Depression increasingly predicts mortality in the course of congestive heart failure Jana Jqnger a, * , Dieter Schellberg a , Thomas Mqller-Tasch a , Georg Raupp a , Christian Zugck b , Armin Haunstetter b , Stephan Zipfel a , Wolfgang Herzog a , Markus Haass b,c a Department of General Internal and Psychosomatic Medicine, University of Heidelberg, INF 410, D-69120 Heidelberg, Germany b Department of Cardiology, University of Heidelberg, Heidelberg, Germany c Department of Cardiology, Theresienkrankenhaus, Mannheim, Germany Received 8 August 2003; received in revised form 5 May 2004; accepted 24 May 2004 Available online 27 October 2004 Abstract Background: Congestive heart failure (CHF) is frequently associated with depression. However, the impact of depression on prognosis has not yet been sufficiently established. Aims: To prospectively investigate the influence of depression on mortality in patients with CHF. Methods: In 209 CHF patients depression was assessed by the Hospital Anxiety and Depression Scale (HADS-D). Results: Compared to survivors (n =164), non-survivors (n =45) were characterized by a higher New York Heart Association (NYHA) functional class (2.8F0.7 vs. 2.5F0.6), and a lower left ventricular ejection fraction (LVEF) (18F8 vs. 23F10%) and peakVO 2 (13.1F4.5 vs. 15.4F5.2 ml/kg/min) at baseline. Furthermore, non-survivors had a higher depression score (7.5F4.0 vs. 6.1F4.3) (all Pb0.05). After a mean follow-up of 24.8 months the depression score was identified as a significant indicator of mortality ( Pb0.01). In multivariate analysis the depression score predicted mortality independent from NYHA functional class, LVEF and peakVO 2 . Combination of depression score, LVEF and peakVO 2 allowed for a better risk stratification than combination of LVEF and peakVO 2 alone. The risk ratio for mortality in patients with an elevated depression score (i.e. above the median) rose over time to 8.2 after 30 months (CI 2.62–25.84). Conclusions: The depression score predicts mortality independent of somatic parameters in CHF patients not treated for depression. Its prognostic power increases over time and should, thus, be accounted for in risk stratification and therapy. D 2004 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. Keywords: Congestive heart failure; Depression; Prognosis; Mortality; Risk stratification 1. Introduction Despite advances in the treatment of congestive heart failure (CHF), this epidemic continues unabated worldwide [1,2]. The high morbidity and mortality as well as the marked decrease in quality of life [3] associated with CHF points to the need for increased attention towards additional risk factors for the course of CHF. While depression has been well-established as an independent risk factor for development of coronary artery disease [4] and as an independent predictor for its prognosis [5–7], only recently have the unfavorable effects that depression exerts on CHF been reported. Until the studies of Abramson et al. [8] and Williams et al. [9], it was not well understood that depression is a risk factor for predisposition to CHF. The few studies on the prognostic value of depression in CHF patients have shown inconsistent results. Two studies with an observation time of 6–12 months found no predictive value of depression after multivariate controlling for somatic 1388-9842/$ - see front matter D 2004 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejheart.2004.05.011 Abbreviations: CHF, Congestive heart failure; LVEF, Left ventricular ejection fraction; NYHA, New York Heart Association; PeakVO 2 , peak oxygen uptake in cardiopulmonary exercise testing; HADS-D, Hospital Anxiety and Depression Scale in German. * Corresponding author. Tel.: +49 6221 568657; fax: +49 6221 565749. E-mail address: Jana _ [email protected] (J. Jqnger). The European Journal of Heart Failure 7 (2005) 261 – 267 www.elsevier.com/locate/heafai at unihd on April 28, 2011 eurjhf.oxfordjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.elsevier.com/locate/heafai
The European Journal of Heart
Depression increasingly predicts mortality in the course of congestive
heart failure
Jana Jqngera,*, Dieter Schellberga, Thomas Mqller-Tascha, Georg Rauppa, Christian Zugckb,
Armin Haunstetterb, Stephan Zipfela, Wolfgang Herzoga, Markus Haassb,c
aDepartment of General Internal and Psychosomatic Medicine, University of Heidelberg, INF 410, D-69120 Heidelberg, GermanybDepartment of Cardiology, University of Heidelberg, Heidelberg, GermanycDepartment of Cardiology, Theresienkrankenhaus, Mannheim, Germany
Received 8 August 2003; received in revised form 5 May 2004; accepted 24 May 2004
Available online 27 October 2004
at unihd on April 28, 2011
eurjhf.oxfordjournals.orgD
ownloaded from
Abstract
Background: Congestive heart failure (CHF) is frequently associated with depression. However, the impact of depression on prognosis has
not yet been sufficiently established.
