Infants and Young Children Vol. 17, No. 2, pp. 114–124 c 2004 Lippincott Williams & Wilkins, Inc. Detecting and Managing Developmental and Behavioral Problems in Infants and Young Children The Potential Role of the DSM-PC Dennis Drotar, PhD The Diagnostic and Statistical Manual for Primary Care (DSM-PC), Child and Adolescent Ver- sion, provides a comprehensive method to facilitate professional recognition, management, and referral of a wide spectrum of children’s behavioral and developmental problems, as well as stress- ful situations. This article describes the utility of the DSM-PC for a multidisciplinary group of prac- titioners who work with infants and young children. Four areas of potential application of the DSM-PC are described: (1) diagnosis and management of problems that are specific to infants and young children; (2) description of environmental stressors; (3) description of developmental varia- tion and change in infant problem behaviors; and (4) implications for research concerning infants’ behavioral and developmental problems. Key words: behavioral problems, developmental prob- lems, diagnosis, DSM-IV, DSM-PC, early identification, infant mental health P RIMARY CARE PRACTITIONERS (PCPs) (eg, pediatricians and family practition- ers), preschool teachers, day care providers, and early intervention providers are in a crit- ical position to provide monitoring and pre- ventive management of the behavior and de- velopment of infants and toddlers. However, substantial numbers of infants and young chil- dren who present with behavioral and devel- opmental problems such as sleep disturbance, irritable behavior, feeding problems, repeti- tive behavior patterns, delays in cognitive and language development, and problems relat- From the Rainbow Babies and Children’s Hospital, and the Department of Pediatrics, Case Western Reserve University School of Medicine, Cleveland, Ohio. The assistance of Susan Wood and Steve Nipple in pro- cessing this manuscript is gratefully acknowledged. Corresponding author: Dennis Drotar, PhD, Rainbow Babies and Children’s Hospital, 11100 Euclid Ave, Cleveland, OH 44106 (e-mail: [email protected]). ing to behavioral control may not be identi- fied. As a consequence, considerable oppor- tunities for early preventive management of such problems may be lost. Research has con- sistently noted that large numbers, anywhere from 12% to 25%, of children who are seen in primary care, have significant psychoso- cial problems (Costello, 1986; Costello et al., 1988; Kelleher & Rickert, 1994) but only a subset of these children is identified and re- ferred for treatment (Costello et al., 1988; Lavigne et al., 1993). Multiple factors influence the discrepancy between the prevalence of behavioral and developmental problems among infants and young children and the typical frequency of their recognition and management by pedi- atricians and other practicing professionals (Drotar, 2002). For example, practice-based time constraints may affect practitioners’ abil- ities to diagnose and manage infants’ behav- ioral and developmental problems. In addi- tion, some practitioners may be reluctant to identify behavioral and developmental 114

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
Infants and Young ChildrenVol. 17, No. 2, pp. 114–124c© 2004 Lippincott Williams & Wilkins, Inc.
Detecting and ManagingDevelopmental andBehavioral Problems inInfants and Young ChildrenThe Potential Role of the DSM-PC
Dennis Drotar, PhD
The Diagnostic and Statistical Manual for Primary Care (DSM-PC), Child and Adolescent Ver-sion, provides a comprehensive method to facilitate professional recognition, management, andreferral of a wide spectrum of children’s behavioral and developmental problems, as well as stress-ful situations. This article describes the utility of the DSM-PC for a multidisciplinary group of prac-titioners who work with infants and young children. Four areas of potential application of theDSM-PC are described: (1) diagnosis and management of problems that are specific to infants andyoung children; (2) description of environmental stressors; (3) description of developmental varia-tion and change in infant problem behaviors; and (4) implications for research concerning infants’behavioral and developmental problems. Key words: behavioral problems, developmental prob-lems, diagnosis, DSM-IV, DSM-PC, early identification, infant mental health
PRIMARY CARE PRACTITIONERS (PCPs)(eg, pediatricians and family practition-
ers), preschool teachers, day care providers,and early intervention providers are in a crit-ical position to provide monitoring and pre-ventive management of the behavior and de-velopment of infants and toddlers. However,substantial numbers of infants and young chil-dren who present with behavioral and devel-opmental problems such as sleep disturbance,irritable behavior, feeding problems, repeti-tive behavior patterns, delays in cognitive andlanguage development, and problems relat-
From the Rainbow Babies and Children’s Hospital,and the Department of Pediatrics, Case WesternReserve University School of Medicine, Cleveland,Ohio.
The assistance of Susan Wood and Steve Nipple in pro-cessing this manuscript is gratefully acknowledged.
Corresponding author: Dennis Drotar, PhD, RainbowBabies and Children’s Hospital, 11100 Euclid Ave,Cleveland, OH 44106 (e-mail: [email protected]).
ing to behavioral control may not be identi-fied. As a consequence, considerable oppor-tunities for early preventive management ofsuch problems may be lost. Research has con-sistently noted that large numbers, anywherefrom 12% to 25%, of children who are seenin primary care, have significant psychoso-cial problems (Costello, 1986; Costello et al.,1988; Kelleher & Rickert, 1994) but only asubset of these children is identified and re-ferred for treatment (Costello et al., 1988;Lavigne et al., 1993).
