Detection of BRAF p.V600E Mutations in Melanomas Comparison of Four Methods Argues for Sequential Use of Immunohistochemistry and Pyrosequencing Emeline Colomba,* Zofia Hélias-Rodzewicz,* y Andreas Von Deimling, zx Cristi Marin,* y Nathalie Terrones, y Dominique Pechaud, y Sylvie Surel, y Jean-François Côté,* y Frédérique Peschaud,* x David Capper, zx Hélène Blons, {k Ute Zimmermann, y Thierry Clerici, y Philippe Saiag,** yy and Jean-François Emile* y From EA4340* and EA4339, yy University of Versailles, Boulogne, France; the Departments of Pathology, y Surgery, { and Dermatology,** Ambroise Paré Hospital, APHP, Boulogne, France; the Department of Neuropathology, z Ruprecht-Karls-University Heidelberg, Heidelberg, Germany; the Clinical Cooperation Unit Neuropathology, x German Cancer Research Center, Heidelberg, Germany; and UMR-S775, k INSERM, Paris, France Accepted for publication September 13, 2012. Address correspondence to Jean-François Emile, M.D., Ph.D., Pathology Department, Ambroise Paré Hospital, 9 Av. Charles de Gaulle, F-92104 Boulogne, France. E-mail: jean- [email protected]. BRAF p.V600 mutation detection recently became necessary to treat metastatic melanoma patients with vemurafenib. This study compares different methods of detection of BRAF mutations. Melanoma samples from 111 patients were analyzed for BRAF mutations, and for 89 of them, results were obtained with the four following methods: Sanger sequencing, real-time PCR, immunohistochemistry, and pyrosequencing. All samples contained at least 60% of tumor cells. Directional Sanger sequencing of PCR products failed to detect 3 of 40 p.V600E-mutated cases (7.5%) (sensitivity, 92.5%; 95% CI, 78.5% to 98.0%). BRAF p.V600E-specific real-time PCR identified 39 of 40 p.V600E-mutated cases (97.6%) (sensitivity, 97.5%; 95% CI, 87.1% to 99.6%) and all 39 wild-type (WT) cases and surprisingly was also positive for 6/6 p.V600K (specificity, 87.8%; 95% CI, 75.8% to 94.3%). However, other mutations, p.V600R (n Z 1), p.K601E (n Z 2), and p.600_601delinsE (n Z 1), were not detected. Immunohistochemistry with VE1, specific for p.V600E, identified all p.V600E and WT cases (sensitivity, 100%; 95% CI, 91.2% to 100%) but was negative for all other BRAF mutations. Pyrosequencing successfully identified all WT and mutated cases. Immu- nohistochemistry is highly specific for p.V600E, and could be used as a first-line method, as is currently performed for HER2 amplification detection. Pyrosequencing proved to be the most efficient method to detect BRAF mutations in melanomas and could be performed on VE1-negative or uninterpretable cases. (J Mol Diagn 2013, 15: 94e100; http://dx.doi.org/10.1016/j.jmoldx.2012.09.001) Detection of BRAF p.V600 mutations has recently become mandatory to treat patients with advanced or metastatic melanomas. Indeed, treatment of these patients with vemurafenib was been found to improve survival in a phase 3 clinical trial, 1 and US and European regulation agencies approved its use in clinical daily practice. An objective response was observed in approximately 50% of patients, and overall survival and progression-free survival are significantly increased. 1,2 BRAF mutations were found in 7% of human cancers. 3 They are rare in some tumors, such as myeloma (4%), 4 and are present in 100% of hairy cell leukemia. 5 In mela- noma, the frequency of BRAF mutations is 40% to 50% 6 and depends on the type of melanoma and on exposure to the sun. 7,8 Several methods have been used to detect BRAF Supported by grants from the nonprofit associations Ligue contre le Cancer, AREP (Association Pour la Recherche de l’Enseignement en Patho- logie), and AROLD (Association Pour la Recherche en Oncologie Digestive). Disclosures: J.F.E. and P.S. received honoraria for counseling on diagnosis and/or treatment of patients with melanomas from Roche and Glaxo Smith Kline. D.C. and A.V.D. applied for a patent on the diagnostic use of BRAF p.V600E mutantespecific antibody VE1. All terms are being managed by the German Cancer Research Center in accordance with its conflict of interest policies. Funding sources had no involvement in study design, data collection, data analysis, data interpretation, writing of the manuscript, approval of the manuscript, or the decision to submit the manuscript for publication. No one has been paid to write this article by a pharmaceutical company or other agency. Copyright ª 2013 American Society for Investigative Pathology and the Association for Molecular Pathology. Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jmoldx.2012.09.001 jmd.amjpathol.org The Journal of Molecular Diagnostics, Vol. 15, No. 1, January 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Journal of Molecular Diagnostics, Vol. 15, No. 1, January 2013
jmd.amjpathol.org
Detection of BRAF p.V600E Mutations in Melanomas
Comparison of Four Methods Argues for Sequential Use ofImmunohistochemistry and PyrosequencingEmeline Colomba,* Zofia Hélias-Rodzewicz,*y Andreas Von Deimling,zx Cristi Marin,*y Nathalie Terrones,y Dominique Pechaud,y
Sylvie Surel,y Jean-François Côté,*y Frédérique Peschaud,*x David Capper,zx Hélène Blons,{k Ute Zimmermann,y Thierry Clerici,y
Philippe Saiag,**yy and Jean-François Emile*y
From EA4340* and EA4339,yy University of Versailles, Boulogne, France; the Departments of Pathology,y Surgery,{ and Dermatology,** Ambroise ParéHospital, APHP, Boulogne, France; the Department of Neuropathology,z Ruprecht-Karls-University Heidelberg, Heidelberg, Germany; the ClinicalCooperation Unit Neuropathology,x German Cancer Research Center, Heidelberg, Germany; and UMR-S775,k INSERM, Paris, France
Accepted for publicationSeptember 13, 2012.
