ORIGINAL ARTICLE Derivation of a Risk Index for the Prediction of Massive Blood Transfusion in Liver Transplantation Stuart A. McCluskey, 1,2 Keyvan Karkouti, 1,3 Duminda N. Wijeysundera, 1 Karen Kakizawa, 1 Mohammed Ghannam, 1 Ahmed Hamdy, 1 David Grant, 2 and Gary Levy 2 1 Department of Anesthesia and Pain Management, 2 Multiorgan Transplant Program, University Health Network, and 3 Health Policy, Management, and Evaluation, University of Toronto, Toronto, Ontario, Canada Massive blood transfusion (MBT) remains a serious and common occurrence in liver transplantation surgery. This retrospective cohort study was undertaken to identify preoperative predictors of MBT and to develop a risk index for MBT in liver transplantation. Data were retrospectively collected on all liver transplantations carried out at a single institution between January 1998 and March 2004. Multivariable logistic regression analysis was used to identify independent predictor variables of MBT, defined as 6 units of red blood cell concentrate (RBC) in the first 24 hours of surgery. The model was internally validated by bootstrapping. Of the 460 liver transplant recipients, 193 (42%) received 6 units of RBC within 24 hours of surgery. Unadjusted analyses identified 12 preoperative predictors of MBT: age, height, gender, repeat transplantation, etiology of liver failure, and preoperative laboratory values (hemoglobin concentration, platelet count, international normalized ratio for prothrombin activity [INR], albumin, total bilirubin, and creatinine). In multivariable logistic regression, 7 independent predictors of MBT were identified: age (40 years), hemoglobin concentration (10.0 g/dL), INR (1.2-1.99, and 2.0), platelet count (70 10 9 /L), creatinine (110 mol/L for female subjects and 120 mol/L for male subjects), albumin ( 28 g/L), and repeat transplantation. The area under the receiver-operating characteristic curve (ROC) for the model was 0.82. By using the regression coefficients to derive weights for each of these predictors, a risk index was developed that assigned each patient a score between 0 and 8. The ROC for this risk index was 0.79. MBT in liver transplantation surgery can be accurately predicted by 7 readily available preoperative predictors. Liver Transpl 12:1584-1593, 2006. © 2006 AASLD. Received November 29, 2005; accepted May 16, 2006. Prevention of excessive blood loss is an important ob- jective in the perioperative management of liver trans- plantation surgery because it is associated with pro- longed recovery, increased morbidity, and reduced graft survival. 1,2 Over the last 20 years, changes in surgical and anesthetic management have reduced intraopera- tive blood transfusion in liver transplantation sur- gery. 3-5 Although massive transfusion remains a com- mon event, 10 to 50% of surgeries are conducted without requiring a blood transfusion. 2,3,5-8 To date, an accurate prediction rule for blood transfusion in liver transplantation surgery has not been developed. The lack of such an index precludes the tailoring of inven- tions aimed at reducing blood loss. One reason for the inability to predict blood loss in liver transplantation is that until recently, intraopera- tive variables leading to blood loss have been over- whelming, thus making transfusion requirements im- possible to predict. As a result of improvements in the intraoperative management, however, the relative im- portance of preoperative determinants of blood loss should have increased. Abbreviations: MBT, massive blood transfusion; RBC, red blood cell concentrate; INR, international normalized ratio for prothrombin activity; ROC, area under the receiver-operating characteristic curve; FFP, fresh frozen plasma; MELD, Model for End-Stage Liver Disease. Address reprint requests to Stuart A. McCluskey, MD, PhD, Department of Anesthesia and Pain Management, Toronto General Hospital, University Health Network, Eaton North 3-405, 200 Elizabeth Street, Toronto, Ontario, M5G 2C4, Canada. Telephone: 416-340-5164; FAX: 416-340-3698; E-mail: [email protected] DOI 10.1002/lt.20868 Published online in Wiley InterScience (www.interscience.wiley.com). LIVER TRANSPLANTATION 12:1584-1593, 2006 © 2006 American Association for the Study of Liver Diseases.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL ARTICLE
Derivation of a Risk Index for the Prediction ofMassive Blood Transfusion in LiverTransplantationStuart A. McCluskey,1,2 Keyvan Karkouti,1,3 Duminda N. Wijeysundera,1 Karen Kakizawa,1
Mohammed Ghannam,1 Ahmed Hamdy,1 David Grant,2 and Gary Levy2
1Department of Anesthesia and Pain Management, 2Multiorgan Transplant Program, University HealthNetwork, and 3Health Policy, Management, and Evaluation, University of Toronto, Toronto,Ontario, Canada
Massive blood transfusion (MBT) remains a serious and common occurrence in liver transplantation surgery. This retrospectivecohort study was undertaken to identify preoperative predictors of MBT and to develop a risk index for MBT in livertransplantation. Data were retrospectively collected on all liver transplantations carried out at a single institution betweenJanuary 1998 and March 2004. Multivariable logistic regression analysis was used to identify independent predictor variablesof MBT, defined as �6 units of red blood cell concentrate (RBC) in the first 24 hours of surgery. The model was internallyvalidated by bootstrapping. Of the 460 liver transplant recipients, 193 (42%) received �6 units of RBC within 24 hours ofsurgery. Unadjusted analyses identified 12 preoperative predictors of MBT: age, height, gender, repeat transplantation,etiology of liver failure, and preoperative laboratory values (hemoglobin concentration, platelet count, international normalizedratio for prothrombin activity [INR], albumin, total bilirubin, and creatinine). In multivariable logistic regression, 7 independentpredictors of MBT were identified: age (�40 years), hemoglobin concentration (�10.0 g/dL), INR (1.2-1.99, and �2.0), plateletcount (�70 � 109/L), creatinine (�110 �mol/L for female subjects and �120 �mol/L for male subjects), albumin (� 28 g/L),and repeat transplantation. The area under the receiver-operating characteristic curve (ROC) for the model was 0.82. By usingthe regression � coefficients to derive weights for each of these predictors, a risk index was developed that assigned eachpatient a score between 0 and 8. The ROC for this risk index was 0.79. MBT in liver transplantation surgery can be accuratelypredicted by 7 readily available preoperative predictors. Liver Transpl 12:1584-1593, 2006. © 2006 AASLD.
Received November 29, 2005; accepted May 16, 2006.
Prevention of excessive blood loss is an important ob-jective in the perioperative management of liver trans-plantation surgery because it is associated with pro-longed recovery, increased morbidity, and reduced graftsurvival.1,2 Over the last 20 years, changes in surgicaland anesthetic management have reduced intraopera-tive blood transfusion in liver transplantation sur-gery.3-5 Although massive transfusion remains a com-mon event, 10 to 50% of surgeries are conductedwithout requiring a blood transfusion.2,3,5-8 To date, anaccurate prediction rule for blood transfusion in liver
transplantation surgery has not been developed. Thelack of such an index precludes the tailoring of inven-tions aimed at reducing blood loss.
One reason for the inability to predict blood loss inliver transplantation is that until recently, intraopera-tive variables leading to blood loss have been over-whelming, thus making transfusion requirements im-possible to predict. As a result of improvements in theintraoperative management, however, the relative im-portance of preoperative determinants of blood lossshould have increased.
Abbreviations: MBT, massive blood transfusion; RBC, red blood cell concentrate; INR, international normalized ratio for prothrombinactivity; ROC, area under the receiver-operating characteristic curve; FFP, fresh frozen plasma; MELD, Model for End-Stage LiverDisease.Address reprint requests to Stuart A. McCluskey, MD, PhD, Department of Anesthesia and Pain Management, Toronto General Hospital, UniversityHealth Network, Eaton North 3-405, 200 Elizabeth Street, Toronto, Ontario, M5G 2C4, Canada. Telephone: 416-340-5164; FAX: 416-340-3698;E-mail: [email protected]
DOI 10.1002/lt.20868Published online in Wiley InterScience (www.interscience.wiley.com).
