On the Road to Ghana with Dr. Mammino see page 18 Exploring Monterey Midyear Meeting - March 12-15 see page 14 DermLine Marketing Your Practice on the World Wide Web see pages 10-11 Tanning Beds Under Scrutiny see page 15 S P R I N G 2 0 0 8 Newsletter of the American Osteopathic College of Dermatology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
On the Road to Ghanawith Dr. Mammino see page 18
Exploring Monterey Midyear Meeting - March 12-15see page 14
DermLine
Marketing Your Practiceon the World Wide Websee pages 10-11
Tanning BedsUnder Scrutinysee page 15
SPRING
2008
Newsletter of the American Osteopathic College of Dermatology
CORPORATE SPONSORS
AOCD MIDYEAR MEETINGMarch 12-15, 2008Monterey, CA
AOCD ANNUAL MEETINGOctober 26-30, 2008Las Vegas, NV
AOCD MIDYEAR MEETING 2009January 20-25, 2009Steamboat Springs, CO
Upcoming Events
DI A M O N D SP O N S O R S
Biopelle Inc.Dermpath DiagnosticsGlobal PathologyMedicis - The Dermatology CompanyNeutrogenaOrtho-NeutrogenaPharmadermRanbaxy PharmaceuticalsStiefel Laboratories
PL AT I N U M SP O N S O R S
Graceway Pharmaceuticals
GO L D SP O N S O R S
CollaGenex Pharmaceuticals
SI LV E R SP O N S O R S
Coria LabsDermik Labs/Sanofi-AventisGalderma
BR O N Z E SP O N S O R S
AllerganAmgenDermatopathology Lab. of Central StatesIntendisPierre Fabre Dermo Cosmétique USA
American OsteopathicCollege of DermatologyP.O. Box 75251501 E. IllinoisKirksville, MO 63501Office: (660) 665-2184
(800) 449-2623Fax: (660) 627-2623Site: www.aocd.org
PRESIDENTJay S. Gottlieb, D.O., FAOCD
PRESIDENT-ELECTDonald K. Tillman, D.O., FAOCD
FIRST VICE PRESIDENTMarc I. Epstein, D.O., FAOCD
SECOND VICE PRESIDENTLeslie Kramer, D.O., FAOCD
THIRD VICE PRESIDENTBradley P. Glick, D.O., FAOCD
SECRETARY-TREASURERJere J. Mammino, D.O., FAOCD
IMMEDIATE PAST-PRESIDENTBill V. Way, D.O., FAOCD
TRUSTEESDavid L. Grice, D.O. Karen E. Neubauer, D.O.Mark A. Kuriata, D.O. James B. Towry, D.O.
EXECUTIVE DIRECTORRebecca Mansfield, MA
UPDATE CONTACT INFORMATION
Is your contact information current? If not,you may be missing need-to-know newsfrom the AOCD.Visit www.aocd.org/members. Click on thered box on the right side of the screen toupdate your info. Should you have trouble accessing yourprofile, you can fax the new information tothe AOCD at 660-627-2623. Send the faxto the attention of Marsha Wise, ResidentCoordinator.
CONTRIBUTE TO DERMLINE
If you have a topic you would like to readabout or an article you would like to writefor the next issue of DermLine, contact RuthCarol, the editor, by phone at 847-251-5620, fax at 847-251-5625 or e-mail [email protected].

CORPORATE SPONSORS
Page 3
The holidays are now behind us andthe New Year is in full swing. In thefirst three months, acting in thecapacity as your AOCD president, Ihave been busy working with Drs.Lloyd Cleaver, Jim Towry, and JohnHibler, as well as the residencyprogram directors to ensure that theresident in-training examination goessmoothly this year and in the years tocome. Dr. Cleaver developed andimplemented an on-line website wherethe program directors can easily submittheir questions each month. Dr. Hiblercreated a simple matrix for the programdirectors to utilize to ensure that thequestions submitted cover all of thetopics needed to be addressed in theexamination. We will create a ‘bank’ ofquestions that can simply be updatedand then used for future in-trainingexaminations.
Dr. Leslie Kramer has been working onputting together a very exciting andinformational Midyear Meeting inMonterey, Calif. Monterey is a vibrantand exciting venue for our MidyearMeeting. I hope to see each and everymember and resident member inMonterey. It is going to be great.
Maintaining and growing corporatesponsorship for the AOCD seems to bemore of a challenge each year. Federalrequirements and restrictions makeobtaining funding and grant moniesmore and more time consuming. Iencourage every member to assist ourDirector of Corporate Development bygiving her leads that she can thendevelop.
Becky, Rick, and Marsha continue torun our College’s office in Kirksville.More and more requirements areplaced upon them as our Collegecontinues to grow. They also havemore paperwork each year to completeas regulations and requirements mount.The logistics of keeping the residencyprograms on track is a daunting task. Iencourage the membership to give meboth positive and negative feedback onyour experiences with the AOCDoffice. Each comment is confidentialand considered important by yourBoard of Trustees.
Being the editor of the JAOCD is alsovery exciting. The manuscripts continueto improve in quality and quantity. Oursponsors continue to keep the JAOCD a
Message From The President
reality. Global Pathology Laboratory,Stiefel Laboratories, Medicis, and Colla-Genex have been providing thesupport that we need to keep a qualityproduct in the pipeline.
I am enjoying my year as president ofthe AOCD. It is a learning experienceand quite exciting. I wish you all agreat year and I will see you inMonterey!
Fraternally Yours,Jay Gottlieb, D.O., FAOCD, FOCOO
AOCD President Jay Gottlieb, D.O.,FAOCD, was quoted in a DermatologyTimes article discussing the College’splans to petition the AmericanAcademy of Dermatology (AAD) togrant AOCD fellows full AAD member-ship. In 2004, the AOCD petitioned theAAD to recognize American Osteo-pathic Board of Dermatologycertification. However, the petitionreceived 59 percent of AAD membervotes, short of the required two-thirds.“All the D.O.s have been asking is thatAAD recognize our board training asthey do the Royal College of Physiciansand Surgeons of Canada,” Dr. Gottliebis quoted as saying. This most recentround of proposed bylaws change isexpected to occur within the next 24months, he said. The article appearedDec. 1, 2007.
Mark Kuriata, D.O., was interviewedfor an article in the July 2007 issue ofDermatology Times. The “On Call”column talked to dermatologists acrossthe country to see if primary carephysicians continue to treat patientswith skin problems longer than theyshould. Dermatologists were askedhow they handle such situations andhow it affects their patients’ care. Thedermatologists said that general practi-tioners are much less likely now thanin the past to keep patients beyondtheir ability to treat them. Still, whengeneral practitioners don’t make timelyreferrals, it can be problematic. Similarto other dermatologists’ experiences,Dr. Kuriata said that he witnessed prob-lems when general practitioners handleprocedures that they shouldn’t. He isquoted as saying, “My biggest concernis seeing biopsies done that are just not
appropriate or properly done—forexample, performing shave biopsies onpigmented lesions—because then wearen’t able to determine the Breslow,Clark level. Although procedures aresometimes reimbursed at a higher level,I hope the primary care doctors aren’tdoing it for the money. The problem is,they feel they need to be able to doeverything for a patient. Then, whenthe biopsy comes back showing some-thing like a melanoma, they realizedthat they’ve stepped out of theircomfort zone and now need to referthe patients, when they really shouldhave referred one step before.”
Were you quoted in a recent article? Letus know so we can let your peers know.Contact DermLine’s editor, Ruth Carol, at847-251-5620, fax at 847-251-5625, oremail at [email protected].
Honorable Mention

Page 4
AOA President Peter Ajluni, D.O., andAOA Executive Director John Crosby,J.D., summarized the purpose andgoals of this conference in their closingremarks. They also encouraged atten-dees to share the ideas generated in theconference with their organizations’officers and general membership.