Multiple factors influence the discrepancybetween the prevalence of behavioral anddevelopmental problems among infants andyoung children and the typical frequency oftheir recognition and management by pedi-atricians and other practicing professionals(Drotar, 2002). For example, practice-basedtime constraints may affect practitioners’ abil-ities to diagnose and manage infants’ behav-ioral and developmental problems. In addi-tion, some practitioners may be reluctantto identify behavioral and developmental
114
LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
Role of the DSM-PC 115
problems because they are concerned aboutincorrectly labeling children at a very youngage and/or alarming their parents unneces-sarily. Problems with access to experiencedmental health practitioners and limitationsin insurance coverage may also limit earlyprofessional recognition and management ofyoung children’s behavioral problems (Drotar,2002).
Another significant barrier to the diag-nosis and management of young children’sbehavioral and developmental problems con-cerns available systems of diagnostic cat-egorization of infants and young childrenwith behavioral and developmental problems(Drotar, 2002). The primary diagnostic sys-tem for the classification of behavioral anddevelopmental problems that is currently inuse, the Diagnostic and Statistical Manualof Mental Disorders, 4th edition (DSM-IV)(American Psychiatric Association, 1995) hassalient limitations that limit its utility for pro-fessionals, including PCPs, who work with in-fants and young children. For example, theDSM-IV focuses on child and adolescent men-tal disorders that are both more serious andless prevalent than the broad spectrum ofbehavioral and developmental problems thatare commonly seen in infants and young chil-dren (Jensen & Sinclair, 2002; Lieberman &Zennah, 1995; MacLean & Symons, 2002;Neary & Eyberg, 2002; Robinson, 2002). Pro-fessionals, including PCPs, who work withinfants and young children encounter largenumbers of children with behavioral and de-velopmental problems that simply do not fitthe DSM-IV criteria and/or do not meet spe-cific thresholds for DSM-IV disorders. Con-sequently, when practitioners evaluate suchchildren they may be uncertain about howbest to classify children’s problems using theDSM-IV. On the other hand, when they aregiven an opportunity to use an alternative di-agnostic nomenclature system that includes amore comprehensive language with which todescribe the full range of problems encoun-tered in practice, they may identify behav-ioral problems with greater frequency. In sup-port of this notion, Horwitz, Leaf, Leventhal,
Forsythe, and Speechley (1992) found thatwhen pediatricians used a diagnostic nomen-clature that provided a broader range ofchoices than does the DSM-IV, they identifiedhigher rates of behavior problems than wastypical in studies in which pediatricians haveused the DSM-IV.
Until relatively recently, no organized, log-ically coherent alternative to the DSM-IV hasbeen available to professionals to guide theirdiagnosis and management of behavioral anddevelopmental problems of infants and youngchildren. One major advance that is relevantto diagnostic classification was the Diagnos-tic Classification 0–3 (Zero to Three/NationalCenter for Infant Programs, 1994), which cat-egorizes emotional and behavioral patternsthat represent significant deviations from nor-mal development in the earliest years of life.Some of the categories in this system, such asregulatory disorders, are new formulations ofmental health and developmental problems.Others describe the earliest manifestations ofmental health problems, such as mood dis-orders, which have been identified amongolder children and adults, but have not beenfully described in infants and young children.In addition to a section that describes theprimary diagnosis (Axis 1), the DiagnosticClassification 0–3 includes a classification ofrelationship disorders, (eg, overinvolved, un-derinvolved) (Axis II), which is a list ofpsychosocial stressors and a description ofwhether they are acute, or enduring, and arating of their impact (Axis IV), and an assess-ment of functional developmental level (AxisV), which addresses the way in which the in-fant organizes his or her functioning (eg, mu-tual engagement, representational communi-cation, etc).
The Diagnostic Classification 0–3 also de-scribes any physical (including medical andneurological), mental health, and/or devel-opmental diagnoses that are made based onother diagnostic and classification systems(Axis III). Coding systems identified as rel-evant for this purpose include the DSM-IV, International Classification of Diseases(ICD-10), and the Diagnostic and Statistical

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
116 INFANTS AND YOUNG CHILDREN/APRIL–JUNE 2004
Manual for Primary Care (DSM-PC), Childand Adolescent Version (Wolraich, 1997;Wolraich, Felice, & Drotar, 1996). The newestand perhaps least known of these classifi-cation systems to many professionals whowork with infants and young children andtheir families, the DSM- PC was developedby the American Academy of Pediatrics (AAP)in collaboration with a number of other or-ganizations involving other professional dis-ciplines such as psychology and psychiatry.Potential advantages of the DSM-PC for usewith infants and young children comparedwith alternative coding systems, including theDiagnostic Classification 0–3, are compre-hensiveness (eg, inclusion of a wide rangeof developmental and behavioral problems),availability of an expanded list of environmen-tal stressors, and emphasis on a continuumof behavioral and developmental phenomena,which include normal variations, problems,and disorders.
The DSM-PC has been available for use byPCPs, including pediatricians and family prac-titioners, for more than 4 years. However, tomy knowledge, the specific applications ofthe DSM-PC to the classification and manage-ment of behavioral and developmental prob-lems of infants and young children have notbeen described. To address this need, the pur-pose of this article is to describe the DSM-PC,its application to diagnosis and managementof problems identified in infants and youngchildren, and the implications for interdisci-plinary practice, training, and research.