LIVER TRANSPLANTATION 12:1584-1593, 2006
© 2006 American Association for the Study of Liver Diseases.

The primary objectives of this study were to identifypreoperative predictors of massive blood transfusion(MBT) (�6 units red blood cell concentrate [RBC])within the first 24 hours of liver transplantation, and todevelop a risk index to predict MBT in liver transplan-tation.
MATERIALS AND METHODS
Population and Databases
After we received institutional ethics approval, datawere retrospectively collected on consecutive patientswho underwent liver transplantation (cadaveric or liv-ing-donor) between January 1, 1998, and March 31,2004, at the Toronto General Hospital, UniversityHealth Network (Toronto, Ontario, Canada). Databaseaccuracy was measured by reabstracting the medicalrecords of a randomly selected 10% (n � 50) of thestudy sample. In addition, outlying values were com-pared to patients’ records to identify and correct errorsin the database. Whenever possible, missing valueswere completed from the medical records; otherwise,patients with missing categorical variable values wereexcluded. For continuous variables, missing valueswere imputed on the basis of the mean for the entiresample.
Study Setting and Clinical Practice
The Toronto General Hospital is a tertiary-care teachinghospital affiliated with the University of Toronto. Theliver transplant program was started in 1985 and cur-rently conducts between 80 and 120 transplantationsper year. The live-donor program was initiated in May2000 and accounted for approximately 20% of livertransplantations in 2004. During the study period, pa-tients were managed according to standardized clinicalprotocols, as described below.
Anesthetic Procedure and Monitoring
The anesthetic induction and maintenance was per-formed with a combination of propofol, midazolam, fen-tanyl, and pancuronium. Patients were ventilated withan oxygen-air mixture. Hemodynamic monitoring con-sisted of an arterial line and a pulmonary artery cath-eter. Body temperature was maintained with warmingblankets and intravenous (IV) fluid warmers with a tar-get temperature of 36-37°C.
Surgical Procedures
The most common surgical technique involved the useof the donor inferior vena cava and is referred to as the“classic technique.” In live-donor transplantations andin cadaveric donor cases that were not able to tolerate acomplete inferior vena cava cross-clamp, the piggybacktechnique was used. Venovenous bypass was used inone case, which was excluded from the final analysis.
Blood Conservation Strategies
Cell salvage was used in all cases not involving hepato-cellular cancer or sepsis. Antifibrinolytic use was notstandardized and was used at the discretion of thesurgical team. Those patients that did receive antifi-brinolytics received 1 of 3 regimens: (1) tranexamic acid1 g as a single bolus, (2) tranexamic acid 10 mg/kg/huntil 2 hours after liver reperfusion, and (3) aprotinin1 � 106 KIU bolus followed by 0.5-1.0 � 106 KIU perhour until 2 hours after liver reperfusion.
Blood Transfusion Guidelines
Transfusion of RBC was based on clinical assessment,hemodynamic monitoring, and laboratory measure-ment of hemoglobin and hematocrit. The target hemo-globin concentration was 8.0-10.0 g/dL (hematocrit 25-30%). Cell saver units were used instead of RBC whenavailable, and all cell saver units were returned to thepatient.
Fresh frozen plasma (FFP) (2 units) was indicated foran international normalized ratio for prothrombin ac-tivity (INR) between 1.5 and 2.0 during the preanhe-patic phase or if associated with blood loss. If the INRexceeded 2.0, we administered 4 units of FFP beforerepeating a coagulation profile. Platelets (5 units) wereindicated to keep the platelet count above 80 � 109/L.Cryoprecipitate was indicated for fibrinogen level below1.0 g/L in the bleeding patient. Crystalloids, normalsaline, and colloids (10% Pentaspan, albumin 5%, andalbumin 25%) were used for volume replacement and tomaintain adequate urine output (� 0.5 mL/kg/h) at thediscretion of the attending anesthesiologist.
Outcome Measure
Blood transfusion data (RBC, FFP, platelets, cryopre-cipitate) were collected from the anesthesia, intensivecare unit, and transfusion records over the first 48hours after skin incision. These data were validated bycomparison with the hospital blood bank database(Hemocare). For the blood bank database, any bloodproduct issued and not returned was considered trans-fused.
Potential Predictor Variables and DependentVariables
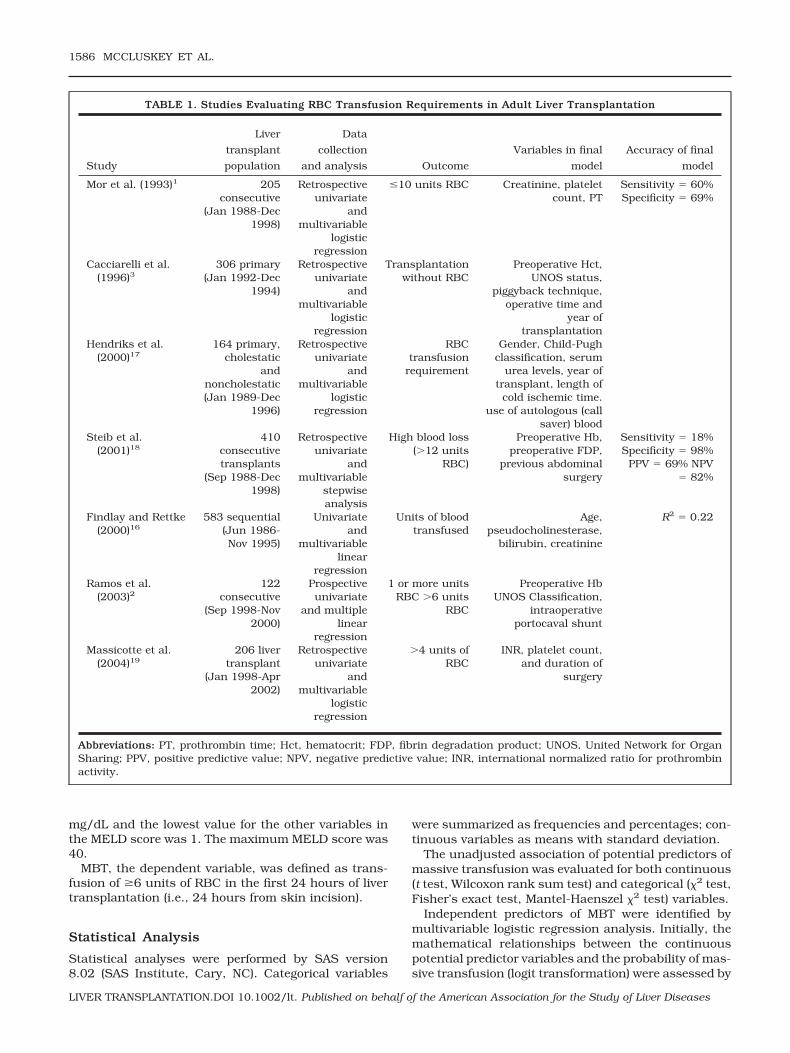
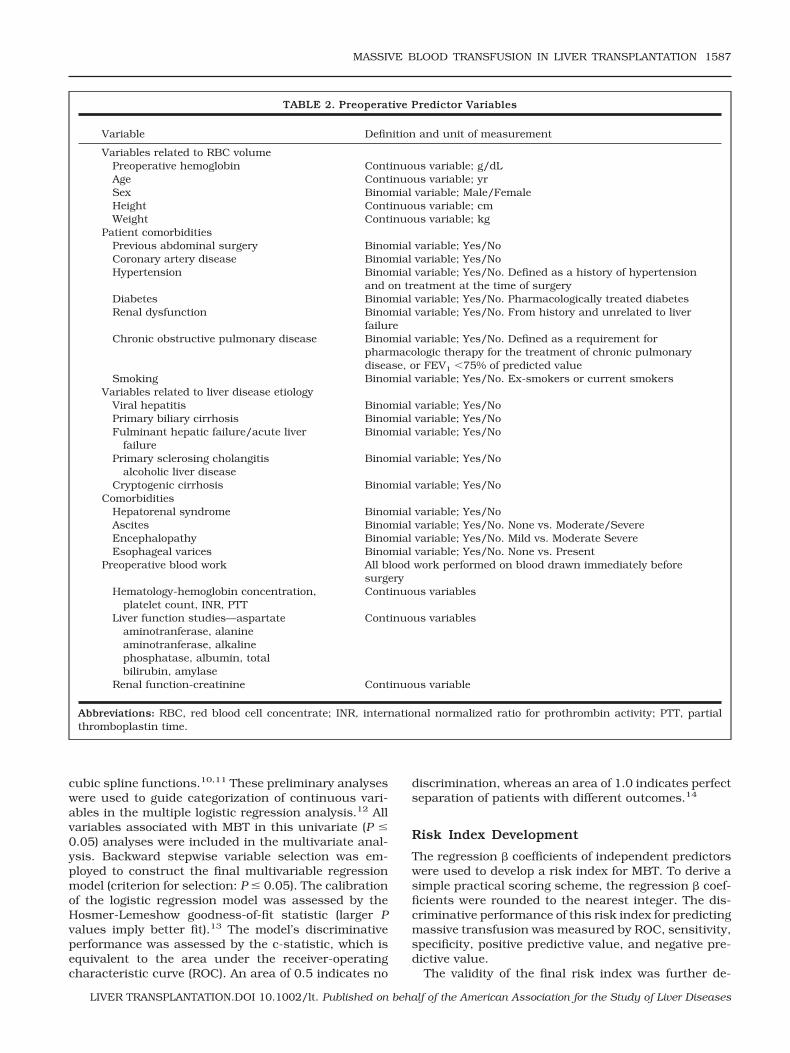
Potential preoperative predictors were selected on thebasis of a review of prior studies that attempted todefine predictors of blood loss in liver transplantation(Table 1). The variables used in this study are defined inTable 2.
