Winterfield – Dermatology for the PCP March 9, 2018 1 Dermatology for the PCP Laura S. Winterfield, MD MPH Associate Professor Medical University of South Carolina I have no relevant conflicts of interest.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Winterfield – Dermatology for the PCP March 9, 2018
1
Dermatology for the PCP
Laura S. Winterfield, MD MPHAssociate Professor
Medical University of South Carolina
I have no relevant conflicts of interest.

Winterfield – Dermatology for the PCP March 9, 2018
2
Learning Objectives
• Identify common skin conditions and potential mimickers
• Describe first‐line therapies for common skin conditions
• Recognize when to refer/collaborate with dermatology
Primary Care Skin Complaints
• Facial breakout
• Rash
• Suspicious Spot(s)

Winterfield – Dermatology for the PCP March 9, 2018
3
19yo Male with breakouts
• Several years
• Tried OTC products
• No systemic meds
Acne vulgaris
Pathogenesis therapeutic targets:1. Abnormal desquamation with
obstruction of the pilosebaceouscanal
2. Androgen‐driven excess sebum production
3. Propionobacterium acnes4. Altered immune activity and
inflammation

Winterfield – Dermatology for the PCP March 9, 2018
4
Acne vulgaris
Topical retinoid: mainstay of therapy
Benzoyl peroxide
Topical antibiotics
Other topicals
Oral antibiotics
Derm referral
Isotretinoin
Sebum production
AlteredKeratinization
P. acnes Inflammation
Benzoylperoxide ++ ++++Topical retinoid +++ ++Salicylic acid +Azelaic acid ++ ++ +Topical Antibiotic ++ +Oral Antibiotic + +++ ++Oral Retinoid (isotretinoin) ++++ +++ + +++Hormonal tx +++ +
Adapted from Farrah and Tan in Dermatol Ther 2016: 29:377‐84.
Winterfield – Dermatology for the PCP March 9, 2018
5
Topical Retinoids
• Options:
– Adapalene
• 0.1% gel: Now OTC
– Tretinoin cream, gel, microsphere gel
• 0.025%, 0.05%, 0.1% and others
• Generics may not be stable in UV (apply at night)
– Tazarotene
• Pregnancy category X
Topical Retinoids
• Once daily application:
– Start every 1‐3 days and increase to QHS
– “Pea” size for entire face
• Thin layer, after gentle washing and drying
• SE: dryness, peeling, redness, irritation, sun sensitivity
• May take 4‐6 weeks to see benefit
• Continue for maintenance

Winterfield – Dermatology for the PCP March 9, 2018
6
Antibiotics for Acne
• Topicals:– Clindamycin gel, lotion, solution
– Erythromycin gel, solution (less effective, more resistance)
• Oral:– Tetracycline
– Doxycycline
– Minocycline
• Avoid use as monotherapy– Use with topical retinoid or benzoyl peroxide
Antibiotics for Acne
• Goal: stop systemic antibiotics in <3 months
• No great data for which antibiotic is best
• Avoid use as monotherapy
• Plan for maintenance topical therapy
• Refer for consideration of isotretinoin in refractory patients, cystic lesions or scarring

Winterfield – Dermatology for the PCP March 9, 2018
7
38yo Female with acne
• “clear skin as a teenager”
• Flares with menses
• Was on OCP, now has IUD
Female adult acne
• Lower face/jawline• Often resistant to traditional combination therapy
• Treat with topical retinoids• Consider topical dapsone• Target hormonal component
– OCP– Spironolactone
• Consider evaluation for PCOS especially if other signs present (hirsutism, irregular menses, etc)

Winterfield – Dermatology for the PCP March 9, 2018
8
Skin Care Products
• Non‐comedogenic, oil‐free, “won’t clog pores”– Moisturizer
– Make‐up
– Sunscreen: helps reduce post‐inflammatory pigmentary alteration
• Gentle cleansers
• Gentle emollients
• Avoid harsh, abrasive, or excessively drying (alcohol)
27yo F with refractory acne
• Acne Excoriee• Predominantly secondary change
• “picker’s acne” or skin‐picking disorder
• More common in females• Consider psychiatric comorbidity– Depression– Anxiety– OCD– ADHD

Winterfield – Dermatology for the PCP March 9, 2018
9
Acne treatment in Pregnancy
• Limited options
• Category B
– Topical clindamycin
– Topical azelaic acid
• Retinoids are category C or X
• Occasional intralesional kenalog for inflamed cysts
Diet in Acne
• Low glycemic diet
– Decreased acne severity
– Smaller sebaceous glands
• Low dairy
– Limit skim milk and ice cream
– Whey protein (derived from milk) reported to trigger truncal acne in adolescents

