PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [University of Pittsburgh] On: 29 June 2009 Access details: Access Details: [subscription number 906385000] Publisher Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Disability and Rehabilitation: Assistive Technology Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t741771157 Design, development and testing of a low-cost electric powered wheelchair for India Jon Pearlman ab ; Rory Cooper ab ; H. S. Chhabra c ; Alexandra Jefferds ab a Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, Pittsburgh, PA, USA b Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA, USA c Indian Spinal Injuries Center, New Delhi, India Online Publication Date: 01 January 2009 To cite this Article Pearlman, Jon, Cooper, Rory, Chhabra, H. S. and Jefferds, Alexandra(2009)'Design, development and testing of a low-cost electric powered wheelchair for India',Disability and Rehabilitation: Assistive Technology,4:1,42 — 57 To link to this Article: DOI: 10.1080/17483100802338440 URL: http://dx.doi.org/10.1080/17483100802338440 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [University of Pittsburgh]On: 29 June 2009Access details: Access Details: [subscription number 906385000]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Disability and Rehabilitation: Assistive TechnologyPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t741771157
Design, development and testing of a low-cost electric powered wheelchair forIndiaJon Pearlman ab; Rory Cooper ab; H. S. Chhabra c; Alexandra Jefferds ab
a Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, Pittsburgh, PA, USA b
Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA, USA c IndianSpinal Injuries Center, New Delhi, India
Online Publication Date: 01 January 2009
To cite this Article Pearlman, Jon, Cooper, Rory, Chhabra, H. S. and Jefferds, Alexandra(2009)'Design, development and testing of alow-cost electric powered wheelchair for India',Disability and Rehabilitation: Assistive Technology,4:1,42 — 57
To link to this Article: DOI: 10.1080/17483100802338440
URL: http://dx.doi.org/10.1080/17483100802338440
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

PRODUCTS AND DEVICES
Design, development and testing of a low-cost electric poweredwheelchair for India
JON PEARLMAN1,2, RORY COOPER1,2, H. S. CHHABRA3 & ALEXANDRA JEFFERDS1,2
1Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, Pittsburgh, PA, USA, 2Department of
Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA, USA, and 3Indian Spinal Injuries Center,
New Delhi, India
Accepted July 2008
AbstractPurpose. To design and develop an appropriate, low-cost electric powered wheelchair (EPW) for the Indian subcontinent.Method. We performed the following multi-phase design process: (1) Conceptual design; (2) System design, Prototype Ifabrication, focus group testing with Indian stakeholders (n¼ 29); (3) System re-design, Prototype II fabrication and usertrials with US (n¼ 5) and Indian (n¼ 25) subjects.Results. (1) Preliminary investigations revealed that a conventional EPW design was infeasible due to the high componentcost. Instead, we constrained our design to incorporate a single drive motor and manual steering, with the option ofupgrading to power steering where economically feasible. (2) The first prototype was fabricated out of easily available, low-cost materials. Focus group testing demonstrated feasibility of the design and revealed differences between stakeholdergroups. (3) Prototype II incorporated feedback from the first focus group and a needs assessment. US subjects providedvaluable design advice prior to the India trials. Indian subjects travelled further in the SIMPL-EPW than their own manualwheelchair (MWC). Depending on spinal injury level, Indian subjects found the entire (tetraplegia) or outdoor portion(paraplegia) of the obstacle course significantly less challenging in the SIMPL-EPW compared with their own MWC.Conclusions. We demonstrated a useful and successful multi-phase design approach for developing assistive technology fordeveloping regions.
Introduction
There is a tremendous need for assistive technologies
(ATs) to improve the quality of life for people with
disabilities (PWD) in developing countries. The need
for wheelchairs (WC), for example, is estimated to be
anywhere between 20 million [1] and 100 million [2].
The World Health Organisation (WHO) estimates that
10% of any population has a disability, and 10% of these
individuals could benefit from a WC [3]. Using these
values, there are approximately 66 million potential WC
users world-wide. In India, a large and developing
country, the WHO estimate suggests that there are
approximately 10 million potential WC users, which is
corroborated by India’s most recent country-wide
census [4]. Unfortunately, because of factors including
an underdeveloped healthcare system, stigmas and
stereotypes associated with disability, and the below-
average income of most PWD in India [5], the need for
suitable WC is unmet [6].
There have been promising developments to help
equalise the rights of PWD by improving their access
to healthcare and AT, as well as reducing the stigma
associated with their disability. The most encoura-
ging development was the recent passage of the
United Nations (UN) Convention on the Rights of
PWD (UN-CRPD) [7], and the ratification of the
document by several countries (including India).
Personal Mobility (Article 20), of the UN-CRPD
mandates that countries provide a choice of high-
quality, affordable devices for PWD. Although
Article 20 is a necessary step to provide PWD the
devices they need, in the WC industry, it represents a
significant challenge.
Considering the tremendous unmet need for
WCs, as well as evidence of poor performance of
Correspondence: Jon Pearlman, PhD, Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, 7180 Highland Drive Building 4, 151R-
1H, Pittsburgh, Pennsylvania, 15206 USA. Tel: þ412-365-4850. Fax: þ412-365-4858. E-mail: [email protected]
Disability and Rehabilitation: Assistive Technology, January 2009; 4(1): 42–57
ISSN 1748-3107 print/ISSN 1748-3115 online ª 2009 Informa Healthcare USA, Inc.
DOI: 10.1080/17483100802338440
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009
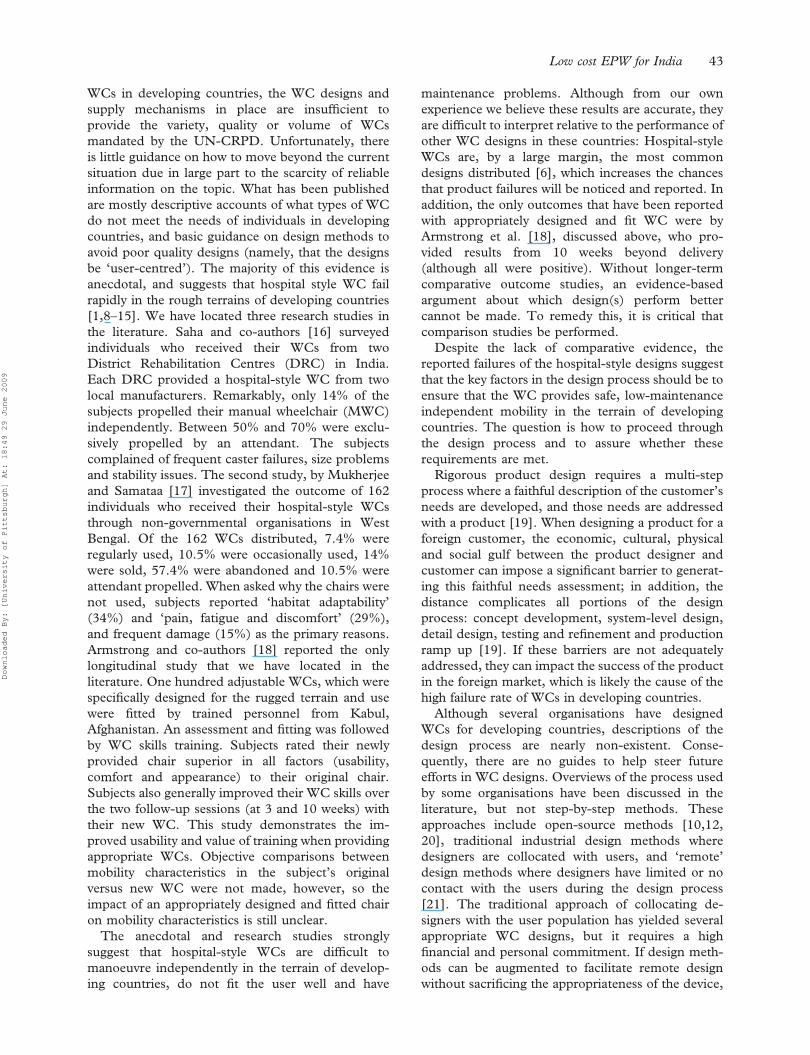
WCs in developing countries, the WC designs and
supply mechanisms in place are insufficient to
provide the variety, quality or volume of WCs
mandated by the UN-CRPD. Unfortunately, there
is little guidance on how to move beyond the current
situation due in large part to the scarcity of reliable
information on the topic. What has been published
are mostly descriptive accounts of what types of WC
do not meet the needs of individuals in developing
countries, and basic guidance on design methods to
avoid poor quality designs (namely, that the designs
be ‘user-centred’). The majority of this evidence is
anecdotal, and suggests that hospital style WC fail
rapidly in the rough terrains of developing countries
[1,8–15]. We have located three research studies in
the literature. Saha and co-authors [16] surveyed
individuals who received their WCs from two
District Rehabilitation Centres (DRC) in India.