The AOA will convene this SpecialtySummit periodically to develop andimprove upon the key componentsoutlined at the meeting.
This was an informative conferencethat should challenge all specialtycolleges, osteopathic institutions, andthe AOA to continue the growth of thisorganization. The AOCD ExecutiveCommittee is expected to discuss thesetopics during the Midyear Meeting inMonterey, Calif.
AOA 2007 Specialty Summit
AOA 2007 Specialty Summit wasconvened in December in Las Vegas.Meeting attendees included the AOAstaff, specialty college executive direc-tors and presidents, deans andpresidents from the osteopathicschools, members of the AOA Board ofTrustees, and other invited guests. Thepurpose of the summit was to addressissues that are key to the continuedgrowth of the AOA and its affiliateorganizations (eg, the AOCD). These
issues were identified through amarketing survey conducted by theAOA last summer.
Participants further defined the topicsas follows:
• Collaborative Vision: What does an‘AOA/Specialty Affiliate Partner-ship’ look like?
• Membership: How should the AOAsupport lifelong membership?
• Convention: How can the AOAimprove convention participationfor specialty affiliates and atten-dees?
• Education: How does the AOAsupport lifelong osteopathiclearning?
• Revenue-Sharing: How should theAOA share its financial successwith the specialty affiliates in orderto strengthen the osteopathicfamily?
• Affiliate Benefits & Services: Whatdo specialty affiliates need from theAOA?
Executive Director’s Reportby Becky Mansfield, Executive Director
is aproud supporter
of the
Page 5
Melanoma Monday kicks offMelanoma/Skin Cancer Detection andPrevention Month in May. Dermatolo-gists across the country participate inactivities that remind the public how toprotect oneself from the sun’sdamaging rays and provide instructionon how to spot the warning signs ofskin cancer.
If you are planning to participate inactivities such as free screenings orlectures designed to promote skincancer detection and prevention, wewould like to hear from you aboutthose activities to be featured in anarticle in an upcoming issue ofDermLine. Contact the editor, RuthCarol, at 847-251-5620, fax at 847-251-5625, or email at [email protected].
Where Will You BeOn MelanomaMonday?
Erik Austin, D.O., M.P.H., co-authored abook chapter in the Seventh Edition ofMarzulli and Maibach's Dermatotoxi-cology published this past January.
He co-wrote chapter 55 entitled“Allergic Contact Dermatitis to TopicalAnesthetics” with Howard Maibach,M.D., FAAD, and ChristopherDannaker, D.O., FAAD, both of theUniversity of California at San FranciscoSchool of Medicine.
Since the development of topical anes-thetics in the latter half of the 19th
century, they have been found to becommon producers of allergic contactdermatitis (ACD), the chapter explains.“Sensitization to topical anesthetics mayinduce a contact dermatitis, as well ascross-reactions to related medications,”says Dr. Austin. “Moreover, exposure totopical anesthetics presents an occupa-tional hazard for certain workers. Thisphenomenon is an under-recognizedproblem for physicians, related health-care personnel, and patients who may
be repeatedly exposed to topical anes-thetics, or other such medicaments.”
Dr. Austin has been involved inresearch in ACD with Drs. Maibach andDannaker since 2000. Their initial workfirst appeared in the American Journalof Contact Dermatitis in 2001. Dr.Austin’s research work in ACDcontinued while he was a resident inthe dermatology program at NortheastRegional Medical Center.
“This edition of the Dermatotoxicologytext is far-reaching and would appealto all those who have an interest in theinteraction between the environmentand the skin,” he says.
The Seventh Edition of Marzulli andMaibach's Dermatotoxicology, the majortextbook in this field, was edited by H.Zhai, Ph.D., H. Maibach, M.D., and K.P.Wilhelm, M.D. The publisher is CRCPress.
Dr. Austin is the medical director ofAustin Dermatology Center in SanDiego. In addition, he recently receivedhospital privileges at Scripps MemorialHospital, an affiliate of the University ofCalifornia at San Diego School of Medi-cine, and was recently appointed to thefaculty at Western University of HealthSciences as a clinical assistant professorof dermatology.
Dr. Austin Contributes Chapter to Major Textbook
DERMATOLOGY OPPORTUNITY
AN ESTABLISHED DERMATOLOGY
OFFICE IS SEEKING A BC/BEGENERAL DERMATOLOGIST TO JOIN A
BUSY PRACTICE IN TULSA, OKLA-HOMA. INTERESTED PARTIES SHOULD
CONTACT EDWARD H. YOB, D.O.,DERMATOLOGY ASSOCIATES OF
TULSA, FOR FURTHER INFORMATION
AT 918-307-0215.

Page 6
We are dedicated to helping patients
attain a healthy and youthful appearance
and self-image.
© 2007 Medicis Pharmaceutical Corporation MED 07-003 01/30/08
With Melanoma Monday coming inMay, why not raise public awarenessby contributing to the Foundation forOsteopathic Dermatology (FOD)?
Like the Dermatology Foundation ofthe American Academy of Derma-tology, part of the FOD’s mission is toraise public and private awareness.This is accomplished by providingpublic health information, largely withregard to skin disease, as well asconducting charitable events. Foundedin 2002, the Foundation’s other goal isto improve the standards of practicewithin the osteopathic dermatologycommunity. To that end, the FODsupports research through grants andawards given to applicants under thejurisdiction of osteopathic dermatolo-gists and the AOCD.
Examples of research awards providedby the FOD include the following:
• The Resident Research Award isgranted to three residents or recentosteopathic residency programgraduates for research performedduring their residency. The firstplace winner is awarded $500, thesecond place winner receives $300,and the third place winner isgranted $100.
• The Attending Physician Award isgiven to a board-certified osteo-pathic dermatologist who submitsthe best research project as judgedby the Research Grant Committee.The winner is awarded $500.
These are just two examples of theavailable grants and awards providedby the FOD, which is supported solelythrough voluntary contributions such asthose provided by members and bene-factors, as well as the generous supportof corporate donors.
This spring, consider giving generouslyto build our Foundation to a level thatprovides much to both the osteopathicdermatology community and the publicat large.
For further information, please visit themembership area of the AOCD website(www.aocd.org/members) and click the“Fellows of Distinction” link on the left,or contact me directly at 954-242-1632.
Supporting the FODby Brad P. Glick, D.O., MPH, FAOCD
Page 7
Hi everyone,
The holidays are behind us and theNew Year is off and running. My newyear began with the arrival of my firstgrandchild—Lily was born January 5,one month early at 5 lbs., 1 ounce and18 inches long. Lily and her mommaare doing great. Naturally I have plansto spoil her rotten!
Our list of new residents for 2008-2011continues to grow. As of February 1,we have 14 new residents. In the nextissue of DermLine, I hope to list all ofthem along with the programs they willbe joining.
All residents are asked to provide thefollowing documents:
• A copy of your medical schooldiploma (and exact date of gradua-tion)
• A copy of your internship diploma(exact dates of attendance andname and address of school)
• A copy of your state license• 2 passport size photos• A current CV
2008 AOCD membership dues are nowdue. You must be current on dues inorder for your training year to beapproved. Please remember to keepyour address and email address current,as well. If you experience problemslogging in using the link at atwww.aocd.org/members, please let meknow.
It will soon be time for annual reportsto be turned in! All forms can be down-loaded from our website. FacultyDisclosure statements and Intent-to-Lecture forms can also be downloadedfrom this same page (www.aocd.org/qualify/annual_reports.html).
Be sure to check out the DermatologyGrand Rounds on our website(www.aocd-grandrounds.org). Eachresidency program has been asked tosubmit a case. January’s case was fromDr. Layne Nisenbaum’s program atColumbia Hospital. February’s caseswere submitted by Dr. Tanya
Ermolovich’s program at FrankfordHospital, and Dr. Kimball Silverton’sprogram at Genesys Regional MedicalCenter. In March, Dr. Don Anderson’sprogram at MWU/Arizona College ofOsteopathic Medicine was expected tosubmit a case.