WORKING ASSUMPTIONS THAT GUIDEDTHE DEVELOPMENT OF THE DSM-PC
The primary working assumptions thatguided the development of the DSM-PC(Wolraich, 1997) included the following: (1)children, including infants and young chil-dren, demonstrate symptoms that vary alonga continuum from normal variations to severemental disorders that can be divided into clin-ically meaningful gradations; (2) the qualityof children’s environments, including their ex-posure to stress, has a critical impact on their
mental health and development; (3) a codingsystem for children’s developmental and be-havioral problems should be fully compatiblewith available classification approaches suchas the DSM-IV and the ICD-10; (4) an effectivecoding system should be clear, concise, andusable; (5) a coding system should be basedon available objective data and professionalconsensus; and (6) the language used in thecoding system should be clear and verifiableby research.
DESCRIPTION OF THE CORE ELEMENTSOF THE DSM-PC
The DSM-PC includes a table of contents,introduction, and 2 major core content areas:Situations and Child Manifestations, and ap-pendices. Each of these selections is brieflydescribed below.
Table of contents and introduction
The table of contents for the DSM-PC is fol-lowed by a detailed list that includes the pagenumber and code number of each diagnosis.A brief introduction then describes the pur-pose, key assumptions, and organization ofthe manual. The introduction also includesguidelines for using the DSM-PC such as locat-ing information in the manual, a flow chart ofsteps in coding, and case illustrations of howto use the manual. Finally, the introduction in-cludes a description of relevant issues in as-sessing the severity of the clinical needs ofchildren and families.
Situations
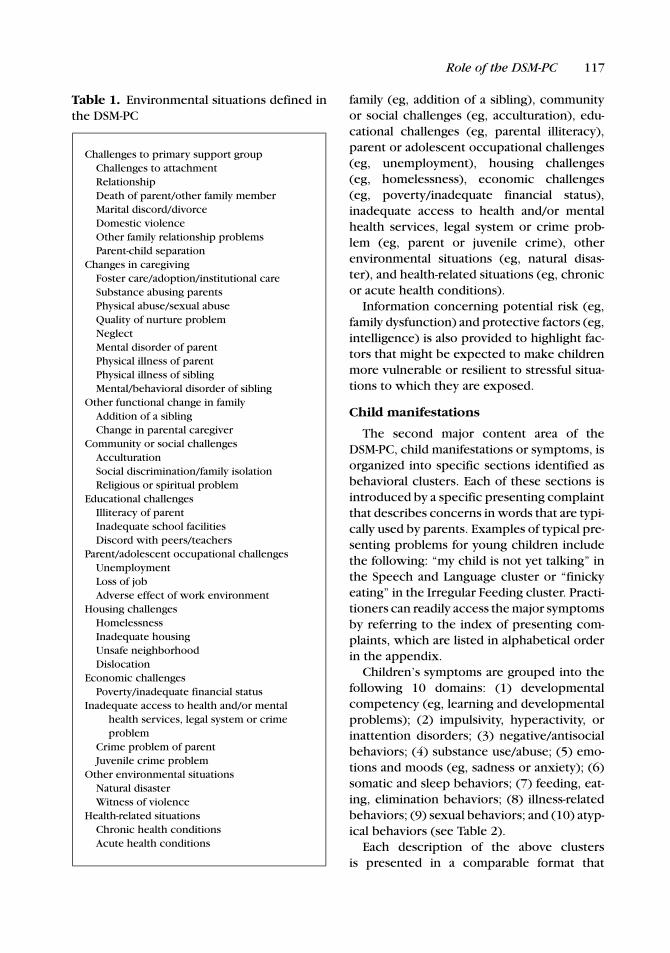
The “Situations” section was designed tohelp practitioners to describe and evaluatethe impact of stressful situations that presentin primary care and community settings andcan affect children’s mental health. As shownin Table 1, the following categories of poten-tially stressful situations that were identifiedas the most common and/or well-documentedare defined in the DSM-PC: challenges to pri-mary support group (eg, marital discord/divorce), changes in caregiving (eg, physicalillness of parent), other functional changes in
LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
Role of the DSM-PC 117
Table 1. Environmental situations defined inthe DSM-PC
Challenges to primary support groupChallenges to attachmentRelationshipDeath of parent/other family memberMarital discord/divorceDomestic violenceOther family relationship problemsParent-child separation
Changes in caregivingFoster care/adoption/institutional careSubstance abusing parentsPhysical abuse/sexual abuseQuality of nurture problemNeglectMental disorder of parentPhysical illness of parentPhysical illness of siblingMental/behavioral disorder of sibling
Other functional change in familyAddition of a siblingChange in parental caregiver
Community or social challengesAcculturationSocial discrimination/family isolationReligious or spiritual problem
Educational challengesIlliteracy of parentInadequate school facilitiesDiscord with peers/teachers
Parent/adolescent occupational challengesUnemploymentLoss of jobAdverse effect of work environment
Housing challengesHomelessnessInadequate housingUnsafe neighborhoodDislocation
Economic challengesPoverty/inadequate financial status
Inadequate access to health and/or mentalhealth services, legal system or crimeproblem
Crime problem of parentJuvenile crime problem
Other environmental situationsNatural disasterWitness of violence
Health-related situationsChronic health conditionsAcute health conditions
family (eg, addition of a sibling), communityor social challenges (eg, acculturation), edu-cational challenges (eg, parental illiteracy),parent or adolescent occupational challenges(eg, unemployment), housing challenges(eg, homelessness), economic challenges(eg, poverty/inadequate financial status),inadequate access to health and/or mentalhealth services, legal system or crime prob-lem (eg, parent or juvenile crime), otherenvironmental situations (eg, natural disas-ter), and health-related situations (eg, chronicor acute health conditions).