C
a
P
h
Address correspondence toJean-François Emile, M.D.,Ph.D., Pathology Department,Ambroise Paré Hospital, 9Av. Charles de Gaulle, F-92104Boulogne, France. E-mail: [email protected].
opyright ª 2013 American Society for Inve
nd the Association for Molecular Pathology.
ublished by Elsevier Inc. All rights reserved
ttp://dx.doi.org/10.1016/j.jmoldx.2012.09.001
BRAF p.V600 mutation detection recently became necessary to treat metastatic melanoma patients withvemurafenib. This study compares different methods of detection of BRAF mutations. Melanoma samplesfrom 111 patients were analyzed for BRAF mutations, and for 89 of them, results were obtained with thefour following methods: Sanger sequencing, real-time PCR, immunohistochemistry, and pyrosequencing.All samples contained at least 60% of tumor cells. Directional Sanger sequencing of PCR products failed todetect 3 of 40 p.V600E-mutated cases (7.5%) (sensitivity, 92.5%; 95% CI, 78.5% to 98.0%). BRAFp.V600E-specific real-time PCR identified 39 of 40 p.V600E-mutated cases (97.6%) (sensitivity, 97.5%;95%CI, 87.1% to 99.6%) and all 39wild-type (WT) cases and surprisingly was also positive for 6/6 p.V600K(specificity, 87.8%; 95% CI, 75.8% to 94.3%). However, other mutations, p.V600R (nZ 1), p.K601E (nZ2), and p.600_601delinsE (n Z 1), were not detected. Immunohistochemistry with VE1, specific forp.V600E, identified all p.V600E andWT cases (sensitivity, 100%; 95%CI, 91.2% to 100%) but was negativefor all other BRAF mutations. Pyrosequencing successfully identified all WT and mutated cases. Immu-nohistochemistry is highly specific for p.V600E, and could be used as a first-line method, as is currentlyperformed for HER2 amplification detection. Pyrosequencing proved to be the most efficient method todetect BRAF mutations in melanomas and could be performed on VE1-negative or uninterpretable cases.(J Mol Diagn 2013, 15: 94e100; http://dx.doi.org/10.1016/j.jmoldx.2012.09.001)
Supported by grants from the nonprofit associations Ligue contre leCancer, AREP (Association Pour la Recherche de l’Enseignement en Patho-logie), and AROLD (Association Pour la Recherche en Oncologie Digestive).Disclosures: J.F.E. and P.S. received honoraria for counseling on diagnosis
and/or treatment of patients with melanomas from Roche and Glaxo SmithKline. D.C. and A.V.D. applied for a patent on the diagnostic use of BRAFp.V600E mutantespecific antibody VE1. All terms are being managed by theGerman Cancer Research Center in accordance with its conflict of interestpolicies. Funding sources had no involvement in study design, data collection,data analysis, data interpretation, writing of the manuscript, approval of themanuscript, or thedecision to submit themanuscript for publication.Noone hasbeen paid to write this article by a pharmaceutical company or other agency.
Detection of BRAF p.V600 mutations has recently becomemandatory to treat patients with advanced or metastaticmelanomas. Indeed, treatment of these patients withvemurafenib was been found to improve survival in a phase3 clinical trial,1 and US and European regulation agenciesapproved its use in clinical daily practice. An objectiveresponse was observed in approximately 50% of patients,and overall survival and progression-free survival aresignificantly increased.1,2
BRAF mutations were found in 7% of human cancers.3
They are rare in some tumors, such as myeloma (4%),4
and are present in 100% of hairy cell leukemia.5 In mela-noma, the frequency of BRAF mutations is 40% to 50%6
stigative Pathology
.
and depends on the type of melanoma and on exposure tothe sun.7,8 Several methods have been used to detect BRAF

Table 1 Sequences of Oligonucleotides
Method Oligonucleotide DNA sequence Size of PCR products, bp
Sanger sequencing BRAF_15.1 fransen 50-TGCTTGCTCTGATAGGAAAATG-30 82BRAF_15.2 fransen 50-AGCATCTCAGGGCCAAAAAT-30
Real-time PCR Primer U 50-CTACTGTTTTCCTTTACTTACTACACCTCAGA-30 136Primer L 50-ATCCAGACAACTGTTCAAACTGATG-30
Probe VIC 50-CTAGCTACAGTGAAATC-30
Probe FAM 50-TAGCTACAGAGAAATC-30
PNA blocker 50-CCATCGAGATTTCACTG-30
Pyrosequencing Braf_Forward 50-TCATGAAGACCTCACAGTAAAAA-30 228Braf_Rbiotine biotine-50-TTCAAACTGATGGGACCCACT-30
Braf_Seq 50-GGTGATTTTGGTCTAGCT-30
Detection of BRAF Mutations in Melanoma
mutations: Sanger sequencing, mismatch ligation assay,ligase detection reaction, denaturating high-performanceliquid chromatography, SNAPshot, high-resolution melting,mutation-specific real-time PCR, pyrosequencing, and massspectrometry.9e14 Each method has its own sensitivity,specificity, cost, and response delay. Recently, detection ofBRAF p.V600E mutation by immunohistochemistry (IHC)with VE1 antibody was found to be possible in braintumors15 and thyroid carcinomas.16
Although BRAF p.V600 mutations have a major clinicaleffect, only a few studies aimed to compare the methods fordetection of these mutations.14,17e20 Furthermore, recentdata indicate that Sanger sequencing failed to detect BRAFmutations in melanomas18 and therefore should no longer beconsidered as the reference test. Thus, we aimed to comparethe different methods for the detection of BRAF mutations inmelanomas to determine which method or combination ofmethods should be used in diagnostic daily practice.
