PAH.17
Patients with PAH had more severe symptoms, reduced exer-cise capacity, and evidence of RV dysfunction. These may well beconsequences rather than causes of PAH. Pulmonary arterialhypertension may limit the rise in pulmonary blood flow duringexercise and impair alveolar–capillary gas exchange,18 thereby lim-iting exercise capacity. Right ventricular dysfunction might beexpected to be associated with reduced cardiac output and pul-monary blood flow. Pulmonary vascular resistance may be under-estimated in these circumstances.
Pulmonary arterial pressureand prognosisWe showed that PAH is a strong predictor of mortality in HF andthat this was independent of another powerful predictor, logNT-pro-BNP, and of echocardiographic variables associated withPA pressure. Few studies have analysed the prognostic value ofPAH in HF4 or, when they have, focused only LVSD or PS-HFpatients.1,5,7 The present study is the first to include such abroad range of variables and patients. Despite a strong associationbetween PAH and RV dysfunction, both were included in the prog-nostic model. Patients with PAH and RV dysfunction had a particu-larly poor prognosis.5 This could reflect intrinsic RV disease that
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Logistic regression studying the determinants of RVTG in patients with heart failure
Binomial logistic regression (Q4vs. Q1–3): clinical,abiological,and echocardiographic variables
Wald’s x2 P-value Category Hazard ratio 95% CI Pair-wisecomparison(P-value)
Mitral regurgitation, class 18.2 0.001 None vs. mild or less 1.67 0.68–4.06 0.26
Moderate vs. mild or less 3.21 0.30–34.4 0.33
Severe vs. mild or less 6.74 2.71–16.74 0.0001
LV filling pressure, class 11.0 0.004 Indeterminate vs. normal 0.65 0.19–2.17 0.48
Increase vs. normal 2.92 1.22–6.94 0.016
LVSD (yes or no) 4.4 0.04 PS-HF vs. LVSD 0.37 0.15–0.94 —
LVEDVind (mL/m2) 3.8 0.05 Per unit 1.01 1.00–1.02 —
Abbreviations as in Table 2.aAll variables in Table 2 except 6 min walk test that was excluded due to a substantial amount of patients unable to complete it.
Determinants and prognostic value of PAH in HF patients 2287
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
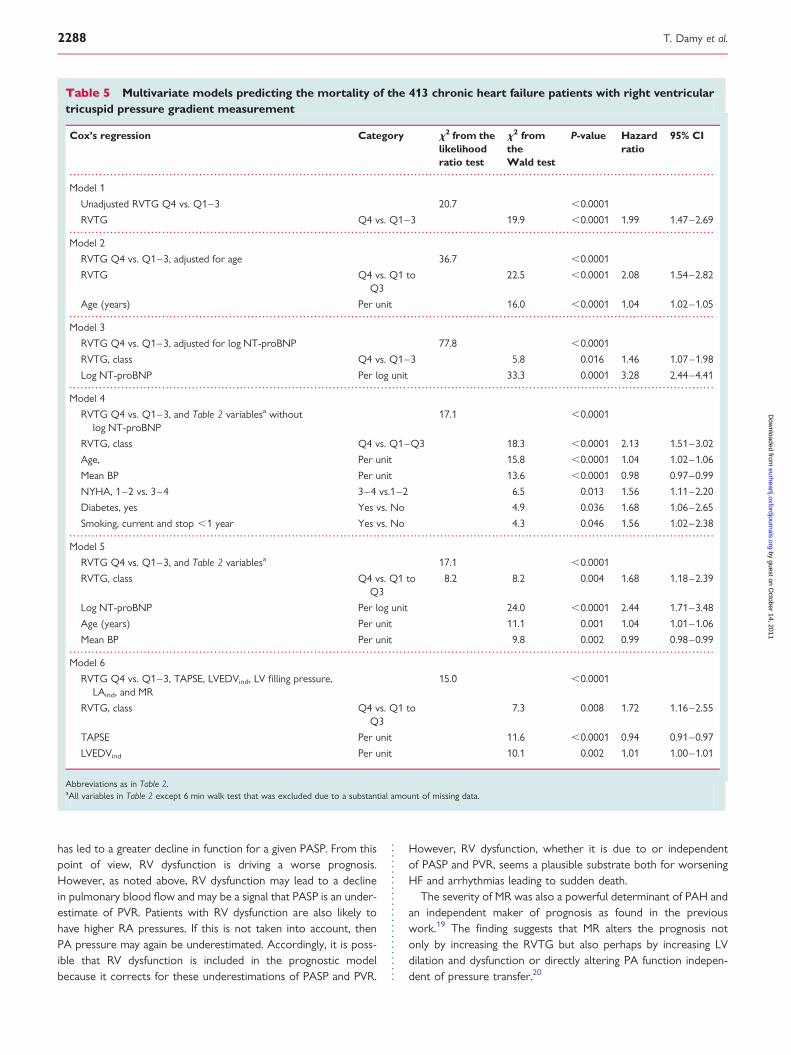
has led to a greater decline in function for a given PASP. From thispoint of view, RV dysfunction is driving a worse prognosis.However, as noted above, RV dysfunction may lead to a declinein pulmonary blood flow and may be a signal that PASP is an under-estimate of PVR. Patients with RV dysfunction are also likely tohave higher RA pressures. If this is not taken into account, thenPA pressure may again be underestimated. Accordingly, it is poss-ible that RV dysfunction is included in the prognostic modelbecause it corrects for these underestimations of PASP and PVR.