The Model for End-Stage Liver Disease (MELD) scorehas not been adopted in Canada. The MELD score wascalculated from the immediate preoperative values forINR, serum creatinine, total bilirubin, and primary eti-ology of liver failure.9 The formula for the MELD score is3.8 ln(bilirubin [mg/dL]) � 11.2 ln(INR) � ln(creatinine[mg/dL]) � 6.4(etiology: 0 if cholestatic or alcoholic, 1otherwise). The highest value for creatinine was 4
MASSIVE BLOOD TRANSFUSION IN LIVER TRANSPLANTATION 1585
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
mg/dL and the lowest value for the other variables inthe MELD score was 1. The maximum MELD score was40.
MBT, the dependent variable, was defined as trans-fusion of �6 units of RBC in the first 24 hours of livertransplantation (i.e., 24 hours from skin incision).
Statistical Analysis
Statistical analyses were performed by SAS version8.02 (SAS Institute, Cary, NC). Categorical variables
were summarized as frequencies and percentages; con-tinuous variables as means with standard deviation.
The unadjusted association of potential predictors ofmassive transfusion was evaluated for both continuous(t test, Wilcoxon rank sum test) and categorical (�2 test,Fisher’s exact test, Mantel-Haenszel �2 test) variables.
Independent predictors of MBT were identified bymultivariable logistic regression analysis. Initially, themathematical relationships between the continuouspotential predictor variables and the probability of mas-sive transfusion (logit transformation) were assessed by
TABLE 1. Studies Evaluating RBC Transfusion Requirements in Adult Liver Transplantation
Study
Liver
transplant
population
Data
collection
and analysis Outcome
Variables in final
model
Accuracy of final
model
Mor et al. (1993)1 205consecutive
(Jan 1988-Dec1998)
Retrospectiveunivariate
andmultivariable
logisticregression
�10 units RBC Creatinine, plateletcount, PT
Sensitivity � 60%Specificity � 69%
Cacciarelli et al.(1996)3
306 primary(Jan 1992-Dec
1994)
Retrospectiveunivariate
andmultivariable
logisticregression
Transplantationwithout RBC
Preoperative Hct,UNOS status,
piggyback technique,operative time and
year oftransplantation
Hendriks et al.(2000)17
164 primary,cholestatic
andnoncholestatic(Jan 1989-Dec
1996)
Retrospectiveunivariate
andmultivariable
logisticregression
RBCtransfusion
requirement
Gender, Child-Pughclassification, serum
urea levels, year oftransplant, length ofcold ischemic time.
use of autologous (callsaver) blood
Steib et al.(2001)18
410consecutivetransplants
(Sep 1988-Dec1998)
Retrospectiveunivariate
andmultivariable
stepwiseanalysis
High blood loss(�12 units
RBC)
Preoperative Hb,preoperative FDP,
previous abdominalsurgery
Sensitivity � 18%Specificity � 98%
PPV � 69% NPV� 82%
Findlay and Rettke(2000)16
583 sequential(Jun 1986-Nov 1995)
Univariateand
multivariablelinear
regression
Units of bloodtransfused
Age,pseudocholinesterase,
bilirubin, creatinine
R2 � 0.22
Ramos et al.(2003)2
122consecutive
(Sep 1998-Nov2000)
Prospectiveunivariate
and multiplelinear
regression
1 or more unitsRBC �6 units
RBC
Preoperative HbUNOS Classification,
intraoperativeportocaval shunt
Massicotte et al.(2004)19
206 livertransplant
(Jan 1998-Apr2002)
Retrospectiveunivariate
andmultivariable
logisticregression
�4 units ofRBC
INR, platelet count,and duration of
surgery
Abbreviations: PT, prothrombin time; Hct, hematocrit; FDP, fibrin degradation product; UNOS, United Network for OrganSharing; PPV, positive predictive value; NPV, negative predictive value; INR, international normalized ratio for prothrombinactivity.
1586 MCCLUSKEY ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
cubic spline functions.10,11 These preliminary analyseswere used to guide categorization of continuous vari-ables in the multiple logistic regression analysis.12 Allvariables associated with MBT in this univariate (P �0.05) analyses were included in the multivariate anal-ysis. Backward stepwise variable selection was em-ployed to construct the final multivariable regressionmodel (criterion for selection: P � 0.05). The calibrationof the logistic regression model was assessed by theHosmer-Lemeshow goodness-of-fit statistic (larger Pvalues imply better fit).13 The model’s discriminativeperformance was assessed by the c-statistic, which isequivalent to the area under the receiver-operatingcharacteristic curve (ROC). An area of 0.5 indicates no
discrimination, whereas an area of 1.0 indicates perfectseparation of patients with different outcomes.14
Risk Index Development
The regression � coefficients of independent predictorswere used to develop a risk index for MBT. To derive asimple practical scoring scheme, the regression � coef-ficients were rounded to the nearest integer. The dis-criminative performance of this risk index for predictingmassive transfusion was measured by ROC, sensitivity,specificity, positive predictive value, and negative pre-dictive value.