Materials and Methods
Patients
Cases were identified from the files of the Department ofPathology of Ambroise Paré Hospital (Assistance PubliqueHôpitaux de Paris, Boulogne, France). All samples repre-sented either regional lymph node metastases or in-transitcutaneous or subcutaneous metastases identified betweenJanuary 2000 and May 2011. BRAF mutation detection wasperformed for treatment with either BRAF or MEK inhibi-tors for patients who were still alive. The ethics committeeCPP IdF 8 allowed performing BRAF mutation detection ontumor samples of dead patients (number 12 01 08, DC2009-933). Melanoma diagnosis was confirmed by histo-logic review of all samples by at least two pathologists(C.M., U.Z., T.C., J.F.E.).
Immunochemistry with the BRAF p.V600E-SpecificAntibody VE1
Immunostaining was performed on TMAs after controllingthe homogeneity of staining on whole slides of 10samples. For each tumor, three cores of 0.6 mm diameterwere available for analysis. Staining was performed within
The Journal of Molecular Diagnostics - jmd.amjpathol.org
2 weeks after cutting the 4-mm sections. The primarymouse monoclonal antibody VE1 has previously beendemonstrated to be highly specific for p.V600E mutatedprotein.15 Immunostaining was performed using Bond-Max Fr4.0 (Leica Biosystem, Newcastle, UK). Antigenretrieval was performed during 60 mn at 96�C in pH 9buffer Bond Epitope Retrival Solution 2 (Leica Bio-system). VE1 hybridoma supernatant was diluted 1/3 andincubated at 37�C for 32 minutes. Staining was revealedwith a Bond polymer refine red detection kit (Leica Bio-system). The best staining conditions were determined ona sample of eight melanomas with known BRAF muta-tional status (not shown). Staining was scored as negative,positive, or not available, according to previously pub-lished criteria,15 by a pathologist (J.F.E.) who was maskedto all genetic results.
Molecular Pathology
Tumor DNA was extracted from formalin-fixed, paraffin-embedded tissues. Four serial sections were performed foreach sample. The first (4 mm thick) was stained with H&Efor histologic control and selection of the areas with thehighest density of melanoma cells, and three others (20 mmthick) were used for dissection at �10 magnification. Eachsample analyzed contained at least 60% tumor cells. TumorDNA was extracted by proteinase K digestion (6 ng/mL at55�C for 18 to 72 hours under continuous stirring) anda QIAamp DNA minikit (Qiagen, Les Ulis, France). BRAFcDNA sequence GenBank NM_004333.4 was used asreference. Sequences of oligonucleotide primers and Taq-man probes are given in Table 1.