However, RV dysfunction, whether it is due to or independentof PASP and PVR, seems a plausible substrate both for worseningHF and arrhythmias leading to sudden death.
The severity of MR was also a powerful determinant of PAH andan independent maker of prognosis as found in the previouswork.19 The finding suggests that MR alters the prognosis notonly by increasing the RVTG but also perhaps by increasing LVdilation and dysfunction or directly altering PA function indepen-dent of pressure transfer.20
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 5 Multivariate models predicting the mortality of the 413 chronic heart failure patients with right ventriculartricuspid pressure gradient measurement
Cox’s regression Category x2 from thelikelihoodratio test
x2 fromtheWald test
P-value Hazardratio
95% CI
Model 1
Unadjusted RVTG Q4 vs. Q1–3 20.7 ,0.0001
RVTG Q4 vs. Q1–3 19.9 ,0.0001 1.99 1.47–2.69
Model 2
RVTG Q4 vs. Q1–3, adjusted for age 36.7 ,0.0001
RVTG Q4 vs. Q1 toQ3
22.5 ,0.0001 2.08 1.54–2.82
Age (years) Per unit 16.0 ,0.0001 1.04 1.02–1.05
Model 3
RVTG Q4 vs. Q1–3, adjusted for log NT-proBNP 77.8 ,0.0001
RVTG, class Q4 vs. Q1–3 5.8 0.016 1.46 1.07–1.98
Log NT-proBNP Per log unit 33.3 0.0001 3.28 2.44–4.41
Model 4
RVTG Q4 vs. Q1–3, and Table 2 variablesa withoutlog NT-proBNP
17.1 ,0.0001
RVTG, class Q4 vs. Q1–Q3 18.3 ,0.0001 2.13 1.51–3.02
Age, Per unit 15.8 ,0.0001 1.04 1.02–1.06
Mean BP Per unit 13.6 ,0.0001 0.98 0.97–0.99
NYHA, 1–2 vs. 3–4 3–4 vs.1–2 6.5 0.013 1.56 1.11–2.20
Diabetes, yes Yes vs. No 4.9 0.036 1.68 1.06–2.65
Smoking, current and stop ,1 year Yes vs. No 4.3 0.046 1.56 1.02–2.38
Model 5
RVTG Q4 vs. Q1–3, and Table 2 variablesa 17.1 ,0.0001
RVTG, class Q4 vs. Q1 toQ3
8.2 8.2 0.004 1.68 1.18–2.39
Log NT-proBNP Per log unit 24.0 ,0.0001 2.44 1.71–3.48
Age (years) Per unit 11.1 0.001 1.04 1.01–1.06
Mean BP Per unit 9.8 0.002 0.99 0.98–0.99
Model 6
RVTG Q4 vs. Q1–3, TAPSE, LVEDVind, LV filling pressure,LAind, and MR
15.0 ,0.0001
RVTG, class Q4 vs. Q1 toQ3
7.3 0.008 1.72 1.16–2.55
TAPSE Per unit 11.6 ,0.0001 0.94 0.91–0.97
LVEDVind Per unit 10.1 0.002 1.01 1.00–1.01
Abbreviations as in Table 2.aAll variables in Table 2 except 6 min walk test that was excluded due to a substantial amount of missing data.