Information concerning potential risk (eg,family dysfunction) and protective factors (eg,intelligence) is also provided to highlight fac-tors that might be expected to make childrenmore vulnerable or resilient to stressful situa-tions to which they are exposed.
Child manifestations
The second major content area of theDSM-PC, child manifestations or symptoms, isorganized into specific sections identified asbehavioral clusters. Each of these sections isintroduced by a specific presenting complaintthat describes concerns in words that are typi-cally used by parents. Examples of typical pre-senting problems for young children includethe following: “my child is not yet talking” inthe Speech and Language cluster or “finickyeating” in the Irregular Feeding cluster. Practi-tioners can readily access the major symptomsby referring to the index of presenting com-plaints, which are listed in alphabetical orderin the appendix.
Children’s symptoms are grouped into thefollowing 10 domains: (1) developmentalcompetency (eg, learning and developmentalproblems); (2) impulsivity, hyperactivity, orinattention disorders; (3) negative/antisocialbehaviors; (4) substance use/abuse; (5) emo-tions and moods (eg, sadness or anxiety); (6)somatic and sleep behaviors; (7) feeding, eat-ing, elimination behaviors; (8) illness-relatedbehaviors; (9) sexual behaviors; and (10) atyp-ical behaviors (see Table 2).
Each description of the above clustersis presented in a comparable format that

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
118 INFANTS AND YOUNG CHILDREN/APRIL–JUNE 2004
Table 2. Childhood manifestations defined inthe DSM-PC
Developmental competencyCognitive/adaptive skills (MR)Academic skillsMotor developmentSpeech and language
Impulsive/hyperactive or inattentivebehaviors
Hyperactive/impulsive behaviorsInattentive behaviors
Negative/antisocial behaviorsNegative emotional behaviorsAggressive/oppositional behaviorsSecretive antisocial behaviors
Substance use/abuseSubstance use/abuse
Emotions and moodsAnxious symptomsSadness and related symptomsSuicidal thoughts or behaviors
Somatic and sleep behaviorsPain/somatic complaintsExcessive daytime sleepinessSleeplessnessNocturnal arousals
Feeding, eating, elimination behaviorsSoiling problemsDay/nighttime wetting problemsPurging/binge eatingDieting/body image problemsIrregular feeding behaviors
Illness-related behaviorsPsychological factors affecting
medical conditionSexual behaviors
Gender identity issuesSexual development behaviors
Atypical behaviorsRepetitive behavioral patternsSocial interaction behaviorsBizarre behavior
includes the cluster title, presenting com-plaints, definitions and symptoms, as well asinformation about epidemiology and etiologyof specific problems. These formats were de-veloped to guide practitioners to considerthe following issues for each cluster: (1) the
spectrum of severity of a child’s presentingproblems; (2) common developmental pre-sentations (eg, how problems in the clusterpresent during infancy, early and middle child-hood, and adolescence; and (3) differentialdiagnosis. In order to facilitate practitioners’abilities to make differential diagnoses, infor-mation for each cluster is presented in analgorithmic format. Examples of differentialdiagnosis in a young child who is not talkingmight include speech and language problem,expressive language disorder, hearing impair-ment, mental retardation, etc.
Common developmental presentations
To help practitioners recognize how com-mon symptoms (eg, anxiety) may be ex-pressed among children of different ages,guidelines for symptom expression are pro-vided in the DSM-PC to facilitate coding ofvariations, problems, and disorders in eachof 4 age groups; infancy (birth to 2 years ofage), early childhood (3–5 years of age), mid-dle childhood (6–12 years of age), and adoles-cence (13 years of age and older).
Differential diagnosis
Information that is provided in each of theclusters that is designed to help practitionersmake a differential diagnosis is divided into2 sections: alternative causes and comorbidand associated conditions. The “DifferentialDiagnosis” section describes phenomena thatneed to be considered as alternative causes forspecific behaviors including (1) general med-ical conditions; (2) substances, legal and il-legal, that could cause behavioral manifesta-tions; or (3) mental disorders that may presentwith similar behavioral symptoms and which,if present, should be coded in place of the dis-order in the cluster.
Appendices
The appendices include a list of presentingcomplaints and page numbers, a section on di-agnostic vignettes, which provide informativecase material that can be used to practice cod-ing, and a section that summarizes frequentlyoccurring DSM-IV diagnoses and criteria that

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
Role of the DSM-PC 119
are likely to be used by practitioners, includ-ing PCPs.
POTENTIAL UTILITY OF THE DSM-PCFOR CLINICAL PRACTICE WITHINFANTS AND YOUNG CHILDREN
The DSM-PC was designed to help practi-tioners accomplish 2 main clinical tasks: (1)distinguish among a range of behavioral anddevelopmental problems that vary widely inseverity and content and (2) identify a widerange of stressful situations that can affect themanagement of young children’s behavioraland developmental problems.