The validity of the final risk index was further de-
TABLE 2. Preoperative Predictor Variables
Variable Definition and unit of measurement
Variables related to RBC volumePreoperative hemoglobin Continuous variable; g/dLAge Continuous variable; yrSex Binomial variable; Male/FemaleHeight Continuous variable; cmWeight Continuous variable; kg
Patient comorbiditiesPrevious abdominal surgery Binomial variable; Yes/NoCoronary artery disease Binomial variable; Yes/NoHypertension Binomial variable; Yes/No. Defined as a history of hypertension
and on treatment at the time of surgeryDiabetes Binomial variable; Yes/No. Pharmacologically treated diabetesRenal dysfunction Binomial variable; Yes/No. From history and unrelated to liver
failureChronic obstructive pulmonary disease Binomial variable; Yes/No. Defined as a requirement for
pharmacologic therapy for the treatment of chronic pulmonarydisease, or FEV1 �75% of predicted value
Smoking Binomial variable; Yes/No. Ex-smokers or current smokersVariables related to liver disease etiology
Viral hepatitis Binomial variable; Yes/NoPrimary biliary cirrhosis Binomial variable; Yes/NoFulminant hepatic failure/acute liver
failureBinomial variable; Yes/No
Primary sclerosing cholangitisalcoholic liver disease
Binomial variable; Yes/No
Cryptogenic cirrhosis Binomial variable; Yes/NoComorbidities
Hepatorenal syndrome Binomial variable; Yes/NoAscites Binomial variable; Yes/No. None vs. Moderate/SevereEncephalopathy Binomial variable; Yes/No. Mild vs. Moderate SevereEsophageal varices Binomial variable; Yes/No. None vs. Present
Preoperative blood work All blood work performed on blood drawn immediately beforesurgery
Hematology-hemoglobin concentration,platelet count, INR, PTT
Continuous variables
Liver function studies—aspartateaminotranferase, alanineaminotranferase, alkalinephosphatase, albumin, totalbilirubin, amylase
Continuous variables
Renal function-creatinine Continuous variable
Abbreviations: RBC, red blood cell concentrate; INR, international normalized ratio for prothrombin activity; PTT, partialthromboplastin time.
MASSIVE BLOOD TRANSFUSION IN LIVER TRANSPLANTATION 1587
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
scribed by bootstrap techniques. Initially, 1000 com-puter-generated samples, each including 459 individu-als (i.e., study sample less one patient), were derivedfrom the study sample by random selection with re-placement. The bootstrap samples were used to esti-mate the 95% confidence interval for the ROC for therisk index. The reliability of the independent predictorsincluded in the index was also described by bootstrapbagging. In summary, 1000 bootstrap samples weregenerated as described above. Within each bootstrapsample, forward stepwise variable selection (criterionfor inclusion: P � 0.05) was employed using all poten-tial independent variables. The reliability of predictorvariables in the final regression model was estimated byhow often they were retained as independent predictorsin the bootstrap samples. Reliable predictors were ex-pected to be retained in a higher proportion of bootstrapsamples.
RESULTS
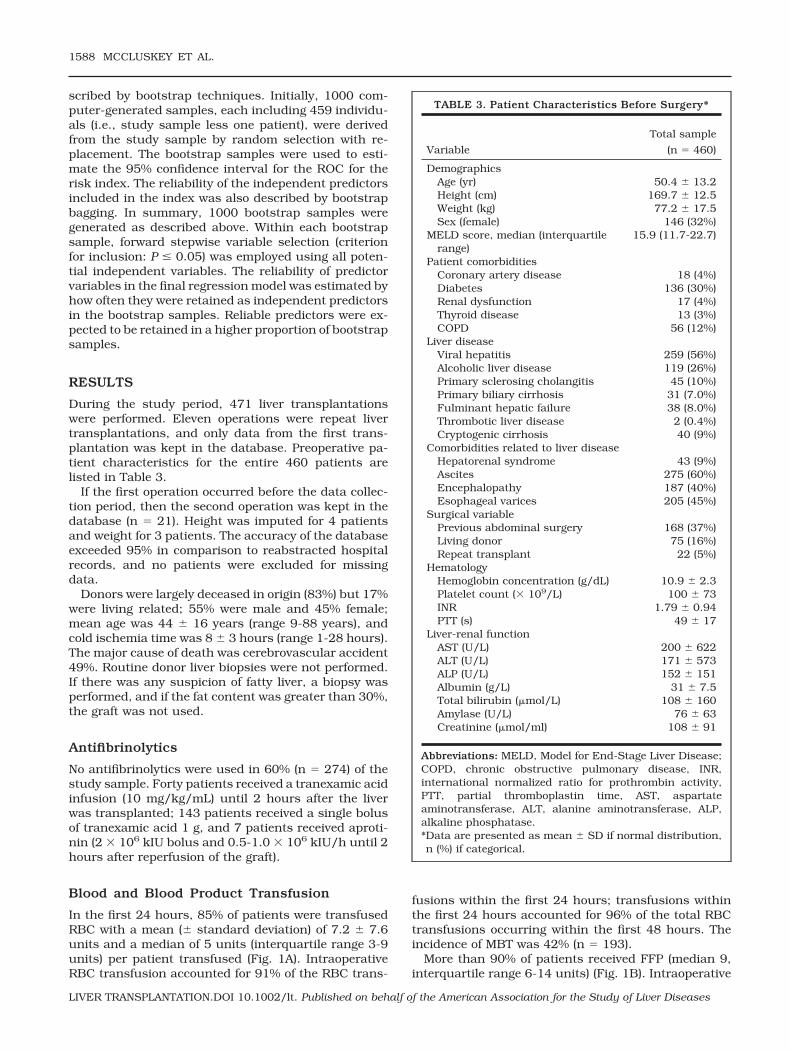
During the study period, 471 liver transplantationswere performed. Eleven operations were repeat livertransplantations, and only data from the first trans-plantation was kept in the database. Preoperative pa-tient characteristics for the entire 460 patients arelisted in Table 3.
If the first operation occurred before the data collec-tion period, then the second operation was kept in thedatabase (n � 21). Height was imputed for 4 patientsand weight for 3 patients. The accuracy of the databaseexceeded 95% in comparison to reabstracted hospitalrecords, and no patients were excluded for missingdata.
Donors were largely deceased in origin (83%) but 17%were living related; 55% were male and 45% female;mean age was 44 � 16 years (range 9-88 years), andcold ischemia time was 8 � 3 hours (range 1-28 hours).The major cause of death was cerebrovascular accident49%. Routine donor liver biopsies were not performed.If there was any suspicion of fatty liver, a biopsy wasperformed, and if the fat content was greater than 30%,the graft was not used.
Antifibrinolytics
No antifibrinolytics were used in 60% (n � 274) of thestudy sample. Forty patients received a tranexamic acidinfusion (10 mg/kg/mL) until 2 hours after the liverwas transplanted; 143 patients received a single bolusof tranexamic acid 1 g, and 7 patients received aproti-nin (2 � 106 kIU bolus and 0.5-1.0 � 106 kIU/h until 2hours after reperfusion of the graft).
Blood and Blood Product Transfusion
In the first 24 hours, 85% of patients were transfusedRBC with a mean (� standard deviation) of 7.2 � 7.6units and a median of 5 units (interquartile range 3-9units) per patient transfused (Fig. 1A). IntraoperativeRBC transfusion accounted for 91% of the RBC trans-
fusions within the first 24 hours; transfusions withinthe first 24 hours accounted for 96% of the total RBCtransfusions occurring within the first 48 hours. Theincidence of MBT was 42% (n � 193).
More than 90% of patients received FFP (median 9,interquartile range 6-14 units) (Fig. 1B). Intraoperative
TABLE 3. Patient Characteristics Before Surgery*
Variable
Total sample
(n � 460)
DemographicsAge (yr) 50.4 � 13.2Height (cm) 169.7 � 12.5Weight (kg) 77.2 � 17.5Sex (female) 146 (32%)
MELD score, median (interquartilerange)
15.9 (11.7-22.7)
Patient comorbiditiesCoronary artery disease 18 (4%)Diabetes 136 (30%)Renal dysfunction 17 (4%)Thyroid disease 13 (3%)COPD 56 (12%)
Liver diseaseViral hepatitis 259 (56%)Alcoholic liver disease 119 (26%)Primary sclerosing cholangitis 45 (10%)Primary biliary cirrhosis 31 (7.0%)Fulminant hepatic failure 38 (8.0%)Thrombotic liver disease 2 (0.4%)Cryptogenic cirrhosis 40 (9%)
Comorbidities related to liver diseaseHepatorenal syndrome 43 (9%)Ascites 275 (60%)Encephalopathy 187 (40%)Esophageal varices 205 (45%)
Surgical variablePrevious abdominal surgery 168 (37%)Living donor 75 (16%)Repeat transplant 22 (5%)
HematologyHemoglobin concentration (g/dL) 10.9 � 2.3Platelet count (� 109/L) 100 � 73INR 1.79 � 0.94PTT (s) 49 � 17
Liver-renal functionAST (U/L) 200 � 622ALT (U/L) 171 � 573ALP (U/L) 152 � 151Albumin (g/L) 31 � 7.5Total bilirubin (mol/L) 108 � 160Amylase (U/L) 76 � 63Creatinine (mol/ml) 108 � 91
Abbreviations: MELD, Model for End-Stage Liver Disease;COPD, chronic obstructive pulmonary disease, INR,international normalized ratio for prothrombin activity,PTT, partial thromboplastin time, AST, aspartateaminotransferase, ALT, alanine aminotransferase, ALP,alkaline phosphatase.*Data are presented as mean � SD if normal distribution,n (%) if categorical.