T. Damy et al.2288
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
Using prognosis to define pulmonaryarterial hypertensionAt present, PAH is defined empirically, rather than by the identifi-cation of a ‘prognostic’ threshold. In our study, PASP . 45 mmHgwas a powerful predictor of death. Mild PAH, according to the ESCguidelines, is defined as an RVTG between 31 and 46 mmHg (cor-responding to a PASP of 40–55 mmHg),21 but this may reflect theyoung age of patients on which the recommendation is made.3,22
Pressure arterial systolic pressure increases with age.3 A recentstudy of patients with PS-HF has shown that PASP . 48 mmHgestimated by echocardiography was strongly associated with mor-tality,7 which is consistent with our findings. These data suggestthat the thresholds used to define PAH in HF should be reviewedto align them with the growing body of evidence and to assist indefining populations who may be targets for specific treatmentof PAH.23,24
Pulmonary arterial hypertensionprevalence in heart failure, leftventricular systolic dysfunction andpreserved systolic heart failureThe prevalence of PAH in patients with HF is uncertain. The Euro-Heart Failure Survey reported that 16% of the patients had PAHbut provided no precise diagnostic criteria.25 Our data suggestthat the prevalence of prognostically adverse PAH is not high inthe general population with HF. In our study, 25% of the HFpatients with an RVTG measurement had an estimated PASP .
45 mmHg, but this represented only 7% of the total HF population.The numbers rise to 50% of the patients with an RVTG measure-ment if a lower value for PASP of 35 mmHg is used, which is verysimilar to another study4 in which RVTG measurements werepossible in 38% of the patients with HF, compared with 30% inour population. However, this represents only 14% of theoverall population with HF. In our study, the prevalence ofPASP . 45 mmHg was similar in patients with PS-HF and LVSDwhether or not RVTG could be measured (Table 1). However,RVTG could be measured in a higher proportion of those withPS-HF (40%) compared with LVSD (26%) and therefore a PASPof .45 mmHg was more common in patients with LVSD whenthe analysis was restricted to those in whom RVTG could bemeasured (Table 4). The prevalence of PAH has also beendescribed in two previous studies of PS-HF using a threshold ofPASP of 35 mmHg. Klapholz et al.26 studied 619 patients withPS-HF and reported a prevalence of PAH of 44%, which issimilar to our population. This contrasts with a rate of 83% in astudy of 244 patients with PS-HF.7 Our data show that thethreshold used to define PAH and the method of patient selectionare critically important determinants of prevalence. Selecting onlypatients in whom RVTG can be measured will lead to a severeoverestimation of prevalence.