Each DRC provided a hospital-style WC from two
local manufacturers. Remarkably, only 14% of the
subjects propelled their manual wheelchair (MWC)
independently. Between 50% and 70% were exclu-
sively propelled by an attendant. The subjects
complained of frequent caster failures, size problems
and stability issues. The second study, by Mukherjee
and Samataa [17] investigated the outcome of 162
individuals who received their hospital-style WCs
through non-governmental organisations in West
Bengal. Of the 162 WCs distributed, 7.4% were
regularly used, 10.5% were occasionally used, 14%
were sold, 57.4% were abandoned and 10.5% were
attendant propelled. When asked why the chairs were
not used, subjects reported ‘habitat adaptability’
(34%) and ‘pain, fatigue and discomfort’ (29%),
and frequent damage (15%) as the primary reasons.
Armstrong and co-authors [18] reported the only
longitudinal study that we have located in the
literature. One hundred adjustable WCs, which were
specifically designed for the rugged terrain and use
were fitted by trained personnel from Kabul,
Afghanistan. An assessment and fitting was followed
by WC skills training. Subjects rated their newly
provided chair superior in all factors (usability,
comfort and appearance) to their original chair.
Subjects also generally improved their WC skills over
the two follow-up sessions (at 3 and 10 weeks) with
their new WC. This study demonstrates the im-
proved usability and value of training when providing
appropriate WCs. Objective comparisons between
mobility characteristics in the subject’s original
versus new WC were not made, however, so the
impact of an appropriately designed and fitted chair
on mobility characteristics is still unclear.
The anecdotal and research studies strongly
suggest that hospital-style WCs are difficult to
manoeuvre independently in the terrain of develop-
ing countries, do not fit the user well and have
maintenance problems. Although from our own
experience we believe these results are accurate, they
are difficult to interpret relative to the performance of
other WC designs in these countries: Hospital-style
WCs are, by a large margin, the most common
designs distributed [6], which increases the chances
that product failures will be noticed and reported. In
addition, the only outcomes that have been reported
with appropriately designed and fit WC were by
Armstrong et al. [18], discussed above, who pro-
vided results from 10 weeks beyond delivery
(although all were positive). Without longer-term
comparative outcome studies, an evidence-based
argument about which design(s) perform better
cannot be made. To remedy this, it is critical that
comparison studies be performed.
Despite the lack of comparative evidence, the
reported failures of the hospital-style designs suggest
that the key factors in the design process should be to
ensure that the WC provides safe, low-maintenance
independent mobility in the terrain of developing
countries. The question is how to proceed through
the design process and to assure whether these
requirements are met.
Rigorous product design requires a multi-step
process where a faithful description of the customer’s
needs are developed, and those needs are addressed
with a product [19]. When designing a product for a
foreign customer, the economic, cultural, physical
and social gulf between the product designer and
customer can impose a significant barrier to generat-
ing this faithful needs assessment; in addition, the
distance complicates all portions of the design
process: concept development, system-level design,
detail design, testing and refinement and production
ramp up [19]. If these barriers are not adequately
addressed, they can impact the success of the product
in the foreign market, which is likely the cause of the
high failure rate of WCs in developing countries.
Although several organisations have designed
WCs for developing countries, descriptions of the
design process are nearly non-existent. Conse-
quently, there are no guides to help steer future
efforts in WC designs. Overviews of the process used
by some organisations have been discussed in the
literature, but not step-by-step methods. These
approaches include open-source methods [10,12,
20], traditional industrial design methods where
designers are collocated with users, and ‘remote’
design methods where designers have limited or no
contact with the users during the design process
[21]. The traditional approach of collocating de-
signers with the user population has yielded several
appropriate WC designs, but it requires a high
financial and personal commitment. If design meth-
ods can be augmented to facilitate remote design
without sacrificing the appropriateness of the device,
Low cost EPW for India 43
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

then presumably more design professionals would be
willing to address the overwhelming need for
appropriate WCs. Advances in communication
technology, as well as a surge of interest in socially
responsible engineering may help make this a reality.
Remote design methods for WCs are best devel-
oped based on the successes and failures of past
projects. Unfortunately, while WC designs have been
described and provide useful design examples
[13,22–24], the design process has not been well
described. Mulholland and colleagues published the
most comprehensive series of articles on the R&D of
a mobility device for developing countries. In their
first study, assessments were performed in India [25]
to understand the needs of Indian women with
disabilities. Their second study [26] details the
design of a mobility device to meet the needs of the
Indian women. In their final study, Mulholland
describes the focus groups that were performed with
the device [27] in India. Although she performed a
thorough needs assessment, she found that there
were mixed responses to the device. This result
could be for several reasons, including the few focus
group participants (n¼ 8), and the fact that other
stakeholders such as clinicians and manufacturers
where not part of the focus groups. These efforts
mark a first step toward evidence-based practice of
design and development of mobility devices for
developing countries.
The goal of this study was to build on the work of
Mulholland and colleagues by describing our ap-
proach to and our experience with a research and
design project to develop an electric powered wheel-
chair (EPW) for Indian users. We augmented a
traditional design strategy in several ways to
accommodate the physical distance between the
designers and customers to ensure faithful needs
assessment were performed. We hope that our work
provides guidance for others and encourages design
projects to be documented and the information
disseminated.
Methods
Phase I: concept generation
As an initial step, we worked with an Indian native
who was a visiting researcher in our laboratories, and
asked him to develop a preliminary design brief for
an EPW for Indian users. The brief included several
aspects of the product, including engineering speci-
fications such as geometric size, obstacle climbing
ability and price point. Based on the results of this
brief, we performed several short research projects to
better understand the implications of some the
design specifications, especially related to the re-
quirement that the EPW be very cost effective
(5US$1000), highly manoeuvrable in rough terrain
and highly durable.
Project I.A: motor component-level and system-level
testing. To maintain a low cost for the device, we
planned to use locally available hub motors as the
propulsion source – these are low-cost and widely
available in India. The goal of this project was to
subject a hub-motor supplied by an Indian colla-
borator to international WC durability standards
[28] to assess its performance (Figure 1, Left). After
durability testing was completed, we adapted the
motors to an existing low-cost, highly manoeuvrable
EPW sold in the US to test the feasibility of the
motors (Figure 1, Right).
Project I.B: price-point analysis based on Indian income
levels. To approximate the sensitivity of the EPW
market size to price, we performed an analysis using
the most recent Indian census data [4] to determine
the approximate market share for three prices (in
US$): $500, $750, $1000. We made several assump-
tions. First, we used relative percentage of EPW
users in the US population [29] to predict the
expected overall market size. Second, we assumed
that a family would purchase an EPW if they could
Figure 1. Candidate Motor for EPW being durability tested (left) Hub motor adapted to an Invacare M50 (right).