1588 MCCLUSKEY ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
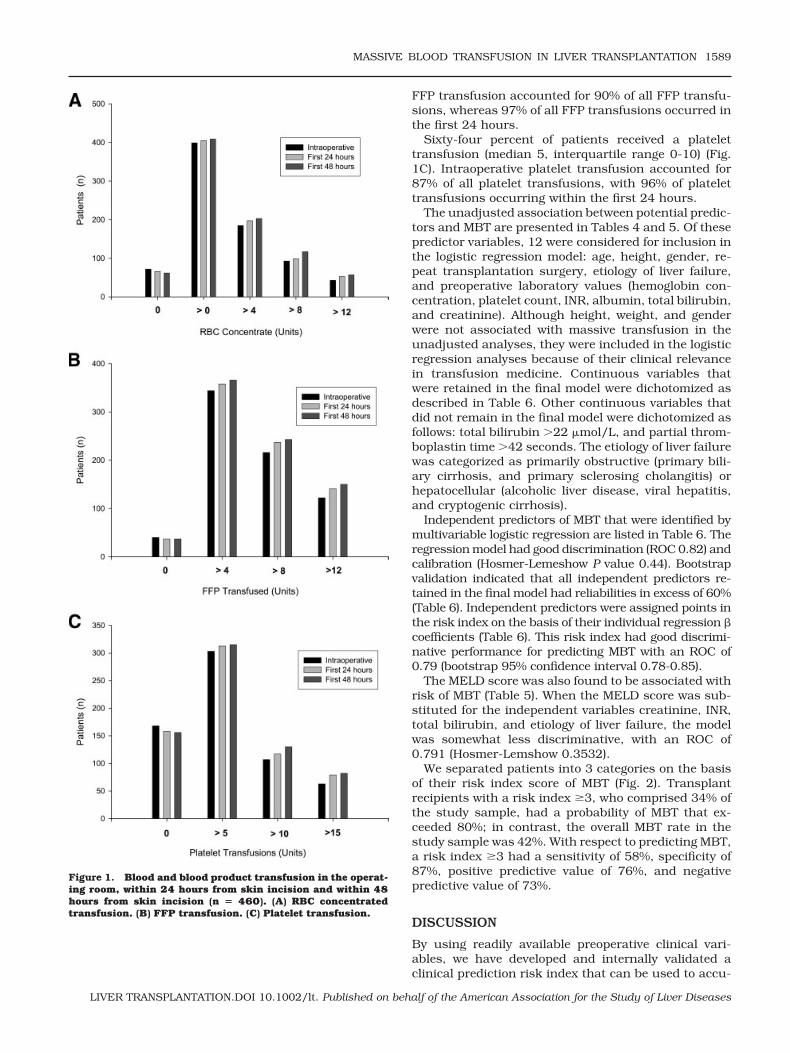
FFP transfusion accounted for 90% of all FFP transfu-sions, whereas 97% of all FFP transfusions occurred inthe first 24 hours.
Sixty-four percent of patients received a platelettransfusion (median 5, interquartile range 0-10) (Fig.1C). Intraoperative platelet transfusion accounted for87% of all platelet transfusions, with 96% of platelettransfusions occurring within the first 24 hours.
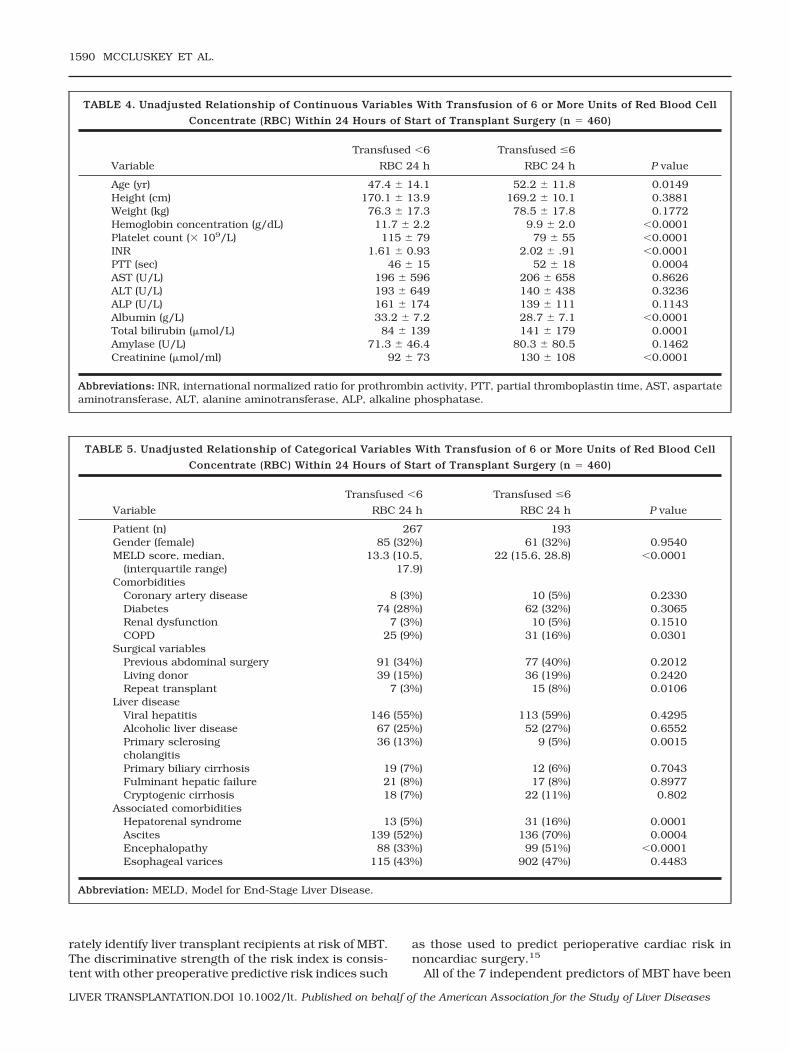
The unadjusted association between potential predic-tors and MBT are presented in Tables 4 and 5. Of thesepredictor variables, 12 were considered for inclusion inthe logistic regression model: age, height, gender, re-peat transplantation surgery, etiology of liver failure,and preoperative laboratory values (hemoglobin con-centration, platelet count, INR, albumin, total bilirubin,and creatinine). Although height, weight, and genderwere not associated with massive transfusion in theunadjusted analyses, they were included in the logisticregression analyses because of their clinical relevancein transfusion medicine. Continuous variables thatwere retained in the final model were dichotomized asdescribed in Table 6. Other continuous variables thatdid not remain in the final model were dichotomized asfollows: total bilirubin �22 mol/L, and partial throm-boplastin time �42 seconds. The etiology of liver failurewas categorized as primarily obstructive (primary bili-ary cirrhosis, and primary sclerosing cholangitis) orhepatocellular (alcoholic liver disease, viral hepatitis,and cryptogenic cirrhosis).