Pulmonary arterial hypertension may not just be a marker ofmore severe cardiac dysfunction but could also be one of the mech-anisms by which HF progresses and therefore a target for therapy.Studies of endothelin antagonists, agents that appear useful inprimary PAH, have suggested little benefit and possible harm in
patients with HF and LVSD. However, these studies did not targetwhat might be the rather modest proportion of patients with HFand prognostically adverse PAH. A series of studies have investi-gated the effects of phosphodiesterase-V inhibitors in patientswith HF and suggested benefit, especially in patients with PAH.24
Pulmonary arterial hypertension may also be a target for newclasses of agents, such as soluble guanylate cyclase activators.27
LimitationWe defined PS-HF as a clinical diagnosis of HF in patients with anLVEF . 45% and an elevated NT-proBNP. This may not haveexcluded patients with other causes of PAH. The most likely alterna-tive cause for PAH is chronic obstructive pulmonary disease andNT-proBNP may also be elevated in this setting, although levelsare generally not as high as seen in HF.28 However, chronic obstruc-tive pulmonary disease was no more common in patients with PAHthan in other patients with HF. Finally, none of our patients wereassessed for sleep-disordered breathing, which might cause PAHby inducing hypoxia and pulmonary vasoconstriction.29 The lackof measurement of pulmonary blood flow or accurate measure-ments of atrial pressures are a further limitation. The measurementof outflow tract velocities or pulmonary venous flow patterns mayhave improved accuracy but would have excluded many morepatients from the analysis and are not practical in a busy clinicalsetting. We only attempted the measurement of PASP at rest. Inhealth, PVR falls dramatically with exercise and therefore PASPchanges little. In patients with HF, the fall in PVR may be impairedleading to further increases in PASP during exercise. The develop-ment of implantable haemodynamic systems to measure PApressure both at rest and during exercise is of considerable scientificand, potentially, clinical interest.30
ConclusionThe prevalence of PAH in HF is highly dependent on patient selec-tion and the threshold of PASP used. A PASP of .45 mmHg isassociated with a worse prognosis in HF. The prevalence of prog-nostically important PAH may be ,10% and is strongly associatedwith factors that may cause pulmonary venous hypertension.Despite the powerful associations between PAH and other impor-tant determinants of prognosis such as MR, NT-proBNP, and RVand LV dysfunction, PAH remains an important independent pre-dictor of mortality and could be a target for therapy, awaitingappropriately designed, randomized, controlled trials.
Supplementary materialSupplementary material is available at European Heart Journalonline.
FundingT.D. has received a grant from the Societe Francaise de Cardiologieand Federation Francaise de Cardiologie.
Conflict of interest: none declared.
Determinants and prognostic value of PAH in HF patients 2289
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
References1. Abramson SV, Burke JF, Kelly JJ Jr, Kitchen JG, Dougherty MJ, Yih DF,
McGeehin FC, Shuck JW, Phiambolis TP. Pulmonary hypertension predicts mor-tality and morbidity in patients with dilated cardiomyopathy. Ann Intern Med 1992;11:888–895.
2. Badesch D, Champion HC, Gomez Sanchez M, Hoeper M, Loyd J, Manes A,McGoon M, Naeije R, Olschewski H, Oudiz R, Torbicki A. Diagnosis and assess-ment of pulmonary artery hypertension. J Am Coll Cardiol 2009;54(Suppl. 1):S55–S66.
3. McQuillan BM, Picard MH, Leavitt M, Weyman AE. Clinical correlates and refer-ence intervals for pulmonary artery systolic pressure among echocardiographi-cally normal subjects. Circulation 2001;23:2797–2802.
4. Kjaergaard J, Akkan D, Iversen KK, Kjoller E, Kober L, Torp-Pedersen C,Hassager C. Prognostic importance of pulmonary hypertension in patients withheart failure. Am J Cardiol 2007;8:1146–1150.
5. Ghio S, Gavazzi A, Campana C, Inserra C, Klersy C, Sebastiani R, Arbustini E,Recusani F, Tavazzi L. Independent and additive prognostic value of right ventri-cular systolic function and pulmonary artery pressure in patients with chronicheart failure. J Am Coll Cardiol 2001;1:183–188.
6. Enriquez-Sarano M, Rossi A, Seward JB, Bailey KR, Tajik AJ. Determinants of pul-monary hypertension in left ventricular dysfunction. J Am Coll Cardiol 1997;1:153–159.