Making diagnostic determinationsacross the spectrum of problem severity
One of the special features of the develop-ment of infants and young children is the ex-traordinary rate of developmental change thatis observed in this age group. For this reason,it can be especially difficult for practitionersand parents to distinguish clinically significantproblems from those that reflect normal de-velopmental variations. One of the primaryfeatures of the DSM-PC is that it gives prac-titioners a method to distinguish among theseverity of behavioral/developmental prob-lems encountered in infants and young chil-dren by defining 3 broad categories: devel-opmental variations, problems, and disorders.The first 2 categories reflect diagnoses thatare newly defined by the DSM-PC. Disordersare those that have already been defined inthe DSM-IV. Developmental variations referto those behaviors that parents may raise asa concern to their PCP or other professionalsbut are within the range of what is expectedfor an infant or young child of that particularage (eg, separation anxiety in a 15-month-oldchild). The management of behaviors that areclassified as developmental variations is mostlikely to be conducted by pediatricians or fam-ily practitioners and may include assuring par-ents that their infants or toddlers have age-appropriate behaviors and providing specificguidance to parents concerning the manage-ment of their children’s behavior.
In contrast to developmental variations,problems are defined as behaviors that areserious enough to disrupt the young child’sfunctioning in any one of a number of rel-evant developmental contexts, such as thefamily situation, in relations with peers, or inpreschool, and cause significant burden or dis-tress for the child and/or parents. Depend-ing on the level of functional impairment thatis associated with a young child’s behavioralor developmental problem and/or degree ofdistress caused by the problem, behaviors orsymptoms that are classified as problems maybe managed by the PCP, referred to other prac-titioners, or referred for early interventionservices.
Case illustration
The following case example illustrates how pro-fessionals can use the distinction between de-velopmental variation and problem to facilitatetheir assessment and management of behavioralsymptoms in infants and young children. The par-ents of Sally, age 2, have been concerned abouther difficulties relating to other children. When-ever unfamiliar children come into her house,she initially avoids them. Eventually, she is ableto establish interactions with children whom sheknows. Having provided care for Sally since shewas an infant, her pediatrician recognizes thatshe has always been a very shy child who has haddifficulty managing any new situation. Her par-ents have always had to help her manage novelevents, especially unfamiliar social situations.
Based on the DSM-PC, Sally’s behavior can becategorized within the cluster: “Atypical Behav-iors,” as a social interaction variation, which is de-fined as “a variation in children’s ability and desireto interact with other people because of constitu-tional and psychological factors” (Wolraich et al.,1996). In managing Sally’s problem, her pediatri-cian might advise the parents that her social be-havior is largely within normal limits and reflectsthe expression of her special temperament, es-pecially her strong preference to withdraw ratherthan approach in response to new situations. Inaddition, her parents might be advised to antici-pate the constraints of her temperament by notoverwhelming her with new peer contacts. Fi-nally, Sally’s parents might be instructed to en-courage and reward her interactions with familiarpeers.

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
120 INFANTS AND YOUNG CHILDREN/APRIL–JUNE 2004
Consider the contrasting social interactionproblems of 3-year-old Alex: His nursery schoolteacher contacted his parents because she wasvery concerned about his difficulty establishingcontact with other children, despite repeated op-portunities for him to do so after a number ofmonths in preschool. He has preferred to staynear her and avoided other children for the mostpart. Alex also demonstrated great difficulty sep-arating from his mother to attend preschool. Histeacher also noted that Alex’s avoidance of otherchildren has interfered significantly with his rela-tionships with peers who now avoid him. His be-havior has become a significant source of con-cern to his mother who wonders whether sheshould take him out of preschool because of theseproblems. On the other hand, Alex’s father doesnot believe that Alex has any problems, and theparents have disagreed strongly about how bestto manage Alex’s behavior.
Alex’s problems are clearly more serious thatwould be expected for a child of his age, yet donot meet threshold for any DSM-IV diagnosis. Us-ing the DSM-PC, one could classify Alex’s be-havior as a social withdrawal problem, definedas “the child’s inability and/or desire to interactwith people is limited enough to begin to inter-fere with the child’s development and activities”(Wolraich et al., 1996). To help Alex’s parentsmanage his problems, the PCP might recom-mend a more intensive evaluation and/or inter-vention that might necessitate referral to a men-tal health practitioner or a community-based earlyintervention program.
Assessing stability and changein young children’s behavioraland developmental problems
As shown in the following clinical problem,the DSM-PC can also be used to assess stabil-ity versus change over time in the severity ofinfants’ and preschoolers’ behavioral and de-velopmental problems.
Case illustration
Johnny is a 15-month-old child whose motherhas been concerned about the fact that he hasshown increased separation anxiety over the pastfew months. An interview revealed that his motherhas recently taken a part-time job and the in-crease in Johnny’s separation anxiety coincidedwith this event. According to the DSM-PC, this
would be coded as developmental variation anx-iety, “which is defined as fears and worries thatare appropriate for developmental age and do notaffect normal development.”
What if Johnny, who is now 3 years old, con-tinues to demonstrate separation anxieties thathave now become more pervasive? He can’t lethis mother out of his sight, becomes very upset,having temper tantrums when she leaves him. Heis unable to attend preschool because of his anx-ieties. His mother is very stressed by this prob-lem and has taken time off work to help manageit. The parents disagree about how to handleJohnny’s problem, which is causing increasedmarital strain. Johnny’s anxiety problem now fitsthe diagnosis of an anxiety problem, defined as“excessive worry or fearfulness that causes sig-nificant distress in the child, but does not meet thethreshold for a DSM-IV diagnosis.” At this point intime, the PCP might make a referral to a men-tal health provider for management of Johnny’sanxiety.