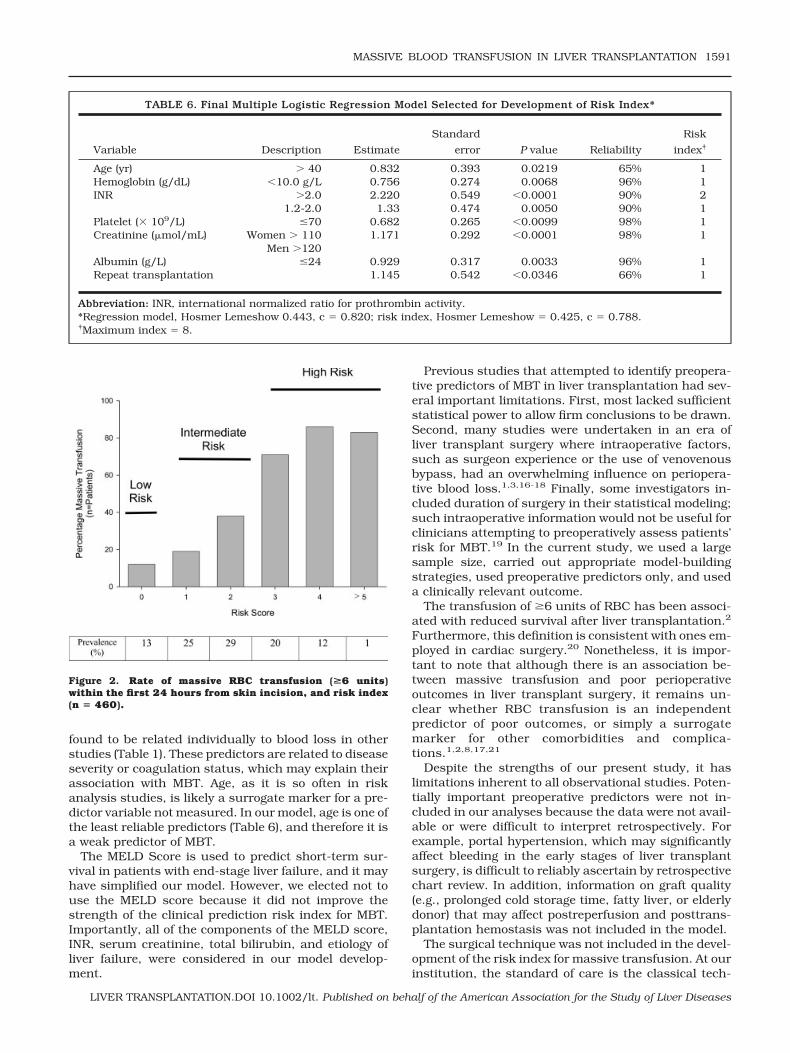
Independent predictors of MBT that were identified bymultivariable logistic regression are listed in Table 6. Theregression model had good discrimination (ROC 0.82) andcalibration (Hosmer-Lemeshow P value 0.44). Bootstrapvalidation indicated that all independent predictors re-tained in the final model had reliabilities in excess of 60%(Table 6). Independent predictors were assigned points inthe risk index on the basis of their individual regression �coefficients (Table 6). This risk index had good discrimi-native performance for predicting MBT with an ROC of0.79 (bootstrap 95% confidence interval 0.78-0.85).
The MELD score was also found to be associated withrisk of MBT (Table 5). When the MELD score was sub-stituted for the independent variables creatinine, INR,total bilirubin, and etiology of liver failure, the modelwas somewhat less discriminative, with an ROC of0.791 (Hosmer-Lemshow 0.3532).
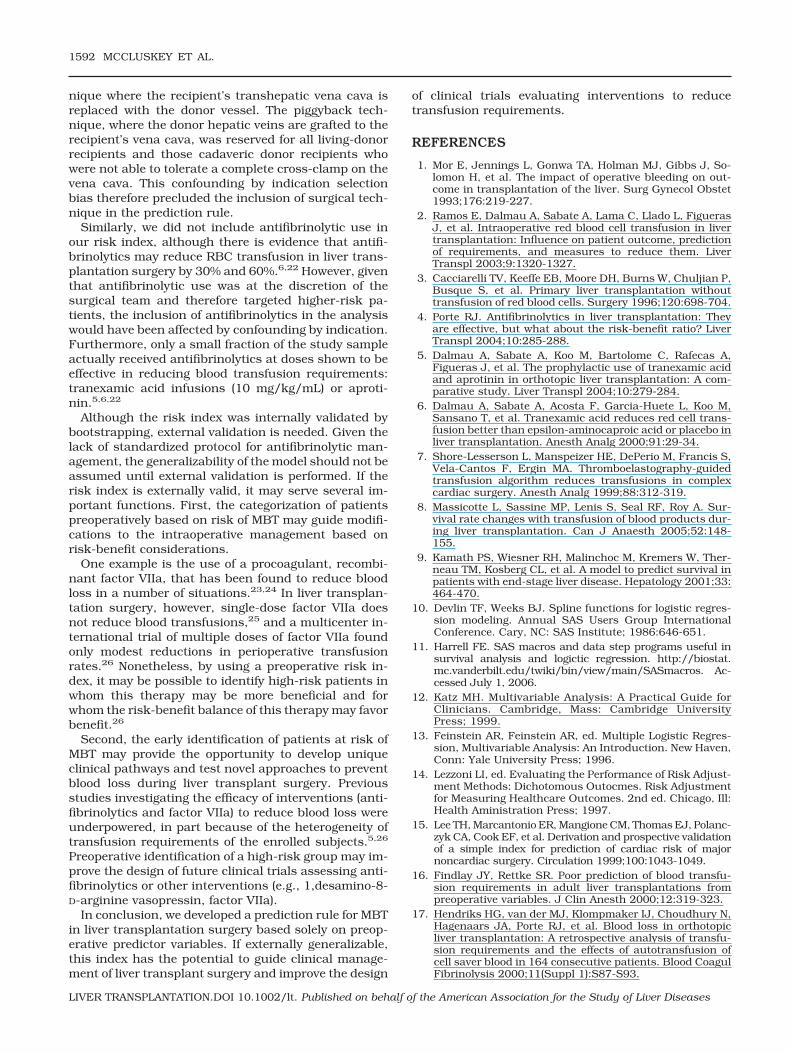
We separated patients into 3 categories on the basisof their risk index score of MBT (Fig. 2). Transplantrecipients with a risk index �3, who comprised 34% ofthe study sample, had a probability of MBT that ex-ceeded 80%; in contrast, the overall MBT rate in thestudy sample was 42%. With respect to predicting MBT,a risk index �3 had a sensitivity of 58%, specificity of87%, positive predictive value of 76%, and negativepredictive value of 73%.
DISCUSSION
By using readily available preoperative clinical vari-ables, we have developed and internally validated aclinical prediction risk index that can be used to accu-
Figure 1. Blood and blood product transfusion in the operat-ing room, within 24 hours from skin incision and within 48hours from skin incision (n � 460). (A) RBC concentratedtransfusion. (B) FFP transfusion. (C) Platelet transfusion.