Aims: To prospectively investigate the influence of depression on mortality in patients with CHF.
Methods: In 209 CHF patients depression was assessed by the Hospital Anxiety and Depression Scale (HADS-D).
Results: Compared to survivors (n=164), non-survivors (n=45) were characterized by a higher New York Heart Association (NYHA)
functional class (2.8F0.7 vs. 2.5F0.6), and a lower left ventricular ejection fraction (LVEF) (18F8 vs. 23F10%) and peakVO2 (13.1F4.5
vs. 15.4F5.2 ml/kg/min) at baseline. Furthermore, non-survivors had a higher depression score (7.5F4.0 vs. 6.1F4.3) (all Pb0.05). After a
mean follow-up of 24.8 months the depression score was identified as a significant indicator of mortality (Pb0.01). In multivariate analysis
the depression score predicted mortality independent from NYHA functional class, LVEF and peakVO2. Combination of depression score,
LVEF and peakVO2 allowed for a better risk stratification than combination of LVEF and peakVO2 alone. The risk ratio for mortality in
patients with an elevated depression score (i.e. above the median) rose over time to 8.2 after 30 months (CI 2.62–25.84).
Conclusions: The depression score predicts mortality independent of somatic parameters in CHF patients not treated for depression. Its
prognostic power increases over time and should, thus, be accounted for in risk stratification and therapy.
D 2004 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
Keywords: Congestive heart failure; Depression; Prognosis; Mortality; Risk stratification
1. Introduction
Despite advances in the treatment of congestive heart
failure (CHF), this epidemic continues unabated worldwide
[1,2]. The high morbidity and mortality as well as the
marked decrease in quality of life [3] associated with CHF
1388-9842/$ - see front matter D 2004 European Society of Cardiology. Publishe
doi:10.1016/j.ejheart.2004.05.011
Abbreviations: CHF, Congestive heart failure; LVEF, Left ventricular
ejection fraction; NYHA, New York Heart Association; PeakVO2, peak
oxygen uptake in cardiopulmonary exercise testing; HADS-D, Hospital
Anxiety and Depression Scale in German.
* Corresponding author. Tel.: +49 6221 568657; fax: +49 6221 565749.
E-mail address: [email protected] (J. Jqnger).
points to the need for increased attention towards additional
risk factors for the course of CHF. While depression has
been well-established as an independent risk factor for
development of coronary artery disease [4] and as an
independent predictor for its prognosis [5–7], only recently
have the unfavorable effects that depression exerts on CHF
been reported. Until the studies of Abramson et al. [8] and
Williams et al. [9], it was not well understood that
depression is a risk factor for predisposition to CHF. The
few studies on the prognostic value of depression in CHF
patients have shown inconsistent results. Two studies with
an observation time of 6–12 months found no predictive
value of depression after multivariate controlling for somatic
Failure 7 (2005) 261–267
d by Elsevier B.V. All rights reserved.

J. Junger et al. / The European Journal of Heart Failure 7 (2005) 261–267262
parameters [10,11], while another showed a predictive value
of depression after 24 months [12]. However, none of these
studies controlled for the established predictors, peakVO2
and left ventricular ejection fraction (LVEF), simultane-
ously. For the latter two a highly predictive value concern-
ing mortality was shown recently in a simple two-variable
model [13].
The first aim of the present study was to test the
hypothesis that depression independently predicts mortality
in patients with CHF, even after adjusting for established
clinical risk variables and concomitant beta-blocking
medication and to show that entering information on
depression score into a model comprising peakVO2 and
LVEF would increase the overall risk stratification. The
second aim was to measure the interaction of the predictive
effect of depression with time.
at unihd on April 28, 2011
eurjhf.oxfordjournals.orgD
ownloaded from
2. Methods
Two hundred and nine patients with stable CHF (New
York Heart Association (NYHA) functional classes I–III)
were prospectively enrolled into the study through the
Department of Cardiology at the University of Heidelberg
between March 1996 and March 1999, after giving written
informed consent. The study complied with the Declaration
of Helsinki and was approved by the Ethics Committee for
human research of the University of Heidelberg.
The cardiac diagnosis was based on left heart catheter-
ization and coronary angiograms prior to enrollment. The
major inclusion criterion was LVEF V45%, as determined
by radionuclide ventriculography [13,14]. Patients in
NYHA functional class IV were excluded, as were those
who had neurological, orthopedic, peripheral vascular or
severe pulmonary diseases, which may have impaired
successful completion of exercise testing (i.e. determination
of peakVO2 by cardiopulmonary exercise testing) [13].