What if Johnny’s anxiety did not respond to in-tervention and he again presents at age 5 withanxiety-related symptoms, which have intensi-fied? He now demonstrates the following symp-toms: persistent and excessive worry about los-ing and possible harm coming to his mother andfather, persistent refusal to go to preschool be-cause of separation concerns, persistent fears ofbeing alone, and persistent refusal to go to sleepwithout being near his mother. His symptoms nowmeet threshold for a separation anxiety disorderbased on the DSM-IV and would warrant moreintensive treatment such as cognitive-behavioralintervention, parental guidance, medication, or acombination of treatments.
Identifying stressful situations thataffect the prognosis and managementof young children’s behavioral anddevelopmental problems
The “Environmental Situations” section ofthe DSM-PC was designed to help practition-ers identify stressful situations that might in-fluence the expression, impact, and prognosisof children’s behavioral and developmentalproblems. The codes for Environmental Sit-uations can be used to describe the focusof clinical encounters in which parents, chil-dren, or other family members are counseledto manage the impact of stressful situations

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
Role of the DSM-PC 121
(eg, parental divorce). By identifying clinicallyrelevant stressful situations, practitioners canassess potential psychological risks to infantsand young children that are associated withknown environmental stressors and monitorthe impact over time on the clinical manage-ment and prognosis of behavioral problems.For example, consider the case of the 18-month-old overly shy child, Sally, describedearlier. What if the family practitioner learnedthat Sally’s family had severe marital problemsand that her mother was being abused by thechild’s father? Such information would clearlyincrease the level of professional concern andnecessitate a number of additional interven-tions such as counseling her mother about theneed to protect Sally and referral to a shelterfor battered women.
Promoting a shared language forinterdisciplinary collaboration,consultation, and training
Another relevant application of the DSM-PC concerns its potential use in promoting ashared language for collaboration and consul-tation among pediatricians and practitionersfrom a range of disciplines. The DSM-PC in-cludes terms and concepts (eg, developmen-tal variation and problems) that can be readilyunderstood and do not depend on a specificprofessional or theoretical orientation. Forthis reason, PCPs and other practicing clini-cians can use the DSM-PC to facilitate referralto other professionals by specifying the sever-ity of a particular presenting problem and clar-ifying the need for interdisciplinary evaluationand management.
My experiences have indicated that theDSM-PC can be a very useful tool to trainpsychologists and mental health professionalswho work in pediatric settings to understandthe full range of clinical problems and en-vironmental stressors seen in children whenproviding consultation to PCPs. Because theDSM-PC emphasizes the concept of a devel-opmental continuum of behavioral problems,it is also quite compatible with teaching con-cepts of child development and developmen-tal psychopathology and has been used for
this purpose in undergraduate level coursesat Case Western Reserve University.
Monitoring community-basedpreventive intervention foryoung children at risk
One of the most interesting future ap-plications of the DSM-PC from a publichealth standpoint concerns its potential to beused to target and monitor interdisciplinary,community-based preventive intervention forchildren at risk (Perrin & Stancin, 2002). Be-cause the DSM-PC uses nontechnical languageand is not tied to profession-specific diagnos-tic classification language, as is the case withthe DSM-IV, it has the potential to be used totarget and monitor interventions for infantsand young children who are showing earlysigns of developmental and/or mental healthproblems and may be at risk for developingclinically significant developmental and/ormental disorders when they become older.In order to implement such community-basedmonitoring, the DSM-PC should be closelyintegrated with developmentally appropriatescreening and assessment techniques (Nickel& Squires, 2002).
Communicating with parentsabout their infants’ behavioraland developmental problems
The language of the DSM-PC describes arange of young children’s presenting prob-lems based on content categories and lev-els of severity that can be used to give par-ents feedback about their children’s problemsand a rationale for a recommended manage-ment approach. For example, in cases of lesssevere symptoms that are nevertheless dis-tressing to family members, parents can behelped to learn that their infants’ problemsreflect average expectable developmentalvariations, such as individual differences intemperament. On the other hand, for moreserious problems, the DSM-PC can also beused to help clarify the need for a referral toa mental health professional to parents (eg,that the child’s symptoms are persistent, se-vere enough to cause distress in the family,

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
122 INFANTS AND YOUNG CHILDREN/APRIL–JUNE 2004
and are more severe than expected develop-mental variations for the child’s age).
Limitations of the DSM-PC anddiagnostic systems for use withinfants and young children
Several limitations of the DSM-PC should beconsidered. For example, the DSM-PC doesnot address parent-child relational problems,which may be the focus of clinical attentionfor any number of infants and young childrenwho present to PCPs and other professionals.Second, the DSM-PC provides relatively lim-ited coverage of the spectrum of developmen-tal problems and delays that are seen by practi-tioners who see infants and young children. Athird limitation is that while the DSM-PC doesoffer an option to practitioners for diagnosticcoding of young children’s problems that donot reach threshold for a DSM-IV diagnosis,it does not provide an alternative to the diag-noses provided in the DSM-IV nomenclature.Finally, the DSM-PC does not provide specificinformation concerning how best to use it inpractice (eg, instruments to be used and/or in-terventions).