44 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

afford financing the device over a 3 year period with
their disposable income. Finally, we assumed that
families eligible for a government subsidy for WCs
[30] would use it to offset the price of the EPW.
Project I.C: material testing of Indian low-carbon steel.
The structural integrity of a WC depends on the
strength and durability of the underlying material.
Engineers typically refer to published material
properties to determine which failure modes are
most likely so they can design accordingly. When
fabricating a prototype for a remote region, it is
important to determine if these published material
properties reflect the properties of the indigenous
materials [31]. To investigate whether these differ-
ences exist, we performed elongation-to-failure and
indentation tests on US and Indian low-carbon steel.
Dog-bone specimens were cut from 2.54 cm tubular
steel and secured to custom clamps fixed to a
uniaxial Instron materials testing machine. Load-
displacement curves were generated with three
specimens of the metal from each country (Figure
2). Indentation tests as well as images of the
microstructure were also recorded. We used de-
scriptive statistics to report the results of this work.
Our design was brief and the results from the
above projects persuaded us to move away from
current EPW designs due to their high component
costs and the unsatisfactory trade-off between dur-
ability and price [32]. Instead, we focused on designs
that would reduce these component costs and still
meet the performance specifications. These costs,
especially in regions where metal fabrication, up-
holstery and assembly are inexpensive, are heavily
weighted toward the electrical components: the
controller, two drive-motors and two batteries. To
limit these expenditures, we constrained our design
to use a single drive motor and require manual
steering, with the option of upgrading to a power
steering system when economically feasible. We also
emphasised locally available components and mate-
rials, when possible, and limited the manufacturing
techniques to those widely available in India. We
named the device the single motor propelled EPW,
or SIMPL-EPW.
Phase II: system-level design, prototype fabrication and
testing
A single engineer (the first author) led the design
process, which was reviewed and discussed in several
informal personal and group meetings with engi-
neers, technicians and clinicians in the US. The
design process was largely unstructured, and the final
design evolved from use of informal sketches, small
mock-ups of the frame and suspension system, and
use of Solidworks to model more complicated
structures of the EPW (such as the steering system).
Several graduate and undergraduate students from
the engineering and rehabilitation sciences assisted
with aspects of the work. The final design was
modelled in Solidworks, and the SIMPL-EPW(1.0)
prototype was fabricated as an operational proof-of-
concept device (rather than a pre-production
model).
To gather feedback about the device, we shipped
the SIMPL-EPW(1.0) to India and performed IRB-
approved focus groups with stakeholders: potential
users, clinicians and manufacturers. These focus
groups were held in New Delhi at the Indian Spinal
Injury Centre during the International Spine &
Spinal Injuries Conference in 2006, and in Kanpur,
at the headquarters of the Artificial Limbs Manu-
facturing Corporation of India. After subjects pro-
vided informed consent for this IRB-approved
protocol, the SIMPL-EPW(1.0) features were de-
scribed and subjects were asked if they would like to
test-drive the device (all agreed). After test-driving
the device, the subjects filled out a questionnaire and
ranked the SIMPL-EPW(1.0) on several factors.
Finally, the subjects answered open-ended questions
in a video-taped interview. We used descriptive
statistics to analyse the results. Based on the mostly
positive feedback, we adopted the basic design, and
advanced to the next design stage.
Phase III: detailed design, prototype II development and
testing
III.A Design upgrades. Two sources of information
were used to guide the design modifications for the
second prototype. First, we catalogued the feedback
from the focus groups held in India which suggestedFigure 2. Dogbone specimen and clamp used for load-deflection
testing of Indian and US steel.
Low cost EPW for India 45
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

a redesign of the steering interface, improvements in
the aesthetics and improvements in the performance.
Second, we integrated results from an ethnographic
study we performed in parallel [33], where Indian
WC users took photographs in and around their
homes with disposable cameras and the photos were
incorporated into an online questionnaire. We
recruited WC experts from around the world to
gauge the accessibility barriers, which were portrayed
in a random selection of the (*500) photos. Subjects
were also asked to provide advice on the design
features and specifications necessary for the EPW to
overcome the accessibility barriers portrayed in the
photos. Results from this study were used to guide
design modifications for the second prototype. In
contrast to the first prototype, we fabricated all of the
non-electrical SIMPL-EPW(2.0) components in our
machine shop. We restricted the fabrication tools to
those would be readily available in India to ensure
that the design could be manufactured in low-
volume workshops in India.
III.B Testing. We tested the SIMPL-EPW(2.0) with
users in the US to gather final design feedback before
the India-based testing. We recruited subjects with
EPW experience to use the SIMPL-EPW(2.0) to
perform a series of tasks: enter/exit/operate an
elevator; approach and use a computer at a desk;
approach and use a kitchen sink; enter and leave a
bathroom and drive over rough terrain. After each
task, subjects were asked a series of questions about
the difficulty of completing the task and what design
upgrades could improve the performance of the
SIMPL-EPW(2.0). A final questionnaire was com-
pleted by each subject to rank the SIMPL-EPW(2.0)
on several different features and performance dimen-
sions. The trial was audio-recorded and transcribed
to document all design ideas.
Final design upgrades were performed on the
SIMPL-EPW(2.0) before it was transported to New
Delhi, India. Testing of the device was performed at
ISIC in February – April 2007. We recruited
potential EPW users in an IRB approved comparison
study. After informed consent was given, demo-
graphic information was collected from each subject.
After completing the enrolment, the subject was
scheduled to participate in the study for 2 days within
the span of 1 week. During the first day, we attached
a datalogger [34] to the subject’s manual WC which
non-invasively recorded the distance they traversed
for 3–4 h during their typical daily activities around
ISIC. After the datalogging was completed, the
subject was asked to complete a 100 m obstacle
course (Figure 3), which included both indoor and
outdoor tasks.
Each subject was asked to perform the obstacle
course three times, and the duration of each trial was
recorded using a stopwatch. The researcher provided
assistance to the subjects when requested, and
recorded the number of times assistance was
provided in each trial. After the first and third trial,
the subject completed a questionnaire which had a
series of 14 cm horizontal lines for each task in the
obstacle course. The subject was asked to place a
mark along each line according to how difficult the
task was to accomplish (the left margin being ‘easy’).
The identical protocols were followed for the
second day, although the subject used the SIMPL-
EPW(2.0) rather than their own manual WC for their
daily activity tasks and the obstacle course trials.
Figure 3. Obstacle course layout at ISIC.
46 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

Most commonly, the researcher met the subject in
the morning and demonstrated the SIMPL-EPW(2.0)
controls and other features. The subject then
transferred into the device and the seating system
was adjusted for comfort. The datalogger was fixed
to the wheel of the SIMPL-EPW(2.0) and the user
was allowed to carry out their daily activity tasks in
the device. In the afternoon (typically after lunch),
the subject would return and navigate through the
obstacle course three times. After completing the
third trial of the obstacle course and required
questionnaires, a final questionnaire was adminis-
tered to gather directed and open-ended feedback
about the SIMPL-EPW(2.0).
We used a two-tailed paired-sample t-test to
determine if the distance the subject travelled during
their daily activities was sensitive to the device used
(SIMPL-EPW(2.0) or their own MWC). Because
normality requirements were not satisfied, we used a
non-parametric Wilcoxon rank-sum [35] to test if
trial duration was sensitive to repeated trials, injury
level or device.