Patients who were not able to speak German fluently were
also excluded.
NYHA functional class was determined by an independ-
ent investigator prior to assessment of somatic variables.
Furthermore, the investigator who applied the standard
Hospital Anxiety and Depression Scale in German (HADS-
D) questionnaires was blinded to the aforementioned data.
All parameters were collected within a period of 48 h.
3. Depression and anxiety
Patients’ self assessment of depression and anxiety were
determined at baseline by the German version of the
Hospital Anxiety and Depression Scale, the HADS-D [15,
16], a validated and reliable 14 item checklist (7 items for
depression and 7 items for anxiety) well-established among
cardiac patients [15]. It has one scale-score for depression
and one for anxiety. Patients with z8 points on the
depression scale are suspected of having depression and
with z10 points of having anxiety [15,16]. As there is no
validated prognostic cutoff point, the median of the
HADS-D depression score was used for survival-analysis.
For analysis of risk stratification, the continuous variable
was used.
4. Predictor and outcome variable
The primary independent, or predictor, variable of
interest was the depression score from the baseline assess-
ment. The primary endpoint was all-cause mortality, defined
as death due to any cause. The dependent variable was time
from baseline to the endpoint (death) or time until trans-
plantation or termination of the study. In this context the
status of censored has to be defined. All patients undergoing
cardiac transplantation were considered as survivors until
the date of the transplantation.
5. Endpoint monitoring
We obtained endpoint information during regular out-
patient visits or by telephone calls to the patients’ home or
their family physician. Information on endpoint status was
available for all patients at the pre-established time point
(i.e. July 2001). Depression was only assessed at baseline.
Mean observation time was 24.8 months (range: minimum
0.6 to maximum 36 months). The predefined endpoint was
all-cause mortality. Death without transplantation was
defined as an outcome event. All patients undergoing
cardiac transplantation were considered as survivors until
the date of their transplantation regardless of the post-
operative outcome.
6. Statistical analysis
Statistical analysis was performed with standard soft-
ware (SAS version 6.09). Spearman rank correlation
coefficient was used as a measure of association between
variables. A nonparametric two-sample Wilcoxon test was
used to test for differences between groups (survivors vs.
non-survivors). Survival curves were calculated using the
Kaplan–Meier method [17]. Multivariate Cox proportional
