March 9, 2015 Emerging Issues in Billing and Coding Volume 2, Issue 1 CPT 11055-11057 Paring/cutting of benign lesions Medicare considers paring/cutting of corns or calluses to be ‘routine foot care,’ only covered for podiatry. Most other payers follow Medicare’s example. *** If you pare/cut warts before cryo, the paring/cutting is included within CPT 17110 . 11200-11201 Skin tag removal Insurers will only cover this with documented evidence of pain, bleeding, irritation, sensitive location, etc. Their default is to deny. ***Just saying “bothersome” or “irritated” isn’t enough – if you want it covered by insurance, get specific! 11060-11061 10140-10180 Incision and drainage Medicare will only cover this for lesions with documented abscess and/or pus collection, e.g. bullae, cysts, carbuncles, furuncles and other lovely things. ***Medical necessity is based on fluid collection, inflammation, pain, and/or infection – be sure to record all the juicy details. 11300-11446 Benign Excision or Shave Molluscum Contagiosum (078.0), Neoplasm of Uncertain Behavior (238.2), and Inflamed Seborrheic Keratosis (702.11) are all acceptable Dx’s by themselves. Lucky them! ***Everything else requires a primary and a secondary Dx to explain why the lesion needs to be removed: e.g. 216.3 Benign neoplasm face + V10.83 Personal hx of NMSC Derm Daily Digest Appearing Quarterly since September 2014 Contents: o The Emperor’s New Clothes o Countdown to Epic o Funny Coding Errors o EHR Popularity Contest o Quotes and Quips o What Do I Need To Know Before Epic Training? o EPIC by the NUMBERS! o The Emperor’s New Clothes: When No One Wants to Say “That’s Not Covered” You’ve probably heard Hans Christian Andersen’s story of the Emperor’s New Clothes – he orders this absolutely fab-ulous suit made from the most expensive material (which is invisible to “stupid” people), and no one except a small child has the courage to tell him that there is no suit and he’s parading around with nothing on. In the same vein, not all Dermatology procedures are created equal, and some are simply not covered by insurers for one reason or another. Here are some of our most frequently denied procedures and the reasoning behind the denials (you have to define “reasoning” loosely sometimes): Like this newsletter? Have a story idea or suggestion? Contact the Editor at [email protected] . Contributions welcome!