A single researcher used a ruler to measure the
location (in millimeters) of the marks placed by the
user along each of the horizontal lines of the
questionnaire to gauge course difficulty. The data
were digitised and three cumulative ‘difficulty’ scores
were calculated: indoor, outdoor and complete
course. Because of non-normality, we used a
Wilcoxon rank-sum test to determine if there were
significant differences in the perceived difficulty of
the obstacle course between the first and third trials,
which would indicate a learning effect. We also used
a Wilcoxon rank-sum test to determine if the
cumulative scores (total, indoor and outdoor) were
sensitive to the device used and injury level. Finally,
we used Wilcoxon rank-sum tests to determine if the
frequency of required assistance was sensitive to the
device used, injury level, or trial number. In all cases,
if trial number was significant we interpreted it as a
learning effect, and discarded the data from the first
trial, which we considered less reliable.
Results
Phase I: conceptual generation
The preliminary design brief, developed by an Indian
native who is familiar with both EPWs and the built
and un-built environments in India is presented
below (Table II).
Project I.A: motor component-level and system-level
testing. When we performed simulated ISO durability
testing on the same motors, we found that the axle-
strength was not sufficient to sustain the abuse from
ISO testing (Figure 1, Left). We found that the hub
motors were a sufficient replacement for higher-cost
gear motors when we adapted them to an EPW
frame (Figure 1, Right).
Project I.B: price-point analysis based on Indian income
levels. Using target prices of $500, $750 and $1000,
our market analysis predicted the size of the EPW
market in India would be would be 152, 68 and 36
thousand units, respectively. Using the number of
units and sales price, these values indicate the market
could be worth $76, $51 and $36 million US dollars,
respectively.
Project I.C: material testing on Indian low-carbon steel.
We found that Indian steel was significantly weaker
than US steel, and its failure properties were less
predictable (Figure 4). When indentation tests were
performed on the materials, the Indian steel indenta-
tion size was larger than could be classified on
traditional tables. The larger grain size of the Indian
Table II. Initial design brief.
Feature Value Comments
Climbing
angle (min)
128 Ramp angle common
to Indian hospitals
Turning radius 2000 Traditional Indian
House spacing
Ground
clearance
400 Height of road
obstacle
Overall
dimensions
3500 long 2000 wide
Obstacle
climbing
height
500 Sidewalks/
footpath height
Weight capacity 230 lb
Caster size 900 To improve
maneuverability
in rough terrain
Drive wheel size 1600 deep-tread
pneumatic
or gel-filled
To allow for
rough terrain
maneuverability
and traction
Cost $800
Other features Suspension,
modular design
Table I. Drive and control system estimated costs for a scooter,
and an EPW.
Device
Scooter EPW
Controller $50 DC R series $220 DC A series
Drive system $440 Fr PoV
trans-axle and motor
$450 DC EPW motors
Total cost $490 $670
DC, dynamic control; Fr, Fracmo.
Low cost EPW for India 47
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

material is the cause of the increased ductility and
reduced strength send in the load-deflection curves.
Phase II: system-level design, prototype I
fabrication and testing
System-level design. A drawback of using a single
motor is that maintaining traction, especially in rough
terrain, requires a unique suspension design. In the
case of a ‘scooter’ design the propulsive force from
the single drive-motor is distributed using a transaxle,
which is a costly component that is not efficient at
distributing propulsive forces. We addressed the
traction problem by using a hub motor as the main
propulsive, braking and turning source, and mount-
ing it on a suspension system which enforces a force-
balance between free-wheeling casters and the hub
motor. As the caster displaces when encountering
rough terrain, force is transferred to the hub-motor
which maintains or increases traction (Figure 5). A
250-watt hub motor (model #280-1342M, Xti Hub
Motor, Rogers, AK, USA) was mounted to a swing-
arm system in the mid-line of the EPW. One end of
the swing-arm pivoted about the large free-wheeling
(back) wheels. The second end of the swing-arm
attached to caster links through a captive spring
system. The caster links pivoted about the uni-strut
frame using a shackle system, and 600 casters where
bolted to caster forks. Load from the user was distri-
buted between the casters and the hub motor nearly
equally. Furthermore, since the force balance must be
maintained, the caster constantly tracks over rough
terrain, maintaining contact with the ground, as well
as applying downward force to the hub motor. The
steering arm projected from one armrest in front of
the user and was operated by either pushing or pulling
the handle. A wigwag throttle was incorporated into
the bottom of the steering arm as the throttle. The
steering arm swung away to allow for transfers.
The frame was built primarily from uni-strut, a
low-carbon steel channel used in commercial build-
ing construction. The seat was borrowed from an old
EPW that we had in our laboratory, and the
controller was adapted from a scooter we had readily
available. The SIMPL-EPW(1.0) (Figure 6) was
completed in January 2006 and shipped to New
Delhi, India. Because of the use of spare parts (seat
and controller), the cost of the prototype was below
$500.
Testing. Twenty-nine subjects (10 consumers, 10
clinicians, 9 manufacturers) participated in the focus
groups and tested the device. User and clinician
feedback was mostly positive about the device
Figure 4. Load-deflection curve of Indian (dashed line) and US steel (solid line), and images of the microstructure and indentation tests
(above).
48 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

(Figure 7) except for the steering system, which
most consumers found was too stiff. Open-ended
discussions about the steering system suggested it
would be difficult for many users who had trunk-
instability, since they would not be able to both push
and pull the steering arm to turn. Users and clinicians
did not have any strong opinions regarding the
comfort of the EPW and how it compared with other
EPWs they had tried. Manufacturer’s had mixed,
and in some cases, conflicting opinions about the
EPW (Figure 7, horizontal bars). Although the
manufacturers were confident that they could
fabricate and sell the device in India, they thought
the overall price and the components would be
expensive and many would need to be imported.
Manufacturers were generally neutral about whether
they could fabricate the steering system and whether
the EPW had a pleasing appearance and was
comfortable.
Phase III: detailed design, prototype II development and
testing
Using feedback the feedback from Phase II, as well as
information gathered from our camera study [33],
we re-designed and fabricated all parts of the second
prototype (Figure 8). Based on the clinician and user
feedback (Figure 7), we completely redesigned the
steering system to use a handlebar control. This
allows the SIMPL-EPW2.0 to be steered with two
hands (one pulling, one pushing) which helps the
user maintain trunk balance. The mechanism uses
two bicycle brake cables to transmit direction from
the user to the steered hub-motor. A fully retractable
steering arm and armrests allow for unencumbered
Figure 5. System design and free body diagram of SIMPL-EPW suspension system.
Figure 6. Photo of the SIMPL-EPW(1.0).
Low cost EPW for India 49
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

transferring into the device, and also provides the
user clear access in front of them when not driving
(Figure 8).
Based on the feedback from the camera study, we
narrowed the base of the WC and reoriented the seat
so that the larger wheels were in the front of the
Figure 7. Median clinician, user and manufacturer responses to final questionnaire during the first set of focus groups.
Figure 8. SIMPL-EPW(2.0) features.
50 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

device, allowing for better obstacle climbing ability.
Design specifications and performance values are
listed in Table III. A tilting seating system was also
incorporated into the device based on camera study
feedback (Figure 9).