7. Lam CS, Roger VL, Rodeheffer RJ, Borlaug BA, Enders FT, Redfield MM. Pulmon-ary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol 2009;13:1119–1126.
8. Gold Global initiative for Chronic Obstructive Lung Disease. Global strategy forthe diagnosis, management, and prevention of chronic obstructive pulmonarydisease: NHLB/WHO workshop report 2006. http://www.goldcopd.com/. 2006.
9. British Society of Echocardiography. Guidelines and statements. www.bsecho.org.10. Yock PG, Popp RL. Noninvasive estimation of right ventricular systolic pressure
by Doppler ultrasound in patients with tricuspid regurgitation. Circulation 1984;4:657–662.
11. Currie PJ, Seward JB, Chan KL, Fyfe DA, Hagler DJ, Mair DD, Reeder GS,Nishimura RA, Tajik AJ. Continuous wave Doppler determination of right ventri-cular pressure: a simultaneous Doppler-catheterization study in 127 patients. J AmColl Cardiol 1985;4:750–756.
12. Brennan JM, Blair JE, Goonewardena S, Ronan A, Shah D, Vasaiwala S,Kirkpatrick JN, Spencer KT. Reappraisal of the use of inferior vena cava for esti-mating right atrial pressure. J Am Soc Echocardiogr 2007;7:857–861.
13. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA,Waggoner AD, Flachskampf FA, Pellikka PA, Evangelisa A. Recommendationsfor the evaluation of left ventricular diastolic function by echocardiography. EurJ Echocardiogr 2009;2:165–193.
14. Habib F, Dutka D, Crossman D, Oakley CM, Cleland JG. Enhanced basal nitricoxide production in heart failure: another failed counter-regulatory vasodilatormechanism? Lancet 1994;344:371–373.
15. Delgado JF, Conde E, Sanchez V, Lopez-Rios F, Gomez-Sanchez MA, Escribano P,Sotelo T, Gomez de la Camara A, Cortina J, de la Calzada CS. Pulmonary vascularremodeling in pulmonary hypertension due to chronic heart failure. Eur J HeartFail 2005;6:1011–1016.
16. Hoeper M, Barbera J, Channick R, Hassoun PM, Lang I, Manes A, Martinez F,Naeije R, Olschewski H, Pepke-Zaba J, Redfield MM, Robbins I, Souza R,Torbicki A, McGoon M. Diagnosis, assessment, and treatment of non-pulmonaryarterial hypertension pulmonary hypertension. J Am Coll Cardiol 2009;54:S85–S96.
17. Mascarenhas J, Lourenco P, Lopes R, Azevedo A, Bettencourt P. Chronic obstruc-tive pulmonary disease in heart failure. Prevalence, therapeutic and prognosticimplications. Am Heart J 2008;3:521–525.
18. Puri S, Baker BL, Dutka DP, Oakley CM, Hughes JM, Cleland JG. Reducedalveolar-capillary membrane diffusing capacity in chronic heart failure. Its patho-physiological relevance and relationship to exercise performance. Circulation1995;11:2769–2774.
19. Trichon B, Fleker G, Shaw L, Cabell C, O’Connor C. Relation of frequency andseverity of mitral regurgitation to survival among patients with left ventricular sys-tolic dysfunction and heart failure. Am J Cardiol 2003;5:538–543.
20. MacIsaac AI, McDonald IG, Kirsner RL, Graham SA, Tanzer D. Left ventricularenergy in mitral regurgitation: a preliminary report. Aust N Z J Med 1992;22(Suppl. 5):532–540.