Winterfield – Dermatology for the PCP March 9, 2018
10
50yo F with facial breakouts
Rosacea
• More common in fair skin types
• Flushing with fixed facial erythema
• +/‐ Papules and pustules
• No comedones
• Triggers of flushing:
– Dietary
– Environmental
– Menopause
Winterfield – Dermatology for the PCP March 9, 2018
11
Treatment of Rosacea
• Trigger avoidance
• Topicals:
– Antibiotics: metronidazole gel or cream
– Anti‐inflammatory: azelaic acid cream or solution
– Anti‐parasitic: ivermectin 1% cream
– Alpha‐2 agonist: brimonidine, oxymetazoline
• May cause rebound flushing in some patients
• Oral antibiotics: tetracyclines, submicrobial dose
• Laser: Best option for persistent redness
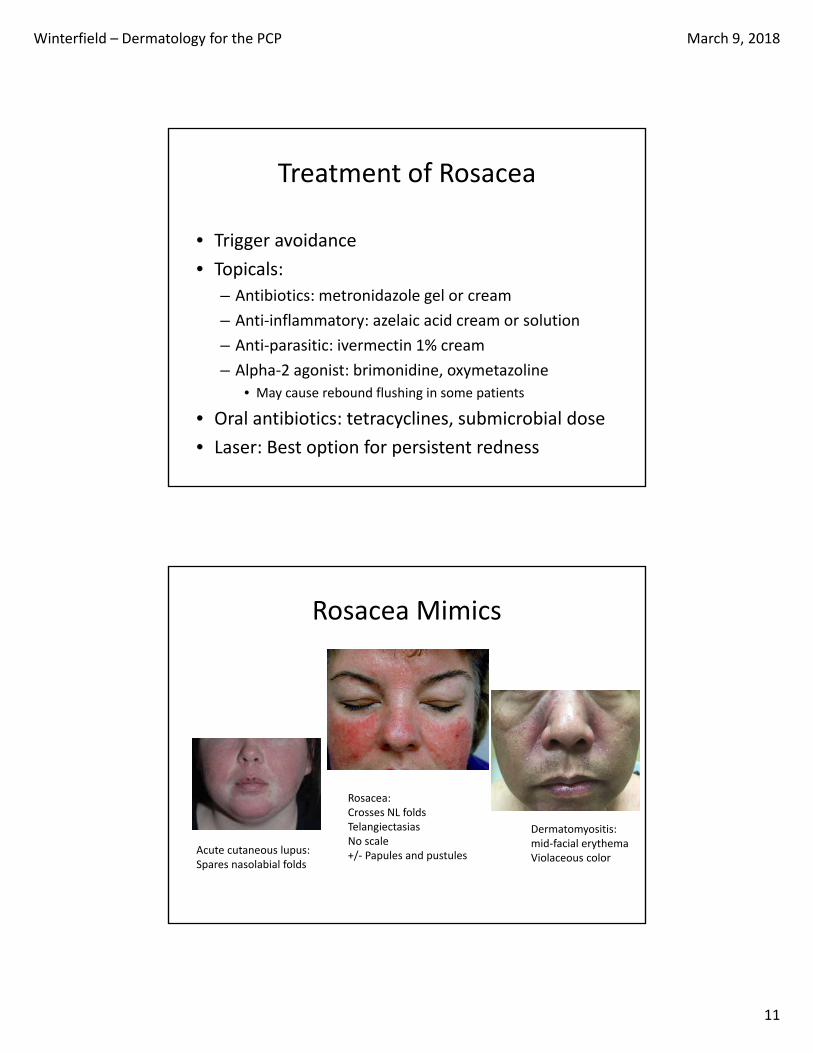
Rosacea Mimics
Acute cutaneous lupus:Spares nasolabial folds
Dermatomyositis:mid‐facial erythemaViolaceous color
Rosacea:Crosses NL foldsTelangiectasiasNo scale+/‐ Papules and pustules

Winterfield – Dermatology for the PCP March 9, 2018
12
20yo rash around the nose
Perioral dermatitis:Monomorphic papules sparing the vermillion
Treat like rosaceaavoid topical steroids and other triggers
Seborrheic dermatitis:Greasy yellow scale, nasolabial folds, ears, beard and scalp
Treat with topical ketoconazoleTopical steroids for itch
72yo F with itchy rash

Winterfield – Dermatology for the PCP March 9, 2018
13
72yo F with itchy rash
• Several weeks
• Started with an abrasion
• Treating with neosporin
• No fever, chills, other sx
• No new medications
Allergic Contact Dermatitis
• Type IV hypersensitivity
• “outside‐in” pattern
• Common allergens:
– Topical antibiotics
– Nickel
– Propylene glycol
– Formaldehyde
– Poison Ivy

Winterfield – Dermatology for the PCP March 9, 2018
14
Allergic Contact Dermatitis
Treatment
• Topical steroids
– High potency
• Systemic steroid taper for severe cases
– Poison ivy 3‐4 weeks
• Recurrent cases with unknown trigger?
– Referral for patch testing
Auto‐eczematization
• Severe focal allergic or eczematous dermatitis becomes generalized
• AKA: “id” reaction

Winterfield – Dermatology for the PCP March 9, 2018
15
Herpes Zoster
• Respects the midline
• Lesions have scalloped borders
– Vesicles
– Erosions
– Ulcers
Herpes
• Unilateral or bilateral, often recurrent
• Scalloped borders
• Vesicles or erosions
• Often no known history of genital HSV
• Blisters on the buttocks are almost always HSV‐‐No such thing as recurrent spider bites on the buttocks!