Testing
The five subjects (2 male, 3 female) recruited for the
US focus groups in January 2007, had an average of
14.5 (+16.0) years of experience with wheeled
mobility products. Based on the open-ended feed-
back during each trial, design upgrades were
performed prior to the subsequent testing of the
device. Four primary design adjustments were made
based on subject feedback: the seat was moved
forward relative to the base to increase rearward
stability, the handlebars were extended to increase
the user’s leverage on the steering mechanism, an
optional twist-throttle was added, and a stop was
integrated into the steering arm to limit the travel
when it is flipped out of the way. Feedback on the
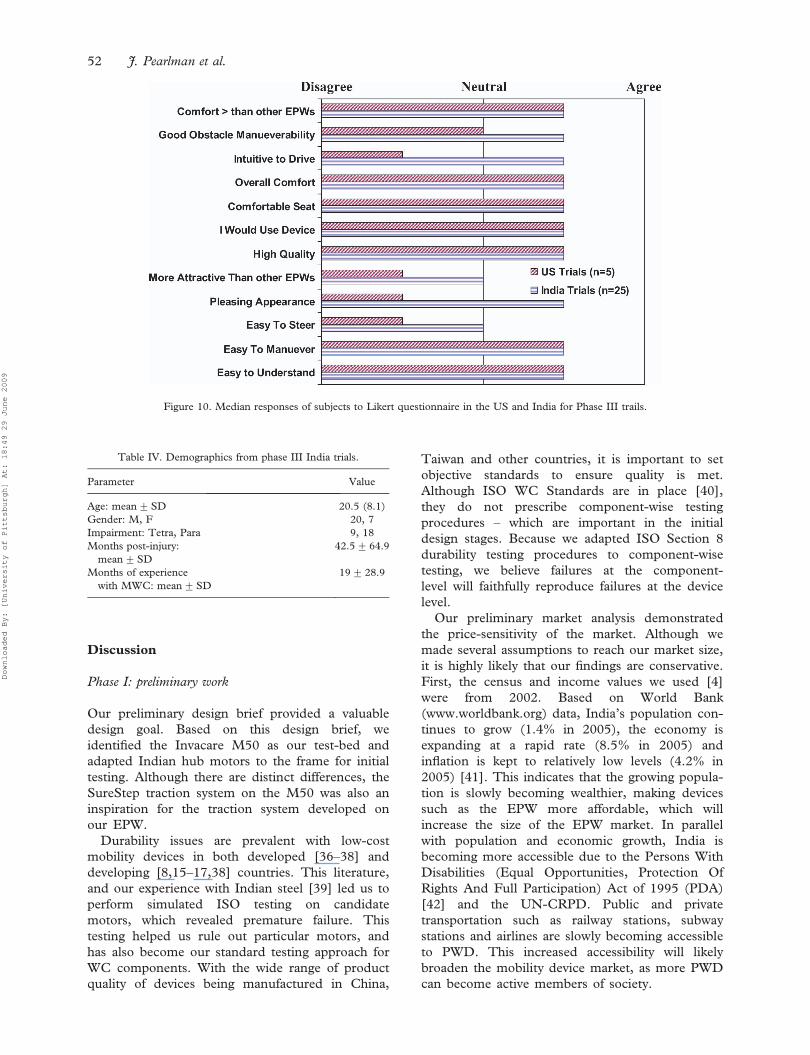
final questionnaire from the US subjects (Figure 10,
US Trials) was positive except related to the ease of
steering, the appearance and how intuitive it was to
drive.
Twenty-seven subjects were recruited to partici-
pate in the trials at the Indian Spinal Injuries Center
(ISIC) in New Delhi, India (Table IV).
A total of twenty five subjects completed the study;
after enrolling, two subjects found it difficult to take
time out of their work schedule to visit ISIC for 2
days.) Of the subjects, the majority were inpatients
(19) and the rest were split among outpatients,
employees and non-affiliated individuals. A sum-
mary of the statistical findings is below (Table V).
We found that subjects drove significantly further
when using the EPW for 3–4 h of their daily activities
compared with driving their MWC. We also found
that subjects with tetraplegia needed significantly less
assistance when using the EPW compared with their
MWC; this was not the case for subjects with
paraplegia.
When comparing trial times for the three
repeated trials (with a repeated measures ANO-
VA), and questionnaire responses between the first
and third trial (with a Wilcoxon rank-sum), we
found most variables significantly different regard-
less of the mobility device used (SIMPL-EPW2.0/
MWC) or impairment level (Tetra/Para), suggest-
ing a learning effect. Thus, we performed statistical
analysis only on the results from the third trial,
assuming that the data were approaching a steady
state. When testing the third trial, we found that
subjects with tetraplegia rated the entire obstacle
course as significantly easier with the SIMPL-
EPW2.0 compared with the MWC. Subjects with
paraplegia only found the outdoor portion of the
course significantly easier. Both of these results are
consistent with our hypotheses. We found that
subjects with paraplegia took significantly longer to
complete the obstacle course with the EPW
compared with their MWC.
Final questionnaire results from subjects in India
were in many cases consistent with US subjects
(Figure 10, Indian Trials), although responses from
Indian subject were generally more positive than
their US counterparts. Indian subjects notably rated
the device higher in ‘appearance’ and ‘intuitiveness’
to drive. The open-ended question at the end of the
questionnaire provided insightful design advice.
The most common suggestion was to shorten the
wheelbase to reduce the swinging arc of the rear
casters. Only three of the subjects noted the stiff
steering as an issue. The simple seating system was
well received – 15 of the 25 subjects had no
suggested changes, or praised how comfortable the
seat was. Several subjects suggested a more
supportive footrest. Subjects were generally pleased
with the appearance; 7 subjects suggested different
colours for the frame, and many subjects suggested
add-on features such as a cup holder, cane-holder
and shrouds over the wheels. One subject gener-
ically stated that the ‘style of the WC’ needed to be
improved, and another stated that the steering arm
was ‘ugly’.
Table III. Specifications of the SIMPL-EPW 2.0.
Spec Value Notes
Length, width,
height (cm)
130, 57, 89 Overall dimensions
Mass (kg) 77
Distance on full
charge (km)
43.1
Max speed (m/s) 1.65
Max obstacle climbing
ability (cm)
7.6, 2.5 Forward, rearward
Figure 9. Tilt feature on the SIMPL-EPW2.0.
Low cost EPW for India 51
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009
Discussion
Phase I: preliminary work
Our preliminary design brief provided a valuable
design goal. Based on this design brief, we
identified the Invacare M50 as our test-bed and
adapted Indian hub motors to the frame for initial
testing. Although there are distinct differences, the
SureStep traction system on the M50 was also an
inspiration for the traction system developed on
our EPW.
Durability issues are prevalent with low-cost
mobility devices in both developed [36–38] and
developing [8,15–17,38] countries. This literature,
and our experience with Indian steel [39] led us to
perform simulated ISO testing on candidate
motors, which revealed premature failure. This
testing helped us rule out particular motors, and
has also become our standard testing approach for
WC components. With the wide range of product
quality of devices being manufactured in China,
Taiwan and other countries, it is important to set
objective standards to ensure quality is met.
Although ISO WC Standards are in place [40],
they do not prescribe component-wise testing
procedures – which are important in the initial
design stages. Because we adapted ISO Section 8
durability testing procedures to component-wise
testing, we believe failures at the component-
level will faithfully reproduce failures at the device
level.
Our preliminary market analysis demonstrated
the price-sensitivity of the market. Although we
made several assumptions to reach our market size,
it is highly likely that our findings are conservative.
First, the census and income values we used [4]
were from 2002. Based on World Bank
(www.worldbank.org) data, India’s population con-
tinues to grow (1.4% in 2005), the economy is
expanding at a rapid rate (8.5% in 2005) and
inflation is kept to relatively low levels (4.2% in
2005) [41]. This indicates that the growing popula-
tion is slowly becoming wealthier, making devices
such as the EPW more affordable, which will
increase the size of the EPW market. In parallel
with population and economic growth, India is
becoming more accessible due to the Persons With
Disabilities (Equal Opportunities, Protection Of
Rights And Full Participation) Act of 1995 (PDA)
[42] and the UN-CRPD. Public and private
transportation such as railway stations, subway
stations and airlines are slowly becoming accessible
to PWD. This increased accessibility will likely
broaden the mobility device market, as more PWD
can become active members of society.