Direct Sanger sequencing on both strands of PCR prod-ucts was performed using a Prism Model 3700 CapillaryArray Sequencer and Big Dye Terminator Chemistry(Applied Biosystems, Foster City, CA).
Real-time PCR was performed as previously described.21
Tumor DNA was used at concentrations of 25 ng/mL. PCRwas performed in Applied Prism 7900 HT (Applied Bio-systems), with Taqman probes specific for wild-type (WT)and BRAF p.V600E alleles. Each sample was analyzed induplicate to detect all BRAF alleles present in the tumor, andin two other duplicates, the WT amplification was inhibited
95
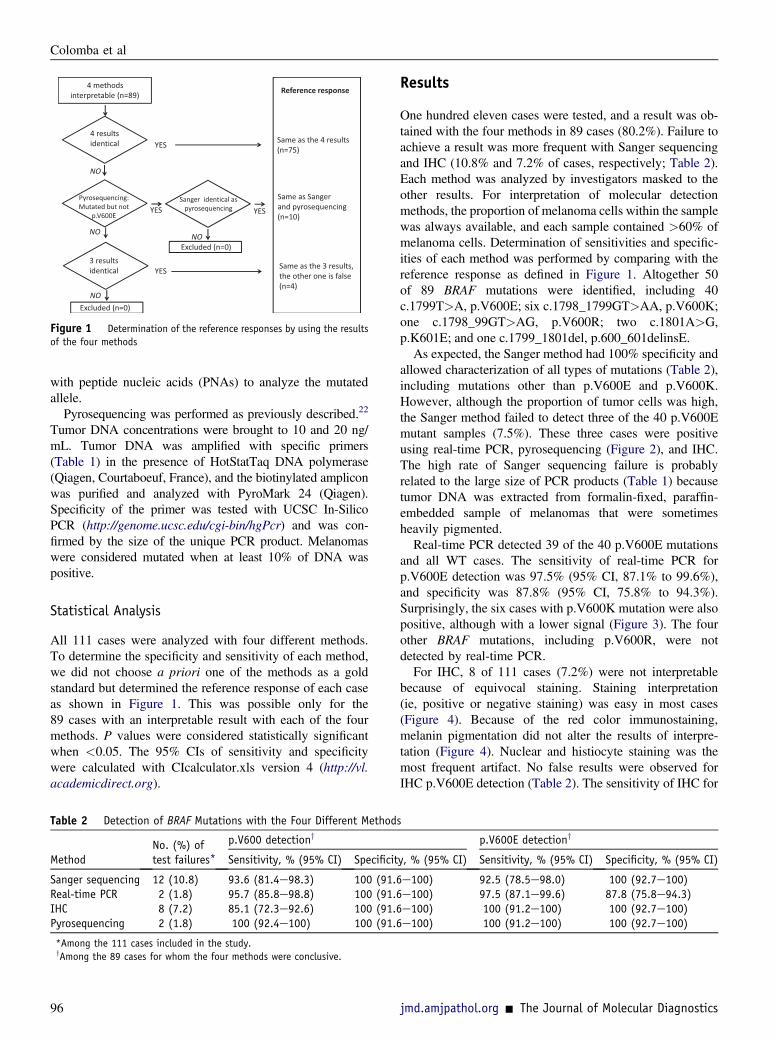
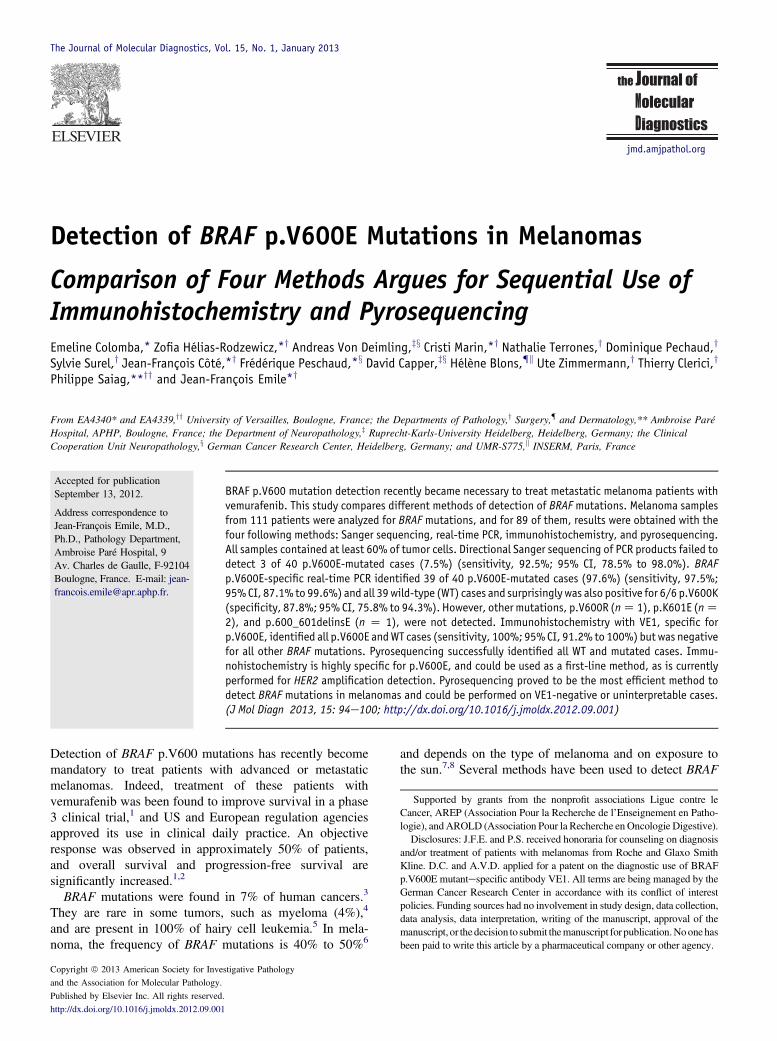
Figure 1 Determination of the reference responses by using the resultsof the four methods
Colomba et al
with peptide nucleic acids (PNAs) to analyze the mutatedallele.
Pyrosequencing was performed as previously described.22
Tumor DNA concentrations were brought to 10 and 20 ng/mL. Tumor DNA was amplified with specific primers(Table 1) in the presence of HotStatTaq DNA polymerase(Qiagen, Courtaboeuf, France), and the biotinylated ampliconwas purified and analyzed with PyroMark 24 (Qiagen).Specificity of the primer was tested with UCSC In-SilicoPCR (http://genome.ucsc.edu/cgi-bin/hgPcr) and was con-firmed by the size of the unique PCR product. Melanomaswere considered mutated when at least 10% of DNA waspositive.
Statistical Analysis
All 111 cases were analyzed with four different methods.To determine the specificity and sensitivity of each method,we did not choose a priori one of the methods as a goldstandard but determined the reference response of each caseas shown in Figure 1. This was possible only for the89 cases with an interpretable result with each of the fourmethods. P values were considered statistically significantwhen <0.05. The 95% CIs of sensitivity and specificitywere calculated with CIcalculator.xls version 4 (http://vl.academicdirect.org).
Table 2 Detection of BRAF Mutations with the Four Different Method
MethodNo. (%) oftest failures*
p.V600 detectiony
Sensitivity, % (95% CI) Specificit
Sanger sequencing 12 (10.8) 93.6 (81.4e98.3) 100 (91.6Real-time PCR 2 (1.8) 95.7 (85.8e98.8) 100 (91.6IHC 8 (7.2) 85.1 (72.3e92.6) 100 (91.6Pyrosequencing 2 (1.8) 100 (92.4e100) 100 (91.6
*Among the 111 cases included in the study.yAmong the 89 cases for whom the four methods were conclusive.