Practitioners who apply the DSM-PC shouldalso consider the limitations of using any di-agnostic system, including the DSM-PC, withinfants and young children. These include po-tential stigma and impact of diagnostic labelson parents and the importance of culturalvariations in parental recognition and report-ing of young children’s problems and symp-toms and acceptance of diagnostic informa-tion from professionals.
RECOMMENDATIONS TO ENHANCEAPPLICATIONS OF THE DSM-PC WITHINFANTS AND YOUNG CHILDREN
The DSM-PC is a promising system for theclassification of children’s behavioral and de-velopmental problems in pediatric and fam-ily practice settings (Wolraich, 1997). Thismethod also has potential for broader uti-lization among professionals, especially thosewho work with infants and young childrenand their parents. Barriers to such utiliza-
tion include lack of professional awarenessof the potential use of the DSM-PC, limitedreimbursement for its use, and a limited re-search base to support the use of the DSM-PC (Wolraich, 1997). A number of strategiesare needed to facilitate greater utilization ofthe DSM-PC including the following: contin-ued dissemination of information concerningthe DSM-PC, especially applications in prac-tice settings, promotion of reimbursement foruse of the DSM-PC, and development of re-search using the DSM-PC.
Disseminating information concerningthe DSM-PC and application in practicesettings
The DSM-PC is available from AmericanAcademy of Pediatrics Publications, PO Box127, 141 Northwest Point Blvd, Elk Grove Vil-lage, IL 60009. Many professionals are stillnot familiar with the DSM-PC and its poten-tial applicability to practice, teaching, and re-search; consequently, one strategy will be topromote awareness of the DSM-PC by dissem-inating information in professional meetingsand articles in professional journals. Somespecific methods have also been developedto facilitate the utilization of the DSM-PC,such as an application of the DSM-PC viacomputerized interviews for parents (Drotar,Sturner, Nobile in press). Moreover, screeningprocedures for behavioral and developmentalproblems are quite compatible with use of theDSM-PC (Perrin & Stancin, 2002).
Methods of training professionals to use theDSM-PC have been developed that can be ap-plied in different settings. One example isthe use of videotapes of parent interviewsthat illustrate common presenting problems(Drotar, 1999). Practitioners can view thesevideotapes and use the DSM-PC to codethe behavioral problems and environmen-tal stressors that they have observed in theinterviews.
Promoting reimbursement for usingthe DSM-PC and other relevantdiagnostic coding systems
The limited reimbursement that pediatri-cians and other professionals receive for their

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
Role of the DSM-PC 123
assessment and management of infants’ andyoung children’s behavioral and developmen-tal problems, including problems coded bythe DSM-PC, are powerful barriers to theiruse (Rappo, 1997). Consequently, an impor-tant strategy to promote reimbursement forprofessional use of the DSM-PC will be to ed-ucate third-party payers concerning the po-tential of the DSM-PC to document clinicalpractices concerning the management of be-havioral and developmental problems in in-fants and young children, including criteriafor referral of behavioral problems to mentalhealth professionals (Rappo, 1997). As moreand more practitioners use the DSM-PC anddevelop a track record of use in various set-tings, more data can eventually be providedto insurance companies. Moreover, it is possi-ble that use of the DSM-PC may enhance theefficiency of referrals for young children withmental health problems from PCPs and ulti-mately reduce the costs of mental health careby encouraging earlier, more informed refer-ral to early intervention services. However,this remains to be demonstrated.
Research applications of the DSM-PC
One of the most important future needsconcerns research concerning various appli-cations of the DSM-PC. One of the most im-portant of these areas is to test the hypothe-sis, which is a central working assumption ofthe DSM-PC, that training pediatricians and/orother professionals to use the DSM-PC will re-sult in increased recognition of behavioral anddevelopmental problems and improved man-agement.
Because the DSM-PC can classify the broadrange of problems that present in primarycare settings, it also provides a potential toolto conduct collaborative descriptive researchconcerning the incidence, prevalence, and
course of developmental and behavioral prob-lems in infants and young children. With somenotable exceptions (Lavigne et al., 1993),such data are very limited. The DSM-PC canalso be used to document the patterns of sta-bility versus change in common behavioraland developmental problems among infantsand young children and to find out how suchproblems respond to various interventions.Other areas for future research applicationsconcern how the DSM-PC categories relateto those used in other systems. For exam-ple, do children who present with develop-mental problems and variations according tothe DSM-PC also present with relationship dis-orders according to the Diagnostic Classifi-cation 0–3? Do children who are identifiedas having problems according to the DSM-PCand who do not receive appropriate interven-tion go on to develop disorders according tothe DSM-IV?
Finally, the DSM-PC can be used to doc-ument the incidence, prevalence, and di-agnostic and treatment patterns concerningyoung children’s behavioral and developmen-tal problems that are at subthreshold levelfor a DSM-IV or Diagnostic Classification0–3 diagnosis but nonetheless reflect substan-tial functional impairment (Angold, Costello,Farmer, Burns, & Erkanli, 1999). The needsof such children for early diagnosis and pre-ventive clinical management underscore theneed for a comprehensive, public health ap-proach to the mental health and developmen-tal problems of infants and young children(Palfrey, Singer, Walker, & Butler, 1987). In or-der to implement such an approach, it wouldbe important to integrate the use of DSM-PC with modern methods of developmentalscreening (Palfrey et al., 1987) and a compre-hensive, community-based approach to earlychildhood mental health services (Knitzer,2000).