21. Galie N, Torbicki A, Barst R, Dartevelle P, Haworth S, Higenbottam T,Olschewski H, Peacock A, Pietra G, Rubin LJ, Simonneau G, Priori SG,Garcia MA, Blanc JJ, Budaj A, Cowie M, Dean V, Deckers J, Burgos EF,Lekakis J, Lindahl B, Mazzotta G, McGregor K, Morais J, Oto A, Smiseth OA,Barbera JA, Gibbs S, Hoeper M, Humbert M, Naeije R, Pepke-Zaba J. Guidelineson diagnosis and treatment of pulmonary arterial hypertension. The Task Forceon Diagnosis and Treatment of Pulmonary Arterial Hypertension of the EuropeanSociety of Cardiology. Eur Heart J 2004;24:2243–2278.
22. Aessopos A, Farmakis D, Taktikou H, Loukopoulos D. Doppler-determined peaksystolic tricuspid pressure gradient in persons with normal pulmonary functionand tricuspid regurgitation. J Am Soc Echocardiogr 2000;7:645–649.
23. Lewis GD, Semigran MJ. The emerging role for type 5 phosphodiesterase inhi-bition in heart failure. Curr Heart Fail Rep 2006;3:123–128.
24. Lewis GD, Shah R, Shahzad K, Camuso JM, Pappagianopoulos PP, Hung J,Tawakol A, Gerszten RE, Systrom DM, Bloch KD, Semigran MJ. Sildenafilimproves exercise capacity and quality of life in patients with systolic heartfailure and secondary pulmonary hypertension. Circulation 2007;14:1555–1562.
25. Cleland JG, Swedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, Dietz R,Gavazzi A, Hobbs R, Korewicki J, Madeira HC, Moiseyev VS, Preda I, vanGilst WH, Widimsky J, Freemantle N, Eastaugh J, Mason J. The EuroHeartFailure survey programme—a survey on the quality of care among patientswith heart failure in Europe. Part 1: patient characteristics and diagnosis. EurHeart J 2003;5:442–463.
26. Klapholz M, Maurer M, Lowe AM, Messineo F, Meisner JS, Mitchell J, Kalman J,Phillips RA, Steingart R, Brown EJ Jr, Berkowitz R, Moskowitz R, Soni A,Mancini D, Bijou R, Sehhat K, Varshneya N, Kukin M, Katz SD, Sleeper LA, LeJemtel TH. Hospitalization for heart failure in the presence of a normal left ven-tricular ejection fraction: results of the New York Heart Failure Registry. J Am CollCardiol 2004;8:1432–1438.
27. Evgenov OV, Ichinose F, Evgenov NV, Gnoth MJ, Falkowski GE, Chang Y,Bloch KD, Zapol WM. Soluble guanylate cyclase activator reverses acute pulmon-ary hypertension and augments the pulmonary vasodilator response to inhalednitric oxide in awake lambs. Circulation 2004;15:2253–2259.
28. McCullough PA, Hollander JE, Nowak RM, Storrow AB, Duc P, Omland T,McCord J, Herrmann HC, Steg PG, Westheim A, Knudsen CW, Abraham WT,Lamba S, Wu AH, Perez A, Clopton P, Krishnaswamy P, Kazanegra R,Maisel AS. Uncovering heart failure in patients with a history of pulmonarydisease: rationale for the early use of B-type natriuretic peptide in the emergencydepartment. Acad Emerg Med 2003;3:198–204.
29. Atwood CW Jr, McCrory D, Garcia JG, Abman SH, Ahearn GS. Pulmonary arteryhypertension and sleep-disordered breathing: ACCP evidence-based clinical prac-tice guidelines. Chest 2004;126(Suppl. 1):72S–77S.
30. Zile MR, Bennet TD, Sutton MS, Cho YK, Adamson PB, Aranda A, Abraham WT,Smart FW, Stevenson LW, Kueffer FJ, Bourge RC. Transition from chronic com-pensated to acute decompensated heart failure: pathophysiological insightsobtained from continuous monitoring of intracardiac pressures. Circulation 2008;118:1433–1441.
T. Damy et al.2290
by guest on October 14, 2011
eurheartj.oxfordjournals.orgD
ownloaded from
Related Documents