hazards analysis was used to identify the most important
predictors of mortality [18]. The log of the negative log
survival curves stratified according to the HADS-D
depression median was used to evaluate the basic propor-
tional hazards assumption of the Cox-model for depression.
This assumption was violated, as the curves did not run
parallel (not shown). Standardized Schoenfeld-smoothed
residuals were analysed to demonstrate the functional form
of interaction between depression and its effect on mortality
over time, as proposed by Grambsch and Therneau [19].
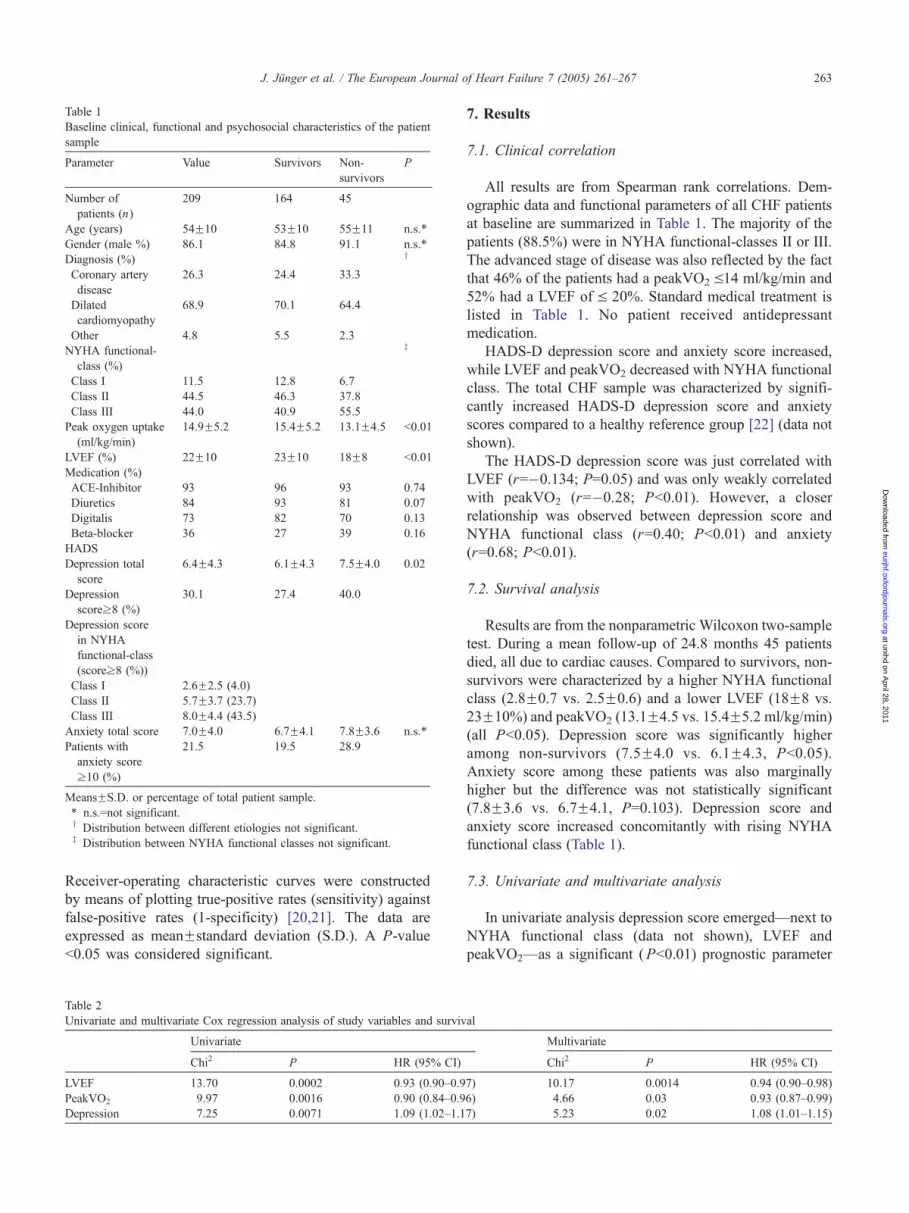
Table 1
Baseline clinical, functional and psychosocial characteristics of the patient
sample
Parameter Value Survivors Non-
survivors
P
Number of
patients (n)
209 164 45
Age (years) 54F10 53F10 55F11 n.s.*
Gender (male %) 86.1 84.8 91.1 n.s.*
Diagnosis (%) y
Coronary artery
disease
26.3 24.4 33.3
Dilated
cardiomyopathy
68.9 70.1 64.4
Other 4.8 5.5 2.3
NYHA functional-
class (%)
z
Class I 11.5 12.8 6.7
Class II 44.5 46.3 37.8
Class III 44.0 40.9 55.5
Peak oxygen uptake
(ml/kg/min)
14.9F5.2 15.4F5.2 13.1F4.5 b0.01
LVEF (%) 22F10 23F10 18F8 b0.01
Medication (%)
ACE-Inhibitor 93 96 93 0.74
Diuretics 84 93 81 0.07
Digitalis 73 82 70 0.13
Beta-blocker 36 27 39 0.16
HADS
Depression total
score
6.4F4.3 6.1F4.3 7.5F4.0 0.02
Depression
scorez8 (%)
30.1 27.4 40.0
Depression score
in NYHA
functional-class
(scorez8 (%))
Class I 2.6F2.5 (4.0)
Class II 5.7F3.7 (23.7)
Class III 8.0F4.4 (43.5)
Anxiety total score 7.0F4.0 6.7F4.1 7.8F3.6 n.s.*
Patients with
anxiety score
z10 (%)
21.5 19.5 28.9
MeansFS.D. or percentage of total patient sample.
* n.s.=not significant.y Distribution between different etiologies not significant.z Distribution between NYHA functional classes not significant.
J. Junger et al. / The European Journal of Heart Failure 7 (2005) 261–267 263
at unihd on April 28, 2011
eurjhf.oxfordjournals.orgD
ownloaded from
Receiver-operating characteristic curves were constructed
by means of plotting true-positive rates (sensitivity) against
false-positive rates (1-specificity) [20,21]. The data are
expressed as meanFstandard deviation (S.D.). A P-value
b0.05 was considered significant.
Table 2
Univariate and multivariate Cox regression analysis of study variables and surviv
Univariate
Chi2 P HR (95% CI)
LVEF 13.70 0.0002 0.93 (0.90–0.9
PeakVO2 9.97 0.0016 0.90 (0.84–0.9
Depression 7.25 0.0071 1.09 (1.02–1.1
7. Results
7.1. Clinical correlation
All results are from Spearman rank correlations. Dem-
ographic data and functional parameters of all CHF patients
at baseline are summarized in Table 1. The majority of the
patients (88.5%) were in NYHA functional-classes II or III.