REFERENCES
American Psychiatric Association. Diagnostic and statis-tical manual of mental disorders (4th ed.). Washing-ton, DC: Author. 1995.
Angold, A., Costello, E. J., Farmer, E., Burns, B. J., &
Erkanli, A. (1999). Impaired but undiagnosed. Journalof American Academy of Child and Adolescent Psy-chiatry, 38, 129–137.
Costello, E. J. (1986). Primary care pediatrics and child

LWW/IYC AS265-03 February 13, 2004 3:45 Char Count= 0
124 INFANTS AND YOUNG CHILDREN/APRIL–JUNE 2004
psychopathology: A review of diagnostic, treatment,and referral practices. Pediatrics, 78, 1044–1051.
Costello, E. J., Edelbrock, C., Costello, A. J., Dulcan, M.K., Burns, B. J., & Brent, D. (1988). Psychopathologyin pediatric primary care: The new hidden morbidity.Pediatrics, 82, 415–424.
Drotar, D. (1999). The Diagnostic and Statistical Manualfor Primary Care (DSM-PC) Child and Adolescent Ver-sion: What pediatric psychologists need to know. Jour-nal of Pediatric Psychology, 24, 369–380.
Drotar, D. (2002). Behavioral and emotional problems ininfants and young children: Challenges of clinical as-sessment and intervention. Infants & Young Children,14, 1–5.
Drotar, D., Sturner, R., & Nobile, C. (in press). Diagnos-ing and managing behavioral and developmental prob-lems in primary care: Applications of the DSM-PC. InB. G. Wildman, & T. Stancin (Eds.) Treating children’spsychosocial problems in primary care. Westport,CT: Greenwood Press.
Horwitz, S. M., Leaf, P. J., Leventhal, J. M., Forsythe, B.,& Speechley, K. N. (1992). Identification and man-agement of psychosocial and developmental problemsin community-based, primary care pediatric practices.Pediatrics, 89, 480–485.
Jensen, V. K., & Sinclair, L. V. (2002). Treatment of autismin young children: Behavioral intervention in appliedbehavior analysis. Infants & Young Children, 14, 42–53.
Kelleher, K., & Rickert VI. Management of pediatric men-tal disorders in primary care. In: J. Miranda, A. A.Hohmann, C. C. Attkinson, D. B. Larson, (Eds.), Men-tal disorders in primary care (pp. 320–346). SanFrancisco: Jossey Bass; 1994.
Knitzer, J. Early childhood mental health services: A pol-icy and systems development perspective. In J. P.Shonkoff, S. J. Meisals (Eds.), Handbook of early child-hood intervention (pp. 416–439). New York: Cam-bridge University Press. 2000.
Lavigne, J. V., Binns, J. H., Christoffel, K. K., Rosenbaum,D. L., Arendt, R., Smith, K., et al. (1993). Behavioraland emotional problems among preschool children inpediatric primary care: Prevalence and pediatricians’recognition. Pediatrics, 91, 649–655.
Lieberman, A. F., & Zennah, C. H. (1995). Disorders ofattachment in infancy. Child and Adolescent Psychi-atric Clinics of North America, 4, 571–587.
MacLean, W. F., & Symons, F. (2002). Self-injurious behav-ior in young children. Infants & Young Children, 14,31–41.
Neary, E. M., & Eyberg, S. M. (2002). Management of dis-ruptive behavior in young children. Infants & YoungChildren, 14, 53–67.
Nickel, R. E., & Squires, J. Developmental screening andsurveillance. In: R. E. Nickel, L. W. Desch (Eds.), Thephysician’s guide to caring for children with disabil-ities and chronic conditions (pp. 15–27). New York:Paul H. Brookes Publishing Co. 2000.
Palfrey, J. S., Singer, J. D., Walker, D. K., & Butler, J. A.(1987). Early identification of children’s special needs:A study in the metropolitan communities. Journal ofPediatrics, 111, 651–659.
Perrin, E., & Stancin, T. (2002). A continuing dilemma:Whether and how to screen for concerns about chil-dren’s behavior. Pediatrics in Review, 23, 264–278.
Rappo, P. D. (1997). Use of DSM-PC and implications forreimbursement. Journal of Developmental and Be-havioral Pediatrics, 18, 175–177.
Robinson, J. R. (2002). Attachment problems and disor-ders in infants and young children. Identification, as-sessment and intervention. Infants & Young Children,14, 6–18.
Wolraich, M. L. (1997). Diagnostic and Statistical Manualfor Primary Care (DSM-PC) Child and Adolescent Ver-sion: Design, intent, and hopes for the future. Jour-nal of Developmental and Behavioral Pediatrics, 18,171–172.
Wolraich, M. L., Felice, M. E., Drotar, D. (Eds). The classi-fication of child and adolescent mental diagnosis inprimary care: Diagnosis and Statistical Manual forPrimary Care (DSM-PC) Child and Adolescent Ver-sion. Elk Grove, IL: American Academy of Pediatrics.1996.
Zero to Three/National Center for Infant Programs. Diag-nostic classification: 0–3. Diagnostic classificationof mental health and developmental disorders ofinfancy and early childhood. Arlington, VA: Author.1994.
Current articles: http://depts.washington.edu/isei/iyc/iyc_comments.html
Back to the list of previous articles:http://depts.washington.edu/isei/iyc/iyc_previous.html
Related Documents