96
Results
One hundred eleven cases were tested, and a result was ob-tained with the four methods in 89 cases (80.2%). Failure toachieve a result was more frequent with Sanger sequencingand IHC (10.8% and 7.2% of cases, respectively; Table 2).Each method was analyzed by investigators masked to theother results. For interpretation of molecular detectionmethods, the proportion of melanoma cells within the samplewas always available, and each sample contained >60% ofmelanoma cells. Determination of sensitivities and specific-ities of each method was performed by comparing with thereference response as defined in Figure 1. Altogether 50of 89 BRAF mutations were identified, including 40c.1799T>A, p.V600E; six c.1798_1799GT>AA, p.V600K;one c.1798_99GT>AG, p.V600R; two c.1801A>G,p.K601E; and one c.1799_1801del, p.600_601delinsE.As expected, the Sanger method had 100% specificity and
allowed characterization of all types of mutations (Table 2),including mutations other than p.V600E and p.V600K.However, although the proportion of tumor cells was high,the Sanger method failed to detect three of the 40 p.V600Emutant samples (7.5%). These three cases were positiveusing real-time PCR, pyrosequencing (Figure 2), and IHC.The high rate of Sanger sequencing failure is probablyrelated to the large size of PCR products (Table 1) becausetumor DNA was extracted from formalin-fixed, paraffin-embedded sample of melanomas that were sometimesheavily pigmented.Real-time PCR detected 39 of the 40 p.V600E mutations
and all WT cases. The sensitivity of real-time PCR forp.V600E detection was 97.5% (95% CI, 87.1% to 99.6%),and specificity was 87.8% (95% CI, 75.8% to 94.3%).Surprisingly, the six cases with p.V600K mutation were alsopositive, although with a lower signal (Figure 3). The fourother BRAF mutations, including p.V600R, were notdetected by real-time PCR.For IHC, 8 of 111 cases (7.2%) were not interpretable
because of equivocal staining. Staining interpretation(ie, positive or negative staining) was easy in most cases(Figure 4). Because of the red color immunostaining,melanin pigmentation did not alter the results of interpre-tation (Figure 4). Nuclear and histiocyte staining was themost frequent artifact. No false results were observed forIHC p.V600E detection (Table 2). The sensitivity of IHC for
s
p.V600E detectiony
y, % (95% CI) Sensitivity, % (95% CI) Specificity, % (95% CI)
e100) 92.5 (78.5e98.0) 100 (92.7e100)e100) 97.5 (87.1e99.6) 87.8 (75.8e94.3)e100) 100 (91.2e100) 100 (92.7e100)e100) 100 (91.2e100) 100 (92.7e100)
jmd.amjpathol.org - The Journal of Molecular Diagnostics
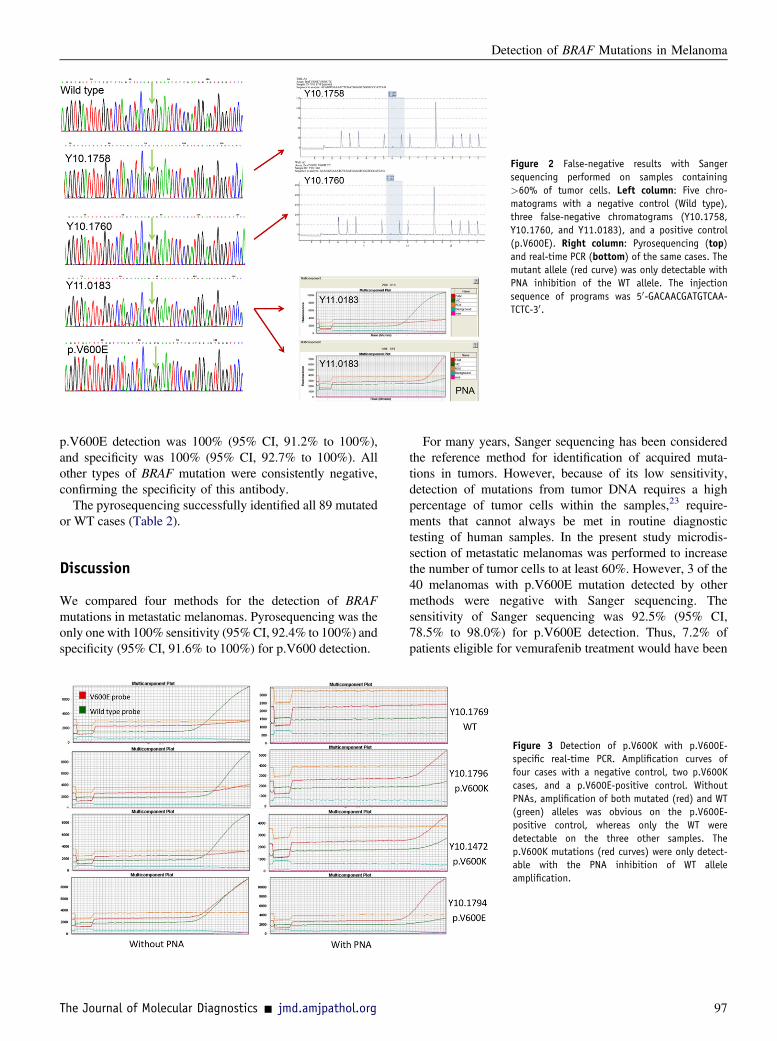
Figure 2 False-negative results with Sangersequencing performed on samples containing>60% of tumor cells. Left column: Five chro-matograms with a negative control (Wild type),three false-negative chromatograms (Y10.1758,Y10.1760, and Y11.0183), and a positive control(p.V600E). Right column: Pyrosequencing (top)and real-time PCR (bottom) of the same cases. Themutant allele (red curve) was only detectable withPNA inhibition of the WT allele. The injectionsequence of programs was 50-GACAACGATGTCAA-TCTC-30.
Detection of BRAF Mutations in Melanoma
p.V600E detection was 100% (95% CI, 91.2% to 100%),and specificity was 100% (95% CI, 92.7% to 100%). Allother types of BRAF mutation were consistently negative,confirming the specificity of this antibody.
The pyrosequencing successfully identified all 89 mutatedor WT cases (Table 2).
Discussion
We compared four methods for the detection of BRAFmutations in metastatic melanomas. Pyrosequencing was theonly one with 100% sensitivity (95%CI, 92.4% to 100%) andspecificity (95% CI, 91.6% to 100%) for p.V600 detection.