The schedule for the rest of the year isas follows: Dr. Lloyd Cleaver’s programat Northeast Regional Medical Centerand Dr. Bill Way’s program at NortheastRegional Medical Center are expectedto submit cases in April. Dr. JohnHibler’s program at O'Bleness MemorialHospital is scheduled to submit a casein May. Dr. Steven Grekin’s program atOakwood Southshore Medical Centerand Dr. Michael Mahon’s program atPontiac/Botsford Osteopathic Hospitalare slated to submit cases in June. Dr.Daniel Stewart’s program at SaintJoseph Mercy Health System and Dr.Cindy Hoffman’s program at St. Barn-abas Hospital are expected to submitcases in July. Dr. Marvin Watsky’sprogram at St. John's EpiscopalHospital, South Shore and Dr. RichardMiller’s program at Sun Coast Hospitalare slated to submit cases in August.Dr. James Del Rosso’sprogram atTUCOM/Valley HospitalMedical Center and Dr.Joan Tamburro’sprogram at UHHS CaseWestern University,Richmond HeightsHospital are scheduledto submit cases inSeptember. Dr. Bradley’sGlick’s program atWellington RegionalMedical Center and Dr.Stephen Kessler’sprogram at WesternU/COMP/Phoenix AreaDermatology areexpected to submitcases in October. Dr.David Horowitz’sprogram at WesternUniversity/PacificHospital and Dr. StanleySkopit’s program at
NSU-COM/BGMC are slated to submitcases in November.
Residents who celebrated January birth-days are: Drs. Julie Malchiodi, ElliottLove, Heather Higgins, Nicole Bright,Elaine Miller, Joe Machuzak, ToddKreitzer, Angela Combs, Mollie Jan,John Coppola, Allison Schwedelson,and Kristen Aloupis.
Those who celebrated February birth-days are Drs. Brooke Sliger, JohnPerroto, and David Bonney.
Residents celebrating March birthdaysare Drs. Daniel Hansen, BradleyNeuenschwander, David Cleaver, andJami Reaves.
Residents Updateby Marsha Wise, Resident Coordinator

Page 8
RESI
DEN
TSSPOTLIGHT
Like many osteopathic residentslooking to enter the field of derma-tology, those applying to the programat St. John’s Episcopal Hospital must bepassionate about the specialty. Butunlike other residents being acceptedinto dermatology programs across thecountry, those being accepted at St.John’s must have a family practicebackground.
A Family Affair“Our program is definitely unique inthat all of our residents do either familypractice or internal medicine first,” saysSuzanne Sirota Rozenberg, the assistantprogram director under ProgramDirector Marvin Watsky, D.O., FAOCD.
“We want our residents to have a verystrong background in medicine becausethis is what we feel makes them suchwell-rounded dermatologists. Itenhances their ability to treat the wholeperson, which is integral to the osteo-pathic tradition.”
Residents are required to have aninternship and then two years of familypractice under their belt before they gointo dermatology. All tolled, four resi-dents are currently in the FarRockaway, New York-based program,five have graduated from it, and twoare expected to graduate this year.
Hands-On ApproachThe program established in 2001 pridesitself on its hands-on approach. “Ourresidents get a lot of one-on-one time
with the attending physicians,” says Dr.Sirota Rozenberg. One reason for thatis residents split their time betweenrotating through hospital clinics andprivate offices of the attendings, eightin all. The settings span Nassau, SuffolkCounty, Westchester, Manhattan,Brooklyn, Queens, and the Five Towns.The different settings scattered acrossNew York expose the residents to adiverse range of patients from those onthe lowest socioeconomic end of thescale to those on the very high end. Inaddition, the residents get a uniqueopportunity to treat patients of alldifferent ethnicities and backgrounds.
Rotations fill up the bulk of the resi-dents’ day onMondays,Tuesdays,Thursdays,and Fridays.Additionallyon Fridays,residents havebook andboard reviews,as well as anafternoon oflearning aboutpediatricdermatologyand dermato-pathology, thelatter of which
occurs at the offices of Dermpath Asso-ciates. “Wednesdays are our academicday, which consist of grand rounds anda journal club meeting held at theSUNY Downstate Medical Center,” shesays. “Our residents get it all, frommedical dermatology to Mohs andsurgery, to lasers and cosmetics,” addsSirota Rozenberg, who should know asshe graduated from the program in2005.
AccomplishmentsMany residents have accomplishedoutstanding achievements.
They have won awards, including threeKoprince Awards (Drs. DarronDiGiulio, Adriana Ros, and James BrileyJr.), an Allergan Research Paper Award(Drs. DiGiulio and Briley), and a New
York State Osteopathic Medical Society(NYSOMS) Intern/Resident ScientificResearch Poster Competition (Drs.Briley, Norma Montel, and LawrenceSchiffman).
Many have published papers in medicaljournals, including the JAOCD, Cutis,the Journal of Drugs in Dermatology,and Emergency Medicine.
They have presented posters atNYSOMS, the AOCD annual meeting,and most recently at the Gross andMicroscopic Conference held at theFebruary 2008 American Academy ofDermatology annual meeting held inSan Antonio (Dr. Schiffman). Residentshave also presented grand roundspresentations at various AOCD annualmeetings.
“We hope to continue exposing ourresidents to as much dermatology aspossible to keep them in the forefrontof the field and increase our contribu-tion to the specialty,” concludes Dr.Sirota Rozenberg.
‘Family’ Comes First at St. John’s Episcopal Hospital Program
From left to Right: Drs. Krina Chavda, Lawrence Schiffman,Adriana Ros, and James Briley Jr.
Page 9
When you think of Indiana, you prob-ably think of corn fields, theIndianapolis Colts and of course, theHoosiers. But did you know thatIndiana University (IU) in Indianapolishas been playing host to a renownedannual dermatology basic sciencereview course for the past 12 years?
Covering the BasicsThe Introduction to Cutaneous BiologyBasic Science Course is directed byStephen Wolverton, M.D., professor ofClinical Dermatology at IU’s School ofMedicine and author of ComprehensiveDermatologic Drug Therapy. It covers avariety of topics including melanocytebiology, carcinogenesis, pharmacology,and immunology. Lectures are designedto review high yield information notonly pertinent for the dermatologyboards, but also for clinical practice.
Dr. Wolverton is joined by such promi-nent presenters as Henry Lim M.D., adermatologist at the Henry FordHospital, and Allison Vidimos, M.D.,chair of the Department of Derma-tology at theCleveland ClinicFoundation. Theone and one-halfday course is free,but attendees areresponsible fortheir lodging.
Every November,residents fromdermatology programsacross the country attend. Residentsfrom participating allopathic programsinclude IU, the Mayo Clinic, DartmouthCollege, Cleveland Clinic Foundation,Wayne State University, and the OhioState University, to name a few.
The Ohio University College of Osteo-pathic Medicine/O’Bleness MemorialHospital (OU-COM/OMH) is the onlyparticipating osteopathic dermatologyresidency program that has attendedthe course over the past four years.
“The IU course offers a unique oppor-tunity for residents to revisit basic
science concepts that remain integral totheir training and allows residents topersonally meet some of the pillars inthe dermatology community today,”notes John P. Hibler, D.O., FAOCD,program director at OU-COM/OMH.“Moreover, it reminds residents thatdermatology has its roots in the basicsciences—a fact that must be remem-bered for boards and never forgotten indaily practice.”