MASSIVE BLOOD TRANSFUSION IN LIVER TRANSPLANTATION 1589
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
rately identify liver transplant recipients at risk of MBT.The discriminative strength of the risk index is consis-tent with other preoperative predictive risk indices such
as those used to predict perioperative cardiac risk innoncardiac surgery.15
All of the 7 independent predictors of MBT have been
TABLE 4. Unadjusted Relationship of Continuous Variables With Transfusion of 6 or More Units of Red Blood Cell
Concentrate (RBC) Within 24 Hours of Start of Transplant Surgery (n � 460)
Variable
Transfused �6
RBC 24 h
Transfused �6
RBC 24 h P value
Age (yr) 47.4 � 14.1 52.2 � 11.8 0.0149Height (cm) 170.1 � 13.9 169.2 � 10.1 0.3881Weight (kg) 76.3 � 17.3 78.5 � 17.8 0.1772Hemoglobin concentration (g/dL) 11.7 � 2.2 9.9 � 2.0 �0.0001Platelet count (� 109/L) 115 � 79 79 � 55 �0.0001INR 1.61 � 0.93 2.02 � .91 �0.0001PTT (sec) 46 � 15 52 � 18 0.0004AST (U/L) 196 � 596 206 � 658 0.8626ALT (U/L) 193 � 649 140 � 438 0.3236ALP (U/L) 161 � 174 139 � 111 0.1143Albumin (g/L) 33.2 � 7.2 28.7 � 7.1 �0.0001Total bilirubin (mol/L) 84 � 139 141 � 179 0.0001Amylase (U/L) 71.3 � 46.4 80.3 � 80.5 0.1462Creatinine (mol/ml) 92 � 73 130 � 108 �0.0001
Abbreviations: INR, international normalized ratio for prothrombin activity, PTT, partial thromboplastin time, AST, aspartateaminotransferase, ALT, alanine aminotransferase, ALP, alkaline phosphatase.
TABLE 5. Unadjusted Relationship of Categorical Variables With Transfusion of 6 or More Units of Red Blood Cell
Concentrate (RBC) Within 24 Hours of Start of Transplant Surgery (n � 460)
Variable
Transfused �6
RBC 24 h
Transfused �6
RBC 24 h P value
Patient (n) 267 193Gender (female) 85 (32%) 61 (32%) 0.9540MELD score, median,
(interquartile range)13.3 (10.5,
17.9)22 (15.6, 28.8) �0.0001
ComorbiditiesCoronary artery disease 8 (3%) 10 (5%) 0.2330Diabetes 74 (28%) 62 (32%) 0.3065Renal dysfunction 7 (3%) 10 (5%) 0.1510COPD 25 (9%) 31 (16%) 0.0301
Surgical variablesPrevious abdominal surgery 91 (34%) 77 (40%) 0.2012Living donor 39 (15%) 36 (19%) 0.2420Repeat transplant 7 (3%) 15 (8%) 0.0106
Liver diseaseViral hepatitis 146 (55%) 113 (59%) 0.4295Alcoholic liver disease 67 (25%) 52 (27%) 0.6552Primary sclerosingcholangitis
36 (13%) 9 (5%) 0.0015
Primary biliary cirrhosis 19 (7%) 12 (6%) 0.7043Fulminant hepatic failure 21 (8%) 17 (8%) 0.8977Cryptogenic cirrhosis 18 (7%) 22 (11%) 0.802
Associated comorbiditiesHepatorenal syndrome 13 (5%) 31 (16%) 0.0001Ascites 139 (52%) 136 (70%) 0.0004Encephalopathy 88 (33%) 99 (51%) �0.0001Esophageal varices 115 (43%) 902 (47%) 0.4483
Abbreviation: MELD, Model for End-Stage Liver Disease.
1590 MCCLUSKEY ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
found to be related individually to blood loss in otherstudies (Table 1). These predictors are related to diseaseseverity or coagulation status, which may explain theirassociation with MBT. Age, as it is so often in riskanalysis studies, is likely a surrogate marker for a pre-dictor variable not measured. In our model, age is one ofthe least reliable predictors (Table 6), and therefore it isa weak predictor of MBT.
The MELD Score is used to predict short-term sur-vival in patients with end-stage liver failure, and it mayhave simplified our model. However, we elected not touse the MELD score because it did not improve thestrength of the clinical prediction risk index for MBT.Importantly, all of the components of the MELD score,INR, serum creatinine, total bilirubin, and etiology ofliver failure, were considered in our model develop-ment.
Previous studies that attempted to identify preopera-tive predictors of MBT in liver transplantation had sev-eral important limitations. First, most lacked sufficientstatistical power to allow firm conclusions to be drawn.Second, many studies were undertaken in an era ofliver transplant surgery where intraoperative factors,such as surgeon experience or the use of venovenousbypass, had an overwhelming influence on periopera-tive blood loss.1,3,16-18 Finally, some investigators in-cluded duration of surgery in their statistical modeling;such intraoperative information would not be useful forclinicians attempting to preoperatively assess patients’risk for MBT.19 In the current study, we used a largesample size, carried out appropriate model-buildingstrategies, used preoperative predictors only, and useda clinically relevant outcome.
The transfusion of �6 units of RBC has been associ-ated with reduced survival after liver transplantation.2
Furthermore, this definition is consistent with ones em-ployed in cardiac surgery.20 Nonetheless, it is impor-tant to note that although there is an association be-tween massive transfusion and poor perioperativeoutcomes in liver transplant surgery, it remains un-clear whether RBC transfusion is an independentpredictor of poor outcomes, or simply a surrogatemarker for other comorbidities and complica-tions.1,2,8,17,21
Despite the strengths of our present study, it haslimitations inherent to all observational studies. Poten-tially important preoperative predictors were not in-cluded in our analyses because the data were not avail-able or were difficult to interpret retrospectively. Forexample, portal hypertension, which may significantlyaffect bleeding in the early stages of liver transplantsurgery, is difficult to reliably ascertain by retrospectivechart review. In addition, information on graft quality(e.g., prolonged cold storage time, fatty liver, or elderlydonor) that may affect postreperfusion and posttrans-plantation hemostasis was not included in the model.
The surgical technique was not included in the devel-opment of the risk index for massive transfusion. At ourinstitution, the standard of care is the classical tech-
TABLE 6. Final Multiple Logistic Regression Model Selected for Development of Risk Index*
Variable Description Estimate
Standard
error P value Reliability
Risk
index†
Age (yr) � 40 0.832 0.393 0.0219 65% 1Hemoglobin (g/dL) �10.0 g/L 0.756 0.274 0.0068 96% 1INR �2.0 2.220 0.549 �0.0001 90% 2
1.2-2.0 1.33 0.474 0.0050 90% 1Platelet (� 109/L) �70 0.682 0.265 �0.0099 98% 1Creatinine (mol/mL) Women � 110 1.171 0.292 �0.0001 98% 1
Men �120Albumin (g/L) �24 0.929 0.317 0.0033 96% 1Repeat transplantation 1.145 0.542 �0.0346 66% 1
Abbreviation: INR, international normalized ratio for prothrombin activity.*Regression model, Hosmer Lemeshow 0.443, c � 0.820; risk index, Hosmer Lemeshow � 0.425, c � 0.788.†Maximum index � 8.
Figure 2. Rate of massive RBC transfusion (>6 units)within the first 24 hours from skin incision, and risk index(n � 460).
MASSIVE BLOOD TRANSFUSION IN LIVER TRANSPLANTATION 1591
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
nique where the recipient’s transhepatic vena cava isreplaced with the donor vessel. The piggyback tech-nique, where the donor hepatic veins are grafted to therecipient’s vena cava, was reserved for all living-donorrecipients and those cadaveric donor recipients whowere not able to tolerate a complete cross-clamp on thevena cava. This confounding by indication selectionbias therefore precluded the inclusion of surgical tech-nique in the prediction rule.
Similarly, we did not include antifibrinolytic use inour risk index, although there is evidence that antifi-brinolytics may reduce RBC transfusion in liver trans-plantation surgery by 30% and 60%.6,22 However, giventhat antifibrinolytic use was at the discretion of thesurgical team and therefore targeted higher-risk pa-tients, the inclusion of antifibrinolytics in the analysiswould have been affected by confounding by indication.Furthermore, only a small fraction of the study sampleactually received antifibrinolytics at doses shown to beeffective in reducing blood transfusion requirements:tranexamic acid infusions (10 mg/kg/mL) or aproti-nin.5,6,22
Although the risk index was internally validated bybootstrapping, external validation is needed. Given thelack of standardized protocol for antifibrinolytic man-agement, the generalizability of the model should not beassumed until external validation is performed. If therisk index is externally valid, it may serve several im-portant functions. First, the categorization of patientspreoperatively based on risk of MBT may guide modifi-cations to the intraoperative management based onrisk-benefit considerations.