The Journal of Molecular Diagnostics - jmd.amjpathol.org
For many years, Sanger sequencing has been consideredthe reference method for identification of acquired muta-tions in tumors. However, because of its low sensitivity,detection of mutations from tumor DNA requires a highpercentage of tumor cells within the samples,23 require-ments that cannot always be met in routine diagnostictesting of human samples. In the present study microdis-section of metastatic melanomas was performed to increasethe number of tumor cells to at least 60%. However, 3 of the40 melanomas with p.V600E mutation detected by othermethods were negative with Sanger sequencing. Thesensitivity of Sanger sequencing was 92.5% (95% CI,78.5% to 98.0%) for p.V600E detection. Thus, 7.2% ofpatients eligible for vemurafenib treatment would have been
Figure 3 Detection of p.V600K with p.V600E-specific real-time PCR. Amplification curves offour cases with a negative control, two p.V600Kcases, and a p.V600E-positive control. WithoutPNAs, amplification of both mutated (red) and WT(green) alleles was obvious on the p.V600E-positive control, whereas only the WT weredetectable on the three other samples. Thep.V600K mutations (red curves) were only detect-able with the PNA inhibition of WT alleleamplification.
97
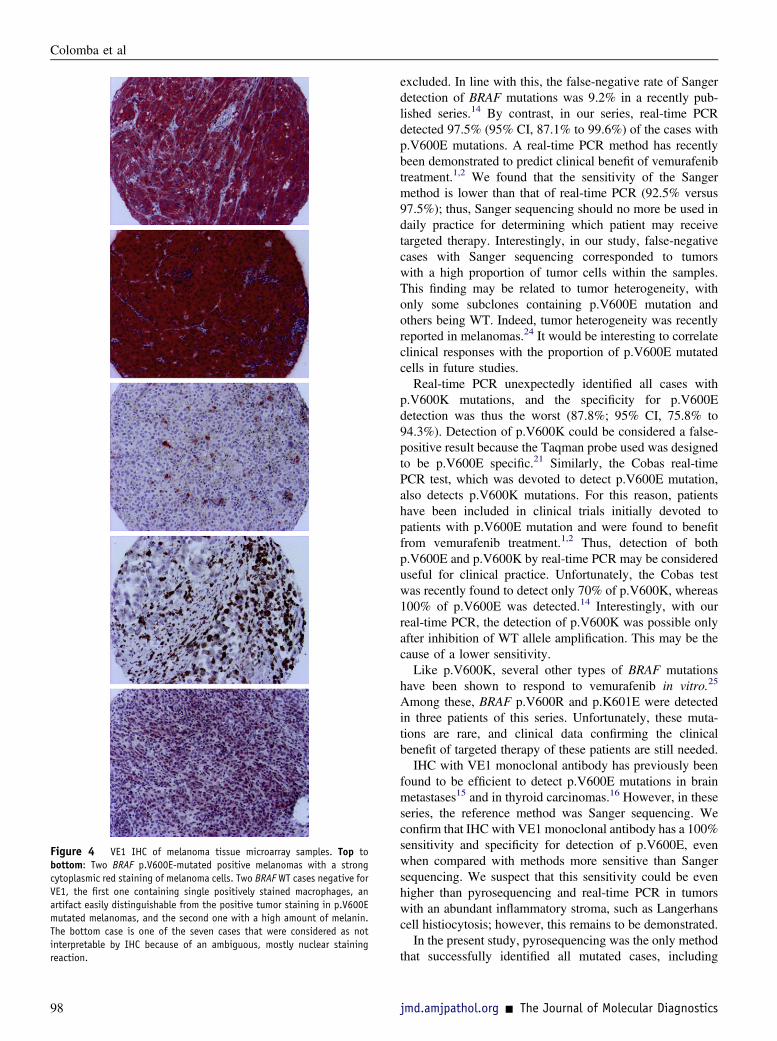
Figure 4 VE1 IHC of melanoma tissue microarray samples. Top tobottom: Two BRAF p.V600E-mutated positive melanomas with a strongcytoplasmic red staining of melanoma cells. Two BRAF WT cases negative forVE1, the first one containing single positively stained macrophages, anartifact easily distinguishable from the positive tumor staining in p.V600Emutated melanomas, and the second one with a high amount of melanin.The bottom case is one of the seven cases that were considered as notinterpretable by IHC because of an ambiguous, mostly nuclear stainingreaction.
Colomba et al
98
excluded. In line with this, the false-negative rate of Sangerdetection of BRAF mutations was 9.2% in a recently pub-lished series.14 By contrast, in our series, real-time PCRdetected 97.5% (95% CI, 87.1% to 99.6%) of the cases withp.V600E mutations. A real-time PCR method has recentlybeen demonstrated to predict clinical benefit of vemurafenibtreatment.1,2 We found that the sensitivity of the Sangermethod is lower than that of real-time PCR (92.5% versus97.5%); thus, Sanger sequencing should no more be used indaily practice for determining which patient may receivetargeted therapy. Interestingly, in our study, false-negativecases with Sanger sequencing corresponded to tumorswith a high proportion of tumor cells within the samples.This finding may be related to tumor heterogeneity, withonly some subclones containing p.V600E mutation andothers being WT. Indeed, tumor heterogeneity was recentlyreported in melanomas.24 It would be interesting to correlateclinical responses with the proportion of p.V600E mutatedcells in future studies.Real-time PCR unexpectedly identified all cases with
p.V600K mutations, and the specificity for p.V600Edetection was thus the worst (87.8%; 95% CI, 75.8% to94.3%). Detection of p.V600K could be considered a false-positive result because the Taqman probe used was designedto be p.V600E specific.21 Similarly, the Cobas real-timePCR test, which was devoted to detect p.V600E mutation,also detects p.V600K mutations. For this reason, patientshave been included in clinical trials initially devoted topatients with p.V600E mutation and were found to benefitfrom vemurafenib treatment.1,2 Thus, detection of bothp.V600E and p.V600K by real-time PCR may be considereduseful for clinical practice. Unfortunately, the Cobas testwas recently found to detect only 70% of p.V600K, whereas100% of p.V600E was detected.14 Interestingly, with ourreal-time PCR, the detection of p.V600K was possible onlyafter inhibition of WT allele amplification. This may be thecause of a lower sensitivity.Like p.V600K, several other types of BRAF mutations
have been shown to respond to vemurafenib in vitro.25
Among these, BRAF p.V600R and p.K601E were detectedin three patients of this series. Unfortunately, these muta-tions are rare, and clinical data confirming the clinicalbenefit of targeted therapy of these patients are still needed.IHC with VE1 monoclonal antibody has previously been