Winterfield – Dermatology for the PCP March 9, 2018
16
Eczema Herpeticum
• Superinfection of dermatitis with HSV
• Look for scalloped edges, crusting
• Increase in symptoms—pain, severe itch/burning
67yo rash all over torso
Started on back, folds and spread
Medication history:

Winterfield – Dermatology for the PCP March 9, 2018
17
Morbilliform Drug Eruption
• Usually starts 7-10 days after initiation of the drug
• May start even after the d/c of a drug• Often starts in intertriginous and dependent
areas• May become erythrodermic• No blisters• No mucous membrane involvement
Morbilliform Drug Eruption
• Treat with topical steroids– Clobetasol for severe symptoms– Triamcinolone 0.1% cream or oint in 1lb jar– May add sauna suit or occlusion
• Antihistamines as needed• OK to treat through the eruption

Winterfield – Dermatology for the PCP March 9, 2018
18
Drug Eruption: Red Flags
• Mucous membrane involvement• Skin pain• Blisters• Systemic symptoms / toxic appearance• Facial edema• Lymphadenopathy• Lab abnormalities:
– Liver function tests– CBC with differential: elevated eosinophils– Renal function
68yo with LE discoloration

Winterfield – Dermatology for the PCP March 9, 2018
19
Stasis Dermatitis
• Topical steroids: Triamcinolone 0.1% cream
• Domeboro or dilute vinegar soaks• Emollients• Compression, elevation• Avoid topical antibiotics when possible• Bilateral lower extremity cellulitis is RARE
45yo rash on knees

Winterfield – Dermatology for the PCP March 9, 2018
20
Psoriasis
• Well‐defined red scaly plaques
• Scalp, elbows, knees, umbilicus, gluteal cleft
• Palmar‐plantar variant
• Pustular variant
• Try to avoid systemic steroids
– may flare with withdrawal
Which topical steroid?
• Clobetasol• Triamcinolone 0.1%• Desoximetasone
• Fluticasone• Desonide• Hydrocortisone 2.5%
STRONGER
STRONGER
Scalp and Body
Face and Folds
Apply BID, 2 weeks on, 1 week off, d/c when flat

Winterfield – Dermatology for the PCP March 9, 2018
21
vehicle for topical agents
Type Penetration Use
Ointment Most Dry areas
Cream Moderate Wet areas
Lotion Less intertriginous
Gel
Solution
Least Scalp, intertiginous
Psoriasis & Cardiovascular Risk
• Psoriasis (especially moderate to severe) is an independent risk factor for MI
• Patients should be educated about risk of CAD and counseled to address modifiable risk factors.
Winterfield – Dermatology for the PCP March 9, 2018
22
Psoriasis and Psoriatic Arthritis
• May present asynchronously
• Unlike skin, joint damage may be permanent
32yo with itchy ankle

Winterfield – Dermatology for the PCP March 9, 2018
23
Tinea
• Always check the feet, too!
• Especially if only 1 scaly hand:
• “1 Hand / 2 Foot tinea”
• KOH shows branching hyphae
Tinea Incognito
• Tinea that has been treated with topical steroids
• May require systemic antifungal therapy
• Terbinafine250mg/d x 2 weeks

Winterfield – Dermatology for the PCP March 9, 2018
24
Granuloma Annulare
• Tinea mimicker
• Non‐scaly
• Does NOT improve with antifungals
• Etiology unknown
Sarcoidosis
Non‐scalyAnnular plaques
Predilection for scars

Winterfield – Dermatology for the PCP March 9, 2018
25
46yo very itchy all over
Courtesy of Nellie Konnikov

Winterfield – Dermatology for the PCP March 9, 2018
26
Crusted Scabies
• Immune compromise
• Huge mite load
Scabies Prep

Winterfield – Dermatology for the PCP March 9, 2018
27
Scabies Treatment• Topical permethrin is most effective
– Treat neck down– Treat folds– Treat under nails– Repeat in a week
• Oral Ivermectin 200mcg/kg single dose– Repeat in 1 week
• Treat close contacts• Treat the environment
Concerning Spots
• Evolving Lesion (ABCD‐E)
• Tender, Burns, Itches, Bleeds
• Company It Keeps
• Solitary Lesion, “Ugly Duckling”
• Unresponsive to therapy