Adds Dawn Sammons, D.O., chief resi-dent of the OU-COM/OMH program,
who has attended the course forthe past three years, "Thebasic sciences are the onearea most of us probably likethe least studying for withregard to boards. It is a realbenefit to attend a course likethis and have experts in thefield outlining what they feelis most important for us toknow,” she says. “I also findthat I retain the information
better when I combine textbookstudying with visual and auditorylearning. For example, I can read Dr.Wolverton's text over and over, butthere's nothing quite like hearing himlecture in person to solidify principalsin your mind.”
NetworkingThe course also offers an opportunityfor dermatology residents to socializeand network. Friday night typicallyboasts a welcome reception at whichattendees can discuss their trainingprograms and develop ties in thedermatology community. Residents
share training experiences, researchinterests, and strategies for performingwell on board examinations. Moreover,some residents develop lasting friend-ships and look to the course as a mockclass reunion every year.
The 2008 Introduction to CutaneousBiology Basic Science Course is sched-uled to be held this fall (a specific datehas not yet been set) at the IU’s Univer-sity Place Conference Center located oncampus.
For more information or to registeryour program, contact Lolita R. Goensin IU’s Department of Dermatology viaemail at [email protected] or phone at317-274-7705, or visit the website athttp://medicine.iu.edu/body.cfm?id=6204&otopid=1000.
IU Course Offers Science Review, Networking Opportunitiesby Shannon Campbell, D.O.
Page 10
In Part I: Marketing YourPractice on the World WideWeb published in theWinter 2007 issue ofDermLine, Dr. Matthysdiscussed why setting up awebsite can serve as apowerful marketing tool.
Knowing that a website can serve as apowerful tool for marketing your prac-tice, many dermatologists are opting tohave one. Fortunately, building awebsite is getting easier and easier todo.
You can either set up a practicewebsite yourself or hire someone to doit. Certain considerations will influencethat decision.
Doing it yourself depends, in part, onyour computer skills. If you enjoysurfing the Web and have some experi-ence designing basic programs such asthose used in the office, then chancesare you can build your own websiteusing a web-based tool and services.
The Internet is loaded with user-friendly tools and services designed tohelp you build your own website. Forexample, www.godaddy.com allows
you to choose from a variety of webdesign plans. You can pick a layout,color schemes, and how you want thewebpages organized. You will need tosupply content including text andphotos. Options include a 5-pagewebsite or 20-page one available withintwo to four weeks. If you prefer usinga service that is geared to physicians,
you can build a website free atwww.doctorpage.com. As an AOAmember, you can create a DO-Onlinepractice website, also for free. Usingwww.vivacare.com, you can get aneasy start to a website that can bemodifiable without a domain name.Additionally, the site offers free derma-tology-specific patient educationmaterials that can be sent to yourpatients.
If you envision a website with moreadvanced features such as music, flashanimation, or e-commerce solutions,then you might want to hire a webdesigner because incorporating suchenhancements may require too steep ofa learning curve.
If your knowledge of the computerstops at how to turn it on, then hiringout is probably your best option.
A web designer will handle developingcontent, designing the site, andpromoting it so that patients seekinghealth information on the Internet willfind your site. I recommend hiring aprofessional web designer. I havefound that web designers who set upwebsites “on the side” are not alwaysas reliable as we would like, so it maybe money well spent.
Ask to see other websites that the webdesigner has done. Then look at otherdermatologists’ websites and see whatyou like and what you don’t. A websiteis ultimately an extension of your officeand personality, so you should becomfortable with what goes in it.
A host of webpage design servicesgeared to physicians exist on theInternet. Among them arewww.jigsawinc.com, www.mednet-
tech.com, www.einsteinmedical.com,and www.md-websites.com. Althoughthe tools, services, and prices varyamong them, they typically offer a staffof graphic designers, content special-ists, copywriters, and programmers tocustomize a website. They will alsoprovide updating, hosting and mainte-nance of the website after it is up andrunning.
Basic InformationThe basic information you shouldinclude on your website is your name,degree, specialty, practice location,contact information, and office policies.I like the idea of adding a biographicalprofile that elaborates on yourschooling, memberships to professionalorganizations, and professionalachievements.
Optional, but valuable information,would be patient education materialsabout diseases and conditions you treatand medical and/or surgical proceduresyou perform. Providing information onwhat you do and how you do it canhelp you develop your practice bytargeting conditions you really enjoytreating and procedures you reallyenjoy performing. You should considerincluding a disclaimer clearly statingthat you are supplying information foreducational purposes only and that youare not prescribing treatments.
I am adding testimonials from satisfiedpatients and a link towww.DrScore.com; a website thatmeasures patient satisfaction and helpsidentify ways to improve one’s practice.
Forms you may want to include are asfollows: privacy practices acknowledge-ment, patient records of disclosures,patient medical history, pre-registration,appointment requests, prescriptionrenewal requests, change of insurance,request referral, and insurance informa-tion.
Extra FeaturesIf you are considering featuring DVDquality video streaming from yourhome page with flash animation,
Part II: Marketing Your Practice on the World Wide Webby Brian Matthys, D.O.

Page 11
understand that only a smallpercentage of your patients logging inwill be able to access it. Moreover, youwant patients to focus on the text andmoving images can distract them fromdoing so.
Blogs, which are growing in popularity,can be used to insert fresh content toyour site on an ongoing basis. Thesemay be in the form of patient notices,commentary on current dermatologicalissues, or personal updates. Forexample, you may include a notice topatients informing them to update theirforms at their next visit due to youroffice switching to an electronic healthrecord, commenting on a controversialprocedure that recently grabbed thenational spotlight, or informing them ofa staff birth announcement.
Other ConsiderationsThe website should reflect the tone ofyour office. When patients go to adermatologist’s office, they expect to be
greeted with professionalism andunderstanding in a calming environ-ment. A flashy, busy, or loud intro mayoffset potential patients. You mighteven consider using the same colors inyour office as the background on thewebsite. There should be consistencyin how the pages are laid out, as well.That will facilitate patients in navigatingthe site. Ideally, patients should be twoclicks of a mouse away from the infor-mation they are seeking.
Attributes that your website shouldhave that are not obvious whenviewing the page include direct links toit from other webpages and the abilityfor patients to link to your page in thefuture. For example, patients should beable to find your website if they lookyou up by insurance, specialty, loca-tion, etc. The website should besearchable via all of the major searchengines such as Google. Every websiteshould have password protection,which enables only certain individualsto access it. This is especially importantif the website has the capability toschedule appointments or have e-commerce transactions.
Websites can be expensive as there is aone-time setup fee and a monthlymaintenance fee. They can be a moneypit as there are always new features,such as scheduling patient visits andchats between you and patients, to beadded over time. Just know what infor-
mation you want to add and recognizethat a website is always a work inprogress.
But a website is also one of the easiestways to market your practice and acost effective way to communicateinformation to patients.
Practice websites range fromfive to 20 pages, and beyond.The following is a list ofcommonly used webpages forphysician offices.
Home PageHours & ScheduleLocation and DirectionInsurancePoliciesEducation PagesFAQs (Frequently Asked Ques-tions)Practice DetailsProceduresPhysician ProfileStaff ProfilesStaff DirectoryEventsAffiliationsArticles & WritingsBefore & After/Case StudiesLinksNewsletterMedical FormsAppointmentsPrescription Renewal RequestContact UsTerms of Use/LiabilityDisclaimerE-mail Services
Source: www.md-websites.com/office.htm
Common Pageson a Website
With the Midyear Meeting slated forMarch 12-15 in Monterey, Calif., thespeakers’ roster is all set.
“Members attending the MidyearMeeting will be updated on a broadrange of new developments in derma-tology and acquire a betterunderstanding of advances in medicaland surgical therapies,” notes LeslieKramer, D.O., FAOCD, second vicepresident. “They will also gain greaterinsight into current trends in practicemanagement, as well as financial andmedical/legal challenges facing today'sclinician.”