The advanced stage of disease was also reflected by the fact
that 46% of the patients had a peakVO2 V14 ml/kg/min and
52% had a LVEF of V 20%. Standard medical treatment is
listed in Table 1. No patient received antidepressant
medication.
HADS-D depression score and anxiety score increased,
while LVEF and peakVO2 decreased with NYHA functional
class. The total CHF sample was characterized by signifi-
cantly increased HADS-D depression score and anxiety
scores compared to a healthy reference group [22] (data not
shown).
The HADS-D depression score was just correlated with
LVEF (r=�0.134; P=0.05) and was only weakly correlated
with peakVO2 (r=�0.28; Pb0.01). However, a closer
relationship was observed between depression score and
NYHA functional class (r=0.40; Pb0.01) and anxiety
(r=0.68; Pb0.01).
7.2. Survival analysis
Results are from the nonparametric Wilcoxon two-sample
test. During a mean follow-up of 24.8 months 45 patients
died, all due to cardiac causes. Compared to survivors, non-
survivors were characterized by a higher NYHA functional
class (2.8F0.7 vs. 2.5F0.6) and a lower LVEF (18F8 vs.
23F10%) and peakVO2 (13.1F4.5 vs. 15.4F5.2 ml/kg/min)
(all Pb0.05). Depression score was significantly higher
among non-survivors (7.5F4.0 vs. 6.1F4.3, Pb0.05).
Anxiety score among these patients was also marginally
higher but the difference was not statistically significant
(7.8F3.6 vs. 6.7F4.1, P=0.103). Depression score and
anxiety score increased concomitantly with rising NYHA
functional class (Table 1).
7.3. Univariate and multivariate analysis
In univariate analysis depression score emerged—next to
NYHA functional class (data not shown), LVEF and
peakVO2—as a significant (Pb0.01) prognostic parameter
al
Multivariate
Chi2 P HR (95% CI)
7) 10.17 0.0014 0.94 (0.90–0.98)
6) 4.66 0.03 0.93 (0.87–0.99)
7) 5.23 0.02 1.08 (1.01–1.15)

J. Junger et al. / The European Journal of Heart Failure 7 (2005) 261–267264
(Table 2). Kaplan–Meier survival curves of depression,
LVEF and peakVO2 divided according to the cutoff-values
(median) are shown in Fig. 1a, b and c. Multivariate Cox
proportional hazard analysis revealed that the depression
score predicted prognosis independent of LVEF and
peakVO2 (Table 2). The combination of depression score,
peakVO2 and LVEF allowed a better risk stratification than
the combination of the established parameters LVEF and
peakVO2 alone (Chi-square 24.93 vs. 20.24, Pb0.001).
Fig. 1. Kaplan–Meier survival curves of the total study population divided
according to cutoff-values (median). (a) HADS-D depression score, cutoff 6
points; Log rank chi-square 11.20, P=0.0008. (b) LVEF, cutoff 20%; Log-
rank chi-square 8.08, P=0.0045. (c) PeakVO2, cutoff 14 ml/min/kg; Log
rank chi-square 6.90, P=0.0086.
Fig. 2. Receiver-operating characteristic curves of prediction of survival at
36 months. The combination of HADS-D depression score, LVEF and
peakVO2 (AUC, 0.831) yields significantly more prognostic information
than combination of LVEF and peakVO2 alone (AUC, 0.774). n=45
patients died within 36 months, n=164 survived; area-test one-tailed
Pb0.0028.
at unihd on April 28, 2011
eurjhf.oxfordjournals.orgD
ownloaded from
Controlling for medication (ACE-inhibitors, diuretics,
digitalis and beta-blockers) and etiolgy (ischaemic vs.
dilated cardiomyopathy) in a multivariable Cox regression
model, the effects of LVEF, peakVO2 and HADS depres-
sion score remained significant and unaltered in size. None
of the former variables controlled for turned out as
significant.
7.4. Receiver-operating characteristic curves for survival at
36 months
After maximum follow-up of 36 months, parameters
identified as independent predictors by multivariate Cox
regression analysis were entered into receiver operating
characteristic analysis: By adding depression score to the
combination of LVEF and peakVO2, risk prediction
improved significantly (Fig. 2).
7.5. Analysis of the time-dependent mortality-risk of
depression
As shown in Table 3, mortality-risk associated with
depression score rises over time. When calculating the
hazard ratios over time, it becomes clear that depression
exerts almost no risk in the first year of follow-up and rises
to an 8-fold level after 30 months (Table 3).