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

March 9, 2015 Emerging Issues in Billing and Coding Volume 2, Issue 1
CPT 11055-11057 Paring/cutting of benign lesions
Medicare considers paring/cutting of corns or calluses to be ‘routine foot care,’ only covered for podiatry. Most other payers follow Medicare’s example.
*** If you pare/cut warts before cryo, the paring/cutting is included within CPT 17110.
11200-11201 Skin tag removal
Insurers will only cover this with documented evidence of pain, bleeding, irritation, sensitive location, etc. Their default is to deny.
***Just saying “bothersome” or “irritated” isn’t enough – if you want it covered by insurance, get specific!
11060-11061 10140-10180
Incision and drainage
Medicare will only cover this for lesions with documented abscess and/or pus collection, e.g. bullae, cysts, carbuncles, furuncles and other lovely things.
***Medical necessity is based on fluid collection, inflammation, pain, and/or infection – be sure to record all the juicy details.
11300-11446 Benign Excision or Shave
Molluscum Contagiosum (078.0), Neoplasm of Uncertain Behavior (238.2), and Inflamed Seborrheic Keratosis (702.11) are all acceptable Dx’s by themselves. Lucky them!
***Everything else requires a primary and a secondary Dx to explain why the lesion needs to be removed: e.g. 216.3 Benign neoplasm face + V10.83 Personal hx of NMSC
Derm Daily Digest Appearing Quarterly since September 2014
Contents: o The Emperor’s New Clothes
o Countdown to Epic
o Funny Coding Errors
o EHR Popularity Contest
o Quotes and Quips
o What Do I Need To Know
Before Epic Training?
o EPIC by the NUMBERS!
o
The Emperor’s New Clothes:
When No One Wants to Say “That’s Not Covered”
You’ve probably heard Hans Christian Andersen’s story of the Emperor’s
New Clothes – he orders this absolutely fab-ulous suit made from the most
expensive material (which is invisible to “stupid” people), and no one
except a small child has the courage to tell him that there is no suit and
he’s parading around with nothing on.
In the same vein, not all Dermatology procedures are created equal, and
some are simply not covered by insurers for one reason or another. Here
are some of our most frequently denied procedures and the reasoning
behind the denials (you have to define “reasoning” loosely sometimes):
Like this newsletter? Have a story idea or suggestion? Contact the Editor at [email protected]. Contributions welcome!
COUNTDOWN TO EPIC
It’s coming...
It will be EPIC!
2 months 20 days 12 hours
or 81.5 days or 11.7 weeks
Quotes and Quips:
“Winter is not a season, it's an occupation.” - Sinclair Lewis
“The most common way people give up their power is by thinking they
don't have any.” - Alice Walker
Funny Coding Errors
We all make mistakes, but let’s admit it – some
mistakes are just funnier than others. :) Here are
a few coding ‘whoopsies!’ that have come up in
Derm in the last few months:
Female pt diagnosed with 606.1 – Oligospermia, aka low
sperm count***
Female pt diagnosed with 939.3 – Foreign body in penis
Male pt diagnosed with 646.5 – Asymptomatic bacteriuria
in pregnancy
Male pt diagnosed with 219.8 – Benign neoplasm, other
specified parts of uterus
Male pt diagnosed with 663.60 – Labor and delivery complicated by vascular lesion of cord
***Actually, that would be pretty accurate! (Insurance did not agree with me).
You know how you start on Wikipedia with
something specific in mind, and end up
someplace completely different (and totally
random)? Here are a few ICD-9 codes
discovered in a similar fashion:
787.62 – Fecal smearing (...um, where...?)
V61.10 – seven year itch (I wanted normal “itch,”
instead found marital problems)
935.2 – hairball in stomach (not just for cats!)
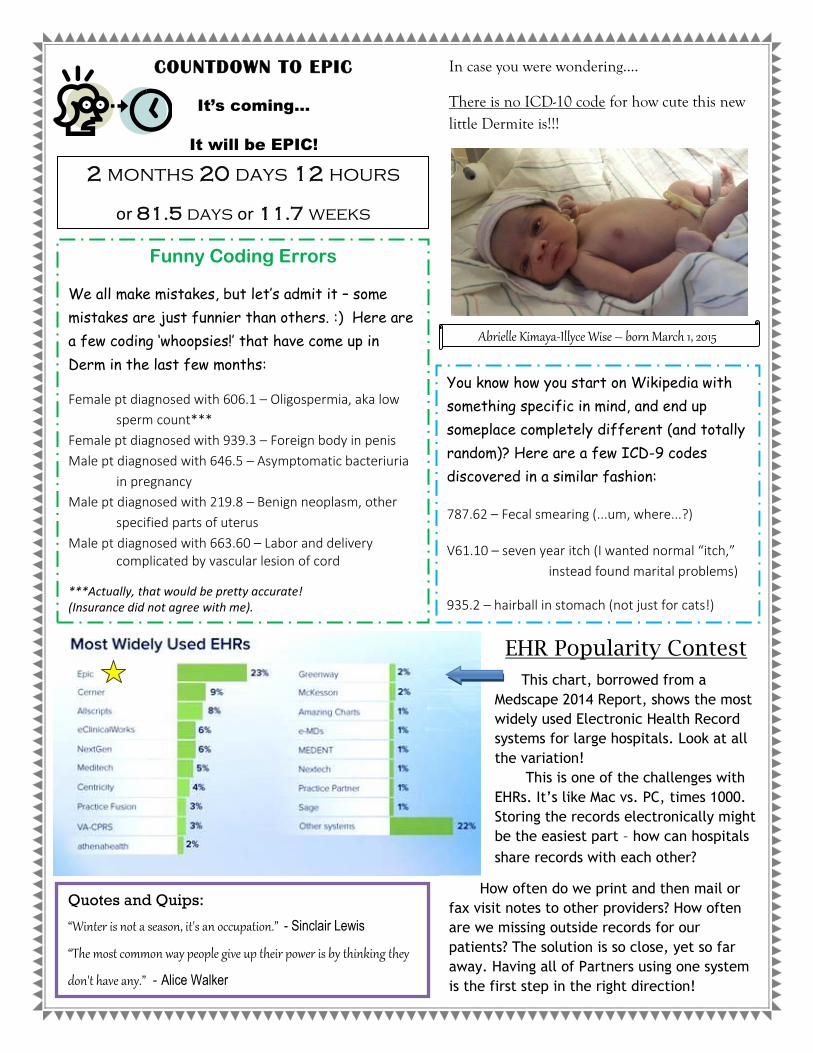
This chart, borrowed from a
Medscape 2014 Report, shows the most
widely used Electronic Health Record
systems for large hospitals. Look at all
the variation!
This is one of the challenges with
EHRs. It’s like Mac vs. PC, times 1000.
Storing the records electronically might
be the easiest part – how can hospitals
share records with each other?
How often do we print and then mail or
fax visit notes to other providers? How often
are we missing outside records for our
patients? The solution is so close, yet so far
away. Having all of Partners using one system
is the first step in the right direction!
In case you were wondering....
There is no ICD-10 code for how cute this new little Dermite is!!!
Abrielle Kimaya-Illyce Wise – born March 1, 2015
EHR Popularity Contest

Low-end estimate
total cost to
Partners
10
60,000 +
62
3.3 million
675
$1.2 billion
Hospitals across Partners
implementing Epic
720,000 +
1500
Employees across
Partners
Credentialed trainers
Super Users/Experts
at BWH & BWFH
Total training hours
across Partners
Patient records
currently in LMR
Freestanding applications
across Partners
WHAT DO I NEED TO KNOW BEFORE EPIC TRAINING?
Courtesy of Chris Landolt – [email protected]
With training beginning TODAY and only 81 days until Go-
Live, here are some basic concepts and policies you should
be familiar with:
In Basket: new form of clinical communication (comparable to Clinical Messages) – used for referrals, medication renewals, patient correspondence, etc.
Patient Gateway: name will remain the same, but functionality will expand with Epic’s MyChart.
Visit types: current visit types will be modified to accommodate new Epic requirements – NEW, RET, EXC, STR will be the only options for all sites/physicians, but will allow for new functionality to schedule accordingly for specialties.
PHS Viewer: limited view access of LMR through Epic to view past notes, medications, visits, etc.
Medications: active medications will need to be manually transferred from LMR to Epic
Hardware: new hardware will be installed and new functionality will exist for the following:
o Printing - Epic will only print to designated network printers which have been mapped accordingly for each device.
o eSignature Pads – front desks will be equipped to allow patients to electronically sign forms
o Check Reader – checks will be scanned at the front desk and funds will be deducted at the time of visit
o Scanning - outside medical records will be sent to HIS to scan
No Cash Policy: Partners will no longer be accepting cash. This communication to staff and patients will begin in the next couple months.
Specimen Collection: different labels must be printed to differentiate micro, path and point of care labs.
Patient Questionnaires/Pre-Visit Forms: new forms have been created to send out via PG, as well as at the time of check-in.
Related Documents