“We’ll start the meeting with Dr. HillaryBaldwin with a much needed ‘iPlegeupdate,’” she says. “A pediatric derma-tology symposium will feature Dr. JoeMorrelli and other masters in the fieldfor the latest updates on common prob-lems in our younger patients. Dr. EdYob will serve as moderator for a multi-faceted surgical symposium,” Dr.Kramer continues. “A workshop in theuse of dermatoscopes will beconducted by one of the leadingexperts Dr. Ash Marghoob from Memo-rial Sloan-Kettering Cancer Center.These are just a few things to temptyour appetite for knowledge andcontinuing medical education.”
In addition to the educational opportu-nities, the Midyear Meeting offersseveral engaging social activities. Awine and cheese reception in NorthernCalifornia’s wine country, golfing onpart of the famous Pebble Beach resort,and a private reception at the worldfamous Monterey Bay Aquarium arejust a few ways that members and theirguests can relax and enjoy thisoutstanding venue, she adds.
For a sneak preview of the speakers’presentations, read on.
Resident SpeakersResident speaker presentations arescheduled to begin on Wednesdayafternoon. The speakers (includingtheir program and year) and theirtopics are as follows:
Marcus Goodman, D.O.NSU-COM/BGMC, 2nd YearToxic Epidermal Necrolysis: A Case Report
Andrew Racette, D.O.COMP/Phoenix, 3rd YearVoriconazole Induced Photoaging: A CaseSeries of 4 Patients
Brett Bender, D.O.Pontiac/Botsford, 3rd YearA Review of the Perforating Disorders
Alice Do, D.O.Genesys Regional Medical Center, 2nd
YearB-Cell Lymphoma
Jami Reaves, D.O.MWU/AZCOM, 2nd YearBotulinum Toxin Type A in the Treatmentof Primary Scalp Hyperhidrosis
Aaron Bruce, D.O.NSUCOM/Sun Coast, 2nd YearCamp Discovery: A Resident’s Experience
Keoni Nguyen, D.O.O’Bleness Memorial Hospital, 1st YearNative American Dermatology: DoesPercent Tribal Heritage Influence Cuta-neous Disorders?
Heather Higgins, D.O.Oakwood Southshore Medical Center,2nd YearLate Onset Focal Elastosis Following Radi-ation Therapy
John Coppola, D.O.Pontiac/Botsford, 2nd YearCalcipotriene as a Treatment for SteroidResistant Granular Parakeratosis
Joseph Machuzak, D.O.COMP/Phoenix, 2nd YearCutaneous Manifestation of MetastaticProstate Cancer
Sanjay Bhambri, D.O.TUCOM/Valley Hospital MedicalCenter, 2nd YearEpidermal Growth Factor ReceptorInhibitors: Dermatologic Implications
Johnny Gurgen, D.O.NSUCOM/Sun Coast, 1st Year
Scarring Alopecias
Patrick Keehan, D.O.NE Regional Medical Center-Texas, 1st
YearFluoroscopy Induced RadiationDermatitis
Dawn Sammons, D.O.O’Bleness Memorial Hospital, 3rd YearThe 308mm Excimer Laser for the Treat-ment of Alopecia Areata: A Case Series
Bradley Neuenschwander, D.O.Pontiac/Botsford Osteopathic Hospital,2nd YearNail Patella Syndrome
Ryan Carlson, D.O.Oakwood Southshore Medical Center,3rd YearNevus Depigmentosus
Daniel Hansen, D.O.Oakwood Southshore Medical Center,2nd YearGeneralized Essential Telangectasia
Elaine Miller, D.O.NE Regional Medical Center-Texas, 2nd
YearDeep Tip Stitch
Ramona Nixon, D.O.O’Bleness Memorial Hospital, 2nd YearA Case Report: Aggressive Melanoma in aPediatric Patient
Michelle Jeffries, D.O.COMP/Phoenix Area, 1st YearAquagenic Syringeal Acrokeratoderma
Shannon Campbell, D.O. O’Bleness Memorial Hospital, 1st YearUnusual and Aggressive Case of CTCL
Risa Ross, D.O.NSUCOM/Sun Coast, 1st YearSunless Tanning: Is it a Safe Alternative?
Lyubov Avshalumova, D.O.NSUCOM/Sun Coast, 1st YearKaposi’s Sarcoma
David R. Bonney, D.O.NSU-COM/BGMC, 3rd Year
Speakers Line Up for Midyear Meeting
Page 12Page 12

Page 13
Siblings with X-Linked Receive Ichthyosis:A Case Report and Brief Review
Kristy Gilbert, D.O.NE Regional Medical Center, 3rd YearVarivax Associated Herpes Zoster
Karthik Krishnamurthy, D.O.St. Barnabas Hospital, 2nd YearBlood Root Necrosis
Chad Peterson, D.O.MWU/AZCOM, 3rd YearWells Syndrome: Eosinophilic CellulitesSecondary to Infliximab Infusion Therapy
The Welcome Reception, sponsored byPharmaDerm, will be held from 6 p.m.to 9 p.m.
Guest SpeakersGuest speakers are slated to presentThursday morning. The speakers andtheir topics are as follows:
Hilary Baldwin, M.D.iPledge Update
Ronald Henrichs, CAEAmerican Academy of DermatologyAAD Update
Sharon Andrews, R.N., CCS-P, andEarlene Vittonne, R.N., CHRMDermResources, L.L.C.Dermatology Coding-Part 1
Sharon Andrews, R.N., CCS-P, andEarlene Vittonne, R.N., CHRMDermResources, L.L.C. Dermatology Coding-Part 2
Mark Kuriata, D.O.Physician Extenders in DermatologyPractice
A golf outing will follow lunch. Areception at the Monterey BayAquarium will be held between 5:30p.m. and 7:00 p.m.
More guest speakers are slated topresent on Friday morning. Thespeakers and their topics are asfollows:
Aurora Badia, D.O.Acne
Joan Tamburro, D.O.Pediatric Vascular Lesions: A Multidisci-plinary Approach
Joe Morelli, M.D.Eczema-Why I Do What I Do
Miles Weinberger, M.D.Urticaria & Atopic Dermatitis—An Aller-gist’s Approach
The Surgical Symposium is scheduledfor the afternoon. Edward H. Yob,D.O., FAOCD, clinical associateprofessor at the University of Okla-homa-Tulsa, and Mohs FellowshipDirector at Dermatology Associates ofTulsa will serve as moderator. Speakerslisted with their topics include thefollowing:
Terrence A. Cronin, Jr., M.D.Cronin Skin Cancer CenterMelbourne, Fla.Unusual Wound Closures
Carol D. Cola, D.O.Mohs Fellow-Dermatology Associatesof TulsaEar Reconstruction Following MohsSurgery
Ronald P. Rapini, M.D.Professor & Chair—Dept of Derma-tologyUniversity of Texas Medical School-M.D. Anderson Cancer CenterHoustonSurgical Margins in Excisional Surgery
Daniel M. Siegel, M.D.Clinical Professor of Dermatology,SUNY Downstate DirectorSmithtown, New YorkThe Graft Universe: New Items, New Inter-pretations, New Uses
Donald K. Tillman, Jr., D.O., president-elect AOCDHays, Kan.Non-Surgical Treatment of Skin Cancer
Craig L. Ziering, D.O.Founder & Medical DirectorZiering Medical, Beverly Hills, Calif.Clinical Associate Professor of Derma-tology, University of California Irvine,Beverly Hills, Calif.New Breakthroughs in Hair Restoration b
The President’s Reception and Banquetwill be held from 6:00 to 9:00 p.m.