found to be efficient to detect p.V600E mutations in brainmetastases15 and in thyroid carcinomas.16 However, in theseseries, the reference method was Sanger sequencing. Weconfirm that IHC with VE1 monoclonal antibody has a 100%sensitivity and specificity for detection of p.V600E, evenwhen compared with methods more sensitive than Sangersequencing. We suspect that this sensitivity could be evenhigher than pyrosequencing and real-time PCR in tumorswith an abundant inflammatory stroma, such as Langerhanscell histiocytosis; however, this remains to be demonstrated.In the present study, pyrosequencing was the only method
that successfully identified all mutated cases, including
jmd.amjpathol.org - The Journal of Molecular Diagnostics

Detection of BRAF Mutations in Melanoma
those with a low proportion of mutated alleles and thosewith rare mutations. The costs, laboratory organization, anddelay for result delivery of pyrosequencing in our hands aresimilar to Sanger sequencing and real-time PCR in ourlaboratory (data not shown). We have thus adopted pyro-sequencing as the reference method for BRAF mutationdetection in melanoma in our laboratory daily practice.However, because IHC is cheaper and results are easilyobtained within 48 hours, it could be used as the firstanalysis. Pyrosequencing would be performed only on casesnot interpretable or negative, corresponding to approxi-mately 50% to 60% of samples analyzed by IHC. A similarsequential analysis with IHC in first-line cases and molec-ular biology in some cases, depending on IHC results, isalready widely used for detection of HER2 amplification.26
Molecular methods with higher sensitivity, such as massiveparallel sequencing, should be evaluated on samples forwhich it is not possible to obtain >20% of tumor cells.
In conclusion, analysis of BRAF mutations in melanomaswith four different methods revealed that Sanger sequencingshould no longer be used to identify patients who couldbenefit from vemurafenib treatment. Our results suggest thatsequential analysis, with initial detection of p.V600E-positive cases by IHC, followed by pyrosequencing innegative or uninterpretable cases is the most efficientmethod to use in laboratory daily practice.
Acknowledgments
We acknowledge Mariama Bakari, Gladys Faucher, Cath-erine Le Gall, Yolaine Pothin, and Véronique Toulza forparticipating in the analysis of samples.
References
1. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J,Dummer R, Garbe C, Testori A, Maio M, Hogg D, Lorigan P,Lebbe C, Jouary T, Schadendorf D, Ribas A, O’Day SJ, Sosman JA,Kirkwood JM, Eggermont AM, Dreno B, Nolop K, Li J, Nelson B,Hou J, Lee RJ, Flaherty KT, McArthur GA, BRIM-3 Study Group:Improved survival with vemurafenib in melanoma with BRAF V600Emutation. N Engl J Med 2011, 364:2507e2516
2. Sosman JA, Kim KB, Schuchter L, Gonzalez R, Pavlick AC,Weber JS, McArthur GA, Hutson TE, Moschos SJ, Flaherty KT,Hersey P, Kefford R, Lawrence D, Puzanov I, Lewis KD,Amaravadi RK, Chmielowski B, Lawrence HJ, Shyr Y, Ye F, Li J,Nolop KB, Lee RJ, Joe AK, Ribas A: Survival in BRAF V600-mutantadvanced melanoma treated with vemurafenib. N Engl J Med 2012,366:707e714
3. Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S,Teague J, et al: Mutations of the BRAF gene in human cancer. Nature2002, 417:949e954
4. Chapman MA, Lawrence MS, Keats JJ, Cibulskis K, Sougnez C,Schinzel AC, et al: Initial genome sequencing and analysis of multiplemyeloma. Nature 2011, 471:467e472
5. Tiacci E, Schiavoni G, Forconi F, Santi A, Trentin L, Ambrosetti A,Cecchini D, Sozzi E, Francia di Celle P, Di Bello C, Pulsoni A, Foà R,Inghirami G, Falini B: Simple genetic diagnosis of hairy cell leukemia
The Journal of Molecular Diagnostics - jmd.amjpathol.org
by sensitive detection of the BRAF-V600E mutation. Blood 2012, 119:192e195
6. Lee JH, Choi JW, Kim YS: Frequencies of BRAF and NRAS muta-tions are different in histological types and sites of origin of cutaneousmelanoma: a meta-analysis. Br J Dermatol 2011, 164:776e784
7. Han J, Colditz GA, Hunter DJ: Risk factors for skin cancers: a nestedcase-control study within the Nurses’ Health Study. Int J Epidemiol2006, 35:1514e1521
8. Armstrong BK, Kricker A, English DR: Sun exposure and skin cancer.Australas J Dermatol 1997, 38(Suppl 1):S1eS6
9. Xing M, Tufano RP, Tufaro AP, Basaria S, Ewertz M, Rosenbaum E,Byrne PJ, Wang J, Sidransky D, Ladenson PW: Detection of BRAFmutation on fine needle aspiration biopsy specimens: a new diagnostictool for papillary thyroid cancer. J Clin Endocrinol Metab 2004, 89:2867e2872
10. Spittle C, Ward MR, Nathanson KL, Gimotty PA, Rappaport E,Brose MS, Medina A, Letrero R, Herlyn M, Edwards RH: Applicationof a BRAF pyrosequencing assay for mutation detection and copynumber analysis in malignant melanoma. J Mol Diagn 2007, 9:464e471