Figure 10. Median responses of subjects to Likert questionnaire in the US and India for Phase III trails.
Table IV. Demographics from phase III India trials.
Parameter Value
Age: mean+SD 20.5 (8.1)
Gender: M, F 20, 7
Impairment: Tetra, Para 9, 18
Months post-injury:
mean+SD
42.5+64.9
Months of experience
with MWC: mean+SD
19+ 28.9
52 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

Phase II: first-generation design and prototyping and
testing
We designed a unique, low-cost proof-of-concept
design during Phase II. Although costs were kept to a
minimum, there were several drawbacks to using
low-cost uni-strut and parts available EPWs to
develop the first prototype. First, use of uni-strut
required fasteners to secure parts of the frame
together. The fasteners added to the weight of the
device and made it less aesthetically appealing in
comparison to a fully customised welded frame and
seating system. Likewise, the frame and suspension
system were not as structurally stiff as they would
have been if welded, reducing overall performance
(manoeuvrability and obstacle climbing ability).
These effects bias the focus group feedback.
Subject responses to our focus groups in India
were important to evaluate the feasibility of the
device, and reveal important design changes. Most
importantly, we identified the steering system as a
critical design shortcoming. Our initial design was
focused on developing a non-invasive steering
system that could be easily flipped behind the user.
Our first design accomplished this, but also
required the user to steer by pushing (right turn)
or pulling (left turn) on the steering arm. For
individuals with spinal cord injury, depending on
the injury level, there are trunk stability deficits and
reduced function of the triceps muscles; this limits
the individuals ability to pull (due to trunk
instability) and push (due to reduced triceps
function), making it nearly impossible for many
individuals with higher level spinal cord injuries to
drive our first prototype. We rectified this problem
by using a balanced steering system in the second
phase, where users can push and pull simulta-
neously on the handlebar to turn in a single
direction.
We held focus groups with potential manufac-
turers to gauge the manufacturing feasibility.
Although other projects of this type have not
addressed manufacturability directly [26,27], we felt
feedback was necessary with a multi-component
device such as an SIMPL-EPW. The results were
mixed (Figure 7) – although manufacturers agreed
that they could fabricate and sell the EPW, they felt
the components were expensive and would need to
be imported, and that the overall device would not
be affordable. The focus group for manufacturers
was held at the Artificial Limbs Manufacturing
Corporation of India (ALIMCO), a large-scale
manufacturing facility in India, which specialises in
making low-cost AT for the poor in India. Although
the company had initially made overtures about
introducing an EPW in their product line, their focus
is on extremely low cost devices that are built at costs
below government subsidy levels (USD125) [30].
Thus, their response, especially related to afford-
ability, may reflect their company’s bias toward
selling inexpensive, low-tech AT. What was most
important and revealing was their confidence in
being able to fabricate the device using available
materials. Based on more recent information, we
know of several importers of the parts that are not
manufactured domestically (specifically the motor
and controller), which can be purchased, in bulk, for
low costs in India.
Table V. Summary of statistical findings from Phase III India trials.
Parameter MWC EPW Notes
Casual driving* 193.0+98.9 651.4+346.3 Mean+SD m/h
Assists
Tetra* 11 (2,14) 2 (2,4) Median (min, max) averaged values for trial 1& 3
Para 1.5 (0,5) 2.0 (0,3) Median (min, max) averaged values for trial 1& 3
Total course score
Tetra* 815 (69,1194) 206 (29,554) Median (min, max) mm for Trial 3
Para 237.5 (14,720) 200.5 (11,738) Median (min, max) mm for Trial 3
Indoor score
Tetra* 258 (20,495) 152 (16,341) Median (min, max) mm for Trial 3
Para 75.5 (5,371) 139.5 (9,450) Median (min, max) mm for Trial 3
Outdoor score
Tetra* 412 (49,814) 106 (13,213) Median (min, max) mm for Trial 3
Para* 189.5 (4,420) 41 (2,288) Median (min, max) mm for Trial 3
Course time
Tetra 317 (125) 227 (65) Mean+SD seconds for Trial 3
Para* 179 (75) 294 (97) Mean+SD seconds for Trial 3
A * denotes statistical differences between MWC and EPW values. Course scores were normalised from the full range from 0 to 2100 mm to
a scale of 0–100 for clarity. Indoor and outdoor scores do not necessarily add to total scores because medians are reported rather than
averages.
Low cost EPW for India 53
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

Phase III: second-generation design, prototyping and
testing
Phase II results and our camera study [33] informed
our design changes, guiding us to improve the
steering and seating and also the dimensions of the
device. Our second device was custom-fabricated,
reducing the number of fasteners and weight. Apart
from the re-designed steering and seating system, we
simplified the suspension system by using leaf
springs in place of the rigid suspension links and
captive spring system on the first prototype. This
design change increased rigidity of the suspension
system, significantly reduced the number of compo-
nents, and was simple and low-cost to fabricate. We
demonstrated the device to two local manufacturers
during focus group testing, and both suggested they
could build the device for approximately $450, and
make a profit if they sold it priced at $550, closely
achieving our goal of a $500 device. Several of the
specifications of the SIMPL-EPW were measured
based on ISO 7176 standards [40] and are shown in
Table III. Specifications of the SIMPL-EPW 2.0
Based on energy consumption tests (ISO 7176
Section 4 [40]), the SIMPL-EPW2.0 can travel a
total of 43.1 km on a single charge (Table III). This
value suggests the SIMPL-EPW can travel, on
average, 48% and 31% further than low-cost [38]
and higher-cost [43] EPWs, respectively. We did not
perform several pertinent tests, such as static stability
(ISO 7176 Section 1) or Static Strength, Impact and
Durability (ISO 7176 Section 8) although this is the
subject of future work.
We had a large subject population in comparison
to similar studies [27,44,45] (n¼ 8–15). Our
breakdown between men and women (Table IV)
(m¼ 74%, w¼ 26%) is similar to the breakdown in
the population of PWD in India (m¼ 62%,
w¼ 38%). A majority of our subjects were inpa-
tients at ISIC, and had recently been injured.
Although all were out of acute care, many had
little experience with MWCs and were propelled
by assistants (regardless of injury level). Although
this is atypical for users in the US and European
countries, data suggests the majority of individuals
do not self-propel their manual WCs [16,17]. This
is due to several reasons, inclusive of, but not
limited to, the poor quality MWCs in India, the
lack of user training, and the low-cost of a personal
assistant (*$2.50/day). We agree that with proper
training and improvements in WC quality (as
suggested by the WHO [3], Chapter 1), MWC
users could be more functionally independent, but
these improvements are likely far in the future.
Meanwhile, the market for WCs is dominated by
low-cost, low-quality hospital style WCs which
limit independent mobility.
The summary of our statistical findings (Table V)
demonstrate several relative improvements when
subjects used the SIMPL-EPW2.0 compared with
their MWC. First, subjects travelled significantly
further, per-hour, when they were driving the
SIMPL-EPW2.0, compared with their MWC. We
attribute a portion of the relative increase (*450 m/
h) on a ‘novelty’ effect of driving a new device.
Regardless, each subject had a daily schedule of tasks
to accomplish (whether it was physical therapy or job-
related tasks), and so drove the EPW more during
their free time. In many cases, the subject would roam
outside, up and down ramps and socialise in wards
that otherwise were difficult to access because they
were not independently mobile in their MWC. In
many cases, their assistant would accompany them
initially during their EPW driving walking behind the
EPW (it cannot be pushed), but in many cases, the
assistant would leave, allowing the subjects to move
unencumbered. Although the comparison between
the distance travelled in the EPW and MWC is
telling, even more telling were the qualitative
observations of the users in the EPW – they seemed
excited to roam outside and speak with others; they
generally seemed happy to be independently mobile,
made positive remarks about the device and com-
monly asked when it would be available for sale.