On Saturday morning, the followingspeakers (and their topics) will present:
Sharon Andrews, R.N., CCS-P, andEarlene Vittonne, R.N., CHRMDermResources, L.L.C.Finding and Keeping the Right Personnel
Joe Susa, D.O.Hot Topics in Dermatopathology
Ashfaq Marghoob, M.D.Dermoscopy Workshop
Graceway Pharmaceuticals
is a proud sponsor of the
American Osteopathic
College of Dermatology
What do osteopathic dermatologistsand dolphins have in common?
Monterey will be teaming with bothtypes of mammals as it hosts the AOCDMidyear Meeting this March.
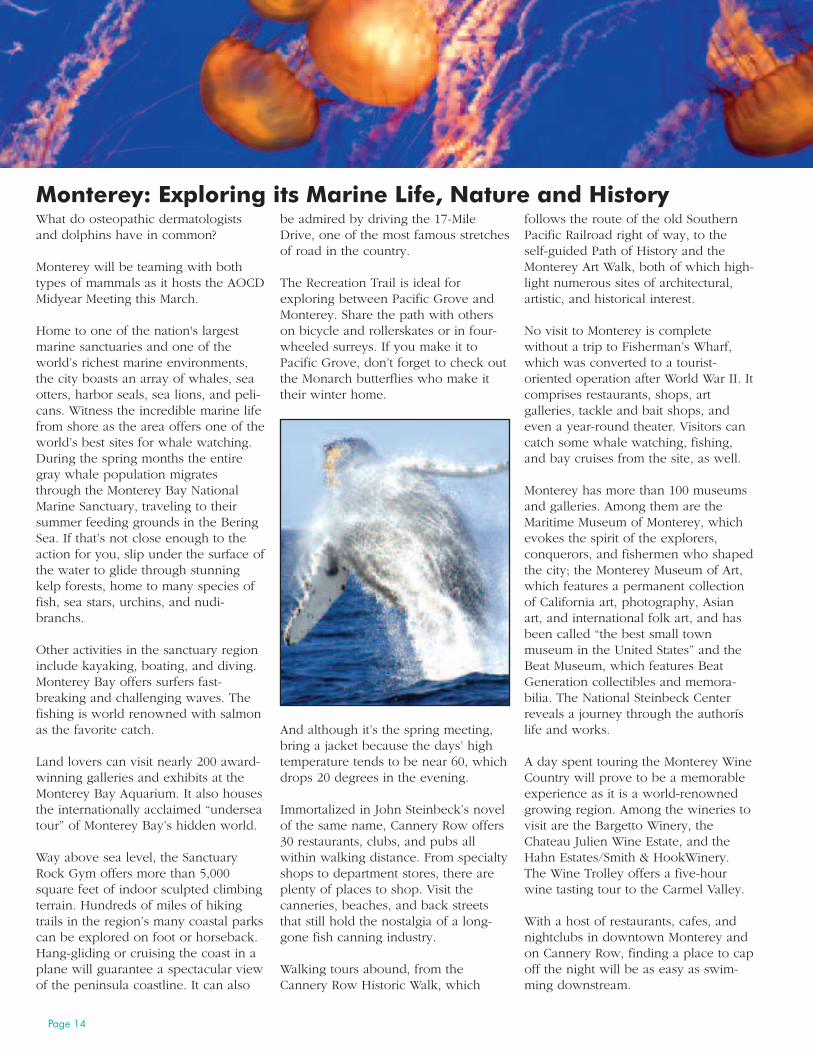
Home to one of the nation's largestmarine sanctuaries and one of theworld’s richest marine environments,the city boasts an array of whales, seaotters, harbor seals, sea lions, and peli-cans. Witness the incredible marine lifefrom shore as the area offers one of theworld’s best sites for whale watching.During the spring months the entiregray whale population migratesthrough the Monterey Bay NationalMarine Sanctuary, traveling to theirsummer feeding grounds in the BeringSea. If that’s not close enough to theaction for you, slip under the surface ofthe water to glide through stunningkelp forests, home to many species offish, sea stars, urchins, and nudi-branchs.
Other activities in the sanctuary regioninclude kayaking, boating, and diving.Monterey Bay offers surfers fast-breaking and challenging waves. Thefishing is world renowned with salmonas the favorite catch.
Land lovers can visit nearly 200 award-winning galleries and exhibits at theMonterey Bay Aquarium. It also housesthe internationally acclaimed “underseatour” of Monterey Bay’s hidden world.
Way above sea level, the SanctuaryRock Gym offers more than 5,000square feet of indoor sculpted climbingterrain. Hundreds of miles of hikingtrails in the region’s many coastal parkscan be explored on foot or horseback.Hang-gliding or cruising the coast in aplane will guarantee a spectacular viewof the peninsula coastline. It can also
be admired by driving the 17-MileDrive, one of the most famous stretchesof road in the country.
The Recreation Trail is ideal forexploring between Pacific Grove andMonterey. Share the path with otherson bicycle and rollerskates or in four-wheeled surreys. If you make it toPacific Grove, don’t forget to check outthe Monarch butterflies who make ittheir winter home.
And although it’s the spring meeting,bring a jacket because the days’ hightemperature tends to be near 60, whichdrops 20 degrees in the evening.
Immortalized in John Steinbeck’s novelof the same name, Cannery Row offers30 restaurants, clubs, and pubs allwithin walking distance. From specialtyshops to department stores, there areplenty of places to shop. Visit thecanneries, beaches, and back streetsthat still hold the nostalgia of a long-gone fish canning industry.
Walking tours abound, from theCannery Row Historic Walk, which
follows the route of the old SouthernPacific Railroad right of way, to theself-guided Path of History and theMonterey Art Walk, both of which high-light numerous sites of architectural,artistic, and historical interest.
No visit to Monterey is completewithout a trip to Fisherman’s Wharf,which was converted to a tourist-oriented operation after World War II. Itcomprises restaurants, shops, artgalleries, tackle and bait shops, andeven a year-round theater. Visitors cancatch some whale watching, fishing,and bay cruises from the site, as well.
Monterey has more than 100 museumsand galleries. Among them are theMaritime Museum of Monterey, whichevokes the spirit of the explorers,conquerors, and fishermen who shapedthe city; the Monterey Museum of Art,which features a permanent collectionof California art, photography, Asianart, and international folk art, and hasbeen called “the best small townmuseum in the United States” and theBeat Museum, which features BeatGeneration collectibles and memora-bilia. The National Steinbeck Centerreveals a journey through the authoríslife and works.
A day spent touring the Monterey WineCountry will prove to be a memorableexperience as it is a world-renownedgrowing region. Among the wineries tovisit are the Bargetto Winery, theChateau Julien Wine Estate, and theHahn Estates/Smith & HookWinery.The Wine Trolley offers a five-hourwine tasting tour to the Carmel Valley.
With a host of restaurants, cafes, andnightclubs in downtown Monterey andon Cannery Row, finding a place to capoff the night will be as easy as swim-ming downstream.
Monterey: Exploring its Marine Life, Nature and History
Page 14
Page 15
Starting in 2008 there are several taxlaw changes that apply specifically tophysicians. The following are key ones:
SUVs will no longer have the imme-diate $25,000 one-year deduction. Allvehicles used for 50% businesspurposes can only be written off oneextended time period.
Beginning in 2010, physicians canconvert their regular IRAs into tax-freeRoth IRAs regardless of their incomelevel. Rules for conversion, such as
immediate taxation on the amount ofthe Roth IRA, will be enforced.
Physicians can no longer shift incometo their children for college expenseson a tax deductible basis. However,children seven years and older canearn up to $5,350 free of federal taxes,in exchange for services rendered tothe practice. These monies can alsoqualify for a Roth IRA. While contribu-tions will not be deductible, theearnings will grow tax free. Unearnedincome greater than $1,700 per child
annually is taxed at the parents’ rateuntil the child graduates from collegeor until the age of 24. If the child usesthese monies for full-time collegepayment, they will qualify for educa-tional tax credits such as “hope andlifetime tax credits.”