11. Thomas RK, Baker AC, DeBiasi RM, Winckler W, LaFramboise T,Lin WM, et al: High-throughput oncogene mutation profiling in humancancer. Nat Genet 2007, 39:347e351
12. Pichler M, Balic M, Stadelmeyer E, Ausch C, Wild M, Guelly C,Bauernhofer T, Samonigg H, Hoefler G, Dandachi N: Evaluation ofhigh-resolution melting analysis as a diagnostic tool to detect the BRAFV600E mutation in colorectal tumors. J Mol Diagn 2009, 11:140e147
13. Jarry A, Masson D, Cassagnau E, Parois S, Laboisse C, Denis MG:Real-time allele-specific amplification for sensitive detection of theBRAF mutation V600E. Mol Cell Probes 2004, 18:349e352
14. Anderson S, Bloom KJ, Vallera DU, Rueschoff J, Meldrum C,Schilling R, Kovach B, Lee JR, Ochoa P, Langland R, Halait H,Lawrence HJ, Dugan MC: Multisite analytic performance studiesof a real-time polymerase chain reaction assay for the detection ofBRAF V600E mutations in formalin-fixed paraffin-embeddedtissue specimens of malignant melanoma. Arch Pathol Lab Med 2012,136:1385e1391
15. Capper D, Berghoff AS, Magerle M, Ilhan A, Wöhrer A, Hackl M,Pichler J, Pusch S, Meyer J, Habel A, Petzelbauer P, Birner P, vonDeimling A, Preusser M: Immunohistochemical testing of BRAFV600E status in 1,120 tumor tissue samples of patients with brainmetastases. Acta Neuropathol 2012, 123:223e233
16. Koperek O, Kornauth C, Capper D, Berghoff AS, Asari R, Niederle B,Deimling A, Birner P, Preusser M. Immunohistochemical detection ofthe BRAF V600E mutated protein in papillary thyroid carcinoma. AmJ Surg Pathol 2012, 36:844e850.
17. Ibrahem S, Seth R, O’Sullivan B, Fadhil W, Taniere P, Ilyas M:Comparative analysis of pyrosequencing and QMC-PCR in conjunc-tion with high resolution melting for KRAS/BRAF mutation detection.Int J Exp Pathol 2010, 91:500e505
18. Halait H, Demartin K, Shah S, Soviero S, Langland R, Cheng S,Hillman G, Wu L, Lawrence HJ: Analytical performance of a real-timePCR-based assay for V600 mutations in the BRAF gene, used as thecompanion diagnostic test for the novel BRAF inhibitor vemurafenibin metastatic melanoma. Diagn Mol Pathol 2012, 21:1e8
19. Heideman DAM, Lurkin I, Doeleman M, Smit EF, Verheul HM,Meijer GA, Snijders PJ, Thunnissen E, Zwarthoff EC: KRAS andBRAF mutation analysis in routine molecular diagnostics: comparisonof three testing methods on formalin-fixed, paraffin-embedded tumor-derived DNA. J Mol Diagn 2012, 14:247e255
20. Carbonell P, Turpin MC, Torres-Moreno D, Molina-Martínez I,García-Solano J, Perez-Guillermo M, Conesa-Zamora P: Comparisonof allelic discrimination by dHPLC, HRM, and TaqMan in thedetection of BRAF mutation V600E. J Mol Diagn 2011, 13:467e473
21. Didelot A, Le Corre D, Luscan A, Cazes A, Pallier K, Emile JF,Laurent-Puig P, Blons H: Competitive allele specific TaqMan PCRfor KRAS, BRAF and EGFR mutation detection in clinical
99

Colomba et al
formalin fixed paraffin embedded samples. Exp Mol Pathol 2012, 92:275e280
22. Moreau S, Saiag P, Aegerter P, Bosset D, Longvert C, Hélias-Rodzewicz Z, Marin C, Peschaud F, Chagnon S, Zimmermann U,Clerici T, Emile JF: Prognostic value of BRAFV600 mutations inmelanoma patients after resection of metastatic lymph nodes. Ann SurgOncol 2012, 19:4314e4321
23. Zhang H, Zheng X, Ji T, Fu L, Bai D, Liao Y, Zhang H, Ding Y,Zheng L: Comparative screening of K-ras mutations in colorectalcancer and lung cancer patients using a novel real-time PCR withADx-K-ras Kit and Sanger DNA sequencing. Cell Biochem Biophys2012, 62:415e420
24. Yancovitz M, Litterman A, Yoon J, Ng E, Shapiro RL, Berman RS,Pavlick AC, Darvishian F, Christos P, Mazumdar M, Osman I,Polsky D: Intra- and inter-tumor heterogeneity of BRAF (V600E)
100
mutations in primary and metastatic melanoma. PLoS ONE 2012, 7:e29336
25. Yang H, Higgins B, Kolinsky K, Packman K, Bradley WD, Lee RJ,Schostack K, Simcox ME, Kopetz S, Heimbrook D, Lestini B,Bollag G, Su F: Antitumor activity of BRAF inhibitor vemurafenib inpreclinical models of BRAF-mutant colorectal cancer. Cancer Res2012, 72:779e789
26. Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC,Cote RJ, Dowsett M, Fitzgibbons PL, Hanna WM, Langer A,McShane LM, Paik S, Pegram MD, Perez EA, Press MF, Rhodes A,Sturgeon C, Taube SE, Tubbs R, Vance GH, van de Vijver M,Wheeler TM, Hayes DF: American Society of Clinical Oncology/College of American Pathologists guideline recommendations forhuman epidermal growth factor receptor 2 testing in breast cancer. JClin Oncol 2007, 25:118e145
jmd.amjpathol.org - The Journal of Molecular Diagnostics
Related Documents