Table 3
Time-dependent risk ratios for mortality for patients with a HADS-D
depression score N6
Survival time in months Chi2 P HR (95% CI)
6 0.01 0.950 1.03 (0.44–2.39)
12 2.71 0.100 1.73 (0.90–3.32)
18 10.18 0.001 2.91 (1.51–5.60)
24 13.34 b0.001 4.90 (2.09–11.45)
24.8 (mean observation time) 13.40 b0.001 5.24 (2.16–12.72)
30 13.01 b0.001 8.22 (2.62–25.84)

J. Junger et al. / The European Journal of Heart Failure 7 (2005) 261–267 265
at unihd on April 28, 2011
eurjhf.oxfordjournals.orgD
ownloaded from
8. Discussion
In this study, depression was an important independent
risk factor for mortality of CHF patients. In multivariate
analysis, depression score predicted prognosis independ-
ent of NYHA functional class, LVEF and peakVO2, as
well as etiology and concomitant medication. The
combination of depression score, LVEF and peakVO2
allowed for a better risk stratification than the combina-
tion of the established parameters LVEF and peakVO2
alone.
In previous studies the investigators focused primarily on
the impact of depression on prognosis without controlling
simultaneously for the established prognostic parameters
LVEF and peakVO2 [10–12]. The studies showed a
predictive value of depression for combined endpoints such
as mortality and re-hospitalization [10] or death and
functional decline [11]. However, after controlling for
multiple variables (such as NYHA functional class, LVEF,
age) and focusing on the single endpoint mortality the
results lost their statistic significance [10,11]. In the more
recent studies of Jiang et al. [10] and Vaccarino et al. [11]
the observation time of CHF patients was restricted to 1
year. Also, Koenig [23] found no prognostic value of
depression after an observation time of 1 year. Faris et al.
[24] showed reduced survival of patients with non-
ischaemic heart failure and depression over a long obser-
vation period of 5 years. However, peakVO2 was available
only in 37% of the study population and the diagnosis of
depression was based on a clinical diagnosis through review
of patients’ medical records, not on an established instru-
ment or questionnaire.
In the present study, patients were followed over a mean
of 24.8 months. The main effect of depression on mortality
began at the end of the first year of observation. This time-
dependent development of the prognostic effect of depres-
sion in patients with CHF was shown here for the first time.
In a previous study we were able to show that patients with
an endstage heart failure and an additional increased
preoperative depression score showed an unfavorable out-
come after heart transplantation, particularly in the long-
term course [25]. Denollet and Brutsaert [26] state an odds
ratio for cardiac death of 7.5 after myocardial infarction
with a reduced LVEF in patients with negative affectivity,
which is part of depressive pathology, after the long
observation period of 6 to 10 years. So, both studies show
depression as a predictor of mortality in the long run.
Abramson et al. [8] found that depression independently
predicts the onset of CHF in patients with isolated systolic
hypertension over an observation period of 4.5 years.
Finally, a study by Fredman et al. [27] showed an
association of depression with mortality in elderly women
that was much stronger after 6 years than after just 2 years.
Thus the effect of depression on mortality seems to develop
over time and might only be recognized in long-term
observation.
There are several mechanisms that could account for the
association between depression and increased heart failure
mortality. In patients with depression, hypercortisolism and
an activation of the sympathetic nervous system can be
observed [28], as well as elevated levels of cytokines [29],
which in turn are predictive factors for CHF mortality
[30,31]. Also, patients with depression show reduced heart
rate variability [32]. Higher platelet activity and consec-
utively an increased risk for cardiovascular events has also
been shown in some studies [4,33]. However, the present
study found no significant difference in the prognostic effect
of depression regarding ischemic or non-ischemic etiology
of heart failure. Likewise, Abramson et al. [8] found that
depression retained its predictive power for the risk of
developing CHF even after controlling for a history of
myocardial infarction.
In addition to these factors, psychological explanations
linking depression and increased mortality in heart failure
are being discussed. Patients with depression are known to
have poor social contacts and support networks [25,34].
Additionally, they show a reduced compliance with treat-
ment because of an appreciable degree of hopelessness,
withdrawal from the social network, with a subsequent loss
of emotional support and possible reductions in the
cognitive functioning essential for following treatment
recommendations [35]. All the above mentioned factors
might increase the risk of non-compliance with medication
regimens and thus increase the risk of cardiac decompensa-
tion [35,36].
8.1. Limitations of the study
This study was performed at a tertiary referral center.