Winterfield – Dermatology for the PCP March 9, 2018
28
What is the most likely diagnosis?
A. Atypical nevi
B. Basal cell carcinoma
C. Dermatitis
D. Actinic keratoses
E. Squamous cell carinoma
Actinic Keratosis
• Premalignant lesion to SCC
• Who? Fair skin types, > age 40
• Where? Sun‐exposed areas
• Treatment? – Cryotherapy
– Field therapy: • topical 5‐FU
• Topical imiquimod
• photodynamic therapy

Winterfield – Dermatology for the PCP March 9, 2018
29
Photo courtesy of S. Desai
Actinic Keratoses
• Poorly defined erythematous macule/papule → gritty thin scale →thicker yellowish scale
• Signs of photodamage
This lesion may be associated with which of these?
A. Verruca
B. Seborrheic keratosis
C. Actinic keratosis
D. Squamous cell carcinoma
E. All of the above

Winterfield – Dermatology for the PCP March 9, 2018
30
Cutaneous Horn
• Column of thick keratotic scale
• Differential Diagnosis
– Wart
– Seborrheic keratosis
– Actinic keratosis
– SCC
Most likely diagnosis?
A. Actinic keratosis
B. Basal cell carcinoma
C. Cutaneous horn
D. Keratoacanthoma
E. Verruca vulgaris

Winterfield – Dermatology for the PCP March 9, 2018
31
Keratoacanthoma
• Low‐grade SCC
• Rapid growth over 4‐6wks
– +/‐ spontaneous regression
• Nodule with keratin filled central crater
Most likely diagnosis?
A. Pigmented basal cell carcinoma
B. Melanoma
C. Atypical nevus
D. Seborrheic keratosis
E. Actinic keratosis

Winterfield – Dermatology for the PCP March 9, 2018
32
Seborrheic Keratosis
‐“stuck‐on”
‐keratotic
‐verrucous
‐+/‐ pigment
‐sharply
‐demarcated
Most likely diagnosis?
A. Pigmented basal cell carcinoma
B. Melanoma
C. Atypical nevus
D. Seborrheic keratosis

Winterfield – Dermatology for the PCP March 9, 2018
33
Melanoma
• Risk factors:– Fair‐skinned
– Red hair
– Atypical nevi
– Multiple nevi (>50)
– Family history
– Blistering sunburns
– Most common malignancy in women age 25‐29
Most likely diagnosis?
A. Squamous cell carcinoma
B. Basal cell carcinoma
C. Keratoacanthoma
D. Amelanoticmelanoma

Winterfield – Dermatology for the PCP March 9, 2018
34
Basal Cell Carcinoma
• Who?– Fair skin types
• What?–Pearly, translucent, telangiectatic, rolled border
• Where?– Sun‐exposed areas
• Face, scalp, ears, neck > trunk, extremities
Why do a total body skin exam?
• To look for clues for diagnosis of a rash or other skin problem

Winterfield – Dermatology for the PCP March 9, 2018
35
Why do a total body skin exam?
• To look for clues for diagnosis of a rash or other skin problem
• Skin cancer screening
Why do a total body skin exam?
Study by Kantor and Kantor. Arch Dermatol. 2009 Aug;145(8):873‐6
How many melanomas from their practice were the noted by the patient vs how many found on dermatologist‐initiated skin exam?

Winterfield – Dermatology for the PCP March 9, 2018
36
Why do a total body skin exam?
Study by Kantor and Kantor. Arch Dermatol. 2009 Aug;145(8):873‐6
How many melanomas from their practice were the noted by the patient vs how many found on dermatologist‐initiated skin exam?
• 56.3% of melanomas were found by the dermatologist and were not part of the presenting complaint.
• Dermatologist detection was significantly associated with thinner melanomas, OR 0.42
• Thinner melanoma = better prognosis
Broad‐spectrum UVA/UVB sunscreen
Physical blockers:
titanium dioxide
zinc oxide
Chemical sunscreens

Winterfield – Dermatology for the PCP March 9, 2018
37
Ultraviolet Radiation and Sunscreen
• UVA and UVB contribute to premature skin aging and skin cancer.
• UVA: Tan• UVB: Burn
• SPF = “Sunburn Protection Factor”– Only quantifies UVB protection
• “Broad Spectrum” sunscreen has UVA + UVB protection
• No UVA protection rating in the US
Sunburn protection factor (SPF)
• Measures only UVB protection
• Recommend SPF 30+
• 1 oz (“golf ball size”) each application
• Apply every 1.5‐2h

Winterfield – Dermatology for the PCP March 9, 2018
38
Water Resistant = 40 minutesVery Water Resistant = 80 minutes
Questions?
Related Documents