Remember, meals for staff can be 100%deductible if they are for certain holi-days (Christmas, Hanukah, etc.) orsocial/recreational outings for thebenefit of the employees. Meals forstaff meetings and continuing medicaleducation meetings, as well as physi-cian meals are only 50% deductible.However, some accountants will deduct100% of lunches purchased for busi-ness meetings if they are carryoutlunches for employees.
Financial Tidbits: Tax Law Changesby Robert Schwarze, D.O., FAOCD
Tanning bed labels will be scrutinizedby the Food and Drug Administration(FDA) under a new law.
The Tanning Accountability and Notifi-cation Act—also known as the TANAct—became law last September.
The law charges the FDA with deter-mining whether the labelingrequirements for indoor tanningdevices, including the positioningrequirements, provide sufficient infor-mation to consumers regarding the riskthat the use of such devices pose for
the development of irreversible damageto the eyes and skin, including skincancer. Additionally, the FDA isexpected to determine whether modi-fying the warning label required ontanning beds to read, “Ultraviolet radia-tion can cause skin cancer,” or anyother additional warning, wouldcommunicate the risk of indoor tanningmore effectively or whether there is nowarning that would be capable ofadequately communicating such risks.
To help make these determinations, theFDA is required to conduct appropriate
consumer testing to determine thepublic’s understanding of label warn-ings. The Secretary of Health andHuman Services is required to reportback to Congress within one year. Thisreport should include the measuresbeing implemented to significantlyreduce the risks associated with indoortanning devices.
The TAN Act was included in the FDAAmendments Act of 2007.
Numerous studies have shown that theuse of tanning beds is a significant riskfactor for the development ofmelanoma. Tanning beds increase therisk of skin cancer much like exposureto the sun, but may be moredangerous, according to the Centers forDisease Control and Prevention. Expo-sure to tanning beds increases chancesfor squamous cell carcinoma by 2.5times and the likelihood of developingbasal cell carcinoma by 1.5 times. TheWorld Health Organization recom-mends that no person under the age of18 use a tanning bed because of theassociated increased risk for skincancer.
Tanning Bed Labels Come Under Scrutiny Thanks to New Law

Page 16
The quest for eternal youth is as old asmankind itself. Some of the earliestprescriptions that have survived fromantiquity are elixirs for creams andsalves designed to produce or maintaina youthful appearance.
Scientifically proven, efficaciousmodalities firstappeared in the nine-teenth century withthe advent ofchemical peels andplastic surgery.Crude and fraughtwith significantrisks, these tech-niques improvedover time and grew inuse throughout the early twentiethcentury. The big breakthrough in anti-aging and skin rejuvenation came inthe 1980s with the discovery of alphahydroxy acids. These chemicals, whenused in high concentrations as peelsand at lower concentrations in dailycare, were shown to reduce wrinklesand increase protein production inskin. Thus, the first “anti-wrinkle” and“anti-aging” products appeared on themarket. Shortly afterward, the Univer-sity of Michigan’s DermatologyDepartment released a study showingsimilar results for topical tretinoin, aprescription drug. The combination ofthese two phenomena coupled with thebaby boom generation reaching middleage launched the “anti-aging” productmarket.
Throughout the 1990s, anti-aging wassynonymous with topical therapy,whether it was an in-office chemicalpeel or a daily home care productregimen. Non-pharmaceutical entitiesproliferated, each touting a new anti-aging benefit. The neologism“cosmeceutical” was invented to coverthese products, which exist in a regula-tory grey area between a traditionalcosmetic and a full-blown drug entity.It is important to note that from a regu-latory standpoint, the Food and DrugAdministration (FDA) does not recog-nize this category.
Simultaneously, energy-based therapiespromising similar or better results thantopicals were being introduced. Thefirst lasers were crude instruments that
“peeled” skin by burning it off. Bythe dawn of the new millen-
nium, non-ablativeenergy-based machineswere showing inter-esting results in thelower epidermis andpapillary dermiswithout the down-time associated with
the earlier instru-ments.
Then a revolution inanti-aging quietly began: the advent offillers and neurotoxins. Both had beenaround for a while, but by 2002 fillershad improved significantly and Botox®was approved for cosmetic use. As aresult, in the past six years fillers andneurotoxins have dominated the fieldof aesthetic medicine, with the use oftopical treatments being pushed furtherto the periphery. At a three-daymedical conference I recently attended,for instance, only one hour wasdevoted to a discussion of cosmeceuti-cals.
In the introduction to the July 2007supplement to Cosmetic Dermatology(“Advancing Facial Aesthetics: Opti-mizing Outcomes and ImprovingPatient Satisfaction”), Joel L. Cohen,M.D., writes:
“When used properly, nonsurgicalfacial cosmetic procedures canprovide patients with a natural,more relaxed look, soften the signsof aging, improve overall appear-ance, and allow patients to moreaccurately reflect their emotions…These therapies are recognized forquickly and remarkably improvingfacial lines, enhancing existingfeatures, de-emphasizing asymme-tries, and minimizing various signsof aging.”
Dr. Cohen clearly and accurately cate-gorizes these procedures as alternativesto surgery and identifies their effectsand benefits as changing the appear-ance of the face. As entities that alterappearance, fillers and neurotoxins areunparalleled by anything that can beachieved topically, in terms of bothdegree and speed, providing thepatient with positive visible resultsalmost instantly. Because of thedramatic improvements in nonsurgicalprocedures and the instant gratificationthat they provide, many aesthetic prac-tices are providing these servicesalmost to the exclusion of topical treat-ments.
By concentrating solely on the appear-ance aspect of aging whilede-emphasizing and reducing the useof topical treatments for aging skin,dermatologists are, in my opinion,missing an important component of theaesthetic practice. Nonsurgical tech-niques that alter appearance do nothing
to improve theoverall health orwellness of theskin, which is,after all, an organof the body thatrequires nourish-ment and care to
function prop-erly.
Considerthe treat-
ment ofanother crit-
Slotting Cosmeceuticals in the ‘Anti-Aging’ MarketTo deliver youth, beauty and wellness to patientsby Elliott Milstein

ical organ, the heart. If a patient pres-ents to the cardiologist with severethrombosis, clearly surgical interventionis necessary to return the heart toproper functioning. But the physicianalso will stress the need for proper dietand exercise to return the heart tocomplete health and maintain wellness.
Cosmeceuticals are the “diet and exer-cise” of the skin. Exfoliants,anti-oxidants, growth factors, peptides,amino acids, lipids, skin lighteningagents, plant extracts, and vitamins allhave their place and each performs afunction, to a greater or lesser extent,in nourishing, correcting, stimulating,and protecting this organ.
The instant results and the tremendouspopularity of nonsurgical procedures isthe primary reason that dermatologistshave migrated away from using cosme-ceuticals. But I suspect that anotherinhibition stems from the confusingplethora of treatment options—most ofwhich have little or no scientificsubstantiation—that is offered to themon a daily basis. Dermatologists have,rightly, come to question whether anyof these products have any worth andhave begun to suspect the entireuniverse of products. Due to this lackof faith in the efficacy of topical treat-ments, many dermatologists havedecided to simply stock and sell what-ever products patients request.
While this may seem like an easy andexpedient way to meet customerdemand, it is of no help to the patientwho, now more than ever, needs theguidance of a skin care expert in navi-gating the confusing market of topicaltreatment options. There are manyproducts and product lines on themarket that are of no real value, butthere are also many of significant value.The problem is the products thatpatients ask for are typically those thatappear most often in the general mediaand are more likely to be of the “novalue” variety. Dermatologists need tosteer their patients clear of media hypeand direct them to efficacious modali-ties.