Thus the current CHF sample does not represent the typical
CHF population seen by a general practitioner. The
majority of CHF-patients in a general practitioner’s
practice are characterized by a smaller impairment in
LVEF, a higher prevalence of coronary artery disease, and
an older age [37]. Also, there was a very high proportion
of male patients in this sample. The clinical diagnosis of
depressive disorder cannot be made with the HADS-D.
However, the HADS-D has been shown to be a reliable
and valid screening instrument for depressive symptoms in
general internal patients [15]. Additionally, it seemed
important to select a simple, clinically applicable instru-
ment that could be completed by the patients themselves
and that could easily be used for screening and follow-up
in other centers.
Since the analysis of the prognostic impact of the HADS-
D was restricted to a single timepoint (baseline), it cannot be
ruled out that the depression score further increased
especially in those patients with a depression score above
the median at baseline. Furthermore, as the patients were not
being treated for depression, the present study allows no
conclusion on the prognostic impact of specifically coping
with depression.

J. Junger et al. / The European Journal of Heart Failure 7 (2005) 261–267266
9. Conclusions
The present findings are of major clinical importance.
Screening for depression is a simple, well-established, non-
invasive method that a patient can self-administer. The
HADS-D offers the physician not only information about
the psychological status of a patient with CHF, but also
prognostic information that is independent of somatic
parameters.
While at the physical level excellent pharmacological
treatments are available to improve prognosis, a diagnosis of
depression is also a state of impaired health that needs to be
treated by pharmacological and/or psychotherapeutic
means. As the negative effect of depression on prognosis
seems to evolve slowly, there may be sufficient time to
initiate this treatment. If these findings are confirmed by
future studies, the influence on risk stratification for these
patients should be investigated.
eurjhD
ownloaded from
Acknowledgements
This study was supported by grants from the faculty for
clinical medicine of the University of Heidelberg (projects
32/95 and 158/97).
at unihd on April 28, 2011
f.oxfordjournals.org
References
[1] Ho KK, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart
failure: the Framingham Study. J Am Coll Cardiol 1993;22:6A–13A.
[2] O’Connell JB. The economic burden of heart failure. Clin Cardiol
2000;23(III):6–10.
[3] Juenger J, Schellberg D, Kraemer D, et al. Health related quality of life
in patients with congestive heart failure: comparison with other chronic
diseases and relation to functional variables. Heart 2002;87:235–41.
[4] Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological
factors on the pathogenesis of cardiovascular disease and implications
for therapy. Circulation 1999;99:2192–217.
[5] Ariyo AA, Haan M, Tangen CM, et al. Depressive symptoms and
risks of coronary heart disease and mortality in elderly Americans
Cardiovascular Health Study Collaborative Research Group. Circu-
lation 2000;102:1773–9.
[6] Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term
mortality risk in patients with coronary artery disease. Am J Cardiol
1996;78:613–7.
[7] Frasure-Smith N, Lesperance F. Coronary artery disease, depression
and social support only the beginning. Eur Heart J 2000;21:1043–5.
[8] Abramson J, Berger AC, Krumholz HM, Vaccarino V. Depression and
risk of heart failure among older persons with isolated systolic
hypertension. Arch Intern Med 2001;161:1725–30.
[9] Williams SA, Kasl SV, Heiat A, Abramson JL, Krumholz HM,
Vaccarino V. Depression and risk of heart failure among the elderly: a
prospective community-based study. Psychosom Med 2002;64:6–12.
[10] Jiang W, Alexander J, Christopher E, et al. Relationship of depression
to increased risk of mortality and rehospitalization in patients with
congestive heart failure. Arch Intern Med 2001;161:1849–56.
[11] Vaccarino V, Kasl SV, Abramson J, Krumholz HM. Depressive
symptoms and risk of functional decline and death in patients with
heart failure. J Am Coll Cardiol 2001;38:199–205.
[12] Murberg TA, Bru E, Svebak S, Tveteras R, Aarsland T. Depressed
mood and subjective health symptoms as predictors of mortality in
patients with congestive heart failure: a two-year follow-up study. Int J
Psychiatry Med 1999;29:311–26.
[13] Zugck C, Krqger C, Kell R, et al. Risk stratification in middle-aged
patients with congestive heart failure: prospective comparison of the
Heart Failure Survival Score (HFSS) and a simplified two-variable
model. Eur J Heart Fail 2001;3:577–85.
[14] Meyer FJ, Borst MM, Zugck C, et al. Respiratory muscle dysfunction
in congestive heart failure: clinical correlation and prognostic
significance. Circulation 2001;103:2153–8.