One example is the use of a procoagulant, recombi-nant factor VIIa, that has been found to reduce bloodloss in a number of situations.23,24 In liver transplan-tation surgery, however, single-dose factor VIIa doesnot reduce blood transfusions,25 and a multicenter in-ternational trial of multiple doses of factor VIIa foundonly modest reductions in perioperative transfusionrates.26 Nonetheless, by using a preoperative risk in-dex, it may be possible to identify high-risk patients inwhom this therapy may be more beneficial and forwhom the risk-benefit balance of this therapy may favorbenefit.26
Second, the early identification of patients at risk ofMBT may provide the opportunity to develop uniqueclinical pathways and test novel approaches to preventblood loss during liver transplant surgery. Previousstudies investigating the efficacy of interventions (anti-fibrinolytics and factor VIIa) to reduce blood loss wereunderpowered, in part because of the heterogeneity oftransfusion requirements of the enrolled subjects.5,26
Preoperative identification of a high-risk group may im-prove the design of future clinical trials assessing anti-fibrinolytics or other interventions (e.g., 1,desamino-8-D-arginine vasopressin, factor VIIa).
In conclusion, we developed a prediction rule for MBTin liver transplantation surgery based solely on preop-erative predictor variables. If externally generalizable,this index has the potential to guide clinical manage-ment of liver transplant surgery and improve the design
of clinical trials evaluating interventions to reducetransfusion requirements.
REFERENCES
1. Mor E, Jennings L, Gonwa TA, Holman MJ, Gibbs J, So-lomon H, et al. The impact of operative bleeding on out-come in transplantation of the liver. Surg Gynecol Obstet1993;176:219-227.
2. Ramos E, Dalmau A, Sabate A, Lama C, Llado L, FiguerasJ, et al. Intraoperative red blood cell transfusion in livertransplantation: Influence on patient outcome, predictionof requirements, and measures to reduce them. LiverTranspl 2003;9:1320-1327.
3. Cacciarelli TV, Keeffe EB, Moore DH, Burns W, Chuljian P,Busque S, et al. Primary liver transplantation withouttransfusion of red blood cells. Surgery 1996;120:698-704.
4. Porte RJ. Antifibrinolytics in liver transplantation: Theyare effective, but what about the risk-benefit ratio? LiverTranspl 2004;10:285-288.
5. Dalmau A, Sabate A, Koo M, Bartolome C, Rafecas A,Figueras J, et al. The prophylactic use of tranexamic acidand aprotinin in orthotopic liver transplantation: A com-parative study. Liver Transpl 2004;10:279-284.
6. Dalmau A, Sabate A, Acosta F, Garcia-Huete L, Koo M,Sansano T, et al. Tranexamic acid reduces red cell trans-fusion better than epsilon-aminocaproic acid or placebo inliver transplantation. Anesth Analg 2000;91:29-34.
7. Shore-Lesserson L, Manspeizer HE, DePerio M, Francis S,Vela-Cantos F, Ergin MA. Thromboelastography-guidedtransfusion algorithm reduces transfusions in complexcardiac surgery. Anesth Analg 1999;88:312-319.
8. Massicotte L, Sassine MP, Lenis S, Seal RF, Roy A. Sur-vival rate changes with transfusion of blood products dur-ing liver transplantation. Can J Anaesth 2005;52:148-155.
9. Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Ther-neau TM, Kosberg CL, et al. A model to predict survival inpatients with end-stage liver disease. Hepatology 2001;33:464-470.
10. Devlin TF, Weeks BJ. Spline functions for logistic regres-sion modeling. Annual SAS Users Group InternationalConference. Cary, NC: SAS Institute; 1986:646-651.
11. Harrell FE. SAS macros and data step programs useful insurvival analysis and logictic regression. http://biostat.mc.vanderbilt.edu/twiki/bin/view/main/SASmacros. Ac-cessed July 1, 2006.
12. Katz MH. Multivariable Analysis: A Practical Guide forClinicians. Cambridge, Mass: Cambridge UniversityPress; 1999.
13. Feinstein AR, Feinstein AR, ed. Multiple Logistic Regres-sion, Multivariable Analysis: An Introduction. New Haven,Conn: Yale University Press; 1996.
14. Lezzoni LI, ed. Evaluating the Performance of Risk Adjust-ment Methods: Dichotomous Outocmes. Risk Adjustmentfor Measuring Healthcare Outcomes. 2nd ed. Chicago, Ill:Health Aministration Press; 1997.
15. Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanc-zyk CA, Cook EF, et al. Derivation and prospective validationof a simple index for prediction of cardiac risk of majornoncardiac surgery. Circulation 1999;100:1043-1049.
16. Findlay JY, Rettke SR. Poor prediction of blood transfu-sion requirements in adult liver transplantations frompreoperative variables. J Clin Anesth 2000;12:319-323.
17. Hendriks HG, van der MJ, Klompmaker IJ, Choudhury N,Hagenaars JA, Porte RJ, et al. Blood loss in orthotopicliver transplantation: A retrospective analysis of transfu-sion requirements and the effects of autotransfusion ofcell saver blood in 164 consecutive patients. Blood CoagulFibrinolysis 2000;11(Suppl 1):S87-S93.
1592 MCCLUSKEY ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

18. Steib A, Freys G, Lehmann C, Meyer C, Mahoudeau G.Intraoperative blood losses and transfusion requirementsduring adult liver transplantation remain difficult to pre-dict. Can J Anaesth 2001;48:1075-1079.
19. Massicotte L, Sassine MP, Lenis S, Roy A. Transfusionpredictors in liver transplant. Anesth Analg 2004;98:1245-1251.
20. Karkouti K, Wijeysundera DN, Yau TM, Beattie WS, Ab-delnaem E, McCluskey SA, et al. The independent associ-ation of massive blood loss with mortality in cardiac sur-gery. Transfusion 2004;44:1453-1462.
21. Cacciarelli TV, Keeffe EB, Moore DH, Burns W, Busque S,Concepcion W, et al. Effect of intraoperative blood trans-fusion on patient outcome in hepatic transplantation.Arch Surg 1999;134:25-29.
22. Porte RJ, Molenaar IQ, Begliomini B, Groenland TH,Januszkiewicz A, Lindgren L, et al. Aprotinin and trans-fusion requirements in orthotopic liver transplantation:A multicentre randomised double-blind study. EMSALTStudy Group. Lancet 2000;355:1303-1309.
23. Karkouti K, Beattie WS, Wijeysundera DN, Yau TM, Mc-Cluskey SA, Ghannam M, et al. Recombinant factor VIIafor intractable blood loss after cardiac surgery: A propen-sity score-matched case-control analysis. Transfusion2005;45:26-34.
24. Mayer SA, Brun NC, Begtrup K, Davis SM, Diringer MN,Skolnick BE, et al. Recombinant activated factor VII foracute intracerebral hemorrhage. N Engl J Med 2005;352:777-785.
25. Planinsic RM, van der MJ, Testa G, Grande L, Candela A,Porte RJ, et al. Safety and efficacy of a single bolus admin-istration of recombinant factor VIIa in liver transplanta-tion due to chronic liver disease. Liver Transpl 2005;11:895-900.
26. Lodge JP, Jonas S, Jones RM, Olausson M, Mir-Pallardo J,Soefelt S, et al, for the rFVIIa OLT Study Group. Efficacyand safety of repeated perioperative doses of recombinantfactor VIIa in liver transplantation. Liver Transpl 2005;11:973-979.
MASSIVE BLOOD TRANSFUSION IN LIVER TRANSPLANTATION 1593
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
Related Documents