Failing to do so is not just a disserviceto the patient; it also devalues the role
of the dermatologist in the patient’seyes. If the skin care experts offer noadded value in the choice of products,what is the point of purchasing them atthe physicians’ office? The consumerdoes not need another retail outlet thatsimply supplies products with thelargest advertising and public relationsbudgets. Not only do dermatologistsfail their patients by turning theiroffices into a retail store; they alsoharm themselves. In the long run, theycannot compete with the Sephoras ofthe world.
Dermatologists are right to bemoan thelack of data provided by the marketersof these products. But they also needto understand that it is the regulatorystatus of the products—not the desireof the manufacturer or the efficacy ofthe products—that makes such testingimpossible. If a company conducts clin-ical studies for products marketed ascosmetics and the results are published,the FDA can use these data to declarethe products “drugs,” thus making itillegal to sell them. Most companiescannot take that chance.
Consequently, dermatologists mustlearn how to evaluate cosmeceuticalswithout the tools they normally usefor product evaluation. Absentsuch evaluation, dermatolo-
gists risk either becoming a meregeneric skin care retailer or ignoringcosmeceuticals altogether. In bothcases, they are denying the benefits ofthese products to their patients, fallingback on procedures exclusively in theiranti-aging armamentarium.
It is here that the osteopathic dermatol-ogist can take a lead over his or herallopathic counterpart. Since one of thehallmarks of osteopathic medicine is awhole body approach, the DO derma-tologist is in the best position toprovide nonsurgical aesthetic proce-dures in combination with appropriatetopical therapy, thus delivering to thepatient a more youthful appearanceand healthier skin.
Elliott Milstein is president andchief operating officer of Fern-dale, Mich.-basedBiopelle, Inc., a Fern-dale Pharma Groupcompany.
Page 17

Page 18
VO
LUN
TEER
SPOTLIGHT
Last September,Jere Mammino,D.O., FAOCD,saw the largestthyroid goiter—the size of agrapefruit—heever saw in hislife. Next was aBuruli ulcercaused by infec-tion withMycobacteriumulcerans, a raretype of bacteriafound in tropicaland subtropicalclimates.
No, he wasn’t at a dermatology sympo-sium. He was on a medical mission inGhana, West Africa.
Probably the most unusual case hesaw—more so for the circumstancessurrounding it—was a woman whopresented with a large bite wound onher cheek. She explained that herhusband’s other wife bit her after hereturned from a business trip.(Polygamy is legal in Ghana.) Appar-ently, he had bought his one wife apurse and not the other. Dr. Mamminotreated the wound with antibiotics anda topical cream.
But the majority of dermatologicalconditions he treated were typical ofthose he treats in his Orlando practice,they just tended to be more severe. Forexample, impetigo is very common inyounger children, resulting from themscratching a mosquito bite that goesinto a secondary infection. There was ahigher prevalence of fungal and staphinfections, as well.
Although patients with skin problemswere sent Dr. Mammino’s way as hewas the only dermatologist on themission, only approximately one-thirdof the patients he saw had derma-tology-related problems. The majorityhad general medical ailments. Acommon one was low back painbecause many of the local people make
their living as farmers. Malaria was alsovery common in the area.
During the two-week trip, Dr.Mammino and his 26 colleagues,including a retired emergency roomphysician, nurse practitioners, physicianassistants, nurses, and a medicalstudent, stayed in a fairly new moteljust outside of Nkwanta, a town ineastern Ghana. “The standards of theaccommodations were very high,” hesays. “Some of us even had hotshowers, which is unusual in this partof the world.”
They ventured to three villages,packing up two buses full of supplies,medication, and the team. The groupwith which he went—the Fellowship ofthe Association of Medical Evange-lists—had done previous medicalmissions in Ghana, so it had good rela-tions with the local government.
Consequently, they wereallowed to treat patientsin school buildings. Aschool is a good sitebecause it has a roof,making it cooler inside,and it is very good forpatient flow, Dr.Mammino explains. “Youstart people at one endof the school and youwork your way down.”The nurse takes thepatient’s name, vitalsigns, and chief concern.The patient sees thedoctor or physician
assistant who gives a diagnosis, writesdown a prescription, and the patientpicks up the medication at themakeshift pharmacy.
“We bring all our own medications andsupplies,” he says. “The supplies thereusually aren’t very good.” Everybodybrings two suitcases, one for personalitems and the other one loaded withmedications and supplies. Pharmaceu-tical representatives are a primarysource for such donations.
Typically when they arrive at a site,there are hundreds of people waiting.“It could be overwhelming if you let it,”says Dr. Mammino. “But you just takeone person at a time and do your best.”
The most important thing is to beorganized, he adds. For example, thefirst day there the team spends sortingout all the medications. They are
On the Road to Ghana with Dr. Mammino

Page 19Page 19
divided into three piles to ensure thatthere will be medications for eachvillage they visit.
“People are used to waiting formedical care all day, which my patientsin the United States wouldn’t tolerate,”says Dr. Mammino. “It’s like an outingfor them.” The team had a personmaking balloon animals and playinggames with the children to keep themoccupied. “If we can’t see everybodyby day’s end, we at least give themvitamins,” he says. The team treatedapproximately 900 patients by the endof the mission.
The team was well received. “Thepeople are happy to see us. They havea very simple lifestyle, yet they are veryhappy, in general,” he observes. Amission trip helps Dr. Mammino keephis life in perspective. “It helps mekeep my priorities straight,” he adds.
Although the medical encounters wentsmoothly, getting around was anotherstory. Apparently there during the rainyseason, the dirt roads quickly becamemud slides. When attempting to reachtheir base, the five-hour ride turnedinto a 12-hour ordeal as the buses gotstuck repeatedly. In fact, older boysand young men from the villagescongregated on the roadside andoffered to push cars out for a fee. “Itwas usually a dollar, and it was wellworth it,” he says. “If you saw a groupof young boys hanging around near theroad, then you knew there was a holecoming up some place down the road.”
Ironically, communicating was not thatdifficult even though 90 percent of thepeople spoke a local tongue called“Tuwuli” as the team enlisted the helpof local translators who were largelypastors. English is the official languageof Ghana, but only approximately 10percent of the people speak it in thelow lying mountainous countryside.
There was not much time for extracur-ricular activities, but the team did get toattend a local church service, andspend a half-day site seeing, whichincluded hiking in a nature preserve.They even spent a couple of hours intown to shop in the tourist area, basi-
cally an acre of wooden stalls wherepeople sold handmade trinkets. “I’mnot a big souvenir person,” he says.
This is Dr. Mammino’s seventh medicalmission. He has also been to Kenya,the Amazon, and Nicaragua. He wenton his first mission when he took theplace of another physician whodropped out at the last minute.Although Dr. Mammino was hesitant,he pushed himself past his comfortzone to go. One of his reservations wasthat Dr. Mammino expected to comeacross weird tropical diseases that hemight not be able to treat. The derma-tologist with 20 years of experience
subsequently learned that the unusualtropical diseases were few and farbetween, although interesting whenthey did come up as was the case inGhana.
There are a host of opportunities forphysicians out there, whether it’s amedical mission or a secular trip, hesays. “You think you are going overthere to help others, but the feelingyou get out of it is much greater thanwhat you put into it.”
Buruli Ulcer

American Osteopathic College of Dermatology1501 E. IllinoisKirksville, MO 63501
PRSRT STD
U.S. POSTAGE PA I D
PERMIT # 1556
ORLANDO, FL
Journal of the American Osteopathic College ofDermatology-JAOCD.
We are now accepting manuscripts for the publicationin the upcoming issue of the JAOCD. ‘Information forAuthors’ is available on our website at www.aocd.org.Any questions may be addressed to the Editor [email protected] . Member and resident membercontributions are welcome. Keep in mind, the key tohaving a successful journal to represent our college isin the hands of each and every member and residentmember of our college. Let’s make it great!
- Jay Gottlieb, D.O.
Related Documents