[15] Herrmann C. International experiences with the Hospital Anxiety and
Depression Scale—a review of validation data and clinical results.
J Psychosom Res 1997;42:17–41.
[16] Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the
Hospital Anxiety and Depression Scale. An updated literature review.
J Psychosom Res 2002;52:69–77.
[17] Kaplan EL, Meier P. Nonparametric estimation from incomplete
observations. J Am Stat Assoc 1958;53:457–81.
[18] Cox DR. Regression Models and Life-Tables. JR Stat Soc 1972;Series
B 34:187–202.
[19] Grambsch P, Therneau T. Proportional hazards tests and diagnostics
based on weighted residuals. Biometrika 1994;81(3):515–26.
[20] Metz CE, Wang P, Kronman H. A new approach for testing the
significance of differences between ROC curves measured from
correlated data. In: Deconinck F, editor. Information processing in
medical imaging. The Hague7 Martinus Nijhoff; 1984. p. 432–45.
[21] Metz CE, Herman BA, Roe CA. Statistical comparison of two ROC-
curve estimates obtained from partially-paired datasets. Med Decis
Making 1998;18:110–21.
[22] Hinz A, Schwarz R. Anxiety and depression in the general population:
normal values in the Hospital Anxiety and Depression Scale.
Psychother Psychosom Med Psychol 2001;51:193–200.
[23] Koenig HG. Depression in hospitalized older patients with congestive
heart failure. Gen Hosp Psychiatry 1998;20:29–43.
[24] Faris R, Purcell H, Henein MY, Coats AJ. Clinical depression is
common and significantly associated with reduced survival in
patients with non-ischaemic heart failure. Eur J Heart Fail 2002;4:
541–51.
[25] Zipfel S, Schneider A, Wild B, et al. Effect of depressive symptoms
on survival after heart transplantation. Psychosom Med 2002;64(5):
740–7.
[26] Denollet J, Brutsaert DL. Personality, disease severity, and the
risk of long-term cardiac events in patients with a decreased
ejection fraction after myocardial infarction. Circulation 1998;97:
167–73.
[27] Fredman L, Magaziner J, Hebel JR, Hawkes W, Zimmerman SI.
Depressive symptoms and 6-year mortality among elderly commun-
ity-dwelling women. Epidemiology 1999;10:54–9.
[28] Musselman DL, Evans DL, Nemeroff CB. The relationship of
depression to cardiovascular disease: epidemiology, biology, and
treatment. Arch Gen Psychiatry 1998;55:580–92.
[29] Gold PW, Chrousos GP. The endocrinology of melancholic and
atypical depression: relation to neurocircuitry and somatic consequen-
ces. Proc Assoc Am Physicians 1999;111:22–34.
[30] Cohn JN, Johnson GR, Shabetai R, et al. Ejection fraction, peak
exercise oxygen consumption, cardiothoracic ratio, ventricular
arrhythmias, and plasma norepinephrine as determinants of prognosis
in heart failure. The V-HeFT VA Cooperative Studies Group.
Circulation 1993;87:VI5–16.
[31] Kell R, Haunstetter A, Dengler TJ, Zugck C, Kqbler W, Haass M. Do
cytokines enable risk stratification to be improved in NYHA functional
class III patients? Comparison with other potential predictors of prog-
nosis. Eur Heart J 2002;23:70–8.
[32] Gorman JM, Sloan RP. Heart rate variability in depressive and anxiety
disorders. Am Heart J 2000;140:S77–83.

J. Junger et al. / The European Journal of Heart Failure 7 (2005) 261–267 267
[33] Musselman DL, Tomer A, Manatunga AK, et al. Exaggerated platelet
reactivity in major depression. Am J Psychiatry 1996;153:1313–7.
[34] Dracup K, Walden JA, Stevenson LW, Brecht ML. Quality of life in
patients with advanced heart failure. J Heart Lung Transplant 1992;
11:273–9.
[35] DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor
for noncompliance with medical treatment: meta-analysis of the
effects of anxiety and depression on patient adherence. Arch Intern
Med 2000;160:2101–7.
[36] Michalsen A, Konig G, Thimme W. Preventable causative factors
leading to hospital admission with decompensated heart failure. Heart
1998;80:437–41.
[37] Cowie MR, Mosterd A, Wood DA, et al. The epidemiology of heart
failure. Eur Heart J 1997;18:208–25.
at unihd on April 28, 2011
eurjhf.oxfordjournals.orgD
ownloaded from
Related Documents