Comparison between the obstacle course assists,
difficulty ratings and course times were similarly
telling of the EPW performance (Table V). Indivi-
duals with tetraplegia required significantly less
assistance during completion of the obstacle course
and found the course significantly easier to accom-
plish when using the SIMPL-EPW2.0. There were no
significant differences between the course times with
the SIMPL-EPW2.0 and MWC for subject with
tetraplegia. Taken in the context of the significant
reduction in assistance for individuals with tetraplegia
in the SIMPL-EPW2.0 over their MWC, these results
suggest the SIMPL-EPW2.0 effectively replaces a paid
assistant, and makes tasks significantly easier.
We found that subjects with paraplegia felt the
outdoor portion of the obstacle course was signifi-
cantly easier to accomplish with the SIMPL-EPW2.0
compared with their MWC. Although this result may
be surprising, the poor quality of MWCs available in
India and the lack of WC skills training significantly
limit outdoor mobility. This is troubling, considering
nearly 75% of individuals with disabilities live in the
rural environments [4]. We also found that subject
with paraplegia took significantly longer to complete
the course in the SIMPL-EPW2.0 than in their
MWC. The reason for this is likely the indoor speed
at which individuals with paraplegia can complete
the obstacle course in their MWC. The course was
setup in the physiotherapy lab, which is ideally
accessible (except for the bathroom doors, which
54 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

have spring-closing systems). Most subjects were
very familiar with approaching the desk, sink and
table; and entering the bathroom in their MWC, so
the individual tasks themselves were not demanding.
When using the EPW, the front-wheel drive man-
oeuvrability of the device slowed many subjects
indoors.
Subject feedback on the Likert portion of the final
questionnaire was revealing especially when com-
pared with feedback by the US subjects (Figure 10).
In general, Indian subjects rated the EPW higher
than their US counterparts. All responses from
Indian subjects were positive except for the question
related to ease of steering and attractiveness, which
were rated as ‘neutral’ (neither agree nor disagree).
Despite the issues Indian subjects conveyed with
steering the device (discussed more below), they
found the EPW substantially more intuitive to drive
than the US subjects. The steering system on the
EPW mimics a motorcycle, with a twist throttle and
handlebars. Although motorcycle use is relatively
uncommon in the US, motorcycles and mopeds are
ubiquitous in India. Similarly, low-cost taxis (‘auto-
rickshaws’) are driven with an identical steering and
throttle control system. This is an example of how
the societal differences have a significant effect in the
response to product design [46].
During the Phase II focus groups, the small casters
were located in front of the device. Based on trials
with the seat reversed, we found obstacle-climbing
ability to be much improved when the seat was
reversed, and so the Phase III prototype was
fabricated with the large diameter wheels at the front
of the device. The consequence of this design change
is reflected in the open-ended comments from
subjects on the final questionnaire. By switching
the orientation of the seat, the device manoeuvres
like a front wheel drive EPW, where the device
rotates about a point approximately between the
user’s knees. This gives the sense that the EPW is
very long, since the rear portion of the device swings
in a wide arc during a turn. Given that few of the
subjects had driven an EPW before, especially a
front-wheel drive design, they were more comforta-
ble with how an automobile steers (which is similar
to how a rear wheel drive EPW steers). Thus, the
feedback that the wheelbase should be shortened
from many of the subjects (which was not given when
the seat was reversed), indicates that possibly the seat
should be oriented in its original position. This
original orientation (Figure) also allows for the users’
feet to be placed between the suspension links,
effectively shortening the overall length of the device.
The SIMPL-EPW was designed for an adult
population although there is a tremendous need for
pediatric mobility devices world-wide. Bias towards
the adult population stems the fact that a parallel
design effort is being made to develop a low-cost
pediatric WC for Indian users. Since the SIMPL-
EPW is a ‘power-base’ EPW [47,48] the design does
not prohibit placing a seating system appropriate for
pediatric clients. Adapting the product for pediatric
clients is the subject of future work.
Conclusions
PWD deserve high quality mobility devices so they
can be more independent and participate more fully
in society. Already implemented [42] and upcoming
[7] policies in developing countries will help in this
vein, but there are still substantial technological
challenges to overcome that will ensure devices meet
the social, economic and technical constraints in
developing countries. To leverage the skills of
rehabilitation specialist and engineers world-wide,
along with the growing interest among students to
participate in international development projects, it
is important to build a wider body of published
experience-based knowledge of the research and
design approaches that are successful and unsuccess-
ful in these countries; this will help avoid situations
like the repeated failures of MWCs technology
transfer to meet the needs in developing countries
[1,8,38].
The project described here has been successful in
developing a low-cost appropriate EPW for indivi-
duals in India. The device will likely be appropriate
in many developing countries, with slight design
changes to accommodate the parts and materials,
which are locally available. Despite the strong
performance of our design, a more comprehensive
engineering analysis could have been performed to
optimise the steering and obstacle climbing ability of
the device prior to user trials. We plan to perform
this analysis for the next prototype.
To complete the project, we plan to perform in-
home trials of the SIMPL-EPW2.0 after design
modifications have been integrated based on our
Phase III results. We may perform these trials
independently, although we feel that it is best to
collaborate with a manufacturer to fabricate the
prototype device so that user-feedback can be
integrated directly into the product design cycle.
Acknowledgements
This work was supported by the grants from the
National Science Foundation (EEC 0552351 and
DGE0333420). We gratefully acknowledge the
clinical staff (Annmarie Kelleher, Emily Teodorski,
Rosemarie Cooper), technical staff (Jeremy Puhl-
man, Mark McCartney) past students (Neil Stegall,
Low cost EPW for India 55
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

Mary Wu, Amy McNeal and Jaideep Karnawat)
and our India-based support (Nekram Upadhyay
and Jyoti Vidhani) who helped make this project
successful.
References
1. Hotchkiss R, Knezevich J. Third World Wheelchair Manu-
facture: Will It Ever Meet The Need? In: RESNA 13th Anual
Conference. 1990. Washington, D.C.: RESNA.
2. WCF. Wheelchair Foundation Website. 2003 [cited 2003;
Available from: http://www.wheelchairfoundation.org/.
3. ISPO, Recommendations and Conclusions in Consensus
Conference on Wheelchair Technology and Provision in
Developing Countries. 2006, International Society of Pros-
thetics and Orthotics: Bangalore, India.
4. India, G.O., Disabled People in India: National Sample
Survey (NSS) 58th Round, 2002, Government of India: New
Delhi. p. 593.
5. Harriss-White B. Onto a Loser: Disabilty in India, in Illfare in
India. Essays on India’s Social Sector in Honor of S. Guhan,
B.a.S. Harriss-White, S, Editor. 1999, Sage: New Delhi. pp.
135–158.
6. Pearlman JL, Cooper RA, Krizack M, Lindsley A, Wu Y,
Reisinger K, Armstrong W, Casanova H, Chhabra HS, Noon
J. Lower-limb prosthetics and wheelchairs in low income
countries. IEEE-EMBS Magazine 2008;27(2):11.
7. UN. Convention on the Rights of People With Disabilities.
2006 [cited; Available from: http://www.un.org/disabilities/
convention/.
8. Kim J, Mulholland SJ. Seating/wheelchair technology. In the
developing world: need for a closer look. Technol Disabil
1999;11:21–27.
9. Hotchkiss R, Pfaelzer P. Measuring success in Third World
wheelchair building. In: Rehabilitation Engineering and
Assistive Technology Society of North America Annual
Conference, 1992. Toronto.
10. Hotchkiss R. Ground swell on wheels: appropriate technology
could bring cheap, sturdy wheelchairs to twenty million
disabled people. The Sciences 1993;33(4):14–18.
11. Hotchkiss R. Putting the Tools in the Hands That Can Use
Them: Wheelchairs in the Third World. In: RESNA 10th
Annual Conference, 1987. San Jose, CA.
12. Hof H, Hotchkiss R, Pfaelzer P. Building wheelchairs,
creating opportunities: collaborating to build wheelchairs in
developing countries. Technol Disabil 1993;2(2):1–14.
13. Werner D, Thuman C, Maxwell J. Nothing About Us
Without Us. Palo Alto: HeathWrights; 1998, p. 350.
14. Werner D. Disabled Village Children: A Guide for Health
Workers, Rehabilitation Workers, and Families. Hesparian
Foundation; 1987. Berkeley, CA.
15. Boonzaier DA. Ten Years of Rehabilitation Technology in a
Developing Country: A Review 1980–1990. In: RESNA 13th
Annual Conference, 1990. Washington, D.C.
16. Saha R, Dey AK, Hatoj M, Poddar S. Study of wheelchair
operations in rural areas covered under the district rehabilita-
tion centre (DRC) scheme. Indian J Disabil Rehab 1990:74–
87.
17. Mukherjee G, Samanta A. Wheelchair charity: a useless
benevolence in community-based rehabilitation. Disabil
Rehabil 2005;27:591–596.
18. Armstrong W, Reisinger KD, Smith WK. Evaluation of CIR-
whirlwind wheelchair and service provision in Afghanistan.
Disabil Rehabil 2007;29:935–948.
19. Ulrich KT, Eppinger SD. Product Design and Development.
New York: McGraw-Hill; 1995.
20. Hotchkiss R. Independence Through Mobility. Assistive
Technology International; 1984. Chicago, IL.
21. Pearlman JL, Cooper RA, Zipfel E, Cooper R, Mccartney M.
Towards the development of an effective technology transfer
model of wheelchairs to developing countries. Disabil Rehab:
Assist Technol 2005;1:103–110.
22. Huckstep RL. Poliomyelitis – A Guide for Developing
Countries. Churchill Livingstone; 1975. New York, NY.
23. Zipfel E, Cooper RA, Pearlman J, Cooper R, McCartney M.
New design and development of a manual wheelchair for
India. Disabil Rehabil 2007;29:949–962.
24. Authier EL, Pearlman J, Allegretti AL, Rice I, Cooper RA. A
sports wheelchair for low-income countries. Disabil Rehabil
2007;29:963–967.
25. Mulholland SJ, Packer TL, Laschinger SJ, Olney SJ, Panchal V.
The mobility needs of women with physical disabilities in India:
a functional perspective. Disabil Rehabil 1998;20:168–178.
26. Lysack JT, Wyss UP, Packer TL, Mulholland SJ, Panchal V.
Designing appropriate rehabilitation technology: a mobility
device for women with ambulatory disabilities in India. Int J
Rehabil Res 1999;22:1–9.
27. Mulholland SJ, Packer TL, Laschinger SJ, Lysack JT, Wyss
UP, Balaram S. Evaluating a new mobility device: feedback
from women with disabilities in India. Disabil Rehabil
2000;22:111–122.
28. ISO, ISO 7176-19. Wheeled mobility devices for use in motor
vehicles, ISO, Editor; 2004. p. 31.
29. LaPlante MP. Demographics of Wheeled Mobility Device
Users. In: Conference on Space Requirements for Wheeled
Mobility. Buffalo, New York, 2003.
30. India, G.O., Scheme of Assistance to Disabled Persons for
Purchasing/Fitting of Aids/Appliances (ADIP Scheme), Min-
istry of Social Justice and Empowerment: New Delhi.
31. Donaldson K. Recommendations for improved development
by design. In: Development by design (dyd02). 2002.
Bangalore, India.
32. Pearlman JL, Cooper RA, Karnawat J, Cooper R,
Boninger ML. Evaluation of the safety and durability of low-
cost nonprogrammable electric powered wheelchairs. Arch
Phys Med Rehabil 2005;86(12):2361–2370.
33. Pearlman J, Jefferds A, Cooper RA, Nagai I, Chhabra HS.
Designing assistive technology for less-resourced environ-
ments: an online method to gauge accessibility barriers and
collect design advice. Int J Rehabil Res, In Review.
34. Tolerico M. Investigation of the Mobility Characteristics and
Activity Levels of Manual Wheelchair Users in Two Real
World Environments, in Rehabilitation Science and Technol-
ogy. University of Pittsburgh: Pittsburgh; 2006.
35. Portney LG, Watkins MP. Foundations of clinical research:
applications to practice. 2nd ed. 2000: Prentice Hall Upper
Saddle River, NJ, p. 768.
36. Cooper RA, Robertson RN, Lawrence B, Heil T, Albright SJ,
VanSickle DP, Gonzalez J. Life-cycle analysis of depot versus
rehabilitation manual wheelchairs. J Rehabil Res Dev 1996;
33:45.
37. Fitzgerald SG, Cooper RA, Boninger ML, Rentschler AJ.
Comparison of fatigue life for 3 types of manual wheelchairs.
Arch Phys Med Rehabil 2002;82:1484.
38. Pearlman JL, Cooper RA, Karnawat J, Cooper R, Boninger
ML. Evaluation of the safety and durability of low-cost
nonprogrammable electric powered wheelchairs. Arch Phys
Med Rehabil 2005;86:2361–2370.
39. McNeal A, Cooper R, Pearlman J. Critical Factors For
Wheelchair Technology Transfers To Developing Countries –
Materials and Design Constraints. In: 28th Annual RESNA
Conference. Atlanta, GA, 2005.
40. ISO, I.S.O., Wheelchair Standards (7176:1-24). 1985–2004,
International Standards Organization.
56 J. Pearlman et al.
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009

41. WorldBank. India Data Profile. 2007 [cited 2007 April 21];
World Bank Statistics on India. Available from: http://
devdata.worldbank.org/external/CPProfile.asp?PTYPE¼CP&
CCODE¼IND.
42. People with Disabilities Act (Equal oppurtunities, protection
of rights and full participation). In: Ministry of social justice
and empowerment. 1995: India.
43. Rentschler AJ, Cooper RA, Fitzgerald SG, Boninger ML,
Song-Feng G, Ammer W, Vitek M, Algood D. Evaluation of
selected electric-powered wheelchairs using the ANSI/RE-
SNA standards. Arch Phys Med Rehabil 2004;85:611–619.
44. Algood D. The Impact of a Pushrim Activated Power Assist
Wheelchair Among Individuals with Tetraplegia, In Rehabi-
litation Science and Technology. University of Pittsburgh:
Pittsburgh; 2003. p. 66.
45. Algood SD, Cooper RA, Fitzgerald SG, Cooper R,
Boninger ML. Effect of a pushrim-activated power-
assist wheelchair on the functional capabilities of persons
with tetraplegia. Arch Phys Med Rehabil 2005;86:380–
386.
46. Cagan J, Vogel C. Creating Breakthrough Products: Innova-
tion from Product Planning to Program Approval. Prentice
Hall PTR: Upper Saddle River; 2002, p. 302.
47. Cooper R. Rehabilitation Engineering Applied to Mobility
and Manipulation. 1 ed. Medical Science Series, ed. I.o.P.
Publishing. Vol. 1. Bristol and Philadelphia: Institute of
Physics Publishing; 1995, p. 516.
48. Cooper R. Wheelchair Selection and Configuration. 1 ed.
Vol. 1. New York: Demos Medical Publishing; 1998.
p. 410.
Low cost EPW for India 57
Downloaded By: [University of Pittsburgh] At: 18:49 29 June 2009
Related Documents